![Draft NHS Model Complaints Handling Procedure [word Web viewAll anonymous complaints are subject to this procedure. ... Draft NHS Model Complaints Handling Procedure [word version]](https://static.fdocuments.in/doc/165x107/5a78283b7f8b9a4b538e8042/draft-nhs-model-complaints-handling-procedure-word-doc-file-web-viewall.jpg)
2014 Test Procedure Draft for 170.314(b)(2 -
22
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012 1 Test Procedure for §170.314 (b)(2) Transitions of care – create and transmit summary care records This document describes the test procedure for evaluating conformance of complete EHRs or EHR modules to the certification criteria defined in 45 CFR Part 170 Subpart C of the Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology, Final Rule. The document 1 is organized by test procedure and derived test requirements with traceability to the normative certification criteria as described in the Overview document located at [available when final]. The test procedures may be updated to reflect on-going feedback received during the certification activities. The HHS/Office of the National Coordinator for Health Information Technology (ONC) has defined the standards, implementation guides and certification criteria used in this test procedure. Applicability and interpretation of the standards, implementation guides and certification criteria to EHR technology is determined by ONC. Testing of EHR technology in the Permanent Certification Program, henceforth referred to as the ONC HIT Certification Program 2 , is carried out by National Voluntary Laboratory Accreditation Program-Accredited Testing Laboratories (ATLs) as set forth in the final rule establishing the Permanent Certification Program (Establishment of the Permanent Certification Program for Health Information Technology, 45 CFR Part 170; February 7, 2011.) Questions or concerns regarding the ONC HIT Certification Program should be directed to ONC at [email protected]. CERTIFICATION CRITERIA This Certification Criterion is from the Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology, Final Rule issued by the Department of Health and Human Services (HHS) on September 4, 2012. §170.314(b)(2) Transitions of care - create and transmit summary care records (i) Create. Enable a user to electronically create a transition of care/referral summary formatted (2) Transitions of care – create and transmit transition of care/referral summaries. (i) Create. Enable a user to electronically create a transition of care/referral summary formatted according to the standard adopted at § 170.205(a)(3) that includes, at a minimum, the Common MU Data Set and the following data expressed, where applicable, according to the specified standard(s): 1 Disclaimer: Certain commercial products may be identified in this document. Such identification does not imply recommendation or endorsement by ONC. 2 Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology, Final Rule
Transcript of 2014 Test Procedure Draft for 170.314(b)(2 -
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
1
Test Procedure for §170.314 (b)(2) Transitions of care – create and transmit summary care records
This document describes the test procedure for evaluating conformance of complete EHRs or EHR
modules to the certification criteria defined in 45 CFR Part 170 Subpart C of the Health Information
Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health
Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health
Information Technology, Final Rule. The document1 is organized by test procedure and derived test
requirements with traceability to the normative certification criteria as described in the Overview document
located at [available when final]. The test procedures may be updated to reflect on-going feedback
received during the certification activities.
The HHS/Office of the National Coordinator for Health Information Technology (ONC) has defined the
standards, implementation guides and certification criteria used in this test procedure. Applicability and
interpretation of the standards, implementation guides and certification criteria to EHR technology is
determined by ONC. Testing of EHR technology in the Permanent Certification Program, henceforth
referred to as the ONC HIT Certification Program2, is carried out by National Voluntary Laboratory
Accreditation Program-Accredited Testing Laboratories (ATLs) as set forth in the final rule establishing
the Permanent Certification Program (Establishment of the Permanent Certification Program for Health
Information Technology, 45 CFR Part 170; February 7, 2011.)
Questions or concerns regarding the ONC HIT Certification Program should be directed to ONC at
CERTIFICATION CRITERIA
This Certification Criterion is from the Health Information Technology: Standards, Implementation
Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions
to the Permanent Certification Program for Health Information Technology, Final Rule issued by the
Department of Health and Human Services (HHS) on September 4, 2012.
§170.314(b)(2) Transitions of care - create and transmit summary care records
(i) Create. Enable a user to electronically create a transition of care/referral summary formatted (2)
Transitions of care – create and transmit transition of care/referral summaries.
(i) Create. Enable a user to electronically create a transition of care/referral summary formatted
according to the standard adopted at § 170.205(a)(3) that includes, at a minimum, the Common MU
Data Set and the following data expressed, where applicable, according to the specified standard(s):
1 Disclaimer: Certain commercial products may be identified in this document. Such identification does not imply
recommendation or endorsement by ONC. 2 Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic
Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology, Final Rule
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
2
(A) Encounter diagnoses. The standard specified in § 170.207(i) or, at a minimum, the version of
the standard specified § 170.207(a)(3);
(B) Immunizations. The standard specified in § 170.207(e)(2);
(C) Cognitive status;
(D) Functional status; and
(E) Ambulatory setting only. The reason for referral; and referring or transitioning provider’s name
and office contact information.
(F) Inpatient setting only. Discharge instructions.
(ii) Transmit. Enable a user to electronically transmit the transition of care/referral summary created in
paragraph (b)(2)(i) of this section in accordance with:
(A) The standard specified in § 170.202(a).
(B) Optional. The standards specified in § 170.202(a) and (b).
(C) Optional. The standards specified in § 170.202(b) and (c).
Per Section III.A of the preamble of the Health Information Technology: Standards, Implementation
Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions
to the Permanent Certification Program for Health Information Technology, Final Rule, the 2014 Edition of
this Certification Criterion is classified as revised from the 2011 Edition. This Certification Criterion meets
at least one of the three factors of revised certification criteria: (1) the certification criterion includes
changes to capabilities that were specified in the previously adopted certification criterion, (2) the
certification criterion has a new mandatory capability that was not included in the previously adopted
certification criterion, or (3) the certification criterion was previously adopted as “optional” for a particular
setting and is subsequently adopted as “mandatory” for that setting.
Per Section III.A of the preamble of the Health Information Technology: Standards, Implementation
Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions
to the Permanent Certification Program for Health Information Technology, Final Rule where the
transitions of care – create and transmit summary care records certification criterion is discussed:
“… based on stakeholder feedback received after the publication of the S&CC July 2010 final
rule, we stated our belief that the criterion should be split into two separate certification criteria
based on the capabilities required. We explained that this approach would provide developers
greater flexibility for certification…”
“…we have decided to finalize our proposal to allow for the use of ICD-10-CM to represent
encounter diagnoses in addition to permitting SNOMED- CT…”
“…In instances where the EP, EH, or CAH’s CEHRT receives data from an outside source, we
acknowledge that requiring the CEHRT to translate the data into an adopted standard vocabulary
could alter its intended meaning … the responsibility of the sending EP or EH/CAH is to send
information with standard terms, and in the case when such standard terms are not used, it
should not be the responsibility of the receiving EP or EH to translate local or proprietary codes
into standard codes …”
“…for the purposes of certification, and demonstrating compliance with this certification criterion,
EHR technology will need to be tested and certified as being able to apply all of the adopted
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
3
standard vocabularies to data required to be included in a Consolidated CDA formatted transition
of care/referral summary …”
“…Further, we expect that the National Coordinator will approve a test procedure for the
transitions of care certification criteria that rigorously assesses EHR technology’s ability to
transmit and receive electronic health information according to the adopted transport, content
exchange, and vocabulary standards. We anticipate that this test procedure will be specified to
ascertain the EHR technology’s ability to engage in standards-based exchange with any other
EHR technology that has also implemented the standards we have adopted …”
“…We acknowledged that care plan, additional care team members, referring or transitioning
provider’s name and contact information as well as certain hospital discharge information are not
explicitly required to be captured by separate certification criteria, unlike most other data included
in the summary care record. We noted that the ability to capture these data elements is both
implicit and necessary to satisfy this certification criterion …”
CHANGES FROM 2011 TO 2014 EDITION
Per Section III.A of the preamble of the Health Information Technology: Standards, Implementation
Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions
to the Permanent Certification Program for Health Information Technology, Final Rule where the
transitions of care – create and transmit summary care records certification criterion is discussed:
“…we proposed to adopt the Consolidated CDA for this certification criterion because its
template structure can accommodate the formatting of a summary care record that includes all of
the data elements that CMS proposed be available for inclusion in a summary care record.”
“We proposed that EHR technology would need to be capable of transmitting a summary care
record according to both of the Direct Project’s specifications for secure transport. We also
proposed to adopt as an optional standard at § 170.202(a)(3) the SOAP-Based Secure Transport
RTM version 1.03 which was developed under the nationwide health information network
Exchange Initiative and to which we stated EHR technology should be able to be certified.”
“We have adopted, as proposed, that the Applicability Statement for Secure Health Transport
specification be a required condition of certification as part of this certification criterion. We have
removed the XDR and XDM for Direct Messaging specification as also being required in lieu of a
broader range of options for certification.”
“Additionally…, all EHR technology used by EPs, EHs, and CAHs and that meets the CEHRT
definition will, at a minimum, be capable of SMTP-based exchange.”
“…we have adopted the updated version of this specification that was established by the
stakeholder community during this final rule’s drafting.”
“…we have adopted two optional certification approaches for transport standards…
o The first option would permit EHR technology to be certified as being in compliance with
our original proposal: certification to both the Applicability Statement for Secure Health
Transport specification and the XDR and XDM for Direct Messaging specification.
3 http://modularspecs.siframework.org/NwHIN+SOAP+Based+Secure+Transport+Artifacts
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
4
o The second option would permit EHR technology to be certified to: the Simple Object
Access Protocol (SOAP)-Based Secure Transport Requirements Traceability Matrix
(RTM) version 1.0 standard and the XDR and XDM for Direct Messaging specification.”
“We have included the XDR and XDM for Direct Messaging specification as a required
specification for both of these options.”
INFORMATIVE TEST DESCRIPTION
This section provides an informative description of how the test procedure is organized and conducted. It
is not intended to provide normative statements of the certification requirements.
ONC provides the test data for this test procedure. This test procedure is organized into two required
sections (and two optional sections):
Create – evaluates the capability to create a transition of care/referral summary from the EHR in C-
CDA format. Included in the test procedure is an evaluation of the capability to use specified
vocabularies as defined by the referenced standards.
o For both ambulatory and inpatient settings: the Common MU Data Set data with named
standards as appropriate (in their English representation if they associate with a
vocabulary/code set):
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
o For ambulatory settings only: encounter diagnoses, immunizations, cognitive status,
functional status, reason for referral, referring provider’s name and contact information
o For inpatient settings only: encounter diagnoses, immunizations, cognitive status, functional
status, and discharge instructions
o The Vendor creates an existing patient record in the EHR technology with health information
based on the ONC-provided test data
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
5
o Tester, logs into the online application as a provider and creates a referral summary/transition
of care
Transmit - Evaluates the capability of EHR technology to allow a provider to electronically transmit the
health information created in the “Create” section of the test procedure another provider or next
setting of care:
o The Tester logs in to the EHR's online technology as the provider who created the
information in the “Create” step
o The Tester verifies that the EHR can discover certificates from other parties in either DNS
CERT records or LDAP servers
o Using the Vendor-identified function(s), the Tester verifies that the EHR is able to create and
store a listing of Direct recipient address(es)
o Using the Vendor-identified function(s), the Tester causes the health information in C-CDA
format to be transmitted to a third party using the Direct transport standard, based on ONC
supplied test information
o The Tester verifies successful transmission and receipt of the health information, and that the
health information can be successfully decrypted
o The Tester verifies that the information transmitted is in conformance with the C-CDA
Using the Vendor-identified EHR function(s), the Tester imports the health
information into the NIST Transport Test Tool
Using the Validation Report produced by the NIST Transport Test Tool, the Tester
verifies that the Implementation Guide conformance requirements tested are met,
and that the named standard vocabularies have been used where applicable for data
in the Common MU Data Set
o Using the provided test data, the Tester verifies that the data rendered in the transmitted C-
CDA are complete and accurate, and that the data in the Common MU Data Set are shown in
their English representation if they associate with a vocabulary/code set
o Optional: Using the Vendor-identified function(s), the Tester causes the health information in
human readable format or C-CDA format to be transmitted to a third party using Direct and
the Cross-Enterprise Document Reliable Interchange (XDR) and Cross-Enterprise Document
Media Interchange (XDM) for Direct Messaging Specification, based on ONC supplied test
information
Optional: Using the Vendor-identified function(s), the Tester causes the health information in
human readable format or C-CDA format to be transmitted to a third party using the SOAP-
Based Secure Transport RTM version 1.0 and XDR, based on ONC supplied test information
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
6
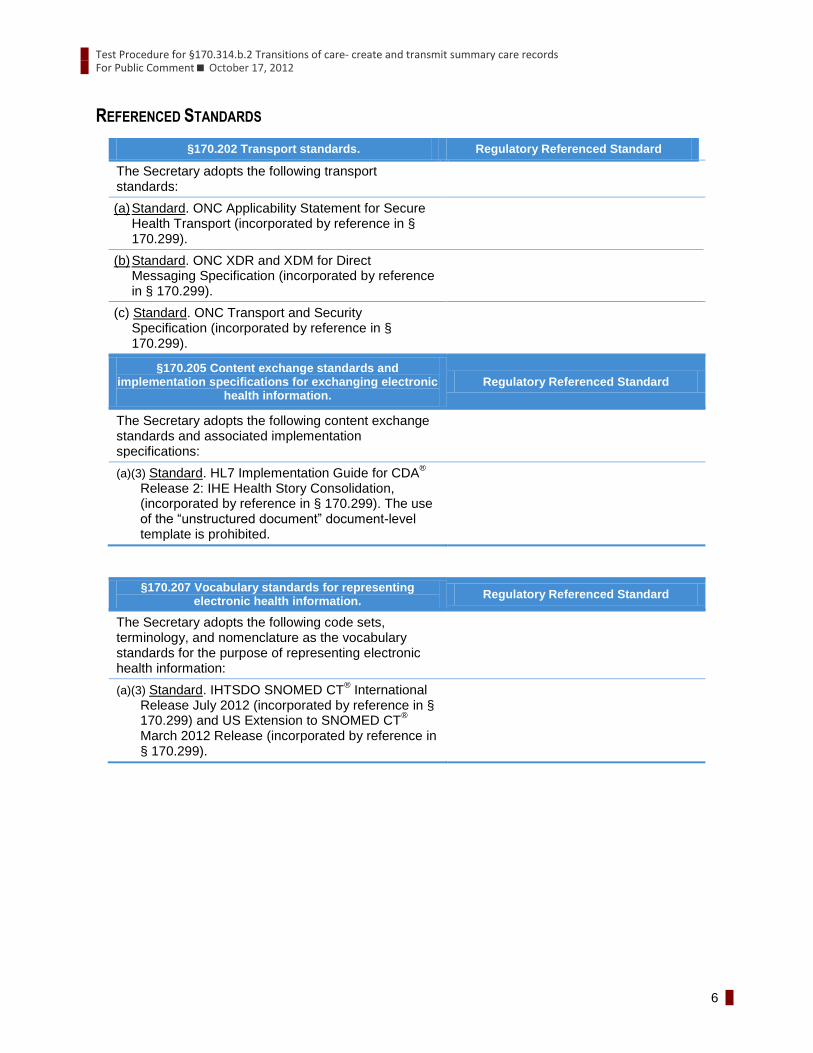
REFERENCED STANDARDS
§170.202 Transport standards. Regulatory Referenced Standard
The Secretary adopts the following transport standards:
(a) Standard. ONC Applicability Statement for Secure Health Transport (incorporated by reference in § 170.299).
(b) Standard. ONC XDR and XDM for Direct Messaging Specification (incorporated by reference in § 170.299).
(c) Standard. ONC Transport and Security Specification (incorporated by reference in § 170.299).
§170.205 Content exchange standards and implementation specifications for exchanging electronic
health information. Regulatory Referenced Standard
The Secretary adopts the following content exchange standards and associated implementation specifications:
(a)(3) Standard. HL7 Implementation Guide for CDA®
Release 2: IHE Health Story Consolidation, (incorporated by reference in § 170.299). The use of the “unstructured document” document-level template is prohibited.
§170.207 Vocabulary standards for representing electronic health information.
Regulatory Referenced Standard
The Secretary adopts the following code sets, terminology, and nomenclature as the vocabulary standards for the purpose of representing electronic health information:
(a)(3) Standard. IHTSDO SNOMED CT® International
Release July 2012 (incorporated by reference in § 170.299) and US Extension to SNOMED CT
®
March 2012 Release (incorporated by reference in § 170.299).
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
7
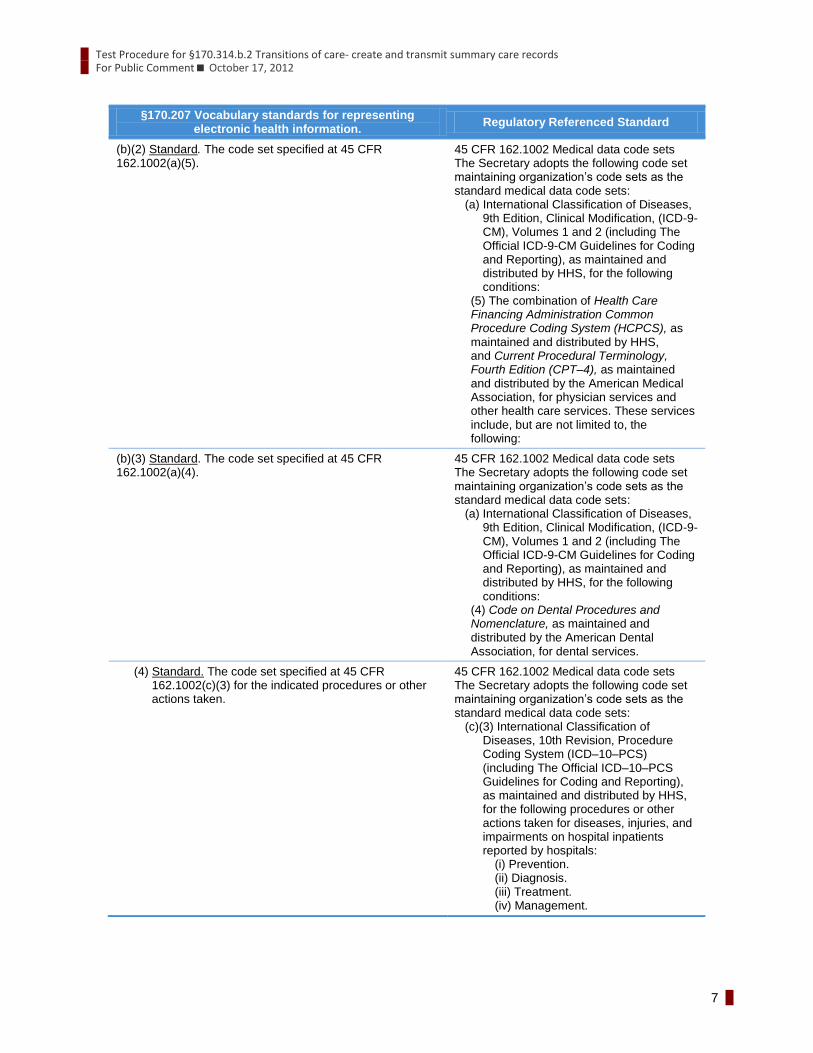
§170.207 Vocabulary standards for representing electronic health information.
Regulatory Referenced Standard
(b)(2) Standard. The code set specified at 45 CFR 162.1002(a)(5).
45 CFR 162.1002 Medical data code sets The Secretary adopts the following code set maintaining organization’s code sets as the standard medical data code sets:
(a) International Classification of Diseases, 9th Edition, Clinical Modification, (ICD-9- CM), Volumes 1 and 2 (including The Official ICD-9-CM Guidelines for Coding and Reporting), as maintained and distributed by HHS, for the following conditions:
(5) The combination of Health Care Financing Administration Common Procedure Coding System (HCPCS), as maintained and distributed by HHS, and Current Procedural Terminology, Fourth Edition (CPT–4), as maintained and distributed by the American Medical Association, for physician services and other health care services. These services include, but are not limited to, the following:
(b)(3) Standard. The code set specified at 45 CFR 162.1002(a)(4).
45 CFR 162.1002 Medical data code sets The Secretary adopts the following code set maintaining organization’s code sets as the standard medical data code sets:
(a) International Classification of Diseases, 9th Edition, Clinical Modification, (ICD-9- CM), Volumes 1 and 2 (including The Official ICD-9-CM Guidelines for Coding and Reporting), as maintained and distributed by HHS, for the following conditions:
(4) Code on Dental Procedures and Nomenclature, as maintained and distributed by the American Dental Association, for dental services.
(4) Standard. The code set specified at 45 CFR 162.1002(c)(3) for the indicated procedures or other actions taken.
45 CFR 162.1002 Medical data code sets The Secretary adopts the following code set maintaining organization’s code sets as the standard medical data code sets:
(c)(3) International Classification of Diseases, 10th Revision, Procedure Coding System (ICD–10–PCS) (including The Official ICD–10–PCS Guidelines for Coding and Reporting), as maintained and distributed by HHS, for the following procedures or other actions taken for diseases, injuries, and impairments on hospital inpatients reported by hospitals:
(i) Prevention. (ii) Diagnosis. (iii) Treatment. (iv) Management.
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
8
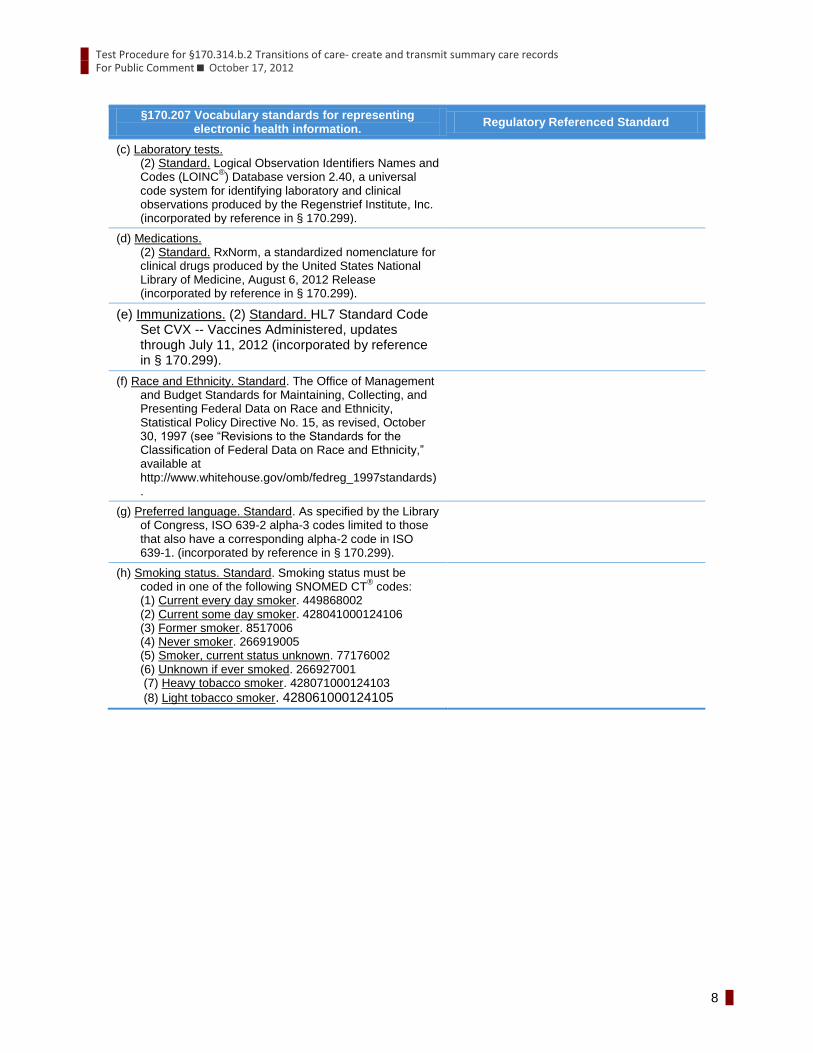
§170.207 Vocabulary standards for representing electronic health information.
Regulatory Referenced Standard
(c) Laboratory tests. (2) Standard. Logical Observation Identifiers Names and Codes (LOINC
®) Database version 2.40, a universal
code system for identifying laboratory and clinical observations produced by the Regenstrief Institute, Inc. (incorporated by reference in § 170.299).
(d) Medications. (2) Standard. RxNorm, a standardized nomenclature for clinical drugs produced by the United States National Library of Medicine, August 6, 2012 Release (incorporated by reference in § 170.299).
(e) Immunizations. (2) Standard. HL7 Standard Code Set CVX -- Vaccines Administered, updates through July 11, 2012 (incorporated by reference in § 170.299).
(f) Race and Ethnicity. Standard. The Office of Management and Budget Standards for Maintaining, Collecting, and Presenting Federal Data on Race and Ethnicity, Statistical Policy Directive No. 15, as revised, October 30, 1997 (see “Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity,” available at http://www.whitehouse.gov/omb/fedreg_1997standards).
(g) Preferred language. Standard. As specified by the Library of Congress, ISO 639-2 alpha-3 codes limited to those that also have a corresponding alpha-2 code in ISO 639-1. (incorporated by reference in § 170.299).
(h) Smoking status. Standard. Smoking status must be coded in one of the following SNOMED CT
® codes:
(1) Current every day smoker. 449868002 (2) Current some day smoker. 428041000124106 (3) Former smoker. 8517006 (4) Never smoker. 266919005 (5) Smoker, current status unknown. 77176002 (6) Unknown if ever smoked. 266927001 (7) Heavy tobacco smoker. 428071000124103
(8) Light tobacco smoker. 428061000124105
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
9
§170.207 Vocabulary standards for representing electronic health information.
Regulatory Referenced Standard
(i) Encounter diagnoses. Standard. The code set specified at 45 CFR 162.1002(c)(2) for the indicated conditions.
45 CFR 162.1002 Medical data code sets. The Secretary adopts the following maintaining organization’s code sets as the standard medical data code sets: (c)(2) International Classification of
Diseases, 10th Revision, Clinical Modification (ICD–10–CM) (including The Official ICD–10–CM Guidelines for Coding and Reporting), as maintained and distributed by HHS, for the following conditions: (i) Diseases. (ii) Injuries. (iii) Impairments. (iv) Other health problems and their
manifestations. (v) Causes of injury, disease,
impairment, or other health problems.
NORMATIVE TEST PROCEDURES
Derived Test Requirements
DTR170.314.b.2–1: Create Referral Summary/Transition of Care
DTR170.314.b.2–2: Transmit Health Information to a Third Party Using Direct
DTR170.314.b.2–3: Transmit Health Information to a Third Party Using Direct and XDM Validation
(Optional)
DTR170.314.b.2–4: Transmit Health Information to a Third Party Using SOAP Protocols (Optional)
DTR170.314.b.2–1: Create Referral Summary/Transition of Care
Required Vendor Information
VE170.314.b.2 – 1.01: Using ONC-supplied test data, the Vendor shall create a test patient with an
existing record in the EHR to be used for this test as indicated in TD170.314.b.2 –
Ambulatory (ambulatory only) or TD170.314.b.2 – Inpatient (inpatient only)
VE170.314.b.2 – 1.02: Vendor shall identify a provider with authorized access to the patient’s record
VE170.314.b.2 – 1.03: Vendor shall identify the EHR function(s) that are available for a provider to view
health information including the named data elements as well as the Common MU
Data Set with associated vocabulary standards and create a referral
summary/transition of care document
Required Test Procedure
TE170.314.b.2 – 1.01: Using the Vendor-identified EHR function(s), the Tester shall access the ONC-
supplied test patient’s record as the provider
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
10
TE170.314.b.2 – 1.02: Using the Vendor-identified EHR function(s), the Tester shall view and create
patient information that includes:
Ambulatory Summary: Common MU Data Set and the following data
elements: encounter diagnoses, immunizations, cognitive status, functional
status, reason for referral, referring provider’s name and contact information
(Ambulatory EHR Only)
Inpatient Summary: Common MU Data Set and encounter diagnoses,
immunizations, cognitive status, functional status, and discharge instructions
(Inpatient EHR Only)
TE170.314.b.2 – 1.03: Using the Inspection Test Guide, the Tester shall verify that the summary
information is complete and accurate and in accordance with TD170.314.b.2 –
Ambulatory (ambulatory only) or TD170.314.b.2 – Inpatient (inpatient only)
TE170.314.b.2 – 1.04: Using the Inspection Test Guide, the Tester shall verify that the created referral
summary/transition of care information is complete and accurate
Inspection Test Guide
IN170.314.b.2 – 1.01: Using the ONC-provided test data, the Tester shall inspect the content of the C-
CDAs is complete and accurate
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
11
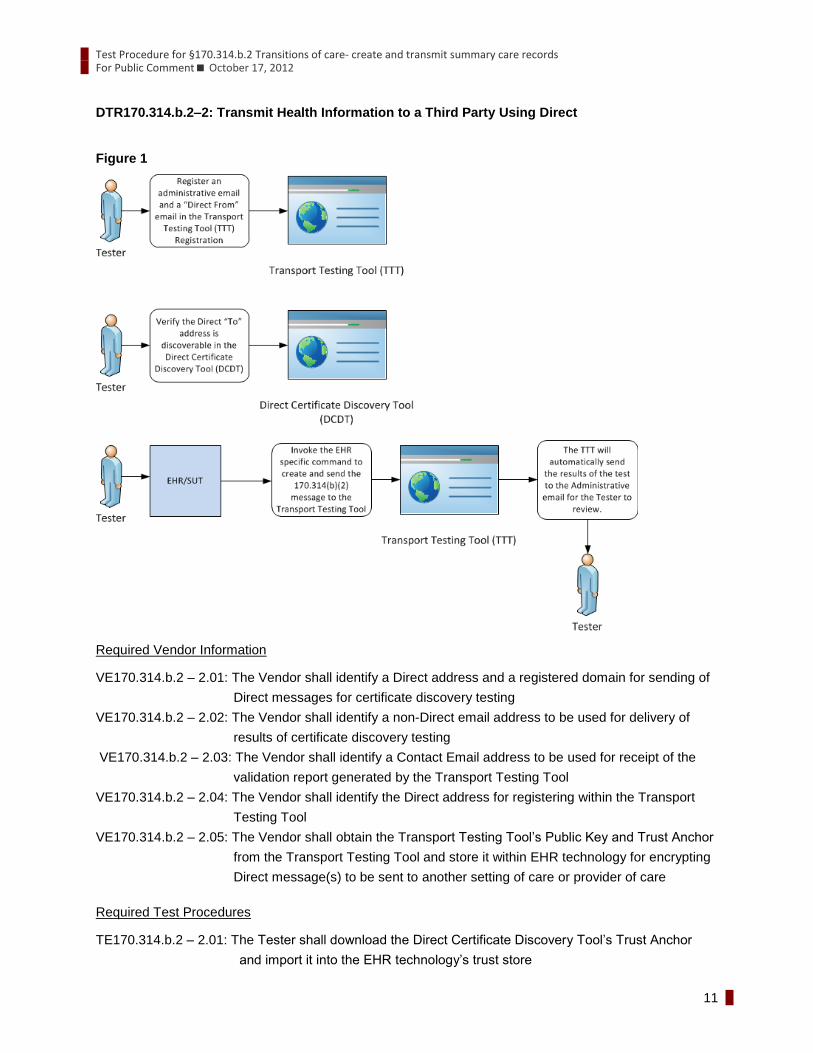
DTR170.314.b.2–2: Transmit Health Information to a Third Party Using Direct
Figure 1
Required Vendor Information
VE170.314.b.2 – 2.01: The Vendor shall identify a Direct address and a registered domain for sending of
Direct messages for certificate discovery testing
VE170.314.b.2 – 2.02: The Vendor shall identify a non-Direct email address to be used for delivery of
results of certificate discovery testing
VE170.314.b.2 – 2.03: The Vendor shall identify a Contact Email address to be used for receipt of the
validation report generated by the Transport Testing Tool
VE170.314.b.2 – 2.04: The Vendor shall identify the Direct address for registering within the Transport
Testing Tool
VE170.314.b.2 – 2.05: The Vendor shall obtain the Transport Testing Tool’s Public Key and Trust Anchor
from the Transport Testing Tool and store it within EHR technology for encrypting
Direct message(s) to be sent to another setting of care or provider of care
Required Test Procedures
TE170.314.b.2 – 2.01: The Tester shall download the Direct Certificate Discovery Tool’s Trust Anchor
and import it into the EHR technology’s trust store
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
12
TE170.314.b.2 – 2.02: The Tester shall use the Direct (From) address provided in VE170.314.b.2-2.01 to
execute the test using the Direct Certificate Discovery Tool
TE170.314.b.2 – 2.03: The Tester shall use the non-Direct email address provided in VE170.314.b.2-2.02
for receipt and validation of results of certificate discovery testing
TE170.314.b.2 – 2.04: The Tester shall execute all test cases within the Direct Certificate Discovery Tool
TE170.314.b.2 – 2.05: Using the Inspection Test Guide, the Tester shall verify that the EHR technology is
able to correctly discover and use address-bound and domain-bound certificates
hosted in both DNS and LDAP
TE170.314.b.2 – 2.06: The Vendor shall provide the recipient with a valid Trust Anchor
TE170.314.b.2 – 2.07: The Tester cause the EHR to register the Direct (To) addresses specified in the
Transport Testing Tool to be available as a recipient for sending of Direct
messages within the EHR
TE170.314.b.2 – 2.08: The Tester shall cause the EHR to transmit Consolidated CDA document(s) using
ONC Applicability Statement for Secure Health Transport (Direct) standard to the
Direct (To) address(es) specified in the Transport Testing Tool. The Direct
message shall be encrypted using the recipient’s (Transport Testing Tool) Public
Key obtained in VE170.314.b.2 – 2.05 and signed using the sender’s (Vendor)
Private Key for the Referral Summary/Transition of Care document created in
VE170.314.b.2 – 1.02
TE170.314.b.2 – 2.09: Using the Inspection Test Guide, the Tester shall verify that the Referral
Summary/Transition of Care is transmitted according to the Consolidated CDA
standard tested and the named vocabulary standards, and is complete and
accurate
Inspection Test Guide
IN170.314.b.2 – 2.01: Using the Direct Certificate Discovery Tool, the Tester shall inspect the results
received via email to verify that all test cases were successful
IN170.314.b.2 – 2.02: The Tester shall verify the appropriate Direct (To) address(es) (provided within the
Transport Testing Tool) have been registered within the EHR technology and are
visible Direct addresses for transmitting of health information to the Transport
Testing Tool according to the ONC Applicability Statement for Secure Health
Transport (Direct) standard
IN170.314.b.2 – 2.03: Using the Transport Testing Tool, the Tester shall verify that the transmitted C-CDA
document has been transmitted and received successfully according to the ONC
Applicability Statement for Secure Health Transport (Direct) standard, including
successful decryption validation and trust anchor validation
IN170.314.b.2 – 2.04: Using the provided test data, and the Validation Report produced by the Transport
Testing Tool identified in the Conformance Test Tools section of this test
procedure, the Tester shall verify that
The C-CDA Implementation Guide conformance requirements tested are met
by the electronically generated (Ambulatory/Inpatient) Transition of
Care/Referral Summary
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
13
The standards for the named vocabularies for the Common MU Data Set,
Encounter diagnoses, and Immunizations are met by the electronically
generated Transition of Care/Referral Summary
IN170.314.b.2 – 2.05: The Tester shall identify the C-CDA .xml files within the transmitted documents
(This may involve parsing files and inspecting the header to identify the C-CDA
documents (vs. style sheet, human readable document, etc.))
IN170.314.b.2 – 2.06: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Ambulatory Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Reason for referral
6) Referring or transitioning provider’s name
7) Provider name
8) Provider office contact information
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
IN170.314.b.2 – 2.07: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Inpatient Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Discharge instructions
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
14
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
DTR170.314.b.2–3: Transmit Health Information Using Direct and XDM Validation (Optional)
Required Vendor Information
VE170.314.b.2 – 3.01: As defined in DTR170.314.b.2 – 1 and DTR170.314.b.2 – 2 no additional
information is required
Required Test Procedures
TE170.314.b.2 – 3.01: The Tester cause the EHR to register the Direct (To) addresses specified in the
Transport Testing Tool to be available for Direct messaging with XDM Validation
within the EHR
TE170.314.b.2 – 3.02: The Tester shall cause the EHR to transmit Consolidated CDA document(s) using
ONC Applicability Statement for Secure Health Transport (Direct) standard with
XDM Validation to the Direct (To) address(es) specified in the Transport Testing
Tool that are available within the EHR following TE170.b.2 – 4.01. The Direct
message shall be encrypted using the recipient’s (Transport Testing Tool) Public
Key obtained in VE170.314.b.2 – 2.05 and signed using the sender’s (Vendor)
Private Key for the Referral Summary/Transition of Care document created in
VE170.314.b.2 – 1.02
TE170.314.b.2 – 3.03: Using the Inspection Test Guide, the Tester shall verify that the Referral
Summary/Transition of Care is transmitted according to the Consolidated CDA
standard tested and the named vocabulary standards, and is complete and
accurate
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
15
Inspection Test Guide
IN170.314.b.2 – 3.01: The Tester shall verify the appropriate Direct (To) address(es) (provided within the
Transport Testing Tool) have been registered within the EHR technology and are
visible Direct addresses for transmitting of health information to the Transport
Testing Tool according to the ONC Applicability Statement for Secure Health
Transport (Direct) standard with XDM Validation
IN170.314.b.2 – 3.02: Using the Transport Testing Tool, the Tester shall verify that the transmitted C-CDA
document has been transmitted and received successfully according to the ONC
Applicability Statement for Secure Health Transport (Direct) standard with XDM
Validation, including successful decryption validation and trust anchor validation
IN170.314.b.2 – 3.03: Using the provided test data, and the Validation Report produced by the Transport
Testing Tool identified in the Conformance Test Tools section of this test
procedure, the Tester shall verify that
The C-CDA Implementation Guide conformance requirements tested are met
by the electronically generated (Ambulatory/Inpatient) Transition of
Care/Referral Summary
The standards for the named vocabularies for the Common MU Data Set,
Encounter diagnoses, and Immunizations are met by the electronically
generated Transition of Care/Referral Summary
IN170.314.b.2 – 3.04: The Tester shall identify the C-CDA .xml files within the transmitted documents
(This may involve parsing files and inspecting the header to identify the C-CDA
documents (vs. style sheet, human readable document, etc.))
IN170.314.b.2 – 3.05: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Ambulatory Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Reason for referral
6) Referring or transitioning provider’s name
7) Provider name
8) Provider office contact information
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
16
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
IN170.314.b.2 – 3.06: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Inpatient Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Discharge instructions
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
17
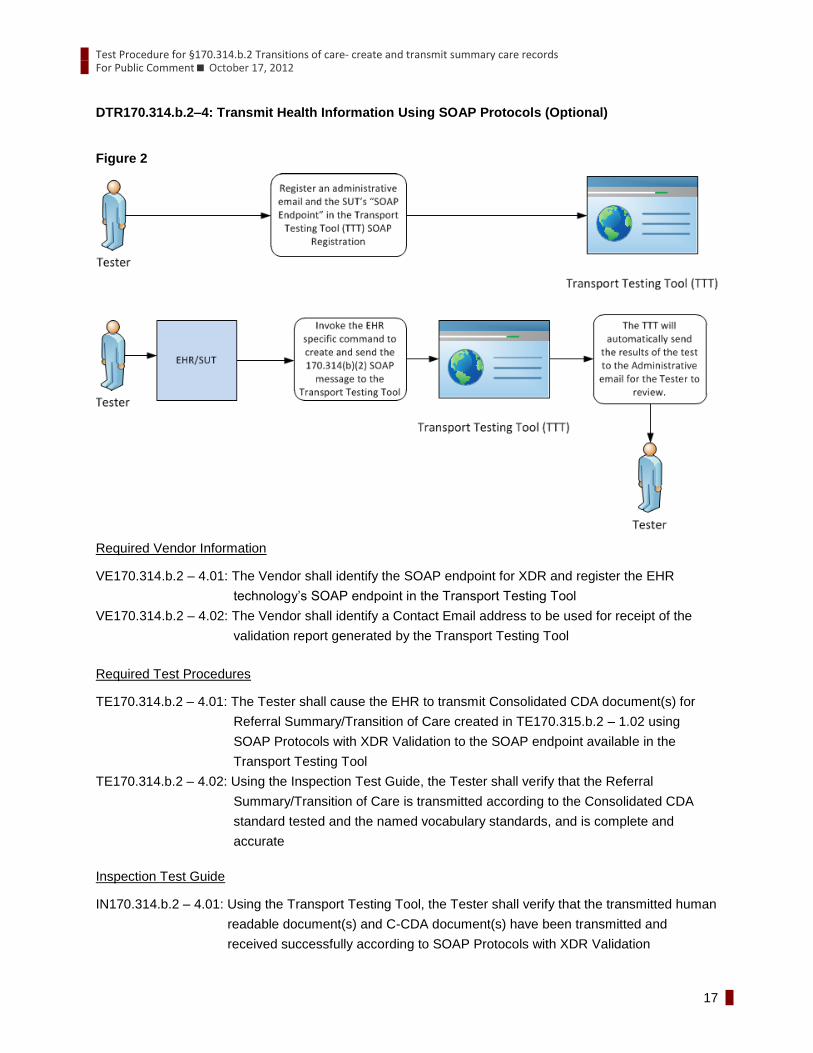
DTR170.314.b.2–4: Transmit Health Information Using SOAP Protocols (Optional)
Figure 2
Required Vendor Information
VE170.314.b.2 – 4.01: The Vendor shall identify the SOAP endpoint for XDR and register the EHR
technology’s SOAP endpoint in the Transport Testing Tool
VE170.314.b.2 – 4.02: The Vendor shall identify a Contact Email address to be used for receipt of the
validation report generated by the Transport Testing Tool
Required Test Procedures
TE170.314.b.2 – 4.01: The Tester shall cause the EHR to transmit Consolidated CDA document(s) for
Referral Summary/Transition of Care created in TE170.315.b.2 – 1.02 using
SOAP Protocols with XDR Validation to the SOAP endpoint available in the
Transport Testing Tool
TE170.314.b.2 – 4.02: Using the Inspection Test Guide, the Tester shall verify that the Referral
Summary/Transition of Care is transmitted according to the Consolidated CDA
standard tested and the named vocabulary standards, and is complete and
accurate
Inspection Test Guide
IN170.314.b.2 – 4.01: Using the Transport Testing Tool, the Tester shall verify that the transmitted human
readable document(s) and C-CDA document(s) have been transmitted and
received successfully according to SOAP Protocols with XDR Validation
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
18
IN170.314.b.2 – 4.02: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Ambulatory Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Reason for referral
6) Referring or transitioning provider’s name
7) Provider name
8) Provider office contact information
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
IN170.314.b.2 – 4.03: Using the ONC-provided test data, the Tester shall verify that the content of the
transmitted C-CDA is complete and accurate and includes, at a minimum, the
following data elements (Inpatient Only):
1) Encounter diagnoses
2) Immunizations
3) Cognitive status
4) Functional status
5) Discharge instructions
and the Common MU Data Set (in their English representation if they associate
with a vocabulary/code set)
1) Patient name
2) Sex
3) Date of birth
4) Race
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
19
5) Ethnicity
6) Preferred language
7) Smoking status
8) Problems
9) Medications
10) Medication Allergies
11) Laboratory test(s)
12) Laboratory value(s)/result(s)
13) Vital signs – height, weight, blood pressure, BMI
14) Care plan field(s), including goals and instructions
15) Procedures
16) Care team member(s)
TEST DATA
Test data is provided with the test procedure to ensure that the functional and interoperable requirements
identified in the criteria can be adequately evaluated for conformance, as well as, to provide consistency
in the testing process across multiple National Voluntary Laboratory Accreditation Program-Accredited
Testing Laboratories (ATLs). The provided test data focus on evaluating the basic capabilities of required
EHR technology, rather than exercising the full breadth/depth of capability that installed EHR technology
might be expected to support. The test data is formatted for readability of use within the testing process.
The format is not prescribing a particular end-user view or rendering. No additional requirements should
be drawn from the format.
The Tester shall use and apply the provided test data during the test, without exception, unless one of the
following conditions exists:
The Tester determines that the Vendor-selected message format requires some modification to
the test data.
The Tester determines that the Vendor product is sufficiently specialized that the provided test
data needs to be modified in order to conduct an adequate test. Having made the determination
that some modification to the provided test data is necessary, the Tester shall record the
modifications made as part of the test documentation.
The Tester determines that changes to the test data will improve the efficiency of the testing
process; primarily through using consistent demographic data throughout the testing workflow.
The Tester shall ensure that the functional and interoperable requirements identified in the
criterion can be adequately evaluated for conformance and that the test data provides a
comparable level of robustness.
Any departure from the provided test data shall strictly focus on meeting the basic capabilities
required of EHR technology relative to the certification criterion rather than exercising the full
breadth/depth of capability that installed EHR technology might be expected to support.
The test procedures require that the Tester enter the test data into the EHR technology being
evaluated for conformance. The intent is that the Tester fully controls the process of entering the
test data in order to ensure that the data are correctly entered as specified in the test procedure.
If a situation arises where it is impractical for a Tester to directly enter the test data, the Tester, at
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
20
the Tester’s discretion, may instruct the Vendor to enter the test data, so long as the Tester
remains in full control of the testing process, directly observes the test data being entered by the
Vendor, and validates that the test data are entered correctly as specified in the test procedure.
CONFORMANCE TEST TOOLS
The following testing tools are available to evaluate conformance to the standards referenced in this test
procedure:
Direct Certificate Discovery Tool (DCDT) – ONC provides a web application certificate discovery
testing tool to support this test procedure. This tool was created to support automated testing of
systems that plan to enact the Certificate Discovery and Provider Directory Implementation
Guide, approved as normative specification by the Direct community, as of July 9, 2012. It is
based on the written test package and requirement traceability matrix created by the Modular
Specifications project under the direction of the Office of the National Coordinator (ONC) and
National Institute of Standards and Technology (NIST).
This application can be installed and deployed locally.
The Direct Certificate Discovery Tool, User’s Guide, configuration instructions, and other
documentation are available at: http://code.google.com/p/direct-certificate-discovery-tool/
Support for this tool is available by contacting:
Avinash Shanbhag ([email protected])
Director, Nationwide Health Information Network Division
Office of Standards and Interoperability
Office of the National Coordinator for Health IT, HHS
Transport Testing Tool (TTT) – NIST provides a web application Transport Testing Tool designed
to support this test procedure. This test will not involve transport testing, however The Transport
Testing Tool includes the capability to verify Consolidated CDA documents. This component of
the Transport Testing Tool relies on Model Driven Health Tools (MDHT) for Consolidated CDA
validation developed by ONC.
The application can be downloaded for local installation
NIST is making available the web-site for pre-testing
The Transport Testing Tool is available at: http://hit-testing.nist.gov:9100/ttt
Documentation for the MDHT project used for C-CDA validation is available at:
https://www.projects.openhealthtools.org/sf/projects/mdht/
Support for this tool is available through the ONC-NIST co-managed Transport Testing Tool Google
Group. Access to the Transport Testing Tool Google Group is available at:
https://groups.google.com/d/forum/transport-testing-tool
Transport Testing Tool Contact:
Kevin Brady ([email protected])
Leader, Systems Interoperability Group
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
21
Acting Leader, Cyber Infrastructure Group
National Institute of Standards and Technology (NIST)
Information Technology Laboratory
The following information is provided to assist the Tester in interpreting the conformance reports
generated by the NIST conformance testing tools:
The NIST Transport Testing Tool, via MDHT, evaluates individual conformance statements which have
been derived from the standards and the "HL7 Implementation Guide for CDA® Release 2: IHE Health
Story Consolidation, DSTU Release 1.1 (US Realm) Draft Standard for Trial Use July 2012" identified in
the Final Rule and the test data provided in this test procedure. The validation tools evaluate the
submitted HL7 message instance for each conformance statement, and then produce a conformance
report. The Tester should consider that a report containing only Affirmative and Warning messages
indicates general conformance to the standard and test data expectations. If reported, errors should be
considered as significant departures from the standard or test data requirements which need to be
corrected in order to claim conformance. ATLs will need to further analyze each error to determine if, in
the context of meeting the criterion and overall meaningful use objective, the error results in a failure of
the test procedure by the EHR technology. The Tester may need to inspection test data values derived
from required vocabularies and code sets.
Test Procedure for §170.314.b.2 Transitions of care- create and transmit summary care records For Public Comment October 17, 2012
22
Document History
Version Number Description Date Published
1.0 Released for public comment October 17, 2012


















