


Tih4i i| Lh 3ih - לימודי תואר ראשון ... · /2 ! "$# /2 %'&)(+*),.-0/+(.1,+2,) ,)
2013שחפת בשנת
ר בן דיין דניאל "ד ח שמואל הרופא "מחלקת ראות שחפת ב

Outline Epidemiology Patho-physiology Diagnosis : Active and Latent TB Treatment : Active and Latent TB Special cases: MDR/XDR-TB HIV/TB Extra-pulmonary TB Non Tuberculosis Mycobacterium (NTM)

Washington D.C., USA, 22-27 July 2012 www.aids2012.org
Estimated number of
cases
Estimated number of
deaths
1.1 million (range 0.9–1.1 million)
12 million (range 11–14 million)
All forms of TB
HIV-associated TB
1.8 million (15%) (1.3–1.6 million)
350,000 (24%)
The global burden of TB in 2010
(25% of HIV deaths worldwide are due to TB - more than 76% burdern in Africa )
MDR-TB 650000





Outline Epidemiology Patho-physiology Diagnosis : Active and Latent TB Treatment : Active and Latent TB Special cases: MDR/XDR-TB HIV/TB Extra-pulmonary TB

Mycobacterium Tuberculosis
Intracellular pathogen Aerobic , non spore forming , non motile Cell wall membrane: 60% HMW lipids ( stain poorly with
gram stain )- Impermeability and resistance to anti microbial agents
Mycolic acids

Mycobacterium Tuberculosis
Form serpentine structure :cord (associated with virulence) Divides every 22 h: slow replication rate, ability to persist in a
latent state

Transmission of TB • M. tuberculosis is carried in airborne particles, called droplet nuclei, of 1– 5 microns
in diameter. • Infectious droplet nuclei are generated when persons who have pulmonary or
laryngeal TB disease cough, sneeze, shout, or sing (in the air for several hours). • M. tuberculosis is transmitted through the air, not by surface contact. Transmission
occurs when a person inhales droplet nuclei containing M. tuberculosis, and the droplet nuclei traverse the mouth or nasal passages, upper respiratory tract, and bronchi to reach the alveoli of the lungs
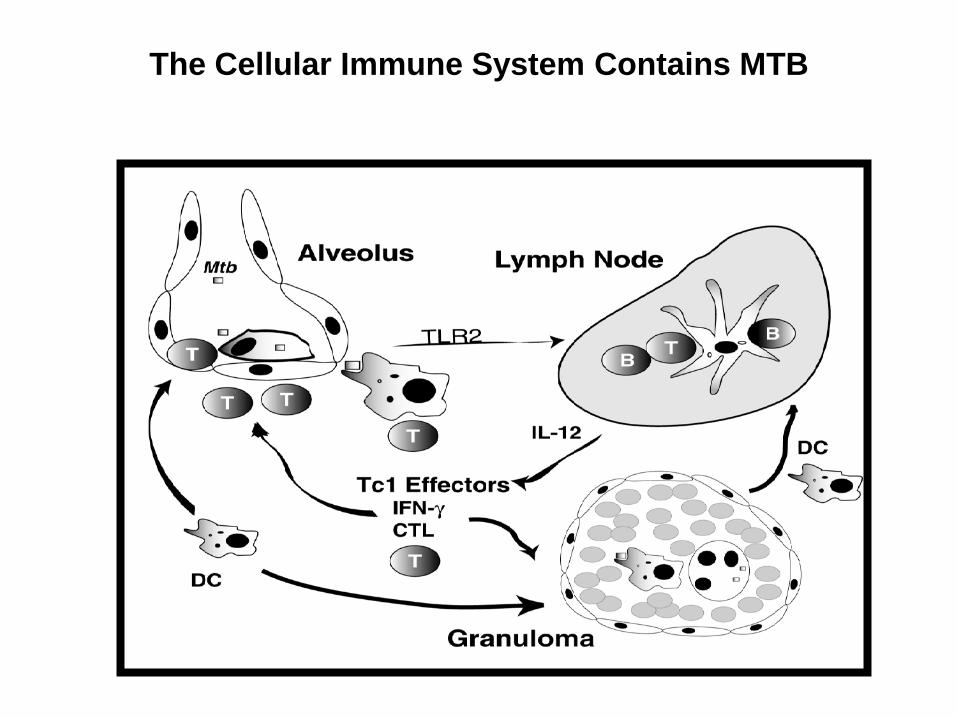
The Cellular Immune System Contains MTB
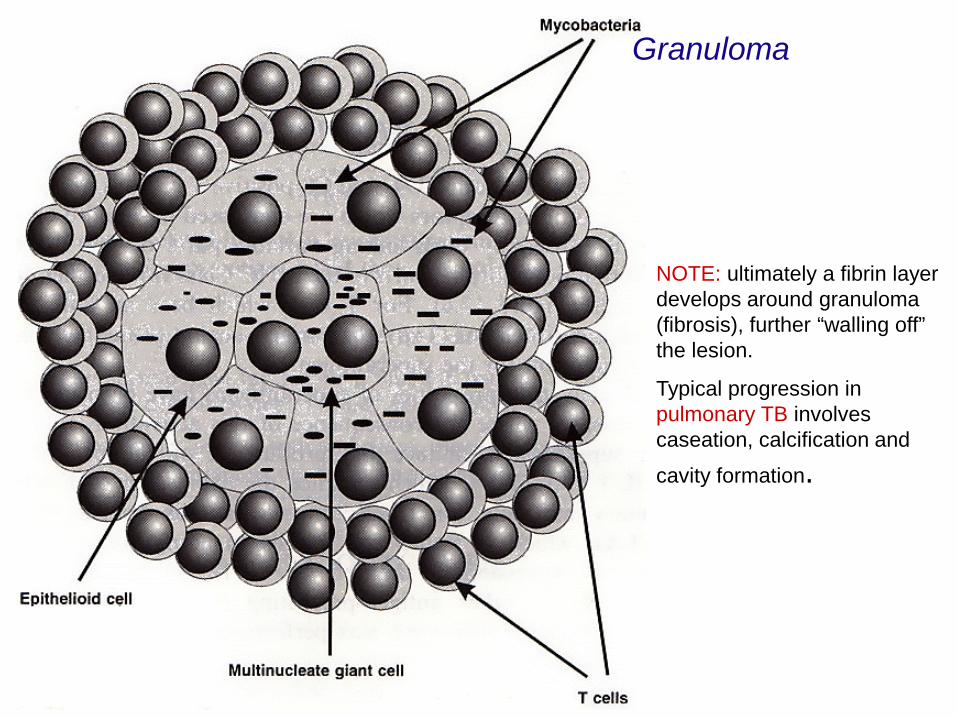
Granuloma
NOTE: ultimately a fibrin layer develops around granuloma (fibrosis), further “walling off” the lesion.
Typical progression in pulmonary TB involves caseation, calcification and cavity formation.

LTBI
M. tuberculosis
exposure
infection
Protective immunity Latency
90%
Never TB
Natural course of M. tuberculosis infection
Latency 5% 2-5%
Progression 10%
TB disease
Rates of reactivation: 1950s 0.10-0.16/100 person-years
1997-2001 0.04-0.06/100 person-years Disappearence of old, healed TB
Horsburgh et al Am J Respir Crit Care Med (2010) 182: 420
Bacterium extinguished?
Live bacilli?
Immunosuppression
Immunosuppression
Chemoprophylaxis efficient
Chemoprophylaxis not necessary
Latency 5% 2-5%
Latency 5% 2-5%

Probability TB will Be Transmitted
Infectiousness of person with TB (AFB +) Immunologic state of the contact Virulence of the organism Exposure in small, enclosed spaces Duration of exposure (>8 hours) Inadequate ventilation, recirculation of air
containing infectious droplets

Health Workers: high risk for infection
Linked to close contact with infectious TB patients during procedures generating aerosols Bronchoscopy Sputum induction Aerosol treatments Endotracheal intubation or suctioning Open abscess irrigation Autopsy

We need new diagnostic tools for the more accurate identification of individuals who are truly infected and who are also at risk of developing
tuberculosis”

Outline Epidemiology Patho-physiology Diagnosis : Active and Latent TB Treatment : Active and Latent TB Special cases: MDR/XDR-TB HIV/TB Extra-pulmonary TB Non Tuberculosis Mycobacterium (NTM)
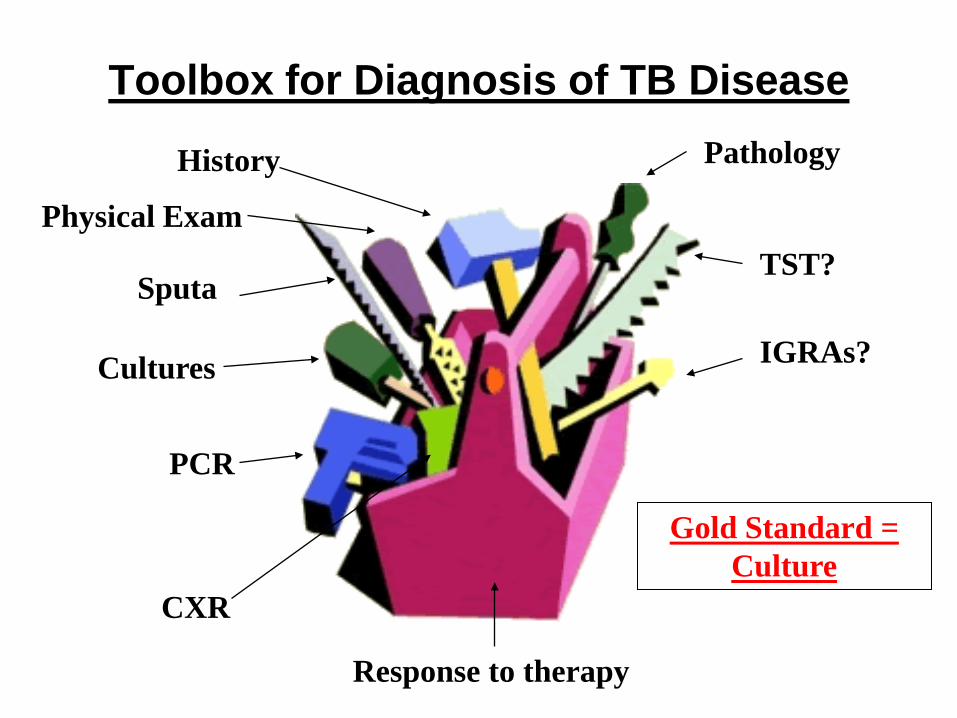
Toolbox for Diagnosis of TB Disease
History
Cultures
Sputa
CXR
Physical Exam
PCR
Pathology
Response to therapy
TST?
IGRAs?
Gold Standard = Culture

Diagnosis of active tuberculosis
• Patient history (cough , night sweat,weight loss....)
• Chest X-ray • Culture/histology
Histology


Decontamination (in non sterile samples) Culture in the adequate media
GOLD STANDARD : CULTURE
• Sometimes the only place where the mycobacteria can be isolated • Gold standard • Molecular epidemiology • Drug susceptibility testing
DST
Growth in solid media
Slow: 15d-2m Division time 18h
Growth in liquid media 7-42d
Inoculums!!
Identification Classical and Molecular
methods

Smear microscopy
Ziehl-Neelsen stain Auramina O stain
Fast; Cheap; Monitorization of treatment; Low sensitivity
Hospital Univ. Germans Trias i Pujol 2004 -2007 Pulmonary Disseminated Extrapulmonary*
TOTAL 125 18 60
Positive smear 83 (66.4%) 11 (61.1%) 11 (18.3%)
Negative smear 42 (33.6%) 7 (38.9%) 49 (81.7%)
*Adenopathy, 4/28 (14.2%); Pleural, 1/17 (5.9%)

IMPACT OF MULTIPLE SAMPLES ON CASE DETECTION

Gene expert: new molecular test
Realוריאקציה DNAהפקת -המערכת מבצעת באופן אוטומטי ישירות מכיח
Time PCR )של ) אמפליפיקציה ודיטקציהM. tuberculosis יחד עם עמידות .ותשובה מתקבלת תוך שעה וחצי, Rifampicin -ל
GeneXpert

Washington D.C., USA, 22-27 July 2012 www.aids2012.org
Workflow • sputum • simple 1-step external sample prep. procedure • time-to-result < 2 h • throughput: > 16 tests / day / module • integrated controls • true random access
Performance • specific for MTB • sensitivity better than smear, similar to culture • 99.5% and 71% sensitive in smear positive and smear negative TB respectively • detection of rif-resistance via rpoB gene
cartridge
GeneXpert System module
MTB
GeneXpert® MTB/RIF Test: game changer for TB diagnosis
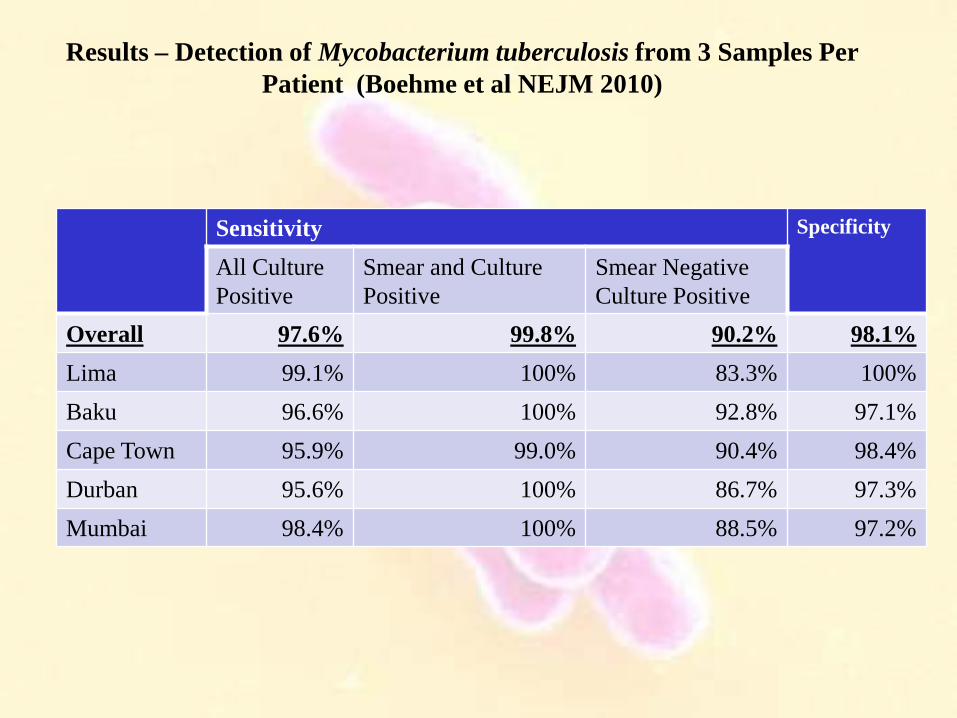
Results – Detection of Mycobacterium tuberculosis from 3 Samples Per Patient (Boehme et al NEJM 2010)
Sensitivity Specificity
All Culture Positive
Smear and Culture Positive
Smear Negative Culture Positive
Overall 97.6% 99.8% 90.2% 98.1% Lima 99.1% 100% 83.3% 100% Baku 96.6% 100% 92.8% 97.1% Cape Town 95.9% 99.0% 90.4% 98.4% Durban 95.6% 100% 86.7% 97.3% Mumbai 98.4% 100% 88.5% 97.2%
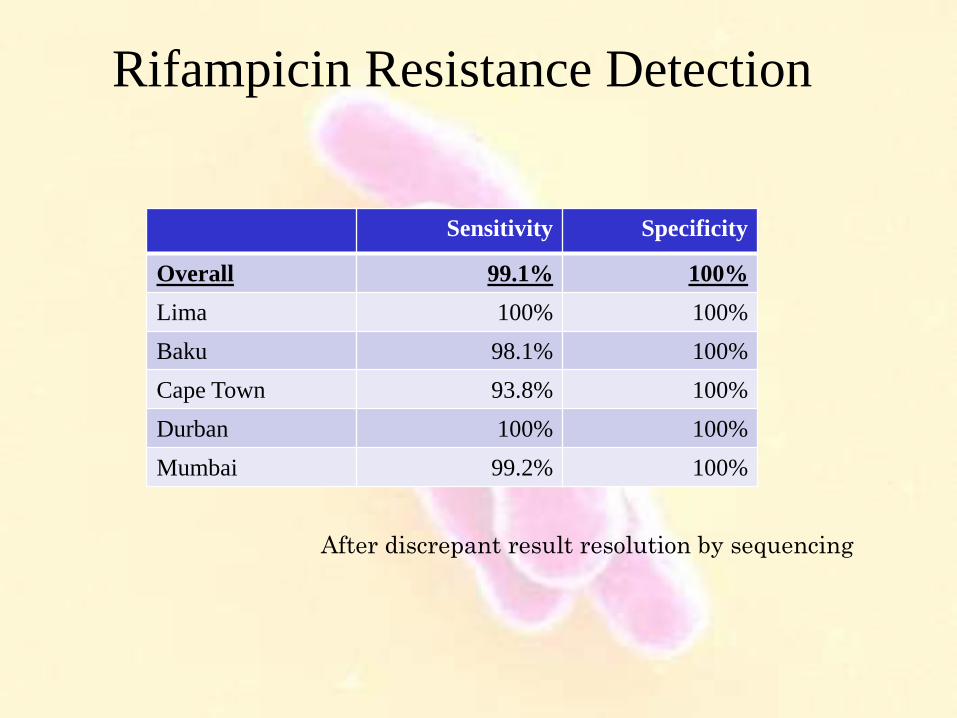
Rifampicin Resistance Detection
Sensitivity Specificity
Overall 99.1% 100% Lima 100% 100% Baku 98.1% 100% Cape Town 93.8% 100% Durban 100% 100% Mumbai 99.2% 100%
After discrepant result resolution by sequencing
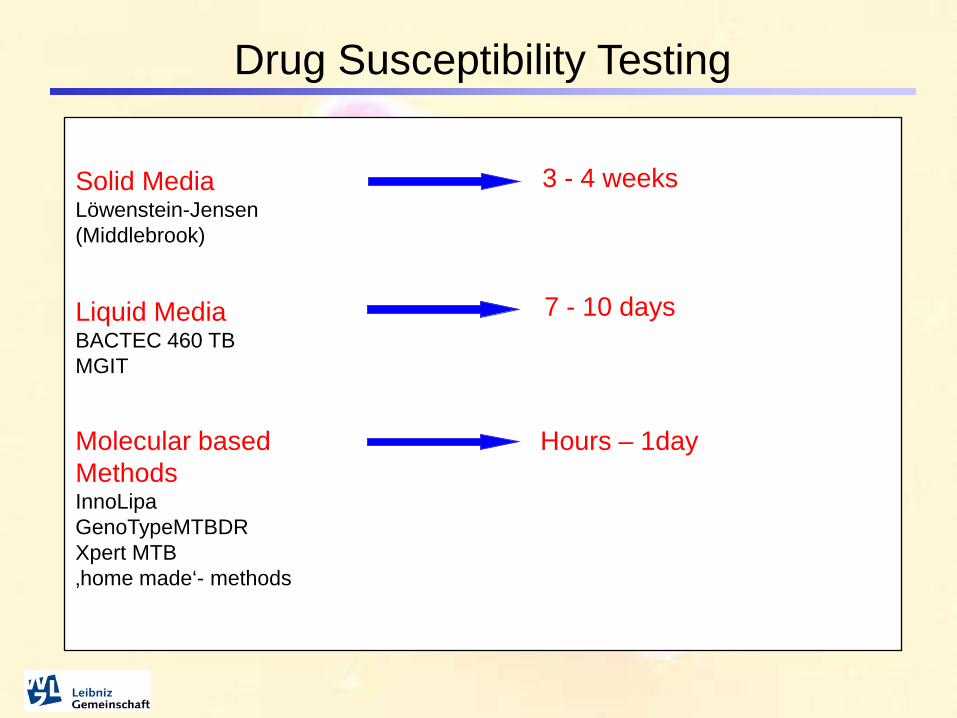
Drug Susceptibility Testing
7 - 10 days
3 - 4 weeks
Solid Media Löwenstein-Jensen (Middlebrook)
Liquid Media BACTEC 460 TB MGIT
Molecular based Methods InnoLipa GenoTypeMTBDR Xpert MTB ‚home made‘- methods
Hours – 1day
Xpert gene: conclusion • It is a fully automated system that allows a relatively untrained
operator to perform sample processing, DNA amplification, • It is one of the fastest and most sensitive ways to detect tuberculosis
and to screen for rifampin resistance in less than 2 hours and only minutes of hands-on time.
• Easy test . In every place . Bed side • The test detects TB in essentially all smear-positive samples and the
majority of smear-negative samples. The presence of non-tuberculous mycobacteria does not confound testing.
• It does not replace the need for MTB culture and complete DST

Extra pulmonary TB
• Lymphadenopathy: 44% -every site / cervical • Pleural 19% ( exudat –lymphocytes - ADA+ ) Empyema- surgical drainage • Bones 11% spine • Peritoneal 5% • CNS –meningitis -6% • Miliary: hematogenous spread (in association with meningitis) • Disseminated tuberculosis
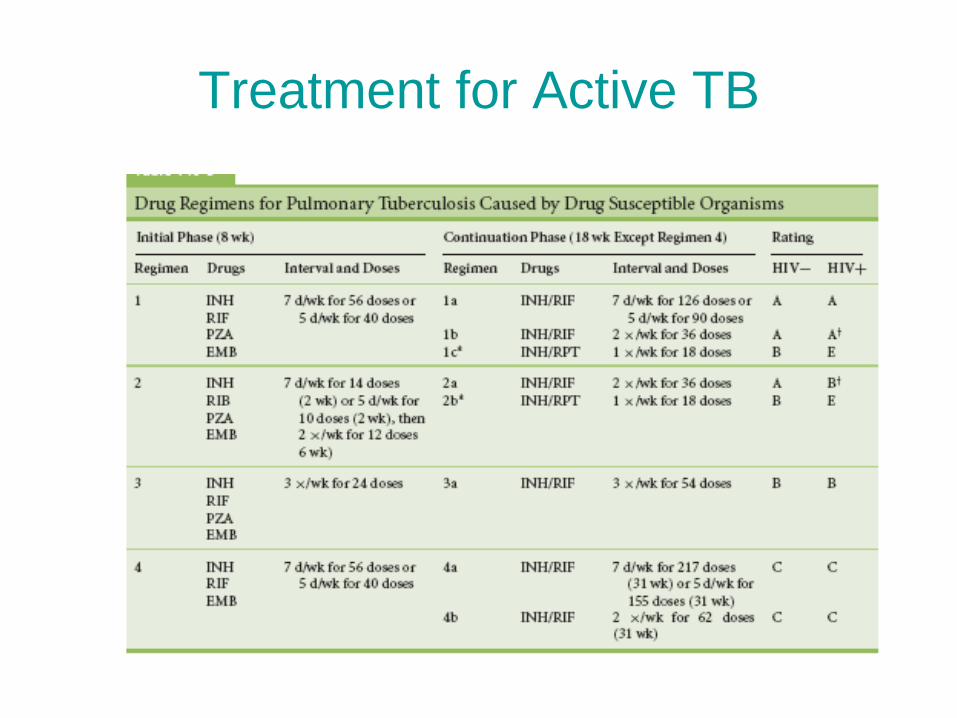
Treatment for Active TB
• First line drugs sensitivity – Initial phase: 2 months Isoniazid (INH), Rifampin (RIF), Pyrazinamide (PZA), and Ethambutol
– Continuation phase: 4 months INH and RIF
• cavitary pulmonary TB positive culture results at end of initiation phase, continuation phase should
be 7 months • HIV-TB • MDR-TB, XDR-TB
Treatment for Active TB

Side effects

Drug Side Effects/Toxicity Some side effects (e.g., nausea) almost universal; do not require
modifications in treatment Some adverse events uncommon but serious, reversible if identified
early; require monitoring Hepatitis-fatal (1%)-mild elevation:30% Hearing loss Visual acuity, color vision 1-3%
Selection of drugs and dosage based on weight, liver function and renal function can prevent toxicity Limit use of hepatotoxic drugs in patients with liver disease Change dosing frequency in patients with renal disease
Some adverse effects cannot be accurately predicted Hepatitis in patients without known liver disease Bone marrow suppression or destruction of red blood cells,
white blood cells, platelets
Toolbox for Diagnosis of Latent TB
TST
IGRAs CXR
History
No Gold Standard!

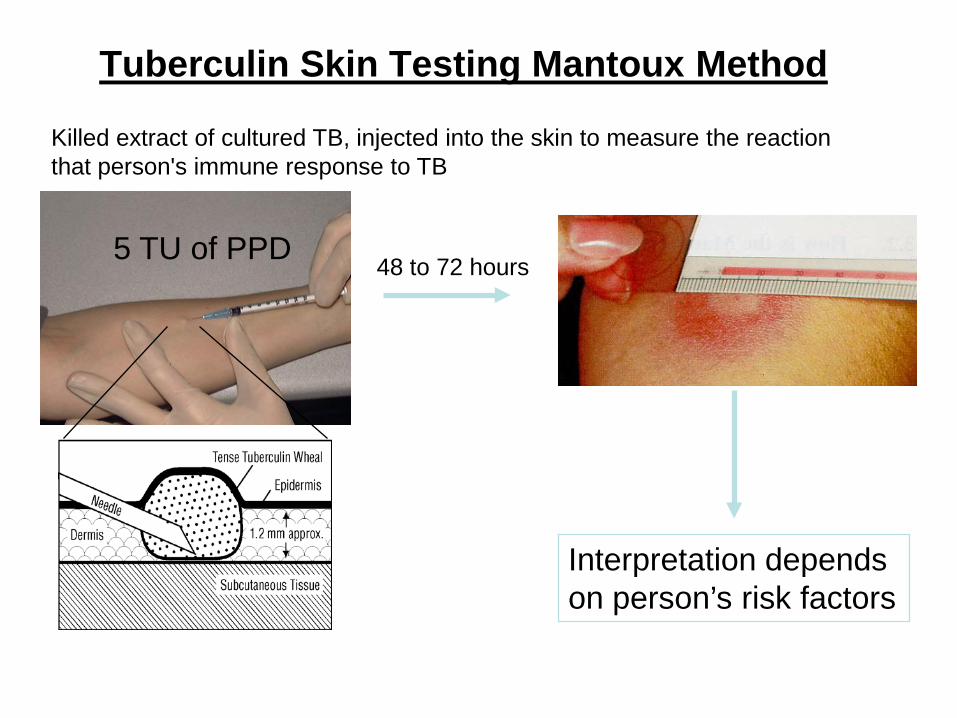
Tuberculin Skin Testing Mantoux Method
48 to 72 hours 5 TU of PPD
Interpretation depends on person’s risk factors
Killed extract of cultured TB, injected into the skin to measure the reaction that person's immune response to TB

Classifying the Tuberculin Reaction
$5 mm is classified as positive in • HIV-positive persons
• Recent contacts of TB case • Persons with fibrotic changes on chest radiograph consistent with old healed TB
• Patients with organ transplants and other immunosuppressed patients
$10 mm is classified as positive in • Recent arrivals from high-prevalence countries • Injection drug users • Residents and employees of high-risk congregate settings • Mycobacteriology laboratory personnel • Persons with clinical conditions that place them at high risk • Children <4 years of age, or children and adolescents exposed to adults in high-risk categories
$15 mm is classified as positive in • Persons with no known risk factors for TB

TST: lack of sensitivity and specificity
False negatives • Technical factors
– Application – Reading – Improper storage of PPD
• Biological factors – Poor nutrition – Infection – Immunosuppressive drugs – Malignancy-sarcoidosis – Age – Stress
False positives • Infection with nontuberculous
mycobacteria • BCG vaccination
Infections with NTM are responsible
for the majority of 5-14 mm PPD reactions among US-born health care workers...”

Meta-analysis of the effect of BCG vaccination on tuberculin skin test measurements . Thorax 2002;57:804-809 • Medline was searched for English language articles published from
1966 to 1999 using the key words "BCG vaccine", "tuberculin test/PPD", and "skin testing
• BCG vaccination were more likely to have a positive skin test • The effect of BCG vaccination on PPD skin test results was less
after 15 years. Positive skin tests with indurations of >15 mm are more likely to be the result of tuberculous infection than of BCG vaccination
• interpretation of the skin test therefore needs to be made in the individual clinical context and with evaluation of other risk factors for infection. The size of the induration should also be considered when making recommendations for treatment of latent infection.
TST >12 mm not related to BCG
Measure release of IFNγ response to MTB specific • Specific antigens used are: CFP10 and ESAT 6 found in all MTB complex organisms NOT present in BCG (RD1) NOT present in most non-TB mycobacterium • If individual has been TB exposed Memory CD4 cells should react to specific antigens These will then release interferon gamma This can then be measured by Serum level or by staining cells

Infection Disease TIME
RESPONSE
IFN-γ
Mycobacterial Load
Immune Response to TB Infection, Disease & Treatment
TST
Rx
As it is now accepted that following TB Rx, TST responses quickly return (95% of cases) whereas IFN-gamma responses remain depressed,
2 tests • Quantiferon-TB Gold assay: which measures the amount
of IFN- γ secreted by T cells after incubation of the blood with synthetic specific tuberculosis antigens (Early Secretory Antigen 6 and Culture Filtrate Protein 10)
• T Spot TB assay which measures the quantity of
secreting T cells after stimulation in vitro of tuberculosis specific antigens.
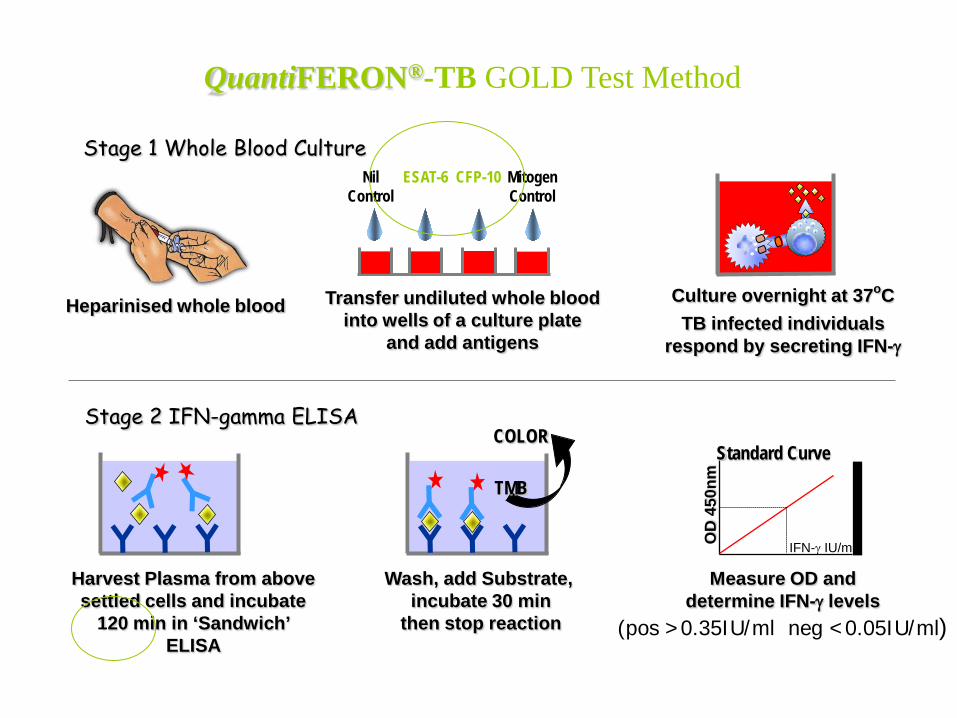
Heparinised whole blood
ESAT-6 CFP-10 Mitogen Control
Transfer undiluted whole blood into wells of a culture plate
and add antigens
Culture overnight at 37oC TB infected individuals
respond by secreting IFN-γ
Harvest Plasma from above settled cells and incubate
120 min in ‘Sandwich’ ELISA
Wash, add Substrate, incubate 30 min
then stop reaction
TMB
COLOR
Measure OD and determine IFN-γ levels
(pos >0.35IU/ml neg <0.05IU/ml)
Stage 1 Whole Blood Culture
Stage 2 IFN-gamma ELISA
QuantiFERON®-TB GOLD Test Method
Nil Control
IFN-γ IU/ml OD
450
nm Standard Curve
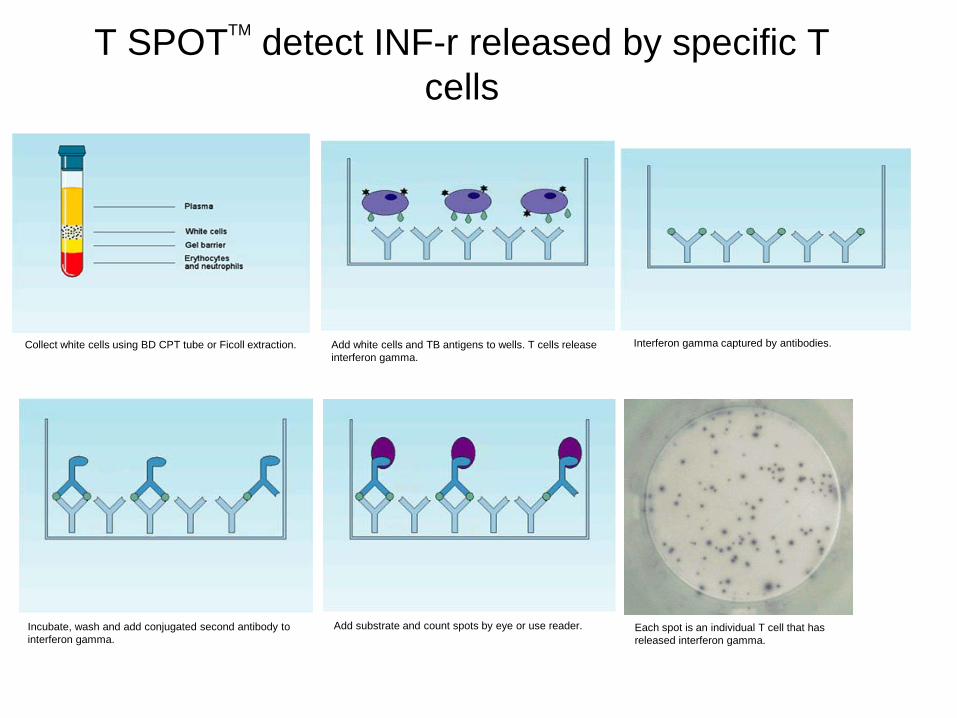
T SPOTTM detect INF-r released by specific T cells
Collect white cells using BD CPT tube or Ficoll extraction. Add white cells and TB antigens to wells. T cells release interferon gamma.
Interferon gamma captured by antibodies.
Incubate, wash and add conjugated second antibody to interferon gamma.
Add substrate and count spots by eye or use reader. Each spot is an individual T cell that has released interferon gamma.


HIGH SPECIFICITY OF IGRA IN IMMUNOCOMPETENT INDIVIDUALS
Pai et al Ann Intern Med (2008) 149: 177
QFT-TB Gold in tube
T-SPOT.TB
QFT-TB Gold: 0.99 (0.98-1.00)
Low-risk individuals

HIGH SENSITIVITY OF IGRA IN IMMUNOCOMPETENT INDIVIDUALS
QFT-TB Gold in tube
T-SPOT.TB
QFT-TB Gold: 0.78 (0.73-0.82)
Patients with active TB
Pai et al Ann Intern Med (2008) 149: 177

T-Spot.TB® Quantiferon Gold®
Sensitivity Immunocompetent
83-97%
70-89%
Immunocompromised + malnourished + children
<1% indeterminate results 20-24% indeterminate results
Specificity 99.99% 98%
Cost (including labour etc)
£55-60 per test
£30 per test
Problems •Must process within 8 hours of venepuncture
•Expertise in cell separation
•Must process within 8 hours of venepuncture -in tube assay?
•Not reliable enough in the Immunocompromised & children

TST vs IGRA
TEST ADVANTAGE DISADVANTAGE
TST •Well studied •Treatment trials based on TST results •Cheap
•2 visits •Lower specificity (BCG) •Less sensitive in immunosuppressed •Subjective observer error
IGRA •High specificity •Higher sensitivity •1 visit
•A lot of conflicting data •Costs ($35-$120US) •Indeterminate results

QuantiFERON®-TB Results from Clinical Studies
QFT-GOLD Mantoux
Sensitivity (N=118) (in untreated, culture confirmed, TB patients)
89.0% 65.7%
Specificity (N=217) (in BCG vaccinated patients, a high proportion of whom are TST positive)
98.2% 42.9%
• Dr Toru Mori Japanese Research Institute of TB 2003 (Unpublished)

Diversity in the use of IGRA (More specific , correlate better to exposure) More than 33 guidelines have been published No consensus
2011NICE recommendations :
• 4 diagnostic approaches:
Two steps approach of TST followed by IGRA if TST negative (to increase sensitivity) and if TST positive (to increases specificity : BCG)
Either TST or IGRA but not both TST and IGRA (to increase sensitivity) Only IGRA
• Healthcare workers : Offer TST if not endemic country or not BCG If TST positive , offer IGRA

IMMUNOCOMPROMISED INDIVIDUALS- 2007 Canadian Guidelines:
Very limited published data – TST should be the initial test used in immunocompromised people
and if TST positive, should be considered to have LTBI. – However, due to high TST negativity in immunocompromised, an
IGRA could be done if the initial TST is negative. • If IGRA positive, consider as LTBI. • If IGRA indeterminate, repeat and if indeterminate again,
use clinical history to make a decision concerning likelihood of LTBI
• If IGRA negative, no LTBI. • By accepting either positive TST or IGRA, sensitivity of
detecting LTBI in immunocompromised populations is achieved.

IGRA : Conclusion
Specificity of IGRAs is higher than that of TST Sensitivity of IGRAs is similar to or higher than TST Like the TST, it is not a perfect test! Both tests have limited prognostic value( a large
proportion of TST- , IGRA + not progress to active TB )

How Much Isoniazid Is Needed for the treatment
of latent TB?
Longer duration of therapy corresponded to lower TB rates among those who took 0-9 mo
No extra increase in protection among those who took >9 mo

Problems Associated with LTBI
• Low adherence with INH therapy, mostly associated with long duration
• Potential better adherence with shorter regiments (4 months of RF )
• Incidence of adverse effects outweigh the potential benefit of disease prevention
Treatment of Latent TB Infection
• Recommended regimen – Isoniazid for 9 months is optimal, 6 months acceptable – Four month course of rifampycin acceptable – Isoniazid and rifapentine 3 months (once weekly)
• Recommendation for PZA/rifamycin has been withdrawn – Problems with liver toxicity – Extremely close monitoring required if used – Remember its still efficacious !

Outline Epidemiology Patho-physiology Diagnosis : Active and Latent TB Treatment : Active and Latent TB Special cases: MDR/XDR-TB HIV/TB Extra-pulmonary TB Non Tuberculosis Mycobacterium (NTM)

HIV and TB • TB is the most common opportunistic infection in HIV infection • Worldwide : 40 millions HIV infected • 15 millions patients HIV-TB co infected in the world. 11% in children ( 85% in SubSaharan Africa ) • TB is the first cause of morbidity and mortality in HIV-infected in the
developing world. (10% -30% of death related AIDS are caused by TB ) • Immunosuppression induced by HIV modifies the clinical presentation
of TB :
1. Subnormal clinical and roentgen presentation 2. High rate of MDR/XDR 3. High rate of treatment failure and relapse (5% vs < 1% in HIV - )

HIV AND TB Interaction Tuberculosis accelerates the progression of HIV infection and HIV increases the likelihood of active TB disease • HIV : Following initial exposure, the rate of progression of tuberculosis infection to
active disease is greater than 40% in HIV positive patients compared to approximately 5% in HIV-negative patients
IFN γ production is decreased in parallel of decreased CD4 1. impairs the host ability to contain infection 2. increases the risk for active tuberculosis. • TB: 1. Enhances HIV replication ( 5-160 fold increase in viral replication, High level of TNF alpha?) 2. Accelerates the natural progression of HIV 3. Leading cause of death in HIV positive
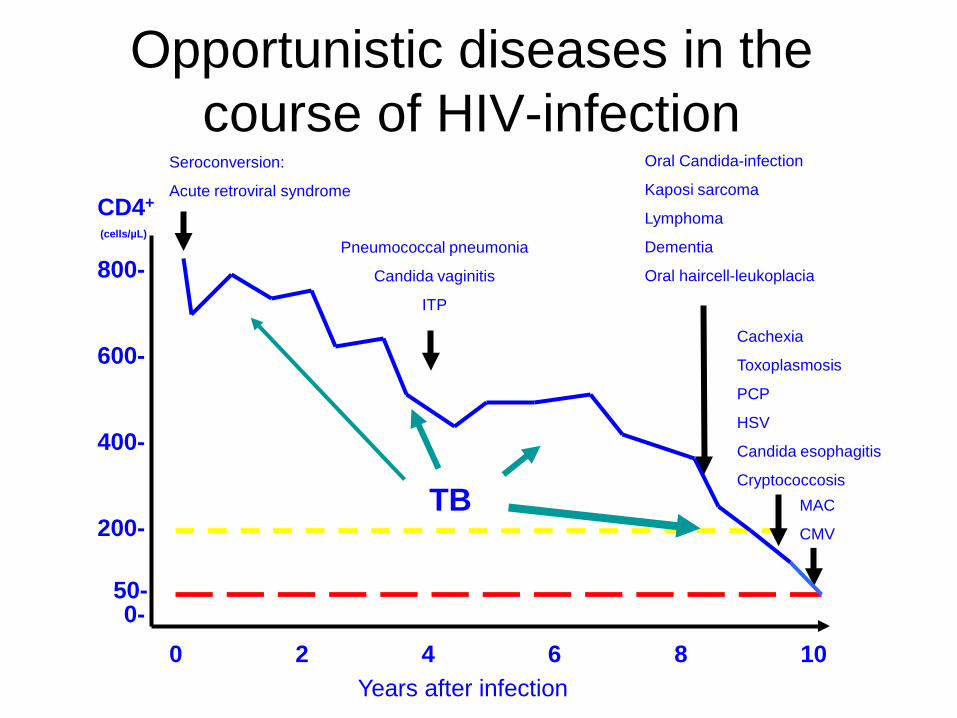
Opportunistic diseases in the course of HIV-infection
CD4+
(cells/µL)
800-
600-
400-
200-
0- 0 2 4 6 8 10
50-
Seroconversion:
Acute retroviral syndrome
MAC
CMV
Pneumococcal pneumonia
Candida vaginitis
ITP
Years after infection
Oral Candida-infection
Kaposi sarcoma
Lymphoma
Dementia
Oral haircell-leukoplacia
Cachexia
Toxoplasmosis
PCP
HSV
Candida esophagitis
Cryptococcosis TB

TB Recurrence in HIV+ and HIV- Patients Successfully Treated for TB
Fitzgerald D, Desvarieux M, Sévère P, Joseph P, Johnson WD Jr, Pape J.W. The Lancet 2000 356 : 1470-74
Time from completion of TB therapy (months)

HIV/TB ISRAEL -2000-2006 Patients: 93/1059 (8.7%) Risk factors: Origin country: 67% (Ethiopian origin) Drug addict: 13% Sexual relation: 2% unknown:15% Mycobacterium: MDR:11% Presentation : Pulmonary: 86% Extra Pulmonary: 32% Both:18% Treatment : ATB and HAART—Side effects IRIS (25%) Death: 3%

HIV-TB problems DIAGNOSIS : Manifestations depend on the state of immune
suppression 1. Atypical clinical presentation: cough, weigh loss 2. Atypical roentgen presentation: Normal Chest xRay: 14-20 % Absence of cavity formation- • Diffuse pulmonary involvement, often LLL-
Prominent hilar /mediastinal LN - Pleural effusions more common-Serositis- pericardial /peritoneal
3. Sputum smears negative despite extensive involvement 4. More EPTB 15% HIV - 20-50% HIV +, More likely to have disseminated
disease
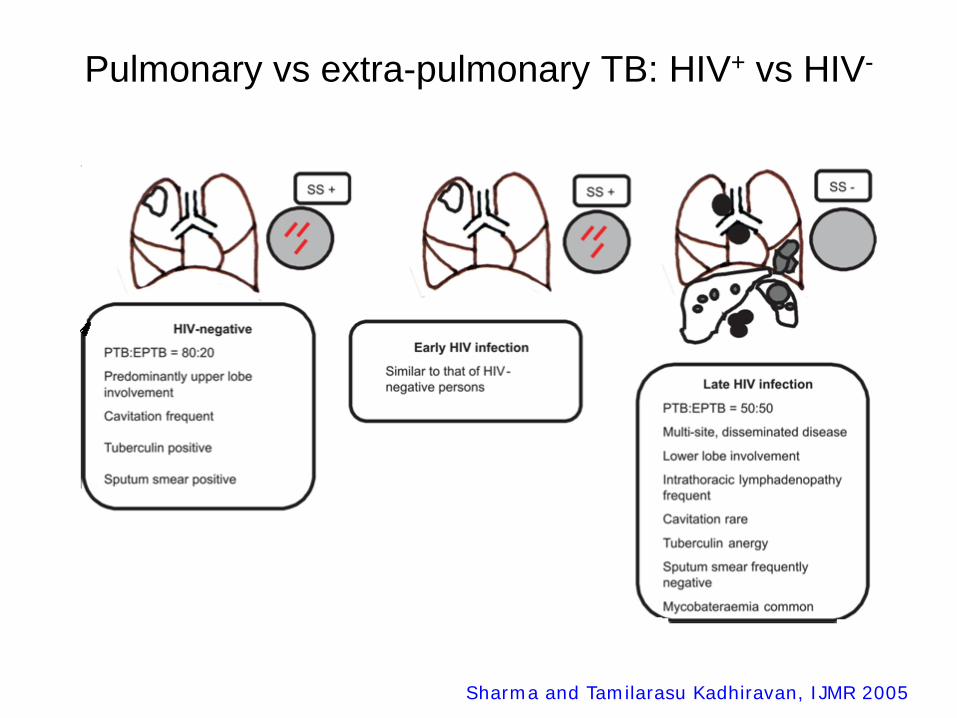
Pulmonary vs extra-pulmonary TB: HIV+ vs HIV-
Sharma and Tamilarasu Kadhiravan, IJMR 2005


Tuberculosis Treatment and HAART • Active TB is an AIDS-defining disease • Begin anti TB treatment immediately Duration of Anti TB treatment 9 months to 1 year Daily therapy
• HAART Timing : no consensus Start antiretroviral therapy as soon as possible (within eight weeks of the
commencement of TB therapy).regardless of their CD4 cell count.
• Problems: Drug toxicities (skin rash, hepatotoxicity) Drug interaction RFP decreases level of ARV drug- resistance Immune restoration induced by HAART may be associated with IRIS Use of HAART results in marked decreases of death and other
opportunistic infection

Immune Reconstitution Syndrome • TB IRIS is characterized by clinical worsening soon after initiation of ART (10-30%) • Cause: recovery of the immune system after HAART institution with
reconstitution of antigen-specific T cell-mediated immunity Suppression of CD4 T cells by HIV causes a subclinical response to infections. As the CD4 count rapidly increases, there is a sudden increase in the
inflammatory response and nonspecific symptoms such as fever or worsening of damage of the infected tissue.
• Symptoms: Fever, adenopathy, respiratory symptoms, increasing pulmonary infiltrates
or effusions, intracranial tuberculomas, ascites, splenomegaly, psoas abscess, intra-
abdominal adenopathy • Two types:
– Paradoxical TB IRIS – Unmasking of an occult opportunistic infection

Management of IRIS
Diagnostic Dilemmas • Immune Reconstitution
Syndrome • Relapse • Drug Toxicity • New Disease Process (M. avium, tuberculosis,Crypto, PCP,
CMV…..)
Therapeutic Dilemmas • Stop or continue ART • Stop or change therapy • Add immunosuppressives
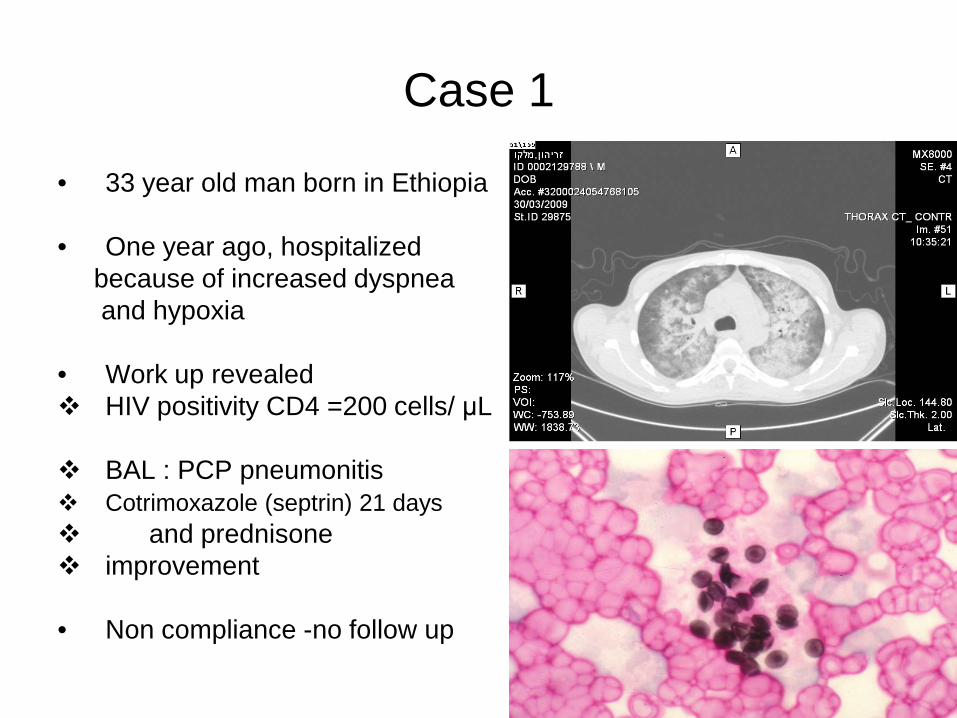
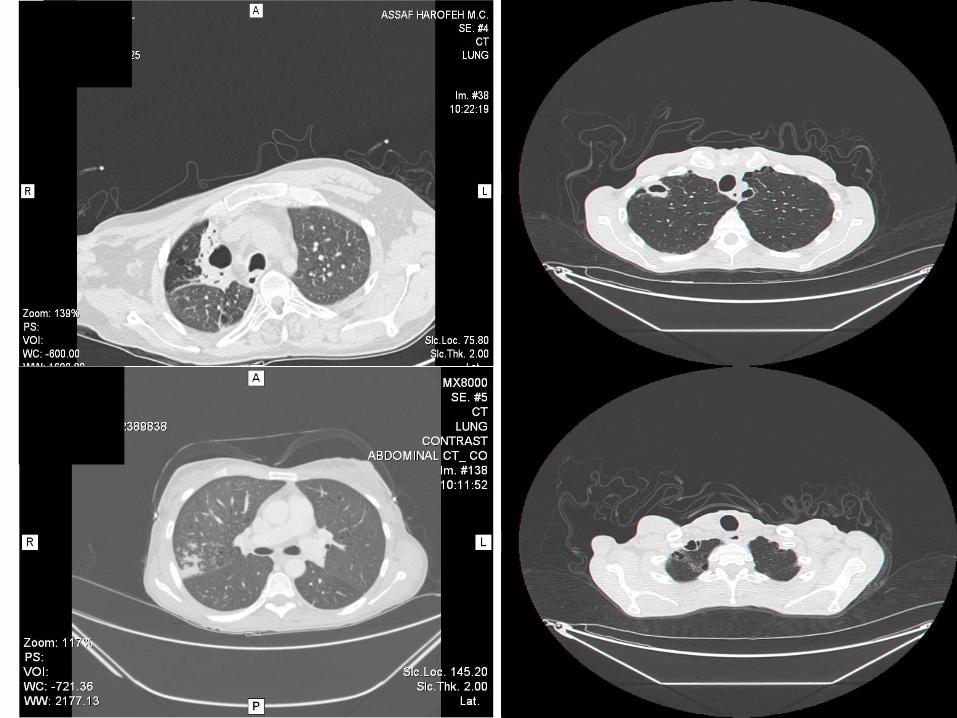
Case 1
• 33 year old man born in Ethiopia
• One year ago, hospitalized because of increased dyspnea and hypoxia
• Work up revealed HIV positivity CD4 =200 cells/ μL
BAL : PCP pneumonitis Cotrimoxazole (septrin) 21 days and prednisone improvement
• Non compliance -no follow up

Case 1 • Few months later, he complained : cough, dry sputum dizziness worsening headache, deviation of the walk on the left side No confusion, no fever • Physical examination: Looks very sick, cachexia Cervical lymph nodes Bilat firm pruritic nodules on the arms and legs • Laboratory examination : CD4 : 26 cells / μL Sputum negative for AFB in ZN stain

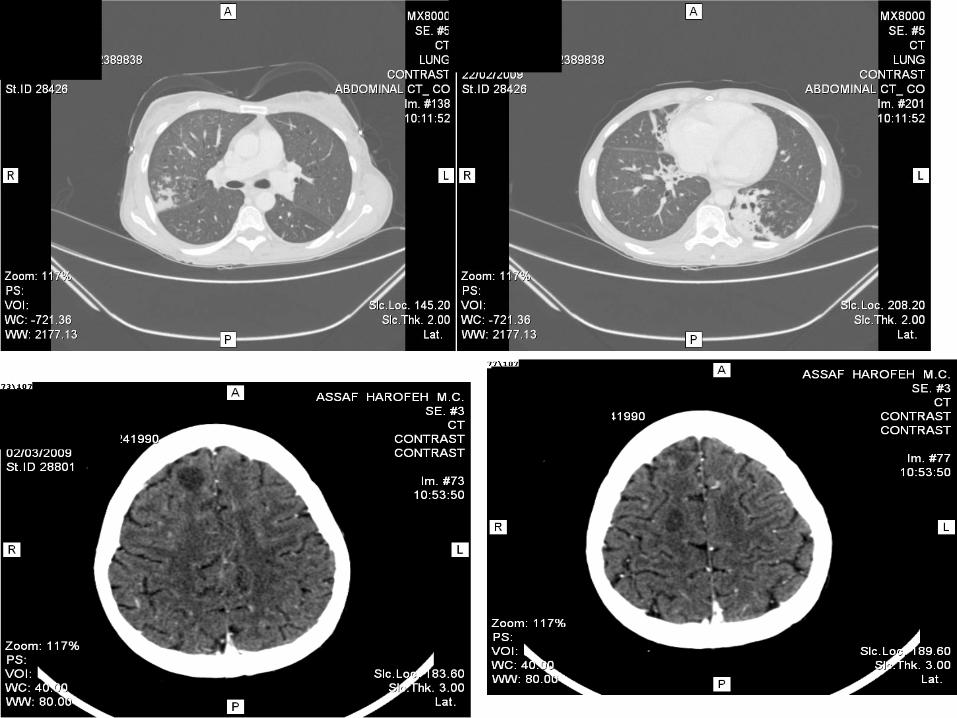

Case 1
Cerebro Spinal Fluid: meningitis with low Glucose level, high protein level and LY cells / AFB negative
Positive sputum cultures for MTB Skin biopsy: prurigo nodularis (epidermal proliferation) LN biopsy: caseiting granuloma Dg: Generalized TB in HIV patient
o Anti TB treatment ( INH, RF, ETB, PZA) and HAART o Initial improvement o After 2 weeks : fever o Dg : IRIS Steroid treatment o Discharge

Definitions: drug resistance MDR-TB = Strains resistant to at least INH and RIF (most important 1st-line drugs) XDR-TB = MDR TB strains with additional resistance to any fluoroquinolone and any of the 3 injectable second-line drugs (amikacin, kanamycin, capreomycin) TDR, XXDR = Resistance to all drugs (not standardised defin)
MDR TB XDR TB TB with any drug resistance
TDR/XXDR TB

TB-Risk factor for development of MDR
• Estimated incidence of 650 000 MDR-TB in 2010 worldwide
(prevalence out of 12 millions)-10% XDR-TB • Primary resistance : Result of the clonal spread of particular MTB
(Beijing type….genotype information is lacking) • Secondary Resistance :Previously unsuccessful treatment
Interruption , inadequate regimen or duration (factors as imprisonment, prior hospitalization or immigration
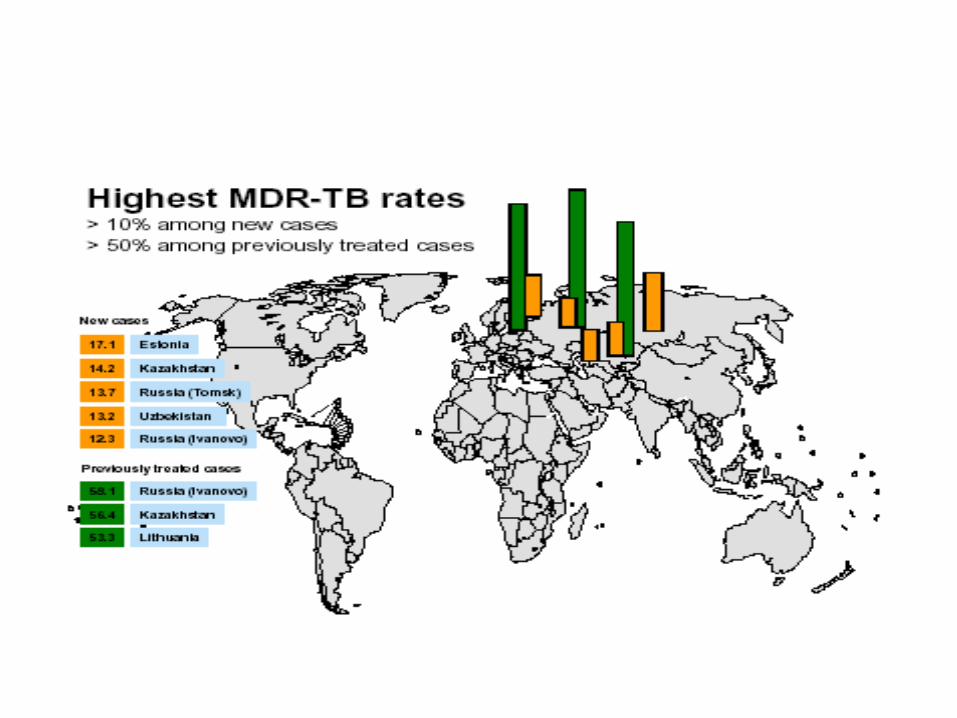
• High MDR-TB prevalence. Asia India, Russian Federations ,,,,, • HIV patients and other immunocompromised • Alcoholism and diabetes


Notifications of MDR-TB increasing BUT only ~ 1 in 6 (16%) of estimated cases of MDR-TB among reported TB patients diagnosed and treated in 2010
Notified cases of MDR-TB
0
10
20
30
40
50
60
2005 2006 2007 2008 2009 2010
Num
ber o
f pat
ient
s (th
ousa
nds)
19,000
53,000
Global Plan target ~270,000 in 2015
0
50
100
150
200
250
300
SE Asia
W. Pac
ific
EuropeAfric
aEMR
America
sWorl
d
Not on treatmentTreated
MDR-TB cases treated and estimated numbers not treated for MDR-TB, among notified TB patients, 2010
290,000

: ProblemsTB-MDR/XDR
• Serious worldwide problem prolonged therapy repeat hospitalizations high rate of treatment failure. • WHO recommendation: 18 months after smear conversion Typical regimen: at least 4- preferably 6 drugs • Toxicity: 40% • Most potent second line reserve: Aminoglycosides and Fluoroquinolones

88
XDR-TB
MDR-TB, resistant to all FLD
MDR-TB, suscep to at least one FLD
Eur Respir J 2007
4,853 C+, 361 MDR, 64 XDR
TDR-TB (MDR+FQ+ Gr IV)


MDR-TB Israel: 2000-2005
• 132 pts -Median age: 40- Smear positive AFB: 70% • Country of origin : FSU : 83% Ethiopia: 8% Israel: 4% • Predisposing conditions: Previous anti-TB treatment(58%) IV drug abuse (23%) Alcohol abuse(25%) • Medical conditions: Hypoalbuminemia (<3.5g/dl) (50%) Diabetes mellitus (12%) Hepatitis B C (22%) HIV sero positivity (6%)

alcohol hypoalbuminemia smear + FQ resistance XDR
p=0.04
p=0.004
p=0.04
p=0.02
p=0.012
Factors related to mortality
dead life
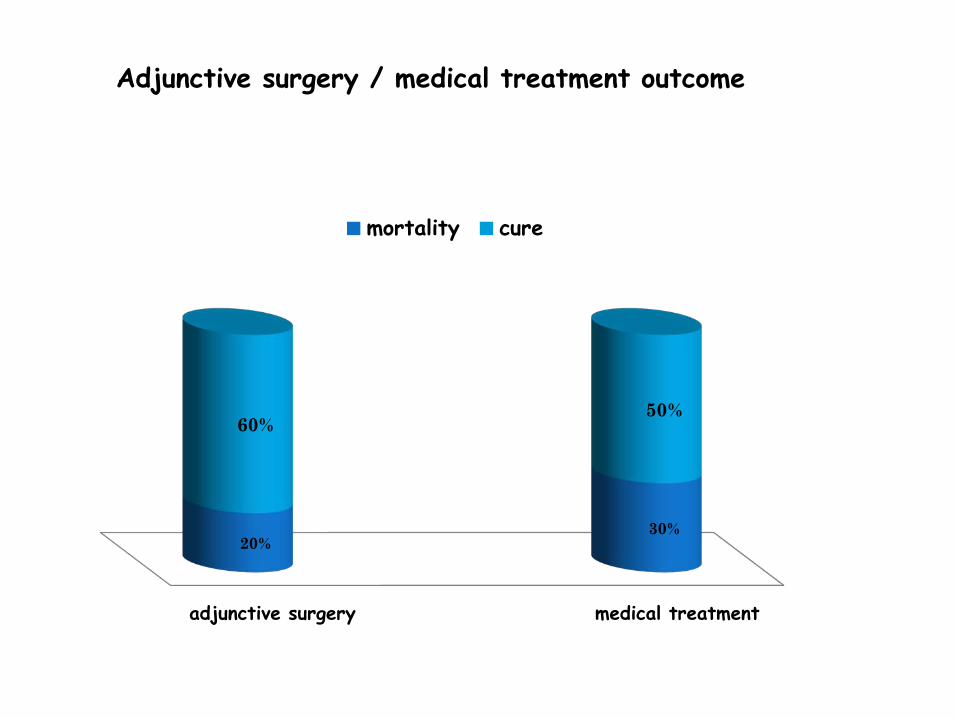
Adjunctive surgery / medical treatment outcome
medical treatment adjunctive surgery
30% 20%
50% 60%
mortality cure

Hong-Bin Xu et al . J Antimicrobial Chemother ;2011;66:1687-
Pulmonary resection for MDR-TB: meta-analysis


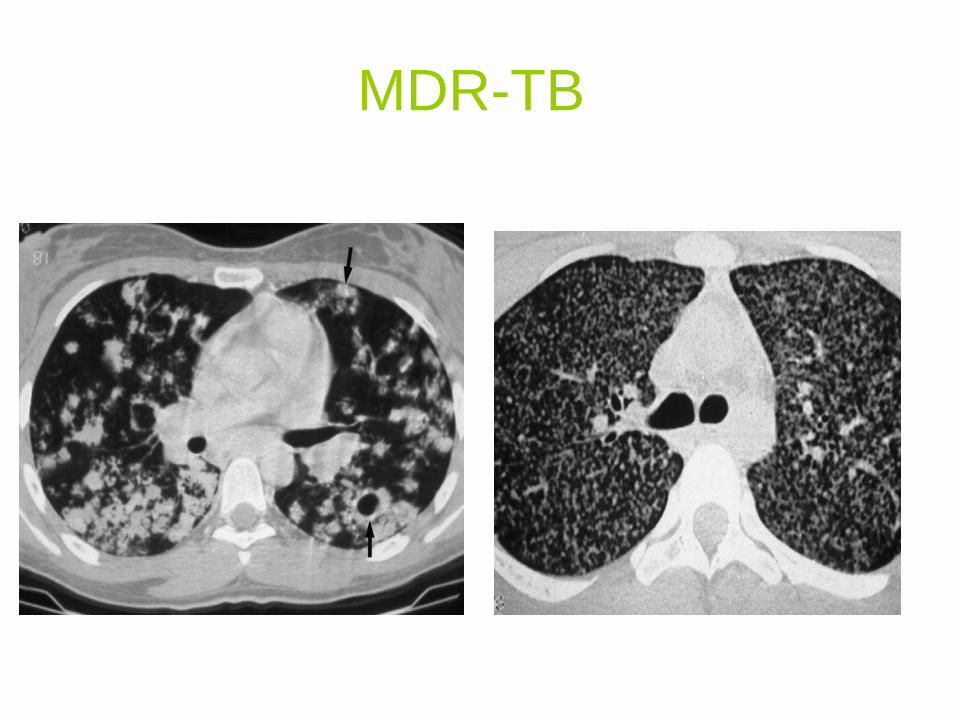
MDR-TB

Outline Epidemiology Patho-physiology Diagnosis : Active and Latent TB Treatment : Active and Latent TB Special cases: MDR/XDR-TB HIV/TB Extra-pulmonary TB Non Tuberculosis Mycobacterium (NTM)

Definition
• NTM are a family of small, rod-shaped bacilli • They are now increasingly being recognized as significant causes of
chronic pulmonary infection in immunocompetent individuals. • Patients with existing pulmonary diseases (CF, COPD, Bronchiectasis..) are
at risk of developing NTM lung disease • The most frequently encountered NTM lung disease is caused by
Mycobacterium avium-intracellulare complex (MAC) and M. Kansasii.


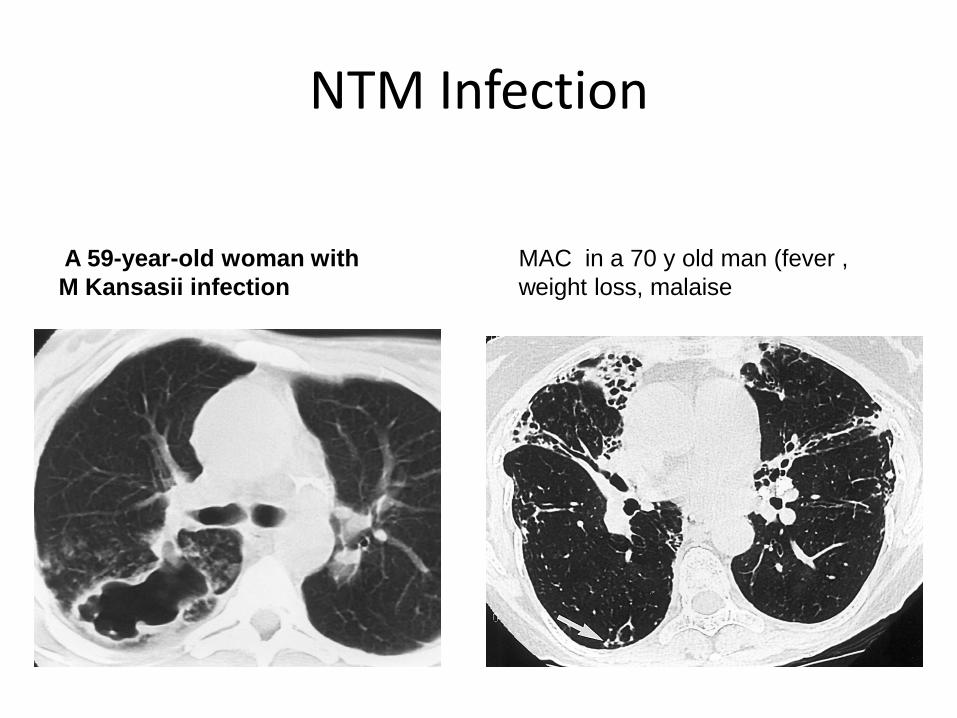
NTM Infection
MAC in a 70 y old man (fever , weight loss, malaise
A 59-year-old woman with M Kansasii infection

NTM treatment Drug Sensitivity test : Subject of debate: MAC : macrolide Kansasii : Rifampicine
Indication varies widely by patient, disease severity and tolerance to
medications Average duration is 12-24 months Rapidly growing NTM infections may require intermittent treatment
across lifetime Naïve treatment patient conversion :74-92% Non-cavitary disease : 82-92% Fibrocavitary disease: 74%

Guidelines for Treatment of NTM (ATS 2007) 1. MAC : 12 months of negative cultures while on therapy a. Clarithromycin 1000 or azithromycin 500 mg b. Ethambutol 25 mg/kg c. Rifampin 600 mg Surgery may be useful in localized disease 2. M. kansasii therapy: a. Rifampin 10 mg/kg/day to maximum 600 mg b. Ethambutol 15 mg/kg/day c. Isoniazid 5 mg/kg/day to maximum 300 mg 3. M. abscessus* Therapy: The only predictably curative therapy of limited disease is surgical resection combined
with multidrug chemotherapy.
Periodic multidrug therapy (a macrolide and 1 or more parenteral agents including amikacin, cefoxitin or imipenem or a combination of the parenteral agents) may help control symptoms and/or progression of disease.

!! Take Home Message
Rapid Diagnosis (Xpert) DOT (decrease incidence) MDR-XDR-TB (??) Urgent need for New drugs Surgery










