2020 Meningococcal 101 - FINAL
14
4/30/2020 1 Meningococcal 101 Heidi Gurov, RN BSN CMSRN ONC Clinical Consultant & Quality Improvement Specialist Wyoming Department of Health Immunization Unit Wyoming Virtual Immunization Conference May 13, 2020 1 Overview • All about the disease • Causative organism • Serogroups • Transmission • Pathogenesis • Risk factors • Disease presentation • Vaccination • MenACWY • Men B • ACIP recommendations • Travel recommendations • Best practices 2 Meningococcal Disease 3
Transcript of 2020 Meningococcal 101 - FINAL
4/30/2020
1
Meningococcal101Heidi Gurov, RN BSN CMSRN ONC
Clinical Consultant & Quality Improvement SpecialistWyoming Department of Health Immunization Unit
Wyoming Virtual Immunization ConferenceMay 13, 2020
1
Overview
• All about the disease• Causative organism• Serogroups• Transmission• Pathogenesis• Risk factors• Disease presentation
• Vaccination• MenACWY• Men B• ACIP recommendations• Travel recommendations• Best practices
2
MeningococcalDisease
3
4/30/2020
2
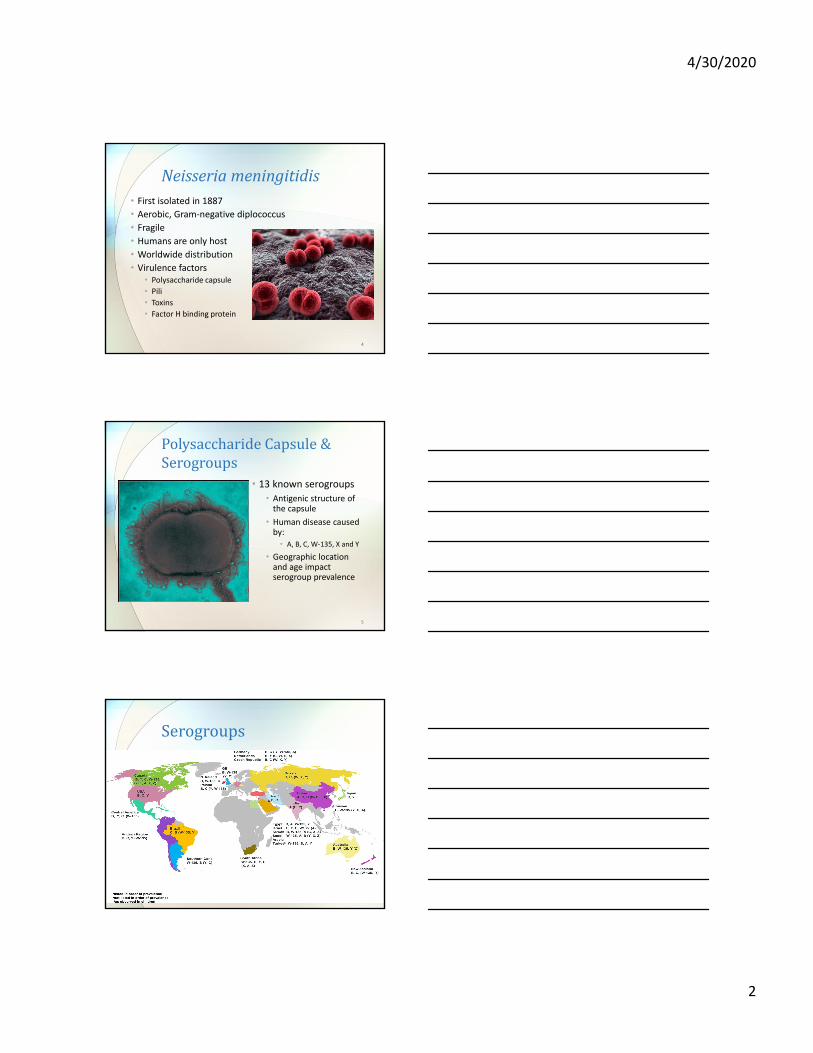
Neisseriameningitidis• First isolated in 1887• Aerobic, Gram‐negative diplococcus
• Fragile• Humans are only host
• Worldwide distribution
• Virulence factors• Polysaccharide capsule• Pili• Toxins• Factor H binding protein
4
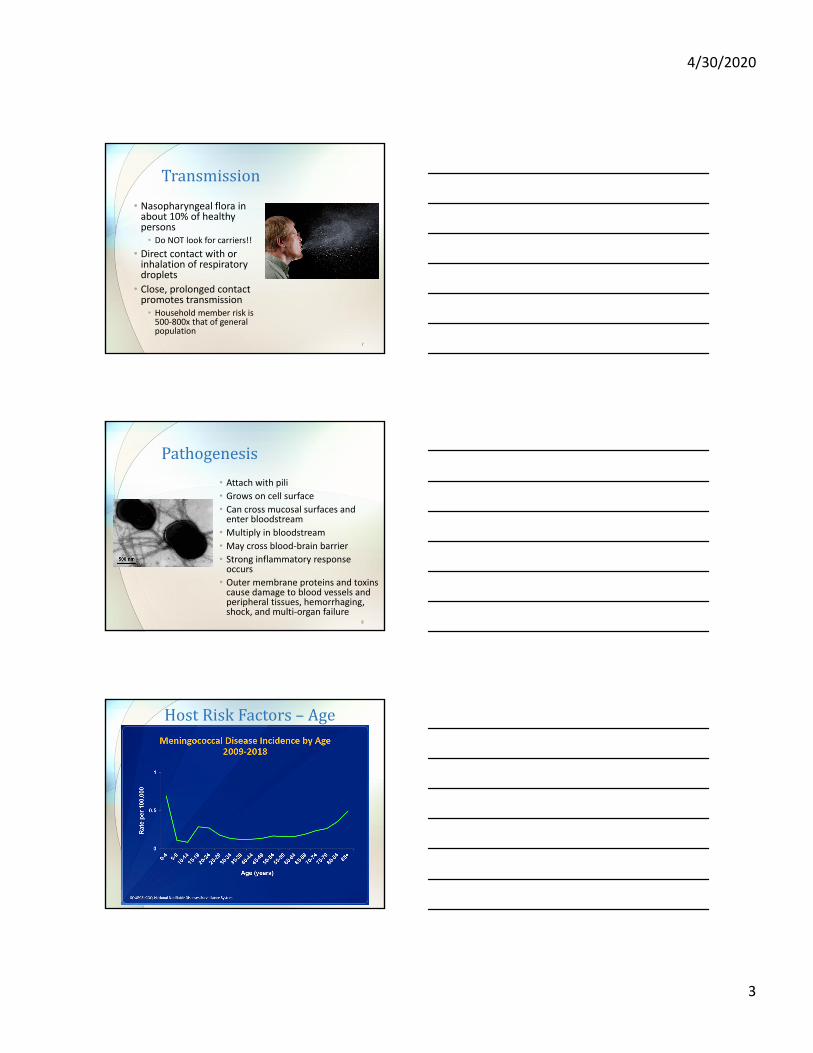
PolysaccharideCapsule&Serogroups
• 13 known serogroups• Antigenic structure of the capsule
• Human disease caused by:• A, B, C, W‐135, X and Y
• Geographic location and age impact serogroup prevalence
5
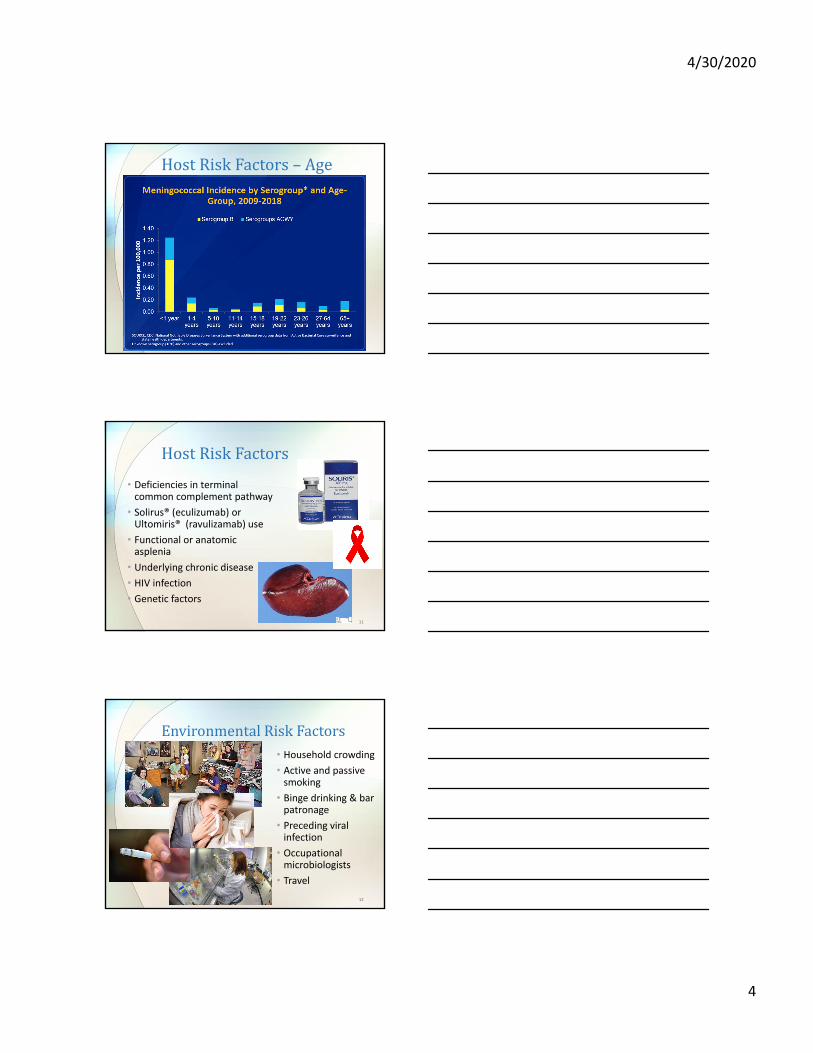
Serogroups
6
4/30/2020
3
Transmission
• Nasopharyngeal flora in about 10% of healthy persons• Do NOT look for carriers!!
• Direct contact with or inhalation of respiratory droplets
• Close, prolonged contact promotes transmission• Household member risk is 500‐800x that of general population
7
Pathogenesis
• Attach with pili• Grows on cell surface• Can cross mucosal surfaces and enter bloodstream
• Multiply in bloodstream
• May cross blood‐brain barrier
• Strong inflammatory response occurs
• Outer membrane proteins and toxins cause damage to blood vessels and peripheral tissues, hemorrhaging, shock, and multi‐organ failure
8
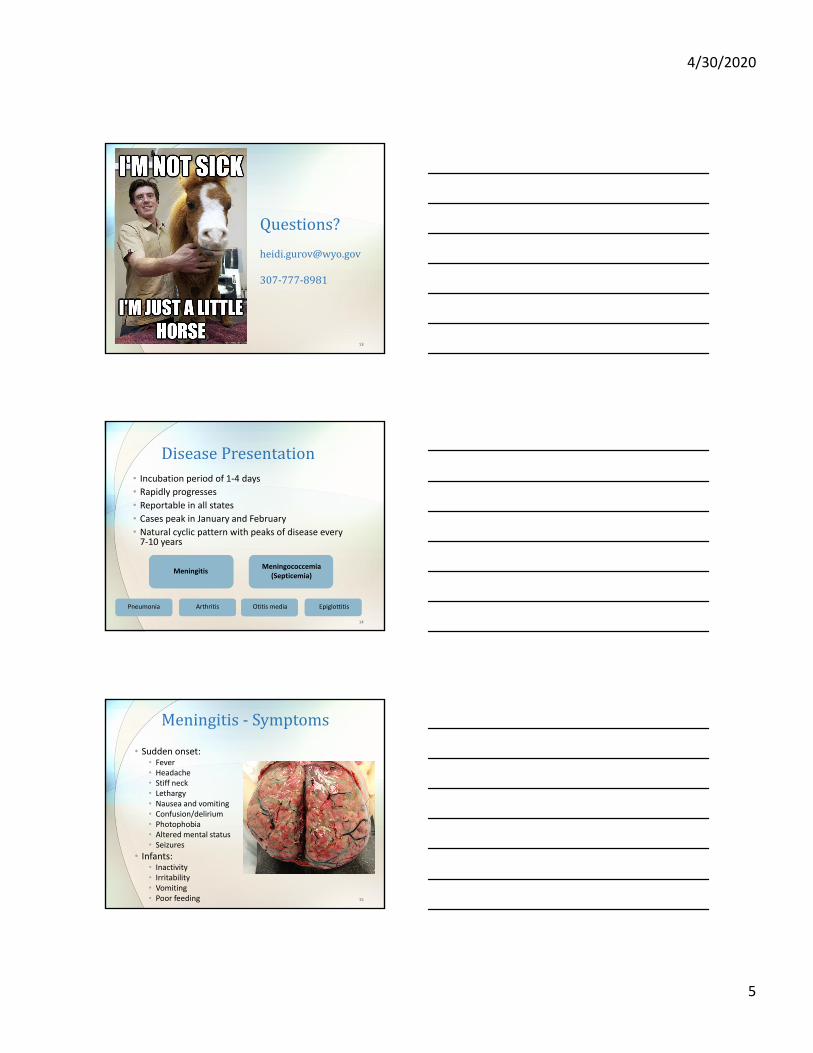
HostRiskFactors– Age
9
4/30/2020
4
HostRiskFactors– Age
10
HostRiskFactors
• Deficiencies in terminal common complement pathway
• Solirus® (eculizumab) or Ultomiris® (ravulizamab) use
• Functional or anatomic asplenia
• Underlying chronic disease
• HIV infection
• Genetic factors
11
EnvironmentalRiskFactors• Household crowding
• Active and passive smoking
• Binge drinking & bar patronage
• Preceding viral infection
• Occupational microbiologists
• Travel
12
4/30/2020
5
Questions?
307‐777‐8981
13
DiseasePresentation• Incubation period of 1‐4 days• Rapidly progresses• Reportable in all states• Cases peak in January and February• Natural cyclic pattern with peaks of disease every 7‐10 years
14
MeningitisMeningococcemia
(Septicemia)
Pneumonia Arthritis Otitis media Epiglottitis
Meningitis‐ Symptoms
• Sudden onset:• Fever• Headache• Stiff neck• Lethargy• Nausea and vomiting• Confusion/delirium• Photophobia• Altered mental status• Seizures
• Infants:• Inactivity• Irritability• Vomiting• Poor feeding 15
4/30/2020
6
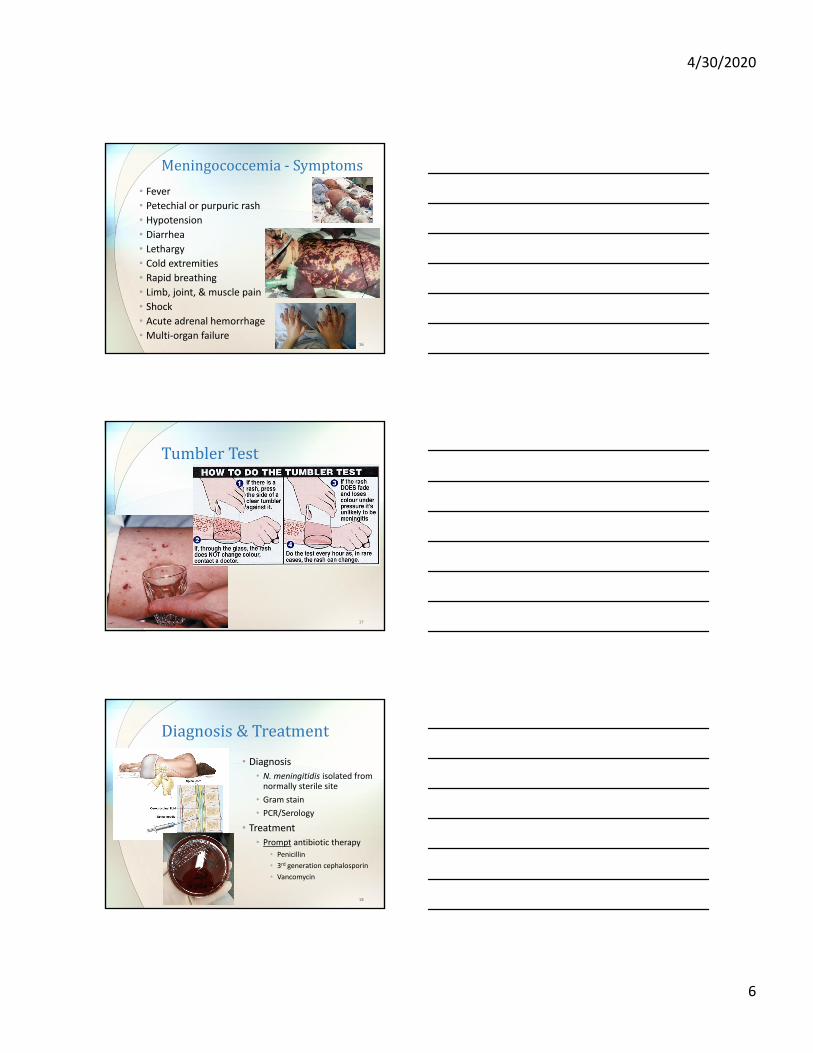
Meningococcemia‐ Symptoms
• Fever• Petechial or purpuric rash• Hypotension• Diarrhea• Lethargy• Cold extremities
• Rapid breathing• Limb, joint, & muscle pain
• Shock• Acute adrenal hemorrhage
• Multi‐organ failure16
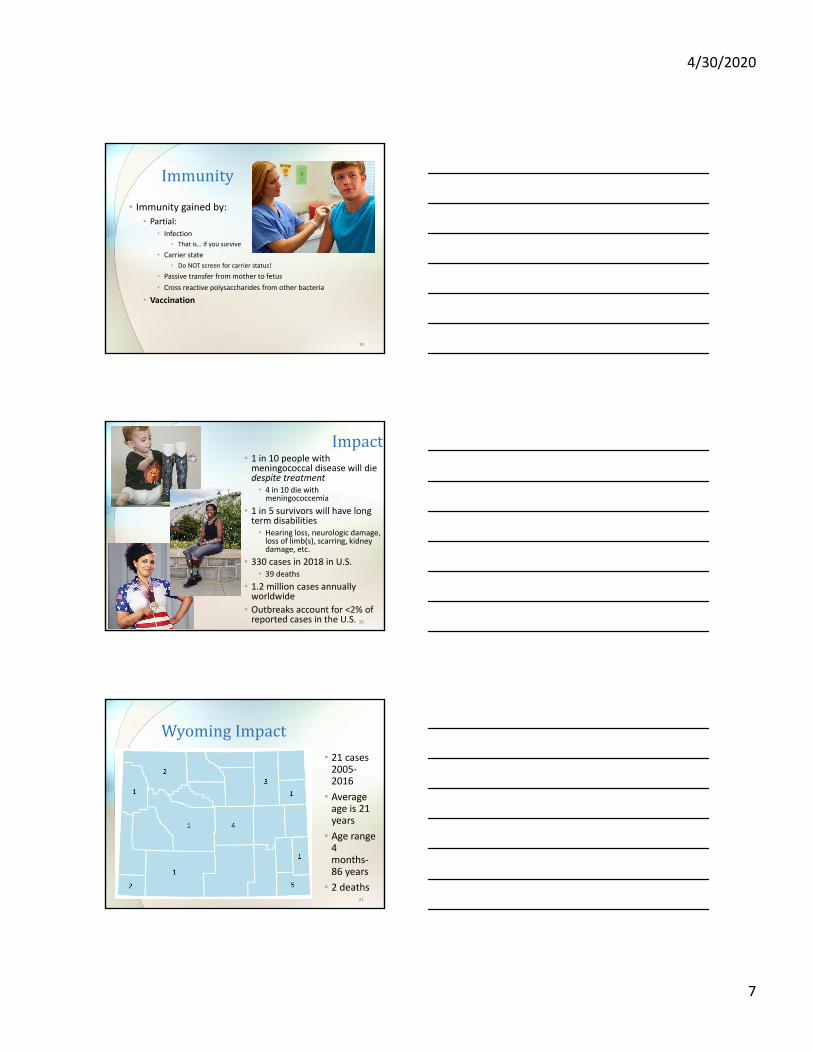
TumblerTest
17
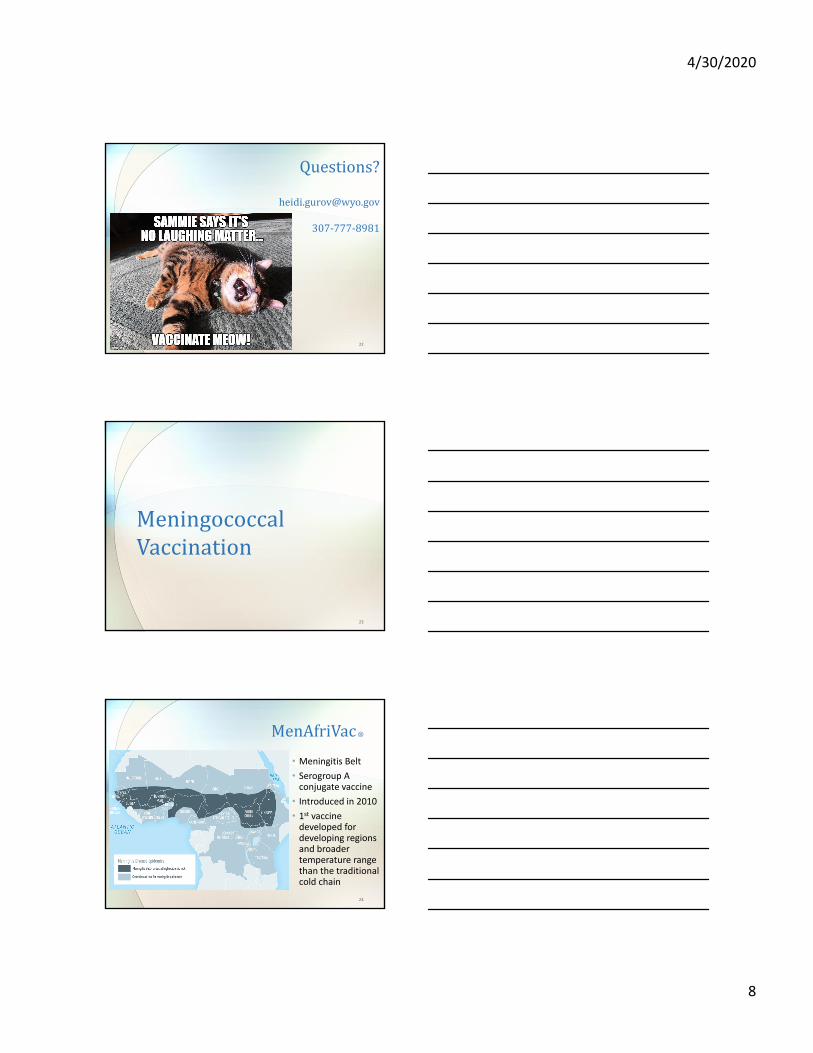
Diagnosis&Treatment
• Diagnosis• N. meningitidis isolated from normally sterile site
• Gram stain
• PCR/Serology
• Treatment
• Prompt antibiotic therapy• Penicillin
• 3rd generation cephalosporin
• Vancomycin
18
4/30/2020
7
Immunity
• Immunity gained by:
• Partial:• Infection
• That is… if you survive
• Carrier state
• Do NOT screen for carrier status!
• Passive transfer from mother to fetus
• Cross reactive polysaccharides from other bacteria
• Vaccination
19
Impact• 1 in 10 people with meningococcal disease will die despite treatment• 4 in 10 die with meningococcemia
• 1 in 5 survivors will have long term disabilities• Hearing loss, neurologic damage, loss of limb(s), scarring, kidney damage, etc.
• 330 cases in 2018 in U.S.• 39 deaths
• 1.2 million cases annually worldwide
• Outbreaks account for <2% of reported cases in the U.S. 20
WyomingImpact• 21 cases 2005‐2016
• Average age is 21 years
• Age range 4 months‐86 years
• 2 deaths21
4/30/2020
8
Questions?
307‐777‐8981
22
MeningococcalVaccination
23
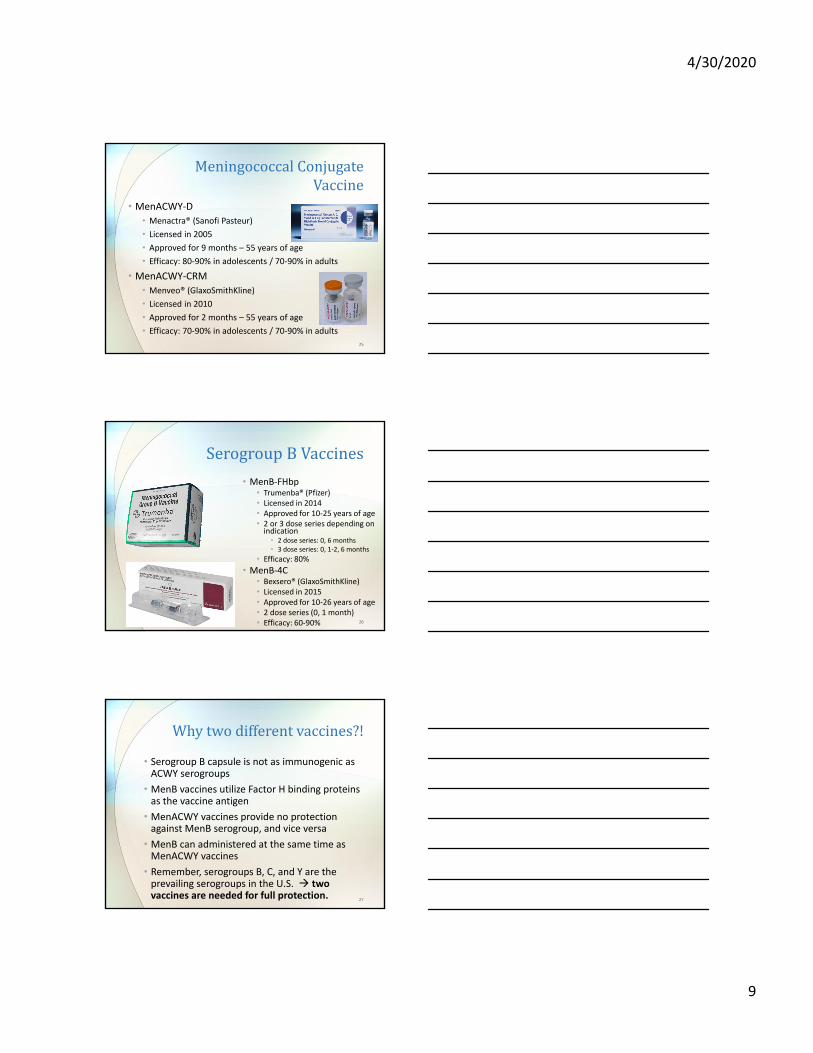
MenAfriVac®
• Meningitis Belt
• Serogroup A conjugate vaccine
• Introduced in 2010
• 1st vaccine developed for developing regions and broader temperature range than the traditional cold chain
24
4/30/2020
9
MeningococcalConjugateVaccine
• MenACWY‐D
• Menactra® (Sanofi Pasteur)
• Licensed in 2005
• Approved for 9 months – 55 years of age
• Efficacy: 80‐90% in adolescents / 70‐90% in adults
• MenACWY‐CRM
• Menveo® (GlaxoSmithKline)
• Licensed in 2010
• Approved for 2 months – 55 years of age
• Efficacy: 70‐90% in adolescents / 70‐90% in adults25
SerogroupBVaccines
• MenB‐FHbp• Trumenba® (Pfizer)• Licensed in 2014• Approved for 10‐25 years of age• 2 or 3 dose series depending on indication• 2 dose series: 0, 6 months• 3 dose series: 0, 1‐2, 6 months
• Efficacy: 80%• MenB‐4C
• Bexsero® (GlaxoSmithKline)• Licensed in 2015• Approved for 10‐26 years of age• 2 dose series (0, 1 month)• Efficacy: 60‐90% 26
Whytwodifferentvaccines?!
• Serogroup B capsule is not as immunogenic as ACWY serogroups
• MenB vaccines utilize Factor H binding proteins as the vaccine antigen
• MenACWY vaccines provide no protection against MenB serogroup, and vice versa
• MenB can administered at the same time as MenACWY vaccines
• Remember, serogroups B, C, and Y are the prevailing serogroups in the U.S. two vaccines are needed for full protection.
27
4/30/2020
10
ACIPRecommendations
28
FDALicensingvs.ACIPRecommendations
• FDA Licensure• Approval from Food & Drug Administration
• Can take years, even decades to occur
• Safety and effectiveness studied in animals and human trials
• ACIP Recommendation
• Occurs after FDA licensure
• Considers costs and benefits
• Determines which groups of people within the population would benefit from the vaccine, and on what schedule the vaccine should be given• Sometimes this can differ from the FDA license 29
Adolescents• MenACWY (Menactra® /Menveo®)
• All 11‐12 year olds should be vaccinated with one dose
• All 16 year olds should be vaccinated with one booster dose
• MenB (Trumenba® /Bexsero®)
• All 16‐23 year olds may be vaccinated with a complete series • Preferably at 16‐18 years old
30
4/30/2020
11
Infants&Children
• See meningococcal footnote of Child/Adolescent ACIP Schedule• MenACWY recommended for certain children 2 months – 10 years of age• Complement component deficiencies (including eculizamab or ravulizamabuse)
• Asplenia• Sickle cell disease• HIV infection• Travel to or reside in countries of hyperendemic or epidemic disease• Outbreak situation
31
Adults‐MenACWY
• See meningococcal footnote of Adult ACIP Schedule• MenACWY is recommended to certain adults at high risk:• Complement component deficiencies (including eculizamaband ravulizumab use)
• Asplenia• HIV infection• Microbiologist routinely exposed to isolates• Travel to or residing in countries of hyperendemic or epidemic disease
• Outbreak situation• First year college student living in a residence hall• Military recruit
• For those who remain high risk:• Booster every 5 years after primary series
32
Adults–MenB
• See meningococcal footnote of Adult ACIP Schedule
• Recommended:
• Those 18‐23 years old with shared clinical decision making
• Complement component deficiencies (including eculizamab and ravulizamab use)
• Asplenia
• Microbiologists
• Outbreak situation attributed to serogroup B
• For those who remain high risk:
• Booster in 1 year, then every 2‐3 years as needed
• Use same vaccine product 33
4/30/2020
12
Travel
• CDC Travel Website: www.cdc.gov/travel• African Meningitis Belt
• MenACWY if traveling December‐June• Booster every 5 years if still at risk• Serogroup B disease is not seen in this region
• Umrah or Hajj Pilgrimage in Saudi Arabia• ≥2 years old: Required to have documentation of conjugate MenACWY vaccination received no more than 5 years before travel 34
Questions?
307‐777‐8981
35
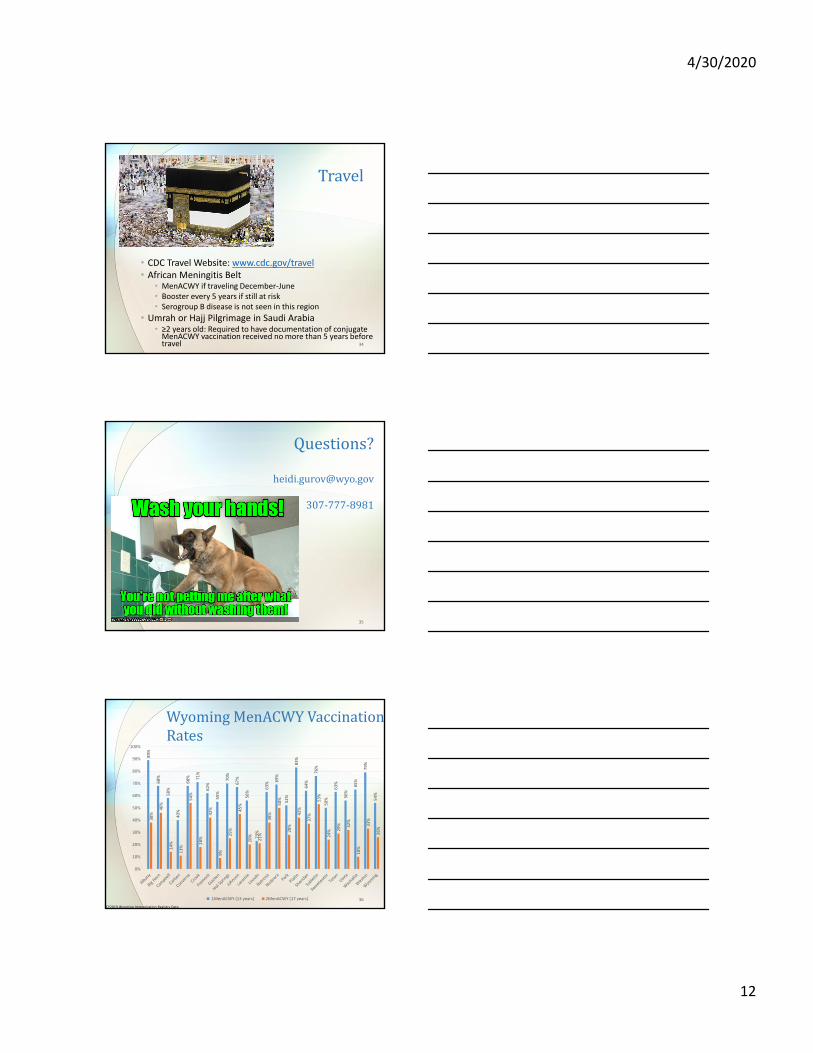
WyomingMenACWY VaccinationRates
89%
68%
58%
40%
68% 71%
62%
55%
70%
67%
56%
23%
63%
69%
52%
83%
64%
76%
50%
63%
56%
65%
79%
54%
38%
46%
14%
11%
54%
18%
42%
9%
25%
45%
20%
21%
38%
50%
28%
42%
37%
53%
24% 29% 32%
10%
33%
26%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1MenACWY (13 years) 2MenACWY (17 years) 36
CY2019 Wyoming Immunization Registry Data
4/30/2020
13
WyomingMandates
• Proposed rules• 1 dose of MenACWY at 11‐12 years
• 1 dose of MenACWY at 16 years
• Will apply to all students
37
IncreasingVaccinationRates• Most parents are aware of the disease, but have little knowledge about the disease
• Key talking points:• Rare but can be deadly• Increased risk is from mid/late teens to early 20s
• Disease can result in severe, lifelong disabilities• Vaccines are safe and effective• 2 vaccines are needed for complete coverage
• 2 doses of MenACWY
• Complete MenB series
• At risk of disease regardless of post‐high school education plans
• A strong provider recommendation is the #1 strategy for vaccine uptake
• Vaccine available through VFC and VUA programs 38
16YearOldPlatform
• Assures the vaccines recommended at 16 years are given on schedule• MenACWY 2nd dose
• MenB series
• Influenza (if in season)• Catch‐up opportunity
• Start/complete HPV series
• Start/complete other recommended immunizations
• Allows vaccination while patients are still covered by public or private insurance
• Creates opportunity to provide developmentally targeted care and guidance
39
4/30/2020
14
Questions??
40
Thankyou!!Heidi Gurov, RN BSN CMSRN ONC
Clinical Consultant & Quality Improvement SpecialistWyoming Department of Health
Immunization Unit
307‐777‐[email protected]
www.immunizewyoming.com
41