(21) Fluid Theraphy - Dr. Pangku
68
Fluid Therapy Dr. Pangkuwidjaja P
description
fluid
Transcript of (21) Fluid Theraphy - Dr. Pangku

Fluid Therapy
Dr. Pangkuwidjaja P

Exsanguination
Predictors of death
• Estimated blood loss > 5,000 mls• Red cell transfusion > 4,000 mls• Total blood transfusion > 5,000 mls
OR fluid transfusion > 12,000 mls• Transfusion rates > 12 mls/min
– pH < 7.2– Temp < 34ºC– HCO3 < 15 mmol/l
Trauma and surgery Alters volumes and composition of IC and EC
spaces
Therapeutic infusion further alters compartmental volumes
and composition

Emergency Resuscitation
• How much?
• What Fluid?
• Which Endpoints?
Goals of Fluid Administration
• Maintain good tissue perfusion• Maintain adequate oxygen delivery• Normal electrolyte concentration• Normoglycemia & pH
Goal of Fluid Resuscitation
↑ Cardiac Output↓Hb
DaO2
CO x CaO2
(Hb x SaO2 x 1,34) + (PaO2 x 0,003)
BP = CO x SVR
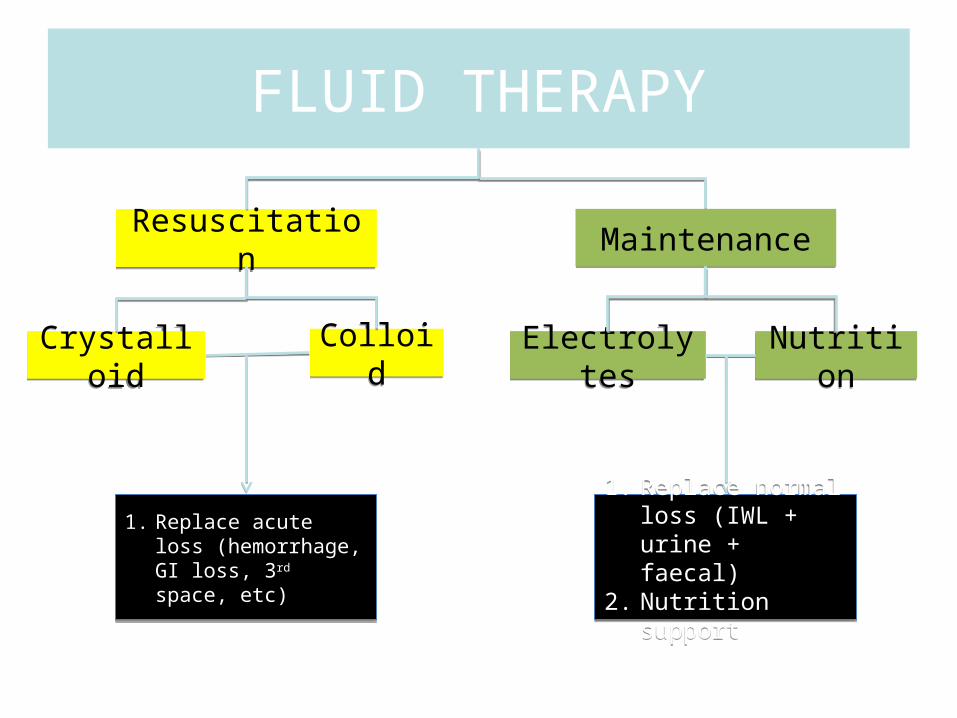
FLUID THERAPY
MaintenanceResuscitation
Electrolytes NutritionColloidCrystalloid
1. Replace acute loss (hemorrhage, GI loss, 3rd space, etc)
1. Replace normal loss (IWL + urine + faecal)
2. Nutrition support
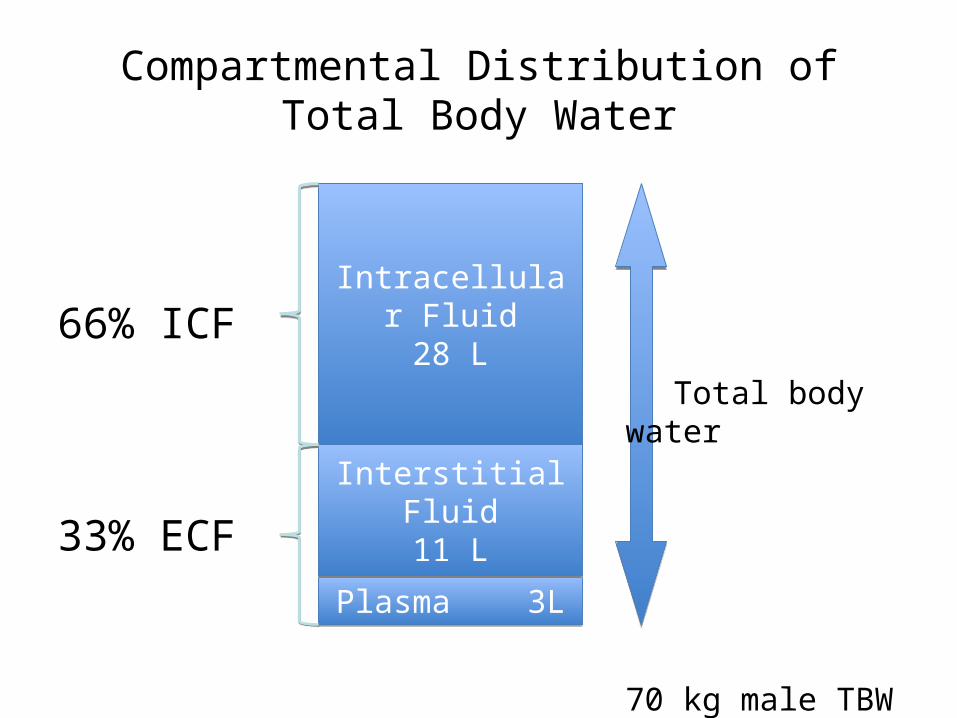
Compartmental Distribution of Total Body Water
66% ICF
33% ECF
Intracellular Fluid28 L
Plasma 3L
Interstitial Fluid11 L
Total body water
70 kg male TBW 42 L

Water HomeostasisIngested fluids 1300Solid food 800Metabolic water 400
Skin 500Lungs 400
Urine 1500Faeces 100
ICF ECF

Solute Composition of Body Fluid Compartments
280 – 310 mOsm/l
Solutes Solutes
Na+ 10 HPO4- Na+ 140 Cl- 114K+ 150 SO4-- K+ 4 SO4--30Mg++ 4 HCO3-
Prot
Water Water
ICF ECF
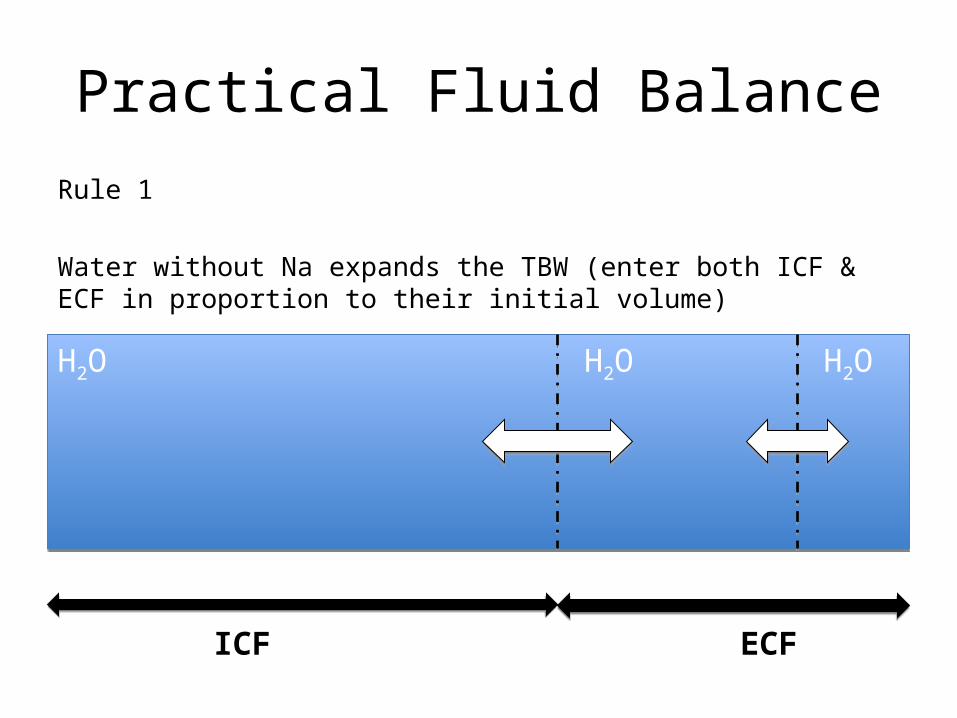
Practical Fluid BalanceRule 1
Water without Na expands the TBW (enter both ICF & ECF in proportion to their initial volume)
H2O H2O H2O
ICF ECF

Practical Fluid BalanceRule 2
All infused Na+ can not gain access to the ICF because of the Sodium Pump
Na+
Na+
Na+
Na+
Na+
Na+
ICF ECFIsotonic = NO Water Exchange
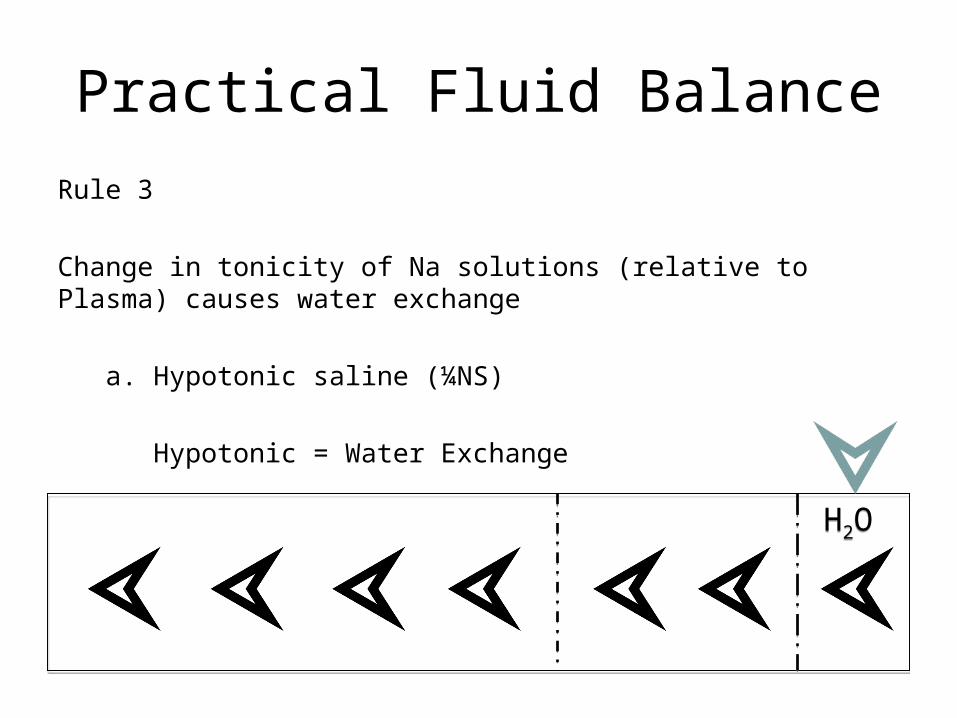
Practical Fluid BalanceRule 3
Change in tonicity of Na solutions (relative to Plasma) causes water exchange
a. Hypotonic saline (¼NS)
Hypotonic = Water Exchange
H2O
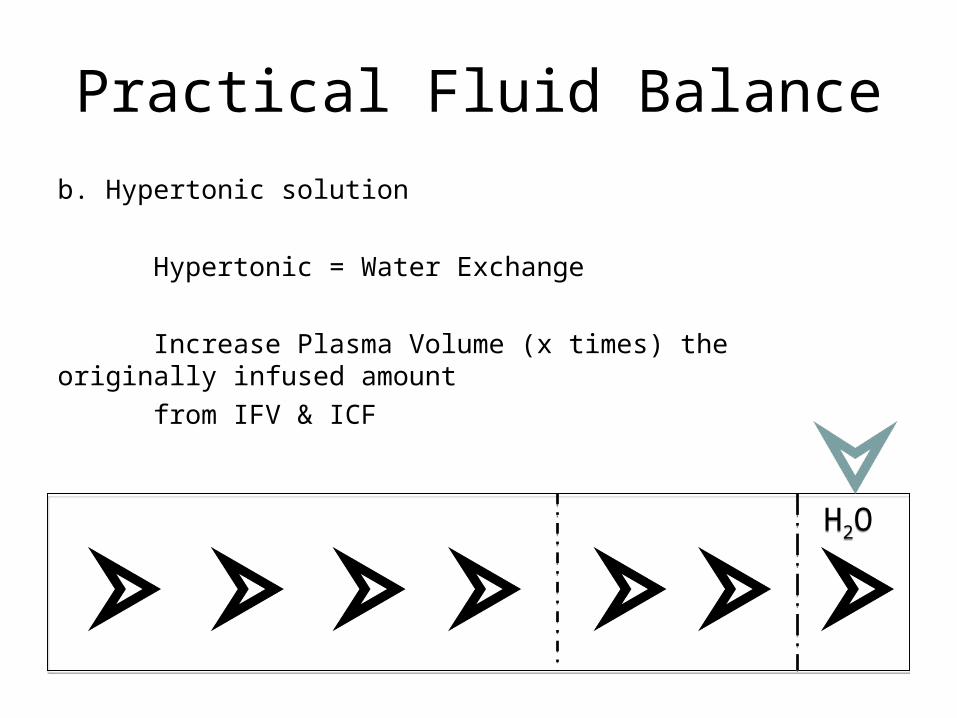
Practical Fluid Balanceb. Hypertonic solution
Hypertonic = Water Exchange
Increase Plasma Volume (x times) the originally infused amount
from IFV & ICF
H2O

Dynamics of IV Fluids
• Water solution IntracellularlyAll hypotonic solutions e.g. 5% dextrose called as maintenance type of fluids
• Electrolyte solutionsInterstitial compartmentIsotonicCalled replacement of fluids
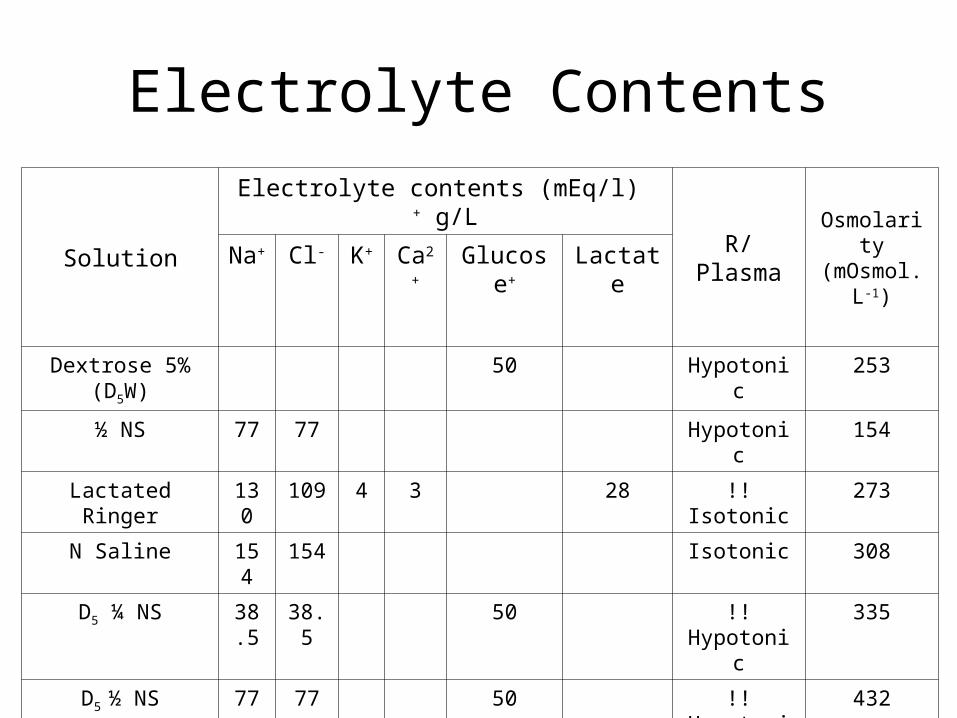
Electrolyte Contents
Solution
Electrolyte contents (mEq/l) + g/L
R/PlasmaOsmolarity(mOsmol.L-
1)Na
+Cl- K+ Ca2
+Glucose+ Lactate
Dextrose 5% (D5W)
50 Hypotonic 253
½ NS 77 77 Hypotonic 154
Lactated Ringer 130 109 4 3 28 !! Isotonic 273
N Saline 154 154 Isotonic 308
D5 ¼ NS 38.5
38.5 50 !! Hypotonic 335
D5 ½ NS 77 77 50 !! Hypotonic 432
3% S 513 513 Hypertonic 1026
Regulation of Extracellular Fluid Volume
Renal adaptation to hypovolemia
• Renal autoregulation↓/↑ renal afferent arteriolar resistance
• Reduction in RBF↑ renal afferent arteriolar resistance
redistributed from the kidney• Reduction in GFR• Increased tubular reabsorption
Regulation of Extracellular Fluid Volume
Vasoconstrictive factors• Renal sympathetic nerves• Angitensin II• Catecholamines
Vasodilatory factors• Intrinsic renal
autoregulation• Renal vasodilatory effect
of prostaglandins
Renal perfusion during hypovolemia
Regulation of Extracellular Fluid Volume
PV preservation:
↑ reabsorption of filtered water and NaADHAldosterone
hypoperfusion renin secretion↓ ANP
vasodilatory effect ↑ renal excretion of Na and water

Clinical Implications of Choices Between Crystalloid and Colloid
If membrane permeability intact
Colloids preferentially expand PV rather than IFPV expansion unaccompanied by IF expansion
lower fluid requirementsless peripheral and pulmonary edema accumulationreduce concern about later fluid mobilization
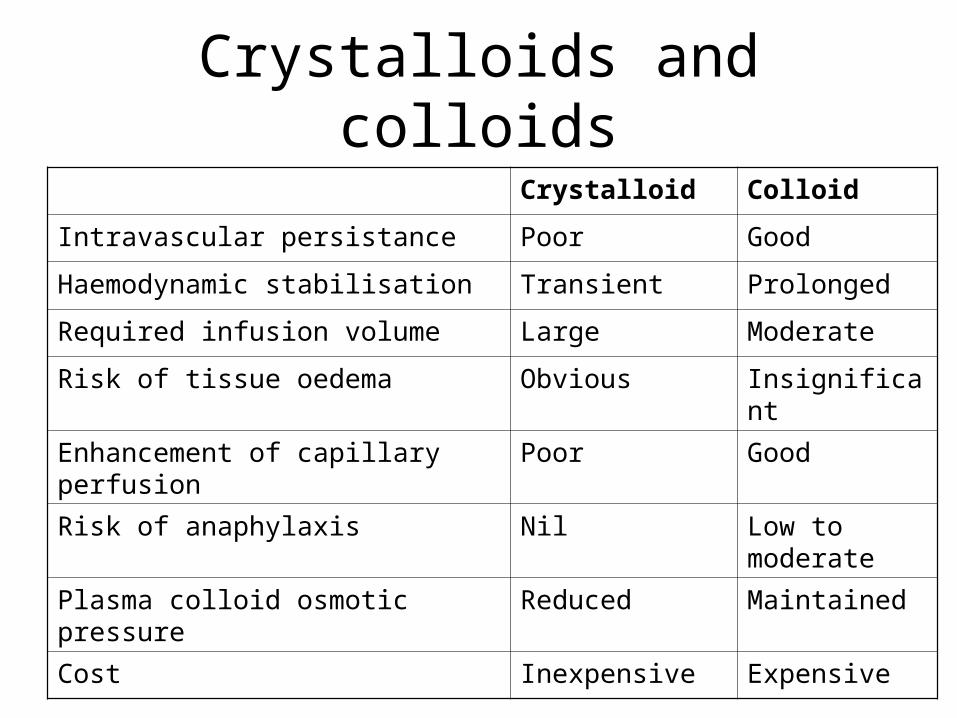
Crystalloids and colloidsCrystalloid Colloid
Intravascular persistance Poor Good
Haemodynamic stabilisation Transient Prolonged
Required infusion volume Large Moderate
Risk of tissue oedema Obvious Insignificant
Enhancement of capillary perfusion Poor Good
Risk of anaphylaxis Nil Low to moderate
Plasma colloid osmotic pressure Reduced Maintained
Cost Inexpensive Expensive
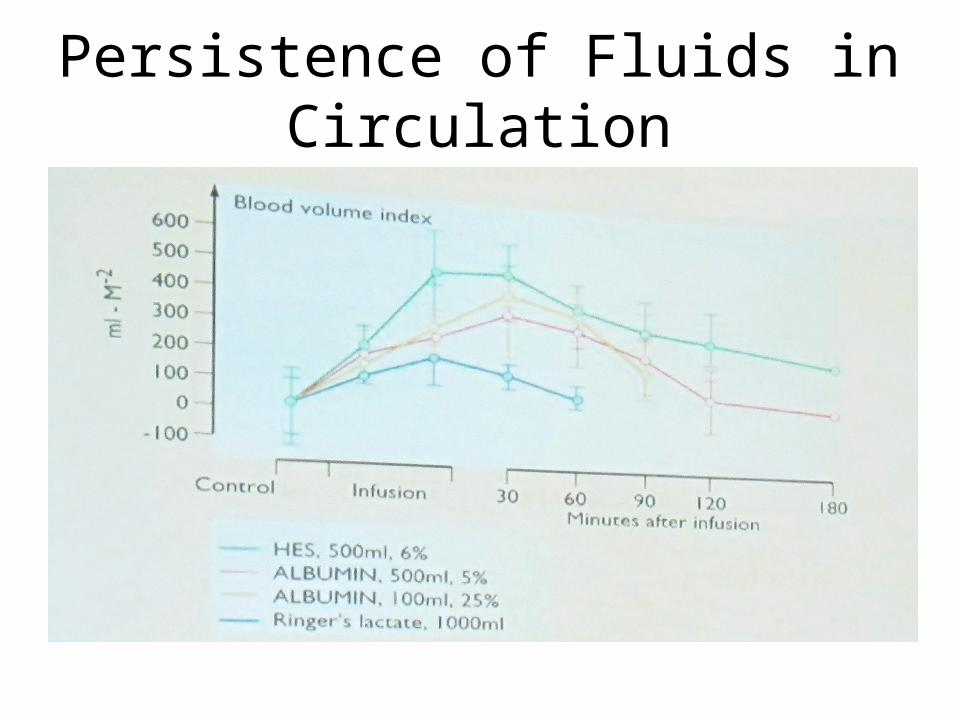
Persistence of Fluids in Circulation
• IMG_2009

Crystalloids (Hypertonic Saline)• Hypertonic Saline 3% and 7.5%
• Increase Plasma Volume from IFV & ICF
• Small Volume Resuscitation
H2O
estimate750 ml
250 ml

Clinical Implication of Hypertonic Fluid Administration
Hypertonic solutions may improveHemodynamics
Cerebral hemodynamicimpermeability of BBB to sodium in uninjured brain
cause brain to shrink in response to acute increase of NaMicrovascular perfusion
through PV expansion
To prolong the therapeutic effectcontinued infusionsubsequent infusion of blood or conventional fluids or addition of colloid

Evaluation of Intravascular Volume
• Physical Examination• Laboratory
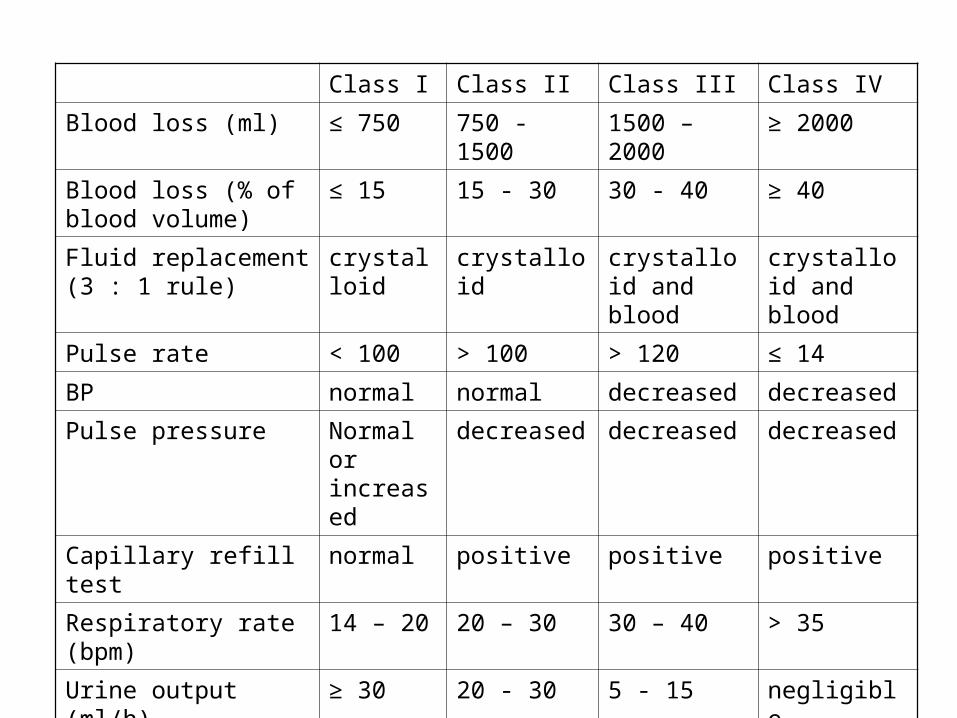
Class I Class II Class III Class IV
Blood loss (ml) ≤ 750 750 - 1500 1500 – 2000 ≥ 2000
Blood loss (% of blood volume)
≤ 15 15 - 30 30 - 40 ≥ 40
Fluid replacement (3 : 1 rule)
crystalloid crystalloid crystalloid and blood
crystalloid and blood
Pulse rate < 100 > 100 > 120 ≤ 14
BP normal normal decreased decreased
Pulse pressure Normal or increased
decreased decreased decreased
Capillary refill test normal positive positive positive
Respiratory rate (bpm) 14 – 20 20 – 30 30 – 40 > 35
Urine output (ml/h) ≥ 30 20 - 30 5 - 15 negligible
Mental status sl. anxiety Mild anxiety anxious or confused
confused or lethargic
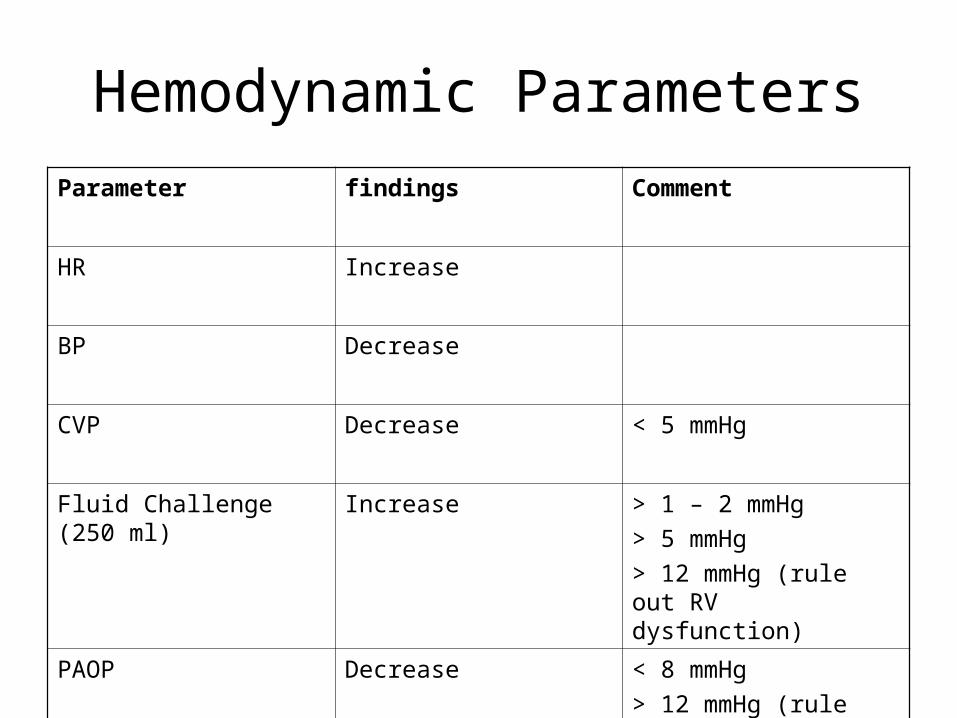
Hemodynamic ParametersParameter findings Comment
HR Increase
BP Decrease
CVP Decrease < 5 mmHg
Fluid Challenge (250 ml) Increase > 1 – 2 mmHg> 5 mmHg> 12 mmHg (rule out RV dysfunction)
PAOP Decrease < 8 mmHg> 12 mmHg (rule out LV dysfunction)

Laboratory Signs of DehydrationTest Findings
HCT Increase M 0.4 – 0.55 F 0.36 – 0.47
pH < 7.36
Urine Specific Gravity > 1010
UO < 0.5 ml/kg/h
Urinary Sodium < 10 mEq/L
Urinary Osmolality > 450 mOsm/kg
Blood Na+ > 145 mEq/L 133 – 148 mEq/L
BUN/creatinine > 10:11
Delay, not reliable

Surgical Fluid RequirementsSurgical patients require:
replacement of PV and ECFmust compensate for the acute reduction of
functional IF3rd space loss
Degree of Tissue Trauma Fluid Requirement
Minimal (e.g. hemiorraphy) 0-2 ml/kg/hr
Moderate (e.g. cholecystectomy)
2-4 ml/kg/hr
Severe (e.g. bowel resection)
4-8 ml/kg/hr

Blood Replacement Therapy

Replacing Blood Losses
Maintain normovolemia
till the danger of anemia outweighsthe risk of transfusion
ie. 7-8 Gm/dl (HCT of 21-24%)
Crystalloid or
Colloids
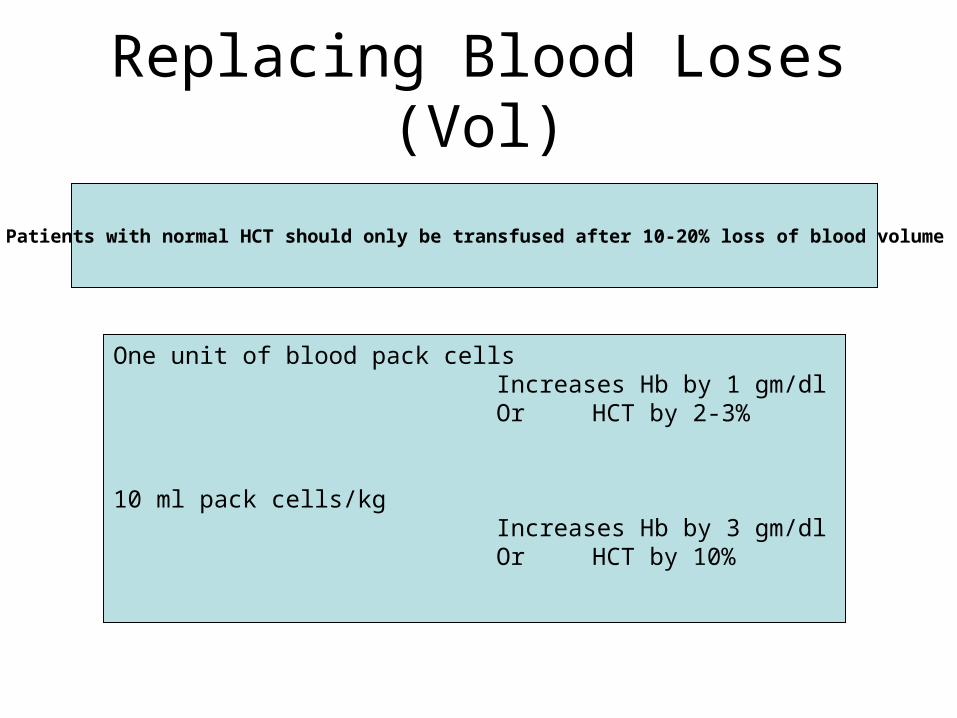
Replacing Blood Loses (Vol)
Patients with normal HCT should only be transfused after 10-20% loss of blood volume
One unit of blood pack cellsIncreases Hb by 1 gm/dlOr HCT by 2-3%
10 ml pack cells/kgIncreases Hb by 3 gm/dlOr HCT by 10%
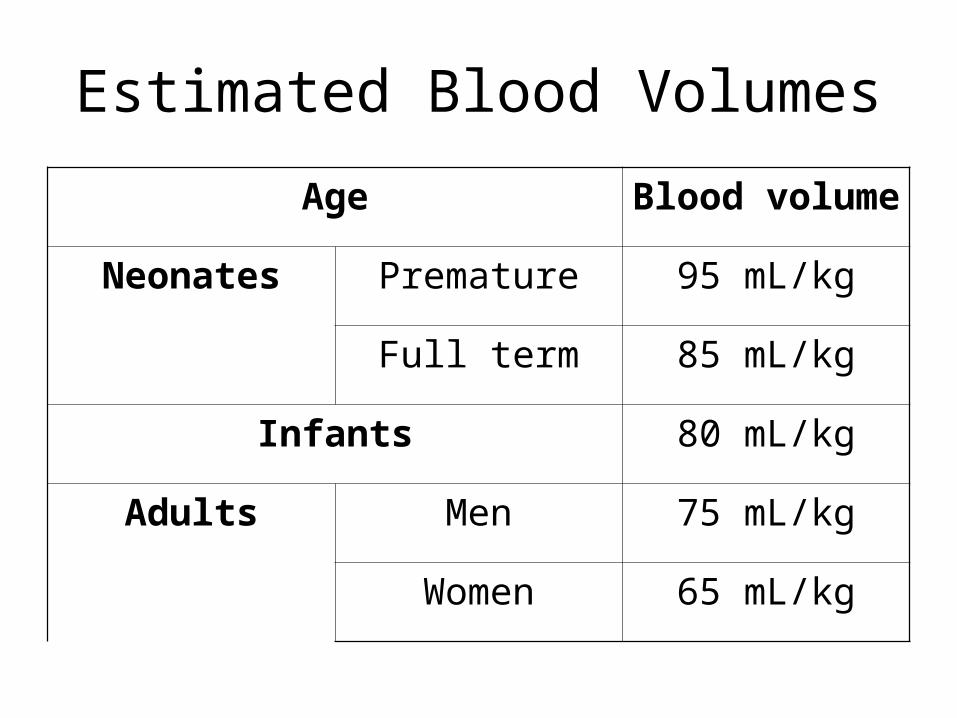
Estimated Blood Volumes
Age Blood volume
Neonates Premature 95 mL/kg
Full term 85 mL/kg
Infants 80 mL/kg
Adults Men 75 mL/kg
Women 65 mL/kg
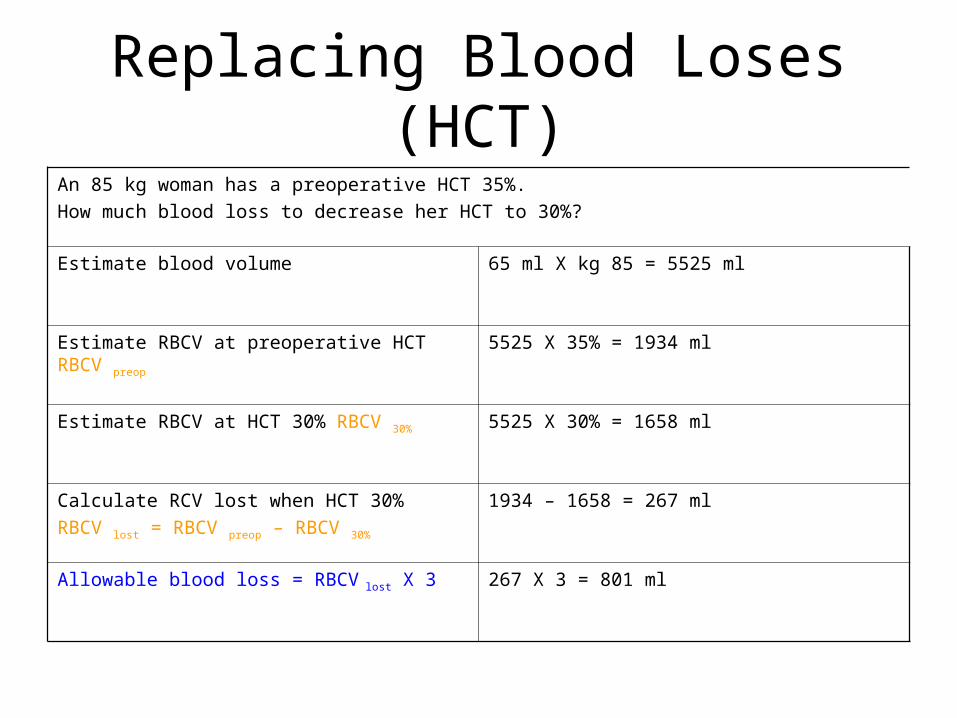
Replacing Blood Loses (HCT)An 85 kg woman has a preoperative HCT 35%.How much blood loss to decrease her HCT to 30%?
Estimate blood volume 65 ml X kg 85 = 5525 ml
Estimate RBCV at preoperative HCT RBCV preop 5525 X 35% = 1934 ml
Estimate RBCV at HCT 30% RBCV 30% 5525 X 30% = 1658 ml
Calculate RCV lost when HCT 30%RBCV lost = RBCV preop – RBCV 30%
1934 – 1658 = 267 ml
Allowable blood loss = RBCV lost X 3 267 X 3 = 801 ml

Evolution of Transfusion Practices
• 10 ε 30 rule• AIDS
A patient specific approach to the decision to transfuse blood components

RBC transfusion threshold
The rationale??? What Hgb/Hct level poses greater risk to the patient than
the threat of contacting a transfusion-transmitted disease
• greater degrees of anemia could be well toleratedchronically anemic renal failure
• Jehovah’s witness
morbidity and mortality rates did not increaseuntil Hgb level fell below 7 g/dl
RBC transfusion threshold
The rationale
Adverse physiologic effects of anemiaNo evidence that mild to moderate anemia impairs:
• Wound healingHct < 15
• Increases bleeding• Increases the length of hospital stay• Increases the frequency or severity of postoperative infection
RBC transfusion threshold
The rationale
• The cause of anemia is thought to be more important in influencing the perioperative course than the severity of anemia
• Maintaining of blood volume was more critical than correcting anemia
RBC transfusion thresholdThe rationale• Goal:
to anticipate, on a patient-by-patient basis, the minimum Hgb level that will avoid organ damage due to O2 deprivation
Do2
Vo2
physiologic capacity for compensatory mechanism
• Decision:should be based upon the clinical judgment that oxygen-
carrying capacity of the blood must be increased to prevent Vo2 from outstripping Do2
Calculation of oxygen delivery (Do2)
Cao2 = Sao2 x Hg x 1.34 + Pao2 x 0.0031
Do2 = Cao2 x CO x 10
Calculation of oxygen consumption (Vo2)
Vo2 = CO x (Cao2 – Cvo2)
normal arteriovenous oxygen content difference is 5 vol%~ Svo2 = 75%
↑Vo2 :
sepsis
hyperthermia
↑ metabolic activity
hyperthyroidism

Oxygen extraction ratio
Fraction of total oxygen delivered is consumed or extracted by the tissues
ER = Vo2 / Do2
= [CO x (Cao2 – Cvo2)] / Cao2 x CO= (Cao2 – Cvo2) / Cao2
Oxygen extraction ratio
Global ≠ Regionalnormal global oxygen delivery may occur in spite of critical levels of regional ischemia
Svo2:vo2 of many vascular beds (global)
heart, under basal condition : 55 – 70%kidney and skin : 7 – 10%
organ with the greatest ER will have the least O2 reserve
Compensatory mechanisms during anemia
• Increased cardiac output• Redistribution of cardiac output• Increased oxygen extraction• Changes in Oxygen-Hemoglobin affinity
Compensatory mechanisms during anemia
Increased cardiac outputWith isovolemic hemodilution
↑ SV↓ SVR
vascular toneviscosity
ageacute or develops slowly
self correcting ↓ oxygen carrying capacity ↑ oxygen transport
Compensatory mechanisms during anemia
Redistribution of cardiac output to organ with greater O2 requirement (brain and heart)
The hearthas a high extraction ratio must rely upon redistribution blood flow to ↑ O2 supply
greatest risk !!!
Compensatory mechanisms during anemia
Increased oxygen extraction
Play an important adaptive rolewhen the normovolemic Hct drops below 25%
↓ mixed venous oxygen saturation
Organs with high ER under basal condition limited capacity to increase Do2 by this mechanism
Compensatory mechanisms during anemia
Changes in Oxygen-Hemoglobin affinity
The sigmoid-shaped oxygen-Hemoglobin dissociation curve:P50 for normal adult Hgb at 37ºC and a pH of 7.4 : 27 mmHg
Left-shiftinghypothermia, alkalosis
Hgb molecule is more ‘stingy’ and requires lower Po2 to release O2 to tissues
Hgb molecules does not release 50% of its O2 until ambient Po2 less than 27 mmHg
Compensatory mechanisms during anemia
Changes in Oxygen-Hemoglobin affinity
When anemia develops slowlythe affinity of Hgb for O2 may be decreased (right-shifted)
accumulation of 2,3 - DPG

Hypovolemic anemia vs Acute blood loss
Acute blood lossstimulation of adrenergic nervous system vasoconstriction and tachycardia! Increased CO does not contribute
Chronic anemiaCO may not change until Hgb decreases to 7 – 8 g/dlsynthesis of supranormal level of 2,3 – DPG begin at Hgb 9 g/dl right shifted
Establishing the RBC transfusion threshold
Transfusion ‘trigger’the Hgb or Hct threshold that justifies RBC transfusion for individual patient
it is presumed that the benefits of RBC transfusion outweigh the risks
• No single criterion could replace clinical judgment as the basis of decision-making
• No evidence that mild-moderate anemia contribute to perioperative morbidity
NIH – Consensus conference on Perioperative Red Cell Transfusion 1988
Establishing the RBC transfusion threshold
Guide therapyclinical assessmentHgb valueLaboratory data (when indicated)
arterial oxygenationmixed venous oxygen tensioncardiac outputoxygen extraction ratioblood volume
estimation of the patient’s myocardial/coronary reserve !!!
Condition that may decrease tolerance for anemia and influence the RBC transfusion threshold
Increased oxygen demandHyperthermiaHyperthyroidismPregnancy
Limited ability to increase COCoronary artery diseaseMyocardial dysfunction (infarction, cardiomyopathy)β-adrenergic blockade
Inability to redistribute COLow SVR state (sepsis, post-CPB)Occlusive vascular disease (cerebral, coronary)
Left shift of O2-Hgb curveAlkalosisHypothermia
Abnormal HemoglobinsPresence of stored Hgb (decreased 2,3-DPG)Hgb S
Acute anemia (limited 2,3-DPG compensation)Impaired oxygenation
Pulmonary diseaseHigh altitude
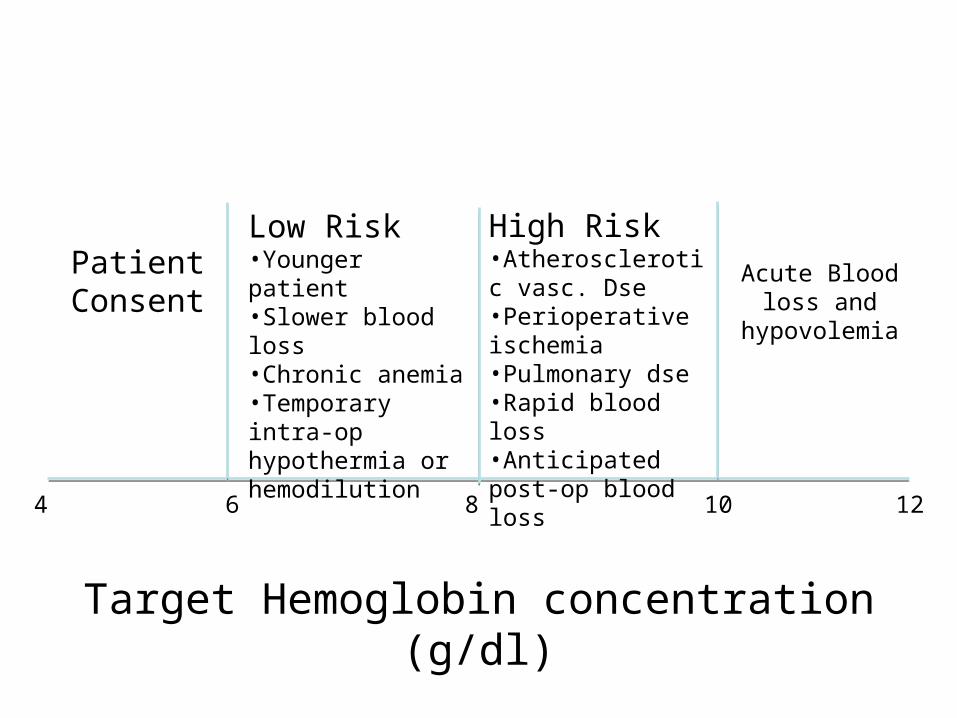
Target Hemoglobin concentration (g/dl)
4 6 8 10 12
High Risk•Atherosclerotic vasc. Dse•Perioperative ischemia•Pulmonary dse•Rapid blood loss•Anticipated post-op blood loss
Low Risk•Younger patient•Slower blood loss•Chronic anemia•Temporary intra-op hypothermia or hemodilution
PatientConsent
Acute Blood loss and hypovolemia

What donor blood group type may be compatible for transfusion to a particular recipient ?
Focus on which antibodies will be present in the recipient serum !!!reaction of these antibodies with donor RBC antigens
can activate complement hemolysis of RBC
Type O-negative blood universal donorsType AB-positive blood universal recipients

Compatibility testingThe cross-match
Donor RBCs mixed with recipient serumstimulating the actual anticipated transfusion
3 phases1. Immediate phase2. Incubation phase3. Antiglobulin phase
Is cross-match necessary?ABO-Rh status alone 99.8% compatibleWith antibody screen 99.94% compatibleWith complete cross-match 99.95% compatible
Those who have not previously exposed or pregnant
incompatibility : 1 in 1000Those who have previously exposed or pregnant
incompatibility : 1 in 100
Type and Screen orders• When blood is ordered preoperatively for surgical cases in which
transfusion is unlikely• If the need arises the blood can be cross-matched prior to
transfusion
Advantages:• If the blood is not needed
the additional expenses for cross-match is eliminated• If cross-match is performed and compatible unit identified
those unit are held in reserve temporarily out of blood supply if the blood is not used
wastage by outdating
Risk of blood product administration
1. Problems related to blood storage2. Problems related to immune-mediated
transfusion reaction3. Infectious risks

Risk of blood product administration
Problems related to blood storage
• Citrate intoxicationCitrate prevent coagulation of stored blood
by chelating ionized Calciumlarge volume (>1 blood volume)administered rapidly (> 1 ml/kg/minor 1 unit/5 mins)impaired liver function temporary reduction of ionized Ca levels
Signs:hypotensionnarrow pulse pressure↑ VEDP↑ CVPECG
prolonged QT intervalwidened QRS complexesflattened T waves
Risk of blood product administration
Problems related to blood storage
• Acid-base ChangesCPD ↓ pH to 7.0 – 7.1during storage
ongoing metabolism of glucose to lactate production of CO2
Citrate metabolized to bicarbonate
• Decreases in 2,3-DPGleft shift of O2-Hgb dissociation curve
less efficient O2

Risk of blood product administration
Problems related to blood storage
• Hyperkalemiato maintain electrochemical neutrality
H+ generated during storageRBCs lysis
with normal infusion rate K+ is distributedrates > 90 – 120 ml/min hyperkalemia
aggravated byhypovolemiahypothermiaacidosis
Risk of blood product administration
Problems related to blood storage
• Hypothermiafrom rapid transfusion of large volumes of cold blood
stored at temp 1 – 6ºC
↓ COtissue perfusion impaired
vasoconstrictionleft-shifting of O2-Hgb dissociation curve
metabolic acidosisshivering
↑ O2 consumption by 300-400%hemostatic dysfunctioncitrate toxicityventricular irritability

Risk of blood product administration
Problems related to blood storage
• Dilutional coagulopathyplateletsclotting factors
V and VIII

Immediate Hemolytic Transfusion Reactions
hemolysis release hemoglobin to the blood
renal damage↓ renal blood flowmechanical obstruction in the renal tubule
free Hgb, RBC stromadeposition of antigen-antibody complexes (G)deposition of fibrin (DIC)
Signs and symptomsfever, chill, nausea and vomitinghypotension and tachycardiaflushed and dyspneicchest and back painrestlesshemoglobinuriadiffuse bleedingrenal failure

Massive Blood Transfusion
≥ one blood volume< 24 h
• Coagulopathy• Hypothermia• Citrate toxicity• Hyperkalemia• ↓ 2,3 DPG
Emergency Transfusion
Choices:• Type-specific partially cross-matched blood• Type-specific uncross-matched blood• O-negative (universal donor) PRBCs
O-negative (universal donor) whole blood
contains high titers of antibodies