2015 09 13 cutaneous porphyrias Langendonk pat day selection … · 2016. 7. 10. · CUTANEOUS...
22
10/16/2015 1 Porphyria Janneke Langendonk Netherlands Porphyria Center Erasmus MC Rotterdam The Netherlands CUTANEOUS PORPHYRIAS 2 Clinical Manifestations Porphyrias 1. Attacks of neurological dysfunction due to accumulation ALA Cardinal feature abdominal pain Acute Intermittent, Hereditary Coproporphyria, Variegate Porphyria 2. Sunlight-induced skin lesions (photosensitivity) Porphyrin accumulation Uroporphyrin - Porphyria Cutanea Tarda Uroporphyrin - Congenital Erythropoietic Porphyria Coproporphyrinogen - Hereditary Coproporphyria, Protoporphyrinogen - Variegate Porphyria Protoporphyrin IX - EPP All Porphyrias Liver porphyrias ALA-D deficiency? Acute Intermittent Porphyria Hereditary Coproporphyria Variegate Porphyria Porphyria Cutanea Tarda Bone marrow porphyrias Congenital Erythropoietic Porphyria Erythropoietic Protoporphyria ACUTE Skin Acquired
Transcript of 2015 09 13 cutaneous porphyrias Langendonk pat day selection … · 2016. 7. 10. · CUTANEOUS...

10/16/2015
1
Porphyria
Janneke Langendonk
Netherlands Porphyria Center
Erasmus MC
Rotterdam
The Netherlands
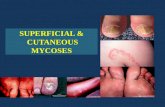
CUTANEOUS PORPHYRIAS
2
Clinical Manifestations Porphyrias
1. Attacks of neurological dysfunction due to accumulation ALA
Cardinal feature abdominal pain
� Acute Intermittent, Hereditary Coproporphyria, Variegate Porphyria
2. Sunlight-induced skin lesions (photosensitivity)
Porphyrin accumulation
� Uroporphyrin - Porphyria Cutanea Tarda
� Uroporphyrin - Congenital Erythropoietic Porphyria
� Coproporphyrinogen - Hereditary Coproporphyria,
� Protoporphyrinogen - Variegate Porphyria
� Protoporphyrin IX - EPP
All Porphyrias
� Liver porphyrias� ALA-D deficiency? � Acute Intermittent Porphyria� Hereditary Coproporphyria� Variegate Porphyria
� Porphyria Cutanea Tarda
� Bone marrow porphyrias� Congenital Erythropoietic Porphyria� Erythropoietic Protoporphyria
ACUTE
Skin
���� Acquired

10/16/2015
2
Age of onset� Hepatic porphyrias
� ALA-D deficiency� Acute Intermittent Porphyria after puberty� Hereditary Coproporphyria� Variegate Porphyria
� Porphyria Cutanea Tarda
� Erythropoietic porphyrias� Congenital Erythropoietic Porphyria� Erythropoietic Protoporphyria childhood
Cutaneous Porphyrias
� Erythropoeitic protoporphyria
� Congenital Erythropoietic
Porphyria
� Porphyria cutania tarda
Acute porphyrias with skin
symptoms
� Hereditary coproporphyria
� Variegate porphyria
� Pain - EPP
� Blisters
� CEP
� PCT
� HCP
� VP
6
Tetrapyrolles: Pigments of life
compounds which make grass green and blood red
(Hans Fischer 1930 )
Skin functions
� Protection
� Immunological barrier
� Large endocrine organ
� Different layers
8

10/16/2015
3
Layers of the skin
9
Layers of the skin
10
Layers of the skin
11
Cutaneous Porphyrias
� Hereditary Coproporphyria� Variegate Porphyria
� Porphyria Cutanea Tarda� Congenital Erythropoietic Porphyria
� Erythropoietic Protoporphyria �
Blisters
•No Blisters•Burning pain•Erythema•Edema

10/16/2015
4
CONGENITAL ERYTHROPOIETIC PORPHYRIA
Congenital Erythropoietic Porphyria
Rare
Severe – mild disease
After light exposure
� Blistering resulting in scarring and skin atrophy
� Social isolation
Multi system disease
� Anemia
� Large spleen
� Conjunctivitis: eyes (blind)
� Contractures
� Low vitamin D
� Osteoporosis
� Orthodontia: teeth
Uro I
Layers of the skin
16

10/16/2015
5
17
Both mother and father are carriers
25 % affectedVariable
Other genesEnvironment
Copyright: US national library of Medicine
Congenital Erythropoietic Porphyria
Treatment
History and physical examination
� Skin / hair / eyes / spleen / joints contractures
Blood exam: iron, vitamine D, porphyrins, DNA
On indication : radiological exams of spleen and bone
� Dermatologist, Ophthalmologist, Rehabilitation/ Ergo therapy, Dentist
� Education: Skin and eyes protection
� Education of social network
Katugampola CEP management guidelines Br J Dermat. 2012
Alternative treatment options
� Variable disease
� Bone marrow transplantation (HSCT)
19
PORPHYRIA CUTANEA TARDA

10/16/2015
6
Porphyria cutanea tarda
� Accumulation of uroporphyrins
� Produced by the liver
� Blisters – erosions – easy bruising
Uro I
Layers of the skin
23
Porphyria cutanea tarda
Acquired disease in most cases
� Alcohol (> 60%)
� Iron* (>90%)
� Autosomal dominant URO-D defect (20-25%)
� Hepatitis B/ C (differs per country)
� HIV
� High dose estrogens
� Chemical compounds*

10/16/2015
7
25
An affected parent50%
VariablePenetrance
Other genesEnvironment
Examples:
Acute porphyrias
Copyright: US national library of Medicine
Porphyria cutanea tarda

10/16/2015
8
29
Hypertrichosis in PCT
From internet
Urine Faeces
URO Icopro
PCT
Plasma
Biochemistry Cutaneous Porphyria
URO IURO Icopro
�Next step: enzymes activity or DNA
Porphyria cutanea tarda
Complications
Liver cancer: hepatocellular carcinoma
Mostly attributable to underlying liver disease

10/16/2015
9
Porphyria Cutanea Tarda
Treatment1. Skin protection: sunlight2. Phlebotomy
Phlebotomy
34
Porphyria Cutanea Tarda
Treatment1. Skin protection: sunlight2. Phlebotomy3. Chloroquine : second line therapy
(Antimalarian drug)
Treatment of underlying condition� Alcohol limitation until remission� Hepatitis / HIV
PCT is a treatable condition
� Treatment can be stopped after 1 year
� Some need lifelong phlebotomies
36

10/16/2015
10
ERYTHROPOÏETIC PROTOPORPHYRIA
Patients are limited in their choices and learn to restrict daily activities by
avoiding exposure to sunlight
Immediately withdrawing into the dark when prodromal tingling and burning sensations occur
Various treatments, none have proved satisfactory
Unique in the severity of the pain induced by often brief exposure to light
Symptoms start in childhood
Diagnostic delay, average 20 years
Low Quality of life, variable
38
Erythropoïetic Protoporphyria (EPP)
Erythropoïetic Protoporphyria (EPP)
� Rare inherited photosensitivity disorder
� Protoporfyrin IX in red blood cells
� Ferrochelatase or ALAS2
Typical for EPP symptoms
� Prodromal Symptoms (a warning)
> pain, edema, erythema, burning and crusts
� Pain relieve difficult: cold, dark,
40

10/16/2015
11
‘Buckets of light’
� After light exposure tolerance to additional light exposure is lower
41
43
Both mother and father are carriers
25 % affectedVariable
Other genesEnvironment
Copyright: US national library of Medicine
44
Men are affectedWomen can be affected
Daughters of affectedfathers are always carriers and can be affected.� Their sons have 50% chance to be affected
Sons of affected fathers are never affected or carrier
• Different mutations• Other genes• Environment
• Copyright: US nationallibrary of Medicine

10/16/2015
12
EPP
� Blue light
� Often no scars
� Waxy skin
UVUVUVUV----CCCC
WAXY SKIN
46
Urine Faeces
URO Icopro
Normal * Proto
PCT
EPP
Plasma
Making the diagnosis?
URO I
Proto in ery’s
URO Icopro
�Next step: enzymes activity or DNA
Erythropoietic protoporphyria
Blood vessels

10/16/2015
13
Layers of the skin
49
Courtesy of the patient andprof Wilson
Pain
Avoidance
No tanning
More pain afterexposure
Fear of pain in EPP patients
51
Life and coping in EPP
52The mean age at diagnosis is 22 years and the mean delay from the onset of symptoms to diagnosis was 18 years (0–49).

10/16/2015
14
EPP patients
Unique condition with pain and low QoL
No effective acceptable standard of care
Afamelanotide is effective and safe
Afamelanotide convincingly improves QoL
53
Details
� Visible blue light spectrum
� Glass does not absorb visible light
� Unimaginable- Incomparable
� Light is basic to life
Standard care for EPP
Totally covering all skin
Long sleeves and trousers, gloves, hat / balaclava
Curtains, special filters
54
Complications
� Low quality of life
� Vitamine D deficiency: 60%
� Osteoporose: 20% vs < 1% (O12)
� Anemia: frequent
� Liver failure: rare, 2%
55
Sunlight, vitamin D and bone mineral density

10/16/2015
15
Riskfactors for osteoporosis
• Age
• Smoking
• Alcohol
• Rest
• Low calcium intake
• Low vitamin D
DXA
hip
spine
Consequences of osteoporosis
• Osteoporotic fractures occur in general osteoporosis studies in
� 30% or ⅓ of women
�20% or 1 in 5 of men with osteoporosis
• Fractures of spine and hip after minimal trauma
• Pain, suffering and high mortality
Bone density in the population
OsteoporosisOsteopenia Normal
84%15%0.6%

10/16/2015
16
Results
Mean: -0.87 P = 0.002 Mean: -0.44 P = 0.006
23% 77% 7% 93%
Summary results on Bone
• Significant lower bone density compared to reference population
• 23% osteoporosis (expected 0.6%)
• 36% osteopenia (expected 15%)
• One EPP patient with proven multiple osteoporotic fractures
Evaluation classical risk factors
• ~50% vitamin D deficiency (even in the treated patients)
• Lower physical ‘bone’ activity level
• No difference in other classical risk factors
O12 Biewenga Tuesday 17.00
EPP patients and osteoporosis
� Vitamin D and calcium should be taken
� Awareness of osteoporosis risk: asses bone density: DXA scan
Additional
� Consider additional treatment for osteoporosis
� “Normal” risk activities in those with osteoporosis/ fracture risk
63
EPP Care path
Yearly visit • Liver ultrasound
• Bone mineral density (DXA)
Education • Skin and eye protection
• Gall stones
• Increase in symptoms
• Osteoporosis prevention and treatment
• ? Vaccination for hepatitis A&B
• Alcohol/ drugs
• Surgery
• Pregnancy
• Genetic counseling

10/16/2015
17
Research
� Working on bone density
� Working on measuring stress levels in hair
� Working on a fund application
65
Non-satisfactory treatment options
Limit exposure to light
Skin and eye protection: Covering clothing sunglasses
� Reflective sunscreen: colored cream; Tin-oxide, Zink-oxide-cremes
� Beta-carotene: orange discoloration of skin
� UV-B therapy; solar treatment
Free radical elimination
� Beta-Carotene
� Cysteine , acetyl cysteine, vitamin E, vitamin C
� Antihistamine
Stem cell transplantation (bone marrow transplantation ) 66
Afamelanotide Implant
67
Analogue α-MSH
Binds to MC1R
Production of photoprotective eumelanin
Absorbs, scatters, and quenches light
Scavenges free radicals
Neutral dense filter

10/16/2015
18
69
Afamelanotide – studies
Decreased pain severity +
- Reduced photo toxicity
- Prolonged sunlight exposure (7 min over 9 mo.)
- Increased melanin density
- Improved quality of life
� Safe
� Adverse Effects mild & comparable treatment vs. pla cebo
- Nausea & Flushing more frequent in treatment group
Implications of marketing authorisation: by Prof Mind er
Steps necesary before start
� EMA European Medicine Agency
� CHMP Commision For Human Medicine Products
� Approval 2014 september: positive advise to European commision
� EC gave marketing authorisation in december 2014 ☺
� Exceptional circumstances: ;-( ……. ……. …….
71
Steps necesary before start
� Exceptional circumstances
Pharmacovigilance Risk Assessment Committee (PRAC)
� EMA committee
� Responsible for monitoring safety issues for human medicines
� Current state: awaiting decisions by PRAC
72

10/16/2015
19
Rules rule Where are they?
www.ema.europa.eu
‘Exceptional Circumstances’ ?
� To obtain complete information about the benefits of Scenesse
� A new review Every year by EMA
� Treatment by porphyria centers
� Monitor side effects
� Monitor effects!
� Registry
� Training centersMANY MORE DETAILS BY PROFESSOR MINDER
And/ But …..
A registry also gives opportunities
Monitoring EPP: more knowledge -- more details
76

10/16/2015
20
After afamelanotide release??
� Registry set up
� Training: both in treatment and in administrative issues
And local government hurdles will need to be taken
Netherlands:
� February 2015 kick-off meeting: with all parties involved including the
patient organisation
�Financial risk assesment by ZiN
�Elaborative Administrative details: ‘Add-on ‘
� Outpatient clinic setup/ staffing : minor
77
Concerns after release
Exposure to UV lightSkin: inflammation (sunburn)
pigment-formation
vitamin D productionaging � wrinklesskincancer
Eye: retinal damage/ macula degeneration
General advise: not to long in the sun, not between 12-15.00Start using UV sun creme SPF > 30+
Sunglasses
79
Skin tan without pain More time outdoors, less fearFreedom for patients to go out on sunny daysChanges in career options
80

10/16/2015
21
lab
Netherlands porphyria center
LaboratoryE. FriesemaF. de RooijA. EdixhovenR. KooleA. BouhuizenJ van Miert
* Prof P. Wilson
ClinicM. LangeveldJ. Langendonk
Research: R. Neeleman
Clinical genetics: F Petrij
Pediatrics: M Williams
Dermatology : E. PrensS. Pasmans
Gastro enterology
de Knegt & Metselaar
Nurse: S. Poldermans
Students: M. BiewengaI. Suijker, R. Matawlie
lab
Outpatient - & clinic
Thank you

10/16/2015
22
Websites
� www.porphyria-europe.com� site of European Porphyria network: EPNET
� Information for patients and professionals
� In several languages
� Information on locations of reference centers in Europe