2017-2018 Employee Benefit Guide Legal Notifications ... · Dental Updates: o We have retained our...
33
Daniel Stafford, President & CEO 608.441.3035 x1 Cynthia Heidke CPA, Director of Finance & Operations 608.441.3035 x4 Amy Campbell, Director of Client Services 608.441.3035 x3 Stafford Financial Consulting Group Fax 608.441.3036 2017-2018 Employee Benefit Guide Legal Notifications Contact Information Prepared by: Stafford Financial Consulting Group LLC 2501 W Beltline Hwy Suite 201 Madison, WI 53713
Transcript of 2017-2018 Employee Benefit Guide Legal Notifications ... · Dental Updates: o We have retained our...
Daniel Stafford, President & CEO 608.441.3035 x1
Cynthia Heidke CPA, Director of Finance & Operations 608.441.3035 x4
Amy Campbell, Director of Client Services 608.441.3035 x3
Stafford Financial Consulting Group Fax 608.441.3036
2017-2018 Employee Benefit Guide
Legal Notifications
Contact Information
Prepared by:
Stafford Financial Consulting Group LLC
2501 W Beltline Hwy
Suite 201
Madison, WI 53713

IMPORTANT BENEFIT INFORMATION
With the new benefit plan year comes very important changes regarding your benefits through Foreman Brothers, Inc. Please be sure to read this communication, which outlines these changes, so you are informed regarding your benefits. 2017 UPDATES
Medical Updates: We have researched a number of excellent options in order to remain cost-effective for our employees while continuing to provide outstanding coverage.
o We have retained our current medical carrier, Blue Care Network and Blue Cross Blue Shield, which offer numerous providers throughout Michigan.
o There are no changes to the benefits provided on the medical plan.
o We are happy to announce that many of you will see a reduction in your healthcare premium; however, employees that have elected spousal or family coverage will see a modest increase in their rates. Please refer to the medical portion of this packet for details on the updated rates.
Dental Updates:
o We have retained our current dental carrier, Ameritas.
o There are no changes to the benefits provided on the dental plan.
o There will be a slight increase in the premium for this benefit.
Short Term Disability (STD) & Life:
o There are no changes to the STD & Life benefit in 2017.
**Please contact Sara Tubbs or Jill Farris
for questions or further information.
Benefits are effective on the 1st of the month following a Probationary Period of 60 days.
Blue Care Network HMO Plan 888.417.3479Blue Cross Blue Shield Simply Blue PPO Plan 877.469.2583
www.bcbsm.com
Ameritas 877.897.4328www.ameritas.com
Dearborn National 800.348.4512www.dearbornnational.com
Benefit Eligibility Requirements
Employee Benefit Plans
Medical
Dental & Vision
Life, AD&D and Short Term Disability
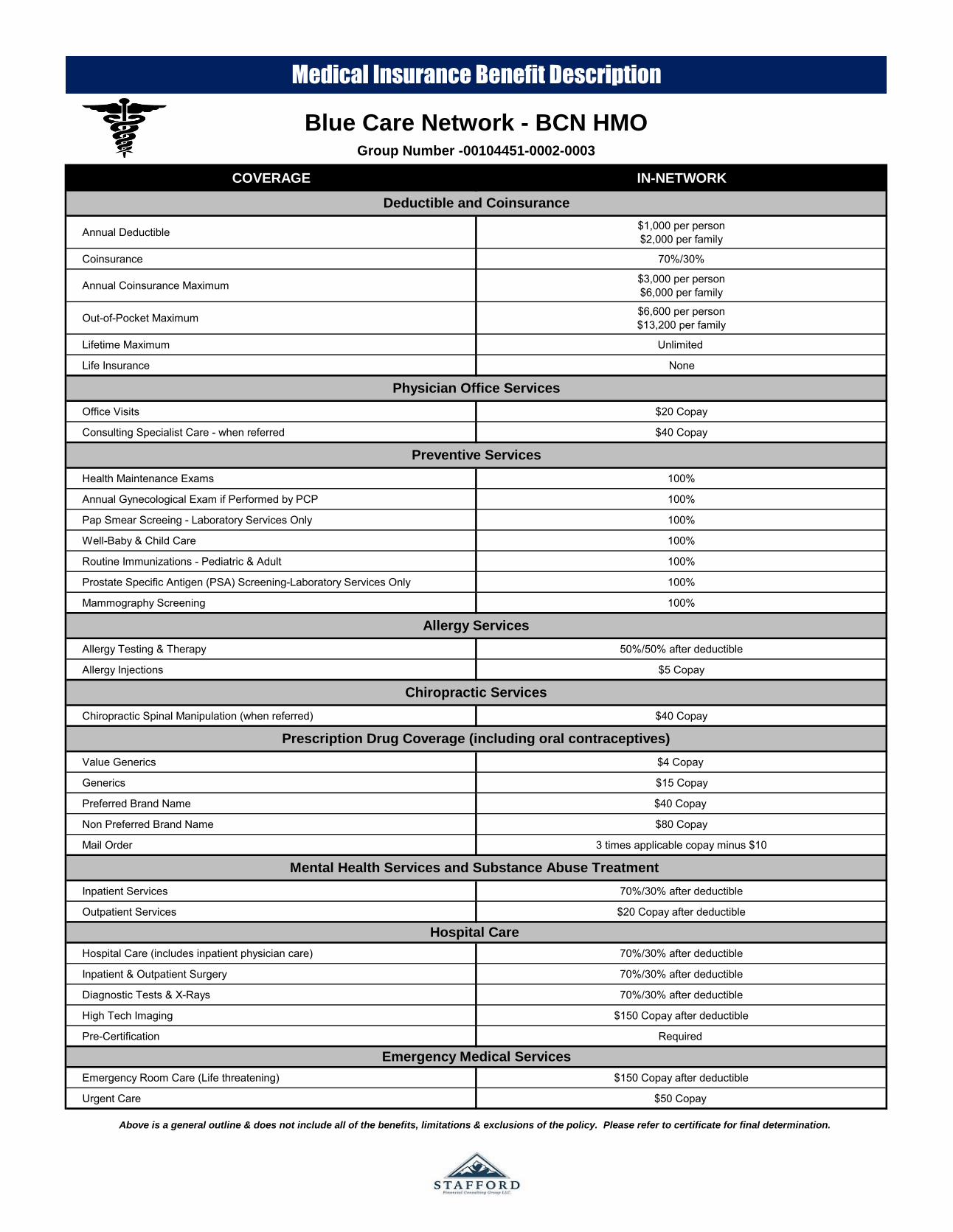
COVERAGE IN-NETWORK
Annual Deductible $1,000 per person$2,000 per family
Coinsurance 70%/30%
Annual Coinsurance Maximum $3,000 per person$6,000 per family
Out-of-Pocket Maximum $6,600 per person$13,200 per family
Lifetime Maximum Unlimited
Life Insurance None
Office Visits $20 Copay
Consulting Specialist Care - when referred $40 Copay
Health Maintenance Exams 100%
Annual Gynecological Exam if Performed by PCP 100%
Pap Smear Screeing - Laboratory Services Only 100%
Well-Baby & Child Care 100%
Routine Immunizations - Pediatric & Adult 100%
Prostate Specific Antigen (PSA) Screening-Laboratory Services Only 100%
Mammography Screening 100%
Allergy Testing & Therapy 50%/50% after deductible
Allergy Injections $5 Copay
Chiropractic Spinal Manipulation (when referred) $40 Copay
Value Generics $4 Copay
Generics $15 Copay
Preferred Brand Name $40 Copay
Non Preferred Brand Name $80 Copay
Mail Order 3 times applicable copay minus $10
Inpatient Services 70%/30% after deductible
Outpatient Services $20 Copay after deductible
Hospital Care (includes inpatient physician care) 70%/30% after deductible
Inpatient & Outpatient Surgery 70%/30% after deductible
Diagnostic Tests & X-Rays 70%/30% after deductible
High Tech Imaging $150 Copay after deductible
Pre-Certification Required
Emergency Room Care (Life threatening) $150 Copay after deductible
Urgent Care $50 Copay
Chiropractic Services
Preventive Services
Deductible and Coinsurance
Above is a general outline & does not include all of the benefits, limitations & exclusions of the policy. Please refer to certificate for final determination.
Emergency Medical Services
Hospital Care
Prescription Drug Coverage (including oral contraceptives)
Mental Health Services and Substance Abuse Treatment
Blue Care Network - BCN HMOGroup Number -00104451-0002-0003
Medical Insurance Benefit Description
Physician Office Services
Allergy Services

COVERAGE IN-NETWORK OUT-OF-NETWORK
Deductible $1,500 per person$3,000 per family
$3,000 per person$6,000 per family
Coinsurance 80%/20% of 24,250(20% of 24,250 = $4,850)
60%/40% of 24,250(40% of 24,250 = $9,700)
Out-of-Pocket Maximum $6,350 per person$12,700 per family
$12,700 per person$25,400 per family
Lifetime Maximum
Pre-existing Condition
Office Visits $40 Copay 60%/40% after deductible
Pre-Natal & Post Natal Care Pre-natal: No chargePost-natal: 80%/20% after deductible 60%/40% after deductible
Health Maintenance Exam 100% Not Covered
Annual Gynecological Exam 100% Not Covered
Pap Smear Screening - Lab & Pathology Services 100% Not Covered
Well Child Care 100% Not Covered
Routine Immunizations - Pediatric & Adult 100% Not Covered
Mammography Screening 100% 60%/40% after deductible
Allergy Testing & Therapy 80%/20% after deductible 60%/40% after deductible
Chiropractic Spinal Manipulation (12 visits) $40 Copay 60%/40% after deductible
Generic $10 Copay $10 Copay plus 25% of approved amountPreferred Brand Name $40 Copay $40 Copay plus 25% of approved amountNon Preferred Brand Name $80 Copay $80 Copay plus 25% of approved amountMail Order Two Copays for a 90-day Supply 90-day Supply no covered out-of-network
Inpatient Services 80%/20% after deductible 60%/40% after deductible
Outpatient Services 80%/20% after deductible 60%/40% after deductible
Inpatient Care 80%/20% after deductible 60%/40% after deductible
Inpatient & Outpatient Surgery 80%/20% after deductible 60%/40% after deductible
Diagnostic Tests, X-Rays & Labwork 80%/20% after deductible 60%/40% after deductible
Emergency Room (life threatening) $250 Copay $250 Copay
Urgent Care Center $60 Copay 60%/40% after deductible
Ambulance Services (medically necessary) 80%/20% after deductible 80%/20% after In Network deductible
Blue Cross/Blue Shield of Michigan
Simply Blue Plan 1,500Group Number - 007001322-0002
Medical Insurance Benefit Description
Physician Office Services
Deductible and Coinsurance
Above is a general outline & does not include all of the benefits, limitations & exclusions of the policy. Please refer to certificate for final determination.
Mental Health Services and Substance Abuse Treatment
Hospital Care
Emergency Medical Services
Unlimited
None
Prescription Drug Coverage (including oral contraceptives)
Allergy Services
Chiropractic Services
Preventive Services
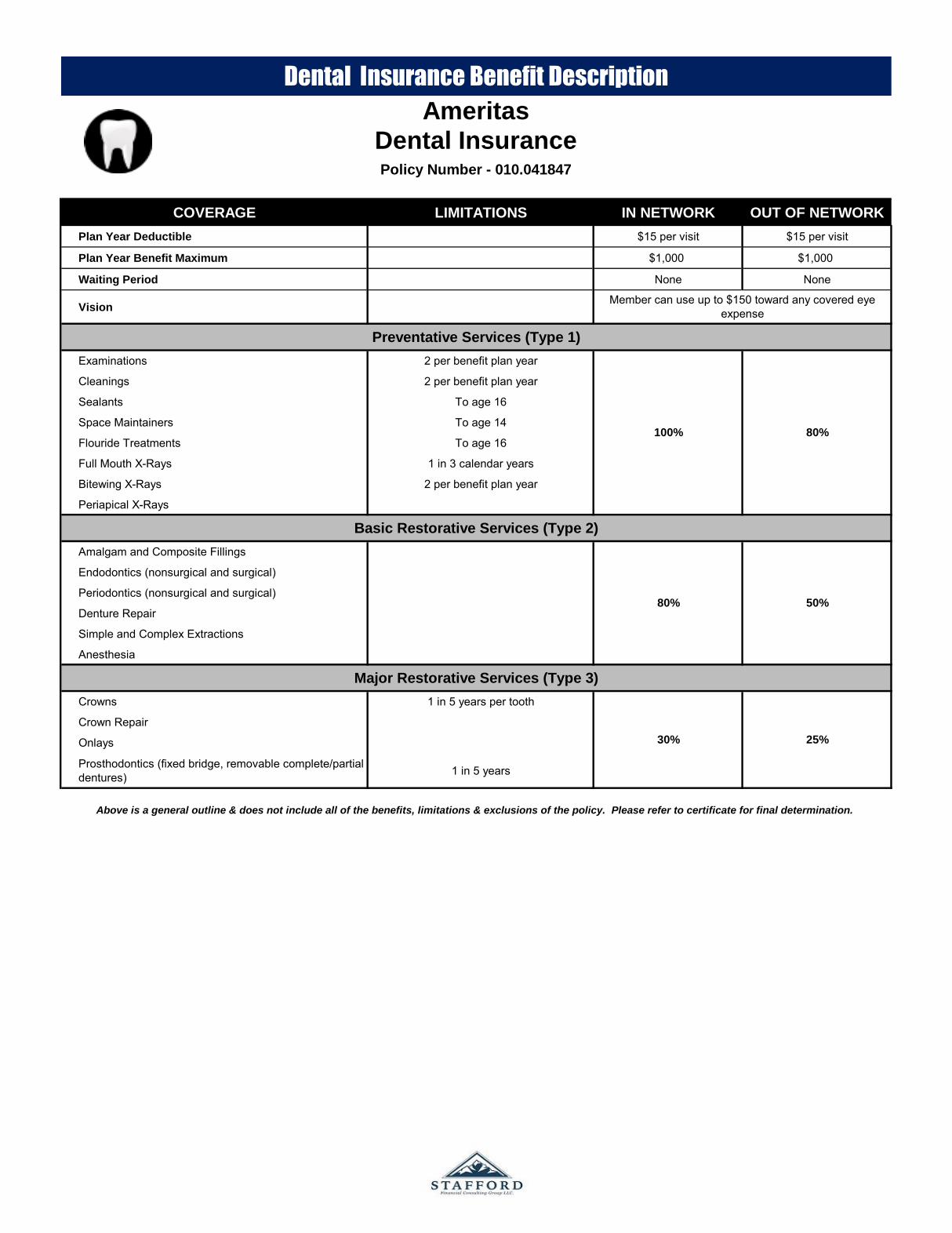
COVERAGE LIMITATIONS IN NETWORK OUT OF NETWORK
Plan Year Deductible $15 per visit $15 per visit
Plan Year Benefit Maximum $1,000 $1,000
Waiting Period None None
Vision
Examinations 2 per benefit plan year
Cleanings 2 per benefit plan year
Sealants To age 16
Space Maintainers To age 14
Flouride Treatments To age 16
Full Mouth X-Rays 1 in 3 calendar years
Bitewing X-Rays 2 per benefit plan year
Periapical X-Rays
Amalgam and Composite Fillings
Endodontics (nonsurgical and surgical)
Periodontics (nonsurgical and surgical)
Denture Repair
Simple and Complex Extractions
Anesthesia
Crowns 1 in 5 years per tooth
Crown Repair
Onlays
Prosthodontics (fixed bridge, removable complete/partial dentures) 1 in 5 years
Member can use up to $150 toward any covered eye expense
Above is a general outline & does not include all of the benefits, limitations & exclusions of the policy. Please refer to certificate for final determination.
Dental Insurance Benefit Description
Basic Restorative Services (Type 2)
Major Restorative Services (Type 3)
Policy Number - 010.041847
Preventative Services (Type 1)
Ameritas
Dental Insurance
100% 80%
80% 50%
30% 25%

PLAN DESIGN COVERAGE
Benefit Amount $15,000
AD&D Benefit $15,000
Waiver of Premium To age 65
Accelerated Death Benefit Up to 50% of the employee's life insurance
Portability (Life Only) Not included
Conversion Included
Reduction Schedule
Age 65 65% of original amount
Age 70 45% of original amount
Age 80 20% of original amount
PLAN DESIGN COVERAGE
Benefit Amount 60%
Maximum Per Week $400
Definition of Earnings Base weekly earnings
Benefit Duration 13 weeks
Waiting Period 8 calendar days
Life Insurance Benefit Description
Short Term Disability Benefit Description
Life Insurance
Dearborn National
Please refer to certificate for final determination.
Short Term Disability
Dearborn National
Above is a general outline & does not include all of the benefits, limitations & exclusions of the policy.
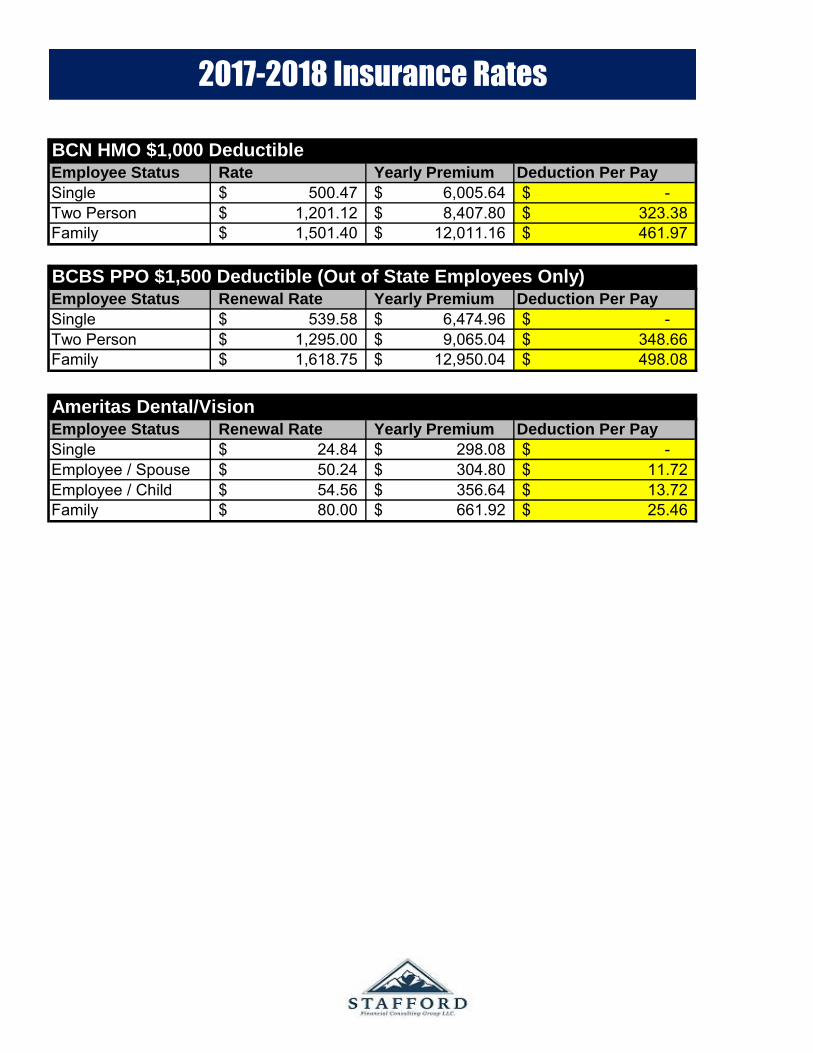
BCN HMO $1,000 DeductibleEmployee Status Rate Yearly Premium Deduction Per Pay
Single 500.47$ 6,005.64$ -$ Two Person 1,201.12$ 8,407.80$ 323.38$ Family 1,501.40$ 12,011.16$ 461.97$
BCBS PPO $1,500 Deductible (Out of State Employees Only)Employee Status Renewal Rate Yearly Premium Deduction Per Pay
Single 539.58$ 6,474.96$ -$ Two Person 1,295.00$ 9,065.04$ 348.66$ Family 1,618.75$ 12,950.04$ 498.08$
Ameritas Dental/VisionEmployee Status Renewal Rate Yearly Premium Deduction Per Pay
Single 24.84$ 298.08$ -$ Employee / Spouse 50.24$ 304.80$ 11.72$ Employee / Child 54.56$ 356.64$ 13.72$ Family 80.00$ 661.92$ 25.46$
2017-2018 Insurance Rates

Combined Insurance Enrollment Form Complete entire form to enroll or make changes Foreman Bros Inc (BCBSM)ENROLLMENT CHANGES
New Hire Name Address Marriage Divorce Beneficiary
Rehire Other (be specific):_______________________________
Open Enrollment Add dependent (check one) Marriage Newborn Other: _________________________________________________
COBRA Waive Drop Dependent (check one) Divorce Over age dependent Other:
SUBSCRIBER INFORMATION Name (First, MI, Last) SSN Gender Marital Status Birthdate
M F S M
Home Street Address City State Zip County
Primary Phone Home Work Cell Secondary Phone Home Work Cell Email Address
Date of Hire Effective Date Average Hours Worked Per Week Job Title Annual Salary
LIST DEPENDENTS TO BE COVERED/DELETED Name (First, MI, Last) Spouse/Child Gender Date of Birth Social Security Number Medical Dental Waive
_______________________________________________________ _______________ M F ______________ __________________________
_______________________________________________________ _______________ M F ______________ __________________________
_______________________________________________________ _______________ M F ______________ __________________________
_______________________________________________________ _______________ M F ______________ ___________________________
_______________________________________________________ _______________ M F ______________ ___________________________
Are any members listed enrolled in Medicare? Yes No If Yes, check reason: Working Aged Retired Disabled ESRD
List Member Name(s) HIC#: Effective Date Part A: Part B: Part D:
Primary Beneficiary (For Life and AD&D) -- Name (First, MI, Last): Relationship:
Contingent Beneficiary (For Life and AD&D) – Name (First, MI, Last): Relationship:
Do you or any members listed maintain other health coverage? Yes No If Yes, complete below:
List Member Name(s) Employer/Group Name: Policy#: Carrier:
COVERAGE TO BE ENROLLED IN: BLUE CROSS BLUE SHIELD MEDICAL 00104451 0002
AMERITAS DENTAL/VISION 010.041847
DEARBORN NATIONAL STD 60% $400 / LTD 60% $2500 / LIFE and AD&D 21485
I have read and understand Signature Date
the conditions of this form:
5/13
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight

Combined Insurance Enrollment Form Complete entire form to enroll or make changes Foreman Bros Inc (BCN)ENROLLMENT CHANGES
New Hire Name Address Marriage Divorce Beneficiary
Rehire Other (be specific):________________________________________________________________________________________________________
Open Enrollment Add dependent (check one) Marriage Newborn Other: _________________________________________________
COBRA Waive Drop Dependent (check one) Divorce Over age dependent Other:
SUBSCRIBER INFORMATION Name (First, MI, Last) SSN Gender Marital Status Birthdate
M F S M
Home Street Address City State Zip County
Primary Phone Home Work Cell Secondary Phone Home Work Cell Email Address
Date of Hire Effective Date Average Hours Worked Per Week Job Title Annual Salary
LIST DEPENDENTS TO BE COVERED/DELETED Name (First, MI, Last) Spouse/Child Gender Date of Birth Social Security Number Medical Dental Waive
_______________________________________________________ _______________ M F ______________ _____________________________
_______________________________________________________ _______________ M F ______________ _____________________________
_______________________________________________________ _______________ M F ______________ _____________________________
_______________________________________________________ _______________ M F ______________ _____________________________
_______________________________________________________ _______________ M F ______________ _____________________________
Are any members listed enrolled in Medicare? Yes No If Yes, check reason: Working Aged Retired Disabled ESRD
List Member Name(s) HIC#: Effective Date Part A: Part B: Part D:
Primary Beneficiary (For Life and AD&D) -- Name (First, MI, Last): Relationship:
Contingent Beneficiary (For Life and AD&D) – Name (First, MI, Last): Relationship:
Do you or any members listed maintain other health coverage? Yes No If Yes, complete below:
List Member Name(s) Employer/Group Name: Policy#: Carrier:
COVERAGE TO BE ENROLLED IN: BLUE CARE NETWORK MEDICAL 00104451 0002 0003 ***Complete PCP Selection Form***
AMERITAS DENTAL/VISION 010.041847
DEARBORN NATIONAL STD 60% $400 / LTD 60% $2500 / LIFE and AD&D 21485
I have read and understand Signature Date
the conditions of this form:
5/13
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight

Policy and Div. # 010- _____________________________
Cert. # ________________________________________ COBRA: If individual is a continuee:
Qualifying Event Date of Event
Name and Address of Employer (Policyholder)
1 to enroll Dental To terminate all coveragesEmployee InformationMarital Status Single Married Civil Union* Domestic Partner* *As defined by state law or your Group.
Social Security number __________________________ Dept. number __________________________
Employee’s last name, first name, MI ____________________________________________________________________________________
Date of birth________________ Male Female Full time date of hire________________ Rehire: Rehire date ________________
Occupation ________________________________________ Hours worked each week_____ Are your earnings paid: Hourly or Salaried
Street address_____________________________________________ City__________________________ State_____ ZIP ____________
E-mail address (limit of 60 characters) ___________________________________________________________________________________
Are you covered under another dental insurance plan? . . . . . . . . . . . . . . . . .Employee: Yes No Dependents: Yes No
Dependent Coverage Information List all eligible dependents to be added or deleted. (Employee must be enrolled to cover dependents)
Print full legal name (last, first. MI)Dental
Relationship Sex Date of birth Social Security no.College
student?add drop
1
2
3
4
5
Please Sign (employee/policyholder) The certificate provides dental benefits only. Review your certificate carefully.As an employee, I hereby apply for, or waive (if indicated), group insurance, for which I am eligible or may become eligible. If contributions are required, I authorize my employer to deduct premiums from my salary. THE FOLLOWING APPLIES ONLY TO SECTION 125 FLEXIBLE BENEFITS PLANS: I am signing up for coverage until the next enrollment period except in the case of a life event. This information was explained in the plan’s solicitation materials which I have read and understand. I represent that the information I have provided is complete and accurate to the best of my knowledge. The policyholder certifies the date of employment, job title, hours worked and salary information are correct according to the Policyholder’s records.
XEmployee Signature (do not print) Date
XPolicyholder Signature (do not print) Date
In several states, we are required to advise you of the following: Any person who knowingly and with intent to defraud provides false, incomplete, or mislead-ing information in an application for insurance, or who knowingly presents a false or fraudulent claim for payment of a loss or benefit, is guilty of a crime and may be subject to fines and criminal penalties, including imprisonment. In addition, insurance benefits may be denied if false information provided by an applicant is materially related to a claim. (State-specific statements on back.)
Employee late entrant date ______________________
Dependent late entrant date _____________________
Effective Date Class Dep. Code
2 to change Name Change New Name _________________________________________ Old Name____________________________________ Add Dependent Coverage
If due to marriage, what is the date of marriage?_____________ If due to birth/adoption, what is the date of event?____________________
If due to loss of coverage, date and reason: _________________________________________________________________________
If other, the date of event and please explain: ________________________________________________________________________
Drop Dependent Coverage Number of dependents still covered: ______ Effective date of drop: _______________________________ Due to divorce Due to death Due to annual election period Exceeds maximum age to qualify as dependent
Other (please explain) _________________________________________________________________________________________
3 to waive IF YOU DO NOT WANT COVERAGE, COMPLETE THE WAIVER SECTION. THE WAIVER MAY NOT BE ALLOWED FOR THIS PLAN, CHECK WITH YOUR EMPLOYER. I have been given an opportunity to apply for Group Insurance offered by my employer, and have decided not to accept the offer for:
myself (does not apply to TRUST policies) spouse/domestic partner child(ren) only spouse/domestic partner and child(ren)
because _________________________________________________________________________________________________________
Name of insurance company and employer of dependent _____________________________________________________________________Should I desire to apply for this group insurance in the future, I realize that a “late entrant” penalty may be applied.
GR 875 Rev. 06-12 Page 1 of 2 Dental 10-30-13
enrollment / change / waiver Group Insurance FormAmeritas Life Insurance Corp. P.O. Box 81889 / Lincoln, NE 68501-1889 / 800-659-2223 / Fax: 402-467-7338
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Sara
Highlight
Note for California Residents: California law prohibits an HIV test from being required or used by health insurance companies as a condition of obtaining health insurance coverage.
For group policies issued, amended, delivered, or renewed in California, dependent coverage includes individuals who are registered domestic partners and their dependents.
No Cost Language Services. You can get an interpreter and have documents read to you in your language. For help, call us at the number listed on your ID card or 877-233-3797. For more help call the CA Dept. of Insurance at 800-927-4357.
Servicios de idiomas sin costo. Puede obtener un intérprete y que le lean los documentos en español. Para obtener ayuda, llámenos al número que figura en su tarjeta de identificación o al 877-233-3797. Para obtener más ayuda, llame al Departamento de Seguros de CA al 800-927-4357.
Note for Colorado Residents: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company. Penalties may include imprisonment, fines, denial of insurance, and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado Division of Insurance within the Department of Regulatory Agencies.
Note for Florida Residents: Any person who knowingly and with intent to injure, defraud or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony of the third degree.
Note for Georgia, Kansas, Nebraska, Oregon, Vermont and Virginia Residents: Any person who, with intent to defraud or knowing that he is facilitating a fraud against insurer, submits an application or files a claim containing a false or deceptive statement may have violated state law.
Note for Kentucky Residents: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime.
Note for Maryland Insureds: Any person who knowingly and willfully presents a false or fraudulent claim for payment of a loss or benefit or who knowingly and willfully presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Note for New Jersey Residents: Any person who includes any false or misleading information on an application for an insurance policy is subject to criminal and civil penalties.
Note for New Mexico and Rhode Island Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to civil fines and criminal penalties.
Note for North Carolina Residents: After 2 years from the date of issue or reinstatement of this policy, no misstatements made by the applicant in the application shall be used to void the policy or deny a claim for loss commencing after the expiration of such 2 year period.
Note for Pennsylvania Residents: Any person who knowingly and with intent to defraud any insurance company or other person, files an application for insurance or statement of claim containing any materially false information or conceals for the purpose of misleading information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties.
Note for Tennessee Residents: It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purposes of defrauding the company. Penalties include imprisonment, fines and denial of coverage.
Note for Texas Residents: Any person who knowingly and with intent to defraud provides false, incomplete or misleading information in an application for insurance, or who knowingly presents a false or fraudulent claim for payment of a loss or benefit, may be guilty of a crime and may be subject to fines and criminal penalties, including imprisonment. In addition, insurance benefits may be denied if false information provided by an applicant is materially related to a claim.
Note for Washington, D.C. Residents: Any person who knowingly presents a false or fraudulent claim for payment of a loss or benefit or knowingly presents false information in an application for insurance is guilty of a crime and may be subject to fines and confinement in prison.
Note for Washington Residents: For groups policies issued, amended, delivered, or renewed in Washington, dependent coverage includes individuals who are registered domestic partners and their dependents.
tips for filling out this formTo EnrollMissing, incomplete or illegible information can cause delays in adding new employees to the system and could create errors in billing. To ensure proper handling of your enrollment forms, please make sure the following areas are completed:• Policy Name and Group Number – to make sure plan members are
added to the correct group.• Department/Division Numbers – so plan members are added in the
proper locations, and appear in the appropriate section on the billing if the group has multiple departments or divisions.
• Social Security Numbers – the most important identifier for plan members when calling in with claims or administrative questions. Please double check to make sure your social security number is accurate and written clearly.
• Full-time Employment Date – needed so the correct effective date is calculated for new members.
• Class Number – needed when the plan has more than one class of employees.
To ChangeChanging Dependent Codes – When adding or dropping dependents, please note whether this change is because of a “life event” or for some other reason. (Examples of life events: marriage, birth of a child, divorce . . . ) Please remember to include the date of the event. Late entrant status will be applied if a life event is not included. Be specific when changing status so all dependents who are still eligible will be covered.
ImagingIn order to provide better service, our administration system utilizes image technology. In the image environment, we scan your enrollment forms into our system, making them easier and faster to access. Better quality forms help us to process your enrollments faster. Unfortunately, certain forms are difficult or impossible to scan. The following list of helpful hints will make your forms easier to scan:Do:1) submit clear, legible enrollment forms.2) underline or circle important information.3) use blue or black ink.
Don’t:1) submit dark copies as they appear black on imaging.2) highlight, which blackens the area so it cannot be read.3) write on the top or bottom margins. This information is not always
captured on the image system.
GR 875 Rev. 06-12 Page 2 of 2 Dental 10-30-13

Insurance Lingo
What is a Copay?
Your portion of the cost, usually a flat dollar amount such as $20 per office visit. Other copays include $15/$40/$80 prescription drug, $150 emergency room, $50 urgent care and $40 chiropractic. These do not count toward the deductible or out of pocket maximum.(HMO copays used in this example.)
What is a Deductible?
The deductible is the amount you pay before BC begins to pay for covered services. Deductiblesare required every calendar year. Example: If you have a $1,000 annual deductible, before BC willpay, you must pay the first $1,000 in covered charges for covered health care services. Anywhereon the benefits page that you see "after deductible" you will have to pay the $1,000 first.(HMO deductibles used in this example.)
What is Coinsurance?
The shared payment between you and BC. For example, BC pays 70% and you pay 30%. Afteryou pay the deductible, the coinsurance kicks in.(HMO coinsurance used in this example.)
What is Out of Pocket Maximum?
The most money you can expect to pay a year for covered expenses that fall under inpatient andoutpatient hospital; inpatient and outpatient mental health and substance abuse; diagnostic, X-ray,lab, ambulance and allergy testing.

Annual Maximum The maximum benefit amount that your plan will pay each year.
Carrier The insurance company through which you have your benefits.
Certificate of Credible CoverageIssued by an insurance carrier after a subscriber has terminated their coverage; the certficate is required by the new carrier to avoid any penalties or benefit limitations.
Claim A bill that is submitted to your carrier for payment.
Copay A flat dollar amount that you pay for an office visit or prescription.
Coinsurance A percentage that you pay after your deductible is met (10%, 20%, etc.).
DeductibleThe amount you pay before your coinsurance kicks in; renews every January and usually does not apply to prescriptions or in-network office visits.
EOBExplanation of Benefits that your carrier sends out to you to show how your services were paid.
Effective Date The date that your coverage goes into effect.
Enrollment
The process that you go through to sign up for your benefits through an employment group; you will need to fill out applications with your information and your dependents' information.
Group NumberThe number assigned by a carrier to your employer group for your particular benefit package.
Group RepresentativeThe contact person at Stafford Financial Consulting Group that you can call if you have any benefit or claims questions.
HMOHealth Maintenance Organization; a plan where you choose one physician for all of your health needs.
Insurance AgentA person who is licensed to administer your group's benefits and who usually works with a contact person at your company; your agent is Dan Stafford.
Lifetime Maximum The maximum amount that a carrier will pay for each person during their lifetime.
Stafford Financial Consulting GroupThe agency that represents employer groups like yours and works as a liason between the carrier and the employer group.
Mail Order Prescriptions Ordering a 90-day supply of your medication by mail at a discounted price.
Master Medical Insurance coverage that requires you to submit a claim form for reimbursement.
NetworkA group of providers that have agreed to accept the terms and conditions of payment offered by a carrier.
New Hire Wait PeriodThe amount of time that a new employee must work for a company before he/she is eligible for that company's insurance plan.
Out-of-Pocket MaximumBased on your deductible and coinsurance, this is the maximum amount that you would have to pay for services rendered throughout the calendar year.
Participating ProviderA physician, hospital, or lab center that has aggreed to accept your carrier's payment schedule.
Glossary of Terms
Page 1

Glossary of Terms
PCPPrimary Care Physician in your HMO plan who takes care of all of your health needs or refers you to another specialist in the network.
POSPoint-of-Service plan that allows you to pick your benefit level when services are rendered.
PPO
Preferred Provider Organization, a plan that uses a network of participating doctors to help keep your costs down. "In-Network" refers to services rendered by a provider that participates with your carriers' payment plans - usually a lower deductible. "Out-of-Network" refers to services rendered by a provider that does not participate with your carriers' payment plans, resulting in a higher deductible and higher coinsurance.
Premium The amount that one pays for their benefits.
Provider A physician, hospital, lab, etc. that performs medical services.
ReimbursementPayment that you will receive from the carrier for services that you paid for up front, then submit a claim form.
Service Refers to the procedures performed by a provider.
SubscriberSomeone who is signed up for insurance through their employer's plan; you are a subscriber if you are enrolled with your company's plan.
Subscriber Number Unique number that Identifies you when you call your insurance carrier.
Traditional Plan An insurance plan that allows you to go to any provider and does not use a network.
Waiver A person who declines the insurance offered to them by their employer.
Page 2
Things You Should Know
EMERGENCY ROOMYou are covered for true medical emergencies.
Medical Emergency is an unexpected life-threatening condition. (i.e., heart attack, stroke, breathing difficulty, unconsciousness, etc.)
First Aid Emergency is an injury caused by trauma or accident (i.e., broken bones, allergic reactions, frostbite, sprains, etc.)
Non-Emergency should be treated at an Urgent Care Facility or to your doctor's office. (i.e., sore throat, flu symptoms, upset stomach, etc.)
OUT-OF-POCKET COSTSOther than your co-pays and deductibles, you may be responsible for additional costs such as:
Balance Billing - Your insurance carrier "reasonable & customary" charges may differ from yourdoctor or dentist's charges. The difference is a bill you would receive from your provider for payment.
Non-Covered Medical Services - Services that are not covered in your insurance policy. These services are the "rejected" and you would receive a bill from your provider (doctor, lab, hospital) for payment. (i.e., limited office visits, experimental procedures, etc.)
See the Phone Number page in this booklet for the Toll-Free numbers to call to verify coverage
before the service is done.
Events That Require Employer Notification
In the event that you should experience any of the following life events, you must notifyHuman Resources within 30 days of the event in order to have your coverage adjustedaccordingly:
Birth of a child Adoption or Legal Guardianship of a child Marriage Dependent stepchild due to marriage Divorce or legal separation Loss of child's dependent status - Child Turns 26 (health only) - Child Turns 19 (dental only) - Entry into Military Family death of a dependent Dependent's loss of coverage through spouse's plan Any other life event not listed
Unless otherwise indicated, changes not reported within 30 days of an event can only be made
during the annual open enrollment period.
Required Annual Notices
FEDERAL WOMEN'S HEALTH & CANCER RIGHTS ACT OF 1998
The Women's Health and Cancer Rights Act of 1998 (WHCRA) was signed into law on October 21, 1998. The WHCRA which amends ERISA, requires group health plans that provide coverage for mastectomies to also provide coverage for reconstructive surgery and prostheses following mastectomies.
Because your group health plan offers coverage for mastectomies, WHCRA applies to your plan. The law mandates that a participant who is receiving benefits, on or after the law's effective date, for a covered mastectomy and who elects breast reconstruction in connection with the mastectomy will also receive coverage for:
1. Reconstruction of the breast on which the mastectomy has been performed
2. Surgery and reconstruction of the other breast to produce a symmetrical appearance; and
3. Prosthesis and treatment of physical complications of all stages of mastectomy, including lymphedemas
This coverage will be provided in consultation with the patient and the patient’s attending physician and will be subject to the same annual deductible, coinsurance and/or copayment provisions otherwise applicable under the policy/plan.
NEWBORNS' AND MOTHERS' HEALTH PROTECTION ACT
Under federal law, group health plans and health insurance issuers offering group health insurance coverage generally may not restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a delivery by cesarean section. However, the plan or issuer may pay for a shorter stay if the attending provider (e.g., your physician, nurse midwife, or physician assistant), after consultation with the mother, discharges the mother or newborn earlier. Also, under federal law, plans and issuers may not set the level of benefits or out-of-pocket costs so that any later portion of the 48-hour (or 96-hour) stay is treated in a manner less favorable to the mother or newborn than any earlier portion of the stay.
In addition, a plan or issuer may not, under federal law, require that you, your physician, or other Health care provider obtain authorization for prescribing a length of stay of up to 48 hours (or 96 hours). However, you may be required to obtain precertification for any days of confinement that exceeds 48 hours (or 96 hours). For information on precertification, contact your plan administrator.
Page 1

Required Annual Notices
PREMIUM ASSISTANCE UNDER MEDICAID AND THE CHILDREN'S HEALTH
INSURANCE PROGRAM (CHIP)
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov. If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available.
If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan.
If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage
within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-
444-EBSA (3272).
Page 2

Foreman Brothers Notice to Employees of Rights under FMLA
Your Rights Under the
Family and Medical Leave Act of 1983
FMLA requires covered employees to provide up to 12 weeks of unpaid, job-protected leave to "eligible" employees for certain family and medical reasons. Employees are eligible if they have worked for a covered employer for at least one year, and for 1,250 hours over the previous 12 months, and if there are at least 50 employees within 75 miles.
REASON FOR TAKING LEAVE
Unpaid leave must be granted for any of the following reasons:
To care for the employee's child after birth, or placement for adoption or foster care;
To care for the employee's spouse, son or daughter, or parent, who has a serious health condition;
For a serious health condition that makes the employee unable to perform the employee's job.
ADVANCE NOTICE AND MEDICAL CERTIFICATION
The employee may be required to provide advance leave notice and medical certification. Taking of leave may bedenied if requirements are not met.
The employee ordinarily must provide 30 days advance notice when the leave is "foreseeable."
An employer may require medical certification to support a request for leave because of a serious health condition, and may require second or third options (at the employer's expense) and a fitness for duty report to return to work.
JOB BENEFITS AND PROTECTION
For the duration of FMLA leave, the employer must maintain the employee's health coverage under any "group health plan."
Upon return from FMLA leave, most employees must be restored to their original or equivalent positions withequivalent pay, benefits, and other employment terms.
The use of FMLA leave cannot result in the loss of any employment benefit that accrued prior to the start of an employee's leave.
Page 1
Foreman Brothers Notice to Employees of Rights under FMLA
Your Rights Under the
Family and Medical Leave Act of 1983
UNLAWFUL ACTS BY EMPLOYER
FMLA makes it unlawful for any employer to:
Interfere with, restrain, or deny the exercise of any right provided under FMLA:
Discharge or discriminate against any person for opposing any practice made unlawful by FMLA or for involvement in any proceeding under or relating to FMLA.
ENFORCEMENT
The U.S. Department of Labor is authorized to investigate and resolve complaints or violations.
An eligible employee may bring a civil action against an employer for violations.
FMLA does not affect any Federal or State law prohibiting discrimination, or supersede any State or local law or collective bargaining agreement which provides greater family or medical leave rights.
FOR ADDITIONAL INFORMATION
Contact the nearest office of the Wage and Hour Division, listed in most telephone directories under U.S. Government, Department of Labor.
Page 2
Group Health Continuation of Coverage Under COBRA On April 7, 1986, a Federal law was enacted (Public Law 99-272, Title X) requiring that most employers sponsering group health plans offer employees and their families the opportunity for a temporary extension of health coverage(called "continuation coverage") at group rates in certain instances where coverage under the plans would otherwise end. This notice is intended to inform you, in a summary fashion, of your rights and obligations under the continuation coverage provisions of the new law. (Both you and your spouse should take the time to read this notice carefully). If you are an employee of:
Foreman Brothers
1799 14th Street
Detroit, MI 48216
and are covered by the Foreman Brothers, Group Health Plan, you have a right to choose this continuation coverage if you lose your group health coverage because of a reduction in your hours of employment or the termination of your employment (for reasons other than gross misconduct on your part).
If you are the spouse of an employee covered by Foreman Brothers Group Health Plan, you have the right to choose continuation of coverage for yourself if you lose group health coverage under the Foreman Brothers Group Health Plan for any of the following four reasons:
(1) The death of your spouse; (2) A termination of your spouse's employment (for reasons other than gross misconduct) or reduction in your spouse's hours of employment with Foreman Brothers;
(3) Divorce or legal separation from your spouse; or (4) Your spouse becomes entitled to Medicare.
In the case of a dependent child of an employee covered by the Foreman Brothers Group Health Plan, he or she has the right to continuation coverage if group health coverage under the Foreman Brothers Group Health Plan is lost for any of the following five reasons:
(1) The death of the employee; (2) A termination of the employee's employment (for reasons other than gross misconduct) or reduction in the employee's hours of employment with Foreman Brothers; (3) The employee's divorce or legal separation; (4) The employee becomes entitled to Medicare; or (5) The dependent child ceases to be a "dependent child" under the Foreman Brothers Group Health Plan.
Under the law, the employee of family member has the responsibility to inform the Plan Administrator of the Foreman
Brothers Group Health Plan of a divorce, legal separation, or a child losing dependent status under the Foreman
Brothers Group Health Plan within 60 days of the date of the later of the event or the date on which coverage would end under the Plan because of the event. Foreman Brothers has the responsibility to notify the Plan Administrator of the employee's death, termination, and reduction in hours of employment or Medicare entitlement. Similar rights may applyto certain retirees, spouses, and dependent children if your employer commences a bankruptcy proceeding and these individuals lose coverage.
When the Plan Administrator is notified that one of these event has occurred, the Plan Administator will in turn notifyyou that you have the right to choose continuation coverage. Under the law, you have at least 60 days from the dateyou would lose coverage because of one of the events described above to inform the Plan Administrator that you wantcontinuation coverage. If you do not choose continuation coverage on a timely basis, your group health insurance coveragewill end.
Page 1

Group Health Continuation of Coverage Under COBRA If you choose coverage, Foreman Brothers is required to give you coverage which, as of the time coverage is being provided, is identical to the coverage provided under the Plan to similarly situated employees or family members. The law requires that you be afforded the opportunity to maintain continuation coverage for 36 months unless you lostgroup health coverage because of a termination of employment or reduction in hours. In that case, the requiredcontinuation coverage peiord is 18 months. These 18 months may be extended for affected individuals to 36 months for termination of employment if other events (such as death, divorce, legal separation, or Medicare entitlement) occur during the 18-month period.
In no event will continuation coverage last beyond 36 months from the date of the event that originally made a qualified beneficiary eligible to elect coverage. The 18 months may be extended to 29 months if a qualified beneficiaryis determined by the Social Security Administration to be disabled (for Social Security disability purposes) at any timeduring the first 60 days of COBRA coverage. This 11-month extension is available to all individuals who are qualifiedbeneficiaries due to a termination or reduction in hours of employment. To benefit from this extension, a qualifiedbeneficiary must notify the Plan Administrator of that determination within 60 days and before the end of the original 18-month period. The affected individual must also notify the Plan Administrator within 30 days of any final determination that the individual is no longer disabled.
A child who is born to or placed for adoption with the covered employee during a period of COBRA coverage will be eligible to become a qualified beneficiary. In accordance with the terms of the Foreman Brothers Group Health Plan, and the requirements of federal law, these qualified beneficiaries can be added to COBRA coverage upon proper notification to Foreman Brothers fo the birth or adoption.
However, the law also provides that your continuation coverage may be cut short for any of the following reasons:
(1) Foreman Brothers no longer provides group health coverage to any of its employees; (2) The premiums for your continuation coverage are not paid on time; (3) The qualified beneficiary becomes covered under another group health plan that does not contain any exclusion or limitation with respect to any pre-existing condition he or she may have;(4) The qualified beneficiary becomes entitled to Medicare; or (5) The qualified beneficiary extends coverage for up to 29 months due to your disability and there has been finaldetermination that the individual is no longer disabled.
The Health Insurance Portability and Accountability Act of 1996 (HIPPA) restricts the extent to which group health plans may impose pre-existing condition limitations. These rules are generally effective for Plan Years beginning after June 30, 1997. HIPPA coordinates COBRA'S other coverage cur-off rule with these new limits as follows:
If you become covered by another group health plan and that plan contains a pre-existing condition limitation thataffects you, your COBRA coverage cannot be terminated. However, if the other plan's pre-existing condition rule does not apply to you by reason of HIPPA's restrictions on pre-existing conditions, then Foreman Brothers Group Health Plan may terminate your COBRA coverage.
When the Plan Administrator is notified that one of these event has occurred, the Plan Administator will in turn notifyyou that you have the right to choose continuation coverage. Under the law, you have at least 60 days from the dateyou would lose coverage because of one of the events described above to inform the Plan Administrator that you wantcontinuation coverage.
Page 2
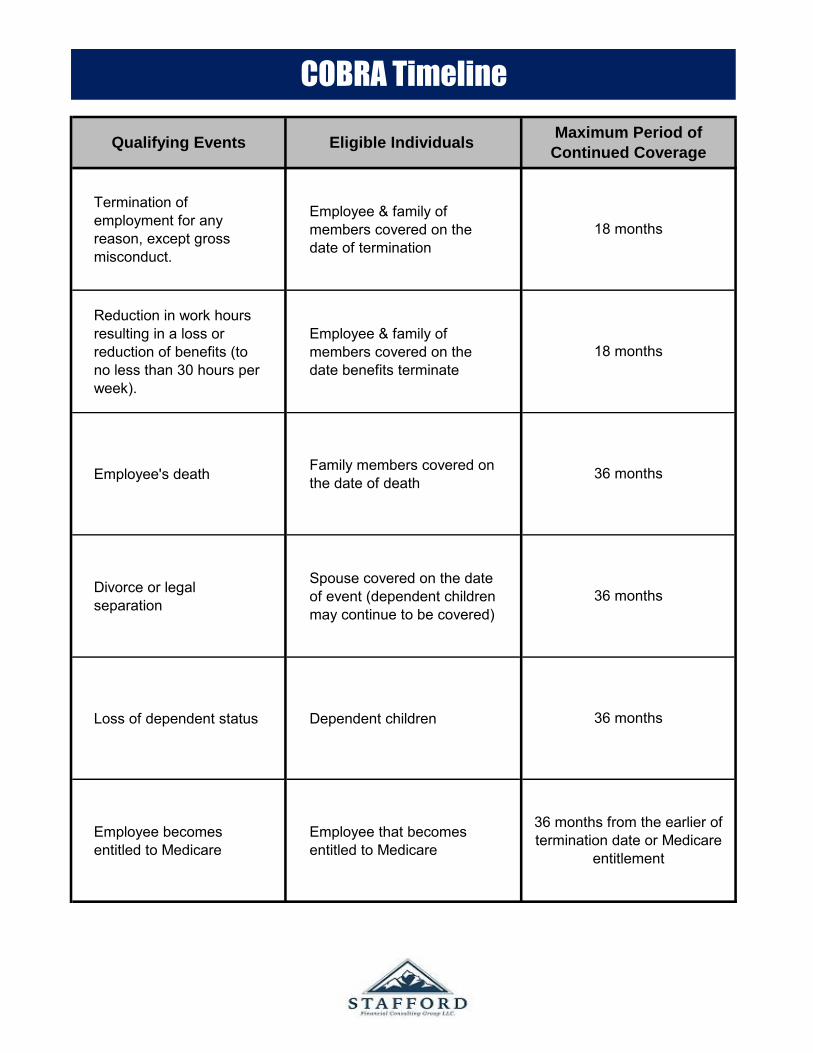
Termination of employment for any reason, except gross misconduct.
Employee & family of members covered on the date of termination
Reduction in work hours resulting in a loss or reduction of benefits (to no less than 30 hours per week).
Employee & family of members covered on the date benefits terminate
Employee's death Family members covered on the date of death
Divorce or legal separation
Spouse covered on the date of event (dependent children may continue to be covered)
Loss of dependent status Dependent children
Employee becomes entitled to Medicare
Employee that becomes entitled to Medicare
36 months
36 months
36 months
36 months from the earlier of termination date or Medicare
entitlement
COBRA Timeline
Qualifying Events Eligible Individuals Maximum Period of
Continued Coverage
18 months
18 months

Average Monthly Salary $2,500 Average Monthly Salary $2,500
Less Estimated FWT/SWT (25%) ($625) Less Medical Premium ($200)
Less Estimated FICA (7.65%) ($191) Taxable Income $2,300
Net Wages $1,684 Less Estimated FWT/SWT (25%) ($575)
Less Medical Premium ($200) Less Estimated FICA (7.65%) ($176)
Net Take Home Pay $1,484 Net Take Home Pay $1,549
Spendable Income $1,484 Spendable Income $1,549
can be amended to accommodate new benefits or terminate if no longer required.
1. Reduce your income tax and,2. Increase your take home pay
Section 125 Plan
W/out Section 125 Flexible Benefit Plan With Section 125 Flexible Benefit Plan
Premium Recovery Plan
Example of Employee Savings
Section 125 refers to a provision of the Internal Revenue Code. A Section 125 plan,commonly referred to as a Cafeteria Plan, permits an employee to pay their share of the cost of employee benefits with pre-tax dollars. The benefits may include Group Life,
The employer reduces the employee's salary by the amount the employee has been
A Section 125 plan is formally established using a plan document and adoption agreementLike other employer-sponsored benefits plans, this plan operates on a plan year basis; it
By using before tax-dollars to pay for employees' benefits, a Section 125 plan allows you to:
Health, Dental coverages, among others.
contributing toward the cost of their benefits.
Page 1

Acupuncture Services Mileage to Doctor's officeAlcoholism & Drug Abuse Treatment Naturopathy Treatment if Prescribed by M.D. Ambulance Hire Nurses Fees (including Nurses' Board & Social Security tax)Artificial Limbs Obstetrical Expenses Birth Control Pills & Devices Operations Braces Organ TransplantsBraille-Books & Magazines Orthopedic Shoes Breast Reconstructive Surgery Following a Mastectomy Oxygen & Oxygen Equipment Car Controls for the Handicapped Physician Fees Care for the Handicapped Child Practical Nurse Fees Childbirth Classes for mother only Psychiatric Care Chiropractors Psychologist Fees Christian Science Practitioners Fees Radial Keratotomy Co-insurance Amounts You Pay Routine physical & other Non-Diagnostic Services/ Contact Lenses for Medical Reasons TreatmentCost of Operations and Related Treatment Smoking Cessation Programs Crutches Specialty Foods to Alleviate an Illness or Condition Day Care Expenses for Eligible Depdendents as Special Education for the Handicapped Necessary for Employment (DCA Account) Sterilization FeesDeductibles for Medical Coverage Amount You Pay Surgical Fees Dental Fees Telephone, Special for Deaf Dentures Television Audio Display Equipment for the DeafDiagnostic Fees Therapeutic Care for Drug & Alcohol Addiction/ Therapy Drug and Medical Supplies Treatments Eyeglasses, including Exam Fee Transportation Expenses primarily in the Rendering of Handicapped Persons' Special Schools Medical Services (Limits Apply)Health Club Dues (to treat a specific illness) Tuition at Special School for Handicapped Tuition FeeHearing Devices and Batteries (Part), If College or Private School furnishes Home Improvements motivated by Medical Considerations breakdown of Medical ServicesHospital Insurance Vaccinations Hypnosis for Treatment of Illness Vasectomy Insulin Vitamins by PrescriptionLaboratory Fees Weight Loss Programs (prescribed by a doctor for Laetrile by Prescription treatment of a specific illness Lasik Eye Surgery Wheelchair Lead-base Paint Remover (For children with lead poisoning) Wig, Prescribed by Doctor for a Person who has lost hair Leader Dog and its upkeep as result of a disease Life Fee to Retirement Homes for Medical Expenses X-Ray Membership Fees in Association Furnishing Medical Services Hospitalization and Clinical Care
Bleaching teeth/whitening Hot tubs Capital expenditures Insurance premiums Cosmetic Procedures Marriage Counseling Dancing & swimming lessons Massage for non-medical reasonsExercise Equipment MattressesExpenses not incurred during period of enrollment Personal use items Expenses reimbursed under any health plan or source VacationHair loss items Vacuum cleaners Health club dues Weight loss expenses Herbs/vitamins/supplements that do not require a prescription for use
Medical Expense Reimbursement Plan
Section 125 Plan
Eligible Expenses
Ineligible Expenses
Page 2

What is a Section 125 Plan?
It is an employer-sponsered benefit plan which allows an employee to select from a list of available benefits, those benefits needed by the employee.
What does this benefit program
mean to me?
This program means that current after-tax expenditures for items such as medical insurances, disability income, dependent care costs, and some medical expenses not covered by insurance can now be paid for with pre-tax dollars. The bottom line is that you may have more dollars available to purchase other benefits you may need or available to you as increased take-home pay.
Will participation in a Section 125
Plan affect my Social Security?
Yes. FICA taxes will not be paid on Section 125 salary reductions. Therefore, your Social Security benefits at retirement may be reduced.
What happens if the tax laws
change next year?
No one can predict what future changes may occur in the tax laws. This Section 125 Plan has been set up in accordance with current laws and regulations. If the laws change, appropriate steps will be taken to bring this plan into compliance with any new rules.
How do I enroll in the Section 125
Plan?
After the group meeting, your Benefit Consultant will meet with you to complete an election form. This election form must be completed and signed by each employee, whether or not you wish to elect to participate in the benefit portion of the plan.
Must I make my election before the
effective date of the plan?
Yes. You must make your benefit election prior to the beginning of the plan year (effective date), or prior to becoming eligible to participate in the plan.
Section 125 PlanQuestions and Answers
Page 3

Can I make changes in my election
during the plan year?
The only time tax law regulations will allow you to make a change is if there is a valid change in you status effecting your need for a benefit. Some examples of a valid status change are a change in legal marital status, change in number of dependents, termination or commencement of employment, change in work schedule, dependent satisfies or ceases to satisfy dependent eligibility requirements, change in residence or work site. These examples may not be all-inclusive. If you elect to participate in the medical expense reimbursement account, election changes are limited, in most cases, to ceasing plan participation because of termination of your employment.
What is a qualified medical expense
for reimbursement under this plan?
Most medical expenses not reimbursed by any other source or an insurance plan, such as deductibles and co-insurance, and items not covered by insurance, such as vision care, dental costs, and routine physicals, are qualified medical expenses. See list of expenses eligible for reimbursement. These expenses may be either for you or for your dependents. Some cosmetic procedures do not qualify for reimbursement. You may only be reimbursed for expenses incurred for services rendered during the plan year, not for services rendered in a different plan year but paid in the current plan year. However, you may submit your claim(s) for reimbursement as long as 90 days afer the end of the plan year during in which you incurred your expenses.
Who is considered a qualified
dependent for reimbursement of
dependent care expenses?
Your dependent(s) under the age of 13 or your dependent(s) or spouse who is physically unable to care for himself or herself is considered to be a qualified dependent if their dependent care expenses could qualify for the federal income tax credit on your tax return.
Am I required to enroll in both the
dependent care and medical
expense reimbursement accounts?
No. You can enroll in either account, both accounts or neither account.
Section 125 PlanQuestions and Answers
Page 4

How do I get money from my
reimbursement accounts?
You must submit a voucher, which will be provided to you, for any expenses incurred during the plan year. This voucher must be accompanied by proper third party documentation of the nature of the expense, date the expense was incurred, and the provider of services and/or the dependent care provider acknowledgement form. The voucher will be processed by the plan record keeper and you will be reimbursed for your expense. The medical expense reimbursement check will be for the expense claimed up to the maximum benefit amount you elected for the plan year. The dependent care expense check will be for the expense you claimed up to the amount you have in your account.
What if my dependent care expense
voucher is for expenses in excess of
the amount in my account?
You will be reimbursed for the amount in your account and the balance of the expenses will be carried forward to future months as additional payments are received for your accounts.
Can I switch dollars between the
dependent care and medical
accounts?
No. The dollars must be used in each account as specified on the election form.
What happens if I don't incur
enough expenses to get back the
money deposited in my
reimbursement account?
Any expense dollars not used are forfeited to your employer. This is what is known as the "use it or lose it" provision of Section 125. It is very important to be conservative and accurate in estimating your expenses for the plan year.
Can I take the tax credit for
dependent care of the medical
expense deduction on my income
tax return if I am in the plan?
No. Expenses reimbursed under this plan may not be used when calculating your medical expense deduction or the dependent care tax credit. Because it is sometimes more advantageous to take the dependent care tax credit on your tax return than to participate in the dependent care expense reimbursement account, you should discuss which alternative is the best for you with you tax advisor.
Section 125 PlanQuestions and Answers
Page 5

Health Care Account Dependent Day Care Account
(Increase Only) (Increases or Decrease)
Marriage, divorce, legal separation, or annulment Marriage, divorce, legal separation, or annulment
Child birth, adoption or placement for adoption of a child Child birth, adoption or placement for adoption of a child
Death of your spouse or dependent childDeath of your spouse or dependent child
Beginning or end of employment of you, your spouse or dependent child Dependent or spouse satisfies or ceases to satisfy
eligibility requirements as a dependent under the Change in work schedule due to an increase in hours, full-time/ planpart-time switch, beginning or end of an unpaid leave of absence, strike or lockout or you or your spouse
Change in residence or work site of you, your spouse or dependent child that results in loss of eligibility
Loss of health care coverage as a result of loss of eligibilityor expiration of COBRA (not due to non payment or voluntary termination of COBRA coverage), termination of other coverage as a result of non-COBRA loss of eligibility(including as a result of legal separation, divorce, death, termination of employment or reduction in hours of unemployment) or termination or significant change or employer contribution
Spouse coverage terminates due to reduction of hours or loss of employment
Your spouse or dependent child initially meets eligibilityrequirements
Compliance with a judgment, decree, or order relating to accident/medical or dental coverage for a child resulting from a divorce, annulment or legal separation, including a QMCSO
Qualifying Events That Allow Employees to Make Changes to Their FSA
Section 125 Plan
Page 6

Notice of Privacy Practices for Private Health Information
THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
This Notice of Privacy Practices describes the practices of Foreman Brothers for safeguarding individually identifiableprivate health information. The terms of this Notice apply to members and dependents for their group medical expense, group dental expense and/or group vision care expense insurance. This Notice is effective April 1, 2003.
We are required by law to maintain the privacy of our members and dependents private health information and toprovide notice or our legal duties and privacy practices with respect to private health information. We are required to abide by the terms of the Notice as long as it remains in effect. We reserve the right to change the terms of the Noticeas necessary and to make the new Notice effective for all private health information maintained by us. Copies of revised Notices will be mailed to plan sponsors for distribution to the members then covered under the policy.
Uses and Disclosures of your Private Health Information
Authorization. Except as explained below, we will not use or disclose your private health information for any purpose unless you have signed a from authorizing a use or disclosure. Unless we have taken any action in reliance on the authorization, you have the right to revoke an authorization if the request for revocation is in writing and sent to: PrivacyOfficer, Foreman Brothers, 1799 14th St., Detroit, MI 48216 A form to revoke an authorization can be obtained fromthe Privacy Officer.
Disclosures for Treatment. We may disclose your private health information as necessary for your treatment. For instance, a doctor or healthcare facility involved in your care may request your private health information in our possession to assist in your care.
Uses and Disclosures for Payment. We will use and disclose your private health information as necessary for payment purposes. For instance, we may use your private health information to process or pay claims, or to perform a hospital admission review to determine whether services are for medically necessary care and to perform prospective reviews. We may also forward information to another insurer in order for it to process or pay claims on your behalf.
Uses and Disclosures for Health Care Operations. We will use and disclose your private health information as necessary for health care operations. For instance, we may use or disclose your private health information for quality assessment and quality improvement, evaluating health care providers, premium rating, conducting or arranging for medical review or compliance. We may also disclose your private health information an another insurer, health carefacility or health care provider for activities such as quality assurance or case management. We may contact your health care providers concerning prescription drug or treatment alternatives.
Other Health-Related Uses and Disclosures. We may contact you to provide reminders for appointments; information about treatment alternatives; or other health-related programs, products or services that may be available to you.
Information Received Pre-enrollment. We may request and receive from you and your health care providers private health information prior to your enrollment under the group policy. We will use this information to determine whetheryou are eligible to enroll under the policy and to determine the rates. If you do not enroll, we will not use or disclose theinformation we obtained about your for any other purpose. Information provided on enrollment forms or applications will be utilized for all coverages being applied for, some of which may be protected by the state, not federal, privacy laws.
Page 1
Notice of Privacy Practices for Private Health Information
Business Associate. Certain aspects and components of our services are performed by outside people or organizations pursuant to agreements or contracts. It may be necessary for us to disclose your private healthinformation to these outside people or organizations that perform services on our behalf. We require them to appropriately safeguard the privacy of your private health information.
Plan Sponsor. As a Plan Sponsor of a fully insured or self--insured medical plan, private health information will be maintained in a confidential manner and will not be utilized or disclosed for employment-related actions and decisionsor in connection with any other employee benefit plan of the plan sponsor.
Family, Friends and Personal Representatives. With your approval we may disclose to family members, closepersonal friends, or another person you identify, your private health information relevant to their involvement with your care or paying for your care. If you are unavailable, incapacitated or involved in an emergency situation, and wedetermine that a limited disclosure is in your best interests, we may disclose your private health information withoutyour approval. We may also disclose your private health information to public or private entities to assist in disasterrelief efforts.
Other Uses and Disclosures. We are permitted or required by law to use or disclose your private health information, without your authorization, in the following circumstances.
For any purpose required by law; For public health activities (for example, reporting of disease, injury, birth, death or suspicion of child abuse or neglect);To a governmental authority if we believe an individual is a victim of abuse, neglect or domestic violence; For health oversight activities (for example, audits, inspections, licensure actions or civil, administrative or criminal proceedings or actions);For judicial or administrative proceedings (for example, pursuant to court order, subpoena or discoveryrequest);For law enforcement purposes (for example, reporting wounds or injuries or for identifying or locating suspects,witnesses or missing people);To coroners and funeral directors; For procurement, banking or transplantation or organ, eye or tissue donations; For certain research purposes;To avert a serious threat to health or safety under certain circumstances; For military activities if you are a member of the armed forces; for intelligence or national security issues;or about an inmate or an individual to a correctional institution or law enforcement official having custody; and For compliance with workers' compensation programs.
We will adhere to all state and federal laws or regulations that provide additional privacy protections. We will only use or disclose AIDS/HIV-related information, genetic testing information and information pertaining to your mental condition or any substance abuse problems as permitted by state and federal law or regulation.
Your Rights
Restrictions on Use and Disclosure of Your private health information. You have the right to request restrictions on how we use or disclose your private health information for treatment, payment or health care operations. You also have the right to request restrictions on disclosures to family members or others who are involved in your care or the paying of you care. To request a restriction, you must send a written request to: Privacy Officer, Foreman Brothers, 1799 14th
St., Detroit, MI 48216. A form to request a restriction can be obtained from the privacy officer. We are not requiredto agree to your request for a restriction. If your request for a restriction is granted, you will receive a written acknowledgement from us.
Page 2

Notice of Privacy Practices for Private Health Information
Receiving Confidential Communications of Your private health information You have the right to request communications regarding your private health information from us by alternative means (for example by fax) or at alternative locations. We will accommodate reasonable requests. To request a confidential communication, you must send a written request to: Privacy Officer, Foreman Brothers, 1799 14th St., Detroit, MI 48216. A form to request a confidential communication can be obtained from the Health Information Protection Analyst.
Access to Your private health information. You have the right to inspect and/or obtain a copy of your private health information if any is maintained in our Personnel files. To request access to your information, you must send a written request to: Privacy Officer, Foreman Brothers, 1799 14th St., Detroit, MI 48216. A form to request access toyour private health information can be obtained from the Health Information Protection Analyst. A fee will be charged forcopying and postage.
Amendment of your private health information. You have the right to request an amendment to your private health information to correct inaccuracies. To request an amendment, you must send a written request to Privacy Officer; Foreman Brothers, 1799 14th St., Detroit, MI 48216. A form to request an amendment to your privatehealth information can be obtain for the Privacy Officer. We are not required to grant the request in certain circumstances.
Accounting of Disclosures of Your Private health information. You have the right to receive an accounting of certain disclosures made by us after April 14, 2003, of your private health information. To request an accounting,you must send a written request to: Privacy Officer, Company Name, address, city, state, zip. A form to request an accounting of your private health information can be obtained for the Privacy Officer. The first accountingin any 12 month period will be free; however, a fee will be charged for any subsequent request for an accounting during that same time period.
Page 3

Contact Information
Medical
Blue Cross Blue Shield Customer Service: 800-637-2227
www.bcbsm.com
Blue Care Network Customer Service: 800-662-6667
www.bcbsm.com
Dental & Vision
AmeritasCustomer Service: 877-897-4328
www.ameritas.com
Short Term Disability, Life, AD&D
Dearborn NationalCustomer Service: 800-348-4512 Claims Life, AD&D: 800-778-2281
Claims Short Term Disability: 877-348-0487www.dearbornnational.com
Insurance Advisors
Stafford Financial Consulting Group2501 W Beltline Hwy Suite 201
Madison, WI 53713Phone: 608-441-3035 Fax: 608-441-3036
www.sfcgus.com
Daniel Stafford, President & CEOCynthia Heidke CPA, Director of Finance & Operations
Amy Campbell, Director of Client Services