2016 Benefit Guide CBEBC - Louise ISD Version
58
COASTAL BEND EMPLOYEE BENEFITS COOPERATIVE EFFECTIVE: 09/01/2016 - 08/31/2017 BENEFIT GUIDE www.cbebc.com 1
description
Â
Transcript of 2016 Benefit Guide CBEBC - Louise ISD Version

COASTAL BEND EMPLOYEE BENEFITS COOPERATIVE
EFFECTIVE:
09/01/2016 - 08/31/2017
BENEFIT GUIDE
www.cbebc.com
1

Benefit Contact Information 3 How to Enroll 4-5 Annual Benefit Enrollment 6-11 1. Benefit Updates 6 2. Section 125 Cafeteria Plan Guidelines 7 3. Annual Enrollment 8 4. Eligibility Requirements 9 5. Helpful Definitions 10 6. Health Savings Account (HSA) vs. Flexible
Spending Account (FSA) 11
MDLIVE Telehealth 12-13 APL MEDlink® Medical Supplement 14-17 APL Accident 18-21 Cigna Dental 22-25 Superior Vision 26-27 Lincoln Financial Short Term Disability 28-29 Lincoln Financial Long Term Disability 30-31 APL Cancer 32-35 Texas Life Individual Life 36-37 UNUM Life and AD&D 38-41 Voya Critical Illness 42-45 HSA Bank Health Savings Account (HSA) 46-49 NBS Flexible Spending Account (FSA) 50-53 ID Watchdog Identity Theft 54-55
Table of Contents
HOW TO ENROLL
PG. 4
YOUR BENEFIT UPDATES: WHAT’S NEW
PG. 6
YOUR BENEFITS PACKAGE
PG. 12
FLIP TO...
2

Benefit Contact Information
CBEBC BENEFITS VISION CRITICAL ILLNESS
Financial Benefit Services (800) 583-6908 http://www.cbebc.com
Group # 28836 Superior Vision (800) 507-3800 https://www.superiorvision.com/
Voya (888) 238-4840 http://www.voya.com
TELEHEALTH DISABILITY HEALTH SAVINGS ACCOUNT
MDLIVE (888) 365-1663 http://www.consultmdlive.com
Lincoln Financial (800) 423-2765 http://www.lincolnfinancial.com
HSA Bank (800) 357-6246 http://www.hsabank.com
MEDICAL SUPPLEMENT—MEDLINK ® CANCER FLEXIBLE SPENDING ACCOUNT
Group # 13254 American Public Life (800) 256-8606 http://www.ampublic.com
Group # 13254 American Public Life (800) 256-8606 http://www.ampublic.com
National Benefit Services (800) 274-0503 http://www.nbsbenefits.com
ACCIDENT INDIVIDUAL LIFE IDENTITY THEFT
Group # 13254 American Public Life (800) 256-8606 http://www.ampublic.com
Texas Life (800) 283-9233 http://www.texaslife.com
ID Watchdog (800) 237-1521 http://www.idwatchdog.com
DENTAL LIFE AND AD&D MEDICAL
Group # 3335865 Cigna (800) 244-6224 http://www.cigna.com
UNUM (800) 858-6843 http://www.unum.com
Aetna (800) 222-9205 http://www.trsactivecareaetna.com
Benefit Contact Information
3

!
How to Enroll
On Your Computer Access the CBEBC benefits website
from your computer, tablet or
smartphone!
Our online benefit enrollment
platform provides a simple and
easy to navigate process. Enroll
at your own pace, whether at
home or at work.
www.cbebc.com delivers
important benefit information
with 24/7 access, as well as
detailed plan information, rates
and product videos.
On Your Device
Enrollment has just become
easier!
Avoid typing long URLs and scan
directly to your benefits websites,
videos, and benefit guides.
Try it yourself! Scan the following
code in the picture.
SCAN:
4

GO www.cbebc.com 1
2
Login Steps
3
Go to:
Click Login
Enter Username & Password
OR SCAN
All login credentials have been RESET to the default
described below:
Username:
The first six (6) characters of your last name, followed
by the first letter of your first name, followed by the
last four (4) digits of your Social Security Number.
If you have six (6) or less characters in your last name,
use your full last name, followed by the first letter of
your first name, followed by the last four (4) digits of
your Social Security Number.
Default Password:
Last Name* (lowercase, excluding punctuation)
followed by the last four (4) digits of your Social
Security Number.
Sample Password
l incola1234
l incoln1234
If you have trouble
logging in, click on the
“Login Help Video”
for assistance.
Click on “Enrollment Instructions” for more information about how to enroll.
Sample Username
LOGIN
Open Enrollment Tip
For your User ID: If you have less than six (6) characters in your last
name, use your full last name, followed by the first letter of your first
name, followed by the last four (4) digits of your Social Security Number.
5

SUMMARY PAGES
Annual Benefit Enrollment
Due to the Affordable Care Act (ACA), every employee is required to login & complete the enrollment process, even if you are declining benefits
Social Security Numbers for your dependents are
required regardless if they are enrolled in coverage or not. Please make sure you have these items on hand when going through your open enrollment.
NEW– Critical Illness by Voya CHANGE– Vision by Superior now offers frames every
12 months instead of 24 beginning the 2016-2017 plan year.
CHANGE– Dental by Cigna now includes Cigna Dental
Wellness Plan– when you or your family members receive any preventive care in one plan year, the annual dollar maximum will increase in the following plan year.
Telehealth services allow you the ability to save on
out-of-pocket expenses and will reduce time away from your work and your family. Please remember to utilize your Telehealth services for minor medical needs.
Medical, HSA, & FSA elections will NOT be enrolled until the August enrollment for the 2016-2017 plan year.
Please remember, in order to maximize insurance
coverage and reduce out of pocket expenses you should utilize In-Network providers for both your Dental and Vision benefits.
Benefit elections will become effective 9/1/2016
(elections requiring evidence of insurability, such as life Insurance, may have a later effective date, if approved). After annual enrollment closes, benefit changes can only be made if you experience a qualifying event (and changes must be made within 30 days of event).
Benefit Updates - What’s New:
Enrollment assistance is available by calling Financial Benefit Services at (800) 583-6908 to
speak to a representative.
Please be sure to update your profile information (home address, phone numbers, email).
August 2016 enrollment for medical elections is mandatory due to the Affordable Care Act
(ACA).
6

SUMMARY PAGES
CHANGES IN STATUS (CIS):
QUALIFYING EVENTS
Marital Status A change in marital status includes marriage, death of a spouse, divorce or annulment (legal separation is not recognized in all states).
Change in Number of Tax Dependents
A change in number of dependents includes the following: birth, adoption and placement for adoption. You can add existing dependents not previously enrolled whenever a dependent gains eligibility as a result of a valid change in status event.
Change in Status of Employment Affecting
Coverage Eligibility
Change in employment status of the employee, or a spouse or dependent of the employee, that affects the individual's eligibility under an employer's plan includes commencement or termination of employment.
Gain/Loss of Dependents' Eligibility Status
An event that causes an employee's dependent to satisfy or cease to satisfy coverage requirements under an employer's plan may include change in age, student, marital, employment or tax dependent status.
Judgment/Decree/Order
If a judgment, decree, or order from a divorce, annulment or change in legal custody requires that you provide accident or health coverage for your dependent child (including a foster child who is your dependent), you may change your election to provide coverage for the dependent child. If the order requires that another individual (including your spouse and former spouse) covers the dependent child and provides coverage under that individual's plan, you may change your election to revoke coverage only for that dependent child and only if the other individual actually provides the coverage.
Eligibility for Government Programs
Gain or loss of Medicare/Medicaid coverage may trigger a permitted election change.
A Cafeteria plan enables you to save money by using pre-tax dollars to pay for eligible group insurance premiums sponsored and offered by your employer. Enrollment is automatic unless you decline this benefit. Elections made during annual enrollment will become effective on the plan effective date and will remain in effect during the entire plan year.
Changes in benefit elections can occur only if you experience a qualifying event. You must present proof of a qualifying event to your Benefit Office within 30 days of your qualifying event and meet with your Benefit/HR Office to complete and sign the necessary paperwork in order to make a benefit election change. Benefit changes must be consistent with the qualifying event.
Section 125 Cafeteria Plan Guidelines
7

Annual Enrollment
During your annual enrollment period, you have the opportunity
to review, change or continue benefit elections each year.
Changes are not permitted during the plan year (outside of
annual enrollment) unless a Section 125 qualifying event occurs.
Changes, additions or drops may be made only during the
annual enrollment period without a qualifying event.
Employees must review their personal information and verify
that dependents they wish to provide coverage for are
included in the dependent profile. Additionally, you must
notify your employer of any discrepancy in personal and/or
benefit information.
Employees must confirm on each benefit screen (medical,
dental, vision, etc.) that each dependent to be covered is
selected in order to be included in the coverage for that
particular benefit.
New Hire Enrollment
All new hire enrollment elections must be completed in the
online enrollment system within the first 31 days of benefit
eligibility employment. Failure to complete elections during this
timeframe will result in the forfeiture of coverage.
Q&A
Who do I contact with Questions?
For supplemental benefit questions, you can contact your
Benefits/HR department or you can call Financial Benefit Services
at 866-914-5202 for assistance.
Where can I find forms?
For benefit summaries and claim forms, go to your school
district’s benefit website:
www.cbebc.com. Click on the benefit plan you need
information on (i.e., Dental) and you can find the forms you
need under the Benefits and Forms section.
How can I find a Network Provider?
For benefit summaries and claim forms, go to the CBEBC
benefit website: www.cbebc.com. Click on your school
district, then click on the benefit plan you need information
on (i.e., Dental) and you can find provider search links under
the Quick Links section.
When will I receive ID cards?
If the insurance carrier provides ID cards, you can expect to
receive those 3-4 weeks after your effective date. For most
dental and vision plans, you can login to the carrier website
and print a temporary ID card or simply give your provider the
insurance company’s phone number and they can call and
verify your coverage if you do not have an ID card at that
time. If you do not receive your ID card, you can call the
carrier’s customer service number to request another card.
SUMMARY PAGES
8
SUMMARY PAGES
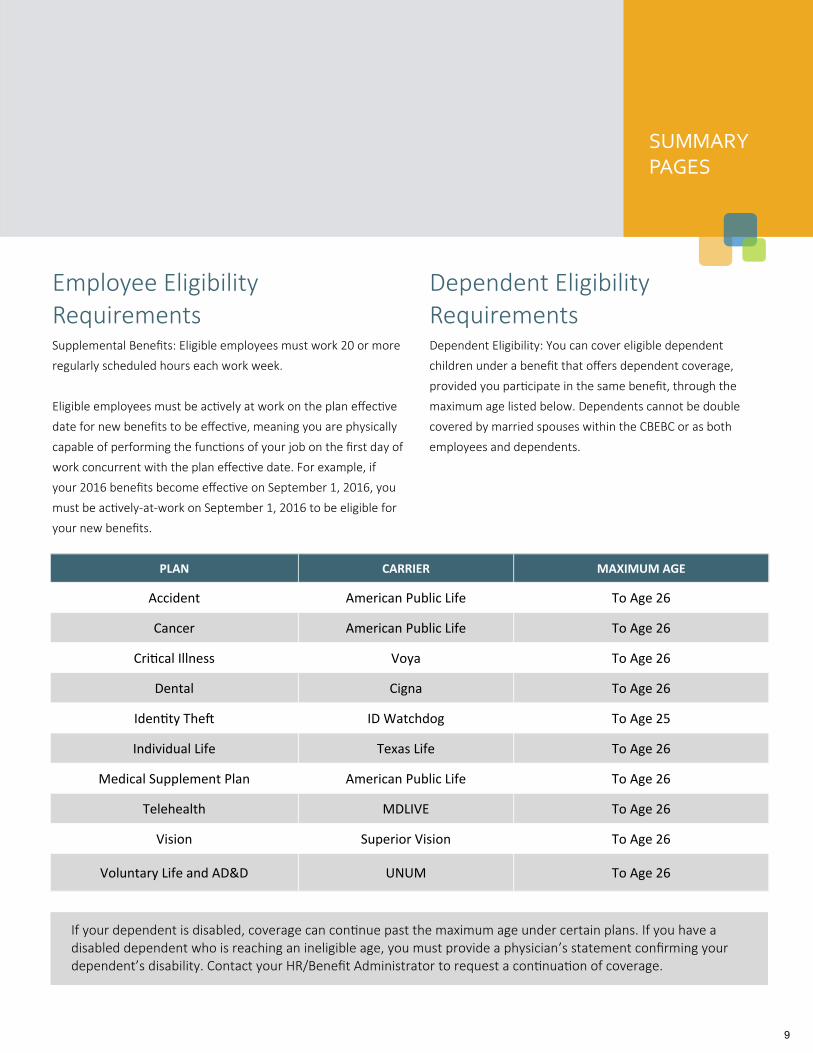
PLAN CARRIER MAXIMUM AGE
Accident American Public Life To Age 26
Cancer American Public Life To Age 26
Critical Illness Voya To Age 26
Dental Cigna To Age 26
Identity Theft ID Watchdog To Age 25
Individual Life Texas Life To Age 26
Medical Supplement Plan American Public Life To Age 26
Telehealth MDLIVE To Age 26
Vision Superior Vision To Age 26
Voluntary Life and AD&D UNUM To Age 26
Employee Eligibility Requirements
Supplemental Benefits: Eligible employees must work 20 or more
regularly scheduled hours each work week.
Eligible employees must be actively at work on the plan effective
date for new benefits to be effective, meaning you are physically
capable of performing the functions of your job on the first day of
work concurrent with the plan effective date. For example, if
your 2016 benefits become effective on September 1, 2016, you
must be actively-at-work on September 1, 2016 to be eligible for
your new benefits.
Dependent Eligibility Requirements
Dependent Eligibility: You can cover eligible dependent
children under a benefit that offers dependent coverage,
provided you participate in the same benefit, through the
maximum age listed below. Dependents cannot be double
covered by married spouses within the CBEBC or as both
employees and dependents.
If your dependent is disabled, coverage can continue past the maximum age under certain plans. If you have a disabled dependent who is reaching an ineligible age, you must provide a physician’s statement confirming your dependent’s disability. Contact your HR/Benefit Administrator to request a continuation of coverage.
9

Actively at Work You are performing your regular occupation for the employer
on a full-time basis, either at one of the employer’s usual
places of business or at some location to which the employer’s
business requires you to travel. If you will not be actively at
work beginning 9/1/2016 please notify your benefits
administrator.
Annual Enrollment The period during which existing employees are given the
opportunity to enroll in or change their current elections.
Annual Deductible The amount you pay each plan year before the plan begins to
pay covered expenses.
Calendar Year January 1st through December 31st
Co-insurance After any applicable deductible, your share of the cost of a
covered health care service, calculated as a percentage (for
example, 20%) of the allowed amount for the service.
Guaranteed Coverage The amount of coverage you can elect without answering any
medical questions or taking a health exam. Guaranteed
coverage is only available during initial eligibility period.
Actively-at-work and/or pre-existing condition exclusion
provisions do apply, as applicable by carrier.
In-Network Doctors, hospitals, optometrists, dentists and other providers
who have contracted with the plan as a network provider.
Out of Pocket Maximum The most an eligible or insured person can pay in co-insurance
for covered expenses.
Plan Year September 1st through August 31st
Pre-Existing Conditions Applies to any illness, injury or condition for which the
participant has been under the care of a health care provider,
taken prescriptions drugs or is under a health care provider’s
orders to take drugs, or received medical care or services
(including diagnostic and/or consultation services).
Helpful Definitions SUMMARY PAGES
10
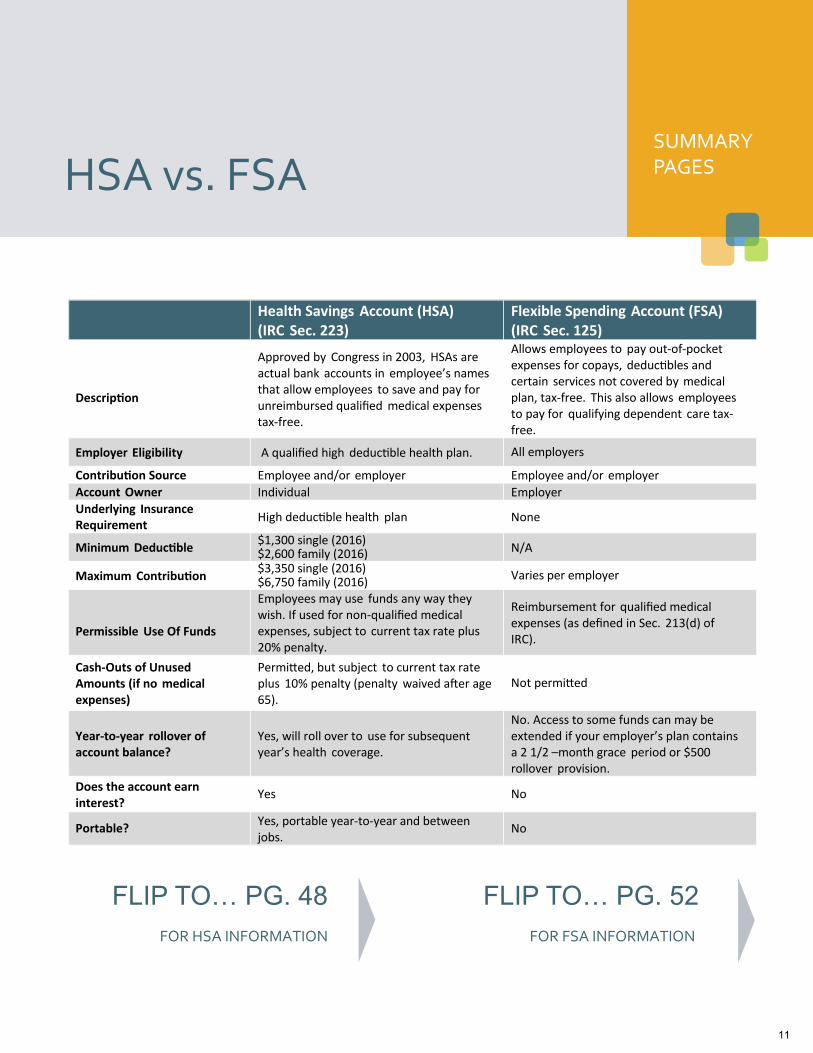
SUMMARY PAGES HSA vs. FSA
Health Savings Account (HSA) (IRC Sec. 223)
Flexible Spending Account (FSA) (IRC Sec. 125)
Description
Approved by Congress in 2003, HSAs are actual bank accounts in employee’s names that allow employees to save and pay for unreimbursed qualified medical expenses tax-free.
Allows employees to pay out-of-pocket expenses for copays, deductibles and certain services not covered by medical plan, tax-free. This also allows employees to pay for qualifying dependent care tax-free.
Employer Eligibility A qualified high deductible health plan. All employers
Contribution Source Employee and/or employer Employee and/or employer
Account Owner Individual Employer
Underlying Insurance Requirement
High deductible health plan None
Minimum Deductible $1,300 single (2016) $2,600 family (2016) N/A
Maximum Contribution $3,350 single (2016) $6,750 family (2016)
Varies per employer
Permissible Use Of Funds
Employees may use funds any way they wish. If used for non-qualified medical expenses, subject to current tax rate plus 20% penalty.
Reimbursement for qualified medical expenses (as defined in Sec. 213(d) of IRC).
Cash-Outs of Unused Amounts (if no medical expenses)
Permitted, but subject to current tax rate plus 10% penalty (penalty waived after age 65).
Not permitted
Year-to-year rollover of account balance?
Yes, will roll over to use for subsequent year’s health coverage.
No. Access to some funds can may be extended if your employer’s plan contains a 2 1/2 –month grace period or $500 rollover provision.
Does the account earn interest?
Yes No
Portable? Yes, portable year-to-year and between jobs.
No
FOR HSA INFORMATION
FLIP TO… PG. 48
FOR FSA INFORMATION
FLIP TO… PG. 52
11
Telehealth provides 24/7/365 access to board-certified doctors via telephone consultations that can diagnose, recommend treatment and prescribe medication. Whether you are at home, traveling or at work, Telehealth makes care more convenient and accessible for non-emergency care when your primary care physician is not available.
About this Benefit
Telehealth YOUR BENEFITS PACKAGE
DID YOU KNOW?
75%
of all doctor, urgent care, and ER visits could be handled safely and effectively via
telehealth.
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
MDLIVE
12
Telehealth
When should I use MDLIVE? If you’re considering the ER or urgent care for a non-
emergency medical issue
Your primary care physician is not available
At home, traveling, or at work
24/7/365, even holidays!
What can be treated? Allergies
Asthma
Bronchitis
Cold and Flu
Ear Infections
Joint Aches and Pain
Respiratory Infection
Sinus Problems
And More!
Pediatric Care related to: Cold & Flu
Constipation
Ear Infection
Fever
Nausea & Vomiting
Pink Eye
And More!
Who are our doctors? MDLIVE has the nation’s largest network of telehealth doctors. On average, our doctors have 15 years of experience practicing medicine and are licensed in the state where patients are located. Their specialties include primary care, pediatrics, emergency medicine and family medicine. Our doctors are committed to providing convenient, quality care and are always ready to take your call.
Are children eligible? Yes. MDLIVE has local pediatricians on-call 24/7/365. Please note, a parent or guardian must be present during any interactions involving minors. We ask parents to establish a child record under their account. Parents must be present on each call for children 18 or younger.
How much does it cost? $8 for Employee Only. $16 for Family. One cost covers entire family with unlimited phone consultations.
Download the App Doctor visits are easier and more convenient with the MDLIVE App. Be prepared. Download today. www.mdlive.com/getapp
Access to a doctor anywhere: at home, at work, or on the go
Choose doctors from one of the nation's largest telehealth networks
Available 24/7 by video or phone
Private, secure and confidential visits
Connect instantly with MDLIVE Assist
Disclaimers: MDLIVE does not replace the primary care physician. MDLIVE operates subject to state regulation and may not be available in certain states. MDLIVE does not guarantee that a prescription will be written. MDLIVE does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. MDLIVE physicians reserve the right to deny care for potential misuse of services. For complete terms of use visit www.mdlive.com/pages/terms.html 010113
Call us at (888) 365-1663 or visit us at www.consultmdlive.com
Scan with your smartphone to get the app.
13
MEDlink® is designed to help supplement your Employer's major medical plan. This plan provides supplemental coverage to help offset out-of-pocket costs that you may experience due to deductibles, co-payments and coinsurance of your medical plan.
About this Benefit
MEDlink® YOUR
BENEFITS
DID YOU KNOW?
33%
of total healthcare costs are paid
out-of-pocket.
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
AMERICAN PUBLIC LIFE
14

SUMMARY OF BENEFITS
Base Policy Option 1 Option 2
In-Hospital Benefit - Maximum In-Hospital Benefit $1,500 per confinement $2,500 per confinement
Outpatient Benefit up to $200 per treatment up to $200 per treatment
Physician Outpatient Treatment Benefit $25 per treatment; $125 max per family per Calendar Year
$25 per treatment; $125 max per family per Calendar Year
Option 1 Total Monthly Premiums by Plan*
Issue Ages 17-54 Issue Ages 55-59 Issue Ages 60-69
Employee Only $21.50 $32.00 $49.00
Employee + Spouse $39.50 $59.00 $88.00
Employee + Child(ren) $36.50 $47.00 $64.00
Family Coverage $54.50 $74.00 $103.00
Option 2 Total Monthly Premiums by Plan*
Hospital Emergency Room Issue Ages 17-54 Issue Ages 55-59 Issue Ages 60-69
Employee Only $28.00 $44.50 $68.50
Employee + Spouse $51.50 $81.50 $122.50
Employee + Child(ren) $45.50 $62.00 $86.00
Family Coverage $69.00 $99.00 $140.00
Plans available to employees age 70 and over if You work for an employer employing 20 or more employees on a typical workday in the preceding
Calendar Year.
*Total premium includes the Plan selected and any applicable rider premium. Premiums are subject to increase with notice.
Limitations Eligibility This policy will be issued to those persons who meet American Public Life Insurance Company’s insurability requirements. Evidence of insurability acceptable to us may be required. If our underwriting rules are met, you are on active service, you are covered under your Employer’s Medical Plan and premium has been paid, your insurance will take effect on the requested Effective Date or the Effective Date assigned by us upon approval of your written application, whichever is later.
Covered Charges mean those charges that are incurred by a Covered Person because of an Accident or Sickness; are for necessary treatment, services and medical supplies and recommended by a Physician; are not more than any dollar limit set forth in the Schedule; are incurred while insured under the Policy, subject to any Extension of Benefits; and are not excluded under the Policy.
A Hospital is not any institution used as a place for rehabilitation; a place for rest, or for the aged; a nursing or convalescent home; a long term nursing unit or geriatrics ward; or an extended care facility for the care of convalescent, rehabilitative or ambulatory patients.
In-Hospital Benefit Benefits payable are limited to any out-of-pocket deductible amount; any out-of-pocket co-payment or coinsurance amounts the Covered Person actually incurs after the Employer’s Medical Plan has paid; any out-of-pocket amount the Covered Person actually incurs for surgery performed by a Physician after the Employer’s Medical Plan has paid; and the Maximum In-Hospital Benefit shown in the Policy Schedule. The Covered Person must be an Inpatient and covered by your Employer’s Medical Plan when the Covered Charges are incurred.
Outpatient Benefits Treatment is for the same or related conditions, unless separated by a period of 90 consecutive days. After 90 consecutive days, a new Outpatient Benefit will be payable. The Covered Person must be covered by your Employer’s Medical Plan when the Covered Charges are incurred.
Physician Outpatient Treatment Benefit Benefit maximum of $125 per family per Calendar Year. The Covered Person must be covered by your Employer’s Medical Plan when the Covered Charges are incurred. The Covered Person must not be an Inpatient when the Covered Charges are incurred.
APSB-22330(TX)-0116 MGM/FBS CBEBC
MEDlink® Limited Benefit Medical Expense Supplemental Insurance
THE POLICY UNDER WHICH THIS CERTIFICATE IS ISSUED IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. THE EMPLOYER DOES NOT BECOME A
SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM BY PURCHASING THE POLICY AND IF THE EMPLOYER IS A NON-SUBSCRIBER, THE EMPLOYEE LOSES
THOSE BENEFITS WHICH WOULD OTHERWISE ACCRUE UNDER THE WORKERS’ COMPENSATION LAWS. THE EMPLOYER MUST COMPLY WITH THE WORKERS’
COMPENSATION LAW AS IT PERTAINS TO NON-SUBSCRIBERS AND THE REQUIRED NOTIFICATIONS THAT MUST BE FILED AND POSTED.
CBEBC
15

Premiums The premium rates may be changed by Us. If the rates are changed, We will give You at least 31 days advance written notice. If a change in benefits increases Our liability, premium rates may be changed on the date Our liability is increased.
This plan may be continued in accordance with the Consolidated Omnibus Reconciliation Act of 1986.
Exclusions We will pay no benefits for any expenses incurred during any period the Covered Person does not have coverage under your Employer’s Medical Plan, except as provided in the Absence of your Employer’s Medical Plan provision or which result from: (a) suicide or any attempt, thereof, while sane or insane; (b) any intentionally self-inflicted injury or Sickness; (c) rest care or rehabilitative care and treatment; (d) outpatient routine newborn care; (e) voluntary abortion except, with respect to You or Your covered
Dependent spouse: (1) where Your or Your Dependent spouse’s life would be
endangered if the fetus were carried to term; or (2) where medical complications have arisen from abortion;
(f) pregnancy of a Dependent child; (g) participation in a riot, civil commotion, civil disobedience, or
unlawful assembly. This does not include a loss which occurs while acting in a lawful manner within the scope of authority;
(h) commission of a felony; (i) participation in a contest of speed in power driven vehicles,
parachuting, or hang gliding; (j) air travel, except:
(1) as a fare-paying passenger on a commercial airline on a regularly scheduled route; or
(2) as a passenger for transportation only and not as a pilot or crew member;
(k) intoxication; (Whether or not a person is intoxicated is determined and defined by the laws and jurisdiction of the geographical area in which the loss occurred.)
(l) alcoholism or drug use, unless such drugs were taken on the advice of a Physician and taken as prescribed;
(m) sex changes; (n) experimental treatment, drugs, or surgery; (o) an act of war, whether declared or undeclared, or while
performing police duty as a member of any military or naval organization; (This exclusion includes Accident sustained or Sickness contracted while in the service of any military, naval, or air force of any country engaged in war. We will refund the pro rata unearned premium for any such period the Covered Person is not covered.)
(p) Accident or Sickness arising out of and in the course of any occupation for compensation, wage or profit; (This does not apply to those sole proprietors or partners not covered by Workers’ Compensation.)
(q) mental illness or functional or organic nervous disorders, regardless of the cause;
(r) dental or vision services, including treatment, surgery, extractions, or x-rays, unless: (1) resulting from an Accident occurring while the Covered
Person’s coverage is in force and if performed within 12 months of the date of such Accident; or
(2) due to congenital disease or anomaly of a covered newborn child.
(s) routine examinations, such as health exams, periodic check-ups, or routine physicals, except when part of Inpatient routine newborn care;
(t) any expense for which benefits are not payable under the Covered Person’s Employer’s Medical Plan; or
(u) air or ground ambulance.
Termination of Coverage Your Insurance coverage will end on the earliest of these dates: the date You no longer qualify as an Insured; the end of the last period for which premium has been paid; the date the Policy is discontinued; the date You retire; if You work for an employer employing less than 20 employees on a typical work day in the preceding Calendar Year, the date You attain age 70; the date You cease to be on Active Service; the date Your coverage under Another Medical Plan ends; or the date You cease employment with the employer through whom You originally became insured under the Policy.
Insurance coverage on a Dependent will end on the earliest of these dates: the date Your coverage terminates; the end of the last period for which premium has been paid; the date the Dependent no longer meets the definition of Dependent; the date the Dependent’s coverage under Another Medical Plan ends; or the date the Policy is modified so as to exclude Dependent coverage.
We may end the coverage of any Covered Person who submits a fraudulent claim.
We may end the coverage of a Subscribing Unit if fewer persons are insured than the Policyholder’s application requires.
MEDlink® Limited Benefit Medical Expense Supplemental Insurance
Underwritten by American Public Life Insurance Company. This is a brief description of the coverage. For complete benefits, limitations, exclusions and other provisions, please refer to the policy and riders. This coverage does not replace Workers’ Compensation Insurance. This product is inappropriate for people who are eligible for Medicaid coverage. | This policy is considered an employee welfare benefit plan established and/or maintained by an association or employer intended to be covered by ERISA, and will be administered and enforced under ERISA. Group policies issued to governmental entities and municipalities may be exempt from ERISA guidelines. | Policy Form MEDlink® Series | Texas | Limited Benefit Medical Expense Supplemental Insurance | (10/14) | CBEBC
APSB-22330(TX)-0116 MGM/FBS CBEBC
2305 Lakeland Drive | Flowood, MS 39232
ampublic.com | 800.256.8606
16

MEDlink® Limited Benefit Medical Expense Supplemental Insurance
17

Accident insurance is designed to supplement your medical insurance coverage by covering indirect costs that can arise with a serious, or a not-so-serious, injury. Accident coverage is low cost protection available to you and your family without evidence of insurability.
About this Benefit
Accident YOUR
BENEFITS
of disabling injuries
suffered by American
workers are not work
related.
DID YOU KNOW?
36% of American workers
report they always or
usually live paycheck
to paycheck.
2/3
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan
details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
AMERICAN PUBLIC LIFE
18

APSB-22329 (TX) MGM/FBS CBEBC
A-3 Supplemental Limited Benefit Accident Expense Insurance CBEBC
SUMMARY OF BENEFITSBenefit Description Level 1 - 1 Unit Level 2 - 2 Units
Accidental Death - per unit $5,000 $10,000Medical Expense Accidental Injury Benefit - per unit
actual charges up to $500 actual charges up to $1,000
Daily Hospital Confinement Benefit $75 per day $150 per dayAir and Ground Ambulance Benefit actual charges up to $1,250 actual charges up to $2,500Accidental Dismemberment Benefit Single finger or toe Multiple fingers or toes Single hand, arm, foot or leg Multiple hands, arms, feet or legs
$500$500
$2,500$5,000
$1,000$1,000$5,000
$10,000Accidental Loss of Sight Benefit - per unit Loss of Sight in one eye Loss of Sight in both eyes
$2,500$5,000
$5,000$10,000
THE POLICY UNDER WHICH THIS CERTIFICATE IS ISSUED IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. THE EMPLOYER DOES NOT BECOME A SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM BY PURCHASING THE POLICY AND IF THE EMPLOYER IS A NON-SUBSCRIBER, THE EMPLOYEE LOSES THOSE BENEFITS WHICH WOULD OTHERWISE ACCRUE UNDER THE WORKERS’ COMPENSATION LAWS. THE EMPLOYER MUST COMPLY WITH THE WORKERS’ COMPENSATION LAW AS IT PERTAINS TO NON-SUBSCRIBERS AND THE REQUIRED NOTIFICATIONS THAT MUST BE FILED AND POSTED.
Total Monthly Premiums by Plan*Individual Individual & Spouse 1 Parent Family 2 Parent Family
Level 1 - 1 Unit $10.80 $19.40 $21.20 $29.80Level 2 - 2 Units $17.10 $29.80 $34.90 $47.60
*Total premium includes the Plan selected and any applicable rider premium. Premiums are subject to increase with notice.The premium and amount of benefits vary dependent upon the Plan selected at time of application.
Limitations and ExclusionsEligibilityThis policy will be issued to only those persons who meet American Public Life Insurance Company’s insurability requirements. Persons not meeting APL’s insurability requirements will be excluded from coverage by an endorsement attached to the policy.
Base PolicyNo benefits are payable for a pre-existing condition. Pre-existing condition means an Injury that pertains solely to an Accidental Bodily Injury which resulted from an accident sustained before the Effective Date of coverage. Pre-Existing Conditions specifically named or described as permanently excluded in any part of this contract are never covered.
A Hospital is not an institution which is primarily a place for alcoholics or drug addicts; the aged; a nursing, rest or convalescent nursing home; a mental institution or sanitarium; a facility contracted for or operated by the United States Government for treatment of members or ex-members of the armed forces (unless You are legally required to pay for services rendered in the absence of insurance); or, a long-term nursing unit or geriatrics ward.
Medical Expense Accidental Injury BenefitExpenses must commence within 60 days of the covered accident. The maximum benefit amount payable for any one accident for the Insured Person shall not exceed the Medical Expense Benefit.
Air and Ground Ambulance BenefitEmergency transportation must occur within 21 calendar days of the accident causing such Injury.
Daily Hospital Confinement BenefitThe maximum benefit period for this benefit is 30 days per covered accident.
Accidental DeathAccidental Death must result within 90 days of the covered accident causing the injury.
Accidental Dismemberment BenefitThe total amount payable for all Losses resulting from the same accident will not exceed the Maximum Dismemberment Benefit of $5,000 cumulative per unit, per Accident. Loss must be within 90 days of the accident causing such Injury.
19

APSB-22329 (TX) MGM/FBS CBEBC
Underwritten by American Public Life Insurance Compnay. This is a brief description of the coverage. For complete benefits, limitations, exclusions and other provisions, please refer to the policy. This coverage does not replace Workers’ Compensation Insurance. This product is inappropriate for people who are eligible for Medicaid coverage. | Policy Form A-3 Series | Texas | Supplemental Limited Benefit Accident Expense Insurance Policy | (10/14) | CBEBC
ExclusionsBenefits otherwise provided by this Policy will not be payable for services or expenses or any such Loss resulting from or in connection with:
(1) sickness, illness or bodily infirmity;(2) suicide, attempted suicide or intentional self-inflicted Injury,
whether sane or insane;(3) dental care or treatment unless due to accidental Injury to
natural teeth;(4) war or any act of war (whether declared or undeclared) or
participating in a riot or felony;(5) alcoholism or drug addiction;(6) travel or flight in or descent from any aircraft or device which
can fly above the earth’s surface in any capacity other than as a fare paying passenger on a regularly scheduled airline;
(7) Injury originating prior to the effective date of the Policy;(8) Injury occurring while intoxicated (Intoxication means that
which is determined and defined by the laws and jurisdiction of the geographical area in which the loss or cause of loss is incurred.);
(9) Voluntary inhalation of gas or fumes or taking of poison or asphyxiation;
(10) Voluntary ingestion or injection of any drug, narcotic or sedative, unless administered on the advice and taken in such doses as prescribed by a Physician;
(11) Injury sustained or sickness which first manifests itself while on full-time duty in the armed forces; (Upon notice, We will refund the proportion of unearned premium while in such forces.)
(12) Injury incurred while engaging in an illegal occupation;(13) Injury incurred while attempting to commit a felony or an assault;(14) Injury to a covered person while practicing for or being a part
of organized or competitive rodeo, sky diving, hang gliding, parachuting or scuba diving;
(15) driving in any race or speed test or while testing an automobile or any vehicle on any racetrack or speedway;
(16) hernia, carpal tunnel syndrome or any complication therefrom;
If You are entitled to benefits under this Policy as a result of sprained or lame back, or any intervertebral disk conditions, such benefits shall be payable for a maximum period of time, not exceeding in the aggregate three (3) months for any Injury.
Guaranteed Renewable You have the right to renew this Policy until the first premium due date on or after Your 69th birthday, if you pay the correct premium when due or within the Grace Period. When an Insured’s coverage terminates at age 70, coverage for other Insured Persons, if any, shall continue under this Policy. We have the right to change premium rates by class.
2305 Lakeland Drive | Flowood, MS 39232ampublic.com | 800.256.8606
20

A-3 Supplemental Limited Benefit Accident Expense Insurance
21

Dental insurance is a coverage that helps defray the costs of dental care. It insures against the expense of routine care, treatment and dental disease.
About this Benefit
Dental YOUR BENEFITS PACKAGE
Good dental care may improve your overall health.
Also Women with gum disease may be at greater risk of giving birth to a preterm or low birth weight baby.
DID YOU KNOW?
CIGNA
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 22

Dental PPO - High Option
Benefits Cigna Dental PPO - High Option
In-Network Out-of-Network
Network Total Cigna DPPO Calendar Year Maximum (Class I, II, and III expenses)
$1,500 $1,500
Annual Deductible Individual Family
$50 per person $150 per family
$50 per person $150 per family
Reimbursement Levels** Based on Reduced Contracted Fees
90th percentile of Reasonable and
Customary Allowances
Plan Pays You Pay Plan Pays You Pay
Class I - Preventive & Diagnostic Care Oral Exams Routine Cleanings Bitewing X-rays Full Mouth X-rays Panoramic X-ray Fluoride Application Sealants Emergency Care to Relieve Pain
100% No Charge 100% No Charge
Class II - Basic Restorative Care Fillings Root Canal Therapy/Endodontics Osseous Surgery Periodontal Scaling and Root Planing Surgical Extractions of Impacted Teeth Brush Biopsies Oral Surgery—All except simple extractions Oral Surgery—Simple extractions
80%* 20%* 80%* 20%*
Class III - Major Restorative Care Crowns Anesthetics Denture Repairs Denture Relines, Rebases and Adjustments Repairs to Bridges, Crowns and Inlays Dentures Bridges Inlays/Onlays Prosthesis Over Implant Space Maintainers
50%* 50%* 50%* 50%*
Class IV - Orthodontia Lifetime Maximum
50% $1,000
Dependent children to
age 19
50%
50% $1,000
Dependent children to
age 19
50%
Monthly PPO Premiums
Tier Rate
EE Only $30.50
EE + Spouse $58.66
EE + Child(ren) $60.28
Family Coverage $85.02
Missing Tooth Limitation – The amount payable is 50% of the amount otherwise payable until insured for 12 months; thereafter, considered a Class III expense. Pretreatment review is available on a voluntary basis when extensive dental work in excess of $200 is proposed. * Subject to annual deductible Dental Oral Health Integration Program (OHIP) - All dental customers = Clinical research shows an association between oral health and overall health. The Cigna Dental Oral Health Integration Program (OHIP)® is designed to provide enhanced dental coverage for customers with certain eligible medical conditions. Eligible conditions for the program include cardiovascular disease, cerebrovascular disease (stroke), diabetes, maternity, chronic kidney disease, organ transplants, and head and neck cancer radiation. The program provides:
100% coverage for certain dental procedures
guidance on behavioral issues related to oral health
discounts on prescription and non-prescription dental products For more information and to see the complete list of eligible conditions, go to www.mycigna.com or call customer service 24/7 at 1.800.CIGNA24. **For services provided by a Cigna Dental PPO network dentist, Cigna Dental will reimburse the dentist according to a Contracted Fee Schedule. For services provided by an out-of-network dentist, Cigna Dental will reimburse according to Reasonable and Customary Allowances but the dentist may balance bill up to their usual fees.
23

Dental PPO - Low Option
Benefits Cigna Dental PPO - Low Option
In-Network Out-of-Network
Network Total Cigna DPPO Calendar Year Maximum (Class I, II, and III expenses)
$1,000 $1,000
Annual Deductible Individual Family
$50 per person $150 per family
$50 per person $150 per family
Reimbursement Levels** Based on Reduced Contracted Fees
Based on Maximum Allowable Charge (In-
network fee level)
Plan Pays You Pay Plan Pays You Pay
Class I - Preventive & Diagnostic Care Oral Exams Routine Cleanings Bitewing X-rays Full Mouth X-rays Panoramic X-ray Fluoride Application Sealants Emergency Care to Relieve Pain
80% 20% 80% 20%
Class II - Basic Restorative Care Fillings Root Canal Therapy/Endodontics Osseous Surgery Periodontal Scaling and Root Planing Surgical Extractions of Impacted Teeth Brush Biopsies Oral Surgery—All except simple extractions Oral Surgery—Simple extractions
50%* 50%* 50%* 50%*
Class III - Major Restorative Care Crowns Anesthetics Denture Repairs Denture Relines, Rebases and Adjustments Repairs to Bridges, Crowns and Inlays Dentures Bridges Inlays/Onlays Prosthesis Over Implant Space Maintainers
25%* 75%* 25%* 75%*
Class IV - Orthodontia Lifetime Maximum
50% $1,000
Dependent children to
age 19
50%
50% $1,000
Dependent children to
age 19
50%
Monthly PPO Premiums
Tier Rate
EE Only $16.50
EE + Spouse $32.98
EE + Child(ren) $36.22
Family Coverage $52.72
Missing Tooth Limitation – The amount payable is 50% of the amount otherwise payable until insured for 12 months; thereafter, considered a Class III expense. Pretreatment review is available on a voluntary basis when extensive dental work in excess of $200 is proposed. * Subject to annual deductible Dental Oral Health Integration Program (OHIP) - All dental customers = Clinical research shows an association between oral health and overall health. The Cigna Dental Oral Health Integration Program (OHIP)® is designed to provide enhanced dental coverage for customers with certain eligible medical conditions. Eligible conditions for the program include cardiovascular disease, cerebrovascular disease (stroke), diabetes, maternity, chronic kidney disease, organ transplants, and head and neck cancer radiation. The program provides:
100% coverage for certain dental procedures
guidance on behavioral issues related to oral health
discounts on prescription and non-prescription dental products For more information and to see the complete list of eligible conditions, go to www.mycigna.com or call customer service 24/7 at 1.800.CIGNA24. **For services provided by a Cigna Dental PPO network dentist, Cigna Dental will reimburse the dentist according to a Contracted Fee Schedule. For services provided by an out-of-network dentist, Cigna Dental will reimburse according to Reasonable and Customary Allowances but the dentist may balance bill up to their usual fees.
24

Dental PPO - High and Low Options
Procedure Exclusions and Limitations Late Entrants Limit None Exams Two per Calendar year Prophylaxis (Cleanings) Two per Calendar year Fluoride 1 per Calendar year for people under 19 Histopathologic Exams Various limits per Calendar year depending on specific test X-Rays (routine) Bitewings: 2 per Calendar year X-Rays (non-routine) Full mouth: 1 every 36 consecutive months., Panorex: 1 every 36 consecutive months Model Payable only when in conjunction with Ortho workup Minor Perio (non-surgical) Various limitations depending on the service Perio Surgery Various limitations depending on the service Crowns and Inlays Replacement every 5 years Bridges Replacement every 5 years Dentures and Partials Replacement every 5 years Relines, Rebases Covered if more than 6 months after installation Adjustments Covered if more than 6 months after installation Repairs - Bridges Reviewed if more than once Repairs - Dentures Reviewed if more than once Sealants Limited to posterior tooth. One treatment per tooth every three years up to age 14 Space Maintainers Limited to non-Orthodontic treatment Prosthesis Over Implant 1 per 60 consecutive months if unserviceable and cannot be repaired. Benefits are based on the amount payable for nonprecious metals. No porcelain or white/tooth colored material on molar crowns or bridges Alternate Benefit When more than one covered Dental Service could provide suitable treatment based on common dental standards, Cigna HealthCare will determine the covered Dental Service on which payment will be based and the expenses that will be included as Covered Expenses
Benefit Exclusions Services performed primarily for cosmetic reasons Replacement of a lost or stolen appliance Replacement of a bridge or denture within five years following the date of its original installation Replacement of a bridge or denture which can be made useable according to accepted dental standards Procedures, appliances or restorations, other than full dentures, whose main purpose is to change vertical dimension, diagnose or treat
conditions of TMJ, stabilize periodontally involved teeth, or restore occlusion Veneers of porcelain or acrylic materials on crowns or pontics on or replacing the upper and lower first, second and third molars Bite registrations; precision or semi-precision attachments; splinting A surgical implant of any type Instruction for plaque control, oral hygiene and diet Dental services that do not meet common dental standards Services that are deemed to be medical services Services and supplies received from a hospital Charges which the person is not legally required to pay Charges made by a hospital which performs services for the U.S. Government if the charges are directly related to a condition
connected to a military service Experimental or investigational procedures and treatments Any injury resulting from, or in the course of, any employment for wage or profit Any sickness covered under any workers’ compensation or similar law Charges in excess of the reasonable and customary allowances To the extent that payment is unlawful where the person resides when the expenses are incurred; Procedures performed by a Dentist who is a member of the covered person’s family (covered person’s family is limited to a spouse,
siblings, parents, children, grandparents, and the spouse’s siblings and parents); For charges which would not have been made if the person had no insurance; For charges for unnecessary care, treatment or surgery; To the extent that you or any of your Dependents is in any way paid or entitled to payment for those expenses by or through a public
program, other than Medicaid; To the extent that benefits are paid or payable for those expenses under the mandatory part of any auto insurance policy written to
comply with a “no-fault” insurance law or an uninsured motorist insurance law. Cigna HealthCare will take into account any adjustment option chosen under such part by you or any one of your Dependents.
In addition, these benefits will be reduced so that the total payment will not be more than 100% of the charge made for the Dental Service if benefits are provided for that service under this plan and any medical expense plan or prepaid treatment program sponsored or made available by your Employer.
This benefit summary highlights some of the benefits available under the proposed plan. A complete description regarding the terms of coverage, exclusions and limitations, including legislated benefits, will be provided in your insurance certificate or plan description. Benefits are insured and/or administered by Connecticut General Life Insurance Company. "Cigna HealthCare" refers to various operating subsidiaries of Cigna Corporation. Products and services are provided by these subsidiaries and not by Cigna Corporation. These subsidiaries include Connecticut General Life Insurance Company, Cigna Health and Life Insurance Company, and HMO or service company subsidiaries of Cigna Health Corporation and Cigna Dental Health, Inc. DPPO insurance coverage is set forth on the following policy form numbers: AR: HP-POL77; CA: HP-POL57; CO: HP-POL78; CT: HP-POL58; DE: HP-POL79; FL: HP-POL60; ID: HPPOL82; IL: HP-POL62; KS: HP-POL84; LA: HP-POL86: MA: HP-POL 63; MI: HP-POL88; MO: HP- POL65; MS: HP-POL90; NC: HP-POL96; NE: HP-POL92; NH: HP-POL94; NM: HP-POL95; NV: HP-POL93; NY: HP-POL67; OH: HP-POL98; OK: HP-POL99; OR: HP-POL68; PA: HP-POL100; RI: HP-POL101; SC: HP-POL102; SD: HP-POL103; TN: HP-POL69; TX: HP-POL70; UT: HP-POL104; VA: HP-POL72; VT: HP-POL71; WA: POL-07/08; WI: HP-POL107; WV: HP-POL106; and WY: HP-POL108. “Cigna,” the “Tree of Life” logo and “Cigna Dental Care” are registered service marks of Cigna Intellectual Property, Inc., licensed for use by Cigna Corporation and its operating subsidiaries. All products and services are provided by or through such operating subsidiaries and not by Cigna Corporation. Such operating subsidiaries include Connecticut General Life Insurance Company (CGLIC), Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Connecticut, Inc., and Cigna Dental Health, Inc. and its subsidiaries. Cigna Dental PPO plans are underwritten or administered by CGLIC or CHLIC, with network management services provided by Cigna Dental Health, Inc. and certain of its subsidiaries. In Arizona and Louisiana, the insured Dental PPO plan offered by CGLIC is known as the “CG Dental PPO”. In Texas, the insured dental product offered by CGLIC and CHLIC is referred to as the Cigna Dental Choice Plan, and this plan utilizes the national Cigna Dental PPO network. Cigna Dental Care (DHMO) plans are underwritten or administered by Cigna Dental Health Plan of Arizona, Inc., Cigna Dental Health of California, Inc., Cigna Dental Health of Colorado, Inc., Cigna Dental Health of Delaware, Inc., Cigna Dental Health of Florida, Inc., a Prepaid Limited Health Services Organization licensed under Chapter 636, Florida Statutes, Cigna Dental Health of Kansas, Inc. (Kansas and Nebraska), Cigna Dental Health of Kentucky, Inc. (Kentucky and Illinois), Cigna Dental Health of Maryland, Inc., Cigna Dental Health of Missouri, Inc., Cigna Dental Health of New Jersey, Inc., Cigna Dental Health of North Carolina, Inc., Cigna Dental Health of Ohio, Inc., Cigna Dental Health of Pennsylvania, Inc., Cigna Dental Health of Texas, Inc., and Cigna Dental Health of Virginia, Inc. In other states, Cigna Dental Care plans are underwritten by CGLIC, CHLIC, or Cigna HealthCare of Connecticut, Inc. and administered by Cigna Dental Health, Inc. BSD46380 © 2015 Cigna
25

Vision insurance provides coverage for routine eye examinations and may cover all or part of the costs associated with contact lenses, eyeglasses and vision correction, depending on the plan.
About this Benefit
Vision YOUR BENEFITS PACKAGE
75%
DID YOU KNOW?
of U.S. residents between age 25 and 64 require some sort of vision
correction.
SUPERIOR VISION
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 26

Co-Pays
Exam $10
Materials₁ $25
Contact Lens Fitting (standard & specialty)
$25
Services/Frequency
Exam 12 months
Frame 12 months
Contact Lens Fitting 12 months
Lenses 12 months
Contact Lenses 12 months
Benefits In-Network Out-of-Network
Exam (ophthalmologist) Covered in full Up to $42 retail
Exam (optometrist) Covered in full Up to $37 retail
Frames $125 retail allowance Up to $68 retail
Contact Lens Fitting (standard₂) Covered in full Not Covered
Contact Lens Fitting (specialty₂) $50 retail allowance Not Covered
Contact Lenses4 $120 retail allowance Up to $100 retail
Lenses (standard) per pair
Single Vision Covered in full Up to $32 retail
Bifocal Covered in full Up to $46 retail
Trifocal Covered in full Up to $61 retail
Progressive lens upgrade See description3 Up to $61 retail
Co-pays apply to in-network benefits; co-pays for out-of-network visits are deducted from reimbursements. ₁ Materials co-pay applies to lenses & frames only, not contact lenses. ₂Visit FAQs on www.superiorvision.com for definitions of standard and specialty CLF. ₃Covered to the provider's retail amount for a standard lined trifocal lens; member pays the difference between the retail price of the progressive lens they have chose and their provider's standard lined trifocal lens, plus applicable co-pay. 4Contact lenses are in lieu of eyeglass lenses and frames benefit.
Vision
Discounts on Covered Materials5
Frames: 20% off amount over allowance Lens options: 20% off retail Progressives: 20% off amount over retail lined trifocal lens, including lens options The following options have out-of-pocket maximums on standard (not premium, brand, or progressive) plastic lenses. 5Discounts and maximums may vary by lens type. Please check with your
provider.
Maximum Member Out-of-Pocket
Single Vision Bifocal & Trifocal Scratch coat $13 $13
Ultraviolet coat $15 $15
Tints, solid or gradients $25 $25
Anti-reflective coat $50 $50
Polycarbonate $40 20% off retail
High index 1.6 $55 20% off retail
Photochromics $80 20% off retail
Discounts on Non-Covered Exam and Materials5 Exams, frames, and prescription lenses: 30% off retail Lens options, contacts, other prescription materials: 20% off retail Disposable contact lenses: 10% off retail
5Discounts and maximums may vary by lens type. Please check with your
provider.
Refractive Surgery Superior Vision has a nationwide network of refractive surgeons and leading LASIK networks who offer members a discount. These discounts range from 5%-50%, and are the best possible discounts available to Superior Vision. The Plan discount features are not insurance. All allowances are retail; member is responsible for any amount over the allowance, minus available discounts.
Discounts are subject to change without notice.
Disclaimer: All final determinations of benefits, administrative duties, and definitions are governed by the Certificate of Insurance for your vision plan. Please check with your Human Resources department if you have any questions.
Monthly Premiums
EE Only $8.03
EE + Spouse $15.96
EE + Child(ren) $15.62
EE + Family $23.79
27

Short Term Disability YOUR BENEFITS PACKAGE
LINCOLN FINANCIAL
Disability insurance protects one of your most valuable assets, your ability to earn a living. This insurance will replace a portion of your income in the event that you become physically unable to work. Short term disability coverage provides benefits when you are unable to work for a short period of time due to a covered sickness or injury.
About this Benefit DID YOU KNOW?
60% of Americans do not have a “rainy day” fund to cover three
months of unanticipated financial emergencies.
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
Short Term Disability
28

Short Term Disability
Short-term disability is intended to protect your income for a short duration in case you become ill or injured. Eligibility—All employees in an eligible class. You are able to take advantage of this coverage now without a health examination. You may not be offered this opportunity again until your annual open enrollment. . Maximum Weekly Benefit—60% of weekly salary up to $1,500 per week Maximum Benefit Duration—25 weeks Elimination Period—Benefits begin on: 8 day(s) from an accident 8 day(s) from an illness Rehabilitation Assistance Benefit—Employees who participate in an approved rehabilitation program are eligible to receive an additional percent of benefit. Additionally, approved program costs may be reimbursed. Survivor Income—A benefit may be paid to your survivor if you should die while you were eligible to receive benefits under this policy. Pre-Existing Condition—You may not be eligible for benefits if you have received treatment for a condition within 3 months prior to your effective date under this policy until you have been covered under the policy for 6 months. Waiver of Premium—You will not be required to pay premium during any time of approved total or partial disability. Integration of Benefits—The benefits from this policy will be reduced by benefits you receive from state disability or worker’s compensation programs. Portability—You may be able to port your coverage if you have been covered under the policy for 12 months and terminate due to reasons other than disability, retirement, or leave of absence. Understanding Your Benefits Total Disability You are considered totally disabled if, due to an injury or illness, you are unable to perform each of the main duties of your regular occupation. Partial Disability You are considered partially disabled if you are unable, due to an injury or illness, to perform the main duties of your regular
occupation on a full-time basis. Partial Disability benefits may be payable if you are earning at least 20% of the income you earned prior to becoming disabled, but not more than 99%. Partial disability benefits allow you to work and earn income from your employer as well as continue to receive benefits, which may enable you to receive 100% of your income during your time of disability. Continuation of Disability If you return to work full-time but become disabled from the same disability within two weeks of returning to work, you will begin receiving benefits again immediately. Pre-Existing Condition Any sickness or injury for which you have received medical treatment, consultation, care, or services (including diagnostic measures or the taking of prescribed medications) during the specified months prior to the coverage effective date. A disability arising from any such sickness or injury will be covered only if it begins after you have performed your regular occupation on a full-time basis for the specified months following the coverage effective date. Benefit Exclusions You will not receive benefits in the following circumstances:
Your disability is the result of a self-inflicted injury.
You are not under the regular care of a doctor when requesting disability benefits.
Your disability is covered under a worker's compensation plan and/or is due to a job related sickness or injury.
Benefit Reductions Your benefits may be reduced if you are receiving benefits from any of the following sources:
Any governmental retirement system earned as a result of working for the current policyholder;
Any disability or retirement benefit received under a retirement plan;
Any Social Security, or similar plan or act, benefits;
Earnings the insured earns or receives from any form of employment.
Disability income benefits received under state disability laws.
Benefit Termination This coverage will terminate when you terminate employment with this policyholder, or at your retirement. For assistance or additional information Contact Lincoln Financial Group at (800) 423-2765 or log on to www.LincolnFinancial.com.
29

About this Benefit
YOUR BENEFITS PACKAGE
Just over 1 in 4 of today's 20 year-olds will become disabled before
they retire.
DID YOU KNOW?
34.6 months is the duration of the
average disability claim.
LINCOLN FINANCIAL
Disability insurance protects one of your most valuable assets, your paycheck. This insurance will replace a portion of your income in the event that you become physically unable to work due to sickness or injury for an extended period of time.
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
Long Term Disability
30

Long Term Disability
When a covered disability keeps you out of work, long-term disability insurance helps keep your finances protected. It pays a portion of your income while you recover, with benefits continuing for the policy’s benefit period or until you are no longer disabled—whichever comes first. Conditions that could lead to a long-term disability claim include:
Surgery
Injury
Illness
Accident
How does long-term disability coverage work? Mike signed up for long-term disability insurance when he became a full-time employee several years ago. Two months ago, he was injured in a traffic accident that resulted in a covered disability. His policy has an elimination period of 90 days. If he is disabled after that time, he is eligible to begin collecting benefits. The policy provides a maximum benefit of 50% of pay, up to $5,000 a month, and a maximum benefit duration of five years. Mike paid for his insurance with after-tax dollars, so his benefits are tax-free.* If Mike’s disability prevents him from working for 10 months, here are the benefits he could collect:
*If the cost of Mike’s coverage is paid pretax, he will pay tax on the benefits he receives during his disability. **Mike’s policy includes a 90-day elimination period, so his benefit duration is seven month.
Two forms of income protection If you have short-term disability coverage, do you need a long-term policy? The answer is yes. Sixty-five percent of working Americans couldn’t cover living expenses for a year, according to the Council for Disability Awareness (March 2010).
You decide how benefits are used Benefits could be spent on anything: food, car payments, utilities or even a night out at the movies.
More benefits of your insurance Survivor Income Benefit. A lump sum is paid to your beneficiaries if you die while on disability. Waiver of Premium. You don’t have to pay premiums during periods of approved disability under our policy.
How much coverage do you need? Long-term disability insurance pays benefits for up to a specific period of time or until you are no longer disabled. Your expenses don’t stop while you aren’t working:
Food
Car payments and maintenance
Utilities
Mortgage or rent Long-term disability income insurance can help protect your hard-earned savings.
Protect your paycheck There are some important advantages to buying insurance that’s offered to employees as a group.
Cost. This coverage is offered at group rates, which are often less expensive than rates for individual policies.
Convenience. Payroll deduction is simple and easy.
Confidence. You can choose the right coverage at work.
We help you get back to work EmployeeConnectSM services. You have access to counselors and other assistance for personal, legal, financial and other issues. Progressive Partial Disability Benefit. If you’re only able to do part of your job or work part time, you can receive partial benefits. With part-time earnings and a partial disability benefit, you could receive up to 100% of your predisability earnings
Sample LTD benefit payment
Mike’s monthly pay $3,500
Mike’s maximum monthly benefit x 50%
Mike’s monthly benefit = $1,750
Mike’s approved benefit duration** x 7
Mike’s total long-term disability benefit = $12,250
31
Cancer insurance offers you and your family supplemental insurance protection in the event you or a covered family member is diagnosed with cancer. It pays a benefit directly to you to help with expenses associated with cancer treatment.
About this Benefit
Cancer YOUR
BENEFITS
Breast Cancer is
the most commonly
diagnosed cancer
in women.
DID YOU KNOW?
If caught early,
prostate cancer is one
of the most treatable
malignancies.
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan
details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
AMERICAN PUBLIC LIFE
32

GC3 Limited Benefit Group Cancer Indemnity InsuranceCBEBC
THE POLICY UNDER WHICH THIS CERTIFICATE IS ISSUED IS NOT A POLICY OF WORKERS’ COMPENSATION INSURANCE. THE EMPLOYER DOES NOT BECOME A SUBSCRIBER TO THE WORKERS’ COMPENSATION SYSTEM BY PURCHASING THE POLICY AND IF THE EMPLOYER IS A NON-SUBSCRIBER, THE EMPLOYEE LOSES THOSE BENEFITS WHICH WOULD OTHERWISE ACCRUE UNDER THE WORKERS’ COMPENSATION LAWS. THE EMPLOYER MUST COMPLY WITH THE WORKERS’ COMPENSATION LAW AS IT PERTAINS TO NON-SUBSCRIBERS AND THE REQUIRED NOTIFICATIONS THAT MUST BE FILED AND POSTED.
Summary of BenefitsBenefits Level 1 Plan Level 2 Plan
Radiation Therapy/Chemotherapy/ Immunotherapy Benefit
$500 per calendar month of treatment $1,500 per calendar month of treatment
Hormone Therapy Benefit $50 per treatment, up to 12 per calendar year $50 per treatment, up to 12 per calendar year
Surgical Schedule Benefit $1,600 max per operation; $15 per surgical unit $4,800 max per operation; $45 per surgical unit
Anesthesia Benefit 25% of the amount paid for covered surgery 25% of the amount paid for covered surgery
Hospital Confinement Benefit $100 per day 1-90 days; $100 per day, 91+ days in lieu of other benefits
$300 per day 1-90 days; $300 per day, 91+ days in lieu of other benefits
US Government/Charity Hospital/HMO $100 per day in lieu of most other benefits $300 per day in lieu of most other benefits
Outpatient Hospital or Ambulatory Surgical Center Benefit
$200 per day of surgery $600 per day of surgery
Drugs & Medicine Benefit - Inpatient $150 per confinement $150 per confinement
Drugs & Medicine Benefit - Outpatient $50 per prescription, up to $50 per cal month $50 per prescription, up to $150 per cal month
Transportation & Outpatient Lodging Benefit
$0.50 per mile per round trip $100 per day, up to 100 days per calendar year
$0.50 per mile per round trip $100 per day, up to 100 days per calendar year
Family Member Transportation & Lodging Benefit
$0.50 per mile per round trip $100 per day, up to 100 days per calendar year
$0.50 per mile per round trip $100 per day, up to 100 days per calendar year
Blood, Plasma & Platelets Benefit $150 per day, up to $7,500 per calendar year $250 per day, up to $12,500 per calendar year
Bone Marrow/Stem Cell Transplant Autologous - $500 per calendar year Non-Autologous - $1,500 per calendar year
Autologous - $1,500 per calendar year Non-Autologous - $4,500 per calendar year
Experimental Treatment Benefit Pays as any non-experimental benefit Pays as any non-experimental benefit
Attending Physician Benefit $30 per day of confinement $50 per day of confinement
Surgical Prosthesis Benefit $1,000 per device (includes surgical fee); max 1 device per site, 2 lifetime max
$3,000 per device (includes surgical fee); max 1 device per site, 2 lifetime max
Hair Prosthesis Benefit $50 per hair prosthetic, 2 lifetime max $50 per hair prosthetic, 2 lifetime max
Dread Disease Benefit $100 per day, 1-90 days of hospital confinement $300 per day, 1-90 days of hospital confinement
Hospice Care Benefit $50 per day, $9,000 lifetime max $100 per day, $18,000 lifetime max
Inpatient Special Nursing Services $150 per day of confinement $150 per day of confinement
Ambulance Ground Benefit $200 per ground trip $200 per ground trip
Ambulance Air Benefit $2,000 per air trip; up to 2 trips per hospital confinement (any combination of ground/air)
$2,000 per air trip; up to 2 trips per hospital confinement (any combination of ground/air)
Extended Care Benefit $100 per day $300 per day
Home Health Care Benefit $100 per day $300 per day
Second & Third Surgical Opinions $300 per diagnosis; additional $300 if third opinion required
$300 per diagnosis; additional $300 if third opinion required
Waiver of Premium Premium waived after 90 days of primary insured continuous total disability due to cancer
Premium waived after 90 days of primary insured continuous total disability due to cancer
Physical/Speech Therapy Benefit $25 per visit, up to 4 visits per calendar month, $1,000 lifetime max
$25 per visit, up to 4 visits per calendar month, $1,000 lifetime max
RidersDiagnostic Testing Benefit Rider $50; 1 person, per calendar year $50; 1 person, per calendar year
Critical Illness Rider: Heart Attack/Stroke $2,500 lump sum benefit $2,500 lump sum benefit
Optional Benefit Rider
Intensive Care Unit Rider $600 up to a max of 30 days per confinement $600 up to a max of 30 days per confinement
APSB-22356(TX) MGM/FBS CBEBC 33

EligibilityThis policy/certificate will be issued only to those persons who meet American Public Life Insurance Company’s insurability requirements. The policy/certificate and the Internal Cancer coverage under the Critical Illness Rider will not be issued to anyone who has been diagnosed or treated for Cancer in the previous ten years. The Heart Attack or Stroke coverage under the Critical Illness Rider will not be issued to anyone who has been diagnosed or treated for any heart or stroke related conditions. The Hospital Intensive Care Unit Rider will not cover heart conditions for a period of two years following the Effective Date of coverage for anyone who has been diagnosed or treated for any heart related condition prior to the 30th day following the Covered Person’s Effective Date of coverage.
If You are working either under contract to or as a Full-Time Employee for the Policyholder, or You are a member in or employed by the association, You are eligible for insurance provided You qualify for coverage as defined in the Master Application. You must apply for insurance within thirty (30) days of the Policy Effective Date or the date that You become eligible for coverage. If You do not apply within thirty (30) days of the Policy Effective Date or the date You become eligible for coverage, You may be subject to additional underwriting by Us.
Base PolicyAll diagnosis of cancer must be positively diagnosed by a legally licensed doctor of medicine certified by the American Board of Pathology or American Board of Osteopathic Pathology. This policy/certificate pays only for loss resulting from definitive cancer treatment including direct extension, metastatic spread or recurrence. Proof must be submitted to support each claim. This policy/certificate also covers other conditions or diseases directly caused by cancer or the treatment of cancer.
No benefits are payable for any covered person for any loss incurred during the first year of this policy/certificate as a result of a Pre-Existing Condition. A Pre-Existing Condition is a specified disease for which, within 12 months prior to the covered person’s effective date of coverage, medical advice, consultation or treatment, including prescribed medications, was recommended by or received from a member of the medical profession, or for which symptoms manifested in such a manner as would cause an ordinarily prudent person to seek diagnosis, medical advice or treatment. Pre-Existing Conditions specifically named or described as excluded in any part of this contract are never covered. This policy/certificate contains a 30-day waiting period during which no benefits will be paid under this policy/certificate. If any covered person has a specified disease diagnosed before the end of the 30-day period immediately following the covered person’s effective date, coverage for that person will apply only to loss that is incurred after one year from the effective date of such person’s coverage. If any covered person is diagnosed as having a specified disease during the 30-day period immediately following the effective date, you may elect to void the policy/certificate from the beginning and receive a full refund of premium. All benefits payable only up to the maximum amount listed in the schedule of benefits in the policy/certificate.
A Hospital is not an institution which is primarily a place for alcoholics or drug addicts; the aged; a nursing, rest or convalescent nursing home; a mental institution or sanitarium; a facility contracted for or operated by the United States Government for treatment of members or ex-members of the armed forces (unless You are legally required to pay for services rendered in the absence of insurance); or, a long-term nursing unit or geriatrics ward.
Diagnostic Testing Benefit RiderWe will pay the indemnity amount for one generally medically recognized internal cancer screening test per covered person per calendar year. Screening test include, but limited to: mammogram; breast ultrasound; breast thermography; breast cancer blood test (CA15-3); colon cancer blood test (CEA); prostate-specific antigen blood test (PSA); flexible sigmoidoscopy; colonoscopy; virtual colonoscopy; ovarian cancer blood test (CA-125); pap smear (lab test required); chest x-ray; hemocult stool specimen; serum protein electrophoresis (blood test for myeloma); thin prep pap test. Screening tests payable under this benefit will only be paid under this benefit. Benefits will only be paid for tests performed after the 30-day period following the covered person’s effective date of coverage.
Critical Illness RiderBenefits will only be paid for a covered critical illness as shown on the policy/certificate schedule page in the policy. No benefits will be provided for any loss caused by or resulting from: intentionally self-inflicted bodily injury, suicide or attempted suicide, whether sane or insane; or alcoholism or drug addiction; or any act of war, declared or undeclared , or any act related to war; or military service for any country at war; or a pre-existing condition; or a covered critical illness when the date of diagnosis occurs during the waiting period; or participation in any activity or event while intoxicated or under the influence of any narcotic unless administered by a physician or taken according to the physician’s instructions; or participation in, or attempting to participate in a felony, riot or insurrection (a felony is as defined by the law of the jurisdiction in which the activity takes place). Internal cancer does not include: other conditions that may be considered pre-cancerous or having malignant potential such as: acquired immune deficiency syndrome (AIDS); or actinic keratosis; or myelodysplastic and non-malignant myeloproliferative disorders; or aplastic anemia; or atypia; or non-malignant monoclonal gamopathy; or Leukoplakia; or Hyperplasia; or Carcinold; or Polycythemia; or carcinoma in situ or any skin cancer other than invasive malignant melanoma into the dermis or deeper. For a pre-existing condition no benefits are payable.
Hospital Intensive Care Unit RiderNo benefits will be provided during the first two years of this rider for hospital intensive care unit confinement caused by any heart condition when any heart condition was diagnosed or treated prior to the 30th day following the covered person’s effective date of this rider. The heart condition causing the confinement need not be the same condition diagnosed or treated prior to the effective date. No benefits will be provided if the loss results from: attempted suicide, whether sane or insane; or intentional self-injury; or alcoholism or drug addiction; or any act of war, declared or undeclared, or any act related to war; or military service for a country at war. No benefits will be paid for confinements in units such as surgical recovery rooms, progressive care, burn units, intermediate care, private monitored rooms, observation units, telemetry units or psychiatric units not involving intensive medical care; or other facilities which do not meet the standards for intensive care unit as defined in the rider. For a newborn child born within the ten-month period following the effective date of this rider, no benefits will be provided for hospital intensive care unit confinement that begins within the first 30 days following the birth of such child.
APSB-22356(TX) MGM/FBS CBEBC
GC3 Limited Benefit Group Cancer Indemnity Insurance
Monthly Premium Level 1 Level 1 + ICU Rider Level 2 Level 2 + ICU RiderIndividual $13.80 $17.10 $29.90 $33.20One-Parent Family $19.10 $23.60 $40.90 $45.40Two-Parent Family $24.30 $31.20 $51.90 $58.80
*Premium and amount of benefits provided vary dependent upon the level selected at time of application.
34

Underwritten by American Public Life Insurance Company. This is a brief description of the coverage. For complete benefits, limitations, exclusions and other provisions, please refer to the policy and riders. This coverage does not replace Workers’ Compensation Insurance. This product is inappropriate for people who are eligible for Medicaid coverage. | This policy is considered an employee welfare ben-efit plan established and/or maintained by an association or employer intended to be covered by ERISA, and will be administered and enforced under ERISA. Group policies issued to governmental entities and municipalities may be exempt from ERISA guidelines. | Policy Form GC-3 Series | Texas | Limited Benefit Group Cancer Indemnity Insurance Policy | (11/14) | CBEBC
Conditionally RenewableThis policy/certificate is conditionally renewable. This means that We have the right to terminate your policy/certificate on any premium due date after the first Policyholder’s Anniversary Date. We must give the Policyholder at least 60 days written notice prior to cancellation. We cannot cancel Your coverage because of a change in Your age or health. We can change Your premiums if We change premiums for all similar Certificates issued to the Policyholder. We must give the Policyholder at least 60 days written notice before We change Your premiums.
Continuation RiderContinuation Coverage is continued when the Insured (You) cease employment with the employer through whom You originally became insured under the Policy. You will have the option to continue this Certificate (including any Riders, if applicable) by paying the premiums directly to Us at Our home office. Premiums must be paid within thirty-one (31) days after employment with your employer terminates. Premium rates required under this Continuation provision will be the same rates as those charged under the Employer’s Policy as if You had continued employment. We will bill You for these premiums after You notify Us to continue this coverage. Coverage will continue until the earlier of: (1) the Policy under which You originally became insured ends; or (2) You stop paying premiums under this option (subject to the terms of the Grace Period).
ConversionIf the Employer’s Policy is terminated, this Certificate will terminate. Upon termination of the Employer’s Policy, the employee (You) will be entitled to convert to an individual policy of insurance issued by Us without evidence of insurability provided the required premiums have been paid on your behalf and You notified Us in writing within thirty-one (31) days of the Employer’s Policy termination. Premiums for the individual policy of insurance will be figured from the premium rate table in effect on the date of conversion.
Subject to the terms of this provision, a covered child who ceases to be eligible may convert to an individual policy of insurance and a covered spouse who ceases to be eligible for coverage because of divorce or annulment may convert to an individual policy.
Terms of this provision include: (1) Application for the individual policy and payment of the first premium must be made within 60 days after coverage ceases under the Policy/Certificate. Premiums will be figured from the premium rate table in effect on the date of conversion. (2) The individual policy will be issued without proof of insurability. It will provide benefits that most nearly approximates those of the Policy/Certificate. (3) The individual policy will take effect the day after coverage ceases under the Policy/Certificate. However, no benefits will be payable under the individual policy for any loss for which benefits are payable under the Policy/Certificate. (4) The Pre-Existing Condition Limitation and Time Limit on Certain Defenses provisions for the individual policy will be figured from the Covered Person’s Effective Date of coverage under the Policy/Certificate. (5) Any benefit maximums will be figured from the Effective Date of the Policy/Certificate.
This rider is subject to all the provisions of the Policy and Certificate to which it is attached that are not in conflict with this rider.
Termination of CoverageYour Insurance coverage will end on the earliest of these dates: (a) the date You no longer qualify as an Insured; (b) the last day of the period for which a premium has been paid, subject to the Grace Period; (c) the date the Policy terminates (See Conversion provision); (d) the date You retire; (e) the date You cease employment, or terminate Your contract with the employer through whom You originally became insured under the Policy (See Conversion provision); or (f) the date We receive Your written request for termination. Termination of Dependent(s) Insurance coverage on Your Dependent(s) will end on the earliest of these dates: (a) the date the coverage under the Certificate terminates; (b) the date the Dependent no longer meets the definition of Dependent, as defined in the Policy/Certificate (See Conversion provision); (c) the date We receive Your written request for termination.
Termination of Rider Coverage This rider terminates: (a) when Your coverage terminates under the Policy/Certificate to which this Rider is attached; or, (b) when any premium for this rider is not paid before the end of the Grace Period; or, (c) when You give Us a written request to do so. Coverage on a Dependent terminates under this rider when such person ceases to meet the definition of Dependent, as defined in the Policy.
APSB-22356(TX) MGM/FBS CBEBC
2305 Lakeland Drive | Flowood, MS 39232ampublic.com | 800.256.8606
GC3 Limited Benefit Group Cancer Indemnity Insurance
35

Individual life is a policy that provides a specified death benefit to your beneficiary at the time of death. The advantage of having an individual life insurance plan as opposed to a group supplemental term life plan is that this plan is guaranteed renewable, portable and typically premiums remain the same over the life of the policy.
About this Benefit
Individual Life YOUR BENEFITS PACKAGE
x 10
Experts recommend at least
your gross annual income in coverage when purchasing life insurance.
DID YOU KNOW?
TEXAS LIFE
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 36

Individual Life
Life Insurance Highlights
Voluntary permanent life insurance can be an ideal complement to the group term and optional term your employer might provide. Designed to be in force when you die, this voluntary universal life product is yours to keep, even when you change jobs or retire, as long as you pay the necessary premium. Group and voluntary term, on the other hand, typically are not portable if you change jobs and, even if you can keep them after you retire, usually costs more and declines in death benefit. The policy, PureLife-plus, is underwritten by Texas Life Insurance Company, and it has these outstanding features:
High Death Benefit. With one of the highest death benefit available at the worksite,1 PureLife-plus gives your loved ones peace of mind, knowing there will be significant life insurance in force should you die prematurely.
Minimal Cash Value. Designed to provide high death benefit, PureLife-plus does not compete with the cash accumulation in your employer-sponsored retirement plans.
Long Guarantees. Enjoy the assurance of a policy that has a guaranteed death benefit to age 121 and level premium that guarantees coverage for a significant period of time (after the guaranteed period, premiums may go down, stay the same, or go up).
Refund of Premium. Unique in the marketplace, PureLife-plus offers you a refund of 10 years’ premium, should you surrender the policy if the premium you pay when you buy the policy ever increases. (Conditions apply.)
Accelerated Death Benefit Rider. Should you be diagnosed as terminally ill with the expectation of death within 12 months (24 months in Illinois), you will have the option to receive 92% (84% in Illinois) of the death benefit, minus a $150 ($100 in Florida) administrative fee. This valuable living benefit gives you peace of mind knowing that, should you need it, you can take the large majority of your death benefit while still alive. (Conditions apply.)
You may apply for this permanent, portable coverage, not only for yourself, but also for your spouse, minor children and grandchildren. Like most life insurance policies, Texas Life policies contain certain exclusions, limitations, exceptions, reductions of benefits, waiting periods and terms for keeping them in force. Please contact a Texas Life representative for costs and complete details. 1Voluntary and Universal Whole Life Products, Eastbridge Consulting Group, October 2008
DID YOU KNOW? Those with no life insurance think it’s 3 times more expensive than it actually is.
37

Group term life is the most inexpensive way to purchase life insurance. You have the freedom to select an amount of life insurance coverage you need to help protect the well-being of your family. Accidental Death & Dismemberment is life insurance coverage that pays a death benefit to the beneficiary, should death occur due to a covered accident. Dismemberment benefits are paid to you, according to the benefit level you select, if accidentally dismembered.
About this Benefit
Life and AD&D YOUR BENEFITS PACKAGE
cause of accidental deaths in the US, followed by poisoning, falls,
drowning, and choking.
DID YOU KNOW?
#1
Motor vehicle crashes are the
UNUM
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 38

Term Life Insurance and AD&D
Eligibility
All employees working at least 20 hours each week in active employment in the U.S. with the employer, and their eligible spouses and children to age 26.
Coverage Amounts
Your Term Life coverage options are: Employee: Up to 5 times salary in increments of $10,000. Not to exceed $500,000. Spouse: Up to 100% of employee amount in increments of $5,000. Not to exceed $500,000. Benefits will be paid to the employee. Child: Up to 100% of employee coverage amount in increments of $2,000. Not to exceed $10,000. The maximum death benefit for a child between the ages of live birth and 6 months is $1000. Benefits will be paid to the employee. In order to purchase Life coverage for your spouse and/or child, you must purchase Life coverage for yourself. Your AD&D coverage options are: Employee: Up to 5 times salary in increments of $10,000. Not to exceed $500,000. You may purchase AD&D coverage for yourself regardless of whether you purchase Life coverage. Spouse: 50% of Employee AD&D amount. Not to exceed $250,000. Benefits will be paid to the employee. Child: 10% of Employee AD&D amount. Not to exceed $50,000. The maximum death benefit for a child between the ages of live birth and 6 months is $1,000. Benefits will be paid to the employee. In order to purchase AD&D coverage for your spouse and/or child, you must purchase AD&D coverage for yourself. AD&D Benefit Schedule: The full benefit amount is paid for loss of:
Life
Both hands or both feet or sight of both eyes
One hand and one foot
One hand and the sight of one eye
One foot and the sight of one eye
Speech and hearing Other losses may be covered as well. Please see your Plan Administrator.
Coverage amount(s) will reduce according to the following schedule: Age: Insurance Amount Reduces to: 65 65% of original amount 70 50% of original amount
Guarantee Issue Current Employees: If you and your eligible dependents enroll on or before the enrollment deadline, you may apply for any amount of Life insurance coverage up to $220,000 for yourself and any amount of coverage up to $50,000 for your spouse. Any Life insurance coverage over the Guarantee Issue amount(s) will be subject to evidence of insurability. If you and your eligible dependents do not enroll on or before the enrollment deadline, you can apply for coverage only during an annual enrollment period and will be required to furnish evidence of insurability for the entire amount of Life insurance coverage. AD&D coverage does not require evidence of insurability. If you and your eligible dependents enroll on or before the enrollment deadline and later wish to increase your Life insurance coverage, you may increase your coverage with evidence of insurability at anytime during the year. However, you may wait until the next annual enrollment and only coverage over one benefit unit increase will be subject to evidence of insurability. Employees hired on or after 09/01/2012: If you and your eligible dependents enroll within 31 days of your eligibility date, you may apply for any amount of Life insurance coverage up to $220,000 for yourself and any amount of coverage up to $50,000 for your spouse. Any Life insurance coverage over the Guarantee Issue amount(s) will be subject to evidence of insurability. If you and your eligible dependents do not enroll within 31 days of your eligibility date, you can apply for coverage only during an annual enrollment period and will be required to furnish evidence of insurability for the entire amount of coverage. AD&D coverage does not require evidence of insurability. If you and your eligible dependents enroll within 31 days of your eligibility date, and later, wish to increase your coverage, you may increase your Life insurance coverage, with evidence of insurability, at anytime during the year. However, you may wait until the next annual enrollment and only coverage over one benefit unit increase will be subject to evidence of insurability. Please see your Plan Administrator for your eligibility date.
39

Term Life Insurance and AD&D
Term Life Coverage Rates Rates shown are your Monthly deduction:
NOTE: Your rate will increase as you age and move to the next age band.
AD&D Coverage Rates
Insurance Age Your rate is based on your insurance age, which is your age immediately prior to and including the anniversary/effective date.
Additional Benefits Life Planning Financial & Legal Resources
This personalized financial counseling service provides expert, objective financial counseling to survivors and terminally ill employees at no cost to you. This service is also extended to you upon the death or terminal illness of your covered spouse. The financial consultants are master level consultants. They will help develop strategies needed to protect resources, preserve current lifestyles, and build future security. At no time will the consultants offer or sell any product or service.
Portability/Conversion If you retire, reduce your hours or leave your employer, you can take this coverage with you according to the terms outlined in the contract. However, if you have a medical condition which has a material effect on life expectancy, you will be ineligible to port your coverage. You may also have the option to convert your Term life coverage to an individual life insurance policy.
Accelerated Benefit If you become terminally ill and are not expected to live beyond a certain time period as stated in your certificate booklet, you may request up to 50% of your life insurance amount up to $750,000, without fees or present value adjustments. A doctor must certify your condition in order to qualify for this benefit. Upon your death, the remaining benefit will be paid to your designated beneficiary(ies). This feature also applies to your covered dependents.
Waiver of Premium If you become disabled (as defined by your plan) and are no longer able to work, your premium payments will be waived during the period of disability.
Retained Asset Account Benefits of $10,000 or more are paid through the Unum Retained Asset Account. This interest bearing account will be established in the beneficiary's name. He or she can then write a check for the full amount or for $250 or more, as needed.
Additional AD&D Benefits
Education Benefit: If you or your insured spouse die within 365 days of an accident, an additional benefit is paid to your dependent child(ren). Your child(ren) must be a full-time student beyond grade 12. (Not available in Illinois or New York.) Seat Belt/Air Bag Benefit: If you or your insured dependent(s) die in a car accident and are wearing a properly fastened seat belt and/or are in a seat with an air bag, an amount will be paid in addition to the AD&D benefit.
Limitations/Exclusions/Termination of Coverage Suicide Exclusion Life benefits will not be paid for deaths caused by suicide in the first twenty-four months after your effective date of coverage. No increased or additional benefits will be payable for deaths caused by suicide occurring within 24 months after the day such increased or additional insurance is effective.
Age Band
Employee per $1,000
Spouse per $1,000
Child per $1,000
$.160
24 and under
$.048 $.048
NOTE: The premium paid for child coverage is
based on the cost of coverage for
one child, regardless of how many children you
have.
25-29 $.048 $.048
30-34 $.067 $.067
35-39 $.076 $.076
40-44 $.095 $.095
45-49 $.143 $.143
50-54 $.228 $.228
55-59 $.371 $.371
60-64 $.561 $.561
65-69 $1.083 $1.083
70-74 $1.758 $1.758
75+ $2.480 $2.480
AD&D Cost Per: Monthly Rate
Employee $1,000 $.030
Spouse $1,000 $.030
Child $1,000 $.030
40

Term Life Insurance and AD&D
AD&D Benefit Exclusions AD&D benefits will not be paid for losses caused by, contributed to by, or resulting from:
Disease of the body or diagnostic, medical or surgical treatment or mental disorder as set forth in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders;
Suicide, self-destruction while sane, intentionally self-inflicted injury while sane, or self-inflicted injury while insane;
War, declared or undeclared, or any act of war;
Active participation in a riot;
Attempt to commit or commission of a crime;
The voluntary use of any prescription or non-prescription drug, poison, fume, or other chemical substance unless used according to the prescription or direction of your or your dependent’s doctor. This exclusion does not apply to you or your dependent if the chemical substance is ethanol;
Intoxication. (“Intoxicated” means that the individual’s blood alcohol level equals or exceeds the legal limit for operating a motor vehicle in the state or jurisdiction where the accident occurred.)
Termination of Coverage Your coverage and your dependents’ coverage under the Summary of Benefits ends on the earliest of:
The date the policy or plan is cancelled;
The date you no longer are in an eligible group;
The date your eligible group is no longer covered;
The last day of the period for which you made any required contributions;
The last day you are in active employment unless continued due to a covered layoff or leave of absence or due to an injury or sickness, as described in the certificate of coverage;
For dependent’s coverage, the date of your death. In addition, coverage for any one dependent will end on the earliest of:
The date your coverage under a plan ends;
The date your dependent ceases to be an eligible dependent;
For a spouse, the date of divorce or annulment. Unum will provide coverage for a payable claim which occurs while you and your dependents are covered under the policy or plan.
Next Steps How to Apply Current employees: To apply for coverage, complete your enrollment by the enrollment deadline
For employees hired on or after 09/01/2012: To apply for coverage, complete your enrollment form within 31 days of your eligibility date. All employees: If you apply for coverage after your effective date, or if you choose coverage over the guarantee issue amount, you will need to complete a medical questionnaire which you can get from your Plan Administrator. You may also be required to take certain medical tests at Unum’s expense.
Delayed Effective Date of Coverage Employee: Insurance coverage will be delayed if you are not in active employment because of an injury, sickness, temporary layoff, or leave of absence on the date that insurance would otherwise become effective. Dependent: Insurance coverage will be delayed if that dependent is totally disabled on the date that insurance would otherwise be effective. Exception: infants are insured from live birth. “Totally disabled” means that, as a result of an injury, a sickness or a disorder, your dependent is confined in a hospital or similar institution; is unable to perform two or more activities of daily living (ADLs) because of a physical or mental incapacity resulting from an injury or a sickness; is cognitively impaired; or has a life threatening condition.
Changes to Coverage Each year you and your spouse will be given the opportunity to change your Life coverage and AD&D coverage. You and your spouse may purchase additional Life coverage up to one benefit unit increase without evidence of insurability if you are already enrolled in the plan. Elected Life coverage over the one benefit unit increase will be medically underwritten and will require evidence of insurability and approval by Unum’s Medical Underwriters. The suicide exclusion will apply to any increase in coverage. AD&D coverage does not require evidence of insurability for increase amounts.
Questions Your coverage will become effective on 09/01/2012. For employees who become eligible after this date, please see your Plan Administrator for your effective date.
41
Critical illness insurance is designed to supplement your medical and disability coverage easing the financial impacts by covering some of your additional expenses. It provides a benefit payable directly to the insured upon diagnosis of a covered condition or event, like a heart attack or stroke.
About this Benefit
YOUR BENEFITS PACKAGE Critical Illness
Is the aggregate cost of a hospital stay for a heart
attack.
DID YOU KNOW?
$16,500
VOYA
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 42

Critical Illness
What is Critical Illness Insurance? Critical Illness Insurance pays a lump-sum benefit if you are diagnosed with a covered illness or condition. Critical Illness Insurance is a limited benefit policy. It is not health insurance and does not satisfy the requirement of minimum essential coverage under the Affordable Care Act. Features of Critical Illness Insurance include:
Guaranteed Issue: No medical questions or tests required for coverage.
Flexible: You can use the benefit money for any purpose you like.
Payroll deductions: Premiums are paid through convenient payroll deductions.
Portable: Should you leave your current employer or retire, you can take your coverage with you.
For what critical illnesses and conditions are benefits available? Critical Illness Insurance provides a benefit for the following illnesses and conditions. Covered illnesses/conditions are broken out into groups called “modules”. Benefits are paid at 100% of the Maximum Critical Illness Benefit amount unless otherwise stated. For a complete description of your benefits, along with applicable provisions, conditions on benefit determination, exclusions and limitations, see your certificate of insurance and any riders. Base Module
Heart attack
Stroke
Coronary artery bypass (25%)
Coma
Major organ failure
Permanent paralysis
End stage renal (kidney) failure Cancer Module
Cancer
Skin cancer (10%)
Carcinoma in situ (25%)
How can Critical Illness Insurance help? Below are a few examples of how your Critical Illness Insurance benefit could be used (coverage amounts may vary):
Medical expenses, such as deductibles and copays
Child care
Home healthcare costs
Mortgage payment/rent and home maintenance
Who is eligible for Critical Illness Insurance? You—all active employees working 20+ hours per
week**.
Your spouse*— under age 70. Coverage is available only if employee coverage is elected.
Your child(ren)— to age 26. Coverage is available only if employee coverage is elected.
*The use of “spouse” in this document means a person insured as a spouse as described in the certificate of insurance or rider.
What Maximum Critical Illness Benefit am I eligible for? For you
You have the opportunity to purchase a Maximum Critical Illness Benefit of $5,000 - $30,000 in $5,000 increments.
For your spouse You also have the opportunity to purchase a Maximum Critical Illness Benefit of $5,000 - $15,000 in $5,000 increments for your spouse.
For your children You also have the opportunity to purchase a Maximum Critical Illness Benefit of $5,000 or $10,000 for each covered child.
How many times can I receive the Maximum Critical Illness Benefit? Usually you are only able to receive the Maximum Critical Illness Benefit for one covered illness or disease within each module. Your plan includes the Restoration Benefit*, which provides a one-time restoration of 100% of the maximum benefit amount in order to pay an additional benefit if you experience a second covered illness for a different condition. Your plan also includes the Recurrence Benefit*, which allows you to receive a benefit for the same condition a second time. It’s important to note that in order for the second covered illness or the second occurrence of the illness to be covered, it must occur after 6 consecutive months without the occurrence of any covered critical illness named in your certificate, including the illness from the first benefit payment. If a partial benefit is paid out, it will not reduce the available maximum benefit amount for the illnesses or diseases in that same module. If you have reached the benefit limit by receiving the maximum benefit in each module, you may choose to end your coverage; however, if you have coverage for your spouse and/or child(ren), you must continue your
43

coverage in order to keep their coverage active. Please see the certificate of coverage for details. *This benefit does not apply to the cancer module.
What does my Critical Illness Insurance include? The benefits listed below are included with your critical illness coverage. There may be some variation by state. For a list of standard exclusions and limitations, please refer to the end of this document. For a complete description of your available benefits, along with applicable provisions, exclusions and limitations, see your certificate of insurance and any riders. Spouse* Critical Illness Insurance: If you have coverage for yourself, you may enroll your spouse, as long as your spouse is under age 70 and is not covered under the Policy as an employee.
Your spouse will receive coverage for the same covered conditions as you.
Your spouse will be able to receive a benefit the same number of times as you, as outlined above.
Guaranteed issue: No medical questions or tests required for coverage.
*The use of “spouse” in this form means a person insured as a spouse as described in the certificate of insurance or benefit. Please contact your employer for more information. Children’s Critical Illness Insurance: As long as you have critical illness coverage on yourself, your natural child(ren), stepchild(ren), adopted child(ren) or child(ren) for whom you are a legal guardian are eligible to be covered under your employer’s plan, up to the age of 26.
Your children are covered for the same covered conditions as you are with the exception of carcinoma in situ and coronary artery bypass; however, actual benefit amounts may vary.
Your child(ren) will be able to receive a benefit the same number of times as you, as outlined above.
One premium amount covers all of your eligible children.
Guaranteed issue: No medical questions or tests required for coverage.
If both you and your spouse are covered under the policy as an employee, then only one, but not both, may cover the same child(ren) under this benefit. If the parent who is covering the child(ren) stops being insured as an employee then the other parent may apply for children’s coverage.
Wellness Benefit: This provides an annual benefit payment if you complete a health screening test. You may only receive a benefit once per year, even if you complete multiple health screening tests.
Examples of health screening tests include but are not limited to: Pap test, serum cholesterol test for HDL and LDL levels, mammography, colonoscopy, and stress test on bicycle or treadmill.
The annual benefit is $50 for completing a health screening test.
If your spouse and/or children are covered for Critical Illness Insurance, they are also covered by the Wellness Benefit. Your spouse’s benefit amount is also $50. The benefit for child coverage is 50% of your coverage with an annual maximum of $100 for children’s benefits.
Exclusions and Limitations Benefits are not payable for any critical illness caused in whole or directly by any of the following*:
Participation or attempt to participate in a felony or illegal activity.
Suicide, attempted suicide or any intentionally self-inflicted injury, while sane or insane.
War or any act of war, whether declared or undeclared, other than acts of terrorism.
Loss that occurs while on full-time active duty as a member of the armed forces of any nation. We will refund, upon written notice of such service, any premium which has been accepted for any period not covered as a result of this exclusion.
Alcoholism, drug abuse, or misuse of alcohol or taking of drugs, other than under the direction of a doctor.
Benefits reduce 50% for the employee and/or covered spouse on the policy anniversary following the 70th birthday, however, premiums do not reduce as a result of this benefit change. *See the certificate of insurance and any riders for a complete list of available benefits, along with applicable provisions, exclusions and limitations.
Who do I contact with questions? For more information, please call the Voya Employee Benefits Customer Service Team at (800) 955-7736.
Critical Illness
44

Employee Coverage—Non-Tobacco User
Monthly Rates Includes Wellness Benefit Rider
Issue
Age $5,000 $10,000 $15,000 $20,000 $25,000 $30,000
25 $2.40 $4.80 $7.20 $9.60 $12.00 $14.40
25-29 $2.40 $4.80 $7.20 $9.60 $12.00 $14.40
30-34 $3.40 $6.80 $10.20 $13.60 $17.00 $20.40
35-39 $3.40 $6.80 $10.20 $13.60 $17.00 $20.40
40-44 $6.60 $13.20 $19.80 $26.40 $33.00 $39.60
45-49 $6.60 $13.20 $19.80 $26.40 $33.00 $39.60
50-54 $11.05 $22.10 $33.15 $44.20 $55.25 $66.30
55-59 $11.05 $22.10 $33.15 $44.20 $55.25 $66.30
60-64 $15.05 $30.10 $45.15 $60.20 $75.25 $90.30
65-69 $21.15 $42.30 $63.45 $84.60 $105.75 $126.90
70+ $28.85 $57.70 $86.55 $115.40 $144.25 $173.10
Spouse Coverage*—Non-Tobacco User
Monthly Rates Includes Wellness Benefit Rider
IssueAge
$5,000 $10,000 $15,000
Under 25 $2.90 $5.80 $8.70
25-29 $2.90 $5.80 $8.70
30-34 $4.00 $8.00 $12.00
35-39 $4.00 $8.00 $12.00
40-44 $8.20 $16.40 $24.60
45-49 $8.20 $16.40 $24.60
50-54 $15.00 $30.00 $45.00
55-59 $15.00 $30.00 $45.00
60-64 $20.20 $40.40 $60.60
65-69 $26.85 $53.70 $80.55
70+ $34.85 $69.70 $104.55
Children Coverage Monthly Rates
Includes Wellness Benefit Rider
Coverage Amount Rate
$5,000 $3.05
$10,000 $6.10
Critical Illness
How much does Critical Illness Insurance cost? See the chart below for the premium amounts. Rates shown are guaranteed until September 1, 2018. *Spouse rates are based on the age of the Spouse.
Employee Coverage—Tobacco User
Monthly Rates Includes Wellness Benefit Rider
Issue
Age $5,000 $10,000 $15,000 $20,000 $25,000 $30,000
25 $3.20 $6.40 $9.60 $12.80 $16.00 $19.20
25-29 $3.20 $6.40 $9.60 $12.80 $16.00 $19.20
30-34 $5.10 $10.20 $15.30 $20.40 $25.50 $30.60
35-39 $5.10 $10.20 $15.30 $20.40 $25.50 $30.60
40-44 $10.45 $20.90 $31.35 $41.80 $52.25 $62.70
45-49 $10.45 $20.90 $31.35 $41.80 $52.25 $62.70
50-54 $17.85 $35.70 $53.55 $71.40 $89.25 $107.10
55-59 $17.85 $35.70 $53.55 $71.40 $89.25 $107.10
60-64 $25.05 $50.10 $75.15 $100.20 $125.25 $150.30
65-69 $32.20 $64.40 $96.60 $128.80 $161.00 $193.20
70+ $43.85 $87.70 $131.55 $175.40 $219.25 $263.10
Spouse Coverage*—Tobacco User
Monthly Rates Includes Wellness Benefit Rider
IssueAge
$5,000 $10,000 $15,000
Under 25 $3.90 $7.80 $11.70
25-29 $3.90 $7.80 $11.70
30-34 $5.95 $11.90 $17.85
35-39 $5.95 $11.90 $17.85
40-44 $12.85 $25.70 $38.55
45-49 $12.85 $25.70 $38.55
50-54 $24.40 $48.80 $73.20
55-59 $24.40 $48.80 $73.20
60-64 $34.05 $68.10 $102.15
65-69 $41.45 $82.90 $124.35
70+ $53.35 $106.70 $160.05
45

A Health Savings Account is a tax-advantaged medical savings account available to employees who are enrolled in a high-deductible health plan. The funds contributed to the account are not subject to federal income tax at the time of deposit. Unlike a flexible spending account (FSA), funds roll over and accumulate year to year if not spent.
About this Benefit
HSA (Health Savings Account)
YOUR BENEFITS PACKAGE
The interest earned in an HSA is tax free.
DID YOU KNOW?
Money withdrawn for medical spending never falls under taxable income.
HSA BANK
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 46

HSA Bank has teamed up with your employer to create an affordable health coverage option that helps you save on healthcare expenses. This plan is only available for those who are participating in the Active Care 1-HD medical plan. You may not enroll in the MEDlink® plan if you participate in the HSA. Depending on your district, you may or may not be able to participate in the FSA plan if you participate in HSA. Medicare, Medicaid, and Tricare participants are not eligible to participate in an HSA. You can use your Health Savings Account (HSA) to pay for a wide range of IRS-qualified medical expenses for yourself, your spouse or tax dependents. An IRS-qualified medical expense is defined as an expense that pays for healthcare services, equipment, or medications. Funds used to pay for IRS-qualified medical expenses are always tax-free.
What is an HSA? A tax-advantaged savings account that you use to pay for
eligible medical expenses as well as deductible, co-insurance, prescriptions, vision and dental care. Allows you to save while reducing your taxable income.
Unused funds that will roll over year to year. There’s no “use it or lose it” penalty.
A way to accumulate additional retirement savings. After age 65, funds can be withdrawn for any purpose without penalty.
Using Funds Debit Card
You may use the card to pay merchants or service providers that accept VISA credit cards, so there is no need to pay cash up front and wait for reimbursements.
You can make a withdrawal at any time. Reimbursements for qualified medical expenses are tax free. If you are disabled or reach age 65, you can receive non-medical distributions without penalty, but you must report the distributions as taxable income. You may also use your funds for a spouse or tax dependent not covered by your HDHP.
2016 Annual HSA Contribution Limits Individual: $3,350 Family: $6,750 Catch-Up Contributions: Accountholders who meet the qualifications noted below are eligible to make an HSA catch-up contribution of an additional $1,000.
Health Savings accountholder
Age 55 or older (regardless of when in the year an accountholder turns 55)
Not enrolled in Medicare (if an accountholder enrolls in Medicare mid-year, catch contributions should be prorated)
Authorized Signers who are 55 or older must have their own HSA in order to make the catch-up contribution Monthly Fee: Your account will be charged a monthly fee of $1.75, waived with an average daily balance at or above $3,000.
Examples of Qualified Medical Expenses Surgery
Braces
Contact lenses
Dentures
Eyeglasses
Vaccines For a list of sample expenses, please refer to the CBEBC website at www.cbebc.com
HSA Bank Contact Information 605 N. 8th Street, Ste 320 Sheboygan, WI 53081 Phone: 800-357-6246 www.hsabank.com
HSA (Health Savings Account)
47

A Health Savings Account (HSA) is an individually-owned, tax-advantaged account that you can use to pay for current or future IRS-qualified medical expenses. With an HSA, you’ll have the potential to build more savings for healthcare expenses or additional retirement savings through self-directed investment options1.
How an HSA works: You can contribute to your HSA via payroll deduction,
online banking transfer, or by sending a personal check to HSA Bank. Your employer or third parties, such as a spouse or parent, may contribute to your account as well.
You can pay for qualified medical expenses with your HSA Bank Debit Card directly to your medical provider or pay out-of-pocket. You can either choose to reimburse yourself or keep the funds in your HSA to grow your savings.
Unused funds will roll over year to year. After age 65, funds can be withdrawn for any purpose without penalty (subject to ordinary income taxes).
Check balances and account information via HSA Bank’s Internet Banking 24/7.
Are you eligible for an HSA? If you have a qualified High Deductible Health Plan (HDHP) - either through your employer, through your spouse, or one you’ve purchased on your own - chances are you can open an HSA. Additionally:
You cannot be covered by any other non-HSA-compatible health plan, including Medicare Parts A and B.
You cannot be covered by TriCare.
You cannot have accessed your VA medical benefits in the past 90 days (to contribute to an HSA).
You cannot be claimed as a dependent on another person’s tax return (unless it’s your spouse).
You must be covered by the qualified HDHP on the first day of the month.
When you open an account, HSA Bank will request certain information to verify your identity and to process your application.
What are the annual IRS contribution limits? Contributions made by all parties to an HSA cannot exceed the annual HSA limit set by the Internal Revenue Service (IRS). Anyone can contribute to your HSA, but only the accountholder and employer can receive tax deductions on those contributions. Combined annual contributions for the accountholder, employer, and third parties (i.e., parent, spouse, or anyone else) must not exceed these limits2.
2016 Annual HSA Contribution Limits Individual = $3,350 Family = $6,750
Catch-up Contributions Accountholders who meet these qualifications are eligible to make an HSA catch-up contribution of $1,000: Health Savings accountholder; age 55 or older (regardless of when in the year an accountholder turns 55); not enrolled in Medicare (if an accountholder enrolls in Medicare mid-year, catch-up contributions should be prorated). Authorized signers who are 55 or older must have their own HSA in order to make the catch-up contribution. According to IRS guidelines, each year you have until the tax filing deadline to contribute to your HSA (typically April 15 of the following year). Online contributions must be submitted by 2:00 p.m., Central Time, the business day before the tax filing deadline. Wire contributions must be received by noon, Central Time, on the tax filing deadline, and contribution forms with checks must be received by the tax filing deadline.
How can you benefit from tax savings? An HSA provides triple tax savings3. Here’s how:
Contributions to your HSA can be made with pre-tax dollars and any after-tax contributions that you make to your HSA are tax deductible.
HSA funds earn interest and investment earnings are tax free.
When used for IRS-qualified medical expenses, distributions are free from tax.
IRS-Qualified Medical Expenses You can use your HSA to pay for a wide range of IRS-qualified medical expenses for yourself, your spouse, or tax dependents. An IRS-qualified medical expense is defined as an expense that pays for healthcare services, equipment, or medications. Funds used to pay for IRS-qualified medical expenses are always tax-free. HSA funds can be used to reimburse yourself for past medical expenses if the expense was incurred after your HSA was established. While you do not need to submit any receipts to HSA Bank, you must save your bills and receipts for tax purposes.
How the HSA Plan Works
48

How the HSA Plan Works
Examples of IRS-Qualified Medical Expenses4:
For assistance, please contact the Client Assistance Center 800-357-6246 Monday – Friday, 7 a.m. – 9 p.m., and Saturday, 9 a.m. - 1 p.m., CT www.hsabank.com | 605 N. 8th Street, Ste. 320, Sheboygan, WI 53081 1 Investment accounts are not FDIC insured, may lose value and are not a deposit or other obligation of, or guarantee by the bank. Investment losses which are replaced are subject to the annual contribution limits of the HSA. 2 HSA funds contributed in excess of these limits are subject to penalty and tax unless the excess and earnings are withdrawn prior to the due date, including any extensions for filing Federal Tax returns. Accountholders should consult with a qualified tax advisor in connection with excess contribution removal. The Internal Revenue Service requires HSA Bank to report withdrawals that are considered refunds of excess contributions. In order for the withdrawal to be accurately reported, accountholders may not withdraw the excess directly. Instead, an excess contribution refund must be requested from HSA Bank and an Excess Contribution Removal Form completed. 3 Federal Tax savings are available no matter where you live and HSAs are taxable in AL, CA, and NJ. HSA Bank does not provide tax advice. Consult your tax professional for tax‐related questions. 4 This list is not comprehensive. It is provided to you with the understanding that HSA Bank is not engaged in rendering tax advice. The information provided is not intended to be used to avoid Federal tax penalties. For more detailed information, please refer to IRS Publication 502 titled, “Medical and Dental Expenses”. Publications can be ordered directly from the IRS by calling 1-800-TAXFORM. If tax advice is required, you should seek the services of a professional. 5 Insurance premiums only qualify as an IRS-qualified medical expense: while continuing coverage under COBRA; for qualified long-term care coverage; coverage while receiving unemployment compensation; for any healthcare coverage for those over age 65 including Medicare (except Medicare supplemental coverage).
Acupuncture Alcoholism treatment Ambulance services Annual physical examination Artificial limb or prosthesis Birth control pills (by prescription) Chiropractor Childbirth/delivery Convalescent home (for medical treatment only) Crutches Doctor’s fees Dental treatments (including x-rays, braces, dentures, fillings, oral surgery) Dermatologist Diagnostic services Disabled dependent care Drug addiction therapy Fertility enhancement (including in-vitro fertilization) Guide dog (or other service animal)
Gynecologist Hearing aids and batteries Hospital bills Insurance premiums5
Laboratory fees Lactation expenses Lodging (away from home for outpatient care) Nursing home Nursing services Obstetrician Osteopath Oxygen Pregnancy test kit Podiatrist Prescription drugs and medicines (over-the-counter drugs are not IRS- qualified medical expenses unless prescribed by a doctor) Prenatal care & postnatal treatments Psychiatrist Psychologist Smoking cessation programs
Special education tutoring Surgery Telephone or TV equipment to assist the hearing or vision impaired Therapy or counseling Medical transportation expenses Transplants Vaccines Vasectomy Vision care (including eyeglasses, contact lenses, lasik surgery) Weight loss programs (for a specific disease diagnosed by a physician – such as obesity, hypertension, or heart disease) Wheelchairs X-rays
49

A Cafeteria Plan is designed to take advantage of Section 125 of the Internal Revenue Code. It allows you to pay certain qualified expenses on a pre-tax basis, thereby reducing your taxable income. You can set aside a pre-established amount of money per plan year in a Healthcare Flexible Spending Account (FSA). Funds allocated to a healthcare FSA must be used during the plan year or are forfeited unless your plan contains a $500 rollover or grace period provision.
Unlimited FSA (Non HSA Compatible) The funds in the unlimited healthcare FSA can be used to pay for eligible medical expenses like deductibles, co-payments, orthodontics, glasses and contacts.
About this Benefit
FSA (Flexible Spending Account)
YOUR BENEFITS PACKAGE
NBS
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com
FOR HSA VS. FSA COMPARISON
FLIP TO… PG. 11
50

NBS Flexcard You may use the card to pay merchants or service providers that accept MasterCard® credit cards, so there is no need to pay cash up front, then wait for reimbursement. If you are participating in the Dependent Care portion, the money isn’t loaded to the card. You must file web or paper claims or enroll in continual reimbursement.
Current plan participants: KEEP YOUR CARDS! NBS debit cards are good for 3 years. If you need a replacement card please contact NBS directly at (800) 274-0503.
New Plan Participants NBS will mail out your new benefit cards to the address listed in THEbenefitsHUB. They will be sent in unmarked envelopes so please watch for them as they should arrive within 21 business days of effective date. NBS debit cards are good for 3 years.
FSA Annual Contribution Max: $2,550
Dependent Care Annual Max: $5,000
Account Information: Participant Account Web Access: www.participant.nbsbenefits.com Participants may call NBS and talk to a representative during regular business hours, Monday-Friday, 8 am to 7 pm Central Time. Participants can also obtain account information using the Automated Voice Response Unit, 24 hours a day, 7 days a week at (801) 838-7324 or toll free (800) 274-0503. For immediate access to your account information at any time, log on to the NBS website www.NBSbenefits.com. Detailed claim history and processing status Health Care and Dependent Care account balances Health Care and Dependent Care account balances Claim forms, Direct Deposit form, worksheets, etc. Online webclaim FAQs
For a list of sample expenses, please refer to the CBEBC benefit website: www.cbebc.com
NBS Contact Information:
8523 South Redwood Road West Jordan, UT 84088 Phone (800) 274‐0503 Fax (800) 478‐1528 Email: [email protected]
When Will I Receive My Flex Card? Expect Flex Cards to be delivered to the address listed in THEbenefitsHUB near the end of September. Don’t forget, Flex Cards Are Good For 3 Years!
FSA (Flexible Spending Account)
DID YOU KNOW? FSAs use tax-free funds to help pay for your Health Care Expenses?
NBS Prepaid MasterCard® Debit Card
51

What is a Flexible Spending Account? A Flexible Spending Account allows you to save money by paying out-of-pocket health and/or dependent care related expenses with pre-tax dollars. Your contributions are deducted from your pay before taxes are withheld and your account is up fronted with an annual amount. Because you are taxed on a lower amount of pay, you pay less in taxes and you have more to spend.
How does a Flexible Spending Account Benefit Me? A Cafeteria plan enables you to save money on group insurance, health-related expenses, and dependent-care expenses. You may save as much as 35 percent on the cost of each benefit option! Eligible expenses must be incurred within the plan year and contributions are use-it-or- lose-it. Remember to retain all your receipts.
Health Care Expense Account Example Expenses:
Dependent Care Expense Account Example Expenses: Before and After School and/or Extended Day Programs
The actual care of the dependent in your home.
Preschool tuition.
The base costs for day camps or similar programs used as care for a qualifying individual.
What Can I Use My Flexible Spending Account On? For a full list of eligible expenses, please refer to www.cbebc.com
What Happens If I Don’t Use All of My Funds by The End of the Plan Year (August 31st)? Eligible expenses must be incurred within the plan year +75 day grace period. Contributions are use-it-or- lose-it. Remember to retain all your receipts (including receipts for card swipes). Please contact your benefits admin to determine if your district has the grace period or the $500 Roll-Over option. If your district does not have the roll-over, your plan contributions are use-it-or-lose-it.
How Do I File A Claim? In most situations, you will be able to swipe your card however, in the event you lose your card or are waiting to receive one, you can visit www.cbebc.com and complete the “Claim Form” to send to NBS or use the web or phone app to file online.
Hearing aids & batteries
Lab fees
Laser Surgery
Orthodontia Expenses
Physical exams
Pregnancy tests
Prescription drugs
Vaccinations
Vaporizers or humidifiers
Acupuncture
Body scans
Breast pumps
Chiropractor
Co-payments
Deductible
Diabetes Maintenance
Eye Exam & Glasses
Fertility treatment
First aid
FSA Frequently Asked Questions
How To Receive Your Dependent Care Reimbursement Faster.
A Direct Deposit form is available on the Benefits Website which will help you get reimbursed quicker!
52

How the FSA Plan Works
You designate an annual election of pre-tax dollars to be deposited into your health and dependent-care spending accounts. Your total election is divided by the number of pay periods in the Plan year and deducted equally from each paycheck before taxes are calculated. By the end of the Plan year, your total election will be fully deposited. However, you may make a claim for eligible health FSA expenses as soon as they are incurred during the Plan year. Eligible claims will be paid up to your total annual election even if you have not yet contributed that amount to your account.
Get Your Money 1. Complete and sign a claim form (available on our website) or an online webclaim. 2. Attach documentation; such as an itemized bill or an Explanation of Benefits (EOB) statement from a health insurance provider. 3. Fax or mail signed form and documentation to NBS. 4. Receive your non-taxable reimbursement after your claim is processed either by check or direct deposit.
NBS Flexcard—FSA Pre-paid Benefit Card Your employer may sponsor the use of the NBS Flexcard, making access to your flex dollars easier than ever. You may use the card to pay merchants or service providers that accept credit cards, so there is no need to pay cash up front then wait for reimbursement.
Account Information Participants may call NBS and talk to a representative during our regular business hours, Monday–Friday, 7am to 6pm Mountain Time. Participants can also obtain account information using the Automated Voice Response Unit, 24 hours a day, 7 days a week at (801) 838-7324 or toll free (800) 274-0503. For immediate access to your account information at any time, log on to our website www.NBSbenefits.com. Information includes:
Detailed claim history and processing status
Health Care and Dependent Care account balances
Claim forms, worksheets, etc.
Online Claim Submission
Enrollment Considerations After the enrollment period ends, you may increase, decrease, or stop your contribution only when you experience a qualifying “change of status” (marriage status, employment change, dependent change). Be conservative in the total amount you elect to avoid forfeiting money that may be left in your account at the end of the year. Your employer may allow a short grace period after the Plan year ends for you to submit qualified claims for any unused funds.
53

Identity theft protection monitors and alerts you to identity threats. Resolution services are included should your identity ever be compromised while you are covered.
About this Benefit
YOUR BENEFITS PACKAGE Identity Theft
ID WATCHDOG
An identity is stolen every
2 seconds,
and takes over
300 hours to resolve, causing an
average loss of $9,650.
DID YOU KNOW?
This is a general overview of your plan benefits. If the terms of this outline differ from your policy, the policy will govern. Additional plan details on covered expenses, limitations and exclusions are included in the summary plan description located on the
CBEBC Benefits Website: www.cbebc.com 54

Identity Theft
Identity theft can strike anyone, at any time. More than 11 million Americans were victimized by identity theft in 2011, including more than 500,000 children.
Identity theft devastates its victims financially. The average victim will lose $4,841, and spend an additional $1,400 in out-of-pocket expenses resolving their case.
Repairing the damage caused by identity theft is frustrating and time consuming. The average victim spends 330 hours repairing the damage from identity theft—the equivalent of working a full-time job for more than 2 months.
The impact of identity theft follows victims for years. 50% of identity theft victims experience trouble getting loans or credit cards as a result of identity theft. 12% of identity theft victims end up having warrants issued by law enforcement in their name for crimes committed by the identity thief.
Who’s Evaluating your Credit Report? Potential Creditors, Potential Employers, Insurance Companies, Current Creditors, Government Agencies
ID Watchdog Dual Monthly Pricing
Plus Platinum
Individual Plan $7.95 $11.95
Family Plan $14.95 $22.95
Basic & Advanced Identity Monitoring Cyber Monitoring Full-Service Identity Restoration Non-Credit Loan Monitoring Address Monitoring Credit Report Monitoring 100% Resolution Guarantee
ID Watchdog Services
55

NOTES
56

NOTES
57

www.cbebc.com
58