
2016 PQRS and VBM for Radiology - Medical Billing Company...
7
PERFORMANCE THAT MATTERS AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611 2016 PQRS and VBM for Radiology
-
Upload
nguyenduong -
Category
Documents
-
view
213 -
download
0
Transcript of 2016 PQRS and VBM for Radiology - Medical Billing Company...
PERFORMANCE THAT MATTERS
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
2016 PQRS and VBMfor Radiology
Table of Contents
Summary 1PQRS 1 Definitions 2 PQRSBasics 2 MAV 2 Claims-basedvs.Registry-based Reporting 3RadiologyPQRSmeasuresfor2016 3Value-BasedPaymentModifier(VBM) 5
SUMMARY
RadiologyPQRSreportingrequirementsfor2016aresimilartothosein2015butwiththeadditionofthreenewmeasures. If2016PQRSisnotreported,ornotreportedaccurately (acommonproblem),radiologistsingroupsof10ormoreproviderswillseea-6%adjustmenttoMedicarepaymentsin2018.Thoseinsmallergroupswillseea-4%adjustment.
ThereareseveralwaystoreportPQRSmeasuresbutaregistryisstronglyrecommendedforradiolo-gists,sinceCMSisphasingoutclaims-basedreportingandEHRreportingusuallyisn’tpractical.Mostimportant,however,aregistryapproachcaneliminatetheriskofthe-4%to-6%penalty.
PQRSresultsalsoshowupon“PhysicianCompare”andproposedchangeswillmapPQRSperformanceintoa5starratingsystemforconsumersbycomparingresultsacrossproviders.
PQRS
ToavoidpenaltiesfornotreportingPQRSandVBM,radiologistsmustmeettheBasic Reporting Requirements: -Individualsorgroupswhoreportindividualmeasuresmustcompleteninemeasuresforat
least50%of theeligibledenominator,andthosemeasuresmust include three National Quality Strategy Domains.
-Oneofthosemeasuresmustbe“cross-cutting,”asdefinedbyMedicare:apopulation-widemeasurerequiredforproviderswhoseeatleastonepatientina“face-to-face”encounter.
However,theserequirementsdonotmatchwellwithmanyradiologistssincecross-cuttingmeasuresmaynotapplyand9measuresmaynotapplytoeveryradiologist.Inthesecircumstances,radiologistsaresubjecttothe“MAV”audit,describedbelow.
PQRSissettoexpireafterthisyear(the2016PQRSreportingyearaffects2018Medicarepayments)andbereplacedbytheMerit-BasedIncentivePaymentSystem(MIPS)in2017(whichwillaffect2019
AT A GLANCE:
-PQRS/VBMpenaltiesare-4%to-6%
-Registryreportingisstronglyrecommended
-Thereare3newmeasuresfordiagnosticradiologyin2016
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 1

AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
payments).MIPSismandatedbyMACRA(theMedicareAccessandCHIPReauthorizationActof2015).MACRA eliminated the annual SGR payment reductions and, among other items, replaces PQRS,MeaningfulUseandtheVBM(ValueBasedModifier)programs.
However,whilethenamePQRSwilleventuallydisappear,thequalityreportingcomponentofMIPSwillbeheavilybasedonPQRS,meaningthatworkdonetocomplywithPQRSwilltransitionintotheMIPS environment. Furthermore, non-reporting penalties increase with MIPS, adding additionalincentivetohavegoodqualityreportinginplace.
DEFINITIONS
Thefollowingabbreviationsareusedinthispaper,consistentwithCMSterminology:EP–EligibleprofessionalGP–GroupPracticeEHR–ElectronicHealthRecordQCDR–QualifiedClinicalDataRegistry
PQRSBASICS
-There isno incentivepayment forreportingPQRSmeasures in2016. However,bonuspayments may be earned via the Value Based Modifier Program (which starts withPQRSdata).
-EPswhodonotsuccessfullyparticipatein2016willreceivea-2%PQRSpaymentadjustmentanda-2%or-4%VBMadjustmentontheir2018Medicarepayments.
-WhiletherearehundredsofPQRSmeasures,only12orfewertypicallyapplytodiagnosticradiology,asdescribedbelow.
-PQRScanbereportedviaclaims,registry,EHR,QCDRorGPRO(groupsonly).Thefirst4methodsaretypicallyusedforindividualEPs,evenwhenpartofagroup.However, claims-based reporting is being phased out by CMS so it is recommended to use one of the other methods.
-Forat least50%ofMedicarepatients,CMSrequiresreportingon9measures,at leastoneofwhichisaso-called“cross-cuttingmeasure”.Butmanyradiologists,donothave9applicablemeasures,inwhichcasetheMAVapplies(seebelow).
Itisveryimportanttonotethatmeasuresaredefinedonameasure-by-measurebasis,not by specialty.Thatisbecausetwoprovidersinthesamespecialtymaynotperformthesameservices.
MAV
For those who report fewer than nine measures or fewer than three domains, the MeasureApplicabilityValidation(MAV)Auditapplies.MedicarecomparesyourPQRSdatatoitsmeasurespecificationstoidentifyothermeasureswhichcouldhavebeenreported,butwerenot.Whilethemeasurestheyidentifymaynotseemrelevant,iftheymeetMedicare’sdefinition,theydirectlyaffectyourPQRScompliance.
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 2

145
146
147
195
225
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
Claims-based vs. Registry-based Reporting
Inthispaper,wefocusprimarilyonclaimsandregistry-basedreportingsincemanyradiologygroupsdonothavetheabilitytouseanEHRforEHR-basedreporting(andmanyEHRsdonothavethenecessaryCEHRTcertification to report themeasures).QCDR isabroader topicas that reportingmethodtypicallyrequiresadditionalqualitymeasuresbeyondthoseinPQRS.
WithPQRSpenaltiesnowsignificant (-4% to -6%when combined with the VBM penalty), registryreporting is becoming almost essential. This is because claims-based reporting doesn’t provideanyMAVinsight,untilitistoolate.Furthermore,theprocesstoreviewclaims-filedPQRSdataiscumbersome,atbest.In2015,thosewhousedclaims-basedreportingspentcountlesshourstryingtodeterminewhatdataCMSactuallyhad.Andevenwhenbaddatawasappealed,penaltieswerestillapplied.Registryreportingprovidesongoingfeedbackand,importantly,providesfeedbackonhowanEPorgroupwillfareinaMAVAudit.Inaddition,witharegistry,PQRSdatacanbeupdatedorevenreplaced,somethingthatisimpossiblewithclaims-basedfiling.Asaresult,usingaregistryeliminatesMAVandPQRSpenaltyrisks.
RADIOLOGYPQRSMEASURESFOR2016
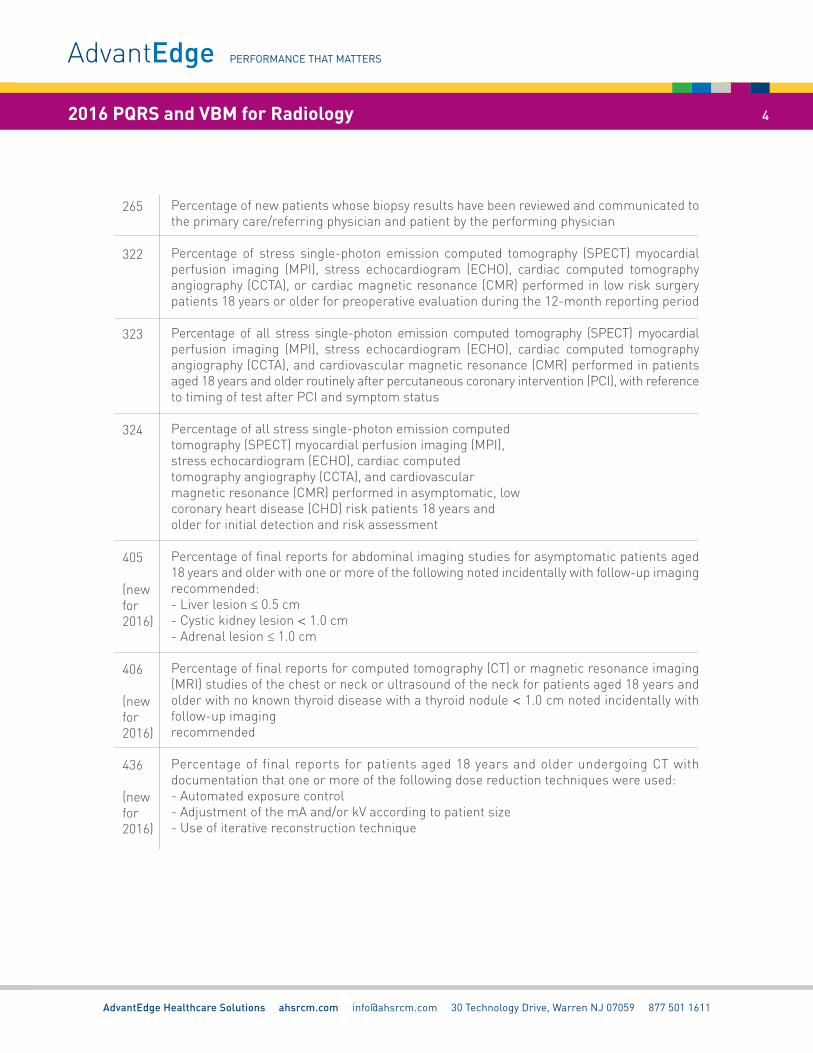
The2016PQRSmeasuresforDiagnosticRadiology,asidentifiedbytheACRareshownhere.Thelast3inthetablearenewfor2016.TheCMSlistforradiologywhichincludesmeasuresforInterventionalRadiologycanbefoundhere.Notethatthesearethepossiblemeasures,buteachEPandgroupneedstodeterminewhichapplytotheircircumstances:
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 3
Percentageoffinalreportsforproceduresusingfluoroscopythatdocumentradiationexposureindices,orexposuretimeandnumberoffluorographicimages(ifradiationexposureindicesarenotavailable)
Percentageoffinalreportsforscreeningmammogramsthatareclassifiedas“probablybenign”
NuclearMedicine:CorrelationwithExisting ImagingStudies forAllPatientsUndergoingBoneScintigraphy:Percentageoffinalreportsforallpatients,regardlessofage,undergoingbonescintigraphythatincludephysiciandocumentationofcorrelationwithexistingrelevantimagingstudies(e.g.,x-ray,MRI,CT,etc.)thatwereperformed
Percentageoffinalreportsforcarotid imagingstudies(neckmagneticresonanceangiography[MRA], neck computed tomographyangiography [CTA],neck duplexultrasound, carotidangiogram)performedthatincludedirectorindirectreferencetomeasurementsofdistalinternalcarotiddiameterasthedenominatorforstenosismeasurement
Percentageofpatientsundergoingascreeningmammogramwhoseinformationisenteredintoaremindersystemwithatargetduedateforthenextmammogram
265
322
323
324
405
(newfor2016)
406
(newfor2016)
436
(newfor2016)
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 4
Percentageofnewpatientswhosebiopsyresultshavebeenreviewedandcommunicatedtotheprimarycare/referringphysicianandpatientbytheperformingphysician
Percentage of stress single-photon emission computed tomography (SPECT) myocardialperfusion imaging (MPI), stress echocardiogram (ECHO), cardiac computed tomographyangiography(CCTA),orcardiacmagneticresonance(CMR)performedinlowrisksurgerypatients18yearsorolderforpreoperativeevaluationduringthe12-monthreportingperiod
Percentage of all stress single-photon emission computed tomography (SPECT) myocardialperfusion imaging (MPI), stress echocardiogram (ECHO), cardiac computed tomographyangiography(CCTA),andcardiovascularmagneticresonance(CMR)performedinpatientsaged18yearsandolderroutinelyafterpercutaneouscoronaryintervention(PCI),withreferencetotimingoftestafterPCIandsymptomstatus
Percentageofallstresssingle-photonemissioncomputedtomography(SPECT)myocardialperfusionimaging(MPI),stressechocardiogram(ECHO),cardiaccomputedtomographyangiography(CCTA),andcardiovascularmagneticresonance(CMR)performedinasymptomatic,lowcoronaryheartdisease(CHD)riskpatients18yearsandolderforinitialdetectionandriskassessment
Percentageoffinalreportsforabdominalimagingstudiesforasymptomaticpatientsaged18yearsandolderwithoneormoreofthefollowingnotedincidentallywithfollow-upimagingrecommended:-Liverlesion≤0.5cm-Cystickidneylesion<1.0cm-Adrenallesion≤1.0cm
Percentageoffinalreportsforcomputedtomography(CT)ormagneticresonanceimaging(MRI)studiesofthechestorneckorultrasoundoftheneckforpatientsaged18yearsandolderwithnoknownthyroiddiseasewithathyroidnodule<1.0cmnotedincidentallywithfollow-upimagingrecommended
Percentageof finalreportsforpatientsaged18yearsandolderundergoingCTwithdocumentationthatoneormoreofthefollowingdosereductiontechniqueswereused:-Automatedexposurecontrol-AdjustmentofthemAand/orkVaccordingtopatientsize-Useofiterativereconstructiontechnique
AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
Inaddition,groupsusingQCDRreportinghavetheoptionof“measuresgroup”reporting.Itrequiresreporting for20patients, themajorityofwhichareMedicare.The“OptimizingPatientExposure toIonizingRadiation”istheonlymeasuresgroupthatappliestoRadiologyfor2016.Itcontains:
-#359 Optimizing Patient Exposure to Ionizing Radiation: Utilization of a StandardizedNomenclatureforComputedTomography(CT)ImagingDescription
-#360OptimizingPatientExposuretoIonizingRadiation:CountofPotentialHighDoseRadiationImagingStudies:ComputedTomography(CT)andCardiacNuclearMedicineStudies
-#361OptimizingPatientExposure to IonizingRadiation:Reporting toaRadiationDoseIndexRegistry
-#362OptimizingPatientExposuretoIonizingRadiation:ComputedTomography(CT)ImagesAvailableforPatientFollow-upandComparisonPurposes
-#363OptimizingPatientExposuretoIonizingRadiation:SearchforPriorComputedTomography(CT)StudiesThroughaSecure,Authorized,Media-Free,SharedArchive
-#364OptimizingPatientExposuretoIonizingRadiation:Appropriateness:Follow-upCTImagingforIncidentallyDetectedPulmonaryNodulesAccordingtoRecommendedGuidelines
DetailsforeachmeasureareavailableintheCMSIndividualMeasuresGuide,availableasadownloadatthisCMS page.
VALUE-BASEDPAYMENTMODIFIER(VBM)
LikePQRS,theValue-BasedModifier(VBM)affectsMedicarepaymentswithaone-yeardelay.Hence,performancein2015hasalreadydeterminedPQRSandVBMpaymentadjustmentsfor2017.Andperformanceduringthisyear(2016)willdetermineadjustmentsfor2018payments.
For2015,CMSdescribedtheVBMasfollows:“Inordertobeeligibleforupward,downward,orneutralpaymentadjustmentsundertheValueModifierquality-tieringmethodologyandtoavoidanautomaticnegative twopercent (“-2.0%”) (forphysiciangroupswithbetween2 to9EPsandphysiciansolopractitioners) or negative four percent (“-4.0%”) (for physician groups with 10 or more EPs) ValueModifierpaymentadjustmentinCY2017,EPsingroupsandsolopractitionersMUSTparticipateinthePQRSandsatisfyreportingrequirementsasagrouporasindividualsinCY2015.Quality-tieringismandatoryforgroupsandsolopractitionerssubjecttotheValueModifierinCY2017.Groupswith10ormoreEPsaresubjecttoupward,neutral,ordownwardadjustmentunderquality-tiering,andgroupswithbetween2to9EPsandphysiciansolopractitionersaresubjecttoonlyupwardorneutraladjustmentunderquality-tieringin2017.”
Whilethepreciserulesfor2016arenotclearontheCMSwebsite,itappearsthatgroupsunder10providersarenowsubjecttoa-2%VBMpenalty,andcontinuetobeeligiblefora+2xincentive,basedontheirqualityandcostresults.ButthisassumesthatthegroupreportsitsPQRSmeasures.Anygroupunder10providersthatdoesnotreportPQRSsuccessfullywilldefinitelyseea-4%penalty.
Inaddition,for2016,non-physicianpractitioners(NPPs)areincludedintheVBM:PAs,NPs,etc.Asinpreviousyears,theseprovidersnewtotheprogramarenotsubjecttodownwardadjustments,but
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 5

AdvantEdge Healthcare Solutions ahsrcm.com [email protected] 30 Technology Drive, Warren NJ 07059 877 501 1611
thatappliesonlytosoloNPPsorthoseinagroupofonlyNPPs.Solophysiciansandgroupsoftwoormorephysiciansand/orNPPsaresubjecttopaymentadjustments(upordown)basedontheirratioofqualitytocostascomparedtootherprovidersintheMedicareprogram.
Tosummarize,theupwardordownwardpaymentadjustmentfactorsandpercentagesfor2016VBMareasfollows: -Forsolophysiciansandgroupsuptonineproviders:+2.0xand-2.0%. -Forgroupswith10ormoreproviders:+4.0xand-4.0%.
PERFORMANCE THAT MATTERS
2016 PQRS and VBM for Radiology 6


















