2021 Medication Safety Study
14
Baptist Health Medication Study Guide Learning and Development, June 2020 Page 1 of 14 2021 Medication Safety Study BH Policy # 7.01.03: Medication Administration
Transcript of 2021 Medication Safety Study

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 1 of 14
2021 Medication Safety Study
BH Policy # 7.01.03: Medication
Administration

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 2 of 14
TABLE OF CONTENTS
Converting Pounds to Kilograms………………………………..………………….………………… 3
Legal Responsibilities for Medication Administration………………………………….………………… 3
Independent Nurse Double Check ……………………………………………………………………….. 4
Verbal Orders ………………………………………………………………………………………….. 4
Barcode Medication Administration………………………………….………………………………… 4 Medications Linked to Fall Risk…………………………………………………………………………… 4
Do Not Use Abbreviations……………………………………………………………............................... 5
Alaris Pumps…………………………………………………………….............................................. 5
Prevention of Medication Errors……………………………………………………………..….................. 6
Wasting/Discarding Medications……………………………………………………………………… 6
Parenteral Administration of Medication for Adults……………………………………………………… 7
Procedural Techniques for Pediatrics…………………………………..………………..…………….. 7
Calculating Dosage for Non-Parenteral Medications………………………………………………..…….. 9
Practice Medication Calculation Problems……………………………………………………………….. 10
Answers to Practice Medication Calculation Problems………………………………………………….. 12

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 3 of 14
The purpose of this study guide is to help you prepare for the medication test and to assist you in
strengthening your medication calculation skills. This test also includes questions that relate to basic nursing
practice and critical thinking.
The medication test will be given during your first week of orientation and you cannot give medications
until successful completion of the test. An overall passing score of 90% or above is required.
Converting pounds to kilograms? There are 2.2 pounds for each kilogram when you are converting. For
example, 16 pounds = 7.27kg; 220 pounds = 100kg
LEGAL RESPONSIBILITIES FOR MEDICATION ADMINISTRATION
Nurses and are legally accountable for the patient's safety when administering medications. The
following eight rights serve as the standard for this accountability.
1. Right Patient:
a. Patient Identifiers When administering medication or performing a procedure on an alert,
conscious patient you must use the following patient identifiers: Ask the patient to state
their first and last name and their date of birth every time while scanning the armband
to compare with the Medication Administration Record (MAR).
b. If the patient is unable to respond, you must verify the arm band with the eMAR.
2. Right Medication
3. Right Dose
4. Right Route: a. Always verify.
b. Remember to also verify if a medication can be crushed prior to administration through an NG, OG,
or Gastric tube.
c. Sustained release tablets should never be crushed.
5. Right Time:
a. Timing can be an important factor for certain drugs in order to maintain a therapeutic level.
b. There is generally a 60 minute grace period before or after a drug is scheduled in order to be in
compliance with prescribed therapy.
c. Drugs given before or after this period should be recorded as a variance.
d. “Time Critical” medications such as time-released medications, those requiring blood level
monitoring, anticonvulsants, insulin, etc. must be given within 30 minutes before or after the
scheduled dose time.
6. Right Documentation: a. For adult patients, use a 0 – 10 Pain scale based on the patient’s perception of pain for adults
b. For pediatric patients, please ensure you are using the correct pain scale according to their age
and developmental stage.
c. Make sure to return and reassess your patient’s level of pain 30 – 60 minutes after administering
oral pain medication and (15 – 30 minutes for IV/IM meds) using the same pain scale prior to
the medication administration.
d. Document the pain scale values and score (pre and post intervention), and be as specific as
possible.
7. Right circumstance:
a. For example, if NPO, hold oral anti-glycemics.
b. You still may give covering insulin, but call the physician, if not sure.
8. Patient’s Right to refuse

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 4 of 14
Independent nurse double check
To be most effective, the double check must be conducted independently by a second licensed nurse. If
the double check is conducted independently, it reduces the risk of confirmation bias that may occur if the
same person prepares and checks a medication, as they likely will see only what they expect to see, even
if an error has occurred.
Barcode Medication Administration (BCMA)
Patient Safety: Barcode assisted medication administration reduces errors by as much as 54 – 80%
Most medications are barcoded and you are required to scan the medication and the patient armband at
the bedside before administration.
• Exceptions: Code Blue, Rapid Response, Intra-operatively, outpatient areas, downtime, free
water.
eMAR is the source of truth for all medications administered
ONLY the armband can be scanned as Positive Patient ID. If the armband does not scan, place an
armband reprint order in the EMR and PAS will print it on the unit within 5 minutes.
Scan each medication BEFORE adminsitering to check for alerts!!
Verbal Orders
Verbal Order-Read back/verified – When a provider verbally communicates an order to a nurse, nurses may
enter order only be used in emergency situations or when the provider cannot directly enter into the EMR i.e.
scrubbed for surgery or a procedure or is actively involved in urgent/emergent patient care.
Medications Linked to Patient Fall Risk
Class Examples of Medications in Class
Anticonvulsants
Carbamazepine, Divalproex Sodium, Ethotoin, Ethosuximide, Felbamate,
Fosphenytoin, Gabapentin, Lamotrigine, Lacosamide, Mephenytoin,
Methsuximide, Phenobarbitol, Phenytoin, Pregabalin, Primidone,
Topiramate, Trimethadione, Valproic Acid
Antihistamines Chlorpheniramine, Cyproheptadine, Diphenhydramine, Hydroxyzine,
Promethazine
Antipsychotics
Chlorpromazine, Clozapine, Droperidol, Fluphenazine, Haloperidol,
Loxapine, Olanzapine, Perphenazine, Quetiapine, Risperidone,
Thioridazine, Thiothixene, Trifluoperazine, Ziprasidone
Anxiolytics / Sleep Aids Buspirone, Chloral Hydrate, Zolpidem
Barbiturates Butabarbital, Methohexital,
Benzodiazepines
Alprazolam, Chlordiazepoxide, Clonazepam, Clorazepate Dipotassium,
Diazepam, Flurazepam, Halazepam, Lorazepam, Midazolam, Oxazepam,
Temazepam, Triazolam
Narcotic Analgesic Codeine, Fentanyl, Hydromorphone, Meperidine, Morphine, Nalbuphine,
Oxycodone, Pentazocine
Antihypertensive Agents:
ACE Inhibitors Captopril, enalapril, benazepril, lisinopril, trandolapril (Prils)
Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 5 of 14
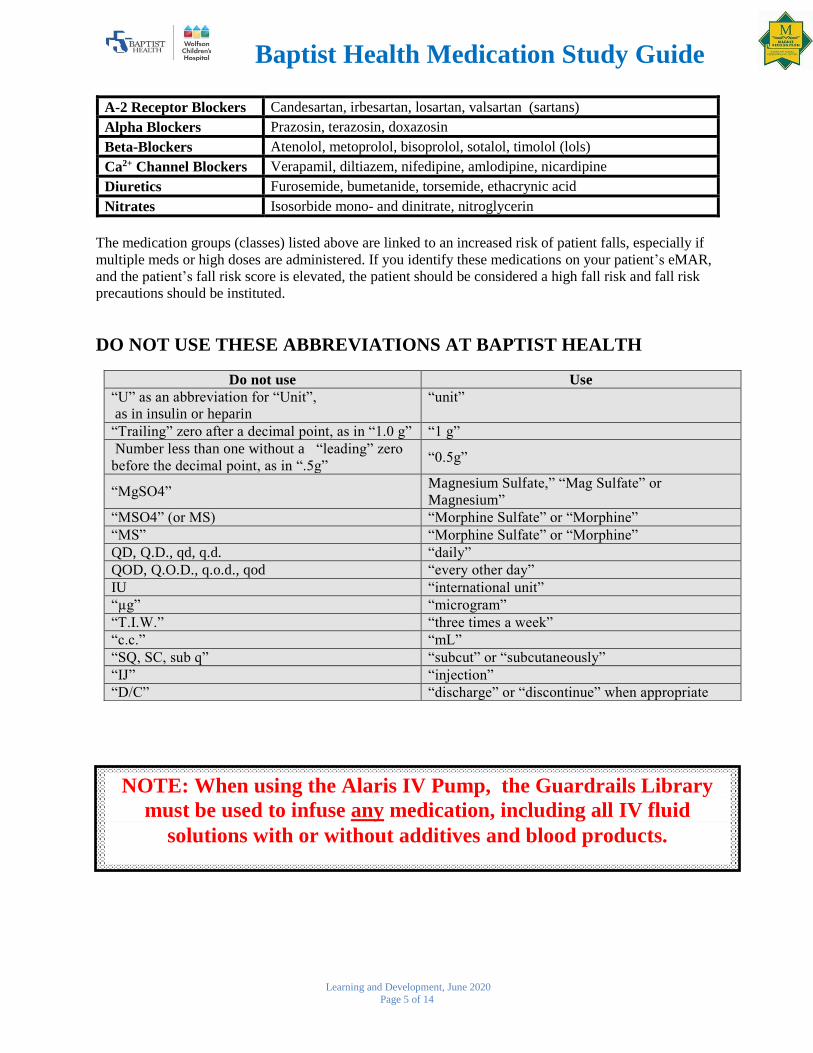
NOTE: When using the Alaris IV Pump, the Guardrails Library
must be used to infuse any medication, including all IV fluid
solutions with or without additives and blood products.
A-2 Receptor Blockers Candesartan, irbesartan, losartan, valsartan (sartans)
Alpha Blockers Prazosin, terazosin, doxazosin
Beta-Blockers Atenolol, metoprolol, bisoprolol, sotalol, timolol (lols)
Ca2+ Channel Blockers Verapamil, diltiazem, nifedipine, amlodipine, nicardipine
Diuretics Furosemide, bumetanide, torsemide, ethacrynic acid
Nitrates Isosorbide mono- and dinitrate, nitroglycerin
The medication groups (classes) listed above are linked to an increased risk of patient falls, especially if
multiple meds or high doses are administered. If you identify these medications on your patient’s eMAR,
and the patient’s fall risk score is elevated, the patient should be considered a high fall risk and fall risk
precautions should be instituted.
DO NOT USE THESE ABBREVIATIONS AT BAPTIST HEALTH
Do not use Use
“U” as an abbreviation for “Unit”,
as in insulin or heparin
“unit”
“Trailing” zero after a decimal point, as in “1.0 g” “1 g”
Number less than one without a “leading” zero
before the decimal point, as in “.5g” “0.5g”
“MgSO4” Magnesium Sulfate,” “Mag Sulfate” or
Magnesium”
“MSO4” (or MS) “Morphine Sulfate” or “Morphine”
“MS” “Morphine Sulfate” or “Morphine”
QD, Q.D., qd, q.d. “daily”
QOD, Q.O.D., q.o.d., qod “every other day”
IU “international unit”
“µg” “microgram”
“T.I.W.” “three times a week”
“c.c.” “mL”
“SQ, SC, sub q” “subcut” or “subcutaneously”
“IJ” “injection”
“D/C” “discharge” or “discontinue” when appropriate

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 6 of 14
Alaris Smart Pumps
All primary and secondary infusions should always be programmed using Guardrails which has prevented
significant medication errors. If you have difficulty locating a medication in the pump library (or have any
other pump issues), contact your pharmacist so that the issue may be corrected with future enhancements.
PREVENTION OF MEDICATION ERRORS
Why writing it out is important:
An error occurred in a Midwestern hospital when a nurse who was taking a
patient’s history recorded his insulin dose using the letter “u” instead of the word “unit”. The physician
misread the “u” as a “4” (fig. 1) and wrote orders for doses dramatically different from what the patient
had been taking. The patient received a single overdose of insulin, but fortunately was not harmed. The
only way to safely express units is to write it out. Another safe practice is to tell the patient what the
medication and dose is. Further overdoses were averted when the nurse said to the patient, “Here’s your
insulin, 44 units.” The patient replied, “44 units? I take 4 units!” Source: ISMP Medication Safety Alert
Wasting/Discarding of Controlled Substances
1. Any medications in packages that are not intact should be wasted and not returned.
2. Controlled medications require two licensed practitioners (one an RN) to witness and document the
wasting.
3. Controlled medications from the Acudose should have the waste documented in the Acudose at the
time of wasting.
4. Wastage from epidurals, PCAs, and narcotic infusions not obtained from the Acudose shall be
documented on the eMAR/MAR or epidural/PCA flowsheet or on the unit’s Controlled Substance
Record.
5. After withdrawing the correct IV dose and prior to administering, the remaining medication will be
discarded down the narcotic waste sink (cactus), when available, or sink, when not available.
6. Emptied ampules and PCAs shall be discarded in the sharps container. Empty IVs, vials, and syringes
without needles or blood can be placed in the regular trash. Emptied epidural and narcotic infusion
bags shall be discarded in the trash receptacle. (Sharps should always be discarded in the sharps
container).
7. Contents of an opened or unused oral syringe containing a controlled substance should be discarded in
the cactus sink, when available, or sink, when not available.
8. A narcotic patch should be folded upon itself and placed in the cactus for disposal. Units without a
cactus sink must flush down the toilet.
Verbal Orders Problem: An order for Fentanyl was heard as “5,200 mcg per hour” and read
back to the prescriber for verification. A pharmacist called the physician and learned that he
had prescribed Fentanyl “50 to 100 mcg per hour”. When reading back verbal orders, express
doses in single digits such as “5-2-0-0” to avoid confusion.
Remember: use of range orders is prohibited and use of the Alaris Guardrails would “catch”
this error and protect the patient from overdose.

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 7 of 14
9. Tablets and capsules should be placed in the cactus. Units without a cactus sink must flush down the
toilet.
10. Unused chemotherapy should be returned to pharmacy for destruction.
Parenteral Administration of Medications
Procedural Techniques for Adults
1. Intramuscular
a. Select needle (18 – 22gauge of suitable length)
b. Medication volume: 1 – 3 mL
c. Insert the needle into site at a 90° angle
2. Z Track (to prevent irritation and leakage) Example of medications: Iron Dextran
a. Do not inject into the arm.
b. Retract skin and subcutaneous tissue laterally to the side of needle entry point before injecting.
Doing this allows the muscle to return to its original position following the injection and avoids
leakage of the medication from the site.
c. Insert 2” (18 – 22gauge) needle with a dart-like motion into the skin at a 90° angle. A long needle
is needed for deep entry into the muscle.
d. Wait 10 seconds after injection before withdrawing needle.
e. DO NOT MASSAGE THE SITE. Massaging may force the medication out into the surrounding
tissue.
3. Subcutaneous
a. Insert needle at a 45° or 90° angle into the fold.
b. Do not withdraw on the plunger when administering subcutaneous anti-thrombotics.
c. Inject medication slowly.
d. Withdraw needle and massage site gently with a swab. EXCEPTION: You may apply gentle
pressure but DO NOT MASSAGE when giving insulin or heparin.
e. Medication volume: No more than 2mL
Procedural Techniques for Pediatrics
1. Intravenous (WCH Policy #5021: Peripheral IV Insertion)
a. Preferred sites for insertions are hands, forearms, and feet with goal of restricting extremity
movement as little as possible. Insertion attempt should begin distally, move proximally and avoid
vein junctions when possible.
b. Utilize PANDA Protocol to promote safe, effective, and practical methods to reduce fear, anxiety
and pain.
i. Prepare patient and family
ii. Analgesia (J-Tips are for >6months of age and “sweet ease” is good for <1year of age)
iii. New technology such as vein viewer or ultrasound
iv. Distract: utilize extra help if needed to maintain patient safety and provide distraction
(example: Child-life)
v. Allow comfort items and/or comfort hold techniques
2. Peripheral IV attempts
a. An individual staff nurse should not attempt venipuncture more than twice on any patient.
Do not aspirate for immunizations or
vaccines

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 8 of 14
b. After 4 unsuccessful attempts, request additional attempts by another highly skilled caregiver i.e.
Pediatric Vascular Access Team or Transport Nurse, if available.
c. If still unsuccessful, the physician should be notified to consider alternative interventions.
3. Intramuscular
a. Select needle (21 – 22g for thick medication and 23 – 25g for thin medications)
b. Guidelines for maximum injected medication volume per site
weight 3 – 5kg 6 –
11kg 12 – 18kg 19 – 36kg 37 – 50kg
51 – 60kg
61 – 130kg
volume 0.5 – 1mL
1mL 1 – 1.5mL 1.5 – 2mL
2mL 2-3mL 3mL
c. Vastus lateralis is the site of choice for IM injections
4. Subcutaneous
a. Same as adult.
Please visit the Baptist intranet for further information on medication resources, including:
Look-A-Like Sound – A-Like-Medications
High Alert Medication List
Hotsheet for Insulin Calculation
http://intranet.e-baptisthealth.com/clinicalcare/Pages/default.aspx
The child’s muscle mass and development dictates the maximum volume to be injected
per site, site selection, and needle size

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 9 of 14
SUGGESTED FORMULA FOR CALCULATION (METHOD TWO)
This method allows you to set up a ratio of what you have to what you need.
Example: Using the same example as in Method one, the physician orders Keflex 750 mg.
and you have Keflex 250 mg per tablet.
Dose on hand : 1 :: Dose desired : X
250mg : 1 tab : 750mg : X tabs multiply the
means together and the extremes together.
250 X= 750
X = 750
250 X = 3
SUGGESTED FORMULA FOR CALCULATION (METHOD ONE)
Dose ordered x tablet, capsule, etc. = amount to give
Drug strength on hand
Desired x volume = Amount to give
have
Example: The physician orders Keflex 750 mg.
On hand: Keflex 250 mg per capsule.
Using the formula above:
Drug ordered = 750mg x1 capsule = dose to give
Dose on hand = 250mg
750 x 1 = 3 capsules of 250mg each.
250
Check your answer by the alternative method of reasoning:
250mg x 3 = 750mg
Appendix A
Calculating Dosage for Non-Parenteral Medications
Calculating dosages for non-parenteral medications such as pills, capsules, unscored tablets, or
suppositories should be rounded to the nearest whole number.
Calculated dosage for scored tablets should be rounded to the nearest half or quarter depending on how
the tablet is scored.
With problems involving oral liquid medications, it is generally accurate enough to round one decimal
place.

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 10 of 14
PRACTICE PROBLEMS
INSTRUCTIONS: The questions on this practice test are similar to the medication test. Read the
questions carefully.
1. Diphenhydramine hydrochloride (Benadryl) elixir 25mg is ordered for a patient. It is supplied as
12.5mg/5mL. How many milliliters should you administer?
a. 10mL
b. 5mL
c. 2.5mL
2. Digoxin is ordered 0.25mg p.o .daily A 0.125mg tablet is available in unit stock for administration.
The correct amount to give is:
a. 1 tablet
b. ½ tablet
c. 2 tablets
3. Your patient has a positive blood culture and the physician ordered Gentamycin 35mg IV every 8
hours. How many mL of Gentamycin would you draw up if given 80mg/2mL?
a. 0.9mL
b. 1.5mL
c. 2.9mL
4. Your patient is to receive 8,000 units heparin subcutaneously. The drug is supplied in a vial
containing 5,000 units/mL. How many mL should be administered?
a. 1.6mL
b. 0.63mL
c. 4 mL
5. A patient is receiving heparin via an infusion pump. The bag is labeled as containing 25,000 units of
heparin in 500mL of D5W. The infusion pump is set to deliver 25mL/hr. How many units of heparin
per hour is the patient receiving?
a. 625 units/hour
b. 125 units/hour
c. 1250 units/hour
6. Your patient is to receive regular insulin at 3 units/hr. You mix regular insulin 100 units in 100mL of
normal saline. At how many mL/hr would you set the infusion pump to deliver the ordered dose?
a. 3mL/hr
b. 17mL/hr
c. 0.6mL/hr
7. Versed is ordered 2mg IV once. Versed 5mg/mL is available in unit stock for administration. The
correct amount in mL to give is:
a. 0.1mL
b. 0.4mL
c. 10mL

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 11 of 14
8. Your patient has an order for Tylenol 250mg by mouth. Tylenol standard concentration is
160mg/5mL. How many mL would you administer to the patient?
a. 3.2mL
b. 7.8mL
c. 9.2mL
9. Sam is a 3 year old who weighs 19kg and admitted to your floor for osteomyelitis. Which of the
following is a safe/ therapeutic first dose of Gentamicin to give Sam? (Gentamicin 6 – 7.5mg/kg/24hr
dosing q8hr IV)
a. 140mg
b. 70mg
c. 40mg

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 12 of 14
ANSWERS TO PRACTICE PROBLEMS
1. Diphenhydramine hydrochloride (Benadryl) elixir 25mg is ordered for a patient. It is supplied as
12.5mg/5mL. How many milliliters should you administer?
a. 10 mL
b. 5 mL
c. 2.5 mL
12.5x = 125mL x = 10mL
2. Digoxin is ordered 0.25mg p.o .daily. A 0.125mg tablet is available in unit stock for administration. The
correct amount to give is:
a. 1 tablet
b. ½ tablet
c. 2 tablets
0.125x = 0.25 tab x = 2 tabs
3. Your patient has positive blood culture and the physician ordered Gentamycin 35mg IV every 8 hours.
How many mL of Gentamycin would you draw up if given 80mg/2mL?
a. 0.9 mL
b. 1.5 mL
c. 2.9 mL 80 mg : 2 mL = 35 mg : x 80x = 70mL x = 70 mL x =0.875 ml or
0.9 mL
80
4. Your patient is to receive 8,000 units heparin subcutaneously. The drug is supplied in a vial containing
5,000 units/mL. How many mL should be administered?
a. 1.6 mL
b. 0.63 mL
c. 4 mL
5000 units : 1mL = 8000 units : x mL (multiply extremes by means)
5000 x = 8000 (1)
x = 5000
8000 x = 1.6 mL
OR
Desired dose = _x_ (cross multiply) 5000x = 8000 x = 8000 = 1.6 mL
Available dose 1 mL 5000
25 mg
12.5 mg
x .
5 mL =
0.25 mg
0.125 mg
x .
1 tab =

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 13 of 14
5. A patient is receiving heparin via an infusion pump. The bag is labeled as containing 25,000 units of
heparin in 500mL of D5W. The infusion pump is set to deliver 25mL/hr. How many units of heparin per
hour is the patient receiving?
a. 625 units per hour
b. 125 units per hour
c. 1250 units per hour
25,000 units = 50 units/mL 50 units/mL X 25 mL/hr = 1250 units/hr
500 mL
25,000 units : 500 mL = X units : 25 mL
(multiply extremes by the means, etc.)
6. Your patient is to receive regular insulin at 3 units/hr. You mix regular insulin 100 units in 100mL of
normal saline. At how many mL/hr would you set the infusion pump to deliver the ordered dose?
a. 3mL/hr
b. 17mL/hr
c. 0.6mL/hr
Desired = X
Available Total solution
3 units = X 100 X = 100 x 3 100 X = 300 X = 300 = 3mL
100 units 100 mL 100
7. Versed is ordered 2mg IV once. Versed 5mg/1mL is available in unit stock for administration. The
correct amount in mL to give is:
a. 0.1mL
b. 0.4mL
c. 10mL
5x = 2mg x = 0.4mL
5 mg 1mL
2mg x
=

Baptist Health Medication Study Guide
Learning and Development, June 2020
Page 14 of 14
8. Your patient has an order for Tylenol 250mg by mouth. Tylenol standard concentration is 160mg/5mL.
How many mL would you administer to the patient.
a. 3.2mL
b. 7.8mL
c. 9.2mL
250mg=160mg 1250= 160x x=7.8mL
X 5mL
9. Sam is a 3 year old who weighs 19kg and admitted to your floor for osteomyelitis. Which of the
following is a safe/ therapeutic first dose of Gentamicin to give Sam? (Gentamicin 6 – 7.5mg/kg/24hr
dosing q8hr IV)
a. 140mg
b. 70mg
c. 40mg
Low 19×6=114÷3=38mg/ 8hrs High 19×7.5=143÷3=48mg/ 8hrs