
2021 UPMC for Life Medicare Product Training
92
2021 UPMC for Life Medicare Product Training
Transcript of 2021 UPMC for Life Medicare Product Training

2021 UPMC for Life Medicare Product Training
Training agenda
1
• UPMC for Life Plans• Service Area• Plan Terminations• Global Plan Changes• VBID Updates• Provider Specific Plans• Individual Plan Changes• Benefit Reminders• Benefit Changes• Maximum Out-of-pocket
• Employer Group
• Prescription Drug Coverage
• Member Document Changes
• Find Plan Documents Online

Medicare Advantage HMO/PPO state landscape
2
PennsylvaniaMedicare Advantage HMO/PPO Service Area State Landscape
Medicare Eligibles1 1,835,595
YOY Eligible Growth1 4.5%
Percent Enrolled in a MA Plan1 47.0%
YOY MA Enrollment Growth1 5.5%
UPMC’s MA Enrollment Percent2 18.9%
1June 2020 CMS.gov State/County Penetration within UPMC 2021 Medicare Advantage HMO/PPO Individual Service Area.2Based on 2020 UPMC Medicare Advantage HMO/PPO Individual Service Area.
YOY = Year Over YearMA = Medicare Advantage
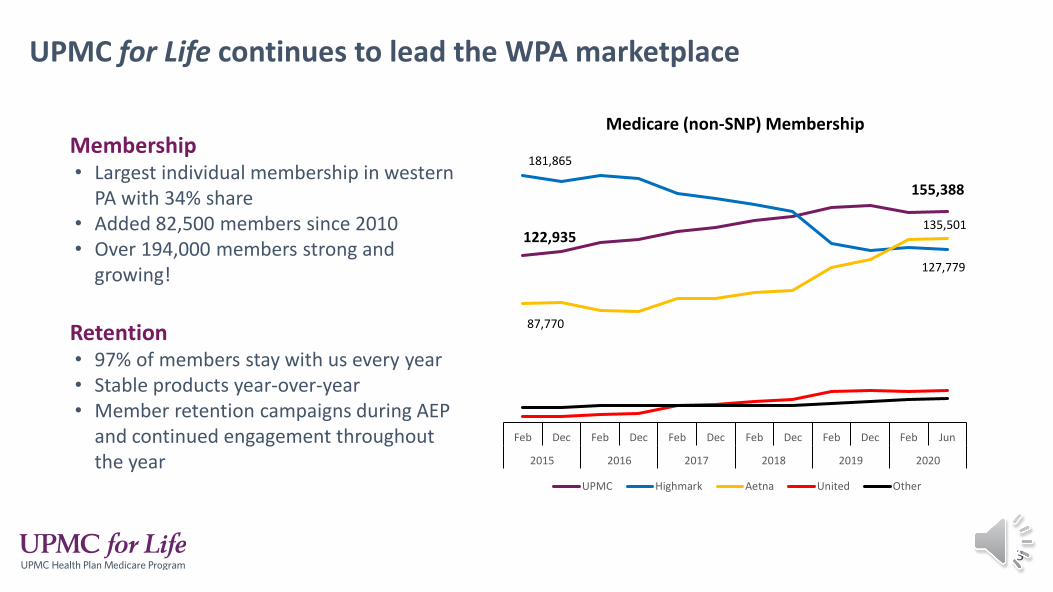
Membership• Largest individual membership in western
PA with 34% share• Added 82,500 members since 2010• Over 194,000 members strong and
growing!
Retention• 97% of members stay with us every year• Stable products year-over-year• Member retention campaigns during AEP
and continued engagement throughout the year
For the third year in a row, UPMC Health Plan earned three 2020 Gold Stevie Awards for its outstanding sales and customer service:
UPMC for Life continues to lead the WPA marketplace
• Best Back-Office Customer Service Team
• Innovation in Customer Service
• Customer Service Team of the Year—Recovery Situation 3
122,935
155,388
181,865
127,779
87,770
135,501
Feb Dec Feb Dec Feb Dec Feb Dec Feb Dec Feb Jun
2015 2016 2017 2018 2019 2020
Medicare (non-SNP) Membership
UPMC Highmark Aetna United Other
For the third year in a row, UPMC Health Plan earned three 2020 Gold Stevie Awards for its outstanding sales and customer service:
• Best Back-Office Customer Service Team
• Innovation in Customer Service
• Customer Service Team of the Year—Recovery Situation 4
Access to high-quality care, coverage, and customer service
UPMC for Life value propositionOur focus is on providing members with the care they need, when and where they need it. Our plans support this goal by offering high-quality, affordable coverage from a large network of UPMC and local community providers.
5
• High-quality UPMC providers• Price/affordability• Prescription coverage• Vision, dental, hearing, fitness, travel, OTC
• Guaranteed UPMC access/trusted brand• Price consistency• Personal customer service• Coordination of care
• Award-winning customer service• Care management• Health coaching• Member portal
• Ease of seeing doctors• Ease of getting care needed• Ease of enrollment• Ease of claims payment
Value
Security
Support
Simplicity

We understand that having the right doctors and hospitals is important to our members. That’s why we offer high-quality access to the care our members need where and when they need it!
Our network includes thousands of doctors and hospitals that members can use for care:• Freedom to self-refer to in-network providers.• Access to all the doctors and hospitals of UPMC.
Doctors and hospitals our members know and trust
6
• A large network of additional providers in the community, including:
• WPA: Butler Health System, Cleveland Clinic, Corry Memorial Hospital, Excela Health, Heritage Valley Health System, Jefferson Hospital, Millcreek Community Hospital, Monongahela Valley Hospital, Saint Vincent Hospital, St. Clair Hospital, Washington Hospital, and many AHN doctors.
• EPA: Crozer-Keystone Medical Center, Doylestown Health, Evangelical Medical Center, Guthrie, Grand View Health, Jefferson Health, Main Line Health, Lancaster General Health, Lehigh Valley Health Network, Penn State Health Milton S. Hershey Medical Center, and Tower Health System.

UPMC for Life Plan Updates
7
8
Parts A and B together provide coverage both in and out of the hospital.
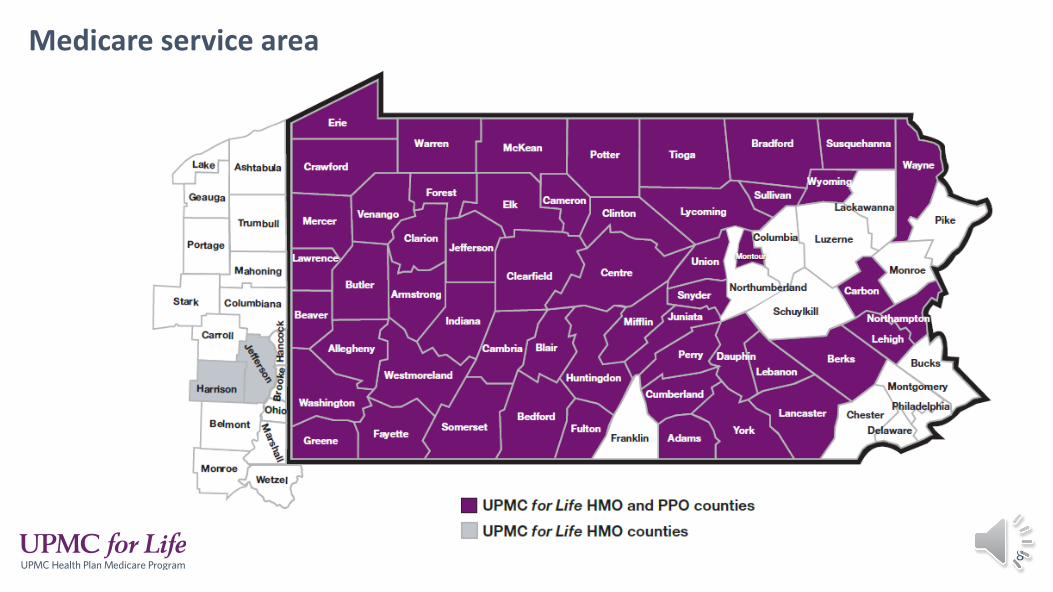
Medicare service area
8

9Plans terming for 2021
9
C
The below plans are terming at the end of 2020.These plans will not be cross-walked into another existing plan.
HMO Deductible with Rx SEPA(H3907 044)
Bucks, Chester, Delaware, Montgomery, Philadelphia counties
CHMO Rx SEPA(H3907 048)
Bucks, Chester, Delaware, Montgomery, Philadelphia counties

• Added Treat No Transport ambulance benefito Treat and no transport services are covered (for HMO and PPO individual plans) when you are treated by an
emergency medical provider and not transported to a medical facility.o This may be determined by the EMS team or if transport is declined.
• Emergency Room copay for all plans will be $90.
• Urgent care copay for all plans will be $65.
• Lower telehealth specialist visit copays across all plans.
• Added quantity limit for diabetic supplieso Test strips are limited to 150 per 30 days (Lifescan brand only).o An exception process is available upon medical necessity request if more than 150 test strips per 30 days are needed.o One glucometer every 365 days (Lifescan brand only).
10
Global Medicare plan updates
10
Make Time to Talk (LIS VBID)• Contract: H3907• PBPs: 002 and 029• Make Time to Talk VBID members are automatically enrolled based on having LIS.• Once a member is identified as LIS eligible for 2021, they will remain in the Make Time to Talk
program even if they lose LIS during the year. • Make Time to Talk members are eligible for cost-share reduction on outpatient mental health
visits. • H3907 002 (HMO no Rx)- $20 copay for Outpatient Mental Health Specialty Services• H3907 029 (HMO Rx)- $18 copay for Outpatient Mental Health Specialty Services
• These members are not eligible for the debit card or the nebulizer benefit, unless they are also eligible to participate in the Spark Your Health program.
11
VBID updates
11
Spark Your Health VBID • Contracts: H3907 and H5533, PBPs: 002, 037, 029, 006, 003, and 005• Members with CHF & COPD or CHF & Diabetes• Spark Your Health members must complete their VBID Personal Health Review (PHR) to start the program. • The VBID PHR kicks off the member’s participation in the Spark Your Health VBID program and is the first step to earning a
$75 reward. Members are mailed a debit card that has their reward dollars loaded onto it. • After the VBID PHR is completed, members can receive $25 each quarter for their completed healthy activities. Members
that complete a healthy activity in Q4 will earn $50 for that quarter. Members can earn up to $200 on their debit card by completing the PHR and a healthy activity in each quarter.
• Members eligible for Spark Your Health can also receive a Part B nebulizer at no cost. Members do not have to complete the PHR to receive the $0 cost share for Part B nebulizers.
• Medicare Operations will be pulling a report every Tuesday based on the prior week’s completed PHR and activities. • If a member should be rewarded, a file will be sent to BlackHawk to load a specified amount on the debit card. • Debit cards for this program will read “UPMC for Life - Spark Your Health.” • This is how you can see that the card is for VBID versus the Medicare preventive incentive program. Debit cards for
the Medicare preventive incentive program just read UPMC for Life.
12
VBID updates
12
13
What is a PSP?
Provider specific plans (PSP)
• A select network of providers that members can use for their medical care.• Typically the network is smaller allowing members to get high-quality care
that’s closely coordinated between the Health Plan and the providers.• This helps members to receive more personal support and better care.• There is now only one PSP network for Berks County.
Meals for members with COPD, CHF, and diabetes• All HMO and PPO plans (only applies to individual plans).• For members with all three diagnoses of chronic obstructive pulmonary disease (COPD),
congestive heart failure (CHF), and diabetes. • This benefit is for a member who has been discharged from either an inpatient hospital stay,
observation stay, or a skilled nursing facility stay.• 56 meals (two meals per day for four weeks (28 days)) will be delivered to the member’s
home in four deliveries (one delivery per week). • One meal benefit per year.• The meal benefit can only be used once after a discharge, it cannot be broken up into
separate weeks.
14
Flexible benefit updates
14
15
• Medicare Network
15
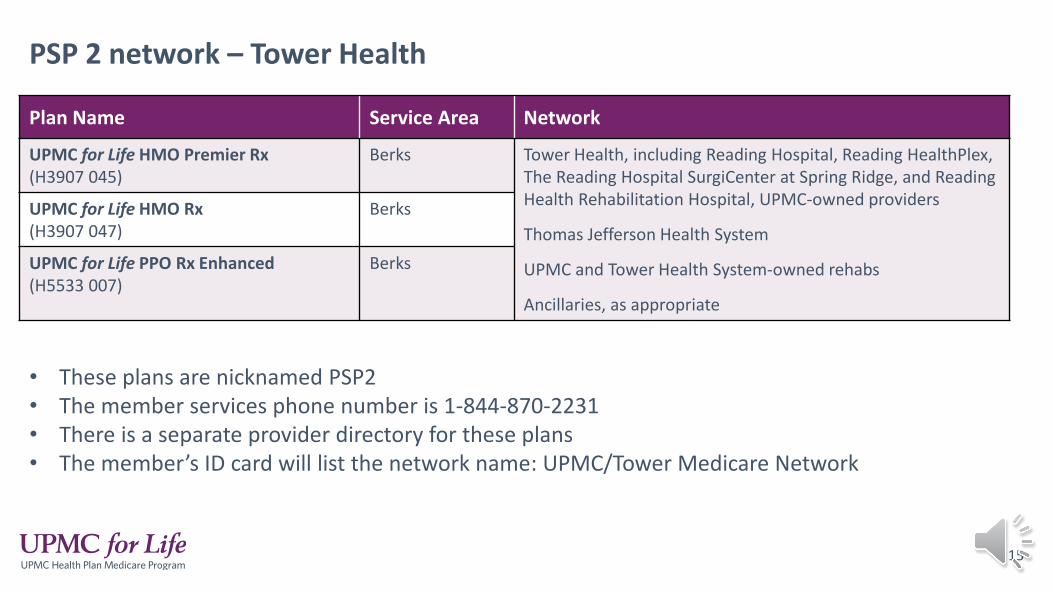
PSP 2 network – Tower Health
Plan Name Service Area Network
UPMC for Life HMO Premier Rx (H3907 045)
Berks Tower Health, including Reading Hospital, Reading HealthPlex, The Reading Hospital SurgiCenter at Spring Ridge, and Reading Health Rehabilitation Hospital, UPMC-owned providers
Thomas Jefferson Health System
UPMC and Tower Health System-owned rehabs
Ancillaries, as appropriate
UPMC for Life HMO Rx (H3907 047)
Berks
UPMC for Life PPO Rx Enhanced (H5533 007)
Berks
• These plans are nicknamed PSP2• The member services phone number is 1-844-870-2231• There is a separate provider directory for these plans• The member’s ID card will list the network name: UPMC/Tower Medicare Network
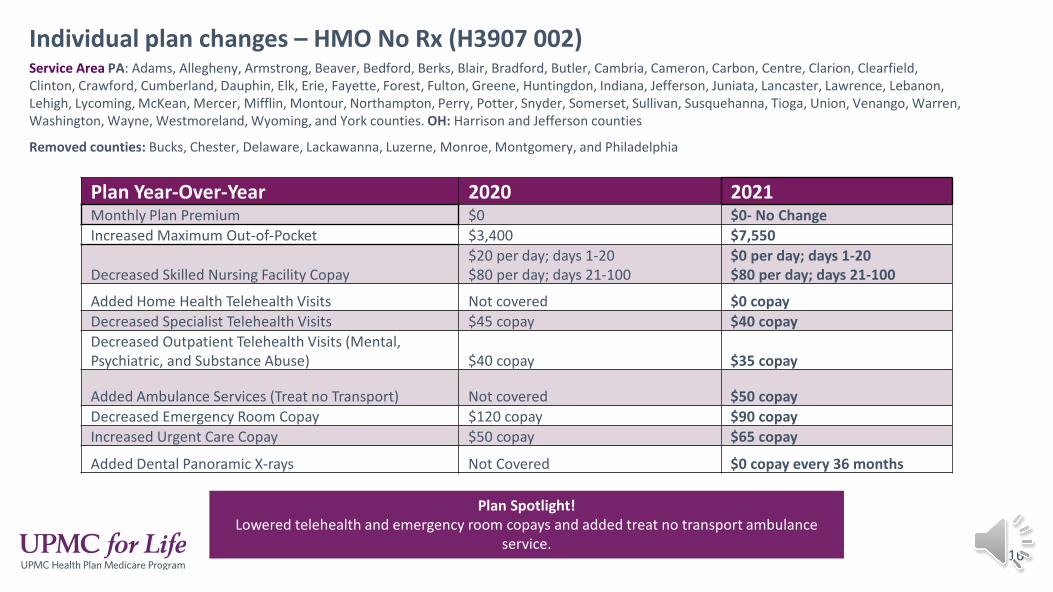
Individual plan changes – HMO No Rx (H3907 002)
16
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Berks, Blair, Bradford, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lehigh, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Susquehanna, Tioga, Union, Venango, Warren, Washington, Wayne, Westmoreland, Wyoming, and York counties. OH: Harrison and Jefferson counties
Removed counties: Bucks, Chester, Delaware, Lackawanna, Luzerne, Monroe, Montgomery, and Philadelphia
Plan Year-Over-Year 2020 2021Monthly Plan Premium $0 $0- No ChangeIncreased Maximum Out-of-Pocket $3,400 $7,550
Decreased Skilled Nursing Facility Copay$20 per day; days 1-20$80 per day; days 21-100
$0 per day; days 1-20$80 per day; days 21-100
Added Home Health Telehealth Visits Not covered $0 copayDecreased Specialist Telehealth Visits $45 copay $40 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay $35 copay
Added Ambulance Services (Treat no Transport) Not covered $50 copayDecreased Emergency Room Copay $120 copay $90 copayIncreased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Plan Spotlight! Lowered telehealth and emergency room copays and added treat no transport ambulance
service.
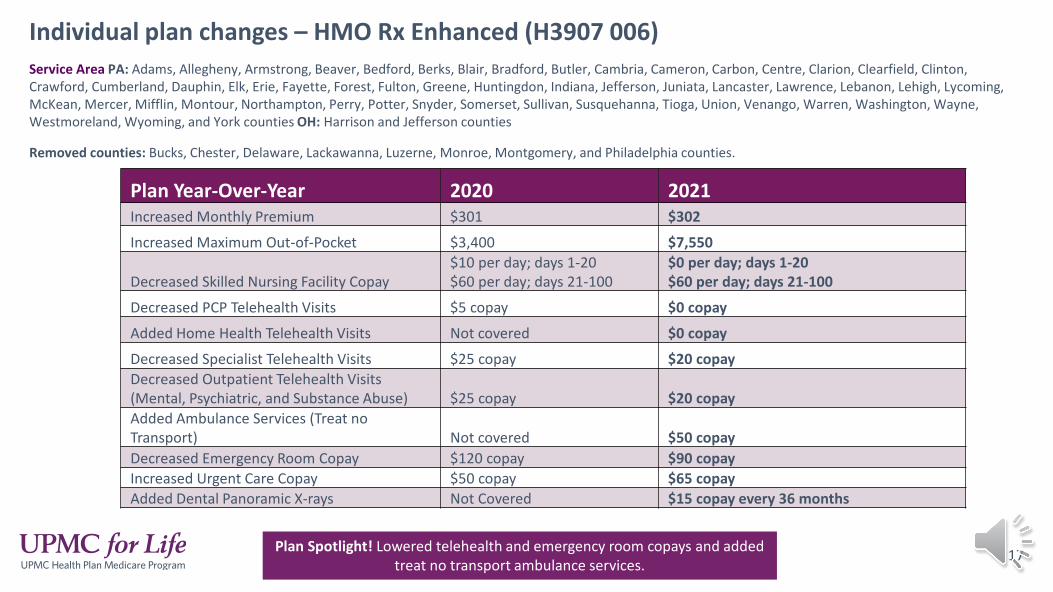
Individual plan changes – HMO Rx Enhanced (H3907 006)
17
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Berks, Blair, Bradford, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lehigh, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Susquehanna, Tioga, Union, Venango, Warren, Washington, Wayne, Westmoreland, Wyoming, and York counties OH: Harrison and Jefferson counties
Removed counties: Bucks, Chester, Delaware, Lackawanna, Luzerne, Monroe, Montgomery, and Philadelphia counties.
Plan Year-Over-Year 2020 2021Increased Monthly Premium $301 $302
Increased Maximum Out-of-Pocket $3,400 $7,550
Decreased Skilled Nursing Facility Copay$10 per day; days 1-20$60 per day; days 21-100
$0 per day; days 1-20$60 per day; days 21-100
Decreased PCP Telehealth Visits $5 copay $0 copay
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $25 copay $20 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $25 copay $20 copayAdded Ambulance Services (Treat no Transport) Not covered $50 copayDecreased Emergency Room Copay $120 copay $90 copayIncreased Urgent Care Copay $50 copay $65 copayAdded Dental Panoramic X-rays Not Covered $15 copay every 36 months
Plan Spotlight! Lowered telehealth and emergency room copays and added treat no transport ambulance services.
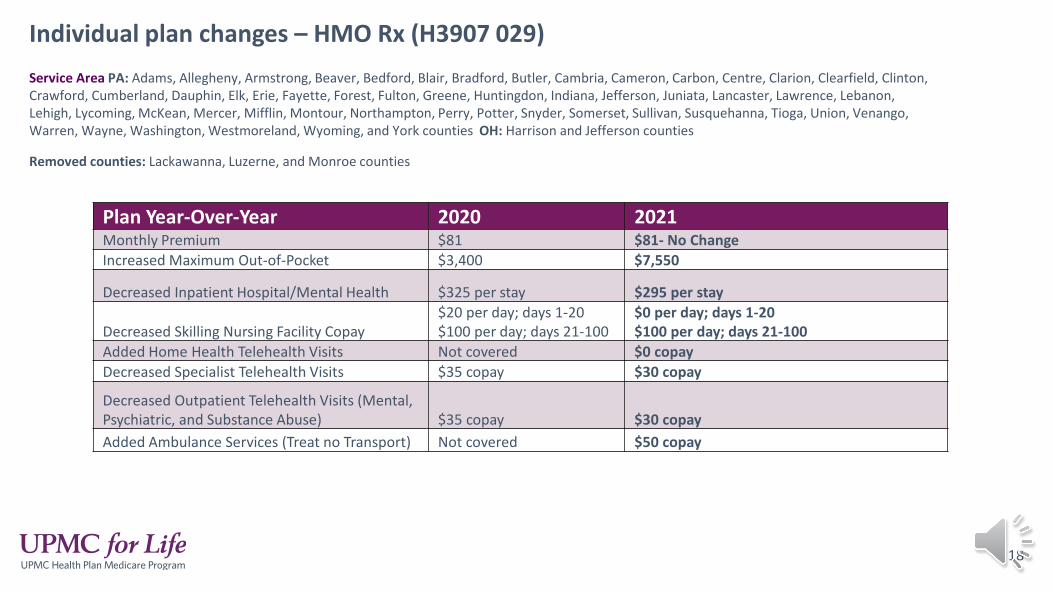
Individual plan changes – HMO Rx (H3907 029)
18
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Blair, Bradford, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lehigh, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Susquehanna, Tioga, Union, Venango, Warren, Wayne, Washington, Westmoreland, Wyoming, and York counties OH: Harrison and Jefferson counties
Removed counties: Lackawanna, Luzerne, and Monroe counties
Plan Year-Over-Year 2020 2021Monthly Premium $81 $81- No ChangeIncreased Maximum Out-of-Pocket $3,400 $7,550
Decreased Inpatient Hospital/Mental Health $325 per stay $295 per stay
Decreased Skilling Nursing Facility Copay$20 per day; days 1-20$100 per day; days 21-100
$0 per day; days 1-20$100 per day; days 21-100
Added Home Health Telehealth Visits Not covered $0 copayDecreased Specialist Telehealth Visits $35 copay $30 copay
Decreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $35 copay $30 copayAdded Ambulance Services (Treat no Transport) Not covered $50 copay
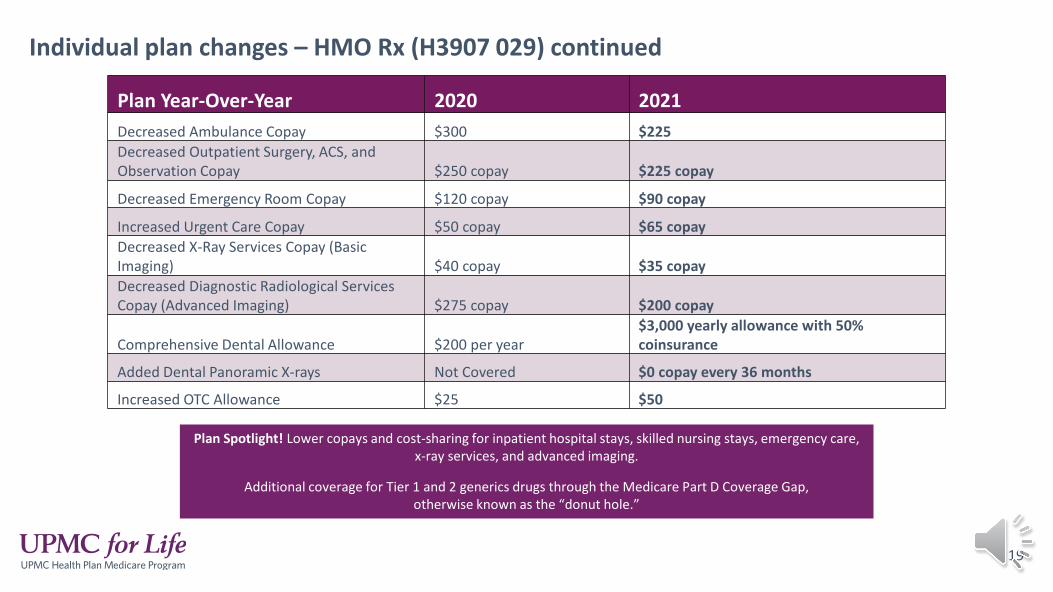
Individual plan changes – HMO Rx (H3907 029) continued
19
Plan Year-Over-Year 2020 2021Decreased Ambulance Copay $300 $225Decreased Outpatient Surgery, ACS, and Observation Copay $250 copay $225 copay
Decreased Emergency Room Copay $120 copay $90 copay
Increased Urgent Care Copay $50 copay $65 copayDecreased X-Ray Services Copay (Basic Imaging) $40 copay $35 copayDecreased Diagnostic Radiological Services Copay (Advanced Imaging) $275 copay $200 copay
Comprehensive Dental Allowance $200 per year$3,000 yearly allowance with 50% coinsurance
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Increased OTC Allowance $25 $50
Plan Spotlight! Lower copays and cost-sharing for inpatient hospital stays, skilled nursing stays, emergency care, x-ray services, and advanced imaging.
Additional coverage for Tier 1 and 2 generics drugs through the Medicare Part D Coverage Gap, otherwise known as the “donut hole.”
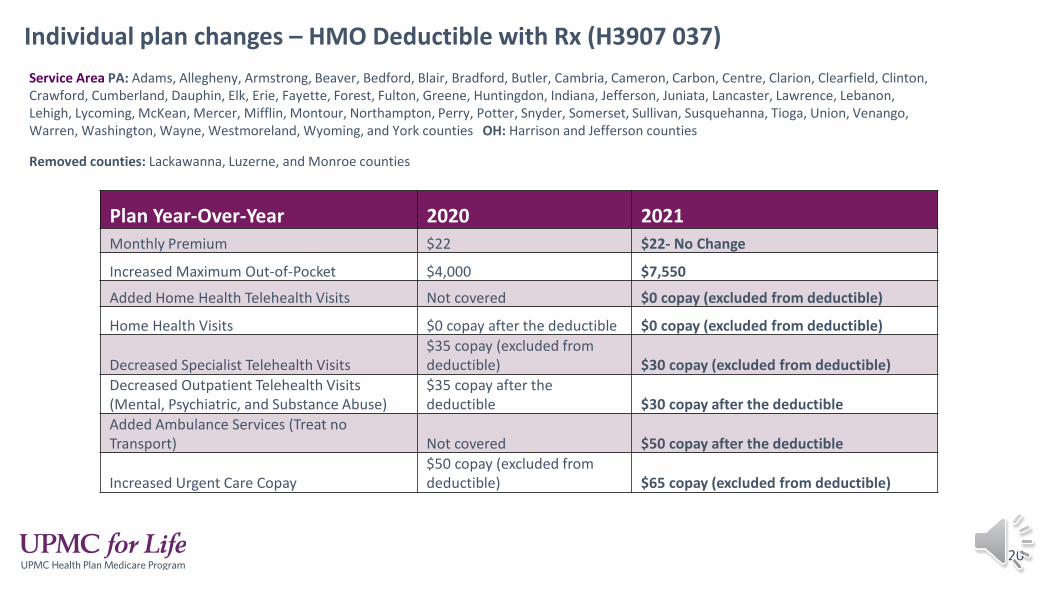
Individual plan changes – HMO Deductible with Rx (H3907 037)
20
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Blair, Bradford, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lehigh, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Susquehanna, Tioga, Union, Venango, Warren, Washington, Wayne, Westmoreland, Wyoming, and York counties OH: Harrison and Jefferson counties
Removed counties: Lackawanna, Luzerne, and Monroe counties
Plan Year-Over-Year 2020 2021Monthly Premium $22 $22- No Change
Increased Maximum Out-of-Pocket $4,000 $7,550
Added Home Health Telehealth Visits Not covered $0 copay (excluded from deductible)
Home Health Visits $0 copay after the deductible $0 copay (excluded from deductible)
Decreased Specialist Telehealth Visits$35 copay (excluded fromdeductible) $30 copay (excluded from deductible)
Decreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse)
$35 copay after the deductible $30 copay after the deductible
Added Ambulance Services (Treat no Transport) Not covered $50 copay after the deductible
Increased Urgent Care Copay$50 copay (excluded from deductible) $65 copay (excluded from deductible)
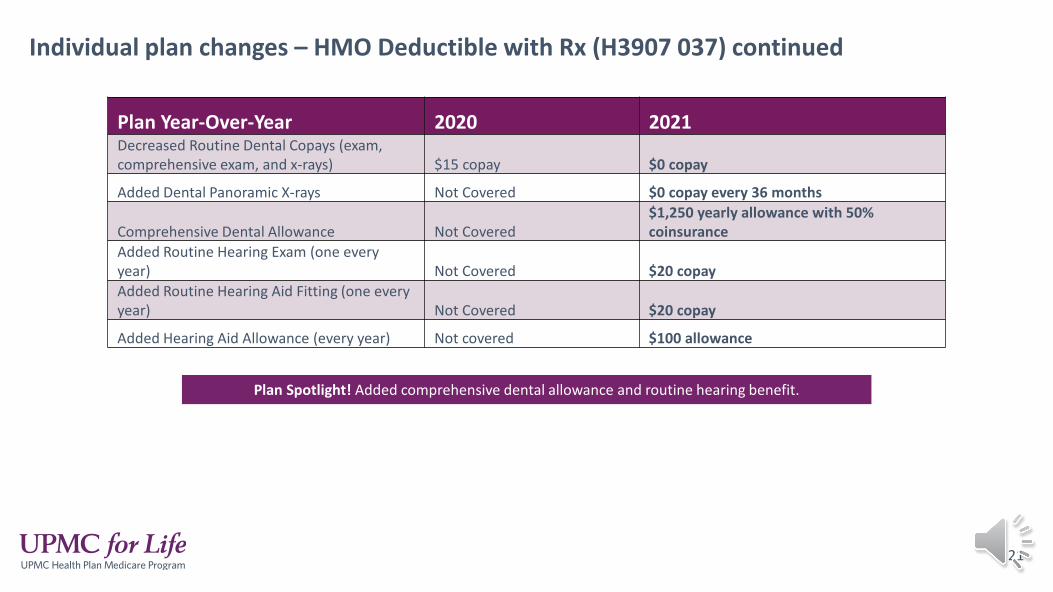
Individual plan changes – HMO Deductible with Rx (H3907 037) continued
21
Plan Year-Over-Year 2020 2021Decreased Routine Dental Copays (exam, comprehensive exam, and x-rays) $15 copay $0 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Comprehensive Dental Allowance Not Covered$1,250 yearly allowance with 50% coinsurance
Added Routine Hearing Exam (one every year) Not Covered $20 copayAdded Routine Hearing Aid Fitting (one every year) Not Covered $20 copay
Added Hearing Aid Allowance (every year) Not covered $100 allowance
Plan Spotlight! Added comprehensive dental allowance and routine hearing benefit.
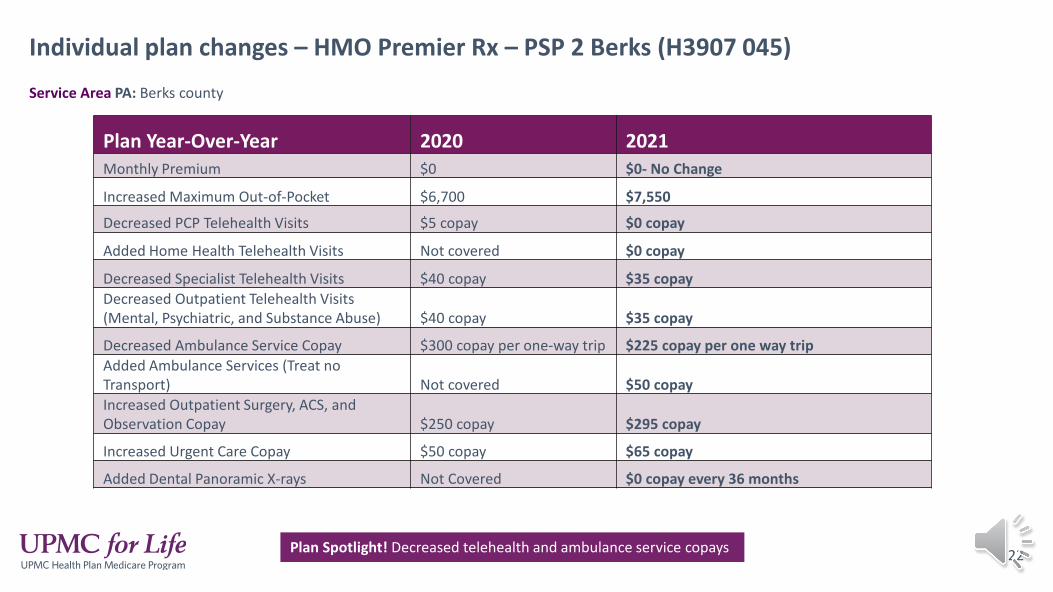
Individual plan changes – HMO Premier Rx – PSP 2 Berks (H3907 045)
22
Service Area PA: Berks county
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No Change
Increased Maximum Out-of-Pocket $6,700 $7,550
Decreased PCP Telehealth Visits $5 copay $0 copay
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $40 copay $35 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay $35 copay
Decreased Ambulance Service Copay $300 copay per one-way trip $225 copay per one way tripAdded Ambulance Services (Treat no Transport) Not covered $50 copayIncreased Outpatient Surgery, ACS, and Observation Copay $250 copay $295 copay
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Plan Spotlight! Decreased telehealth and ambulance service copays
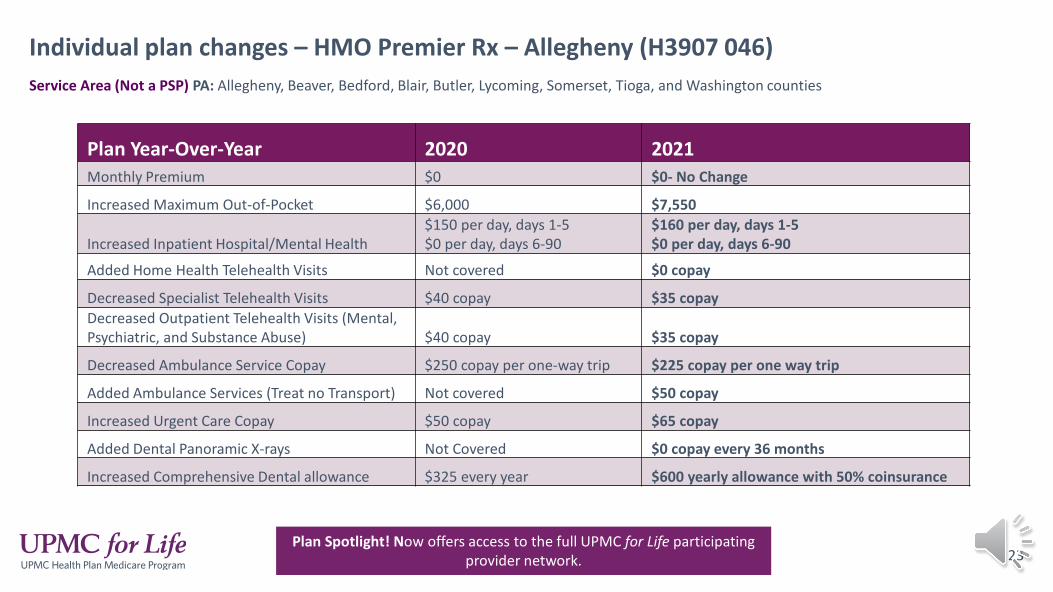
Individual plan changes – HMO Premier Rx – Allegheny (H3907 046)
23
Service Area (Not a PSP) PA: Allegheny, Beaver, Bedford, Blair, Butler, Lycoming, Somerset, Tioga, and Washington counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No Change
Increased Maximum Out-of-Pocket $6,000 $7,550
Increased Inpatient Hospital/Mental Health$150 per day, days 1-5$0 per day, days 6-90
$160 per day, days 1-5$0 per day, days 6-90
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $40 copay $35 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay $35 copay
Decreased Ambulance Service Copay $250 copay per one-way trip $225 copay per one way trip
Added Ambulance Services (Treat no Transport) Not covered $50 copay
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Increased Comprehensive Dental allowance $325 every year $600 yearly allowance with 50% coinsurance
Plan Spotlight! Now offers access to the full UPMC for Life participating provider network.

Individual plan changes – HMO Rx – PSP 2 Berks (H3907 047)
24
Service Area PA: Berks county
Plan Year-Over-Year 2020 2021Increased Monthly Premium $83 $84
Increased Maximum Out-of-Pocket $4,500 $7,550
Decreased PCP Telehealth Visits $5 $0 copay
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $35 copay $30 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $35 copay $30 copay
Decreased Ambulance Service Copay$300 copay per one-way trip $225 copay per one way trip
Added Ambulance Services (Treat no Transport) Not covered $50 copay
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Plan Spotlight! Decreased telehealth and ambulance service copays
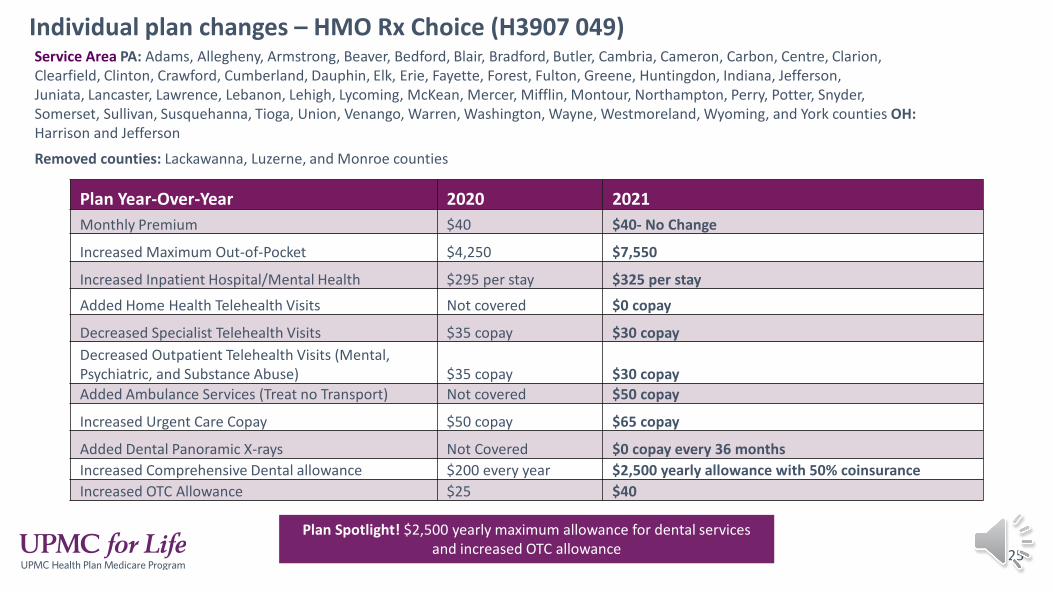
Individual plan changes – HMO Rx Choice (H3907 049)
25
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Blair, Bradford, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lehigh, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Susquehanna, Tioga, Union, Venango, Warren, Washington, Wayne, Westmoreland, Wyoming, and York counties OH: Harrison and Jefferson
Removed counties: Lackawanna, Luzerne, and Monroe counties
Plan Year-Over-Year 2020 2021Monthly Premium $40 $40- No Change
Increased Maximum Out-of-Pocket $4,250 $7,550
Increased Inpatient Hospital/Mental Health $295 per stay $325 per stay
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $35 copay $30 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $35 copay $30 copayAdded Ambulance Services (Treat no Transport) Not covered $50 copay
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 monthsIncreased Comprehensive Dental allowance $200 every year $2,500 yearly allowance with 50% coinsuranceIncreased OTC Allowance $25 $40
Plan Spotlight! $2,500 yearly maximum allowance for dental services and increased OTC allowance
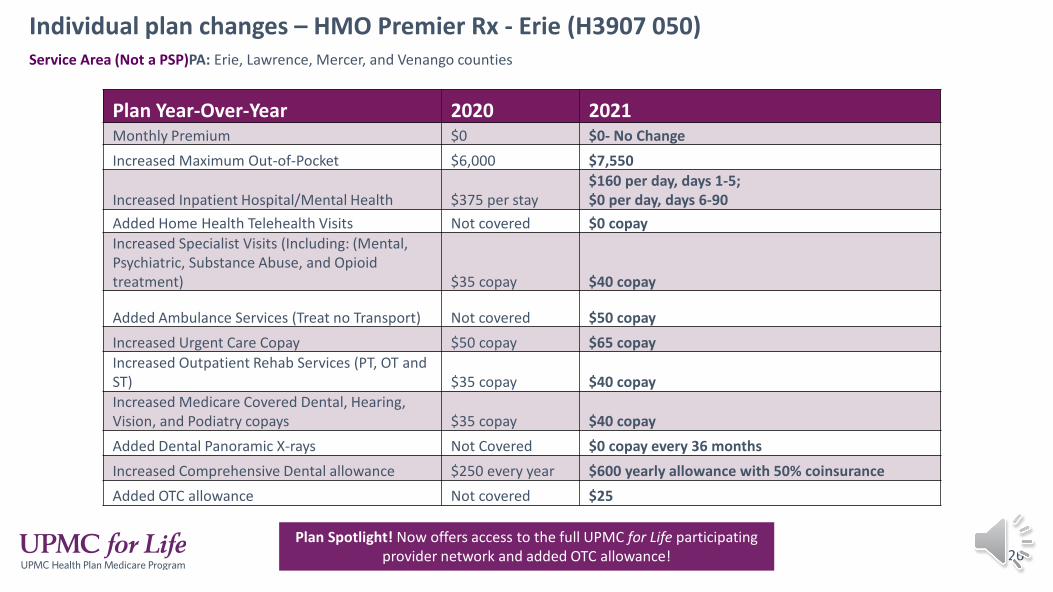
Individual plan changes – HMO Premier Rx - Erie (H3907 050)
26
Service Area (Not a PSP)PA: Erie, Lawrence, Mercer, and Venango counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No ChangeIncreased Maximum Out-of-Pocket $6,000 $7,550
Increased Inpatient Hospital/Mental Health $375 per stay$160 per day, days 1-5;$0 per day, days 6-90
Added Home Health Telehealth Visits Not covered $0 copayIncreased Specialist Visits (Including: (Mental, Psychiatric, Substance Abuse, and Opioid treatment) $35 copay $40 copay
Added Ambulance Services (Treat no Transport) Not covered $50 copayIncreased Urgent Care Copay $50 copay $65 copayIncreased Outpatient Rehab Services (PT, OT and ST) $35 copay $40 copayIncreased Medicare Covered Dental, Hearing,Vision, and Podiatry copays $35 copay $40 copayAdded Dental Panoramic X-rays Not Covered $0 copay every 36 monthsIncreased Comprehensive Dental allowance $250 every year $600 yearly allowance with 50% coinsuranceAdded OTC allowance Not covered $25
Plan Spotlight! Now offers access to the full UPMC for Life participating provider network and added OTC allowance!
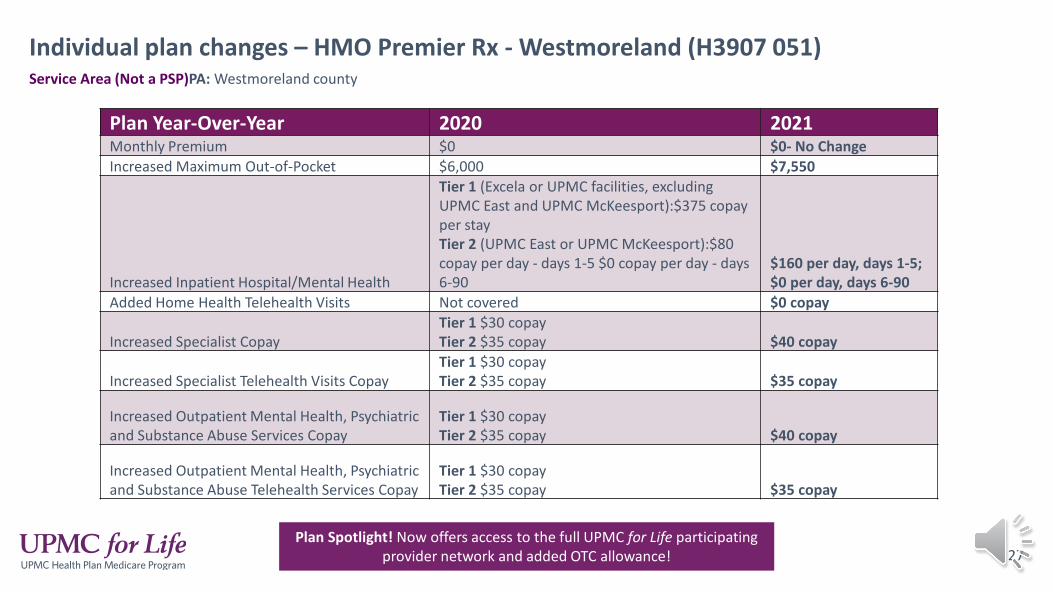
Individual plan changes – HMO Premier Rx - Westmoreland (H3907 051)
27
Service Area (Not a PSP)PA: Westmoreland county
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No ChangeIncreased Maximum Out-of-Pocket $6,000 $7,550
Increased Inpatient Hospital/Mental Health
Tier 1 (Excela or UPMC facilities, excluding UPMC East and UPMC McKeesport):$375 copay per stayTier 2 (UPMC East or UPMC McKeesport):$80 copay per day - days 1-5 $0 copay per day - days 6-90
$160 per day, days 1-5;$0 per day, days 6-90
Added Home Health Telehealth Visits Not covered $0 copay
Increased Specialist CopayTier 1 $30 copay Tier 2 $35 copay $40 copay
Increased Specialist Telehealth Visits CopayTier 1 $30 copay Tier 2 $35 copay $35 copay
Increased Outpatient Mental Health, Psychiatric and Substance Abuse Services Copay
Tier 1 $30 copay Tier 2 $35 copay $40 copay
Increased Outpatient Mental Health, Psychiatric and Substance Abuse Telehealth Services Copay
Tier 1 $30 copay Tier 2 $35 copay $35 copay
Plan Spotlight! Now offers access to the full UPMC for Life participating provider network and added OTC allowance!
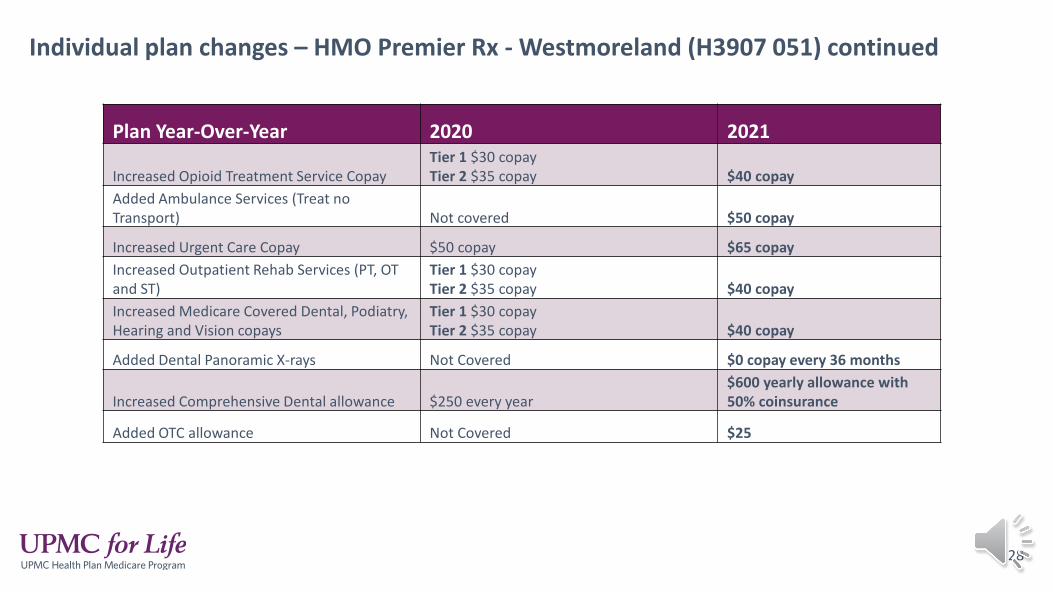
Individual plan changes – HMO Premier Rx - Westmoreland (H3907 051) continued
28
Plan Year-Over-Year 2020 2021
Increased Opioid Treatment Service CopayTier 1 $30 copay Tier 2 $35 copay $40 copay
Added Ambulance Services (Treat no Transport) Not covered $50 copay
Increased Urgent Care Copay $50 copay $65 copayIncreased Outpatient Rehab Services (PT, OT and ST)
Tier 1 $30 copay Tier 2 $35 copay $40 copay
Increased Medicare Covered Dental, Podiatry, Hearing and Vision copays
Tier 1 $30 copay Tier 2 $35 copay $40 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Increased Comprehensive Dental allowance $250 every year$600 yearly allowance with 50% coinsurance
Added OTC allowance Not Covered $25
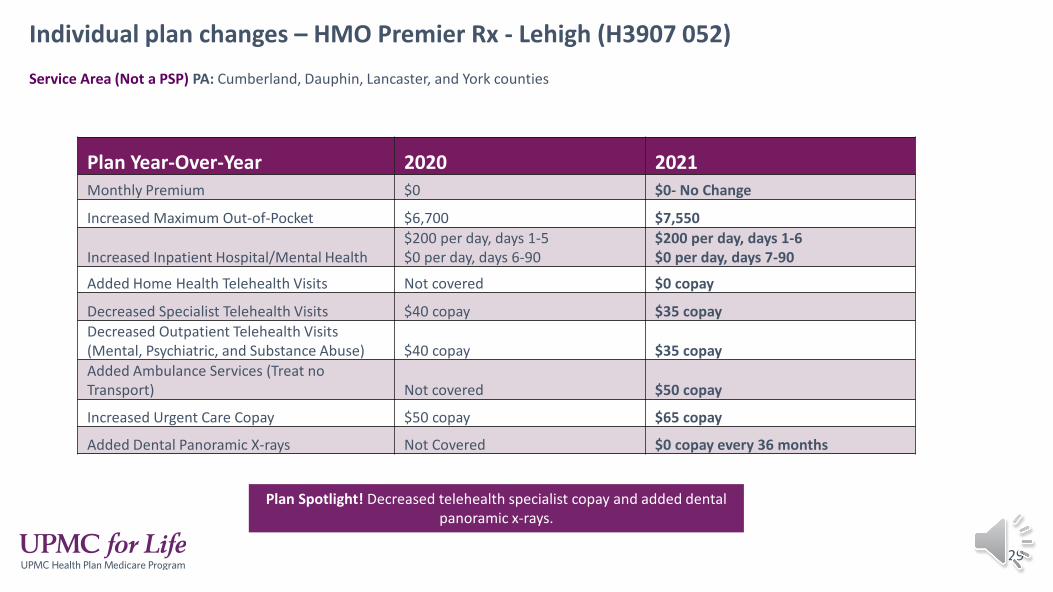
Individual plan changes – HMO Premier Rx - Lehigh (H3907 052)
29
Service Area (Not a PSP) PA: Cumberland, Dauphin, Lancaster, and York counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No Change
Increased Maximum Out-of-Pocket $6,700 $7,550
Increased Inpatient Hospital/Mental Health$200 per day, days 1-5$0 per day, days 6-90
$200 per day, days 1-6$0 per day, days 7-90
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Specialist Telehealth Visits $40 copay $35 copayDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay $35 copayAdded Ambulance Services (Treat no Transport) Not covered $50 copay
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered $0 copay every 36 months
Plan Spotlight! Decreased telehealth specialist copay and added dental panoramic x-rays.
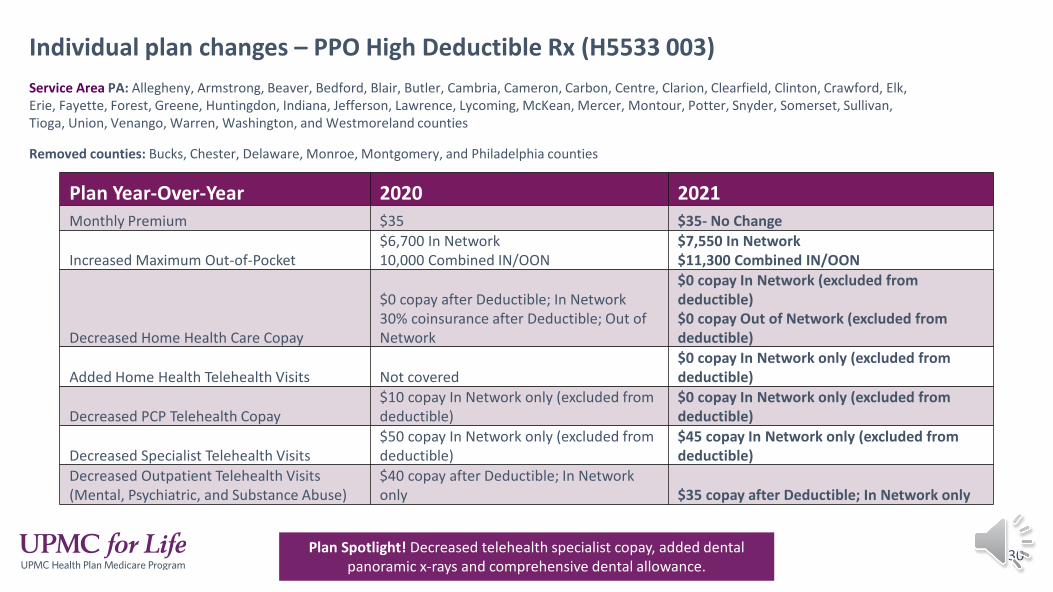
Individual plan changes – PPO High Deductible Rx (H5533 003)
30
Service Area PA: Allegheny, Armstrong, Beaver, Bedford, Blair, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Elk, Erie, Fayette, Forest, Greene, Huntingdon, Indiana, Jefferson, Lawrence, Lycoming, McKean, Mercer, Montour, Potter, Snyder, Somerset, Sullivan, Tioga, Union, Venango, Warren, Washington, and Westmoreland counties
Removed counties: Bucks, Chester, Delaware, Monroe, Montgomery, and Philadelphia counties
Plan Year-Over-Year 2020 2021Monthly Premium $35 $35- No Change
Increased Maximum Out-of-Pocket$6,700 In Network10,000 Combined IN/OON
$7,550 In Network$11,300 Combined IN/OON
Decreased Home Health Care Copay
$0 copay after Deductible; In Network 30% coinsurance after Deductible; Out of Network
$0 copay In Network (excluded from deductible)$0 copay Out of Network (excluded from deductible)
Added Home Health Telehealth Visits Not covered$0 copay In Network only (excluded from deductible)
Decreased PCP Telehealth Copay$10 copay In Network only (excluded from deductible)
$0 copay In Network only (excluded from deductible)
Decreased Specialist Telehealth Visits$50 copay In Network only (excluded from deductible)
$45 copay In Network only (excluded from deductible)
Decreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse)
$40 copay after Deductible; In Network only $35 copay after Deductible; In Network only
Plan Spotlight! Decreased telehealth specialist copay, added dental panoramic x-rays and comprehensive dental allowance.
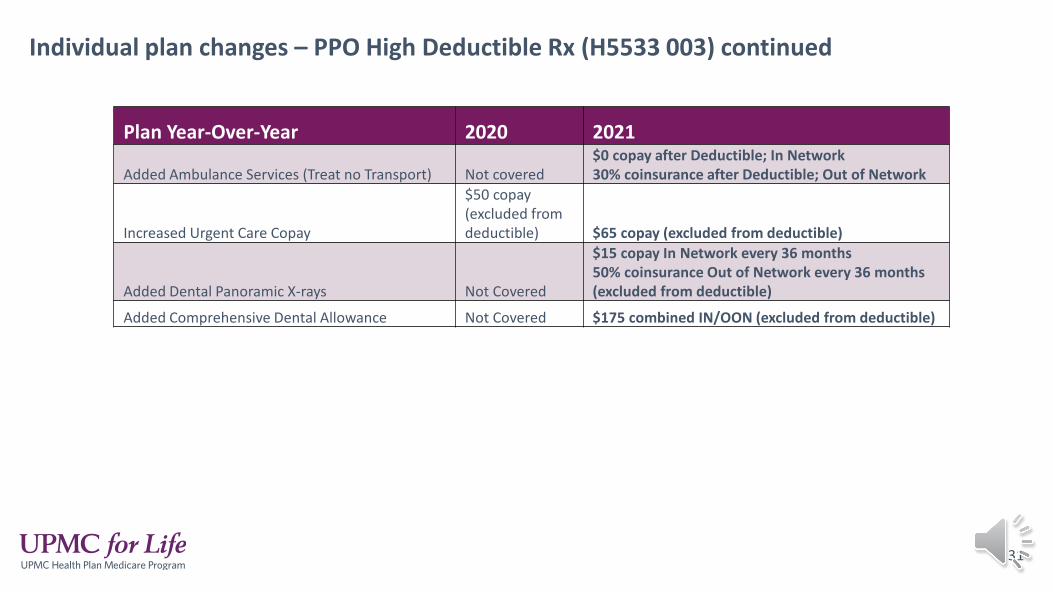
Individual plan changes – PPO High Deductible Rx (H5533 003) continued
31
Plan Year-Over-Year 2020 2021
Added Ambulance Services (Treat no Transport) Not covered$0 copay after Deductible; In Network30% coinsurance after Deductible; Out of Network
Increased Urgent Care Copay
$50 copay (excluded from deductible) $65 copay (excluded from deductible)
Added Dental Panoramic X-rays Not Covered
$15 copay In Network every 36 months50% coinsurance Out of Network every 36 months (excluded from deductible)
Added Comprehensive Dental Allowance Not Covered $175 combined IN/OON (excluded from deductible)

Individual plan changes – PPO Rx Enhanced (H5533 005)
32
Service Area PA: Allegheny, Armstrong, Beaver, Bedford, Blair, Butler, Cambria, Cameron, Carbon, Centre, Clarion, Clearfield, Clinton, Crawford, Elk, Erie, Fayette, Forest, Greene, Huntingdon, Indiana, Jefferson, Lawrence, Lycoming, McKean, Mercer, Montour, Potter, Snyder, Somerset, Sullivan, Tioga, Union, Venango, Warren, Washington, and Westmoreland counties
Removed counties: Bucks, Chester, Delaware, Monroe, Montgomery, and Philadelphia counties
Plan Year-Over-Year 2020 2021Increased Monthly Premium $135 $136
Increased Maximum Out-of-Pocket$6,700 In Network10,000 Combined IN/OON
$7,550 In Network$11,300 Combined IN/OON
Decreased Home Health Care Copay
$0 copay In Network30% coinsurance after Deductible; Out of Network
$0 copay In Network $0 copay Out of Network (excludedfrom deductible)
Added Home Health Telehealth Visits Not covered$0 copay In Network only (excluded from deductible)
Decreased PCP Telehealth Copay $5 copay In Network only $0 copay In Network only
Decreased Specialist Telehealth Visits $40 copay In Network only $35 copay In Network only Decreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay; In Network only $35 copay; In Network only
Plan Spotlight! Decreased telehealth specialist copay and added dental panoramic x-rays.
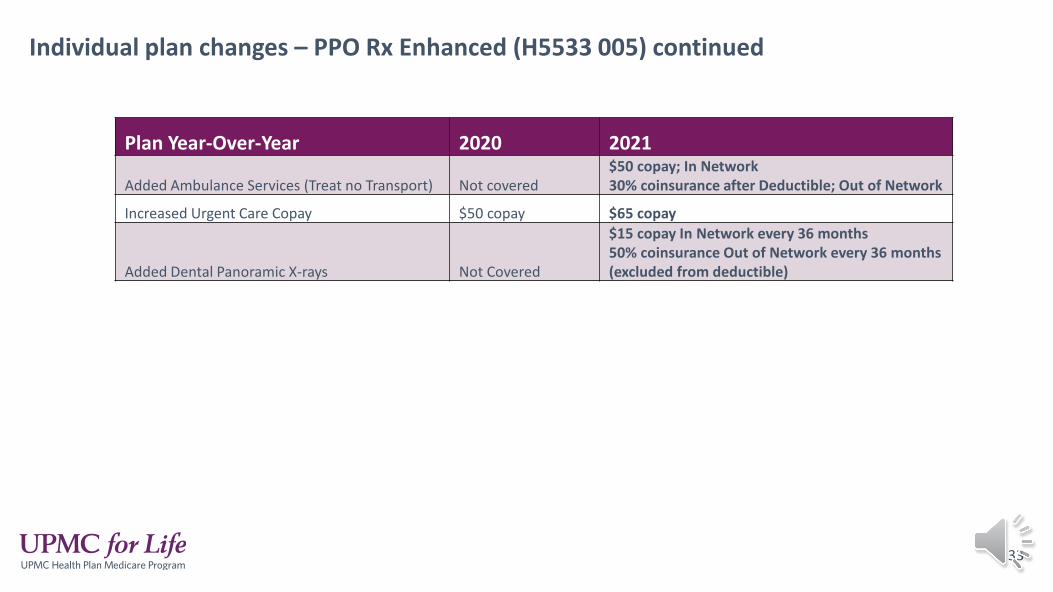
Individual plan changes – PPO Rx Enhanced (H5533 005) continued
33
Plan Year-Over-Year 2020 2021
Added Ambulance Services (Treat no Transport) Not covered$50 copay; In Network30% coinsurance after Deductible; Out of Network
Increased Urgent Care Copay $50 copay $65 copay
Added Dental Panoramic X-rays Not Covered
$15 copay In Network every 36 months50% coinsurance Out of Network every 36 months (excluded from deductible)
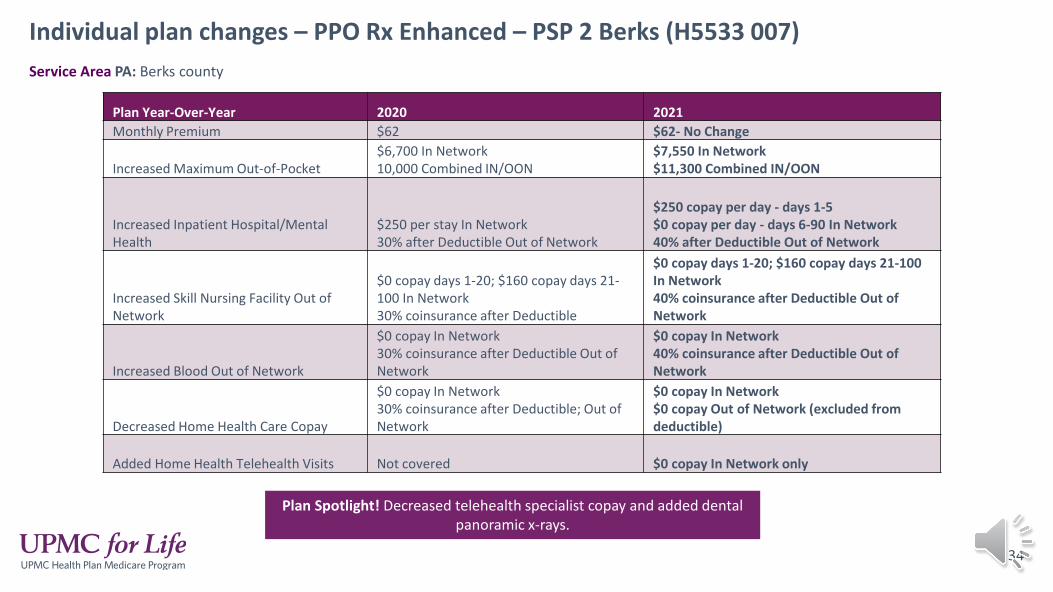
Individual plan changes – PPO Rx Enhanced – PSP 2 Berks (H5533 007)
34
Service Area PA: Berks county
Plan Year-Over-Year 2020 2021Monthly Premium $62 $62- No Change
Increased Maximum Out-of-Pocket$6,700 In Network10,000 Combined IN/OON
$7,550 In Network$11,300 Combined IN/OON
Increased Inpatient Hospital/Mental Health
$250 per stay In Network 30% after Deductible Out of Network
$250 copay per day - days 1-5$0 copay per day - days 6-90 In Network40% after Deductible Out of Network
Increased Skill Nursing Facility Out of Network
$0 copay days 1-20; $160 copay days 21-100 In Network 30% coinsurance after Deductible
$0 copay days 1-20; $160 copay days 21-100 In Network 40% coinsurance after Deductible Out of Network
Increased Blood Out of Network
$0 copay In Network 30% coinsurance after Deductible Out of Network
$0 copay In Network40% coinsurance after Deductible Out of Network
Decreased Home Health Care Copay
$0 copay In Network 30% coinsurance after Deductible; Out of Network
$0 copay In Network $0 copay Out of Network (excluded from deductible)
Added Home Health Telehealth Visits Not covered $0 copay In Network only
Plan Spotlight! Decreased telehealth specialist copay and added dental panoramic x-rays.

Individual plan changes – PPO Rx Enhanced – PSP 2 Berks (H5533 007) continued
35
Plan Year-Over-Year 2020 2021
Increased PCP Copay$5 In Network$30 after Deductible Out of Network
$5 In Network40% after Deductible Out of Network
Decreased PCP Telehealth Copay $5 copay In Network only $0 copay In Network only
Increased Out of Network Specialist Visit
$40 copay In Network$50 copay after Deductible Out of Network
$40 copay In Network40% coinsurance after Deductible Out of Network
Decreased Specialist Telehealth Visits $40 copay In Network only $35 copay In Network onlyIncreased Out of Network Outpatient Visits (Mental, Psychiatric, and Substance Abuse) 30% coinsurance after Deductible 40% coinsurance after DeductibleDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay In Network only $35 copay In Network onlyIncreased Out of Network Coinsurance for Medicare covered Chiropractic and Podiatry Services 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Coinsurance for Routine Chiropractic and Podiatry Services 30% coinsurance after Deductible
40% coinsurance (excluded from Deductible)
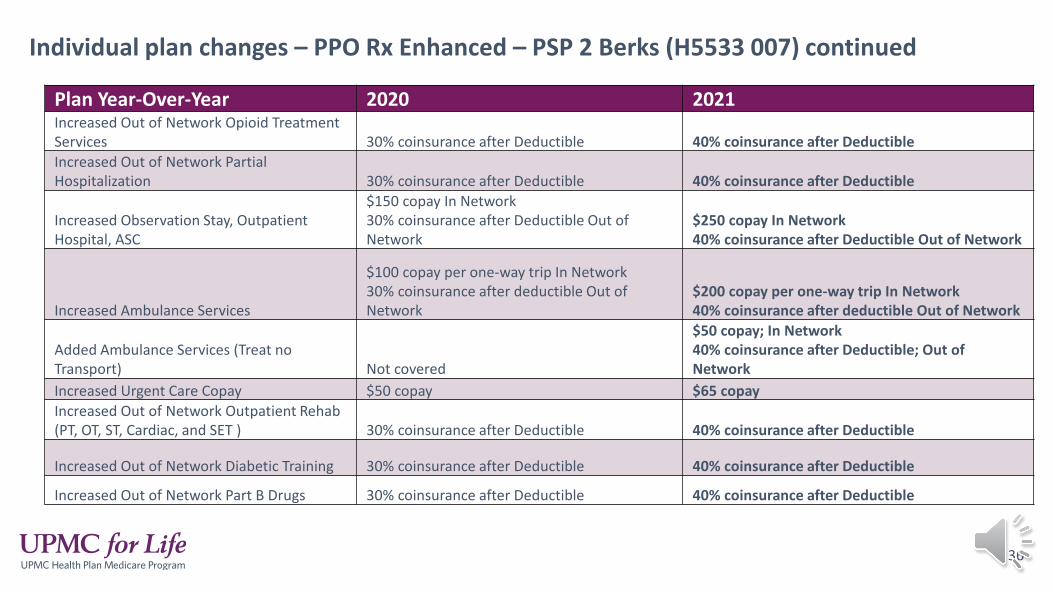
Individual plan changes – PPO Rx Enhanced – PSP 2 Berks (H5533 007) continued
36
Plan Year-Over-Year 2020 2021Increased Out of Network Opioid Treatment Services 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Partial Hospitalization 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Observation Stay, Outpatient Hospital, ASC
$150 copay In Network30% coinsurance after Deductible Out of Network
$250 copay In Network40% coinsurance after Deductible Out of Network
Increased Ambulance Services
$100 copay per one-way trip In Network30% coinsurance after deductible Out of Network
$200 copay per one-way trip In Network40% coinsurance after deductible Out of Network
Added Ambulance Services (Treat no Transport) Not covered
$50 copay; In Network40% coinsurance after Deductible; Out of Network
Increased Urgent Care Copay $50 copay $65 copayIncreased Out of Network Outpatient Rehab (PT, OT, ST, Cardiac, and SET ) 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Out of Network Diabetic Training 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Out of Network Part B Drugs 30% coinsurance after Deductible 40% coinsurance after Deductible
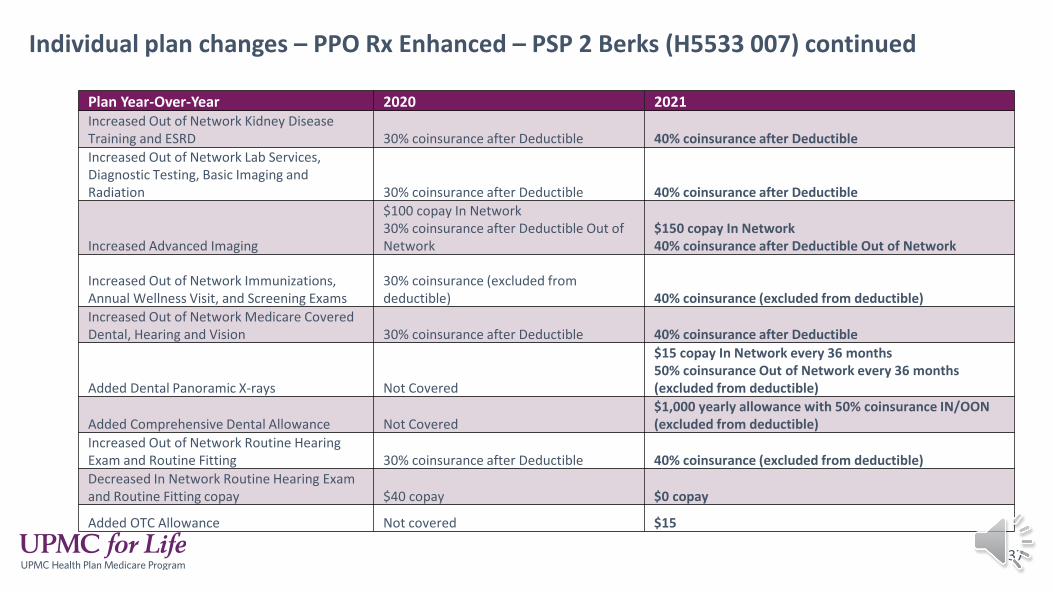
Individual plan changes – PPO Rx Enhanced – PSP 2 Berks (H5533 007) continued
37
Plan Year-Over-Year 2020 2021Increased Out of Network Kidney Disease Training and ESRD 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Lab Services, Diagnostic Testing, Basic Imaging and Radiation 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Advanced Imaging
$100 copay In Network30% coinsurance after Deductible Out of Network
$150 copay In Network40% coinsurance after Deductible Out of Network
Increased Out of Network Immunizations, Annual Wellness Visit, and Screening Exams
30% coinsurance (excluded from deductible) 40% coinsurance (excluded from deductible)
Increased Out of Network Medicare Covered Dental, Hearing and Vision 30% coinsurance after Deductible 40% coinsurance after Deductible
Added Dental Panoramic X-rays Not Covered
$15 copay In Network every 36 months50% coinsurance Out of Network every 36 months (excluded from deductible)
Added Comprehensive Dental Allowance Not Covered$1,000 yearly allowance with 50% coinsurance IN/OON (excluded from deductible)
Increased Out of Network Routine Hearing Exam and Routine Fitting 30% coinsurance after Deductible 40% coinsurance (excluded from deductible)Decreased In Network Routine Hearing Exam and Routine Fitting copay $40 copay $0 copay
Added OTC Allowance Not covered $15

Individual plan changes – PPO Rx Enhanced – Lehigh Cap/NEPA (H5533 008)
38
Service Area PA: Adams, Bradford, Cumberland, Dauphin, Fulton, Juniata, Lancaster, Lebanon, Lehigh, Mifflin, Northampton, Perry, Susquehanna, Wayne, Wyoming, and York counties
Removed counties: Lackawanna and Luzerne
Plan Year-Over-Year 2020 2021Monthly Premium $47 $60
Increased Maximum Out-of-Pocket$6,700 In Network10,000 Combined IN/OON
$7,550 In Network$11,300 Combined IN/OON
Increased Inpatient Hospital/Mental Health
$250 per stay In Network;30% after Deductible Out of Network
$275 copay per day - days 1-5$0 copay per day - days 6-90 In Network;40% after Deductible Out of Network
Increased Out of Network Skilled Nursing Facility
$0 copay days 1-20; $160 copay days 21-100 In Network30% coinsurance after Deductible Out of Network
$0 copay days 1-20; $160 copay days 21-100 In Network40% coinsurance after Deductible Out of Network
Increased Out of Network Blood
$0 copay In Network;30% coinsurance after Deductible Out of Network
$0 copay In Network40% coinsurance after Deductible Out of Network
Decreased Home Health Care Copay
$0 copay In Network30% coinsurance after Deductible; Out of Network
$0 copay In Network$0 copay Out of Network (excluded from deductible)
Added Home Health Telehealth Visits Not covered $0 copay In Network only
Plan Spotlight! Decreased telehealth specialist copay, added dental panoramic x-rays, and added OTC

Individual plan changes – PPO Rx Enhanced – Lehigh Cap/NEPA (H5533 008) continued
39
Plan Year-Over-Year 2020 2021
Increased Out of Network PCP Copay
$5 In Network;30% after deductible Out of Network
$5 In Network;40% after deductible Out of Network
Decreased PCP Telehealth Copay $5 copay In Network only $0 copay In Network only
Increased Out of Network Specialist Visit
$40 copay In Network30% after Deductible Out of Network
$40 copay In Network40% coinsurance after Deductible Out of Network
Decreased Specialist Telehealth Visits $40 copay In Network only $35 copay In Network onlyIncreased Out of Network Outpatient Visits (Mental, Psychiatric, and Substance Abuse) 30% coinsurance after Deductible 40% coinsurance after DeductibleDecreased Outpatient Telehealth Visits (Mental, Psychiatric, and Substance Abuse) $40 copay In Network only $35 copay In Network onlyIncreased Out of Network Medicare covered Chiropractic and Podiatry Services 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Coinsurance for Routine Chiropractic and Podiatry Services
30% coinsurance (excluded from Deductible) 40% coinsurance (excluded from Deductible)
Increased Out of Network Opioid Treatment Services 30% coinsurance after Deductible 40% coinsurance after Deductible
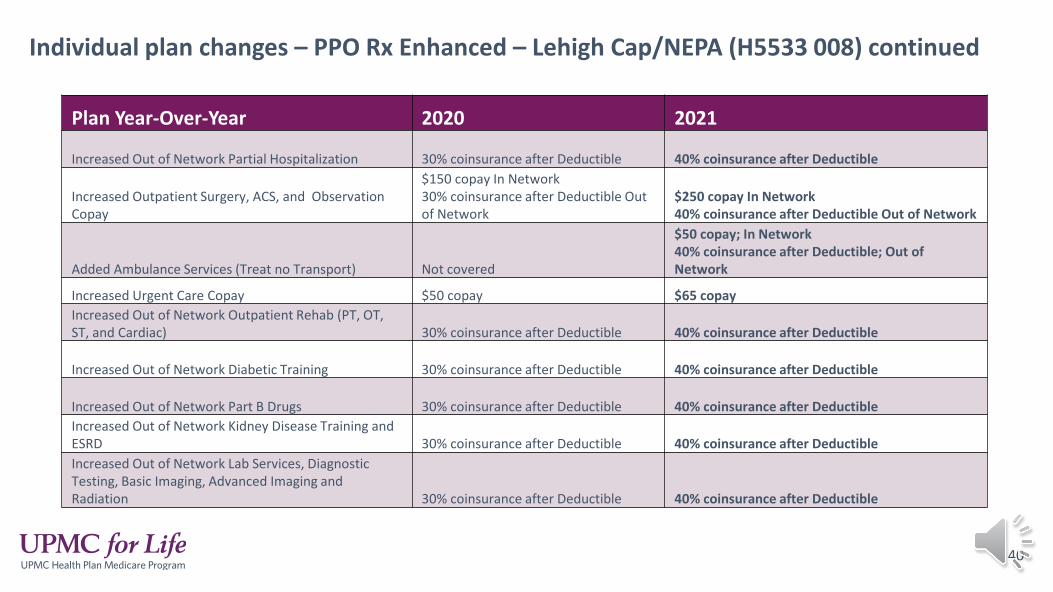
Individual plan changes – PPO Rx Enhanced – Lehigh Cap/NEPA (H5533 008) continued
40
Plan Year-Over-Year 2020 2021
Increased Out of Network Partial Hospitalization 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Outpatient Surgery, ACS, and Observation Copay
$150 copay In Network30% coinsurance after Deductible Out of Network
$250 copay In Network40% coinsurance after Deductible Out of Network
Added Ambulance Services (Treat no Transport) Not covered
$50 copay; In Network40% coinsurance after Deductible; Out of Network
Increased Urgent Care Copay $50 copay $65 copayIncreased Out of Network Outpatient Rehab (PT, OT, ST, and Cardiac) 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Out of Network Diabetic Training 30% coinsurance after Deductible 40% coinsurance after Deductible
Increased Out of Network Part B Drugs 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Kidney Disease Training and ESRD 30% coinsurance after Deductible 40% coinsurance after DeductibleIncreased Out of Network Lab Services, Diagnostic Testing, Basic Imaging, Advanced Imaging and Radiation 30% coinsurance after Deductible 40% coinsurance after Deductible
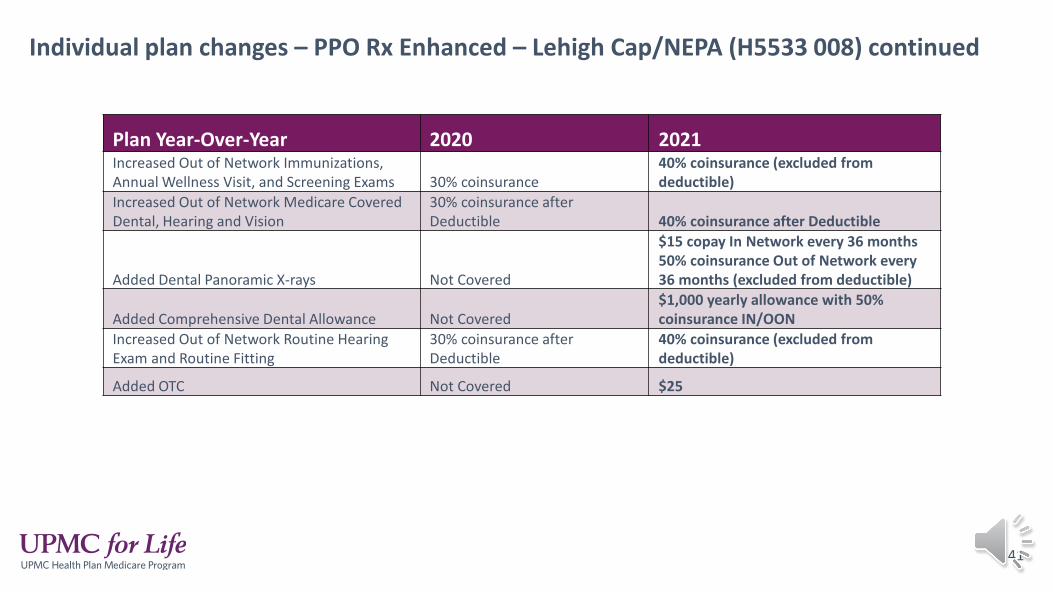
Individual plan changes – PPO Rx Enhanced – Lehigh Cap/NEPA (H5533 008) continued
41
Plan Year-Over-Year 2020 2021Increased Out of Network Immunizations, Annual Wellness Visit, and Screening Exams 30% coinsurance
40% coinsurance (excluded fromdeductible)
Increased Out of Network Medicare Covered Dental, Hearing and Vision
30% coinsurance after Deductible 40% coinsurance after Deductible
Added Dental Panoramic X-rays Not Covered
$15 copay In Network every 36 months50% coinsurance Out of Network every 36 months (excluded from deductible)
Added Comprehensive Dental Allowance Not Covered$1,000 yearly allowance with 50% coinsurance IN/OON
Increased Out of Network Routine Hearing Exam and Routine Fitting
30% coinsurance after Deductible
40% coinsurance (excluded from deductible)
Added OTC Not Covered $25
Benefit reminders
42
Chiropractic Services• All Medicare plans will have tiered benefits for
Chiropractic services.
• Tier 1: $18, Tier 2: $20.
• Member materials we will be required to list the tiering because it is in the bid. However, no chiropractors are tier 2 and the copay will always be $18.
Telehealth benefit• Members can virtually visit with their doctor over the
phone or online if their provider participates in telehealth. A virtual specialist visit has a lower copay thanan in-person visit. The provider must be in the same state as the member during the visit.
• This benefit includes PCP visits, specialist visits, home health, outpatient mental health, outpatient substance abuse, psychiatric services, and diabetes self-management services
• Telehealth is only offered in network. There is no out-of-network benefit for PPO plans.

Benefit reminder – Travel concierge program
43
Travel Concierge Program• Included for all UPMC for Life HMO Individual and Group plans
• Medicare HMO members have in-network coverage while traveling in Arizona, Florida, Georgia, North Carolina, South Carolina, and Tennessee.There is a six-month limit for travel coverage
• Members are encouraged to contact the Health Plan prior to services being rendered, however, it is not required.
• Must provide all plan-covered services (including supplemental benefits) at in-network member cost sharing levels.
• Services that currently require an authorization will also require an authorization under the Travel Concierge Program
• Providers cannot balance bill members.
• Does not apply for members in the Complete Care SNP plan or PPO plans. PPO members will still continue to have out-of-network cost sharing amounts.
Please note: There are contracted providers in these states. PPO members will pay in network cost-sharing for these providers.

Benefit reminder – over-the-counter (OTC) allowance
44
OTC Allowance
Medicare HMO and PPO plan allowance• Some UPMC for Life HMO and PPO plans now
include a quarterly allowance that can be used to buy covered health care products.
• Members will be sent a mail order catalog with hundreds of items to choose from. Members WILL NOT receive a retail card; they must purchase through the mail order catalog.
• This allowance does not roll over from quarter to quarter. It must be used in full each quarter or the remaining amount is lost.
Plan name OTC allowanceHMO Premier Rx (Allegheny, Beaver, Bedford, Blair, Butler, Lycoming, Tioga, Somerset, Washington)-046 $25 allowance per quarterHMO Premier Rx (Erie, Lawrence, Mercer, Venango)-050 $25 allowance per quarterHMO Premier Rx (Westmoreland)-051 $25 allowance per quarter
HMO No Rx -002 $50 allowance per quarter
HMO Deductible Rx- 037 $25 allowance per quarter
HMO Rx Choice- 049 $40 allowance per quarterHMO Rx- 029 $50 allowance per quarter
PPO Rx Enhanced (Berks)- 007 $15 allowance per quarterPPO Rx Enhanced (Lehigh Cap)-008 $25 allowance per quarter

45
Benefit updates – prior authorization and step therapy
Added for:• Observation Stays• Acupuncture Services (specialist visit)• Outpatient Dialysis (for initiating and
coordinating)• Step Therapy for Part B drugs (Part B to Part B
drugs and Part D to Part B drugs)
*Authorization for these services is the responsibility of the provider.
46
Benefit updates – dental coverage
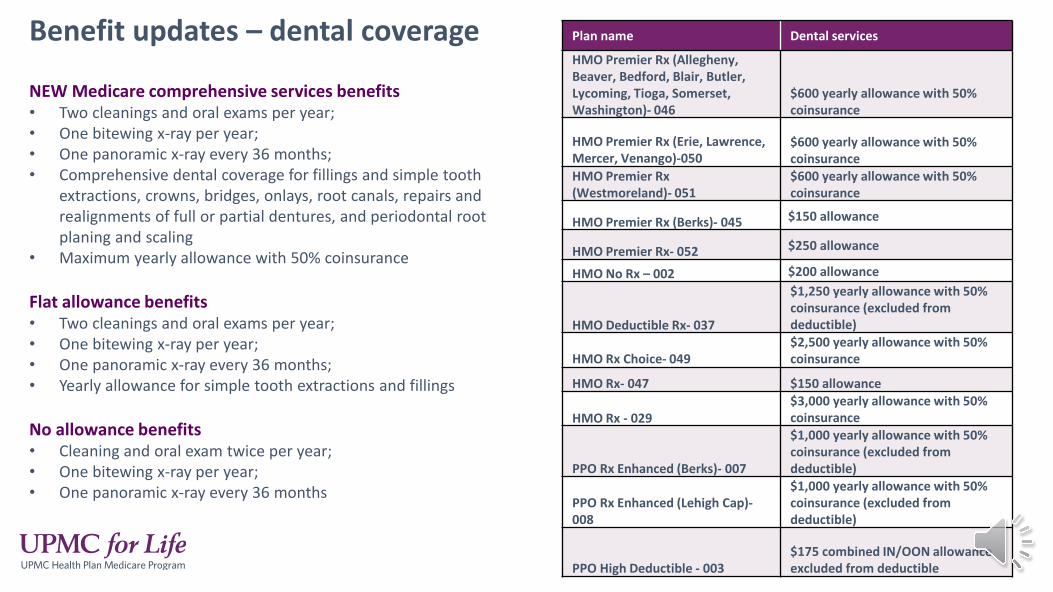
NEW Medicare comprehensive services benefits• Two cleanings and oral exams per year;• One bitewing x-ray per year;• One panoramic x-ray every 36 months;• Comprehensive dental coverage for fillings and simple tooth
extractions, crowns, bridges, onlays, root canals, repairs and realignments of full or partial dentures, and periodontal root planing and scaling
• Maximum yearly allowance with 50% coinsurance
Flat allowance benefits• Two cleanings and oral exams per year;• One bitewing x-ray per year;• One panoramic x-ray every 36 months;• Yearly allowance for simple tooth extractions and fillings
No allowance benefits• Cleaning and oral exam twice per year;• One bitewing x-ray per year;• One panoramic x-ray every 36 months
Plan name Dental services
HMO Premier Rx (Allegheny, Beaver, Bedford, Blair, Butler, Lycoming, Tioga, Somerset, Washington)- 046
$600 yearly allowance with 50% coinsurance
HMO Premier Rx (Erie, Lawrence, Mercer, Venango)-050
$600 yearly allowance with 50% coinsurance
HMO Premier Rx (Westmoreland)- 051
$600 yearly allowance with 50% coinsurance
HMO Premier Rx (Berks)- 045 $150 allowance
HMO Premier Rx- 052 $250 allowance
HMO No Rx – 002 $200 allowance
HMO Deductible Rx- 037
$1,250 yearly allowance with 50% coinsurance (excluded from deductible)
HMO Rx Choice- 049$2,500 yearly allowance with 50% coinsurance
HMO Rx- 047 $150 allowance
HMO Rx - 029$3,000 yearly allowance with 50% coinsurance
PPO Rx Enhanced (Berks)- 007
$1,000 yearly allowance with 50% coinsurance (excluded from deductible)
PPO Rx Enhanced (Lehigh Cap)-008
$1,000 yearly allowance with 50% coinsurance (excluded from deductible)
PPO High Deductible - 003$175 combined IN/OON allowance excluded from deductible
Maximum out-of-pocketThe maximum out-of-pocket cost, otherwise known as a “safety net,” helps members with chronic conditions and other serious health problems to limit their yearly health care costs. This is not a deductible. It is the most a member would pay should they have a serious medical problem and need a lot of medical care. This year, because of changes to the Medicare program, the maximum out-of-pocket cost has increased.
Maximum out-of-pocket increases:• HMO plans - $7,550• PPO Plans - $7,550 in-network / $11,300 out-of-network
47
Key points• After the member has paid the maximum out-of-pocket amount in copays, coinsurance, and deductible, our
plan pays 100% of the cost for covered benefits. • The member does not pay anything for covered medical care after reaching the maximum out-of-pocket.• The increase in maximum out-of-pocket means that Medicare beneficiaries may pay more out-of-pocket for
covered services in 2021.• The over-whelming majority of UPMC for Life members, around 95%, do not hit the maximum out-of-pocket
each year. • For additional information please reference the talking points and FAQ that have been provided.

Employer Group
48
There are two types of employer group sponsored plans:
Contributory Groups (group bill) The employer group sponsor subsidizes all or a portion of the monthly premium. UPMC for Life will bill the employer group sponsor (or their designee) for the monthly premium.• Most of our custom plans are contributory plans.• The premium amount will NOT be listed.
Sponsorship Groups (individual bill)The employer group sponsor offers a Medicare Advantage or stand-alone prescription drug plan and the retirees pays the monthly premium directly to UPMC for Life. The premium amount will be listed.
2021 Employer Groups
49
• UPMC for Life offers “cookie” cutter HMO and PPO group plans• UPMC for Life HMO Standard with Rx• UPMC for Life HMO Prime with Rx• UPMC for Life HMO Deluxe with Rx• UPMC for Life PPO Prime with Rx• UPMC for Life PPO Deluxe with Rx
• What is a “cookie” cutter plan?• This means that multiple groups can share the same benefits and cost-share• For example, all groups that have the HMO Standard with Rx share the same plan
code, Summary of Benefits, ANOC, and Evidence of Coverage
• UPMC for Life also offers custom and National Complementary plans• National complementary plans have a national network and Original Medicare is the
primary payer. UPMC for Life then pays as secondary on these plans.
2021 Employer Groups
50
UPMC for Life employer groups don’t follow the same timeline as the Individual Plans• Our employer group plans do not follow the same strict CMS guidelines and timelines
like our individual plans. This means Product Operations has additional time to create and review the plan documents.
• The plan documents includes items like the Annual Notice of Change (ANOC), Summary of Benefits (SB), and Evidence of Coverage (EOC).
• The employer group documents aren’t created until the group sends back the renewal form.
• The plan documents will be posted to KIP as soon as they are available
2021 Employer Groups
51
UPMC for Life employer group benefit changes:• Reduced PCP telehealth copays to $0• Added home health telehealth at $0• Reduced telehealth specialist, outpatient mental health, outpatient
psychiatric services, and outpatient substance abuse copays by $5 • Added prior authorization for acupuncture (under specialist)• Added prior authorization for observation stays• Added prior authorization for outpatient services for dialysis• Added palliative care benefit• Added support for caregivers benefit• Service Area Counties: added Carbon, Centre, Monroe, and Montour
2021 Employer Groups
52

PrescriptionDrug Coverage
53
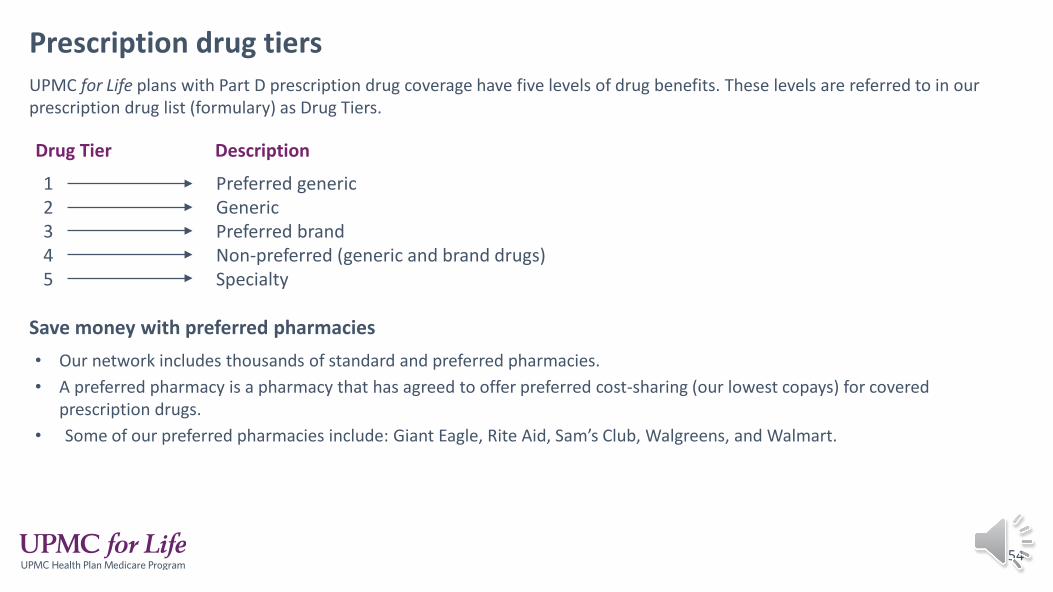
Prescription drug tiersUPMC for Life plans with Part D prescription drug coverage have five levels of drug benefits. These levels are referred to in our prescription drug list (formulary) as Drug Tiers.
54
Drug Tier
12345
Description
Preferred genericGenericPreferred brandNon-preferred (generic and brand drugs)Specialty
Save money with preferred pharmacies• Our network includes thousands of standard and preferred pharmacies.• A preferred pharmacy is a pharmacy that has agreed to offer preferred cost-sharing (our lowest copays) for covered
prescription drugs.• Some of our preferred pharmacies include: Giant Eagle, Rite Aid, Sam’s Club, Walgreens, and Walmart.
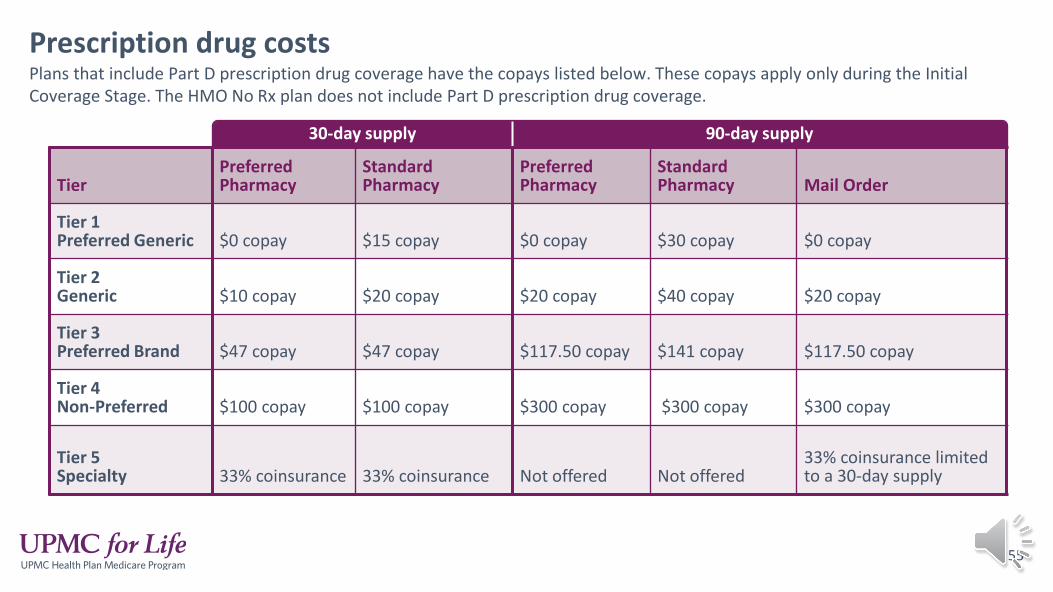
Prescription drug costsPlans that include Part D prescription drug coverage have the copays listed below. These copays apply only during the InitialCoverage Stage. The HMO No Rx plan does not include Part D prescription drug coverage.
30-day supply 90-day supply
TierPreferred Pharmacy
Standard Pharmacy
Preferred Pharmacy
Standard Pharmacy Mail Order
Tier 1 Preferred Generic $0 copay $15 copay $0 copay $30 copay $0 copay
Tier 2 Generic $10 copay $20 copay $20 copay $40 copay $20 copay
Tier 3 Preferred Brand $47 copay $47 copay $117.50 copay $141 copay $117.50 copay
Tier 4 Non-Preferred $100 copay $100 copay $300 copay $300 copay $300 copay
Tier 5 Specialty 33% coinsurance 33% coinsurance Not offered Not offered
33% coinsurance limitedto a 30-day supply
55
56
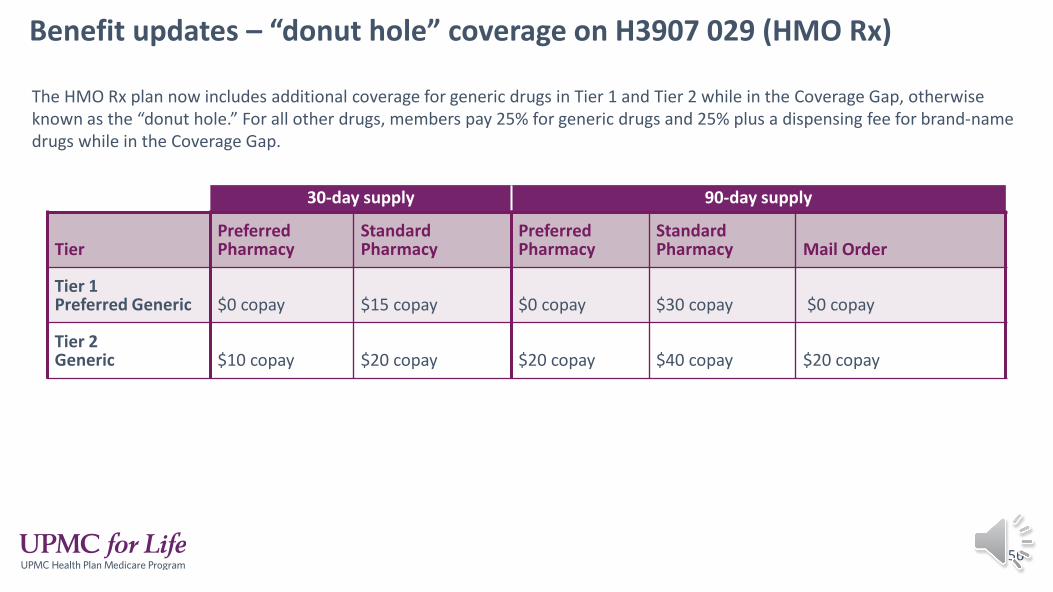
Benefit updates – “donut hole” coverage on H3907 029 (HMO Rx)
The HMO Rx plan now includes additional coverage for generic drugs in Tier 1 and Tier 2 while in the Coverage Gap, otherwise known as the “donut hole.” For all other drugs, members pay 25% for generic drugs and 25% plus a dispensing fee for brand-name drugs while in the Coverage Gap.
30-day supply 90-day supply
TierPreferred Pharmacy
Standard Pharmacy
Preferred Pharmacy
Standard Pharmacy Mail Order
Tier 1 Preferred Generic $0 copay $15 copay $0 copay $30 copay $0 copay
Tier 2 Generic $10 copay $20 copay $20 copay $40 copay $20 copay
57
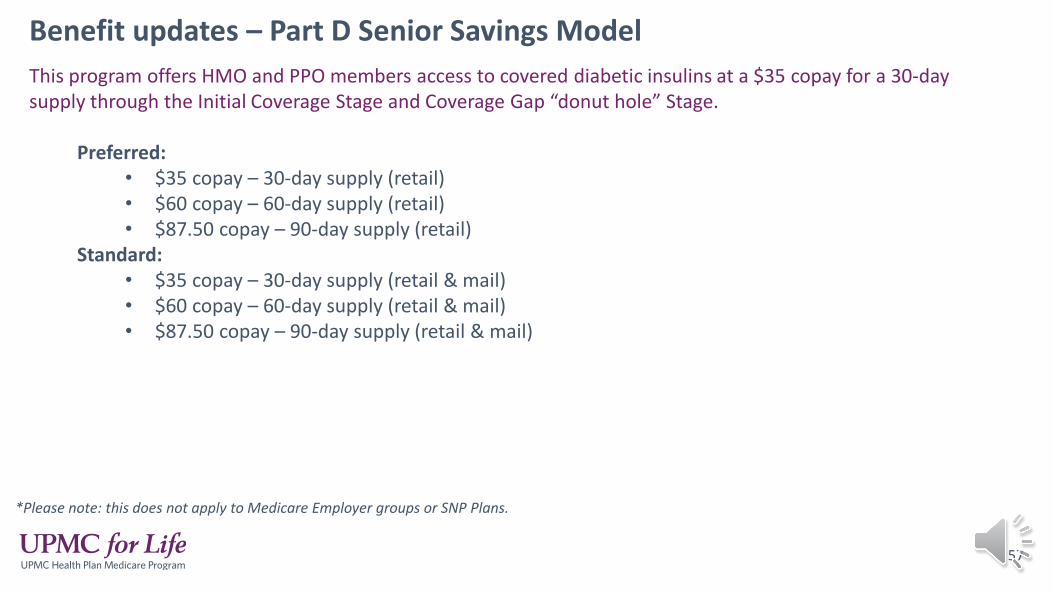
Benefit updates – Part D Senior Savings ModelThis program offers HMO and PPO members access to covered diabetic insulins at a $35 copay for a 30-day supply through the Initial Coverage Stage and Coverage Gap “donut hole” Stage.
Preferred: • $35 copay – 30-day supply (retail) • $60 copay – 60-day supply (retail) • $87.50 copay – 90-day supply (retail)
Standard: • $35 copay – 30-day supply (retail & mail) • $60 copay – 60-day supply (retail & mail) • $87.50 copay – 90-day supply (retail & mail)
*Please note: this does not apply to Medicare Employer groups or SNP Plans.
For 2021, there will be three comprehensive formularies:
• HMO/PPO – Main
• HMO Premier Rx - $0/$0
• Complete Care (HMO SNP)
Formulary updates
View the comprehensive formularies online for a full list of the drugs we cover for each plan. Select the plan type, state, and county to generate the appropriate formulary.
58

Find Plan Documents Online
59
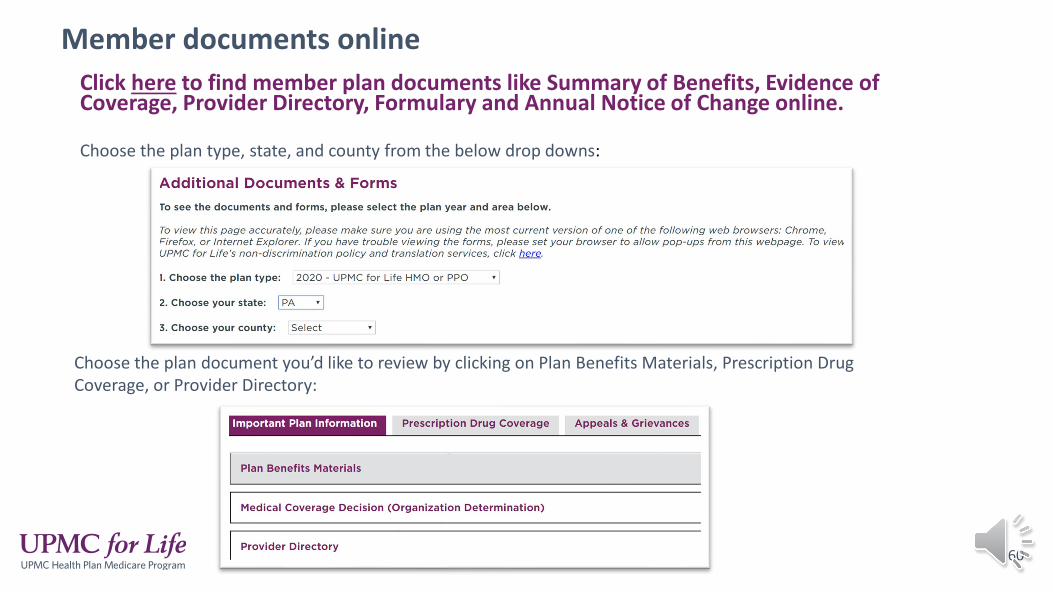
Click here to find member plan documents like Summary of Benefits, Evidence of Coverage, Provider Directory, Formulary and Annual Notice of Change online.
Member documents online
Choose the plan type, state, and county from the below drop downs:
Choose the plan document you’d like to review by clicking on Plan Benefits Materials, Prescription Drug Coverage, or Provider Directory:
60
Provider directory updatesStarting January 1, 2021 there will be five directories:1. UPMC Main (Full Network)2. Complete Care (HMO SNP)3. PSP2 (Tower Health/Berks) 4. Spanish PSP2 (Tower Health/Berks) 5. Pharmacy Directory
We are removing the PSP1 and PSP 3 full and radius directories because those plans now use the full UPMC for Life provider network.
Updates to the directories:• Added phone number to Cancer Center listing• Added Telehealth indicator
=Offers video visits (telehealth)
The Provider directories are posted to the website every month under documents and forms.
61

Online provider search tool – telehealth servicesTelehealth Program Page has been added to the online provider search tool to explain the program. Click here to view the online provider search tool.
62

Have questions?
Copyright 2020 UPMC Health Plan Inc. All rights reserved.<2021_PPTTEMP_20MC-SNP1337924 (AG) 5/13/20>
If you have any questions please email [email protected]!

2021 UPMC for Life SNP Product Training
Training Agenda
65
• UPMC for Life Complete Care Plans• Plan Overview• Service Area• New Plan for 2021• Benefit Changes
• Additional Information• Maximum Out-of-Pocket• Pharmacy Coverage• Find Plan Documents Online
We are changing our name!UPMC for Life Dual (HMO SNP) has changed its name to UPMC for Life Complete Care (HMO SNP) for 2021
This name change will be on the Member ID Cards and all Plan Materials
66
New plan name, same great coverage• Our SNP plans are now called UPMC for Life Complete Care (HMO SNP). • Our new name reflects the whole person care and security that we
provide to all our members. • We know that health isn’t just about access to doctors and hospitals. It’s
about each member and their needs as a person. That includes physical and emotional health, the money our members spend on keeping themselves healthy, and access to programs and services that allow our members to live their best life.
• SNP plan members will be receiving communications with their new plan name in mid-September.

UPMC for Life Complete Care Plans
67
Special needs plan overview
68
What is a Special Needs plan?• Medicare SNPs are a type of Medicare Advantage Plan (like an HMO or PPO). • Medicare SNPs limit membership to people with specific diseases or characteristics. • Medicare SNPs tailor their benefits, provider choices, and drug formularies to best meet the specific
needs of the groups they serve.
Who is eligible to enroll?• Individuals who qualify for a Special Needs Plan must meet one of the guidelines established by the
Centers for Medicare & Medicaid Services (CMS):• Institutionalized Medicare beneficiaries.• Individuals with severe or disabling chronic conditions.• Dual eligible beneficiaries.
Enrollment requirements• An individual can join UPMC for Life Complete Care if they are entitled to Medicare Part A, enrolled
in Medicare Part B, and receive full Medical Assistance. • An individual must live in the service area.
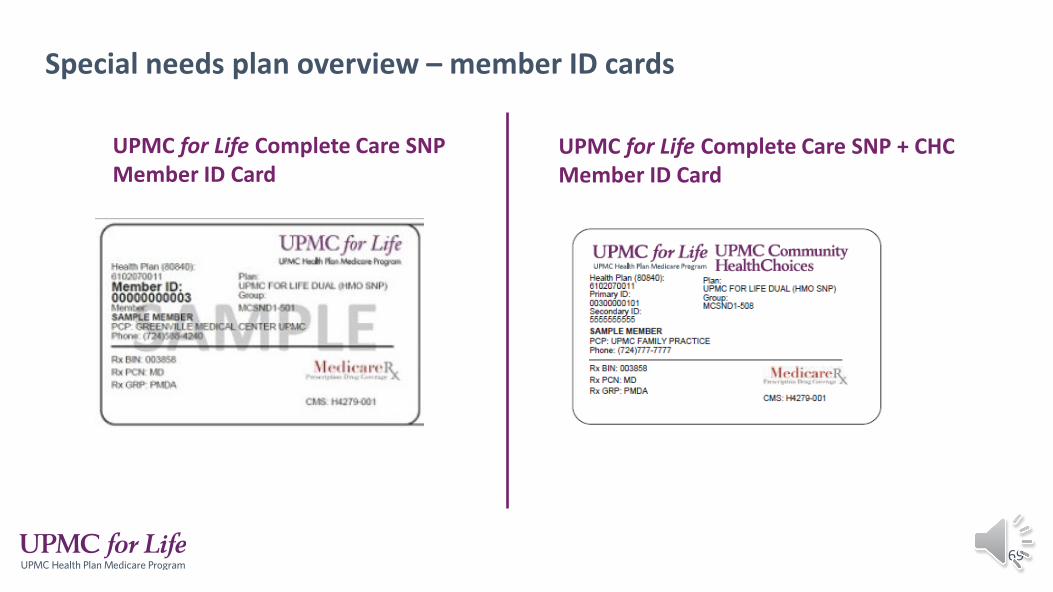
Special needs plan overview – member ID cards
69
UPMC for Life Complete Care SNP Member ID Card
UPMC for Life Complete Care SNP + CHC Member ID Card
UPMC for Life Complete Care (HMO SNP) service areas
70
UPMC for Life Complete Care • H4279 001 Operates under UPMC for You, Inc. license• H4279 004 Operates under UPMC for You, Inc. license• H7123 001 Operates under UPMC Health Coverage Inc.
H4279 - 001 service area• Adams, Allegheny, Armstrong, Beaver, Bedford, Blair, Bradford, Butler, Cambria, Cameron, Centre, Clarion,
Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Franklin, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lycoming, McKean, Mercer, Mifflin, Montour, Northampton, Perry, Potter, Snyder, Somerset, Sullivan, Tioga, Union, Venango, Warren, Washington, Westmoreland, and York
H4279 - 004 service area - NEW• Berks, Carbon, Lackawanna, Lehigh, Luzerne, Monroe, Northampton, Pike, Schuylkill, Susquehanna, Wayne, and
Wyoming
H7123 - 001 service area• Bucks, Chester, Delaware, Montgomery, and Philadelphia
71
72
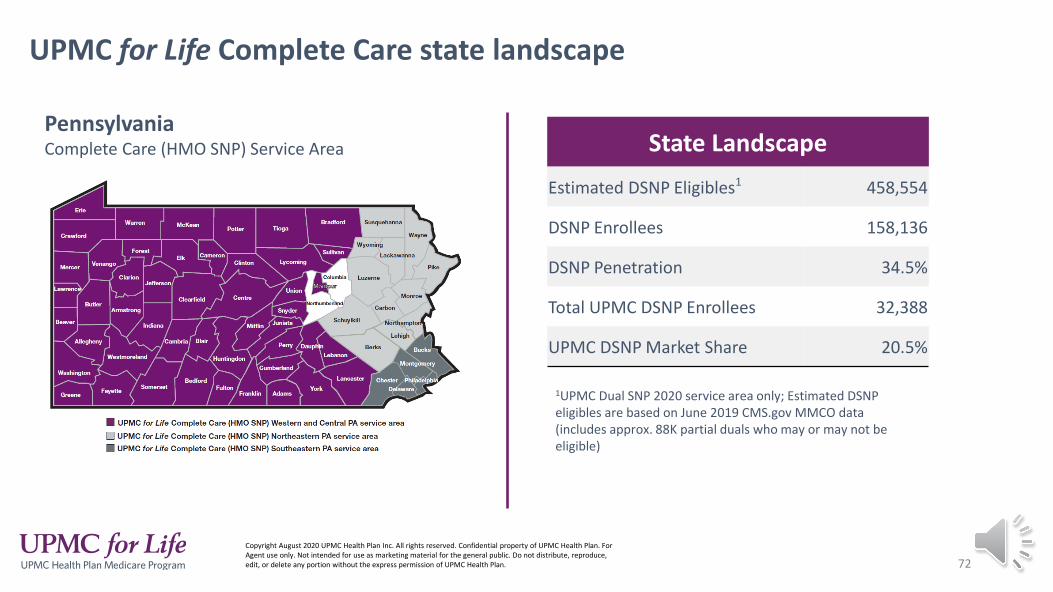
UPMC for Life Complete Care state landscape
PennsylvaniaComplete Care (HMO SNP) Service Area State Landscape
Estimated DSNP Eligibles1 458,554
DSNP Enrollees 158,136
DSNP Penetration 34.5%
Total UPMC DSNP Enrollees 32,388
UPMC DSNP Market Share 20.5%
1UPMC Dual SNP 2020 service area only; Estimated DSNP eligibles are based on June 2019 CMS.gov MMCO data (includes approx. 88K partial duals who may or may not be eligible)
Copyright August 2020 UPMC Health Plan Inc. All rights reserved. Confidential property of UPMC Health Plan. For Agent use only. Not intended for use as marketing material for the general public. Do not distribute, reproduce, edit, or delete any portion without the express permission of UPMC Health Plan.

New Plan for 2021
73
• UPMC for Life Complete Care (HMO SNP) – H4279 001 is not terming, but instead there is a new UPMC for Life Complete Care (HMO SNP) – H4279 004 plan.
• This new SNP plan covers Berks, Carbon, Lackawanna, Lehigh, Luzerne, Monroe, Northampton, Pike, Schuylkill, Susquehanna, Wayne, and Wyoming.
• Members currently enrolled in these counties will be termed from UPMC for Life Complete Care (H4279 001) and will need to re-enroll into UPMC for Life Complete Care (H4279 004).
• The members will receive a SAR (service area reduction) letter to inform them of this.

Plan Benefits
74
75
Plan benefits
• The SNP Plans provide all the usual services covered by original Medicare and some additional enhanced benefits.
• Members must use our network of doctors, specialists, and hospitals to receive covered care services.
• If member has UPMC CHC and UPMC for Life Complete Care, they will receive only one ID card and it will contain two member ID numbers. The first ID # will be listed as Primary which will be their DSNP member number; the second ID # will be listed as Secondary which will be their CHC number.
• UPMC for Life Complete Care members that have not enrolled with UPMC CHC must also show their Access or Community Health Choices card along with their UPMC for Life Complete Care card.
• These members will only receive a UPMC for Life card.
• The Secondary ID will be the member’s recipient ID number
The Medicare coverage through UPMC for Life Complete Care pays as primary and Medical Assistance (Medicaid) whether the member has coverage through UPMC CHC, another CHC or ACCESS pays as secondary.
76
Benefit updates – prior authorization and step therapy
Added for:
• Observation Stays• Acupuncture Services (Specialist Visit)• Outpatient Dialysis (for initiating and coordinating)• Step Therapy for Part B drugs (Part B to Part B drugs
and Part D to Part B drugs)
*Authorization for these services is the responsibility of the provider

Individual plan changes - Complete Care (DSNP) - (H4279 001)
77
Service Area PA: Adams, Allegheny, Armstrong, Beaver, Bedford, Blair, Bradford, Butler, Cambria, Cameron, Centre, Clarion, Clearfield, Clinton, Crawford, Cumberland, Dauphin, Elk, Erie, Fayette, Forest, Franklin, Fulton, Greene, Huntingdon, Indiana, Jefferson, Juniata, Lancaster, Lawrence, Lebanon, Lycoming, McKean, Mercer, Mifflin, Montour, Perry, Potter, Snyder, Somerset, Sullivan, Tioga, Union, Venango, Warren, Washington, Westmoreland, and York counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No Change
Added Home Health Telehealth Visits Not covered $0 copay
Increased Comprehensive Dental allowance $3,900 per year $5,000 per year
Increased Routine Vision Allowance $300 per year $400 per year
Added Health Savings Card (SSBCI) n/a $50 per quarter for healthy foods
Increased Mail-order OTCRetail card: $125; Mail-order: $200; Total: $325 allowance (with rollover)
Retail card: $125; Mail-order: $225; Total: $350 allowance (with rollover)
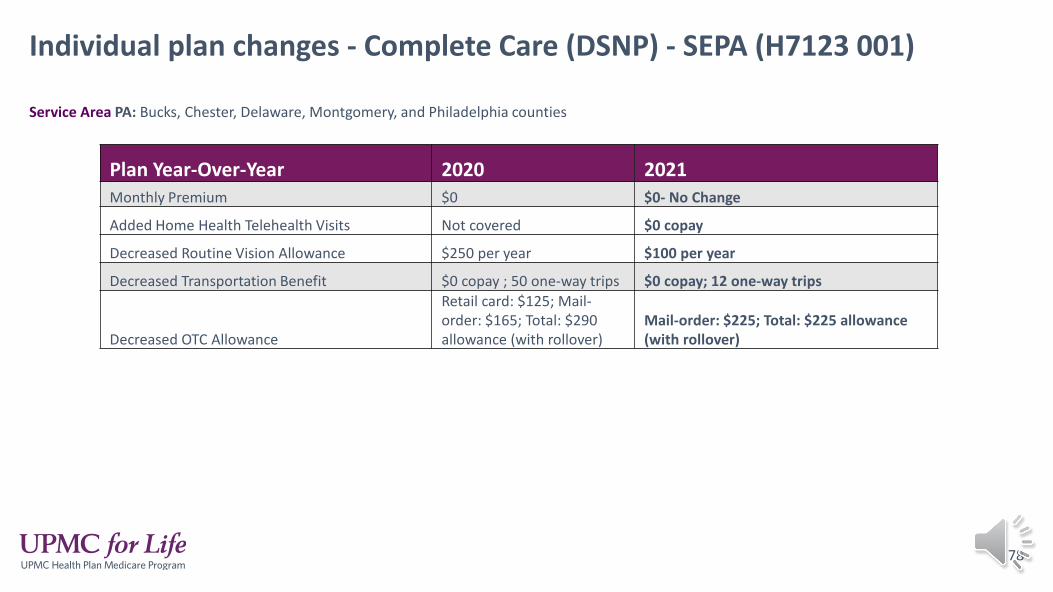
Individual plan changes - Complete Care (DSNP) - SEPA (H7123 001)
78
Service Area PA: Bucks, Chester, Delaware, Montgomery, and Philadelphia counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0- No Change
Added Home Health Telehealth Visits Not covered $0 copay
Decreased Routine Vision Allowance $250 per year $100 per year
Decreased Transportation Benefit $0 copay ; 50 one-way trips $0 copay; 12 one-way trips
Decreased OTC Allowance
Retail card: $125; Mail-order: $165; Total: $290 allowance (with rollover)
Mail-order: $225; Total: $225 allowance (with rollover)
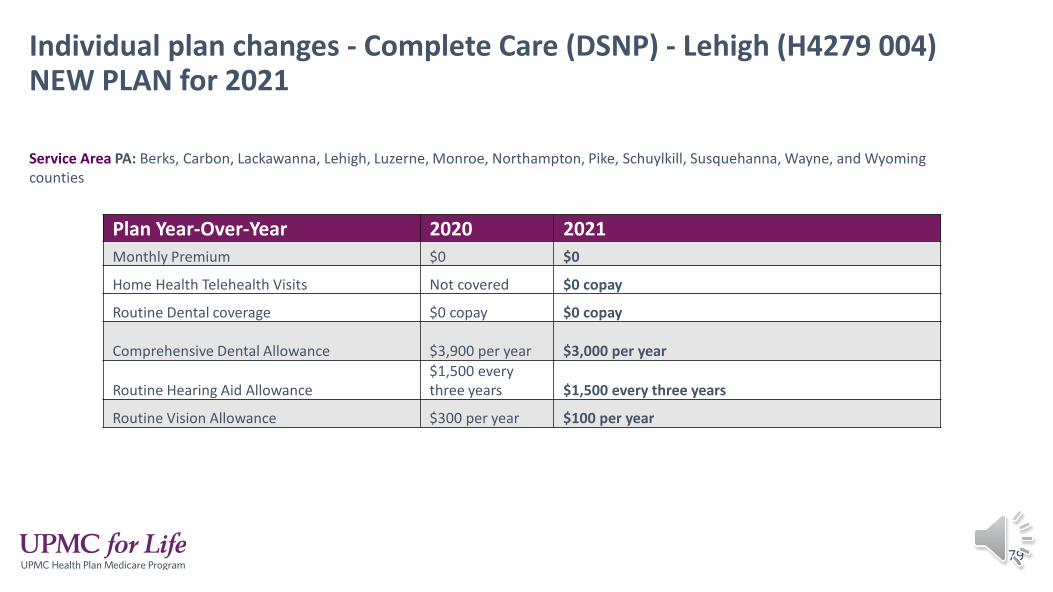
Individual plan changes - Complete Care (DSNP) - Lehigh (H4279 004)NEW PLAN for 2021
79
Service Area PA: Berks, Carbon, Lackawanna, Lehigh, Luzerne, Monroe, Northampton, Pike, Schuylkill, Susquehanna, Wayne, and Wyoming counties
Plan Year-Over-Year 2020 2021Monthly Premium $0 $0
Home Health Telehealth Visits Not covered $0 copay
Routine Dental coverage $0 copay $0 copay
Comprehensive Dental Allowance $3,900 per year $3,000 per year
Routine Hearing Aid Allowance$1,500 every three years $1,500 every three years
Routine Vision Allowance $300 per year $100 per year
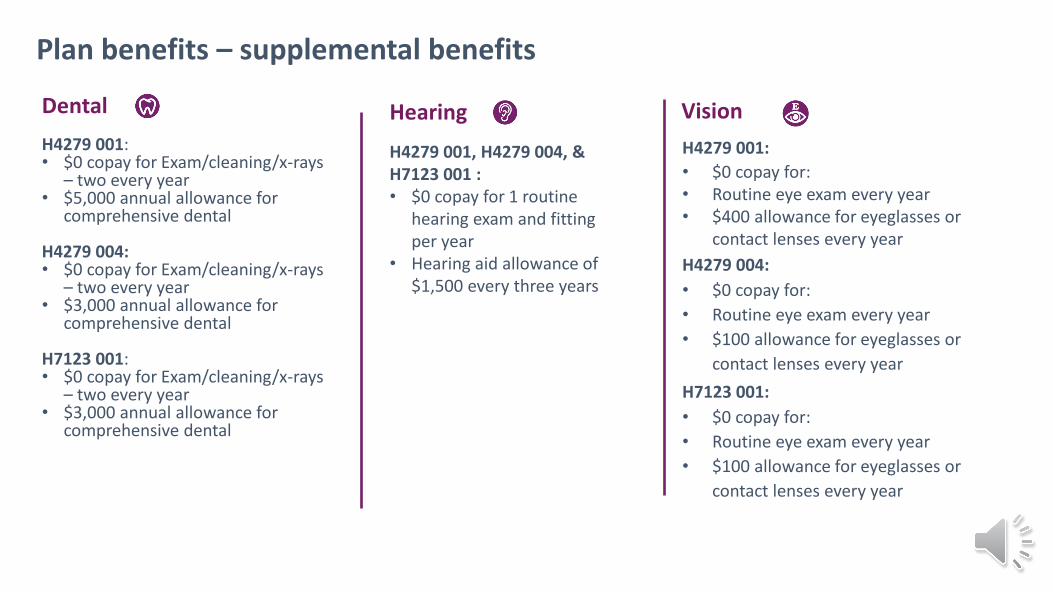
Plan benefits – supplemental benefits
Dental H4279 001:• $0 copay for Exam/cleaning/x-rays
– two every year• $5,000 annual allowance for
comprehensive dental
H4279 004:• $0 copay for Exam/cleaning/x-rays
– two every year• $3,000 annual allowance for
comprehensive dental
H7123 001:• $0 copay for Exam/cleaning/x-rays
– two every year• $3,000 annual allowance for
comprehensive dental
Hearing
H4279 001, H4279 004, & H7123 001 :• $0 copay for 1 routine
hearing exam and fitting per year
• Hearing aid allowance of $1,500 every three years
VisionH4279 001:• $0 copay for:• Routine eye exam every year• $400 allowance for eyeglasses or
contact lenses every year
H7123 001:• $0 copay for:• Routine eye exam every year• $100 allowance for eyeglasses or
contact lenses every year
H4279 004:• $0 copay for:• Routine eye exam every year• $100 allowance for eyeglasses or
contact lenses every year
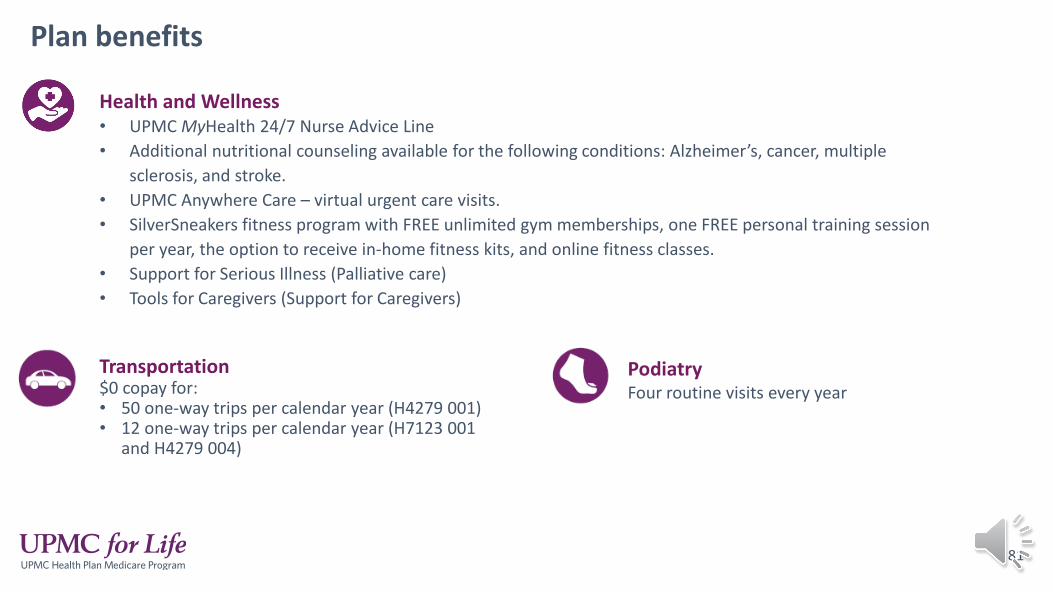
Plan benefits
81
Health and Wellness• UPMC MyHealth 24/7 Nurse Advice Line• Additional nutritional counseling available for the following conditions: Alzheimer’s, cancer, multiple
sclerosis, and stroke.• UPMC Anywhere Care – virtual urgent care visits.• SilverSneakers fitness program with FREE unlimited gym memberships, one FREE personal training session
per year, the option to receive in-home fitness kits, and online fitness classes.• Support for Serious Illness (Palliative care)• Tools for Caregivers (Support for Caregivers)
Transportation$0 copay for:• 50 one-way trips per calendar year (H4279 001)• 12 one-way trips per calendar year (H7123 001
and H4279 004)
PodiatryFour routine visits every year
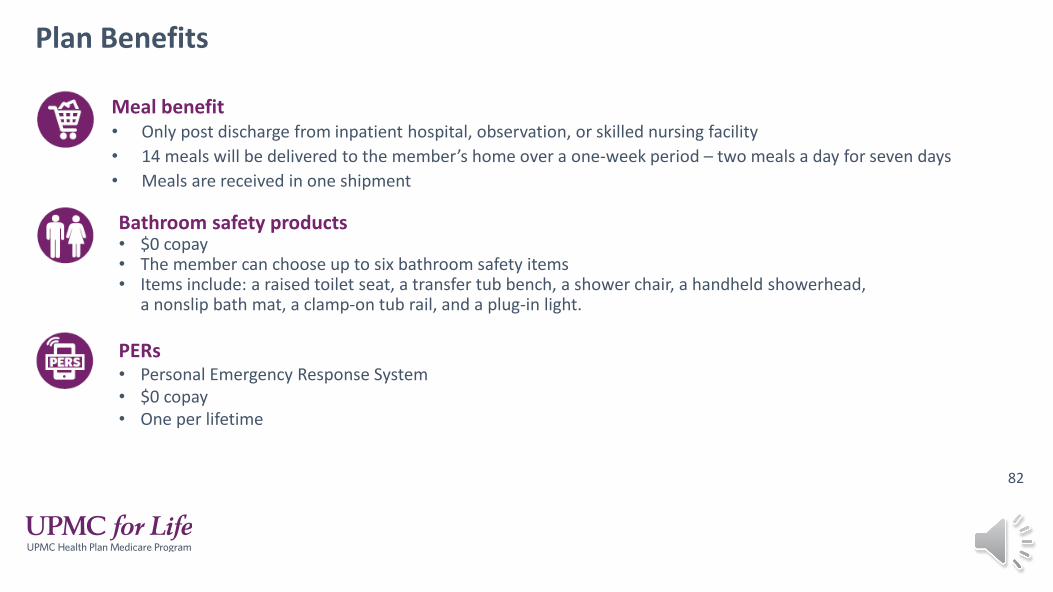
Plan Benefits
82
Meal benefit• Only post discharge from inpatient hospital, observation, or skilled nursing facility• 14 meals will be delivered to the member’s home over a one-week period – two meals a day for seven days• Meals are received in one shipment
Bathroom safety products• $0 copay• The member can choose up to six bathroom safety items• Items include: a raised toilet seat, a transfer tub bench, a shower chair, a handheld showerhead,
a nonslip bath mat, a clamp-on tub rail, and a plug-in light.
PERs• Personal Emergency Response System• $0 copay• One per lifetime

Plan Benefits
83
Healthy food allowance (only for H4279 001)• Special Supplement Benefit for the Chronically Ill (SSBCI)
• For members who have diabetes
• $50 per quarter for healthy foods
• Balance will roll over
OTC – Over-the-counter allowance• The SNP over-the-counter allowance can be used with the retail card and through mail order
catalog for H4279 001 plan.$125 can be used at participating retail stores with the retail card$225 can be used through our mail order catalog
• For H4279 004 and H7123 001 the over the counter allowance can only be used through the mail order catalog ($225 per quarter).
• For all SNP allowances, they will roll over each quarter but must be used in full by the end of the calendar year
Additional Plan Benefits Benefits focused on the whole person, including social determinants of health
Fitness Remote Technologies Post-discharge meals
Falls Prevention Transportation to appointments
Home Safety/PERS

Additional Information
Copyright 2020 UPMC Health Plan Inc. All rights reserved.<2021_PPTTEMP_20MC-SNP1337924 (AG) 5/13/20>

Maximum out-of-pocket costs for Medical Services (MOOP)
The out-of-pocket maximum is the maximum amount that a member would pay out of their pocket during the calendar year for covered Part A (hospital insurance) and Part B (medical insurance) services. Part D copays are not applied to this out of pocket.
Members will remain responsible for any Medical Assistance copays.
Maximum Out-of-Pocket
86
• 2021 MOOP: UPMC for Life Complete Care members have a $3,400 maximum out-of-pocket amount for covered Part A and Part B services.
• This applies only when the member falls into the grace period (lost Medical Assistance)
• Medical Assistance picks up the balances after the Medicare payment for dual eligible members and the out-of-pocket is not applicable.
Grace Period• UPMC for Life Complete Care members will be provided with a 180-day grace period, when they lose their Medical Assistance
coverage.
• During the grace period, UPMC for Life Complete Care members are encouraged to contact their County Assistance Office to regain full Medical Assistance.
• UPMC for Life Complete Care members who are unable to regain full Medical Assistance coverage will be disenrolled after the grace period ends.
• Once the member is disenrolled, they will return to Original Medicare unless they enroll in another Medicare Advantage plan.
While in the grace period:
• Members will not be responsible for copayments or coinsurance for covered services, except for Part D prescription drug copayments.
• Members will remain responsible for the Part B premium at all times, unless this amount is paid on their behalf.
• If a member receives a balance bill from a provider, they are encouraged to call Member Services, as members are not responsible for balance bills.
• UPMC for Life Complete Care providers are not allowed to balance bill our members.

Pharmacy coverageUPMC for Life Complete Care has a 5-tier drug list:
Tier 1 – Preferred Generic DrugsTier 2 – Generic DrugsTier 3 – Preferred Brand DrugsTier 4 – Non-Preferred DrugsTier 5 – Specialty Drugs
• Part D Rx’s are dispensed as a 30-day supply (except for long-term care facility residents).
• Temporary transition supply is dispensed in a 30-day supply for non-formulary drugs.
• For long-term care facility residents, the transition drug supply remains at 31-days
• There will now be Preferred and Standard Pharmacy locations. The cost share will remain the same for the members because they will continue to pay their LIS copays.
Click here and fill out the drop downs to view the UPMC for Life Complete Care Comprehensive Formulary online
Click here to find member plan documents like Summary of Benefits, Evidence of Coverage, Provider Directory, and Annual Notice of Change online.
Find plan documents online
Choose the plan type, state, and county from the below drop downs:
Choose the plan document you’d like to review by clicking on Plan Benefits Materials, Prescription Drug Coverage, or Provider Directory:

Low Income Subsidy (LIS)Low Income Subsidy
• Medicare beneficiaries with limited income and resources may qualify for extra help to pay for prescription drugs costs. This low-income subsidy (LIS) assistance will help pay for monthly premiums, yearly deductibles, and copayments.
• Full benefit dual eligibles, such as those in the UPMC for Life Complete Care, are automatically eligible for the low-income subsidy.
• Low Income Subsidy Rider – Needs to be in member’s hands by September 30th.
To find LIS information online, click here. Click on Prescription Drug Coverage then choose, Help for Prescription Drug Costs (LIPST).

Have questions?
Copyright 2020 UPMC Health Plan Inc. All rights reserved.<2021_PPTTEMP_20MC-SNP1337924 (AG) 5/13/20>
If you have any questions please email [email protected]!


















