2012;Vol.54 The Indian Journal of Chest Diseases & Allied … Revised.pdf · 2012-08-13 · 2 The...
78
Editor-in-Chief S.N. GAUR, Delhi Editors S.K. Jindal, Chandigarh Ashok Shah, Delhi S.K. Sharma, New Delhi Alladi Mohan, Tirupati S.K. Chhabra, Delhi Associate Editors Dheeraj Gupta, Chandigarh J.M. Joshi, Mumbai J.C. Suri, New Delhi THE INDIAN JOURNAL OF CHEST DISEASES AND ALLIED SCIENCES THE INDIAN JOURNAL OF CHEST DISEASES AND ALLIED SCIENCES (ISSN 0377-9343) is published quarterly, by the Vallabhbhai Patel Chest Institute, University of Delhi, Delhi in association with the National College of Chest Physicians (India). The Journal covers the Clinical and Experimental work dealing with all aspects of Chest Diseases and Allied Sciences. It publishes Original Articles, Review Articles, Radiology Forum, Case Reports, Short Communications, Book Reviews. Copyright © with Vallabhbhai Patel Chest Institute, University of Delhi, Delhi. All rights reserved; no part of this publication should be reproduced and/or stored in a retrieved system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission from the Publishers in India and/or in the USA by the Copyright Clearance Center, 222, Rosewood Drive, Danvers, MA 01923. The statements and opinions contained in this Journal are solely those of the authors/advertisers. The Publishers and Editor-in-Chief, its Editorial Board Members, and employees disown all responsibility for any injury to persons or property resulting from any ideas or products referred to in in the articles or advertisements contained in this Journal. The Journal has a wide International and National Circulation/ Exchange and is abstracted and indexed in Index Medicus, Medline, IndMed, INSEAR, and Ulrich's Directory. 2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 1 Founded by: Professor R. Viswanathan Founder-Director, Vallabhbhai Patel Chest Institute Editorial Board Journal Coordinators R.K. Gupta, Delhi D.K. Sahu, Delhi R. Agarwal, Chandigarh A.N. Aggarwal, Chandigarh G. Ahluwalia, Ludhiana J.N. Banavaliker, Delhi R.S. Bedi, Patiala D. Behera, New Delhi Kazi S. Bennoor, Bangladesh Arati Bhatia, Delhi Narendra Bhatta, Nepal Mridula Bose, Delhi Dhruva Chaudhry, Rohtak P.N. Chhajed, Mumbai Anuradha Chowdhary, Delhi D.J. Christopher, Vellore Brian H. Davies, UK R.K. Dewan, New Delhi R. Guleria, New Delhi K. Guntupalli, USA K.B. Gupta, Rohtak V.K. Jain, Bikaner A.K. Janmeja, Chandigarh T. Kadhiravan, Puducherry S. Kashyap, Shimla G.C. Khilnani, New Delhi Jai Kishan, Patiala Raj Kumar, Delhi Dushantha Madegedara, Sri Lanka T. Mohan Kumar, Coimbatore A.A. Mahashur, Mumbai Atul C. Mehta, USA B.K. Menon, Delhi B.N. Panda, Bhubneshwar R. Prasad, Lucknow M. Rahman, Delhi G.K. Rath, New Delhi J.K. Samaria, Varanasi R. Sarin, New Delhi Raj B. Singh, Chennai Virendra Singh, Jaipur R.N. Solanki, Ahmedabad Z.F. Udwadia, Mumbai
Transcript of 2012;Vol.54 The Indian Journal of Chest Diseases & Allied … Revised.pdf · 2012-08-13 · 2 The...
Editor-in-ChiefS.N. GAUR, Delhi
EditorsS.K. Jindal, ChandigarhAshok Shah, DelhiS.K. Sharma, New DelhiAlladi Mohan, TirupatiS.K. Chhabra, Delhi
Associate EditorsDheeraj Gupta, ChandigarhJ.M. Joshi, MumbaiJ.C. Suri, New Delhi
THE INDIAN JOURNAL OFCHEST DISEASES
ANDALLIED SCIENCES
THE INDIAN JOURNAL OF CHEST DISEASES AND ALLIED SCIENCES(ISSN 0377-9343) is published quarterly, by the Vallabhbhai Patel Chest Institute,University of Delhi, Delhi in association with the National College of ChestPhysicians (India). The Journal covers the Clinical and Experimental workdealing with all aspects of Chest Diseases and Allied Sciences. It publishesOriginal Articles, Review Articles, Radiology Forum, Case Reports, ShortCommunications, Book Reviews.
Copyright © with Vallabhbhai Patel Chest Institute, University of Delhi, Delhi.All rights reserved; no part of this publication should be reproduced and/orstored in a retrieved system or transmitted in any form or by any means,electronic, mechanical, photocopying, recording or otherwise, without the priorpermission from the Publishers in India and/or in the USA by the CopyrightClearance Center, 222, Rosewood Drive, Danvers, MA 01923.
The statements and opinions contained in this Journal are solely those of theauthors/advertisers. The Publishers and Editor-in-Chief, its Editorial BoardMembers, and employees disown all responsibility for any injury to persons orproperty resulting from any ideas or products referred to in in the articles oradvertisements contained in this Journal.
The Journal has a wide International and National Circulation/ Exchange and is abstractedand indexed in Index Medicus, Medline, IndMed, INSEAR, and Ulrich's Directory.
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 1
Founded by: Professor R. ViswanathanFounder-Director, Vallabhbhai Patel Chest Institute
Editorial Board
Journal CoordinatorsR.K. Gupta, DelhiD.K. Sahu, Delhi
R. Agarwal, ChandigarhA.N. Aggarwal, ChandigarhG. Ahluwalia, LudhianaJ.N. Banavaliker, DelhiR.S. Bedi, PatialaD. Behera, New DelhiKazi S. Bennoor, BangladeshArati Bhatia, DelhiNarendra Bhatta, NepalMridula Bose, DelhiDhruva Chaudhry, RohtakP.N. Chhajed, MumbaiAnuradha Chowdhary, DelhiD.J. Christopher, Vellore
Brian H. Davies, UKR.K. Dewan, New DelhiR. Guleria, New DelhiK. Guntupalli, USAK.B. Gupta, RohtakV.K. Jain, BikanerA.K. Janmeja, ChandigarhT. Kadhiravan, PuducherryS. Kashyap, ShimlaG.C. Khilnani, New DelhiJai Kishan, PatialaRaj Kumar, DelhiDushantha Madegedara, Sri LankaT. Mohan Kumar, Coimbatore
A.A. Mahashur, MumbaiAtul C. Mehta, USAB.K. Menon, DelhiB.N. Panda, BhubneshwarR. Prasad, LucknowM. Rahman, DelhiG.K. Rath, New DelhiJ.K. Samaria, VaranasiR. Sarin, New DelhiRaj B. Singh, ChennaiVirendra Singh, JaipurR.N. Solanki, AhmedabadZ.F. Udwadia, Mumbai
2 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
NATIONAL COLLEGE OF CHEST PHYSICIANS (INDIA)
GOVERNING COUNCIL[w.e.f.: 1st April 2011]
President (2011-2012) Vice-President (2010-2012)Dr G.C. Khilnani Dr J.C. SuriNew Delhi New Delhi
President-Elect (2012-2013) Immediate Past President (2010-2011)Vacant Dr D. BeheraDue to death of Dr R.C. Jain New Delhi
Secretary (2010-2013) Joint Secretary (2010-2012)Dr S.N. Gaur Dr Rajesh N. SolankiDelhi Ahmedabad
Treasurer (2009-2012)Dr V.K. SinghDelhi
Councillors (2011-2013)
Dr Bharat Gopal Dr Dheeraj Gupta Dr Rajendra PrasadNew Delhi Chandigarh Lucknow
Dr K.B. Gupta Dr V.K. Jain Dr A.K. JanmejaRohtak Bikaner Chandigarh(upto 2012)
Zonal Chairmen
North South Central East WestDr J.C. Suri Dr P. Ravindran Dr S.K. Katiyar Dr S.N. Tripathy Dr N.K. JainNew Delhi Trivandrum Kanpur Cuttack Jaipur
Co-opted Member (NAPCON-2011)
Dr Raj KumarDelhi

THE INDIAN JOURNAL OF CHEST DISEASES AND ALLIED SCIENCES
Vol.54 January–March 2012 No.1
CONTENTSPages
Editorial
Decoding population genetics: impact on tuberculosis control and treatmentMridula Bose .. 5
Original Articles
Role of a pattern-based approach in interpretation of transbronchoscopic lung biopsy and itsclinical implications
Ritu Kulshrestha, B.K. Menon, Rajkumar and V.K. Vijayan .. 9
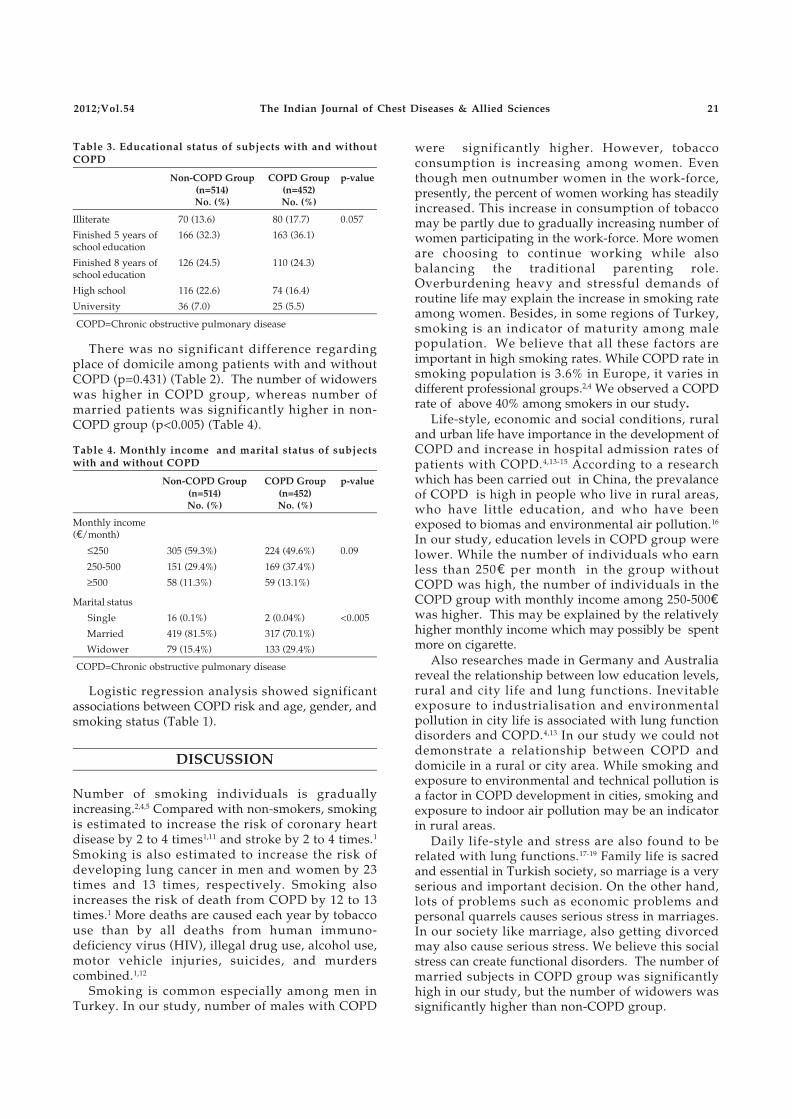
Socio-economic status of smokers presenting to the outpatient service: does chronic obstructivepulmonary disease make a difference?
G. Cakmak, Z.A. Saglam, T. Saler, M. Yenigun and L. U. Temiz .. 19
Pattern of drug-resistance and treatment outcome in multidrug-resistant pulmonary tuberculosisC. Nagaraja, B.L. Shashibhushan, Moh. Asif, Manjunath PH and Sagar C .. 23
Review ArticleExhaled breath condensate analysis in chronic obstructive pulmonary disease
S.K. Chhabra and Mansi Gupta .. 27
Radiology ForumTracheal diverticulum
Mehul Shah and J.M. Joshi .. 39
Case ReportsBronchoscopic management of benign bronchial stenosis by electrocautery and balloon dilatation
M. Garg, Pratibha Gogia, P. Manoria and R. Goyal .. 41
Tracheobronchial compression by right-sided aortic arch in a middle aged maleM.L. Gupta, C. Bhandari, M. Mishra and Jyotsna Sinha .. 45
Giant solitary fibrous tumour of the pleuraR. Burrah, K.V. Veerendra, V. Deshmane, Rama Rao C., S. Althaf, S. Pingali, A.D. Shah and Y. Srinivasalu .. 49
Pulmonary disease due to Mycobacterium massilienseSubhra Mitra, S.R. Tapadar, D. Banerjee, S. Bhattacharjee, Sunanda Dey, and S. Kundu .. 53
Short CommunicationRegression equations for spirometry in children aged 6 to 17 years in Delhi region
S.K. Chhabra, V.K. Vijayan, M. Rahman, V. Mittal and P.D. Singh .. 59
CorrespondenceDifference in the outcome of patients with different grades of initial sputum positivity underthe Revised National Tuberculosis Control Programme .. 64
Abstracts´ Service .. 66
Panel of Reviewers—2011 .. 70
Form-IV .. 71
Guidelines to Authors .. 73
Announcements 2, 4, 8, 18, 38,44, 48, 58, 69, 72
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 3

4 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
37th WORKSHOPON
RESPIRATORY ALLERGY: DIAGNOSIS AND MANAGEMENT
April 2 - 6, 2012
Organised by
VALLABHBHAI PATEL CHEST INSTITUTEUNIVERSITY OF DELHI, DELHI
In collaboration with
INSTITUTE OF GENOMICS AND INTEGRATIVE BIOLOGY, DELHI
Dear Friends,
You are well aware that there is an ever increasing number of patients seeking advice for respiratoryallergy and related problems. Many of these conditions can be improved with appropriate advice andtreatment reducing unnecessary suffering. Vallabhbhai Patel Chest Institute in collaboration withInstitute of Genomics and Integrative Biology is organising the “37th Workshop on Respiratory Allergy:Diagnosis and Management” during April 2-6, 2012. The topics are chosen to give up-to-date basicinformation about respiratory allergy and related conditions and the practical skills involved in theirmanagement. Hands on training in Allergy testing, PFT and laboratory investigations related torespiratory allergy will be provided at the Workshop.
Medical professionals working/with interest in respiratory allergy and applied immunologyare the target group of this Workshop.
Eligibility: Medical graduates with PG qualification in Medicine/Pediatrics/ENT/PulmonaryMedicine
Please send in your bio-data along with copies of certificates to Prof. S.N. Gaur orProf. Rajkumar, latest by March 7, 2012. Selected candidates will be required to pay the registrationfee of R5000/- in favour of Allergy Workshop-2012 through bank draft. Please write your e-mail ID forquick communication.
Organising Secretary Chairman, Organising Committee
Prof. Rajkumar Prof. S.N. GaurProfessor and Head Director (Actg), VPCI, andDepartment of Respiratory Allergy and Professor and HeadApplied Immunology Department of Respiratory MedicineVallabhbhai Patel Chest Institute Vallabhbhai Patel Chest InstituteUniversity of Delhi, Delhi-110 007 University of Delhi, Delhi-110 007E-mail: [email protected] E-mail: [email protected]: 91-11-27667102, 27667441 27667667, [email protected] (Extn 144) Phone: (0) 91-11-27667420, 27667820Mobile: 9810146835 Fax: 91-11-27667420

Editorial
[Indian J Chest Dis Allied Sci 2012;54:5-7]
The advent of chemotherapy in the early 1980’s was aboon for tuberculosis (TB) afflicted human race andsignificantly brought down mortality rate. However,an increase in the number of reported cases of TB inrecent times combined with the emergence of humanimmunodeficiency virus (HIV) and multidrug-resistantTB (MDR-TB) was a serious setback for the efforts toeradicate TB worldwide. Presently, as many as one-third of the global population is latently infected withMycobacterium tuberculosis and 5% to 10% of them runthe risk of developing active disease in their life-time.What could explain this inter-individual variation insusceptibility and proneness to develop active disease?Apart from the environment and socio-economicfactors, genetic predisposition of the host could play asignificant role in determining the outcome of theinfection. It could be possible that wide variation in thegenetic make-up of the human population manifestedin the form of gene polymorphisms could lead to suchinter-individual variation.
The history of the mankind indicates that TB exertsa strong selection pressure on human evolution. Overthe Century, TB significantly wiped out thesusceptible population from various parts of theworld and by the process of natural selection onlythose who could develop resistance to TB wereselected to survive and multiply. For example,European population are generally less susceptible toTB. It is possible that due to their centuries longassociation with the bacterium the Europeans haveevolved into a more resistant population. In contrast,African sub-Saharan population are highlysusceptible to TB probably due to their relativelyrecent contact with the pathogen.1 Motulsky2
suggested that this could have been due to strongselection against susceptibility genes of TB.
Examining the genetic angle of TB susceptibilityreceived impetus from the recent technologicaladvancement in the gene sequencing techniques.Rapid throughput sequencing at a large scale usingSequenom massArray platform (Sequenom Inc.,USA)or Illumina platform have resulted in the completesequencing of the human genome which led to theidentification of a large number of sequencepolymorphisms that were previously unknown. Thisinformation led to the generation of databases, suchas dbSNP3 and Hapmap4 which have facilitated theselection and evaluation of yet unexplored sequencevariants in the genes of interest.
Given the complexity of the disease TB, it can beassumed that there would be numerous geneticcontributing factors. Protection against TB is
determined by the potent immune response in anyindividual. Therefore, susceptibility or resistance todevelop TB may be significantly influenced by thevariation in the immune response genes andcontribute to a scenario where by virtue of theirgenetic make-up most of the individuals mount aneffective immune response and are able to either clearor contain the mycobacterial infection while a certainfew fail to do so. Evidence in support of such a notioncomes from clustering of TB disease with higherconcordance in monozygotic as against dizygotictwins,5 the ethnic clustering of the disease with higherprevalence of TB in individuals of recent Africandescent,6 as well as the demonstration of bothcommon polymorphisms and rare mutations whichconfer susceptibility to mycobacterial infection inhumans.7 These studies further supports the viewthat in addition to unique environment and naturalselection ethnically governed host genetic factors mayplay a part in the susceptibility or resistance to TB.
Since TB is primarily a disease governed by thestate of the host immune response, the focus ofpopulation genetics rested on the extensive analysesof the genes related to innate and acquired immuneresponse. The technological advances as mentionedabove together with the tools of bioinformaticsfacilitated the identification of a range of geneticvariations which include polymorphisms in theinnate and acquired immune factor related genescapable of identifying persons who are geneticallyprone to TB. The studies evaluating the involvementof innate immune response have focused on receptorson macrophages, such as toll-like receptors includingTLR1, TLR2, TLR4 and TLR8, VDR, NOS2, P2X7receptor, SP110, SLC11A (formerly NRAMP1), IRGMand DC-SIGN.8 On the other hand, the adaptiveimmune response was characterised mainly bycytokine and chemokine gene polymorphisms. Thecytokines of note that have been studied and thoughtto play a role in susceptibility to TB include variantsof interferon-gamma (IFN-γ), tumour necrosis factor-alpha (TNF-α), interleukin (IL)-1β, IL-1RA, IL-18, IL-8,IL-12, and TNF-β.9
The impact of genetic variants has also beenexemplified in other associated respiratory ailments,such as asthma,10 and chronic obstructive pulmonarydisease (COPD).11 In both these conditions, selectionof genes studied were those related to inflammatoryprocess and are similar to the genes studied in TB.One possible reason for such overlap might be theinvolvement of an initial inflammatory phase in allthe three diseases. As and when more information
Decoding Population Genetics: Impact on TuberculosisControl and Treatment

66 Editorial Mridula Bose
will be available the interacting role of these genescontributing to each condition may become clearer.
The impact of genetic make-up of the host on thedevelopment of TB has been studied in Indianpopulation also. Recently a database called theIndian genome variation database (IGVDB)12 hasbeen developed on the lines of Hapmap database. TheHapmap database includes the variation frequenciestyped in five world populations but does not includethe Indian population. The IGVDB has typed certainselected sequence polymorphism in samples from allover India and facilitated the classification of theIndian population into structured subgroups. Thisdatabase has shown that the gene pools of north andsouth Indians differ significantly in their geneticmake-up which means variations posing a risk insouth Indians need not be valid for north Indians, asgenetic proneness to susceptibility to TB has aethnicity bias. While some reports are available fromsouth India,13 till recently not much information wasavailable from north India. Abhimanyu et al,14,15 haverecently added to the spectrum of studies on geneticsusceptibility to TB from north India. So far, aftertyping more than 50 variants from 7 cytokine genes,they were able to identify 11 novel variants implicatedin TB susceptibility.14,15 In addition, they have alsoexamined the possible impact of population geneticsin lymph node TB, a form of extra-pulmonary TB, forthe first time in the north Indian patients. Theyexamined 25 variants of SP110 gene for susceptibilityto TB and identified for the first time a variant(rs1427294) that could be a useful marker for lymphnode TB susceptibility in north Indians.16
The benefit of such studies could be multiple. Theinformation generated would help us to identify thegenetic markers to screen people of being “resistant”or “prone” to the disease. Identifying the alleles thatimpart a risk of developing the disease in thepopulation under study and the identified markerscould help in providing appropriate and targetedtherapy to the prone individuals. A few evidence insupport of this notion stems from the work done withthe help of SNPs in other diseases, such as lungcancer,17 Hutington’s disease, etc. Pfister et al18 havedesigned and validated selective siRNAs for the threeSNP sites of Hutington’s disease, laying thefoundation for allele-specific RNA interference(RNAi) therapy for Hutington’s disease. SNPs couldalso be very useful in giving personalised medicine asshown by Chu et al.17 As outlined by Barnes19
immunotherapeutic strategies for TB could includeadministration of Th1 cytokines, such as IL-2 orIFN-γ, or of IL-12 and IL-18, which elicit IFN-γproduction which is vital for protection against TB.Alternatively, natural inhibitors of transforminggrowth factor-β or anti–IL-10 antibodies could be
used to downregulate the Th2 response, in patientswho could be identified successfully by theirsusceptible status utilising SNP information to thiseffect. A personalised medicine on the lines of cancertherapy can also be developed as individuals withTB have been shown to differentially metaboliseisoniazid (INH), categorised as slow acetylators orfast acetylators,20 thereby, affecting the outcome of thetreatment. SNPs identified could help us sort thoseindividuals out who are fast acetylators and treatthem with some alternate drug.
While a large body of data is being generatedglobally, there are still conflicts to recognise therelevance of these genetic markers in the context ofdisease development. The markers reported in acertain population may not be found to be the riskfactors in other population. Such observations couldbe due to lack of carefully planned studies, poorcontrol selection or presence of population sub-structure21 in the analysed data. These points are ofutmost importance and should be taken into accountwhile analysing a genetic dataset to draw a robustand lasting conclusion that would influence thefuture application of the emerging information in thetreatment and control of TB.
At this crucial juncture we find ourselves askingthe question: now what? The future direction could beto validate the commonly reported variantsthroughout the world in the context of Indianregional ethnicity, detecting the changes caused bythe identified polymorphisms to conclusivelydemonstrate the “cause and effect” correlation. Inaddition, there should be persistent efforts to identifynew loci by conducting more carefully planned multi-centre studies. Finally, the “genetic markers”identified must be utilised to develop certainmodules that would aid the current approach todiagnosis and treatment.
The quest for genetic polymorphisms translatinginto population genetics have come a long way andstill has a longer path to traverse. But the systematicefforts should continue to facilitate betterunderstanding of the genetic basis of resistance orsusceptibility to TB which could be translated intotargeted immunotherapy as a preventive measure aswell as an effective adjunct to multidrug therapy for TB.
Mridula BoseMember, Editorial Board, and
Professor and Head,Department of Microbiology
V.P. Chest InstituteUniversity of Delhi
Delhi; IndiaE-mail: [email protected]

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 7
REFERENCES
1. Moller M, Hoal EG. Current findings, challenges and novelapproaches in human genetic susceptibility totuberculosis. Tuberculosis 2010;90:71-83.
2. Motulsky AG. Metabolic polymorphism and the role ofinfectious diseases in human evolution. Hum Biol1960;32:28-62.
3. Database SNP. Available at: http://www.ncbi.nlm.nih.gov/projects/SNP
4. Hapmap database. Available at: http://hapmap.ncbi.nlm.nih.gov
5. Comstock GW. Tuberculosis in twins: a re-analysis of theProphit survey. Am Rev Respir Dis 1978;117:621-4.
6. Stead WW, Senner JW, Reddick WT, Lofgren JP. Racialdifferences in susceptibility to infection by Mycobacteriumtuberculosis. N Engl J Med 1990;322:422-7.
7. Doffinger R, Dupuis S, Picard C, Fieschi C, Feinberg J,Barcenas-Morales G, et al. Inherited disorders of IL-12 andIFN-gamma-mediated immunity: a molecular geneticsupdate. Mol Immunol 2002;38:903-9.
8. Moller M, de Wit E , Hoal EG. Past, present and futuredirections in human genetic susceptibility to tuberculosis.FEMS Immunol Med Microbiol 2010;58:3-26.
9. Yim JJ, Selvaraj P. Genetic susceptibility in tuberculosis.Respirology 2010;15:241-56.
10. Smolonska J, Wijmenga C, Postma DS, Boezen HM. Meta-analyses on suspected chronic obstructive pulmonarydisease genes: a summary of 20 years’ research. Am JRespir Crit Care Med 2009;180:618-31.
11. Haukim N, Bidwell JL, Smith AJP, Keen LJ, Gallagher G,Kimberly R, et al. Cytokine gene polymorphism in humandisease: on-line databases. Gen Immun 2002;3:(Suppl. 2):313-30.
12. Indian Genome Variation Consortium. Genetic landscapeof the people of India: a canvas for disease geneexploration. J Genet 2008;87:3-20.
13. Yim JJ, Selvaraj P. Genetic susceptibility in tuberculosis.Respirology 2010;15:241-56.
14. Abhimanyu, Mangangcha IR, Jha P, Arora K, Mukerji M,Banavaliker JN, et al. Differential serum cytokine levels areassociated with cytokine gene polymorphisms in northIndians with active pulmonary tuberculosis. Infect GenetEvol 2011;11:1015-22.
15. Abhimanyu, Consortium IGV, Jha P, Bose M. Footprints ofgenetic susceptibility to tuberculosis: cytokine gene variantsin north Indians. Indian J Med Res 2011. (In Press)
16. Abhimanyu, Jha P, Jain A, Arora K, Bose M. Geneticassociation study suggests a role of SP110 polymorphismin lymph node tuberculosis but not pulmonary tuberculosisin north Indians. Hum Immunol 2011;72:576-80.
17. Chu CT, Jacoby JJ, Herbst RS. Future directions ofmonoclonal antibody use in personalized lung cancertherapy. Oncology 2010;24:1-4.
18. Pfister EL, Kennington L, Straubhaar J, Wagh S, Liu W,DiFiglia M, et al. Five siRNAs targeting three SNPs mayprovide therapy for three-quarters of huntington’s diseasepatients. Curr Biol 2009;19:774-8.
19. Barnes PF. Immunotherapy for tuberculosis: waves of thefuture or tilting at the windmills. Am J Respir Crit Care Med2003;168:142-3.
20. Augustynowicz-Kopeæ E , Zwolska Z, Niemirowska-Mikulska H. Bioavailability of isoniazid in healthyvolunteers—fast and slow INH acetylators. PneumonolAlergol Pol 2002;70:167-79.
21. Choudhry S, Coyle NE, Tang H, Salari K, Lind D, Clark SL.Population stratification confounds genetic associationstudies among Latinos. Hum Genet 2006;118:652-64.
8 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54

Original Article
[Received: April 8, 2011; accepted after revision: June 27, 2011]
Correspondence and reprint requests: Dr Ritu Kulshrestha, Assistant Professor, Department of Pathology, VallabhbhaiPatel Chest Institute, University of Delhi, Delhi-110 007, India; Phone: 91-11-27667667, 27666182 Extn 114; Fax 91-11-27667549;E-mail: [email protected]
Role of a Pattern-based Approach in Interpretation ofTransbronchoscopic Lung Biopsy and Its Clinical Implications
Ritu Kulshrestha1, B.K. Menon2, Rajkumar2 and V.K. Vijayan3
Departments of Pathology1, Respiratory Allergy and Applied Immunology2 and Respiratory Medicine3,Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India
ABSTRACT
Background. Transbronchial lung biopsy (TBLB) is commonly performed for confirming the tissue diagnosis of diffuseparenchymal lung diseases (DPLDs). There is an urgent need to establish guidelines for interpretation of TBLB in order toimprove its diagnostic utility.
Methods. We retrospectively studied 916 consecutive patients (494 males; mean age 49 years) who underwent TBLB overa 5-year period (July 2005 to July 2010) at Vallabhbhai Patel Chest Institute.
Results. In 615 (67.1%) procedures, material obtained during TBLB was adequate for histopathology interpretation.Pathological features evaluated in each case were: alveolar architecture, inflammatory infiltrate, interstitial fibrosis, atypicalcells, pigment deposition, honey-comb change and fibroblast foci. The cases were categorised on the basis of histopathologyinto six patterns: (1) adequate biopsy without a specific diagnostic abnormality (n=137, 22.3%); (2) acute pneumonitis (n=29,4.7%); (3) neoplasia (n=109, 17.7%); (4) chronic interstitial inflammation with or without fibrosis (n=138, 22.4%); (5)granulomatous inflammation, (n=186, 30.2%); and (6) other specific causes (n=16, 2.6%). Definitive diagnosis could be madeafter correlation of TBLB histopathology with clinical and radiological features in 55.3% cases.
Conclusions. TBLB appears to be an important diagnostic tool for the diagnosis of DPLDs. The use of a pattern-basedapproach to TBLB adds to its diagnostic yield and can be helpful in cases where open lung biopsy is not available.[Indian J Chest Dis Allied Sci 2012;54:9-17]
Key words: TBLB, Diffuse lung disease, Histopathological patterns.
INTRODUCTION
Transbronchial lung biopsy (TBLB) is often employedin the diagnosis of diffuse parenchymal lung diseases(DPLDs). Due to the high morbidity associated withand the non-availability of open lung biopsy (OLB) inmany centres, high resolution computed tomography(HRCT) followed by TBLB continue to remain themainstay of diagnosis of DPLDs. The small size ofTBLB specimen makes it a “histopathologist’snightmare”, leading to difficulty in categorisationwithin the spectrum of DPLDs. Therefore, TBLB isconsidered by some as an ‘ailing gold standard’ andis utilised only to exclude diseases, such as,sarcoidosis, lymphangitis carcinomatosis, infection,etc. There is a need for systematic categorisation of thehistopathological patterns identified on TBLB forincreasing the diagnostic yield and their rigorouscorrelation with clinical and radiological features forconfirming the diagnosis accurately. The present
study was undertaken to evaluate the histo-pathological patterns identified on TBLB and theclinical usefulness of TBLB in the diagnosis ofpatients with DPLDs presenting to a tertiary carepulmonary centre in North India.
MATERIAL AND METHODS
We retrospectively analysed records of 916 patientswho underwent TBLB at the Vallabhbhai Patel ChestInstitute over a 5-year period from July 2005 to July2010. All specimens were stained with haematoxylin-eosin stain; special stains for reticulin and collagen;Gomori silver methenamine; and Masson Trichromestains. Periodic acid-Schiff stain, Gomori silvermethenamine stain, Gram’s stain, Ziehl-Neelsen stain(Z-N) were done to rule out infection. Treatmenthistory was obtained to rule out drug-toxicity.
The number of pieces of alveolated lungparenchyma and bronchial wall were recorded. The
10
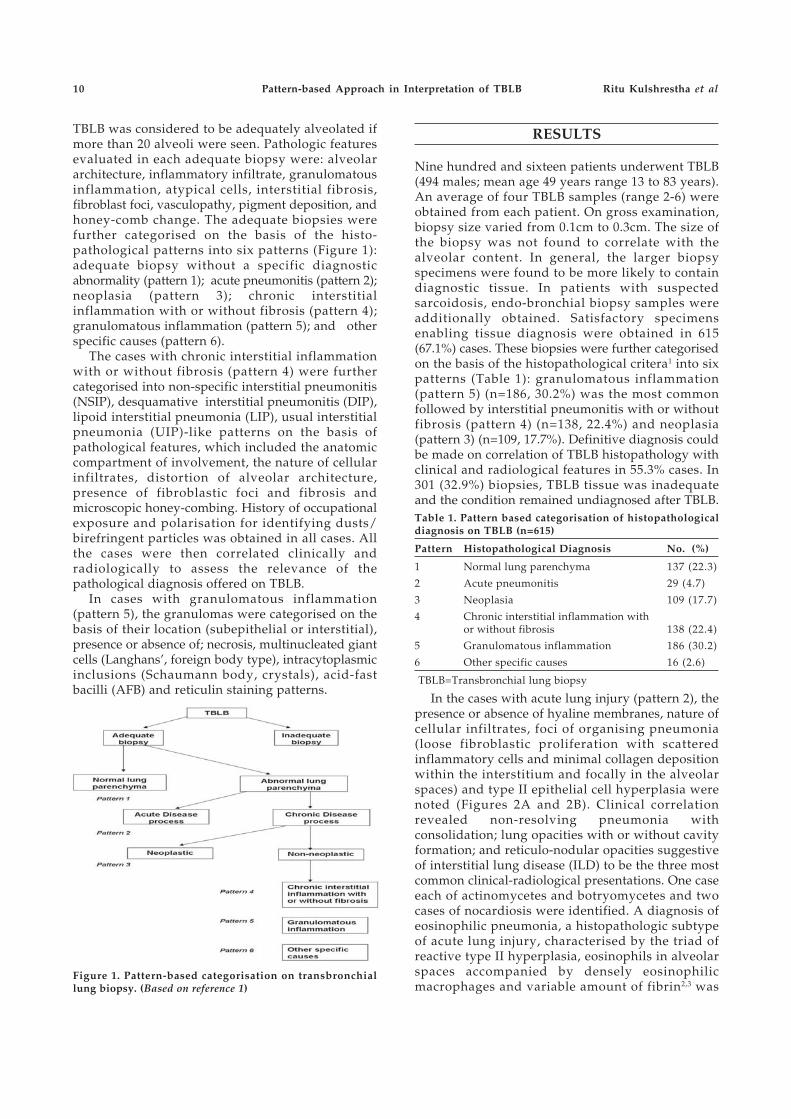
TBLB was considered to be adequately alveolated ifmore than 20 alveoli were seen. Pathologic featuresevaluated in each adequate biopsy were: alveolararchitecture, inflammatory infiltrate, granulomatousinflammation, atypical cells, interstitial fibrosis,fibroblast foci, vasculopathy, pigment deposition, andhoney-comb change. The adequate biopsies werefurther categorised on the basis of the histo-pathological patterns into six patterns (Figure 1):adequate biopsy without a specific diagnosticabnormality (pattern 1); acute pneumonitis (pattern 2);neoplasia (pattern 3); chronic interstitialinflammation with or without fibrosis (pattern 4);granulomatous inflammation (pattern 5); and otherspecific causes (pattern 6).
The cases with chronic interstitial inflammationwith or without fibrosis (pattern 4) were furthercategorised into non-specific interstitial pneumonitis(NSIP), desquamative interstitial pneumonitis (DIP),lipoid interstitial pneumonia (LIP), usual interstitialpneumonia (UIP)-like patterns on the basis ofpathological features, which included the anatomiccompartment of involvement, the nature of cellularinfiltrates, distortion of alveolar architecture,presence of fibroblastic foci and fibrosis andmicroscopic honey-combing. History of occupationalexposure and polarisation for identifying dusts/birefringent particles was obtained in all cases. Allthe cases were then correlated clinically andradiologically to assess the relevance of thepathological diagnosis offered on TBLB.
In cases with granulomatous inflammation(pattern 5), the granulomas were categorised on thebasis of their location (subepithelial or interstitial),presence or absence of; necrosis, multinucleated giantcells (Langhans’, foreign body type), intracytoplasmicinclusions (Schaumann body, crystals), acid-fastbacilli (AFB) and reticulin staining patterns.
Figure 1. Pattern-based categorisation on transbronchiallung biopsy. (Based on reference 1)
RESULTS
Nine hundred and sixteen patients underwent TBLB(494 males; mean age 49 years range 13 to 83 years).An average of four TBLB samples (range 2-6) wereobtained from each patient. On gross examination,biopsy size varied from 0.1cm to 0.3cm. The size ofthe biopsy was not found to correlate with thealveolar content. In general, the larger biopsyspecimens were found to be more likely to containdiagnostic tissue. In patients with suspectedsarcoidosis, endo-bronchial biopsy samples wereadditionally obtained. Satisfactory specimensenabling tissue diagnosis were obtained in 615(67.1%) cases. These biopsies were further categorisedon the basis of the histopathological critera1 into sixpatterns (Table 1): granulomatous inflammation(pattern 5) (n=186, 30.2%) was the most commonfollowed by interstitial pneumonitis with or withoutfibrosis (pattern 4) (n=138, 22.4%) and neoplasia(pattern 3) (n=109, 17.7%). Definitive diagnosis couldbe made on correlation of TBLB histopathology withclinical and radiological features in 55.3% cases. In301 (32.9%) biopsies, TBLB tissue was inadequateand the condition remained undiagnosed after TBLB.Table 1. Pattern based categorisation of histopathologicaldiagnosis on TBLB (n=615)
Pattern Histopathological Diagnosis No. (%)
1 Normal lung parenchyma 137 (22.3)
2 Acute pneumonitis 29 (4.7)
3 Neoplasia 109 (17.7)
4 Chronic interstitial inflammation withor without fibrosis 138 (22.4)
5 Granulomatous inflammation 186 (30.2)
6 Other specific causes 16 (2.6)
TBLB=Transbronchial lung biopsy
In the cases with acute lung injury (pattern 2), thepresence or absence of hyaline membranes, nature ofcellular infiltrates, foci of organising pneumonia(loose fibroblastic proliferation with scatteredinflammatory cells and minimal collagen depositionwithin the interstitium and focally in the alveolarspaces) and type II epithelial cell hyperplasia werenoted (Figures 2A and 2B). Clinical correlationrevealed non-resolving pneumonia withconsolidation; lung opacities with or without cavityformation; and reticulo-nodular opacities suggestiveof interstitial lung disease (ILD) to be the three mostcommon clinical-radiological presentations. One caseeach of actinomycetes and botryomycetes and twocases of nocardiosis were identified. A diagnosis ofeosinophilic pneumonia, a histopathologic subtypeof acute lung injury, characterised by the triad ofreactive type II hyperplasia, eosinophils in alveolarspaces accompanied by densely eosinophilicmacrophages and variable amount of fibrin2,3 was
Pattern-based Approach in Interpretation of TBLB Ritu Kulshrestha et al
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 11
made in 4% cases. In one case with bronchial asthma,the presence of eosinophilic pneumonitis withvasculitis was suggestive of Churg-Strauss syndrome.
A
Figure 2. Acute pneumonitis (Pattern 2). Photomicrographshowing (A) acute neutrophilic parenchymal infiltrateleading to loss of alveolar architecture (Haematoxylin andeosin×40); and (B) high power view of the same(Haematoxylin and eosin×400).
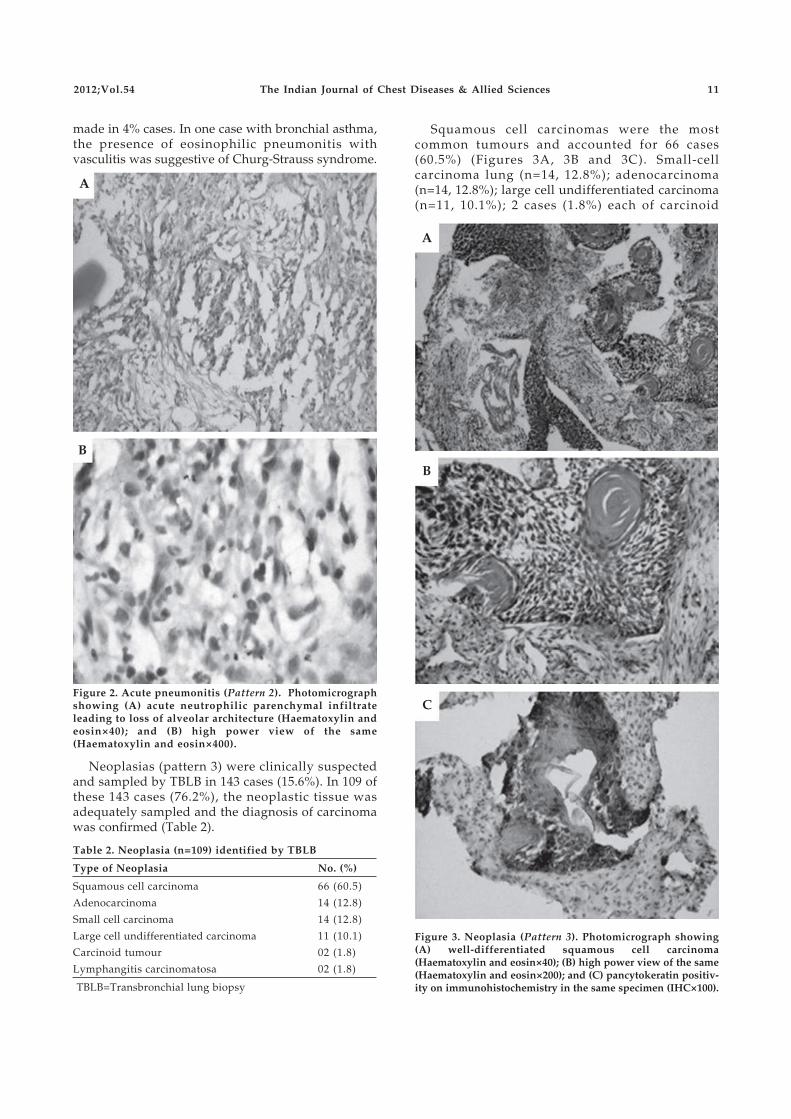
Neoplasias (pattern 3) were clinically suspectedand sampled by TBLB in 143 cases (15.6%). In 109 ofthese 143 cases (76.2%), the neoplastic tissue wasadequately sampled and the diagnosis of carcinomawas confirmed (Table 2).
A
B
C
Figure 3. Neoplasia (Pattern 3). Photomicrograph showing(A) well-differentiated squamous cell carcinoma(Haematoxylin and eosin×40); (B) high power view of the same(Haematoxylin and eosin×200); and (C) pancytokeratin positiv-ity on immunohistochemistry in the same specimen (IHC×100).
Table 2. Neoplasia (n=109) identified by TBLB
Type of Neoplasia No. (%)
Squamous cell carcinoma 66 (60.5)
Adenocarcinoma 14 (12.8)
Small cell carcinoma 14 (12.8)
Large cell undifferentiated carcinoma 11 (10.1)
Carcinoid tumour 02 (1.8)
Lymphangitis carcinomatosa 02 (1.8)
TBLB=Transbronchial lung biopsy
B
Squamous cell carcinomas were the mostcommon tumours and accounted for 66 cases(60.5%) (Figures 3A, 3B and 3C). Small-cellcarcinoma lung (n=14, 12.8%); adenocarcinoma(n=14, 12.8%); large cell undifferentiated carcinoma(n=11, 10.1%); 2 cases (1.8%) each of carcinoid
12
tumour and lymphangitis carcinomatosa wereindentified. Out of 143 cases, TBLB was inadequatein 34 (23.8%) for opinion due to following causes: (a)superficial biopsy taken because of increasedvascularity and bleeding tendency; (b) mass lesionobstructing passage of bronchoscope; and(c) sampling of the periphery of the lesion showing
pneumonitis with or without overlying epithelialdysplasia and/or carcinoma in-situ.
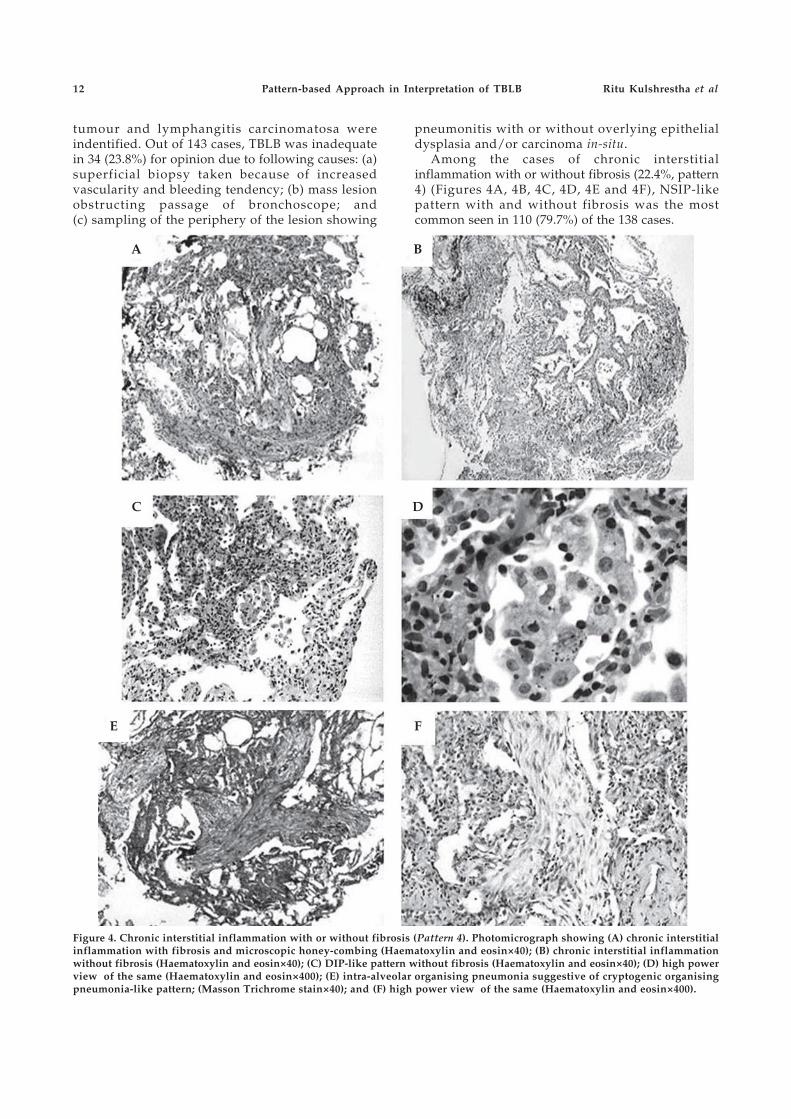
Among the cases of chronic interstitialinflammation with or without fibrosis (22.4%, pattern4) (Figures 4A, 4B, 4C, 4D, 4E and 4F), NSIP-likepattern with and without fibrosis was the mostcommon seen in 110 (79.7%) of the 138 cases.
Figure 4. Chronic interstitial inflammation with or without fibrosis (Pattern 4). Photomicrograph showing (A) chronic interstitialinflammation with fibrosis and microscopic honey-combing (Haematoxylin and eosin×40); (B) chronic interstitial inflammationwithout fibrosis (Haematoxylin and eosin×40); (C) DIP-like pattern without fibrosis (Haematoxylin and eosin×40); (D) high powerview of the same (Haematoxylin and eosin×400); (E) intra-alveolar organising pneumonia suggestive of cryptogenic organisingpneumonia-like pattern; (Masson Trichrome stain×40); and (F) high power view of the same (Haematoxylin and eosin×400).
A B
C D
E F
Pattern-based Approach in Interpretation of TBLB Ritu Kulshrestha et al

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 13
On correlation (Table 3) the final diagnosis offeredincluded ILD associated with collagen vasculardiseases, tuberculosis fibrocavitary lesions,pneumoconiosis, post-radiation fibrosis andidiopathic interstitial pneumonias. DIP-like pattern,seen in 18 of the 138 (13.0%) cases was next mostcommon pattern and was seen in ILD associated withsmokers. Distortion of alveolar architecture withmicroscopic honey-combing and presence offibroblastic foci were the criteria used to differentiateUIP-like pattern from fibrosing NSIP and was seen inseven of the 138 (5.2%) cases. These correlated withhoney-combing and fibrosis on computedtomography. In three (2.2%) cases with rheumatoidarthritis associated lung disease, interstitialinfiltration and widening by lymphocytic infiltratewas seen and categorised as LIP-like pattern. Eventhough the diagnosis offered by TBLB histopathologyalone were not conclusive, the exclusion of theinfectious and neoplastic pathologies in these cases,in the absence of OLB, was very helpful in furthermanagement of these patients, especially in light ofclinical and radiological features and pulmonaryfunction tests.
Table 3. Clinical-radiological-pathological correlation ofcases showing interstitial inflammation with or withoutfibrosis on TBLB (Pattern 4, n=138)
Histopathological Clinical No. (%)Features Diagnosis
NSIP pattern Tuberculosis, collagen 110 (79.7)vascular diseases,sarcoidosis,pneumoconiosis,post-radiation fibrosis,idiopathic ILD
DIP pattern ILD associated with 18 (13.0)smokers
UIP pattern Tuberculosis, collagen 07 (5.2)vascular diseases,pneumoconiosis, IPF
LIP pattern Rheumatoid arthritis 03 (2.2)associated lung disease
TBLB=Transbronchial lung biopsy; NSIP=Non-specificinterstitial pneumonitis; ILD=Interstitial lung disease;DIP=Desquamative interstitial pneumonia; UIP=Usualinterstitial pneumonia; IPF=Idiopathic pulmonary fibrosis;LIP=Lipoid interstitial pneumonia
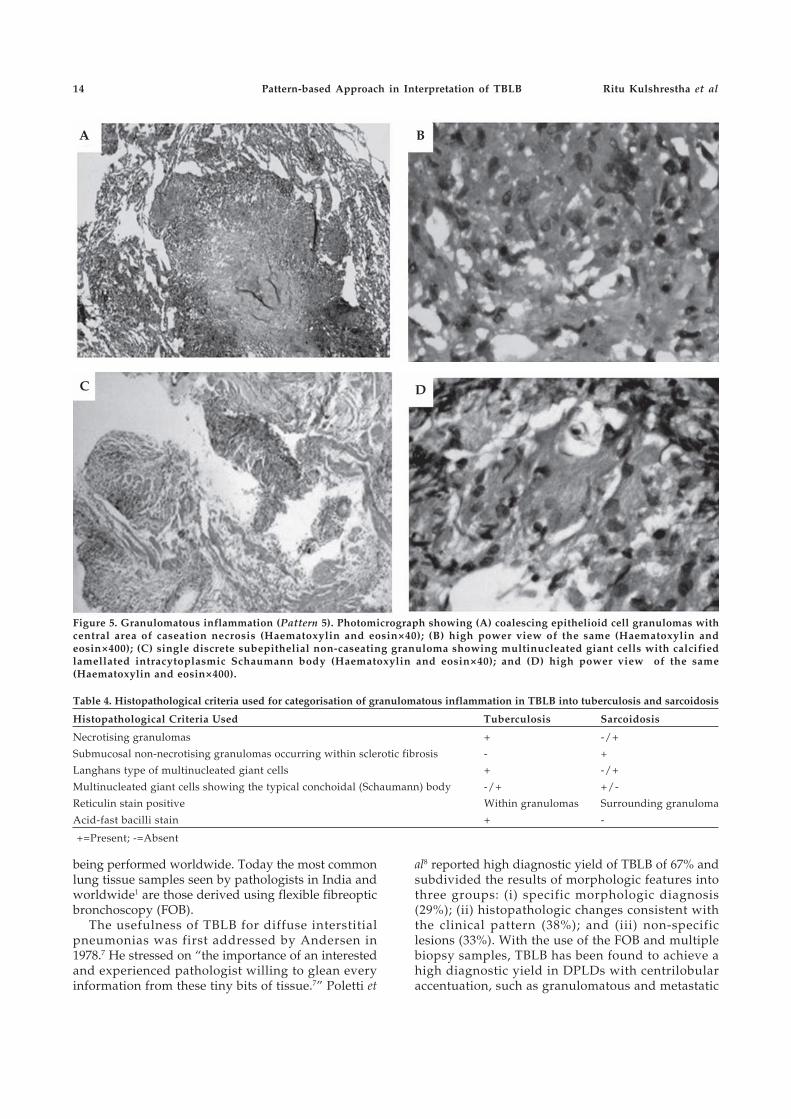
Granulomatous inflammation (pattern 5) was seenin 186 (30.3%) cases. Using the histopathologicalcriteria and correlating with clinical and radiologicalfeatures, bronchoalveolar lavage fluid analysis andAFB culture, the diagnosis of tuberculosis wasconfirmed (Figures 5A and 5B) in 121 (65.1%) cases(Table 4). Submucosal non-necrotising granulomasoccurring within sclerotic fibrosis, with multi-nucleated giant cells showing the typical conchoidal(Schaumann) body (Figures 5C and 5D), diagnosticof sarcoidosis were seen in 46 (24.7%) cases. In
19 (10.2%) cases a definitive diagnosis could not beobtained after bronchoscopy and these subjects werereferred for surgical biopsy or were empiricallystarted on antituberculosis treatment.
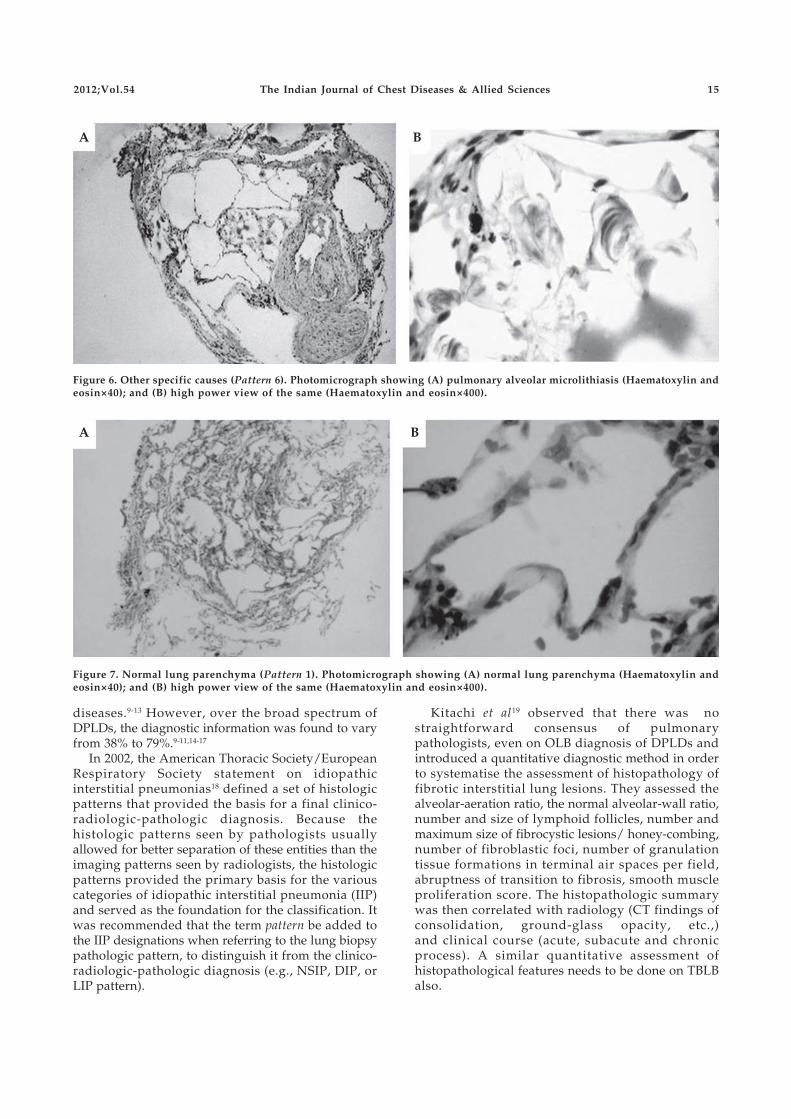
Other specific causes (pattern 6) identified on TBLBaccounted for 16 cases (2.6%). These included 3 caseswith diffuse alveolar haemorrhage, which wereconfirmed by the Perl’s Prussian blue stain.Pulmonary vasculitis, characterised by damage to thevessel wall and accompanied by fibrin depositionwas seen in two cases. Four cases primarily showedfeatures of pulmonary artery hypertension whichwere low grade lesions: grade 1 (muscularhypertrophy) and grade 2 (mild intimalproliferation).4 One case each with pulmonaryalveolar proteinosis, alveolar microlithiasis (Figures6A and 6B) and pulmonary lymphangioleio-myomatosis were identified on TBLB. A rigorousclinical-radiological-pathological correlation wasimportant in coming to a definitive diagnosis in thesecases.
An adequate lung parenchymal biopsy without aspecific diagnostic abnormality (pattern 1) (Figures7A and 7B) was identified in 137 (22.3%) cases. Thesewere the cases with radiological abnormalities buthad no abnormalities seen in the lung biopsies,signifying them to be a result of either ‘minimalchange disease’ or ‘sampling error’. In 301 (32.9%)procedures, tissue was considered inadequate foropinion since it comprised of superficial epitheliumonly and/or alveolar tissue with less than 20 alveoli.Analysis of these cases revealed various factorspredisposing to these failures and included lack ofpatient co-operation, excessive coughing, bleedingleading to termination of the procedure. These caseswere then referred for OLB and/or clinical-radiological correlation.
DISCUSSION
The DPLDs comprise of a wide spectrum of over 200diseases.5 Many of these diseases have similarclinical presentations with widespread shadowingon the chest radiograph and increasing shortness ofbreath. Occasionally the radiographic appearancesare sufficiently characteristic to enable a specificdiagnosis, for example, sarcoidosis, pulmonaryeosinophilia, some occupational lung diseases, etc.However, in most patients, chest radiographicpatterns are not specific. The final diagnosis can bemade from clinical-radiological correlation in about50% of cases only.6 Surgical OLB, considered to be thegold standard for the diagnosis of DPLDs, however, isassociated with greater morbidity and cost. Moreover,OLB is not available in most centres in thedeveloping countries, such as, India. This has lead toa slow but steady increase in the number of TBLBs
14
being performed worldwide. Today the most commonlung tissue samples seen by pathologists in India andworldwide1 are those derived using flexible fibreopticbronchoscopy (FOB).
The usefulness of TBLB for diffuse interstitialpneumonias was first addressed by Andersen in1978.7 He stressed on “the importance of an interestedand experienced pathologist willing to glean everyinformation from these tiny bits of tissue.7” Poletti et
Figure 5. Granulomatous inflammation (Pattern 5). Photomicrograph showing (A) coalescing epithelioid cell granulomas withcentral area of caseation necrosis (Haematoxylin and eosin×40); (B) high power view of the same (Haematoxylin andeosin×400); (C) single discrete subepithelial non-caseating granuloma showing multinucleated giant cells with calcifiedlamellated intracytoplasmic Schaumann body (Haematoxylin and eosin×40); and (D) high power view of the same(Haematoxylin and eosin×400).
A B
C D
Table 4. Histopathological criteria used for categorisation of granulomatous inflammation in TBLB into tuberculosis and sarcoidosis
Histopathological Criteria Used Tuberculosis Sarcoidosis
Necrotising granulomas + -/+
Submucosal non-necrotising granulomas occurring within sclerotic fibrosis - +
Langhans type of multinucleated giant cells + -/+
Multinucleated giant cells showing the typical conchoidal (Schaumann) body -/+ +/-
Reticulin stain positive Within granulomas Surrounding granuloma
Acid-fast bacilli stain + -
+=Present; -=Absent
al8 reported high diagnostic yield of TBLB of 67% andsubdivided the results of morphologic features intothree groups: (i) specific morphologic diagnosis(29%); (ii) histopathologic changes consistent withthe clinical pattern (38%); and (iii) non-specificlesions (33%). With the use of the FOB and multiplebiopsy samples, TBLB has been found to achieve ahigh diagnostic yield in DPLDs with centrilobularaccentuation, such as granulomatous and metastatic
Pattern-based Approach in Interpretation of TBLB Ritu Kulshrestha et al
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 15
Figure 6. Other specific causes (Pattern 6). Photomicrograph showing (A) pulmonary alveolar microlithiasis (Haematoxylin andeosin×40); and (B) high power view of the same (Haematoxylin and eosin×400).
A B
Figure 7. Normal lung parenchyma (Pattern 1). Photomicrograph showing (A) normal lung parenchyma (Haematoxylin andeosin×40); and (B) high power view of the same (Haematoxylin and eosin×400).
diseases.9-13 However, over the broad spectrum ofDPLDs, the diagnostic information was found to varyfrom 38% to 79%.9-11,14-17
In 2002, the American Thoracic Society/EuropeanRespiratory Society statement on idiopathicinterstitial pneumonias18 defined a set of histologicpatterns that provided the basis for a final clinico-radiologic-pathologic diagnosis. Because thehistologic patterns seen by pathologists usuallyallowed for better separation of these entities than theimaging patterns seen by radiologists, the histologicpatterns provided the primary basis for the variouscategories of idiopathic interstitial pneumonia (IIP)and served as the foundation for the classification. Itwas recommended that the term pattern be added tothe IIP designations when referring to the lung biopsypathologic pattern, to distinguish it from the clinico-radiologic-pathologic diagnosis (e.g., NSIP, DIP, orLIP pattern).
A B
Kitachi et al19 observed that there was nostraightforward consensus of pulmonarypathologists, even on OLB diagnosis of DPLDs andintroduced a quantitative diagnostic method in orderto systematise the assessment of histopathology offibrotic interstitial lung lesions. They assessed thealveolar-aeration ratio, the normal alveolar-wall ratio,number and size of lymphoid follicles, number andmaximum size of fibrocystic lesions/ honey-combing,number of fibroblastic foci, number of granulationtissue formations in terminal air spaces per field,abruptness of transition to fibrosis, smooth muscleproliferation score. The histopathologic summarywas then correlated with radiology (CT findings ofconsolidation, ground-glass opacity, etc.,)and clinical course (acute, subacute and chronicprocess). A similar quantitative assessment ofhistopathological features needs to be done on TBLBalso.

16
Berbescu et al20 reported that, characteristichistologic features of UIP, a combination ofpatchwork fibrosis, fibroblast foci, and microscopichoney-combing, could be identified on TBLBspecimens. This has lead to renewed interest in role ofTBLB in diffuse interstitial lung diseases.21 TBLB hasalso been found to be clinically useful in thediagnosis of 75% cases of DPLDs;21 in the 25% ofTBLBs that were clinically unhelpful, there wasfailure of the procedure to obtain an adequate quantityof lung parenchyma for a meaningful histologicalanalysis. Leslie et al1 have elaborated the mostcommon diagnostic entities and histopathologicpatterns seen in TBLB in the setting of diffuse ormultifocal lung disease. These included, acute lunginjury, eosinophilic pneumonia, diffuse alveolarhaemorrhage, chronic cellular infiltrates with orwithout fibrosis, organising pneumonia, alveolarproteinosis, sarcoidosis, Wegener’s granulomatosis,intravenous drug abuse related microangiopathy,Langerhans cell histiocytosis and lymphangio-leiomyomatosis. These were further categorised onthe basis of histopathological pattern of lesion intofive patterns: (i) acute or subacute injury; (ii) chronicinterstitial inflammation with or without fibrosis; (iii)granulomatous inflammation; (iv) vascular diseases(e.g., vasculitis, diffuse alveolar haemorrhage,intravenous drug abuse microangiopathy; and(v) alveolar filling processes (alveolar proteinosis, etc.).
In the present study, we retrospectively analysedthe TBLB submitted over 5-year period and used thesystematic pattern-based approach described byLeslie et al1 to categorise the histopathologicalfeatures into six histopathological patterns. The threemost common diagnostic patterns in our study weregranulomatous inflammation, chronic interstitialpneumonitis and carcinoma lung. In 32.9%procedures, no lung parenchyma was obtained. Thiswas similar to the earlier observations where theproblem of inadequate lung tissue from TBLB wasobserved in up to 20% of patients.22 The pattern-basedcategorisation added the much needed guidelines tointerpretation of TBLB histopathology and providedclarity to clinicians when submitted for correlationwith clinical and radiological features.
TBLB showing chronic interstitial pneumonitis,with or without fibrosis was the second commonestfinding in our series and the most difficult to interpret.Review of existing literature revealed that previouslythis finding was considered to be only helpful insupporting a clinical impression of DPLDs orreported as non-diagnostic since the TBLB specimenswere generally considered to be too small and non-representative to determine the relative degree ofcellularity and fibrosis. 14,15,23 In the present series too,a confirmatory diagnosis could be given in these casesonly after they were correlated clinically andradiologically to assess the relevance of the
pathological diagnosis offered on TBLB. Distortion ofalveolar architecture with microscopic honey-combing and the presence of fibroblastic foci were thecriteria used to differentiate UIP pattern fromfibrosing NSIP and these were seen to correlate withhoney-combing and fibrosis on CT.
Serious questions on the use of TBLB for thediagnosis of UIP have also been raised,24 especiallysince TBLB samples are insufficient to determinetemporal heterogeneity, a critical histologic hallmark.The identification of ‘concordant pattern of UIP’, inwhich all lobes showed UIP and there is no evidenceof intra-patient variation and ‘discordant UIPpattern’ in which intra-patient variation with lunglobes showing a mixture of UIP and NSIP is present25
has further compounded the problem of pattern-based diagnosis by TBLB in these two conditions.Therefore, the current assumption is that there is nogold standard for the diagnosis of DPLDs, and clinical,radiologic, and histopathologic evaluation by OLB,have emerged as the silver standard.18
Interstitial lung diseases appear to be under-reported from India. The lack of recognition andinadequate availability of diagnostic facilities, likeHRCT are thought to be some of the main reasons forthis.26 Previously, Ahluwalia et al27 have assessed therole of TBLB in ILD and concluded that FOB andTBLB are safe and useful adjuncts to the diagnosis ofILD. The correlation of TBLB histological featureswith spirometric indices has also been reported insarcoidosis by Gupta et al.28
TBLB for the diagnosis of lung disease has come along way from the time these specimens were firstobtained via a rigid bronchoscope.7,29 Then, samplingwas a problem and the specimens were often toosmall to enable a definitive diagnosis.14,15 With the useof the FOB, advanced radiological guidance andincreasing user expertise the diagnostic yield hasincreased considerably. However, two crucialquestions remain. First is the problem of “samplingerror”, namely, divergent histopathologic diagnosesin two or more biopsy sites.30 This is likely, to beminimised by using HRCT to select multiple biopsysites representative of the full range of morphologicappearances.31 A second crucial consideration is“inter-observer variation” between histopathologists.In a recent study32 very significant observer variationwas quantified, and the observer agreement wasfound to be barely clinically acceptable. This is likelyto be a result of intermediate histopathologicappearances between two entities in a significantproportion of cases. It is especially because of thisscenario that the systematic categorisation ofhistopathological features seen on TBLB using thepattern-based approach is advocated. These whencorrelated with clinical and imaging data can be thekey determinants of a final consensus diagnosis ofDPLDs, especially in patients from developing
Pattern-based Approach in Interpretation of TBLB Ritu Kulshrestha et al

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 17
countries such as India, with high burden of chronicrespiratory diseases, who are unable to undergosurgical lung biopsy.
REFERENCES
1. Leslie KO, Gruden JF, Parish JM, Scholand MB.Transbronchial biopsy interpretation in the patient withdiffuse parenchymal lung disease. Arch Pathol Lab Med2007;131:407-23.
2. Liebow A, Carrington C. The eosinophilic pneumonias.Medicine (Baltimore) 1969;48:251-85.
3. Tazelaar HD, Linz LJ, Colby TV, Myers JL, Limper AH.Acute eosinophilic pneumonia: histopathologic findings innine patients. Am J Respir Crit Care Med 1997;155:296-302.
4. Wagenvoort CA, Wagenvoort N. Pathology of PulmonaryHypertension. New York: John Wiley and Sons; 1977.
5. Walters EH, du Bois R, editors. Immunology andManagement of Interstitial Lung Diseases. London: Chapmanand Hall; 1995.
6. McLoud TC, Carrington CB, Gaensler EA. Diffuseinfiltrative lung disease: a new scheme for description.Radiology 1983;149:353-63.
7. Andersen HA. Transbronchoscopic lung biopsy fordiffuse pulmonary diseases: results in 939 patients. Chest1978;73:734-6.
8. Poletti V, Patelli M, Ferracini R, Simonetti M, Spiga L.Transbronchial lung biopsy in infiltrative lung disease: theimportance of the pathologic approach. Sarcoidosis 1988;5:43-50.
9. Mitchell DM, Emerson CJ, Collins JV, Stableforth DE.Transbronchial lung biopsy with the fibreopticbronchoscope: analysis of results in 433 patients. Br J DisChest 1981;75:258-62.
10. Haponik EF, Summer WR, Terry PB, Wang KP. Clinicaldecision making with transbronchial lung biopsies. Am RevRespir Dis 1982;125:524-9.
11. Descombes E, Gardiol D, Leuenberger P. Transbronchiallung biopsy: an analysis of 530 cases with reference to thenumber of samples. Monaldi Arch Chest Dis 1997;52:324-9.
12. Curley FJ, Johal JS, Burke ME, Fraire AE. Transbronchiallung biopsy: can specimen quality be predicted at thetime of biopsy? Chest 1998;113:1037-41.
13. Gilman MJ, Wang KP. Transbronchial lung biopsy insarcoidosis. Am Rev Respir Dis 1980;122:721-4.
14. Fechner RE, Greenberg SD, Wilson RK, Stevens PM.Evaluation of transbronchial biopsy of the lung. Am J ClinPathol 1977;68:17-20.
15. Wall CP, Gaensler EA, Carrington CB, Hayes JA.Comparison of transbronchial and open biopsies in chronicinfiltrative lung disease. Am Rev Respir Dis 1981;123:280-5.
16. Ellis JH. Transbronchial lung biopsy via the fibreopticbronchoscope: experience with 107 consecutive cases andcomparison with bronchial brushing. Chest 1975;68:524-32.
17. Zavala DC. Transbronchial biopsy in diffuse lung disease.Chest 1978;73:727-33.
18. American Thoracic Society. American Thoracic Society/European Respiratory Society. InternationalMultidisciplinary Consensus Classification of theIdiopathic Interstitial Pneumonias. Am J Respir Crit CareMed 2002;165:277-304.
19. Kitaichi M, Tamaya M, Nakama T, Inoue Y. Pathology ofnonspecific interstitial pneumonia including anintroduction of quantitative diagnostic method. PatholClin Med 2005;24:828-34.
20. Berbescu EA, Katzenstein A, Snow JL, Zisman DA.Transbronchial biopsy in usual interstitial pneumonia.Chest 2006;129:1126-31.
21. Ensminger SA, Prakash UBS. Is bronchoscopic lungbiopsy helpful in the management of patients with diffuselung disease? Eur Respir J 2006;28:1081-4.
22. Andersen HA, Fontana RS. Transbronchoscopic lungbiopsy for diffuse pulmonary diseases: technique andresults in 450 cases. Chest 1972;62:125-8.
23. British Thoracic Society. Diagnosis and assessment ofdiffuse parenchymal lung disease. Thorax 1999;54(S1):S2-S14.
24. Mukherjee S, Spiteri M. Transbronchial biopsy and usualinterstitial pneumonia: a step backward in diseasemanagement? Chest 2006;130:1628.
25. Flaherty KR, Travis WD, Colby TV, Toews GB, KazerooniEA, Gross BH, et al. Histopathologic variability in usualand nonspecific interstitial pneumonias. Am J Respir CritCare Med 2001; 164:1722-7.
26. Sen T, Udwadia ZF. Retrospective study of interstitiallung disease in a tertiary care centre in India. Indian J ChestDis Allied Sci 2010;52:207-11.
27. Ahluwalia G, Sharma SK, Dattagupta S, Pande JN. Roleof transbronchial lung biopsy in diffuse pulmonarydisease: a review of 25 cases during one year. Indian JChest Dis Allied Sci 1999;41:213-7.
28. Gupta D, Jorapur V, Bambery P, Joshi K, Jindal SK.Pulmonary sarcoidosis: spirometric correlation withtransbronchial biopsy. Sarcoidosis Vasc Diffuse Lung Dis1997;14:77-80.
29. Andersen HA, Fontana RS, Harrison EG Jr. Transbronchiallung biopsy in diffuse pulmonary disease. Dis Chest1965;48:187-92.
30. Monaghan H, Wells AU, Colby TV, du Bois RM, HansellDM, Nicholson AG. Prognostic implications of histologicpatterns in multiple surgical lung biopsies from patientswith idiopathic interstitial pneumonia. Chest2004;125:522-6.
31. Wells AU. Histopathologic diagnosis in diffuse lungdisease: an ailing gold standard. Am J Respir Crit Care Med2004;170:828-9.
32. Nicholson AG, Addis BJ, Bharucha H, Clelland CA,Corrin B, Gibbs AR, et al. Inter-observer variation betweenpathologists in diffuse parenchymal lung disease. Thorax2004;59:500-5.
18 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
SLEEPCON-2012
NATIONAL CONFERENCE ON SLEEP DISORDERS(Under the auspicious of Indian Sleep Disorders Association)
April 6 - 8, 2012
April 6, 2012 : Workshop-I — Polysomnography
: Workshop-II — NIPPV
April 7-8, 2012 : Conference
Abstract Submission Deadline: February 28, 2012(abstract to be sent by e-mail to: [email protected])
Organising Secretary Chairman, Organising Committee
Prof. A.K. Janmeja Prof. D. BeheraProfessor and Head DirectorDepartment of Pulmonary Medicine L.R.S. Institute of TB andGovernment Medical College and Hospital Respiratory DiseasesSector-32, Chandigarh-160 030 Sri Aurobindo Marg, New Delhi-110 030E-mail : [email protected] E-mail: [email protected] : 91-0172-2623621 Phone: 91-011-26963335Moblie : 09646121621Website : www.amch.aov.in/conference

€€
€
€€
€
€
€


Original Article
[Received: March 8, 2011; accepted after revision: August 19, 2011]
Correspondence and reprint requests: Dr C. Nagaraja, Professor and Head, Department of Pulmonary Medicine, RajivGandhi Institute of Chest Diseases, BMCRI, Hosur Road, Bengaluru-560 029 (Karnataka), India; Phone: 919448057093; E-mail:[email protected], [email protected]
Pattern of Drug-resistance and Treatment Outcome inMultidrug-resistant Pulmonary Tuberculosis
C. Nagaraja, B.L. Shashibhushan, Mohamed Asif, Manjunath PH and Sagar C
Department of Pulmonary Medicine, Rajiv Gandhi Institute of Chest Diseases, BMCRI, Bengaluru (Karnataka),India
ABSTRACT
Aims and Objectives. To study the pattern of drug-resistance and treatment outcomes among patients with confirmedmultidrug-resistant pulmonary tuberculosis (MDR-PTB).
Methods. A prospective study was conducted at Rajiv Gandhi Institute of Chest Diseases, Bengaluru, Karnataka, India.Between January 2005 and December 2008, 224 confirmed MDR-PTB cases were studied for various drug-resistance patterns,and their treatment outcomes were analysed until November 2010. Sputum culture and drug sensitivity tests (DST) werecarried out at National Tuberculosis Institute, Bengaluru; DST was done for all first-line drugs except pyrazinamide.
Results. Of the 224 MDR-PTB patients, 146 (65.2%) were resistant to all first-line drugs, 39 (17.4%) to isoniazid, rifampicinand streptomycin; 19 (8.5%) to isoniazid, rifampicin and ethambutol; and 20 (8.9%) to isoniazid and rifampicin. Among them,145 (64.7%) patients were cured, 5 (2.2%) had treatment-failure, 10 (4.4%) died, and 64 (28.5%) defaulted. Among 145 curedcases, 100 (69%) were resistant to all first-line drugs, 23 (16%) to isoniazid, rifampicin and streptomycin, 11(8%) to isoniazid,rifampicin and ethambutol, and 11(8%) to isoniazid and rifampicin.
Conclusions. The most common pattern observed in this study was resistance to all four first-line drugs followed byresistance to isoniazid, rifampicin and streptomycin. Patients resistant to all first-line drugs had early sputum cultureconversion and better cure rate as compared to other resistance patterns. [Indian J Chest Dis Allied Sci 2012;54:23-26]
Key words: MDR-TB, Drug resistance, Treatment outcome.
INTRODUCTION
Tuberculosis (TB) is a major cause of morbidity andmortality in India. India accounts for 1/5th of globalTB incidence. According to the World HealthOrganization (WHO), each year an estimated 9.4million new cases of TB are detected leading to nearly2 million deaths. In India, the numbers of TB patientsare 1.96 million per year, and among them 0.8 millionare new smear-positive cases comprising of 75 newsputum smear-positive cases per lakh annually with0.33 million deaths per year. There is a rising trend ofdrug-resistant TB in different parts of the world, Indiabeing next only to China, both contributing more than50% of global multidrug-resistant (MDR-TB) cases.Frequency of MDR-TB is less than 3% in new casesand 12% to 17% among re-treatment cases as per therecent studies.1, 2 An MDR-TB patient is the onewhose sputum culture is positive for Mycobacteriumtuberculosis that is resistant in vitro to isoniazid (INH)and rifampicin with or without resistance to other
anti-tuberculosis drugs based on drug sensitivitytesting.3 Since second-line anti-tuberculosis treatment(ATT) is more toxic and less efficacious than first-linedrugs, treatment of MDR-TB is more challenging andrequires judicious use of various regimens as perresistance patterns in specialised and designatedcenters. Hence, this study was done to assess thepattern of drug-resistance among confirmedmultidrug-resistant pulmonary tuberculosis (MDR-PTB) patients and their treatment outcomes.
MATERIAL AND METHODS
This study was carried out at the Department ofPulmonary Medicine, Rajiv Gandhi Institute of ChestDiseases, Bengaluru. Between January 2005 andDecember 2008, 224 confirmed MDR-PTB cases wererecruited and their treatment outcomes wereanalysed until November 2010.
All sputum smear-positive category II failures agedmore than 15 years with confirmed reports of MDR-

24
PTB from the National Tuberculosis Institute (NTI),Bengaluru, were included in the study. Culture andsensitivity reports from other non-accreditedlaboratories were not considered. Sputum culture foracid-fast bacilli (AFB) and DST were carried out atNTI, Bengaluru, a Revised National TuberculosisControl Programme (RNTCP)-accredited laboratory.DST was done for all first-line drugs exceptpyrazinamide (PZA). DST for second-line drugs werecarried out in a few MDR failure cases atTuberculosis Research Centre (TRC), Chennai, theonly south Indian centre with DST facility for second-line drugs. Category I and III failures were notincluded in this study as they were not considered asMDR-suspects when the study started.
Sputum specimens were collected in sterile widemouthed bottles from sputum smear-positive patientsof pulmonary TB. The collected specimens wereprocessed by modified Petroff’s method. For eachspecimen, two Lowenstein-Jensen (LJ) slopes wereinoculated each with one 5 mm loopful of thecentrifuged sediment, distributed over the surface. Allcultures were incubated at 35-37 °C for up to 8 weeks.The tests were done in a biosafety class II cabinet.
Various regimens followed depending on the DSTfor the treatment of MDR-PTB in this study are givenbelow.
The initial regimen contained at least three newerdrugs that were not used previously and included atleast one injectable aminoglycoside and PZA, as thiscombination has good bactericidal activity. Thenumber of newer drugs varied in the intensive phasedepending on the resistance pattern. One or moredrugs, preferably weaker drugs (injectable andcycloserine), were not used in the continuation phaseafter sputum conversion. The total duration of thetreatment was 18 to 24 months.
The patients were followed up every monthduring the entire period of treatment with clinicalassessment and sputum smear examination for AFB.Sputum culture was done thrice during the entirecourse of treatment — one at sputum smearconversion, second at the end of intensive phase, andthird at one month before completion of treatment.Five patients that failed treatment for MDR-PTB weresubjected for sputum AFB culture and sensitivity tofirst- and second-line drugs at TRC, Chennai. Chestradiographs were done once in three months in all
Drug-resistance Pattern and Outcome in MDR-TB C. Nagaraja et al
Resistance Pattern Intensive Phase Regimen
HR Streptomycin + Ofloxacin/Levofloxacin + Ethionamide + Ethambutol +Pyrazinamide
HRS Kanamycin + Ofloxacin/Levofloxacin + Ethionamide + Ethambutol +Pyrazinamide
HRE Streptomycin + Ofloxacin/Levofloxacin + Ethionamide + Cycloserine/Para-aminosalicylic acid + Pyrazinamide
HRSE Kanamycin + Ofloxacin/Levofloxacin + Ethionamide + Cycloserine +Pyrazinamide + Para-aminosalicylic acid
H=Isoniazid, R=Rifampicin, S=Streptomycin, E=Ethambutol
Conventional proportion method - LJ media with therecommended drug concentrations of 4mg/L forstreptomycin, 0.2mg/L for INH, 40mg/L forrifampicin, 2mg/L for ethambutol and plain LJmedium for control were prepared. The growth of anisolate from culture was scraped with a loop andbacterial suspension was made in sterile distilledwater, vortexed and matched with McFarland opacitytube No. 1. Dilutions of 10-2 and 10-4 were made andinoculated on both control and drug containingmedia and incubated at 37 °C. The first reading wastaken after 28 days of incubation and if the isolatewas susceptible a second reading was taken on 42nd
day. Colonies were counted only on the slopes seededwith the inoculums that have produced exactreadable counts or actual counts (up to 100 colonieson the slope). Ratio of the number of colonies in drugcontaining slopes by that in drug free slopes wasconsidered as the percentage resistance (R). If R >1%,the isolate was considered resistant. H37Rv strainwas used as standard control.
the patients. Blood urea and serum creatinineestimation were carried out monthly during theintensive phase in all the patients. Liver functiontests were done at baseline in all the patients. Otherrelevant investigations were carried out based onclinical assessment.
RESULTS
In total, 224 patients with confirmed MDR-PTB werestudied. None of the patients were tested for PZAsensitivity. Of the 224 patients (158 males), 18patients had diabetes mellitus, 5 had humanimmunodeficiency virus (HIV) co-infection, 3 hadhypertension, 1 had ischaemic heart disease anddiabetes mellitus, 2 had chronic obstructivepulmonary disease, and 1 had Hansen’s disease. Onehundered and forty-eight patients had cavitarylesions, while the remaining 76 had only infiltrates.Bilateral lesions were seen in 175 patients, right-sided

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 25
lesions in 27 patients and left-sided lesions in theremaining 22 patients.
Table 1 shows the pattern of drug-resistance in thestudy sample. Majority of them (65%) showedresistance to all the first-line drugs tested. The meanduration of sputum culture conversion according tothe resistance pattern is presented in table 2.Treatment outcomes of various MDR-PTB patternsare shown in table 3.
Table 1. Various resistance patterns seen in the studysample
Resistance Pattern Number of Patients
HRSE 146 (65.2)
HRS 39 (17.4)
HR 20 (8.9)
HRE 19 (8.5)
H=Isoniazid, R=Rifampicin, S=Streptomycin, E=EthambutolFigures in parenthesis indicate percentage.
Table 2. Time to culture conversion in the study sample
Resistance Pattern Mean Duration of SputumCulture Conversion (Days)
HRSE 40.3
HRS 48.2
HRE 51.3
HR 55.0
Table 3. Treatment outcomes in 224 patients with MDR-PTB
HRSE HRE HRS HR Total
Cured 100 (69) 11 (58) 23 (59) 11 (55) 145
Defaulter 37 5 15 7 64
Failure 4 1 0 0 5
Death 5 2 1 2 10
Total 146 19 39 20 224
Figures in parenthesis indicate percentage.
Most common adverse drug reactions observedin this study were gastrointestinal disturbancesmainly due to para-aminosalicylic acid (PAS),which subsided with routine management andassurance. Nine patients developed ototoxicitysuch as tinnitus, hard of hearing, positionalimbalance due to streptomycin/kanamicin toxicity(confirmed by audiometry), necessitating us to stopthe drug. Five patients complained of acneattributed to ethionamide; but, the drug was notstopped, and eventually the acne subsided in mostof them. Nine patients developed cycloserine-induced psychosis requiring anti-psychoticmedications. Cycloserine was stopped in twopatients. Three patients developed swelling of thethyroid gland. Investigations confirmedhypothyroidism in them, and they improved
following replacement therapy. Twelve patientsdeveloped arthritis along with elevated serum uricacid levels which warranted us to stop the drugtemporarily; they were treated with non-steroidalanti-inflammatory drugs. Uric acid level estimationwas done monthly and PZA was re-started oncethe uric acid levels normalised.
DISCUSSION
An appropriate assessment of various patterns ofdrug-resistance among patients with confirmed MDR-PTB is required to initiate a proper regimen as perDST to improve the treatment outcome. A merediagnosis of MDR-PTB and initiation of second-lineATT without proper regimens based on DST may nothelp achieve a good treatment outcome. As there is anincreasing trend of MDR-PTB in India, properformulation of treatment regimens consisting of newerdrugs based on various drug resistance patterns inconfirmed MDR-PTB cases is very much required asevident from the present study.
In the present study, 65.2% were resistant to allfirst-line drugs, 91.2% were resistant to at least oneother first-line drug apart from INH and rifampicin.Rao et al4 showed that of the 577 proven MDR-TBpatients, 56.5% had isolates resistant to all first-linedrugs, 88% cases had MDR plus resistance to at leastanother first-line drug. In the present study, MDRplus streptomycin resistance was 17.4% and MDRplus ethambutol resistance was 8.5%, whileKudzawu et al5 reported it to be 25% for MDR plusstreptomycin resistance and 21.4% for MDR plusethambutol resistance.
Isolates resistant only to INH and rifampicin were8.9% in the present study as compared to 10.7% in astudy by Chowgule and Dheodhar,6 25.2% in a studyby Dheodhar et al,7 21.4% in a study by Janmeja et al,8
and 35.7% in the study by Kudzawu et al.5
The mean sputum culture conversion wasanalysed in MDR-PTB patients with various drug-resistance patterns. The patients with resistance to allfirst-line drugs showed a mean sputum conversion of40 days and the conversions observed in otherresistance patterns were 48 days for MDR plusstreptomycin, 51 days for MDR plus ethambutol and55 days for isolated MDR. In the present study, themean time to culture conversion observed in all 224patients was 48.6 days. Joseph et al9 found that of the38 cases, 82% had culture conversion in two monthsor less. Shin et al10 in a study of 230 patients found aculture conversion of 95% after a median period oftwo months.
The treatment outcomes were also analysed in thepresent study. In a total of 224 cases, 145 (64.7%) werecured, 5 (2.2%) had treatment failures, 10 (4.4%)patients died, and 64 (28.5%) patients defaulted.

Drug-resistance Pattern and Outcome in MDR-TB C. Nagaraja et al
Masjedi et al11 in a study of 43 cases, documented that29 (67.5%) had a successful outcome (cured), 6 (14%)had treatment failures, and 8 (18.6%) patients diedwith no defaulters. In the study by Shin et al,10 77%were cured, 5% died, 7% failed, and 12% defaulted.Patients with resistance to all first-line drugs showedan early sputum culture conversion and a better curerate compared to other resistance patterns. Theseobservations were probably due to judicious use ofmore newer drugs in the initial regimen which werenot used previously in those patients and is attributedto the bacilli being fully sensitive to these new drugs.
In the present study, 28.5% of patients defaulteddespite good pre-treatment counselling andproviding the drugs for free under supervision,probably due to a sense of well-being after a fewmonths of treatment or due to social stigma. Inabilityto collect drugs from the centre due to costs involvedin travel and loss of earnings for that particular daywas observed more commonly in males as they werethe only earning members of the family and also dueto broken families. Proper counselling, education, andmotivation are needed to improve the adherence totreatment and cure rates. The cure rate (64.7%) in ourstudy was good mainly because of formulation ofappropriate treatment regimens based on the variousdrug-resistance patterns.
In conclusion, close monitoring of drug-resistancepatterns in confirmed MDR-PTB isolates is requiredto formulate different regimens as per the drug-resistance pattern. The commonest pattern observedin this study was resistance to all four first-line drugsfollowed by resistance to isoniazid plus rifampicinplus streptomycin. Patients resistant to all first-linedrugs showed a better cure rate compared to otherresistance patterns. Hence, early diagnosis of MDR-PTB and treatment under supervision by formulating
appropriate regimens based on resistance pattern arethe keys to success in treating MDR-PTB.
REFERENCES
1. Ramachandran R. Nalini S, Chandrashekar V, Duve PV,Sangghvi, Wares F, et al. Surviellance of drug resistancetuberculosis in the state of Gujarat, India. Int Tuberc LungDis 2009;13:1154-60.
2. Mahadev B, Kumar P, Agarwal SP, Chaughan LS,Srikantaramu N. Surveillance of drug resistance to anti-tuberculosis drugs in districts of Hoogli in West Bengaland Mayurbhanj in Orissa. Indian J Tuber 2005;52:5-10.
3. DOTS Plus guidelines. Available from: http://www.tbcindia.org [Last accessed on 2011 Jan 15].
4 . Rao NA, Irfan M, Soomro MM, Mehfooz Z. Drugresistant pattern in multi drug resistant pulmonarytuberculosis patients. J Coll Physicians Surg Pak2010;20:262-5.
5. Chowgule RV, Dheodhar L. Pattern of secondary acquireddrug resistant to anti tuberculosis drugs in Mumbai, India1991-95. Indian J Chest Dis Allied Sci 1998;40:23-31.
6. Deodhar L, Miskeen P, Chomal S. Drug resistance intuberculosis. BHJ 1999;41:253.
7. Janmeja AK, Raj B. Acquired drug resistance intuberculosis in Haryana, India. J Assoc Physicians India1998;46:194-8.
8. Kudzawu FS, Kwara A, Flanigan T. High frequency offirst line anti tuberculosis drug resistance among personswith chronic pulmonary tuberculosis at a teachinghospital chest clinic. Ghana Med J 2010;44:42-6.
9. Joseph P, Desai VBR, Mohan NS, Fredrick JS,Ramachandran R, Raman B, et al. Outcome ofstandardized treatment for patients with MDR-TB fromTamil Nadu, India. Indian J Med Res 2011;133:529-34.
10. Shin SS, Pasechnikov AD, Gelmanova IY, Peremitin GG,Strelis AK, Mishustin S, et al. Treatment outcomes in anintegrated civilian and prison MDR-TB treatment programin Russia. Int J Tuberc Lung Dis 2006;10:402-8.
11. Masjedi MR, Tabarsi P, Chitsaz E, Baghaei P, Mirsaeidi M,Amiri MV, et al. Outcome of treatment of MDR-TBpatients with standardised regimens, Iran, 2002-2006. IntJ Tuberc Lung Dis 2008;12:750-5.
26

Exhaled Breath Condensate Analysis in Chronic ObstructivePulmonary Disease
Sunil K. Chhabra and Mansi Gupta
Department of Cardio-respiratory Physiology, Viswanathan Chest Hospital, Vallabhbhai Patel Chest Institute,University of Delhi, Delhi, India
ABSTRACT
The increasing focus on airway inflammation in the pathogenesis of chronic obstructive pulmonary disease (COPD) hasled to development and evolution of tools to measure it. Direct assessment of airway inflammation requires invasiveprocedures, and hence, has obvious limitations. Non-invasive methods to sample airway secretions and fluids offer excitingprospects. Analysis of exhaled breath condensate (EBC) is rapidly emerging as a novel non-invasive approach for samplingairway epithelial lining fluid and offers a convenient tool to provide biomarkers of inflammation. It has definite advantagesthat make it an attractive and a feasible option. It is a source of mediators and molecules that are the causes or consequencesof the inflammatory process. Measurement of such markers is increasingly being explored for studying airwayinflammation qualitatively and quantitatively in research studies and for potential clinical applications. These biomarkersalso have the potential to develop into powerful research tools in COPD for identifying various pathways of pathogenesisof COPD that may ultimately provide specific targets for therapeutic intervention. The EBC analysis is still an evolving non-invasive method for monitoring of inflammation and oxidative stress in the airways. The limited number of studies availableon EBC analysis in COPD have provided useful information although definite clinical uses are yet to be defined. Evolvingtechnologies of genomics, proteomics, and metabonomics may provide deeper and newer insights into the molecularmechanisms underlying the pathogenesis of COPD. [Indian J Chest Dis Allied Sci 2012;54:27-37]
Key words: Chronic obstructive pulmonary disease, Exhaled breath condensate, Oxidative stress, 8-isoprostane, Hydrogenperoxide.
INTRODUCTION
A major advancement in the knowledge ofpathogenesis of chronic obstructive pulmonarydisease (COPD) has been the recognition that airwayinflammation plays a key and a central role. It is nowa part of the current definition of COPD and isbelieved to be the major underlying process for thealtered pathophysiology and clinical manifestations.1
Airflow limitation has long been thepathophysiological characteristic of COPD, andtherefore, lung function testing has been consideredas the main investigation for diagnosis, assessment ofseverity, monitoring of response and for following thenatural course of the disease. Indeed, spirometry isconsidered essential to establish permanent airflowlimitation and the diagnosis of COPD. However,limitations of lung function tests in the assessment ofseverity and monitoring of response have been wellrecognised. The increasing focus on airwayinflammation has led to efforts to gain insights intoits nature, development and evolution in researchstudies with an aim to ultimately translate this
knowledge into tools for diagnosis, assessment andmonitoring of COPD.
Conventionally, drugs in COPD have beenevaluated by changes in forced expiratory volume inone second (FEV1) and more recently, using inaddition, patient-centered clinical outcome measures.While these tools may be appropriate to evaluatetherapeutic interventions such as bronchodilators,these may not serve the purpose for newer drugs thatare increasingly targeted at specific pathways of theinflammatory process. Tools to measure airwayinflammation are required for the evaluation of suchdrugs.
Oxidative stress is believed to play a major role inthe pathogenesis of COPD and is characterised by anincreased oxidant load and a relative or absolutedeficiency of antioxidants.2 Oxidative processes andfree radical generation lead to increased bronchialhyperresponsiveness and inflammation, apoptosisand destruction of airway epithelial cells, and impairthe functions of antiproteases and surfactant.3 Themajor mediators of oxidative stress and pro-inflammatory molecules include reactive oxygen
[Received: January 5, 2012; accepted: January 10, 2012]
Correspondence and reprint requests: Dr S.K. Chhabra, Professor and Head, Department of Cardio-respiratory Physiology,Vallabhbhai Patel Chest Institute, University of Delhi, Delhi - 110 007, India; E-mail: [email protected]
Review Article

28
species (ROS) such as the superoxides and hydroxylradicals, reactive nitrogen species (RNS), certaincytokines and eicosanoids, interleukins, tumournecrosis factor-alpha, and activated transcriptionalfactors such as nuclear factor kappa-B and activatorprotein 1.4 These compounds are potentialcandidates to serve as biomarkers of oxidative stressand airway inflammation. An ideal biomarker forCOPD should be stable, be present in sufficientquantities to allow analysis, should have acceptableprecision in measurement, should be responsive tochange in clinical status, either worsening orimprovement, with therapeutic interventions, andshould be specific for the disease.
ASSESSMENT OF AIRWAYINFLAMMATION
Direct assessment of airway inflammation requiresinvasive procedures, such as biopsy andbronchoalveolar lavage that are limited by thisdisadvantage. These tools provide samples andspecimens from limited areas of the lung. Further,these are not feasible options for advanced diseaseand for serial monitoring. While bronchoalveolarlavage fluid (BALF) has been used in several studiesto sample the lower respiratory tract for more thantwo decades, its invasive nature and a definite,though small, risk of adverse events has prevented itfrom evolving into an acceptable clinical tool for theassessment of the airway inflammation.
Peripheral blood markers have been used to studyairway inflammation but may not be appropriatemirrors of the airway pathology. The increase in theinflammatory cell population and markers in theairway may occur earlier than in the peripheralblood, and reflect the degree of airflow limitationbetter than do peripheral blood measurements.5 Non-invasive methods to sample airway secretions andfluids offer exciting prospects. These can providemediators and molecules that are the causes orconsequences of the inflammatory process.Measurement of such markers is increasingly beingexplored for studying airway inflammationqualitatively and quantitatively in research studiesand for potential clinical applications. Thesebiomarkers also have the potential to develop intopowerful research tools for identifying the novelpathways of pathogenesis of COPD that mayultimately provide specific targets for therapeuticinterventions.
Sputum induction is a semi-invasive techniquethat not only provides specimens for cytologicalstudies of the airway lining fluid but provides asource of inflammatory mediators that can bemeasured in the supernatants. However, itsapplication has largely been limited to cytological
analysis though it has also been studied as a sourceof biomarkers reflecting oxidative stress and airwayinflammation.
EXHALED BREATH CONDENSATEANALYSIS
Analysis of exhaled breath is rapidly emerging as anovel and non-invasive approach for samplingairway epithelial lining fluid and offers anotherconvenient tool to provide biomarkers. It has definiteadvantages that make it an attractive and a feasibleoption. Besides being completely non-invasive, it issuitable for serial assessments in longitudinalstudies, and thus, can be used for monitoring ofdisease as well as serve as an outcome parameter inclinical drug trials. Other potential uses includemeasurement of severity of disease, and applicationas a diagnostic aid. It can be used in stable as well aspatients with acute exacerbations and even inpatients on a mechanical ventilator. It can be used inthe out-patient and occupational settings, and also infield studies for epidemiological purposes. Exhaledbreath analysis has been extensively examined as amirror of the inflammatory processes in the airwaysin asthma and such studies are now beingincreasingly carried out in patients with COPD.
Exhaled breath analysis broadly focuses on twoareas: measurement of exhaled nitric oxide (ENO)and the detection of biomarkers in exhaled breathcondensate (EBC). The use of ENO has found limitedsuccess as a potential evaluative tool in COPDcompared to its wider acceptability in themanagement of asthma. This scope of this review islimited to EBC analysis.
The EBC is mainly formed by water vapour but alsocontains several biomolecules, mainly related toneutrophil-derived products and oxidative stress(leukotrienes, prostaglandins, isoprostanes, hydrogenperoxide), endogenous airway acidification(hydrogen ions), and nitric oxide-derived products(nitrosothiols, and nitrite/nitrate). Its collectionsimply involves tidal breathing into a chilledcollection device. Water vapour in exhaled breath iscondensed and collected and various mediators canthen be quantified in the condensate. The EBCprovides a convenient sample of volatile substancesand aerosols and reflects a summation of all areas ofthe lung that are ventilated.
Exhaled Breath Condensate Analysis in COPD
Several studies have been carried out on EBC obtainedfrom patients with COPD. While several potentialclinical applications have been explored includingthe ability of biomarkers to differentiate betweenhealth and disease in smokers, diagnostic specificity
Exhaled Breath Condensate in COPD S.K. Chhabra and Mansi Gupta

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 29
for COPD, assessment of severity, phenotyping, andfor evaluation of therapeutic intervention, most of thestudies have been limited by small sample sizes andlack of standardised methods of collection of EBC andits analysis. The EBC analysis has the potential tooffer clues to diagnosis of infectious agents and mayallow risk stratification. Although most of the studieshave been in stable patients, acute exacerbations ofCOPD (AECOPD) are characteristically associatedwith increased airway inflammation and oxidativestress.6,7 Therefore, EBC analysis may also be used forpredicting the outcomes and monitoring the course ofan exacerbation. However, such studies have beenfew. Clear clinical indications and utility of EBCanalysis in COPD in research studies have not beendefined.
EBC studies on some of the more commonlystudied biomarkers in patients with COPD arereviewed below.
8-isoprostane
One of the major products of oxidative stress in thelungs is 8-isoprostane. It is a prostaglandin-F(2α)isomer that is formed in vivo by free radical-catalysedperoxidation of arachidonic acid, independent of thecyclooxygenase pathway. This has been one of themost studied biomarker in patients with COPD.
The 8-isoprostane concentrations were observed tobe similar in ex-smokers and current smokers withCOPD, were increased about 1.8-fold compared tohealthy smokers who, in turn, had 2.2-fold higherlevels than healthy non-smokers.8 The 8-isoprostanewas similarly reported to be significantly increased inpatients with COPD compared to smokers.9 Theseresults were corroborated in other studies.10,11
While levels of 8-isoprostane in EBC haveconsistently been found to be increased in patientswith COPD, these have usually been lower than thoseobserved in induced sputum or BALF. This was truefor all groups of subjects: non-smokers, healthysmokers, symptomatic smokers at risk for COPD andpatients with AECOPD .12 Similarly, in BALF too,8-isoprostane was found present in significantlyhigher concentrations than in EBC. Both correlatedwell with levels of leukotriene B4 (LTB4) in patientswith COPD.13
The relationship between EBC levels of 8-isoprostane and lung function parameters, and withother measures of severity of COPD has beeninvestigated but found to be inconsistent andvariable in different studies. In one study, levels of 8-isoprostane did not differ significantly across GOLDstages of COPD. Further, no correlations wereobserved between levels of 8-isoprostane and FEV1,neutrophil count, and dyspnoea scores.9 In anotherstudy, the increase in 8-isoprostane levels in EBC wasfound irrespective of the lung function impairment.
However, there was a significant correlation withemphysema scores on high resolution computedtomography (HRCT) and with Medical ResearchCouncil dyspnoea scale scores.14 Levels of8-isoprostane in EBC were found to be significantlylower in patients with emphysema than in patientswith predominantly chronic bronchitis and correlatedsignificantly with diffusion capacity but not withFEV1.
10 On the other hand, inverse correlations wereobserved between 8-isoprostane levels and lungfunction parameters in another study.12 Again, arecent study did not find any relationship between8-isoprostane levels and lung function parametersbut a significant positive correlation was found withthe dyspnoea grade.11 Severity-related differences in8-isoprostane were identified according to the bodymass index (BMI), obstruction, dyspnoea, and exercise(BODE) index in another recent study.15 The laststudy also examined the relationship betweenoxidative stress and pathophysiology in COPD. Instable patients, blood oxygen levels and dynamichyperinflation were reported related to airway8-isoprostane levels in EBC. Concentration of8-isoprostane were higher in patients who developeddynamic hyperinflation. End-expiratory lung volumechange and partial pressure of arterial oxygen (PaO2)independently predicted 8-isoprostane levels.
Phenotyping of COPD offers scope for anindividualised approach to treatment besidesidentifying patients groups with different prognosisand natural history. Till now, the approach tophenotyping has been based mainly on clinical,radiological and physiological characteristics. TheEBC analysis also has the potential to serve thispurpose. Some studies have evaluated this potentialbut with opposing results. Levels of 8-isoprostanein EBC were found to be significantly lower inpatients with emphysema than in patientswith predominantly chronic bronchitis in one study10
but found to have a significant correlation withHRCT emphysema scores in another study.14
The studies examining 8-isoprostane levels in EBCand their significance are summarised in table 1. Ingeneral, these studies have found patients withCOPD to have higher or similar levels as currentsmokers and both have higher levels than non-smokers. Thus, it clearly marks oxidative stress in theairways and appears to be a useful parameter. Thecorrelation with spirometry and severity of thedisease as assessed by lung function or symptoms ismodest or inconsistent. This is not surprisingconsidering that COPD is a disease with multipledimensions and lung function has usually beenfound to have modest or poor relationship with othermeasures of severity. Whether the oxidative stress hasa consistent and predictable relationship withclinical severity is yet to be established and requires

30
further investigation. No study has evaluatedchanges in response to any therapeutic intervention.Thus, 8-isoprostane remains a promising biomarkerin EBC in COPD but requires further evaluationbefore its utility as a clinical tool can be estabilished.
Hydrogen Peroxide (H2O2)
In COPD patients, ROS may be producedendogenously by activated inflammatory cellsincluding neutrophils, macrophages, andeosinophils, or exogenously, by exposures to airpollutants or cigarette smoke that act directly or bycausing neutrophil influx. Even a single cigarette hasbeen shown to cause a significant increase in EBCH2O2 in healthy non-smokers.16 Airway H2O2 isproduced by superoxide dismutase-mediatedconversion of superoxide anions. Being soluble, itappears in the exhaled breath. Therefore, H2O2 canserve as a direct marker of oxidative stress. The H2O2measurements in EBC have been carried out in severalstudies in COPD.
Levels of H2O2 were found increased in EBC ofstable patients with COPD compared to healthycontrols. Patients with AECOPD had even greaterlevels than stable patients suggesting that oxidantproduction was increased further duringexacerbations.17 While confirming increased H2O2 instable COPD, it was found that patients who werecurrent smokers did not exhale more H2O2 than thosewho were ex-smokers or those who had non-smokingCOPD.18,19 Both these studies show that cigarettesmoking made no difference to the EBC H2O2 levelsand the oxidative stress was a feature intrinsic toCOPD irrespective of the cause.
In another study,9 the increased levels of EBC H2O2showed a positive correlation with the levels ofsputum neutrophils, indicating a neutrophil-dependent mechanism for its production. The levelsof H2O2 in severe and moderate COPD weresignificantly higher than in mild disease. The H2O2had significant correlations with FEV1, and withdyspnoea scores in patients with moderate andsevere disease.9 Smokers and patients with COPD
Table 1. Summary of studies on 8-isoprostane in EBC in patients with COPD
Authorref and Study Population ResultsYear
Montuschi et al8 COPD ex-smokers (n=25) COPD ex-smokers and current smokers did not differ; Levels in2000 COPD current smokers (n=15) patient with COPD increased 1.8-fold over healthy smokers;
Control non-smokers (n=10) smokers had 2.2-fold higher levels than non-smokers; SmokingSmokers (n=12) caused an acute increase in exhaled 8-isoprostane by about 50%;
No correlation with severity of airways obstruction or dyspnoea
Biernacki et al24 COPD acute exacerbation (n=21) Levels were increased during exacerbation, decreased on2003 before and after treatment treatment at 2 weeks and further at 2 months
Kostikas et al9 COPD (n=30) Levels were significantly elevated in patients with COPD; No2003 Smokers, Stage 0 (n=10) significant difference across severity groups; No correlation with
lung function and dyspnoea grades
Izquierdo et al10 COPD (n=39) Levels were significantly lower in patients with emphysema than2006 Control smokers (n=15) in patients with chronic bronchitis or in the controls; correlated
significantly with DLCO/VA but not with FEV1
Ko et al30 COPD ex-smokers (n=32) COPD patients had higher levels compared to controls; Levels2006 Control non-smokers (n=17) increased across the groups with worsening FEV1
Makris et al14 COPD patients (n=18) Levels were significantly elevated in COPD; Levels correlated with2008 Control ex-smokers (n=5) emphysema score in HRCT and with dyspnoea scores
Non-smokers (n=7)
Mazur et al12 COPD acute exacerbation (n=10) In induced sputum, levels were at least 10-fold higher compared2009 Control non-smokers (n=14) to EBC levels; Healthy non-smokers had the lowest levels and
Healthy smokers (n=17) patients with AECOPD, the highest levels in EBC; InverseSymptomatic smokers (n=9) correlations with lung function parameters
Inonu et al11 COPD (n=25) COPD and smokers did not differ; Both had significantly higher2011 Control smokers (n=26) levels than non-smokers; No correlation with lung function
Non-smokers (n=29) parameters but significant positive correlation with dyspnoeagrade
García-Rio et al15 COPD (n=76) Significant severity-related differences in levels according to the2011 BODE index; Levels were higher in those who developed
dynamic hyperinflation; Hyperinflation and PaO2 predicted levelson multivariate regression
EBC=Exhaled breath condensate; COPD=Chronic obstructive pulmonary disease; FEV1=Forced expiratory volume in one second;HRCT=High resolution computed tomography; AECOPD=Acute exacerbations of COPD; BODE Index=BMI, obstruction, dyspnoea,and exercise index; PaO2=Partial pressure of arterial oxygen
Exhaled Breath Condensate in COPD S.K. Chhabra and Mansi Gupta

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 31
were observed to have similar levels of H2O2 in EBC.There was no correlation between H2O2 levels andlung function parameters.11
There are uncertainties about the origin of H2O2released in the lung. Fractionated samples of EBCfrom the airways and from the lung peripheryrevealed 2.6 times higher H2O2 in the former that wastwo-fold higher in smokers and five-fold higher inpatients with COPD compared to non-smokers,suggesting that airways may be the dominantlocation of H2O2 production.20
Some studies have looked at the effect oftherapeutic interventions on H2O2 levels in EBC. Atwo-week treatment in stable patients with COPDwith inhaled beclomethasone was not found tochange EBC H2O2 significantly although exhaled NOwas reduced.21 N-acetylcysteine, a precursor ofreduced glutathione that together with glutathioneperoxidase may remove H2O2, given for 12 months instable COPD patients had no effect in the first sixmonths but later reduced EBC H2O2 by about 2.5fold.22 Patients with lower respiratory tract infectionshowed no significant changes in H2O2 concent-rations in EBC on recovery and there were nosignificant correlations between with spirometry and
serum inflammatory parameters. In contrast, severalserum inflammatory markers did decrease duringhospitalisation.23 On the other hand, patients withmoderate to severe COPD during an exacerbationshowed significant decrease in H2O2 concentrations inEBC suggesting that the oxidative stress markers likeH2O2 are suitable in monitoring exacerbated COPD.7
The studies examining H2O2 levels in EBC andtheir significance are summarised in table 2. Fromthese studies, it may be concluded that H2O2 is areliable marker of oxidative stress in patients withCOPD and tends to reflect the severity of airwayinflammation and clinical manifestations. Therefore,it has the potential to serve as a tool for assessmentand monitoring of disease. Responsiveness totherapeutic intervention is not established.
Cytokines and Eicosanoids
Considering the central role of airway inflammationin the pathobiology of COPD, cytokines that play arole in recruiting inflammatory cells, especiallyneutrophils and in activation of inflammatory cellsand perpetuation of airway inflammation may beuseful biomarkers in monitoring its severity. In
Table 2. Summary of studies on hydrogen peroxide (H2O2) in EBC in patients with COPD
Authorref and Study Population ResultsYear
Dekhuijzen et al17 COPD (n=12) Levels were highest in acute exacerbation followed by stable1996 COPD acute exacerbation (n=19) COPD, followed by controls
Controls (n=10)
Nowak et al18 COPD ex-smokers/smokers/non- Levels were higher in COPD than controls; No difference between1998 smokers (n=32) smoker and non-smoker COPD patients
Control non-smokers (n=17)
Nowak et al19 COPD ex-smokers/smokers/non- Levels were higher in COPD than controls; No difference between1999 smokers (n=44) smoker and non-smoker COPD patients
Control non-smokers (n=17)
Ferreira et al21 COPD non-smokers (n=20), 2-week treatment with inhaled beclomethasone did not change2001 before and after 2-week treatment H2O2 significantly
with inhaled beclomethasone 500 μgtwice daily
Kasielski and Nowak22 COPD (n=22), before and after No effect of N-acetylcysteine in the first six months but later2001 N-acetylcysteine, 600 mg once a day reduced H2O2 by about 2.5 fold
for 12 months
van Beurden et al23 COPD (n=25) with lower respiratory No significant changes in H2O2 concentration after treatment of2003 tract infection infection
Kostikas et al9 COPD (n=30) Levels were significantly elevated in COPD patients; severe and2003 Smokers, Stage 0 (n=10) moderate COPD had significantly higher levels than those with
mild disease; significant correlation with lung function, inducedsputum neutrophil counts and dyspnoea scores in moderate andsevere COPD
Inonu et al11 COPD (n=25) COPD and smokers did not differ; Both had significantly higher2011 Healthy smokers (n=26) levels than non-smokers; no correlation with lung function
Non-smokers (n=29) parameters or dyspnoea

32
addition, eicosanoids (different prostaglandins andleukotrienes) that are released following cellularactivation may be other potential candidates. Theseare potent mediators of inflammation and areresponsible for vasodilatation/vasoconstriction,plasma exudation, mucus secretion, broncho-constriction/bronchodilatation, and inflammatorycell recruitment. Therefore, levels in EBC may beassumed to reflect the intensity of the inflammatoryprocesses in the airways.
LTB4, a potent and selective chemoattractant ofneutrophils, is released from macrophages andepithelial cells as well as from activated neutrophils.Exhaled LTB4 may be useful in monitoring ofinflammation and exacerbations in patients withCOPD and has been investigated in a few studies. Theincreased concentration of LTB4 in EBC of patientswith AECOPD and its subsequent decline towardsnormal levels may position it as a marker ofresolution or control of the inflammatory process andthus may have a role in monitoring of response.24 TheLTB4 levels in EBC were reported increased inpatients with COPD compared to controls. Patientswith airflow reversibility had values higher thanthose without airflow reversibility.25 In another study, 10
EBC LTB4 correlated significantly with diffusioncapacity but not with FEV1. Levels of interleukin (IL)-8 were observed to be lower in patients withemphysema than in patients with predominantlychronic bronchitis.
The EBC profiles of other exhaled prostaglandinsand leukotrienes have been studied to differentiatethe inflammatory response in asthma and COPD.Prostaglandin E2 and prostaglandin F2α were foundmarkedly increased in EBC from patients with COPDbut not in asthmatics.26 In contrast, leukotriene E4was increased in asthma but is not detectable innormal subjects or in patients with COPD.27
Whether EBC is the appropriate source for thesebiomarkers is not clear. In one study,28 IL-8 wasmostly undetectable in EBC in patients withAECOPD and stable COPD as well as in healthycontrols. In other studies, though levels in EBC weremuch less than those observed in induced sputum,IL-8 was increased in healthy smokers, symptomaticsmokers at risk for COPD and patients with acuteexacerbation. Inverse correlations with lung functionparameters were observed.12
Similarly, concentrations of cys-LTs and LTB4were found to be significantly higher in BALFcompared to EBC in patients with COPD.13 Nosignificant differences were found between smokersand ex-smokers serum or EBC levels of IL-8 and LTB4in EBC.10
Exacerbations in COPD are most frequently causedby infections which are also responsible for anincrease in inflammation in the airways. Therefore,infective exacerbations of COPD may be associated
with the increased production of other inflammatorymediators, for example, IL-8, IL-6, endothelin-1 andtumour necrosis factor-alpha (TNF-α) levels in EBCduring these exacerbations.29
Chemokines related to neutrophil and monocyteinflammation (growth-related oncogene alpha[GROalpha] and monocyte chemoattractant protein-1[MCP-1]) have been studied in EBC of COPD patientsbut found to have no utility in diagnosis orassessment of the severity.30
EBC Acidification
Studies in asthma have pointed to the role of airwayacidification in the airway pathophysiology. It maycause bronchoconstriction, impaired ciliary motility,increased mucus production and viscosity, andairway epithelial damage.31 The EBC pH is easy tomeasure and therefore is a potential biomarker inairway inflammatory diseases. Exhaled carbondioxide may be a potential confounder especially inpatients with acute or chronic hypercapnoeicrespiratory failure in AECOPD and stable COPD,respectively.
A comparison of asthmatics and mild COPDpatients with healthy controls did not revealsignificant differences.32 However, another study33
found lower pH in more severe COPD patients. Otherworkers reported that EBC pH was lower in COPDpatients compared to asymptomatic normal smokers.It was related to disease severity, and to parametersreflecting airflow limitation, hyperinflation and airtrapping.34 It was also observed that EBC pH waslower in ex-smokers than current smokers suggestinga probability of the presence of more severe disease inthe former.
In a more recent study,35 EBC pH was found to belower in patients with COPD and in smokingcontrols compared with non-smoking controls butwas not different between COPD and smokingcontrols. It was not related to severity of airwaysobstruction or to airway inflammation assessed bysputum leukocyte counts, and was not responsive tocorticosteroids. Its utility as a biomarker wasquestioned.35
Other Biomarkers
Besides the biomarkers discussed above, otherworkers have measured other compounds in EBCwith a view to understand the nature of theinflammatory process and identify clinically usefulsubstances.
Malondialdehyde (MDA) is a product of lipidperoxidation and has long been considered as amarker of oxidative stress. It is measured asthiobarbituric acid-reactive substances (TBARs),which are the end-products of lipid peroxidation.
Exhaled Breath Condensate in COPD S.K. Chhabra and Mansi Gupta

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 33
Paitents with stable COPD exhibited increased lipidperoxidation, measured as TBARs, that were notfound to correlate with cigarette smoking status.19
Two recent studies have differed in theirobservations. Levels of MDA were not found to bedifferent in patients with COPD and non-smokers inone study.11 However, in the other,36 MDA was foundto be significantly higher in patients with COPDcompared to asthmatics and healthy controls. Further,COPD patients showed an inverse correlationbetween MDA concentrations and FEV1%.36
Among other biomarkers under investigation inCOPD are purines that are present on airwaysurfaces in physiologically significant concentrationsand are proposed to play a role in airwayinflammation. These were found to be increased inEBC from patients with COPD, correlating withGOLD severity and FEV1% predicted.37
Products of Nitric Oxide
Nitric oxide (NO) is perhaps the most extensivelystudied marker of airway inflammation in exhaled air.Its utility is fairly well established in asthma.However, in COPD, its status is still evolving. Whilelarger airways are likely the primary source ofexhaled NO in asthma,38 that in COPD appears tooriginate in the peripheral airways.39 NO lead toformation of nitrite, nitrate, and S-nitrosothiol in theepithelial lining fluid. The compounds have beenmeasured in EBC in a few studies.
Increased levels of S-nitrosothiols have beendemonstrated in EBC of patients with COPD.40 Liu etal41 measured nitrite/nitrates (NOx) levels in EBC inCOPD patients and reported no significantdifferences in comparison with healthy non-smokingcontrols. Further, corticosteroid treatment was notfound to have any effect on the levels.
TECHNICAL ISSUES IN EXHALEDBREATH CONDENSATE ANALYSIS
The EBC is usually collected by asking the subject tobreathe tidally using a mouthpiece and a non-rebreathing valve to separate inspiratory andexpiratory air streams. The expired air is passedthrough a condenser, which is cooled to 0 ºC or –20ºC in a refrigerated circuit. The resultant condensateis collected into a cooled vessel. It usually takesbetween 10 and 15 minutes to obtain 1 to 3 mL ofcondensate. The EBC is then stored at –20 ºC or –80 ºCtill further analysis of the biomolecules.42
Methodological issues that may influence resultsare important and were recently reviewed.43 Theseinclude techniques and procedures of collection andstorage, analytical methods, inherent variation of EBCbiomarkers over time, and other factors affecting EBC
composition, such as smoking and demographics.These contribute to the differences and variationsamong different studies reviewed above. The lackof standardisation of the EBC analysis in theearlier studies makes comparison of studiesdifficult. Analytical methods are being improved toincrease their sensitivity. To address the need forstandardised methodologies of EBC analysis,American Thoracic Society/European RespiratorySociety (ATS/ERS) Task Force has publishedmethodological recommendations regarding the useof EBC.44
Besides self-fabricated collection systems, the mostcommonly used commercially available devices forEBC collection are the portable R Tube(Charlottesville, Virginia, USA) and non-portableEcoScreen (Jaeger, Wuerzburg Germany). pHmeasurements in EBC collected by these two systemsare repeatable and reproducible.32
Use of different methods of collection has beenfound to give different results that do not follow auniform pattern. From the comparative studies so far,it appears that the possible differences betweendevices appear to vary with the biomarker measuredand with the presence or absence of the disease. Thephysical and chemical properties of the surface of thecollecting device may affect the yield by differentcapacities for adsorption.45
The effect of differing expiratory flow rates has notbeen examined in patients with COPD. Thedifferences between normals and patients may arisebecause patients have a different breathing pattern.Whether expiratory flow rate and tidal volume needto be controlled has not been addressed in studies inCOPD. Theoretically, hyperventilation, forcedexhalation, greater turbulence in more severe airwaysobstruction or larger tidal volumes should yieldhigher concentrations of the EBC markers byfavouring greater aerosolisation of airway liningfluid. In one study46 in patients with asthma, EBCH2O2 was shown to vary inversely with the expiratoryflow rate during collection. However, the pattern ofbreathing had no significant effect on concentrationsof LTB4, LTE4, prostaglandin (PG) E2, pH, NO3
– ortotal protein.47,26 The EBC collection is invariably doneusing oral breathing. The nasal and oralcontamination while collection may change the pH,NO metabolites and leukotrienes like LTB4.48,49 Oneconcern has been oral contamination with ammoniathat can affect EBC pH measurements. However,studies have shown that this is unlikely to have anysignificant effect.50,51
Oral contamination may also affect EBCNO metabolites. Nitrate levels in EBC are influencedby dietary intake. Nitrate is reduced to nitriteby bacterial activity that takes place primarily inthe oropharyngeal tract of healthy subjects.

34
Oropharyngeal nitrite possibly contributes to exhaledNO in non-inflammed airways.52 The LTB4 levelshave been reported to be raised in EBC samples thatcontained salivary amylase.53 Therefore, thecontribution of oral contamination should beinvestigated with respect to each specific EBCmediator.43
The concentrations of mediators measured in theEBC are likely to be affected by the water vapourcontent and variable degrees of aerosolisation. Thesemay not reflect the true levels in the airway liningfluid. These factors may explain the differing levelsreported for different mediators even in normal non-smoking controls as well as the fairly wide within-session variations. Possible solutions to such sourcesof error include corrections by dilutional factorsestimated from another consistent constituent of EBCor report ratios of mediators rather than absolutelevels. These approaches need validation. As mostspecimens are stored and kept frozen at –20 ºC or –80ºC till analysis, the levels of markers may be affected.However, this has not been found to be true for mostmarkers for storage periods upto 2 or 3 months.43
The extent of nasal contamination as well as theeffect of using a nose-clip to occlude the nose is largelyunknown in patients with COPD. Whether a nose clipshould be worn is not certain. However, thereproducibility of EBC pH (see below) was similar,with and without a nose clip.33
The acute effect of smoking is an increase in theoxidative stress. Smoking was shown to cause anacute increase in exhaled 8-isoprostane in COPDpatients by about 50%.8 In normal subjects, acutesmoking was found to increase levels of H2O2.
54 Onthe other hand, the acute effect of smoking a singlecigarette on other EBC compounds such as NO3
–,nitrosothiols, nitrotyrosine and certain cytokines isvariable or inconsistent.43
The ATS/ERS Task Force methodologicalrecommendations on EBC include the followinggeneral suggestions to ensure uniformity inmethodology among studies:44 collect during tidalbreathing using a nose clip and a saliva trap; definecooling temperature and collection time (10 min isgenerally sufficient to obtain 1-2 mL of sample and iswell tolerated by patients); use inert material forcondenser; do not use resistor and do not use a filterbetween the subject and the condenser. In addition,specific recommendations on methodology ofcollection, storage and analysis have been made forindividual biomarkers.
Several other potential confounders including age,sex, diet, drugs and race as well as other biologicalfactors such as circadian fluctuations may influenceresults. The available information on the effect of thesefactors on EBC composition is scanty. The EBC pHwas found not to be influenced by age.50 Nowak et al54
collected EBC seven times every 4 hour during 24hours and three times every 7 days during twoconsecutive weeks and observed diurnal variation inH2O2 levels with two-peak values at 12:00 and 24:00hour. The mean H2O2 concentration estimated overthe whole two-week period was higher in patientsabove 40 years regardless of smoking habit and itpositively correlated with age in never-smokedsubjects. Neither moderate exercise nor one puff ofsalbutamol nor ipratropium influenced significantlythe concentration of H2O2 and TBARs in EBC. Themean H2O2 concentration was found to be increasedsignificantly during the day in both the COPDpatients and controls.55 The effect of diet on nitratelevels was discussed above.
The large number of measurable biomarkers andthe diversity of the methodologies hamperexploration of wide clinical application anddevelopment of any consensus. Koutsokera et al56
have summarised the ranges of concentrations ofdifferent biomarkers include H2O2, NO-relatedproducts, arachidonic acid metabolites and pH in thestudies that have been carried out so far. The only onemarker with established reference values in healthysubjects is EBC pH, whereas the others need furtherrefinement and standardisation of the methodologies.Until the technical aspects of measurements aresorted out, EBC analysis is likely to remain confined toresearch studies. Even though it appears to be a verypromising tool, its adoption as a clinical tool in nearfuture is unlikely.
Reproducibility of Exhaled Breath Condensate
Variations on repeated measurements are animportant consideration in deciding the utility of anassay. These variations may be natural or biologicalor may simply reflect the effect of technical factorsreviewed above. Variations in any assay must beknown before significance can be assigned to changesobserved in response to changed clinical status ortherapeutic intervention. A change with anyintervention should be shown to be greater thanspontaneous variability to attribute it to the beneficialeffect of treatment. Variations may be within-assay(several measurements performed during the singleassay) or short term (within a day) or over a longerterm (over a few days) in a stable condition. Asairway inflammation is likely to be variable over timedue to variations in environmental exposures,infections and disease-related factors, normal subjectscan be expected to show much greater stabilitycompared to patients and any variability in theformer is likely to reflect the imprecision in the assaythat may be an inherent limitation in the method ormay be influenced by other technical factors.
Van Hoydonck et al57 concluded that levels of 8-isoprostane and H2O2 cannot be reproducibly
Exhaled Breath Condensate in COPD S.K. Chhabra and Mansi Gupta

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 35
assessed in EBC from healthy smokers because oftheir low concentration and/or the lack ofsensitivity of the available assays. Within-assaycoefficient of variation of EBC 8-isoprostane was29.2% that was lower than the corresponding valuesfor within-day (65.3%) and between-day (79.1%)variations. Using the Bland Altman method, therewere wide limits of agreement for within-day andbetween-day reproducibility. While within-assayvariability and group mean changes were small,considerable within-day and between-dayvariability raises questions about its suitability formonitoring and assessment of response totherapeutic interventions. The results were similarwith LTB4.58 In contrast, pH was reported to have amuch better stability—within-assay, within-day,and between-day.33 The EBC pH was observed to berobust and reproducible and not affected by severalpatient-related and technical factors in health.50 TheH2O2 has been shown to have had a better stabilityand repeatability compared to 8-isoprostane inpatients with COPD.9 However, it needs to be notedthat all the studies looking at precision ofmeasurements over time had small sample sizes. Animportant consideration in looking at repeatabilityand reproducibility of measurements is thestatistical method used. Inappropriate methods mayunderestimate variation.43 Correlations andcomparisons of group means can hide vitaldifferences and agreement analysis is the preferredmethod to look at repeatability. The issue of short-term and long-term stability needs to be addressedfor several other mediators, in health and disease,and the minimal clinically important changeremains to be defined.
Safety Issues
The studies in patients with COPD have useddifferent EBC collection devices and in none of theseany adverse effects have been reported. A majorconcern is the possibility of transmission of infectionbetween individuals. Filters cannot be used in theinlets of the collecting devices as these may absorbsome of exhaled substances. Use of disposablesystems is certainly an effective way of preventingany such transmission of infection between patientsbut this adds to the total costs. Use of non-disposableEBC collection systems, however, was not shown tofacilitate transmission of infection in EBC studies inpatients with cystic fibrosis.59
NOVEL METHODS FOR EXHALEDBREATH CONDENSATE ANALYSIS
Application of newer technologies offer excitingavenues for exploring unknown biomarkers. The
tools of genomics, proteomics, and metabonomics,that investigate gene expression, protein expression,and metabolic regulation in the pathogenesis ofdisease, respectively, offer an entirely differentapproach to the characterisation of EBC in COPDthan what has been followed so far.
The development of proteomic techniques such asliquid chromatography-mass spectrometry and gelelectrophoresis-mass spectrometry have been appliedto investigate the proteome of lung specimens such assputum, BALF, EBC, cells and biopsies from COPDpatients. These may provide a better understandingof the proteome differentially expressed by COPDpatients in the course of the disease.60,61 The proteinsrecovered in EBC might be used to monitorrespiratory diseases including COPD non-invasivelyin the future.
Metabonomics may be another important tool thatcan provide qualitative and quantitative informationon low-molecular weight metabolites present in cells,tissues, and fluids. The EBC may provide a suitablematrix for metabonomic studies to investigatebiochemical profiles of metabolites using nuclearmagnetic resonance (NMR) spectroscopy. The use ofnuclear magnetic resonance profiling of EBC mayallow hypothesis-free profiling of biomarkers, ratherthan the traditional hypothesis-driven approach. Itmay now be possible to separate specific EBC profiles,with implication in disease phenotyping andpersonalised therapy.62,63 The application of NMRspectroscopy in study of EBC in COPD is going toevolve in future and at present very little publishedwork is there.
CONCLUSIONS
Exhaled breath condensate analysis is an evolvingnon-invasive tool for monitoring of inflammation andoxidative stress in COPD. It may provide an insightinto the complex pathways of the origin andperpetuation of airway inflammation in COPD.Potential clinical applications include diagnosis,monitoring of severity and evaluation of therapeuticinterventions, phenotyping and prognostication.While studies so far have focused on measurementsof levels of markers such as 8-isoprostane, hydrogenperoxide, products of NO, lipid mediators,eicosanoids and airway fluid acidification, thismethod of studying airway inflammation is still in itsinfancy. Evolving technologies of genomics,proteomics, and metabonomics may provide deeperand newer insights into the molecular mechanismsunderlying the pathogenesis of COPD and identifytargets for therapeutic interventions permittingspecific interventions unlike the present treatmentstrategies that are largely symptomatic andsupportive.
36
REFERENCES
1. Global Strategy for the Diagnosis, Management, andPrevention of Chronic Obstructive Pulmonary Disease.NHLBI/WHO Global Initiative for Chronic ObstructiveLung Disease (GOLD).Executive summary update 2010.www.goldcopd.org.
2. Nadeem A, Raj HG, Chhabra SK. Increased oxidativestress and altered levels of antioxidants in chronicobstructive pulmonary disease. Inflammation 2005;29:23-32.
3. Lee W, Thomas PS. Oxidative stress in COPD and itsmeasurement through exhaled breath condensate. ClinTransl Sci 2009;2:150-5.
4. Lin JL, Thomas PS. Current perspectives of oxidativestress and its measurement in chronic obstructivepulmonary disease. COPD 2010;7:291-306.
5. He Z, Chen Y, Chen P, Wu G, Cai S. Local inflammationoccurs before systemic inflammation in patientswith COPD. Respirology 2010;15:478-84.
6. van Beurden WJC, Harff GA, Dekhuijzen PNR, van denBosch MJ, Creemers JP, Smeenk FW. An efficient andreproducible method for measuring hydrogen peroxide inexhaled breath condensate. Respir Med 2002;96:197-203.
7. Gerritsen WB, Asin J, Zanen P, van den Bosch JM, Haas FJ.Markers of inflammation and oxidative stress inexacerbated chronic obstructive pulmonary diseasepatients. Respir Med 2005;99:84-90.
8. Montuschi P, Collins JV, Ciabattoni G, Lazzeri N, CorradiM, Kharitonov SA, et al Exhaled 8-isoprostane as an invivo biomarker of lung oxidative stress in patientswith COPD and healthy smokers. Am J Respir Crit CareMed 2000;162:1175-7.
9. Kostikas K, Papatheodorou G, Psathakis K, PanagouP, Loukides S. Oxidative stress in expired breathcondensate of patients with COPD. Chest 2003;124:1373-80.
10. Izquierdo JL, Almonacid C, Parra T, Pérez J. Systemic andlung inflammation in 2 phenotypes of chronic obstructivepulmonary disease. Arch Bronconeumol 2006;42:332-7.
11. Inonu H, Doruk S, Sahin S, Erkorkmaz U, Celik D, CelikelS, et al. The comparison of oxidative stress levels inexhaled breath condensate between patients with chronicobstructive pulmonary disease and smokers. RespirCare 2011 Sep 26. [Epub ahead of print]
12. Mazur W, Stark H, Sovijärvi A, Myllärniemi M, Kinnula VL.Comparison of 8-isoprostane and interleukin-8 in inducedsputum and exhaled breath condensate from asymptomaticand symptomatic smokers. Respiration 2009;78:209-16.
13. Antczak A, Piotrowski W, Marczak J, Ciebiada M, GorskiP, Barnes PJ. Correlation between eicosanoids inbronchoalveolar lavage fluid and in exhaled breathcondensate. Dis Markers 2011;30:213-20.
14. Makris D, Paraskakis E, Korakas P, KaragiannakisE, Sourvinos G, Siafakas NM, et al. Exhaled breathcondensate 8-isoprostane, clinical parameters, radiologicalindices and airway inflammation in COPD.Respiration 2008;75:138-44.
15. García-Rio F, Romero D, Lores V, Casitas R, HernanzA, Galera R, et al. Dynamic hyperinflation, arterial bloodoxygen, and airway oxidative stress in stable patients withCOPD. Chest 2011;140:961-9.
16. Guatura SB, Martinez JA, Santos Bueno PC, Santos ML.Increased exhalation of hydrogen peroxide in healthysubjects following cigarette consumption. Sao Paulo MedJ 2000;118:93-8.
17. Dekhuijzen PNR, Aben KKH, Dekker I, AartsLP, Wielders PL, van Herwaarden CL, et al. Increased
exhalation of hydrogen peroxide in patients with stableand unstable chronic obstructive pulmonary disease. Am JRespir Crit Care Med 1996;154:813-6.
18. Nowak D, Kasielski M, Pietras T, Bialasiewicz P, AntczakA. Cigarette smoking does not increase hydrogenperoxide levels in expired breath condensate of patientswith stable COPD. Monaldi Arch Chest Dis 1998;53:268-73.
19. Nowak D, Kasielski M, Antczak A, Pietras T,Bialasiewicz P. Increased content of thiobarbituric acid-reactive substances and hydrogen peroxide in the expiredbreath condensate of patients with stable chronicobstructive pulmonary disease: no significant effect ofcigarette smoking. Respir Med 1999;93:389-96.
20. Möller W, Heimbeck I, Weber N, Khadem Saba G, KörnerB, Neiswirth M, et al. Fractionated exhaled breathcondensate collection shows high hydrogen peroxiderelease in the airways. J Aerosol Med Pulm DrugDeliv 2010;23:129-35.
21. Ferreira IM, Hazari MS, Gutierrez C, Zamel N, ChapmanKR. Exhaled nitric oxide and hydrogen peroxide inpatients with chronic obstructive pulmonary disease:effects of inhaled beclomethasone. Am J Respir Crit CareMed 2001;164:1012-5.
22. Kasielski M, Nowak D. Long-term administration of N-acetylcysteine decreases hydrogen peroxide exhalation insubjects with chronic obstructive pulmonary disease.Respir Med 2001;95:448-56.
23. van Beurden WJ, Smeenk FW, Harff GA, Dekhuijzen PN.Markers of inflammation and oxidative stress during lowerrespiratory tract infections in COPD patients. MonaldiArch Chest Dis 2003;59:273-80.
24. Biernacki WA, Kharitonov SA, Barnes PJ. Increasedleukotriene B4 and 8-isoprostane in exhaled breathcondensate of patients with exacerbations of COPD.Thorax 2003;58:294-8.
25. Kostikas K, Gaga M, Papatheodorou G, KaramanisT, Orphanidou D, Loukides S. Leukotriene B4 in exhaledbreath condensate and sputum supernatant in patientswith COPD and asthma. Chest 2005;127:1553-9.
26. Montuschi P, Barnes PJ. Exhaled leukotrienes andprostaglandins in asthma. J Allergy Clin Immunol2002;109:615-20.
27. Montuschi P, Kharitonov SA, Ciabattoni G, Barnes PJ.Exhaled leukotrienes and prostaglandins in COPD. Thorax2003;58:585-8.
28. Ko FW, Leung TF, Wong GW, Ngai J, To KW, Ng S, et al.Measurement of tumor necrosis factor-alpha, leukotrieneB4, and interleukin-8 in the exhaled breath condensate inpatients with acute exacerbations of chronic obstructivepulmonary disease. Int J Chron Obstruct Pulmon Dis 2009;4:79-86.
29. Bhowmik A, Seemungal TAR, Sapsford RJ, Wedzicha ZA.Relation of sputum inflammatory markers to symptomsand lung function changes in COPD exacerbations. Thorax2000;55:114-20.
30. Ko FW, Lau CY, Leung TF, Wong GW, Lam CW, Hui DS.Exhaled breath condensate levels of 8-isoprostane, growthrelated oncogene alpha and monocyte chemoattractantprotein-1 in patients with chronic obstructive pulmonarydisease. Respir Med 2006;100:630-8.
31. Ricciardolo FL, Gaston B, Hunt J. Acid stress in thepathology of asthma. J Allergy Clin Immunol 2004;113:610-9.
32. Koczulla R, Dragonieri S, Schot R, Bals R, GauwSA, Vogelmeier C, et al. Comparison of exhaled breathcondensate pH using two commercially available devices inhealthy controls, asthma and COPD patients. RespirRes 2009;10:78.
Exhaled Breath Condensate in COPD S.K. Chhabra and Mansi Gupta
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 37
33. Borrill Z, Starkey C, Vestbo J, Singh D. Reproducibility ofexhaled breath condensate pH in chronic obstructivepulmonary disease. Eur Respir J 2005;25:269-74.
34. Papaioannou A, Loukides S, Minas M, Zhang J, Wang C.Exhaled breath condensate pH as a biomarker of COPDseverity in ex-smokers. Respir Res 2011;12:67-73.
35. MacNee W, Rennard SI, Hunt JF, Edwards LD, MillerBE, Locantore NW, et al. Evaluation of exhaled breathcondensate pH as a biomarker for COPD. Respir Med2011;105:1037-45.
36. Bartoli ML, Novelli F, Costa F, Malagrinò L, MelosiniL, Bacci E, et al. Malondialdehyde in exhaled breathcondensate as a marker of oxidative stress in differentpulmonary diseases. Mediators Inflamm 2011;2011:891752
37. Esther CR Jr, Lazaar AL, Bordonali E, Qaqish B, BoucherRC. Elevated airway purines in COPD. Chest 2011;140:954-60.
38. Kharitonov SA, Chung FK, Evans DJ, O’Connor BJ, BarnesPJ. The elevated level of exhaled nitric oxide in asthmaticpatients is mainly derived from the lower respiratory tract.Am J Respir Crit Care Med 1996;153:1773-80.
39. Brindicci C, Cosio B, Gajdocsi R, Collins JV, Bush A,Abdallah S, et al. Extended exhaled NO measurements atdifferent exhalation flows may differentiate betweenbronchial and alveolar inflammation in patients withasthma and COPD. Eur Respir J 2002;20:174s.
40. Corradi M, Montuschi P, Donnelly LE, Pesci A,Kharitonov SA, Barnes PJ. Increased nitrosothiols inexhaled breath condensate in inflammatory airwaydiseases. Am J Respir Crit Care Med 2001;163:854-8.
41. Liu J, Sandrini A, Thurston MC, Yates DH, Thomas PS.Nitric oxide and exhaled breath nitrite/nitrates in chronicobstructive pulmonary disease patients. Respiration 2007;74:617-23.
42. Kharitonov SA, Barnes PJ. Effects of corticosteroids onnoninvasive biomarkers of inflammation in asthma andchronic obstructive pulmonary disease. Proc Am Thorac Soc2004;1:191-9.
43. Borrill ZL, Roy K D. Singh D. Exhaled breath condensatebiomarkers in COPD. Eur Respir J 2008;32:472-86.
44. Horvath I, Hunt J, Barnes PJ. Exhaled breath condensate:methodological recommendations and unresolvedquestions. Eur Respir J 2005;26:523-48.
45. Rosias PP, Robroeks CM, Niemarkt HJ, Kester AD,Vernooy JH, Suykerbuyk J, et al. Breath condenser coatingsaffect measurement of biomarkers in exhaled breathcondensate. Eur Respir J 2006;28:1036-41.
46. Schleiss MB, Holz O, Behnke M, Richter K, Magnussen H,Jorres RA. The concentration of hydrogen peroxide inexhaled air depends on expiratory flow rate. Eur Respir J2000;16:1115-8.
47. McCafferty JB, Bradshaw TA, Tate S, Greening AP, InnesJA. Effects of breathing pattern and inspired airconditions on breath condensate volume, pH, nitrite, andprotein concentrations. Thorax 2004;59:694-8.
48. Gaber F, Acevedo F, Delin I, Sundblad BM, Palmberg L,Larsson K, et al. Saliva is one likely source of leukotrieneB4 in exhaled breath condensate. Eur Respir J 2006;28:1229-35.
49. Vass G, Husza´r E, Bara´t E, Valyon M, Kiss D, PenzesI, et al. Comparison of nasal and oral inhalation duringexhaled breath condensate collection. Am J Respir Crit CareMed 2003;167:850-5.
50. Vaughan J, Ngamtrakulpanit L, Pajewski TN, TurnerR, Nguyen TA, Smith A, et al. Exhaled breath condensatepH is a robust and reproducible assay of airway acidity.Eur Respir J 2003;22:889-94.
51. Wells K, Vaughan J, Pajewski TN, Hom S,Ngamtrakulpanit L, Smith A, et al. Exhaled breathcondensate pH assays are not influenced by oralammonia. Thorax 2005;60:27-31.
52. Marteus H, Tornberg DC, Weitzberg E, Schedin U, AlvingK. Origin of nitrite and nitrate in nasal and exhaled breathcondensate and relation to nitric oxide formation. Thorax2005;60:219-25.
53. Gaber F, Acevedo F, Delin I, Sundblad BM, Palmberg L,Larsson K, et al. Saliva is one likely source of leukotrieneB4 in exhaled breath condensate. Eur Respir J 2006;28:1229-35.
54. Nowak D, Kalucka S, Bialasiewicz P, Krol M. Exhalationof H2O2 and thiobarbituric acid reactive substances(TBARs) by healthy subjects. Free Radic Biol Med 2001;30:178-86.
55. van Beurden WJ, Dekhuijzen PN, Harff GA, Smeenk FW.Variability of exhaled hydrogen peroxide in stable COPDpatients and matched healthy controls. Respiration2002;69:211-6.
56. Koutsokera A, Loukides S, Gourgoulianis KI, Kostikas K.Biomarkers in the exhaled breath condensate of healthyadults: mapping the path towards reference values. CurrMed Chem 2008;15:620-30.
57. Van Hoydonck PG, Wuyts WA, Vanaudenaerde BM,Schouten EG, Dupont LJ, Temme EH. Quantitativeanalysis of 8-isoprostane and hydrogen peroxide inexhaled breath condensate. Eur Respir J 2004;23:189-92.
58. Borrill ZL, Starkey RC, Singh SD. Variability ofexhaled breath condensate leukotriene B4 and 8-isoprostane in COPD patients. Int J Chron ObstructPulmon Dis 2007;2:71-6.
59. Vogelberg C, Hirsch T, Ro¨sen-Wolff A, Kerkmann ML,Leupold W. Pseudomonas aeruginosa and Burkholderia cepaciacannot be detected by PCR in the breath condensate ofpatients with cystic fibrosis. Pediatr Pulmonol 2003;36:348-52.
60. Casado B, Luisetti M, Iadarola P. Advances in proteomictechniques for biomarker discovery in COPD. Expert RevClin Immunol 2011;7:111-23.
61. Casado B, Iadarola P, Luisetti M, Kussmann M.Proteomics-based diagnosis of chronic obstructivepulmonary disease: the hunt for new markers. Expert RevProteomics 2008;5:693-704.
62. de Laurentiis G, Paris D, Melck D, Maniscalco M, MarsicoS, Corso G, et al. Metabonomic analysis of exhaledbreath condensate in adults by nuclear magnetic resonancespectroscopy. Eur Respir J 2008;32:1175-83.
63. Sofia M, Maniscalco M, de Laurentiis G, Paris D, MelckD, Motta A. Exploring airway diseases by NMR-basedmetabonomics: a review of application to exhaledbreath condensate. J Biomed Biotechnol 2011;2011:403260.Epub 2011 Mar 15.

38 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
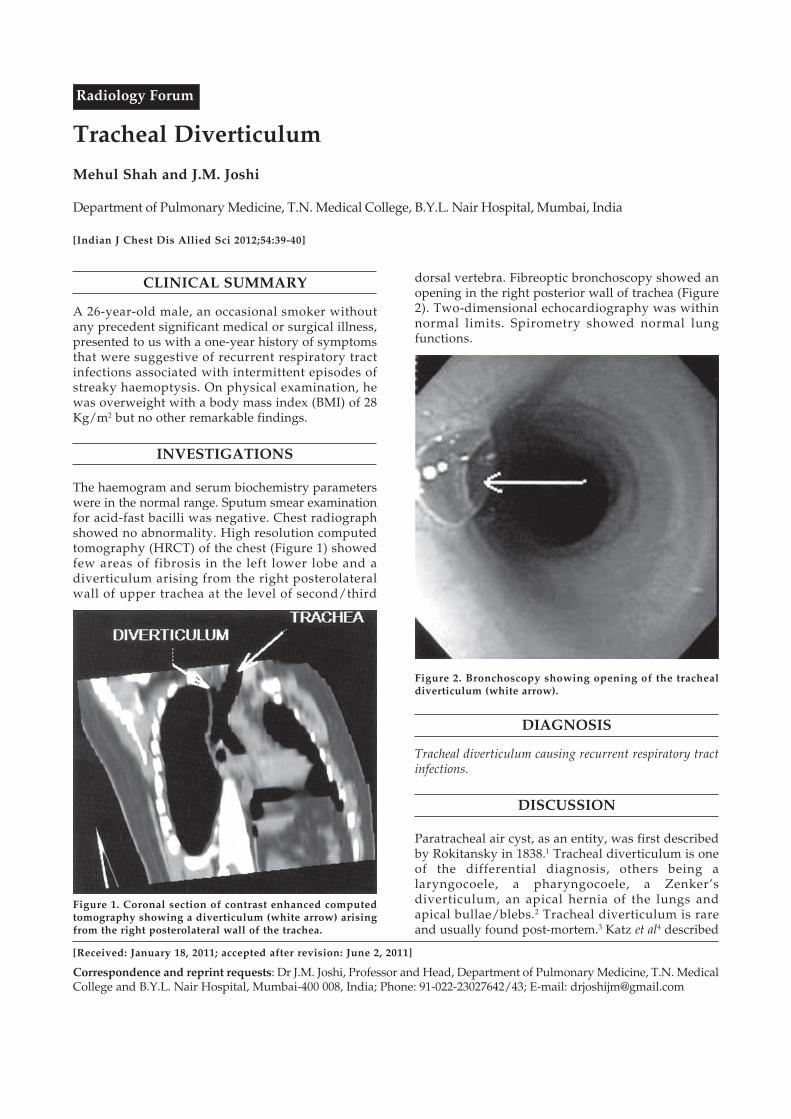
Tracheal Diverticulum
Mehul Shah and J.M. Joshi
Department of Pulmonary Medicine, T.N. Medical College, B.Y.L. Nair Hospital, Mumbai, India
[Indian J Chest Dis Allied Sci 2012;54:39-40]
CLINICAL SUMMARY
A 26-year-old male, an occasional smoker withoutany precedent significant medical or surgical illness,presented to us with a one-year history of symptomsthat were suggestive of recurrent respiratory tractinfections associated with intermittent episodes ofstreaky haemoptysis. On physical examination, hewas overweight with a body mass index (BMI) of 28Kg/m2 but no other remarkable findings.
INVESTIGATIONS
The haemogram and serum biochemistry parameterswere in the normal range. Sputum smear examinationfor acid-fast bacilli was negative. Chest radiographshowed no abnormality. High resolution computedtomography (HRCT) of the chest (Figure 1) showedfew areas of fibrosis in the left lower lobe and adiverticulum arising from the right posterolateralwall of upper trachea at the level of second/third
[Received: January 18, 2011; accepted after revision: June 2, 2011]
Correspondence and reprint requests: Dr J.M. Joshi, Professor and Head, Department of Pulmonary Medicine, T.N. MedicalCollege and B.Y.L. Nair Hospital, Mumbai-400 008, India; Phone: 91-022-23027642/43; E-mail: [email protected]
Radiology Forum
dorsal vertebra. Fibreoptic bronchoscopy showed anopening in the right posterior wall of trachea (Figure2). Two-dimensional echocardiography was withinnormal limits. Spirometry showed normal lungfunctions.
Figure 1. Coronal section of contrast enhanced computedtomography showing a diverticulum (white arrow) arisingfrom the right posterolateral wall of the trachea.
Figure 2. Bronchoscopy showing opening of the trachealdiverticulum (white arrow).
DIAGNOSIS
Tracheal diverticulum causing recurrent respiratory tractinfections.
DISCUSSION
Paratracheal air cyst, as an entity, was first describedby Rokitansky in 1838.1 Tracheal diverticulum is oneof the differential diagnosis, others being alaryngocoele, a pharyngocoele, a Zenker’sdiverticulum, an apical hernia of the lungs andapical bullae/blebs.2 Tracheal diverticulum is rareand usually found post-mortem.3 Katz et al4 described

Radiology Forum Mehul Shah and J.M. Joshi
four types of tracheal diverticuli-rudimentarybronchus, cystic dilatation of mucus gland duct,tracheocoele and diverticulum associated withtracheobronchomegaly. Tracheal diverticuli may becongenital or acquired. Both the varieties are lined byciliated columnar epithelium. The congenital variety,which is thought to represent a malformedsupernumary branch of the trachea,5 hascartilaginous rings in its wall that are similar to thetracheal wall. These usually arise 4 to 5 centimetersbelow the true vocal cords, are relatively small andnarrow-mouthed and may occur in isolation or inassociation with other congenital anomalies withinthe tracheobronchial tree. In the acquired variety, thatis thought to be due to increased intra-luminalpressure causing out-bulging of a weak part in thetracheal wall, the wall is devoid of any cartilaginousrings. Another mechanism that has been proposed forits development is cystic distension of the mucousgland ducts.3 It can arise at any level and is wide-mouthed and larger in size.6 Majority of the trachealdiverticuli arise at the D2 vertebral level.2 Thesupportive presence of oesophagus and aortic arch onthe left side of the tracheal wall makes it lesssusceptible to the development of diverticulaexplaining the preponderant right sided location ofthe diverticula.1 These patients are commonlyasymptomatic. However, they may present withchronic productive cough, dyspnoea, stridor,haemoptysis and repeated episodes oftracheobronchitis.7 A small air cyst orifice is usuallydifficult to visualise on bronchoscopy. In previousstudies,8,9 even in surgically proven trachealdiverticula, no mucosal orifices were detected on pre-operative bronchoscopy. Hence, a computedtomography of the trachea with reconstruction in thecoronal plane is considered the needed modality for
diagnosis.5 Since most of the tracheal diverticula areeither asymptomatic or do not cause significantsymptoms, a conservative symptomatic medicaltreatment with antibiotics, mucolytics andphysiotherapy usually suffices and very rarely asurgical resection is required.6,8
The duration of symptoms in our patient was onlyone year and no other anomaly of the tracheo-bronchial tree was found. Thus, it is most likely thatthe tracheal diverticulum was of an acquired variety.The patient was managed conservatively withphysiotherapy and vaccinations to reduce thefrequency of infections and prevent them.
REFERENCES
1. Soto-Hurtado EJ, Peñuela-Ruíz L, Rivera-Sánchez I,Torres-Jiménez J. Tracheal diverticulum: a review of theliterature. Lung 2006;184:303-7.
2. Goo JM, Im JG, Ahn JM, Moon WK, Chung JW, Park JH, etal. Right paratracheal air cysts in the thoracic inlet: clinicaland radiologic significance. AJR Am J Roentgenol1999;73:65-70.
3. MacKinnon D. Tracheal diverticula. J Pathol Bacteriol1953;65:513-7.
4. Katz I, Levine M, Herman P. Tracheobronchomegaly. AJRAm J Roentgenol 1962;88:1084-9.
5. Rahalkar MD, Lakhkar DL, Joshi SW, Gundawar S.Tracheal diverticula-report of 2 cases. Indian J Radiol Imag2004;14:197-8.
6. Caversaccio M, Becker M, Zbären P. Tracheal diverticulumpresenting with recurrent laryngeal nerve paralysis. AnnOtol Rhinol Laryngol 1998;107:362-4.
7. Early EK, Bothwell MR. Congenital tracheal diverticulum.Otolaryngol Head Neck Surg 2002;127:119-21.
8. Infante M, Mattavelli F, Valente M, Alloisio M, Preda F,Ravasi G. Tracheal diverticulum: a rare cause andconsequence of chronic cough. Eur J Surg 1994;160:315-6.
9. Collins MM, Wight RG. Posterior tracheal wall diverticula:an expected finding. J Laryngol Otol 1997;111:663-5.
40

Case Report
Bronchoscopic Management of Benign Bronchial Stenosis byElectrocautery and Balloon Dilatation
M. Garg, Pratibha Gogia, P. Manoria and R. Goyal
Department of Respiratory Medicine and Critical Care, Jaipur Golden Hospital, New Delhi, India
ABSTRACT
Benign bronchial stenosis is managed by surgical or bronchoscopic methods. Although surgical approach is definitive, it istechnically demanding and is costlier than bronchoscopic treatment. Here, we report the case of a 27-year-old female patientwith symptomatic benign bronchial stenosis of the left main bronchus. The stenosis was dilated successfully through afibreoptic bronchoscope by electrocautery followed by balloon bronchoplasty and application of mitomycin-C. On followup, there was no evidence of re-stenosis. [Indian J Chest Dis Allied Sci 2012;54:41-43]
Key words: Flexible bronchoscope, Benign bronchial stenosis, Electrocautrey, Balloon dilatation.
[Received: January 24, 2011; accepted after revision: July 28, 2011]
Correspondence and reprint requests: Dr Rajiv Goyal, House No. 66, Vaishali, Pitampura, New Delhi-110 034, India; Phone:91-11-27311182; E-mail: [email protected]
INTRODUCTION
Benign tracheobronchial stenosis in adults can bea complication of a variety of diseases/interventions, including tuberculosis (TB),sarcoidosis, Wegener’s granuomatosis, trauma,endotracheal intubation, tracheostomy, bronchialsleeve resection, irradiation, and fibrosingmediastinitis.1,2 Depending on the site of the lesionand severity of the narrowing, the stenosis maycause symptoms of dyspnoea, stridor, wheeze,cough, or recurrent respiratory tract infections.Definitive treatment of such stenoses is surgicalresection and re-anastomosis. However, this maynot be a feasible option in many patients because ofpoor general condition, compromised pulmonaryfunctions, or technical difficulties.
A variety of bronchoscopic techniques, suchas bougie or balloon dilatation (bronchoplasty),3
Nd-YAG laser resection,4 cryotherapy,5 electro-cautery,6 and stent placement7,8 have been used asan alternative, if a surgical approach is notpossible. In some cases, successful manage-ment ofa strictured segment may require more than onemodality or technique through the broncho-scope.
In the present report, we describe the use of amulti-modality treatment consisting of electrocautery,balloon bronchoplasty, and subsequent localapplication of mitomycin-C for the dilatation of abenign tracheobronchial stenosis.
CASE REPORT
A 27-year-old woman presented with complaints ofrecurrent episodes of cough with expectorationduring the last four years. She had been hospitalisedseveral times with complaints of high grade fever,productive cough, and breathlessness and treatedeach time with intravenous antibiotics andbronchodilators, to which she responded. She deniedany history of TB, surgical intervention in the chest,or any other significant medical illness in the past.
On examination of the chest, breath sounds on theleft side were reduced with localised wheeze on thesame side. Chest radiograph showed deviation of themediastinum to the left with crowding of ribs,indicating a loss of volume. The left hemithorax washazy and showed multiple soft, nodular opacitieswith small calcific foci and thickening of the left apicalpleura. A contrast-enhanced computed tomography(CT) of the thorax confirmed loss of lung volume onthe left side with fibrosis and bronchiectasis of the leftupper lobe. The left lower lobe was largely normalwith minimal dilatation of a few bronchi. Areconstructed coronal image of the CT showed thatthe left main bronchus was narrowed with a 2.5cmlong, narrow stricture; however, the distal bronchiwere patent as shown in figure 1.
Routine investigations including complete bloodcounts, renal and liver function tests, and urineexamination were in the normal range. Sputumsmears for acid-fast bacilli, and smears and culturesfor pyogenic organisms and fungi were also negative.An autoimmune screen for collagen vascular diseases
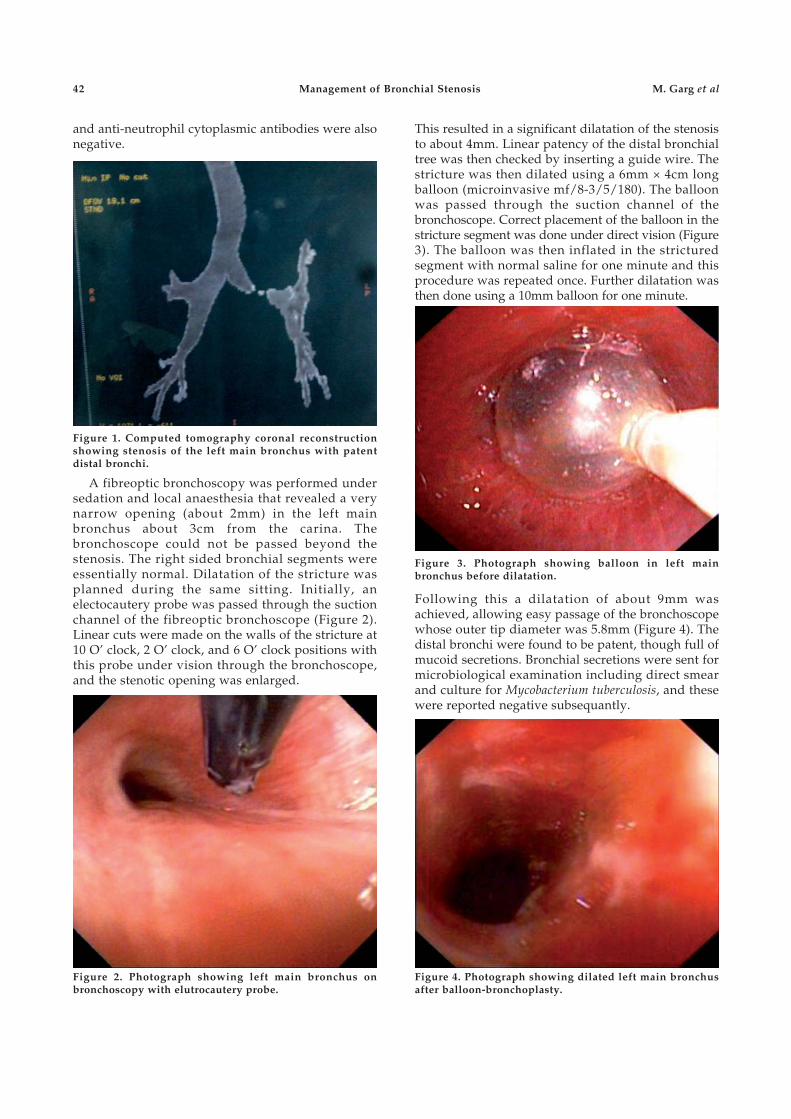
42
and anti-neutrophil cytoplasmic antibodies were alsonegative.
Management of Bronchial Stenosis M. Garg et al
This resulted in a significant dilatation of the stenosisto about 4mm. Linear patency of the distal bronchialtree was then checked by inserting a guide wire. Thestricture was then dilated using a 6mm × 4cm longballoon (microinvasive mf/8-3/5/180). The balloonwas passed through the suction channel of thebronchoscope. Correct placement of the balloon in thestricture segment was done under direct vision (Figure3). The balloon was then inflated in the stricturedsegment with normal saline for one minute and thisprocedure was repeated once. Further dilatation wasthen done using a 10mm balloon for one minute.
Figure 3. Photograph showing balloon in left mainbronchus before dilatation.
A fibreoptic bronchoscopy was performed undersedation and local anaesthesia that revealed a verynarrow opening (about 2mm) in the left mainbronchus about 3cm from the carina. Thebronchoscope could not be passed beyond thestenosis. The right sided bronchial segments wereessentially normal. Dilatation of the stricture wasplanned during the same sitting. Initially, anelectocautery probe was passed through the suctionchannel of the fibreoptic bronchoscope (Figure 2).Linear cuts were made on the walls of the stricture at10 O’ clock, 2 O’ clock, and 6 O’ clock positions withthis probe under vision through the bronchoscope,and the stenotic opening was enlarged.
Figure 1. Computed tomography coronal reconstructionshowing stenosis of the left main bronchus with patentdistal bronchi.
Figure 2. Photograph showing left main bronchus onbronchoscopy with elutrocautery probe.
Following this a dilatation of about 9mm wasachieved, allowing easy passage of the bronchoscopewhose outer tip diameter was 5.8mm (Figure 4). Thedistal bronchi were found to be patent, though full ofmucoid secretions. Bronchial secretions were sent formicrobiological examination including direct smearand culture for Mycobacterium tuberculosis, and thesewere reported negative subsequantly.
Figure 4. Photograph showing dilated left main bronchusafter balloon-bronchoplasty.

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 43
To prevent re-stenosis due to fibrosis, 3mL of0.2mg/mL mitomycin-C was sprayed at the stricturesite. After dilatation and thorough suctioning, theupper lobe, lingular lobe, and lower lobe openingswere clearly visible. The upper lobe opening was alsofound to be narrowed, and it was dilated using a6mm balloon. The patient tolerated the procedurewell and was discharged the same day after a fewhours of observation.
A second bronchoscopy done after a weekconfirmed that the patency of the dilated bronchi wasmaintained. Follow-up bronchoscopies were done at3 and 7 months after the original procedure. Theseshowed a well dilated left main bronchus with nosigns of re-stenosis. The patient had mild cough andexpectoration for a few days after the procedure, thatresponded to symptomatic treatment.
The cause of the bronchial stricture could not beascertained in this patient where investigations failedto show any definitive aetiology.
DISCUSSION
Tracheobronchial strictures can be managed either bysurgery or by employing a variety of endoscopictechniques. Surgical resection of the stenosis is anoption but the associated risks, and the technicallimitations of surgical resection and reconstructionwarrant the need for other therapeutic options inmany patients. Serial dilatation of the stenosis with ablunt-tipped rigid bronchoscope can be performed;but, initial dilatation of a tight stenosis as in ourpatient can prove difficult, especially if there is amismatch between the stenosis and the diameter ofthe rigid bronchoscope. Moreover, the procedurerequires general anaesthesia.9,10
Among the treatment options reported, treatingsuch strictures using a flexible bronchoscope alongwith cautery/laser and balloon dilatation appears tobe least invasive, quick, safe, and inexpensive, and itis associated with a low risk of complications. It canbe done under local anaesthesia with conscioussedation. Post-procedure stay in the hospital isshort and the patient can be discharged on the sameday. The only drawback is a possible need formultiple sittings as serial dilatations may berequired. Various studies have shown that morethan 50% of patients treated with balloon dilatationmay not need any other form of therapeuticintervention. Hence, it may reasonably beconsidered as the preferred option to restore theairway lumen in benign stenosis.1,2
In the case described here, re-stenosis did notoccur, possibly due to the short length of the strictureas well as the use of mitomycin-C to decrease thefibrosis after the dilatation. Various studies haveshown that topical application of mitomycin-C, a
potent inhibitor of fibroblasts, reduces granulationtissue formation and prevents restenosis.11
Complications associated with dilatation aretearing of the bronchial wall due to excessivestretching, resulting in pneumothorax, pneumo-mediastinum, and subcutaneous emphysema. Thesecomplications can be avoided using cautery/Nd-YAG laser for cutting open the fibrotic stricture priorto balloon dilatation, as it avoids the need forexcessively high pressures for dilating the balloon.12
This was done successfully in the present case.To conclude, balloon dilatation along with
electrocautery via a flexible bronchoscope is aneffective and safe multi-modality approach for benigntracheal stenosis. It may be used as a preferred optionto surgery or use of a rigid bronchoscope because oflower costs, avoidance of general anaesthesia andfewer complications. The application of mitomycin-Cto the dilated segment immediately after theprocedure appears to decrease the chances of re-stenosis.
REFERENCES
1. Chhajed PN, Malouf MA, Glanville AR. Bronchoscopicdilatation in the management of benign (non-transplant)tracheobronchial stenosis. Intern Med J 2001;31:512-6.
2. Sheski FD, Mathur PN. Long-term results of fiberopticbronchoscopic balloon dilation in the management ofbenign tracheobronchial stenosis. Chest 1998;114:796-800.
3. Ball JB, Delaney JC, Evans CC, Donnelly RJ, Hind CR.Endoscopic bougie and balloon dilatation of multiplebronchial stenoses: 10 year follow-up. Thorax 1991;46:933-5.
4. Sutedja TG, Schreurs AJ, Vanderschueren RG, Kwa B,vd Werf TS, Postmus PE. Bronchoscopic therapy inpatients with intraluminal typical bronchial carcinoid.Chest 1995; 107:556-8.
5. Mathur PN, Wolf KM, Busk MF, Briete WM, Datzman M.Fiberoptic bronchoscopic cryotherapy in the managementof tracheobronchial obstruction. Chest 1996;110:718-23.
6. Hooper RG, Jackson FN. Endobronchial electrocautery.Chest 1988;94:595-8.
7. Tsang V, Goldstraw P. Self-expanding metal stent fortracheobronchial strictures. Eur J Cardiothorac Surg 1992;6:555-9.
8. Hautmann H, Huber RM. Stent flexibility: an essentialfeature in the treatment of dynamic airway collapse. EurRespir J 1996;9:609-11.
9. Stephens K, Wood D. Bronchoscopic management ofcentral airway obstruction. J Thorac Cardiovasc Surg 2000;119:289-96.
10. Venuta F, Rendina EA, De Giacomo T, Ciccone AM, Anile M,Moretti M, et al. Operative endoscopy of the airway withthe old-fashioned esophageal dilators. Ann Thorac Surg2005;79:718-9.
11. Wong JL, Tie ST, Samril B, Lm CL, Rahman MRA,Rahman, JAA. Succesful treatment of tracheal stenosis byrigid bronchoscopy and topical mitomycin-C: a casereport. Cases Journal 2010;3:2.
12. Kwon Ys, kim H, Kang KW, Koh WJ, Suh GY, Chung MP,et al. The role of ballooning in patients with post tuberculosisbronchial stenosis. Tuberc Respir Dis 2009;66:431-6.

44 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
Full text articles published in IJCDAS from July-September2003 onwards can be accessed online on Internet through thefollowing sites
V.P. Chest Institute’s site: http:// www.vpci.org.in
Indmed’s site: http://medind.nic.in
Guidance for Authors appears in every issue.
Authors’ Index appears in the last issue of the year
Clinical Trials Registry-IndiaA Clinical Trials Registry-India has been set up jointly by the Department of Science andTechnology (DST), World Health Organisation (WHO) and Indian Council of Medical Research atthe National Institute of Medical Statistics (NIMS), New Delhi. This Registry will provide a platformfor registration of all clinical trials. The objective of the Registry is to establish a public record systemby registering all prospective clinical trials of any intervention (drug, surgical procedure, preventivemeasures, lifestyle modifications, devices, educational or behavioural treatment, rehabilitationstrategies and complementary therapies) conducted in India involving human participants. TheRegistry will be made publicly available on the internet at no cost. The website of the IndianRegistry is www.ctri.in.

Case Report
Tracheobronchial Compression by Right-sided Aortic Archin a Middle Aged Male
Manohar Lal Gupta, Chand Bhandari, Mahesh Mishra and Jyotsna Sinha
Department of Chest and Tuberculosis, S.M.S. Medical College, Jaipur (Rajasthan), India
ABSTRACT
Exertional dyspnoea is a common symptom among middle-aged population. Diagnostic evaluation of such patients is oftenchallenging and confusing. We report a patient presenting with exertional dyspnoea and an obstructive ventilatory defecton spirometry that was refractory to bronchodilator therapy. Careful review of the chest radiograph and spirometrypointed towards variable intra-thoracic airways obstruction as a cause of dyspnoea. Contrast enhanced computedtomography (CECT) of the thorax and bronchoscopy established the diagnosis of a right-sided aortic arch resulting intracheobronchial compression and tracheomalacia. [Indian J Chest Dis Allied Sci 2012;54:45-47]
Key words: Tracheomalacia, Exertional dyspnoea, Variable intrathoracic airway obstruction, Right side aortic arch.
[Received: Feburary 23, 2011; accepted after revision: June 27, 2011]
Correspondence and reprint requests: Dr M.L. Gupta, 1/635, Vidhyadhar Nagar, Jaipur-302 023 (Rajasthan), India;Phone: 91-141-2236280, 2236563; E-mail: [email protected]
INTRODUCTION
Right-sided aortic arch with an aberrant origin ofgreat vessels is a rare, but well recognised cause oftracheobronchial/oesophageal compression ininfants and children. Such an anomaly is usuallyassociated with some or other congenital cardiacdefect(s) also. We encountered tracheobronchialcompression secondary to a right-sided aortic arch ina middle-aged male who did not have otheranomalies, such as, vascular ring, aberrant origin ofgreat vessels, or congenital cardiac defect(s).Considering its rarity of occurrence and similarity ofpresentation of this condition with other commonrespiratory disorders, this case is being reported.
CASE REPORT
A 55-year-old, non-smoker male presented withprogressive exertional dyspnoea for the last fouryears. Patient denied any history of fever,expectoration, haemoptysis, and/or chest pain.Patient had received inhaled corticosteroids, short-acting/long-acting beta-2 agonists with oralcorticosteroids on few occasions during this period.None of these measures resulted in a significant reliefin his symptoms.
Vital signs and general physical examination werewithin normal limits. Chest was barrel shaped withbilateral expiratory wheezing. Cardiac andabdominal examination were normal.
Routine blood counts, serum biochemistry andurine analysis were within normal limits. Arterialblood gas analysis (on room air) showed partialpressure of arterial oxygen: 68 mmHg; partialpressure of arterial carbon dioxide: 23.6 mm Hg;pH: 7.46; bicarbonate: 18.8 meq/L suggestive ofcompensated respiratory alkalosis. Chestradiograph postero-anterior view (Figure 1) showedabsence of left aortic knuckle and narrowing of lowertracheal air column from the level of clavicledownwards. Both the lung fields showed evidence ofover-inflation. Electrocardiogram and twodimensional echocardiography were within normallimits.
Figure 1. Chest radiograph (postero-anterior view) showing(A) absent left aortic knuckle shadow and narrowing oflower tracheal air column; and (B) left-sided aortic arch andnormal tracheal lucency in a healthy adult.
A B
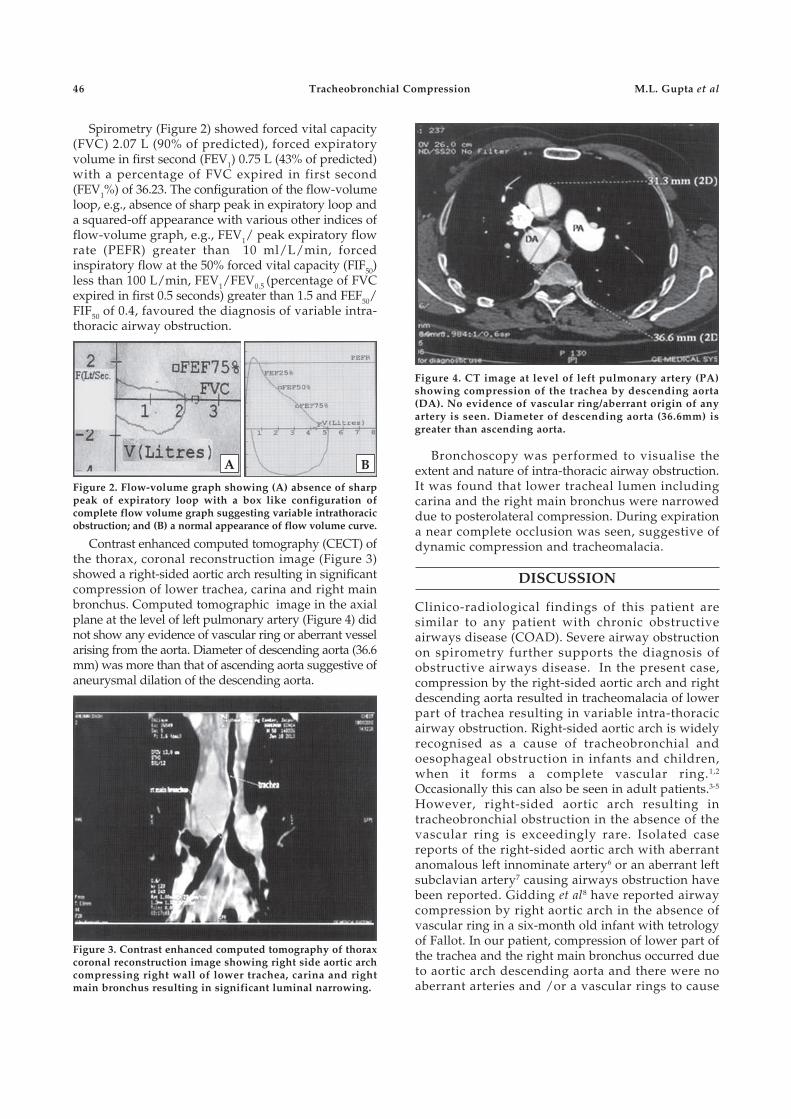
46
Spirometry (Figure 2) showed forced vital capacity(FVC) 2.07 L (90% of predicted), forced expiratoryvolume in first second (FEV1) 0.75 L (43% of predicted)with a percentage of FVC expired in first second(FEV1%) of 36.23. The configuration of the flow-volumeloop, e.g., absence of sharp peak in expiratory loop anda squared-off appearance with various other indices offlow-volume graph, e.g., FEV1/ peak expiratory flowrate (PEFR) greater than 10 ml/L/min, forcedinspiratory flow at the 50% forced vital capacity (FIF50)less than 100 L/min, FEV1/FEV0.5 (percentage of FVCexpired in first 0.5 seconds) greater than 1.5 and FEF50/FIF50 of 0.4, favoured the diagnosis of variable intra-thoracic airway obstruction.
Bronchoscopy was performed to visualise theextent and nature of intra-thoracic airway obstruction.It was found that lower tracheal lumen includingcarina and the right main bronchus were narroweddue to posterolateral compression. During expirationa near complete occlusion was seen, suggestive ofdynamic compression and tracheomalacia.
DISCUSSION
Clinico-radiological findings of this patient aresimilar to any patient with chronic obstructiveairways disease (COAD). Severe airway obstructionon spirometry further supports the diagnosis ofobstructive airways disease. In the present case,compression by the right-sided aortic arch and rightdescending aorta resulted in tracheomalacia of lowerpart of trachea resulting in variable intra-thoracicairway obstruction. Right-sided aortic arch is widelyrecognised as a cause of tracheobronchial andoesophageal obstruction in infants and children,when it forms a complete vascular ring.1,2
Occasionally this can also be seen in adult patients.3-5
However, right-sided aortic arch resulting intracheobronchial obstruction in the absence of thevascular ring is exceedingly rare. Isolated casereports of the right-sided aortic arch with aberrantanomalous left innominate artery6 or an aberrant leftsubclavian artery7 causing airways obstruction havebeen reported. Gidding et al8 have reported airwaycompression by right aortic arch in the absence ofvascular ring in a six-month old infant with tetrologyof Fallot. In our patient, compression of lower part ofthe trachea and the right main bronchus occurred dueto aortic arch descending aorta and there were noaberrant arteries and /or a vascular rings to cause
Tracheobronchial Compression M.L. Gupta et al
A B
Figure 2. Flow-volume graph showing (A) absence of sharppeak of expiratory loop with a box like configuration ofcomplete flow volume graph suggesting variable intrathoracicobstruction; and (B) a normal appearance of flow volume curve.
Contrast enhanced computed tomography (CECT) ofthe thorax, coronal reconstruction image (Figure 3)showed a right-sided aortic arch resulting in significantcompression of lower trachea, carina and right mainbronchus. Computed tomographic image in the axialplane at the level of left pulmonary artery (Figure 4) didnot show any evidence of vascular ring or aberrant vesselarising from the aorta. Diameter of descending aorta (36.6mm) was more than that of ascending aorta suggestive ofaneurysmal dilation of the descending aorta.
Figure 3. Contrast enhanced computed tomography of thoraxcoronal reconstruction image showing right side aortic archcompressing right wall of lower trachea, carina and rightmain bronchus resulting in significant luminal narrowing.
Figure 4. CT image at level of left pulmonary artery (PA)showing compression of the trachea by descending aorta(DA). No evidence of vascular ring/aberrant origin of anyartery is seen. Diameter of descending aorta (36.6mm) isgreater than ascending aorta.

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 47
airways obstruction. This case highlights the need forcritical analysis of chest radiograph and flow-volumecurve in a patient presenting with exertionaldyspnoea. Diagnosis of COAD should not beconsidered on volume-time graph alone. A carefulanalysis of both volume-time graph and flow-volumecurve are needed to exclude intra-thoracic airwayobstruction mimicking COAD.
To the best of our knowledge, this is the first case of its kinddocumenting a right-sided aortic arch without vascularring as a cause of airways compression in a middle-aged patient. Possible mechanisms of delayed onset ofsymptoms in our patient include atheroscleroticchanges in vessel with advancing age5 and progressivetracheomalacia due to prolonged compression.8
REFERENCES
1. Bakker DA, Berger RM, Witsenburg M, Bogers AJ.Vascular rings: a rare cause of common respiratorysymptoms. Acta Paediatr 1999;88:947-52.
2. Stewart JR, Kincaid OW, Titus Jl. Right aortic arch: plainfilm diagnosis and significance. Am J Roentgenol RadiumTher Nucl Med 1966;97:377-89.
3. Greiner A, Perkmann R, Rieger M, Neuhauser B, FraedrichG. Vascular ring causing tracheal compression in an adultpatient. Ann Thorac Surg 2003;75:1959-60.
4. Winn RA, Chan ED, Langmack EL, Kotaru C, Aronsen C.Dysphagia, chest pain and refractory asthma in a 42-year-old woman. Chest 2004;126:1694-7.
5. Ko Y-K, Hsiao C-L, Lee Y-J. Right aortic arch with acomplete vascular ring causing tracheoesophagealcompression. J Intern Med Taiwan 2007;18:104-7.
6. Gross RE, Neuhauser EB. Compression of the trachea byan anomalous innominate artery: an operation for itsrelief. Am J Dis Child 1948;75:570-4.
7. Edwards JR. Congenital cardiovascular causes oftracheobronchial and/or esophageal obstruction. In:Tucker BL, Lindesmith GG, eds First Clinical Conference onCongenital Heart Disease. New York: Grune and Stratton;1979:p.49-95.
8. Gidding SS, Beekman RH, Lebowitz E, Wesley J, Coran A,Behrendt D, et al. Airways compression by a right aorticarch in the absence of a vascular ring. Chest 1984;85:703-5.

The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.5448
NATIONAL COLLEGE OF CHEST PHYSICIANS (INDIA)
Fellowship/Membership Fee
Membership (Annual) : T 500.00Membership (Life) : T 5000.00Fellowship : T 5000.00Enrolement (new members only) : T 1000.00
Payments should be made by Cheque/Demand Draft, drawn in favour of theSecretary, National College of Chest Physicians (I). Please add T75/- to all out-station cheques.
Annual membership is valid for one financial year (April-March) only.
Sd/-Secretary
NATIONAL COLLEGE OF CHEST PHYSICIANS (INDIA)
Fellows and Members of the College are requested to mention their oldaddress also while informing for change of address alongwith their Fellowship/Membership number to the Secretary, NCCP (I) and/or to PublicationDepartment, IJCDAS to avoid any mistake/delay in mailing the Journal'scopy as well as College's information.
Sd/-Secretary

Case Report
Giant Solitary Fibrous Tumour of the Pleura
Rajaram Burrah1, K.V. Veerendra1, V. Deshmane1, Rama Rao C2, S. Althaf1, S. Pingali1,A.D. Shah2 and Y. Srinivasalu1
Departments of Surgical Oncology1 and Pathology2, Kidwai Memorial Institute of Oncology, Bengaluru, Karnataka,India
ABSTRACT
Solitary fibrous tumour of the pleura is a rare primary pleural neoplasm. These tumours are usually asymptomatic andare incidentally detected. Majority of these neoplasms are benign and surgical excision provides excellent results. With thewidespread use of imaging and better diagnostic criteria, this tumour is likely to be detected more frequently. Weencountered a patient with a giant solitary fibrous tumour of the pleura. In this report, we describe the case of a patientwith a giant solitary fibrous tumour of the pleura, review the literature and present the details of management of thispatient. [Indian J Chest Dis Allied Sci 2012;54:49-52]
Key words: Pleural, Localised mesothelioma, Solitary fibrous tumour.
[Received: March 14, 2011; accepted after revision: July 18, 2011]
Correspondence and reprint requests: Dr Veerendra Kumar KV, Department of Surgical Oncology, Kidwai MemorialInstitute of Oncology, Bengaluru-560 029 (Karnataka), India; Phone: 91-80-6560723; E-mail: [email protected];[email protected]
INTRODUCTION
Solitary fibrous tumours of the pleura (SFTP) are rareneoplasms of mesenchymal origin. Most of thetumours are slow growing, benign, pedunculatedand arise from the visceral pleura.1 Most of thepatients are asymptomatic and the presence of thetumour is usually incidentally detected. Though thenumber of cases reported is limited, it appears thatsurgical excision provides good results.2 We presentour experience with a giant SFTP, outline ourmanagement and review the literature.
CASE REPORT
A 39-year-old female presented with a swelling in herneck. She was diagnosed to have a diffuse colloidgoiter. However, during work-up, her chestradiograph showed a large mass lesion in the rightchest. She was referred to our institute for furtherinvestigation and management.
On evaluation, the patient had no respiratorysymptoms or significant past illness. She had nopallor, clubbing, pedal oedema or lymphadenopathy.Respiratory examination revealed dullness in the rightlower hemithorax with decreased air entry.Haemogram and liver function tests were normal.Sputum examination for acid-fast bacilli was negative.The chest radiograph (Figure 1) showed a largehomogeneous mass lesion in the right lower zone.
Figure 1. Chest radiograph (postero-anterior view) showinga mass in the right hemithorax.
Contrast enhanced computed tomography of thethorax showed a large mass (24cm x 14cm) in theright mid and the lower hemithorax. The massappeared heterogeneous, lobulated and had a broadbase towards the pleura, and with contrastenhancement suggesting that it had increased
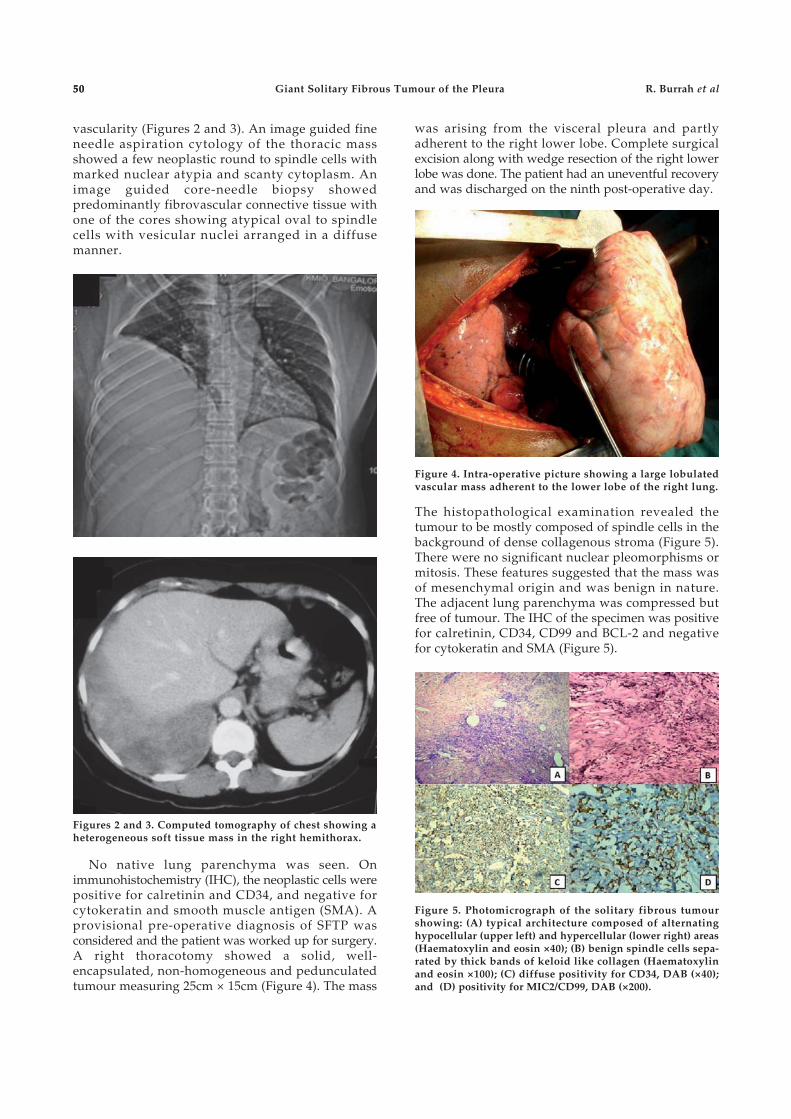
5050
vascularity (Figures 2 and 3). An image guided fineneedle aspiration cytology of the thoracic massshowed a few neoplastic round to spindle cells withmarked nuclear atypia and scanty cytoplasm. Animage guided core-needle biopsy showedpredominantly fibrovascular connective tissue withone of the cores showing atypical oval to spindlecells with vesicular nuclei arranged in a diffusemanner.
Giant Solitary Fibrous Tumour of the Pleura R. Burrah et al
was arising from the visceral pleura and partlyadherent to the right lower lobe. Complete surgicalexcision along with wedge resection of the right lowerlobe was done. The patient had an uneventful recoveryand was discharged on the ninth post-operative day.
Figures 2 and 3. Computed tomography of chest showing aheterogeneous soft tissue mass in the right hemithorax.
No native lung parenchyma was seen. Onimmunohistochemistry (IHC), the neoplastic cells werepositive for calretinin and CD34, and negative forcytokeratin and smooth muscle antigen (SMA). Aprovisional pre-operative diagnosis of SFTP wasconsidered and the patient was worked up for surgery.A right thoracotomy showed a solid, well-encapsulated, non-homogeneous and pedunculatedtumour measuring 25cm × 15cm (Figure 4). The mass
Figure 4. Intra-operative picture showing a large lobulatedvascular mass adherent to the lower lobe of the right lung.
The histopathological examination revealed thetumour to be mostly composed of spindle cells in thebackground of dense collagenous stroma (Figure 5).There were no significant nuclear pleomorphisms ormitosis. These features suggested that the mass wasof mesenchymal origin and was benign in nature.The adjacent lung parenchyma was compressed butfree of tumour. The IHC of the specimen was positivefor calretinin, CD34, CD99 and BCL-2 and negativefor cytokeratin and SMA (Figure 5).
Figure 5. Photomicrograph of the solitary fibrous tumourshowing: (A) typical architecture composed of alternatinghypocellular (upper left) and hypercellular (lower right) areas(Haematoxylin and eosin ×40); (B) benign spindle cells sepa-rated by thick bands of keloid like collagen (Haematoxylinand eosin ×100); (C) diffuse positivity for CD34, DAB (×40);and (D) positivity for MIC2/CD99, DAB (×200).
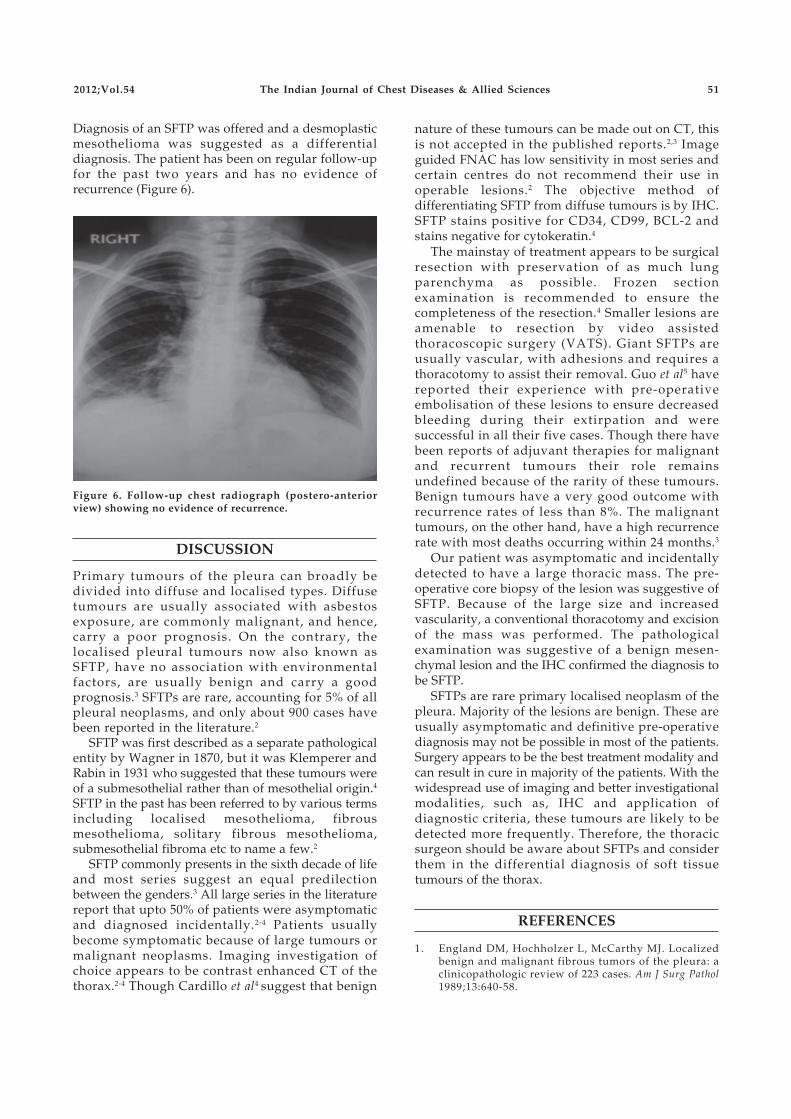
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 51
Diagnosis of an SFTP was offered and a desmoplasticmesothelioma was suggested as a differentialdiagnosis. The patient has been on regular follow-upfor the past two years and has no evidence ofrecurrence (Figure 6).
nature of these tumours can be made out on CT, thisis not accepted in the published reports.2,3 Imageguided FNAC has low sensitivity in most series andcertain centres do not recommend their use inoperable lesions.2 The objective method ofdifferentiating SFTP from diffuse tumours is by IHC.SFTP stains positive for CD34, CD99, BCL-2 andstains negative for cytokeratin.4
The mainstay of treatment appears to be surgicalresection with preservation of as much lungparenchyma as possible. Frozen sectionexamination is recommended to ensure thecompleteness of the resection.4 Smaller lesions areamenable to resection by video assistedthoracoscopic surgery (VATS). Giant SFTPs areusually vascular, with adhesions and requires athoracotomy to assist their removal. Guo et al5 havereported their experience with pre-operativeembolisation of these lesions to ensure decreasedbleeding during their extirpation and weresuccessful in all their five cases. Though there havebeen reports of adjuvant therapies for malignantand recurrent tumours their role remainsundefined because of the rarity of these tumours.Benign tumours have a very good outcome withrecurrence rates of less than 8%. The malignanttumours, on the other hand, have a high recurrencerate with most deaths occurring within 24 months.3
Our patient was asymptomatic and incidentallydetected to have a large thoracic mass. The pre-operative core biopsy of the lesion was suggestive ofSFTP. Because of the large size and increasedvascularity, a conventional thoracotomy and excisionof the mass was performed. The pathologicalexamination was suggestive of a benign mesen-chymal lesion and the IHC confirmed the diagnosis tobe SFTP.
SFTPs are rare primary localised neoplasm of thepleura. Majority of the lesions are benign. These areusually asymptomatic and definitive pre-operativediagnosis may not be possible in most of the patients.Surgery appears to be the best treatment modality andcan result in cure in majority of the patients. With thewidespread use of imaging and better investigationalmodalities, such as, IHC and application ofdiagnostic criteria, these tumours are likely to bedetected more frequently. Therefore, the thoracicsurgeon should be aware about SFTPs and considerthem in the differential diagnosis of soft tissuetumours of the thorax.
REFERENCES
1. England DM, Hochholzer L, McCarthy MJ. Localizedbenign and malignant fibrous tumors of the pleura: aclinicopathologic review of 223 cases. Am J Surg Pathol1989;13:640-58.
Figure 6. Follow-up chest radiograph (postero-anteriorview) showing no evidence of recurrence.
DISCUSSION
Primary tumours of the pleura can broadly bedivided into diffuse and localised types. Diffusetumours are usually associated with asbestosexposure, are commonly malignant, and hence,carry a poor prognosis. On the contrary, thelocalised pleural tumours now also known asSFTP, have no association with environmentalfactors, are usually benign and carry a goodprognosis.3 SFTPs are rare, accounting for 5% of allpleural neoplasms, and only about 900 cases havebeen reported in the literature.2
SFTP was first described as a separate pathologicalentity by Wagner in 1870, but it was Klemperer andRabin in 1931 who suggested that these tumours wereof a submesothelial rather than of mesothelial origin.4
SFTP in the past has been referred to by various termsincluding localised mesothelioma, fibrousmesothelioma, solitary fibrous mesothelioma,submesothelial fibroma etc to name a few.2
SFTP commonly presents in the sixth decade of lifeand most series suggest an equal predilectionbetween the genders.3 All large series in the literaturereport that upto 50% of patients were asymptomaticand diagnosed incidentally.2-4 Patients usuallybecome symptomatic because of large tumours ormalignant neoplasms. Imaging investigation ofchoice appears to be contrast enhanced CT of thethorax.2-4 Though Cardillo et al4 suggest that benign

52
2. Harrison-Phipps KM, Nichols FC, Schleck CD,Deschamps C, Cassivi SD, Schipper PH, et al. Solitaryfibrous tumors of the pleura: results of surgical treatmentand long-term prognosis. J Thorac Cardiovasc Surg 2009;138:19-25.
3. Robinson LA. Solitary fibrous tumor of the pleura. CancerControl 2006;13:264-9.
4. Cardillo G, Carbone L, Carleo F, Masala N, Graziano P,Bray A, et al. Solitary fibrous tumors of the pleura: ananalysis of 110 patients treated in a single institution. AnnThorac Surg 2009;88:1632-7.
5. Guo J, Chu X, Sun YE, Zhang L, Zhou N. Giant solitaryfibrous tumor of the pleura: an analysis of five patients.World J Surg 2010;34:2553-7.
Giant Solitary Fibrous Tumour of the Pleura R. Burrah et al

Case Report
Pulmonary Disease due to Mycobacterium massiliense
Subhra Mitra1, S. Roy Tapadar1, D. Banerjee1, S. Bhattacharjee2, Sunanda Dey3 and S. Kundu2
Department of Respiratory Medicine, Midnapore Medical College and Hospital1, Institute of Postgraduate MedicalEducation and Research2 and Super Religare Laboratories Limited3, Kolkata, West Bengal, India
ABSTRACT
We report a case of a patient suffering from multidrug-resistant pulmonary tuberculosis (MDR-PTB) who later developedan invasive infection of the respiratory tract with a rapidly growing non-tuberculous mycobacteria (NTM), recently identifiedas Mycobacterium massiliense, closely related to M. abscessus. To the best of our knowledge, this is the first case of M. massilienseinfection being reported from India. [Indian J Chest Dis Allied Sci 2011;53:53-57]
Key words: Mycobacterium massiliense, Non-tuberculous mycobacteria, Rapidly growing mycobacteria.
[Received: May 18, 2011; accepted after revision: September 8, 2011]
Correspondence and reprint requests: Dr Subhra Mitra, 603 Auroville, 10 Mandeville Gardens, Kolkata-700 019 (WestBengal), India; Phone: 91-033-24604465; E-mail: [email protected]
INTRODUCTION
Mycobacterium massiliense, a newly-described speciesof rapidly growing mycobacteria (RGM), is closelyrelated to the Mycobacterium chelonae–Mycobacteriumabscessus group.1 First identified by Adekambi et al,1
the name pertaining to Massilia, the Latin name ofMarseille, where the organism was isolated. Since itsfirst recovery from lung secretions in 2004,1 it hasbeen isolated from blood,2,3 intramuscular injectionsites4 and surgical wounds.2,5 It has been implicatedas an invasive pathogen, a claim also supported by itsclose relation to M. abscessus, a known pulmonarypathogen.
CASE REPORT
A 60-year-old woman presented with a 10-yearhistory of cough and mucoid/ mucopurulent sputumalong with occasional haemoptysis. Shortness ofbreath had developed over the last two years. Shereceived anti-tuberculosis treatment (ATT) in variouscourses in 2000, 2002 and 2003. She stayed in aSanatorium from November 2004 to November 2006where she was empirically treated with second-lineanti-tuberculosis drugs.
Past history showed sputum-smear positive foracid-fast bacilli (AFB) in 2000, 2002, 2003 and 2004and culture for Mycobacterium tuberculosis positive in2002 and 2003. Details of mycobaterial isolation andtreatments are presented in table 1. From January2007 onwards, she was managed in our hospital.
This time, she was again found to be sputum-smearpositive and culture positive for M. tuberculosis by
BACTEC 460 TB method. Drug sensitivity testingshowed the growth to be resistant to rifampicin,isoniazid and pyrazinamide. She was prescribedinjection kanamycin, together with ofloxacin,ethionamide, ethambutol, cycloserine and PASaccording to the drug susceptibility report and wasadmitted for the initial period of therapy. She wasfound culture negative for M. tuberculosis in September2007. Kanamycin was stopped after eight months oftherapy and oral anti-tuberculosis drugs werecontinued. She remained sputum-smear negative forAFB, attended the outpatients less regularly butreportedly continued her anti-tuberculosis drugs.
A re-evaluation in April 2009, prompted byrecurrent symptoms, found her to be sputum-smearpositive for AFB on two occasions. Culture forM. tuberculosis by the BACTEC 460 radioactivemethod grew non-tuberculous mycobacteria (NTM).Mycobacterium speciation by deoxyribonucleic acid(DNA) sequencing yielded Mycobacterium massiliense.Anti-tuberculosis drugs were stopped (her last anti-tuberculosis drugs course ran for two years and twomonths) and she was kept under observation. Sheremained sputum-smear positive for AFB and asputum culture for mycobacteria grew NTM again inNovember 2009.
A repeat culture in April 2010 by BACTEC MGIT960 (Fluorescent technology) grew RGM andMycobacterium speciation yielded M. massiliense.This time a drug sensitivity study was done (Table2). BACTEC drug susceptibility for M. tuberculosiswas determined by following the modifiedproportion method. The critical proportion forresistance was taken as 1% for all the anti-tuberculosis drugs.

54
The identification of isolate as NTM in April 2009was done by BACTEC 460 and PNB method(sensitive/resistant to p-nitrobenzoic acid).Speciation of NTM was done by DNA sequencingutilising 16S rRNA6,7 and hsp658 gene targets, and thebacteria was identified as Mycobacterium massiliense.Routine susceptibility testing for treatment of RGM isrecommended.9
Drug susceptibility of NTM (Table 2) was done bybroth microdilution method (MIC testing).Susceptibility testing and subsequent resultinterpretations are as per CLSI guidelines M24-Aa.10
There was a weight loss of 10 Kg since the start ofher illness. Her nutritional status was poor with abody mass index of 10 (weight 24 Kg). She was paleand had clubbing with bilateral, scattered, coarse,mid-to-late inspiratory crackles on chest examination.On investigation, haemoglobin was 10.9 g/dL anderythrocyte sedimentation rate was 22mm in the firsthour and white blood cell count was 7900/mm3.Blood sugar, urea, serum creatinine, liver functionand thyroid function tests were in the normal range.Serology for human immunodeficiency virus (HIV)was negative and CD4+ count was 253/mL.
Mycobacterium massiliense Pulmonary Disease Subhra Mitra et al
Table 1. Summary of isolations of acid-fast bacilli and treatments given
Period Positive Positive Cultures** NTM TreatmentSmears* Identification
MTB NTM
Drugs Start of DurationTreatment
2000–2001 2/3 ND R, H, E ~6 months
2002 2/3 1/1 H,E,Ofx April 2002 ~10 months
2003 2/3 1/1 S,R,H,Z,E, March 2003 ~ 2 monthsR,H,Z,E ~ 6 months
2004–2006 18/24 0/1 Am, Z, E, Ofx, Eto November 2004 ~6 months(sanatorium) Ofx, E, Eto ~18 months
2007–2008 12/26 1/2 Km, Ofx, Eto, E, February 2007 ~8 months(our department) (DST done) PAS, Cs
Ofx, Cs November 2007 ~18 monthsE, Eto, PAS
April 2009 3/3 1/1 M. massiliense None
November 2009 3/3 1/1 ND None
April 2010 2/2 1/1 M. massiliense None
June–July 2010 2/2 DST done Am, Do, Ofx, Clr July 2010 ~1 month
August 2010 0/10 Do, Ofx, Clr August 2010 ~ 8 monthMarch 2011
*=Positive smears/smears done; **=positive culture / cultures done; ND=Not doneMTB=Mycobacterium tuberculosis, NTM=Non-tuberculosis mycobacteria; DST=Drug sensitivity testing; R=Rifampicin; H=Isoniazid; E=Ethambutol;Ofx=Ofloxacin; S=Streptomycin; Z=Pyrazinamide; Am=Amikacin; Eto=Ethionamide; Km=Kanamycin; PAS=Para-aminosalycylic acid;Cs=Cycloserine; Do=Doxycycline; Clr=Clarithromycin
Table 2. Antimicrobial drug resistance pattern of the isolated strain of Mycobacterium massiliense
Drug MIC (mcg/mL) Pattern
Trimethoprin/sulfamethoxazole 0.25/4.75 Susceptible
Ciprofloxacin 0.12 Susceptible
Moxifloxacin 0.25 Susceptible
Cefoxitin 4 Susceptible
Amikacin 1 Susceptible
Doxycycline 0.12 Susceptible
Clarithromycin 0.06 Susceptible
Linezolid 1 Susceptible
Imipenem 2 Susceptible
Cefepime 1 Susceptible
Amoxicillin/clavulanic acid 2:1 ratio 2/1 Susceptible
Ceftriaxone 4 Susceptible
Minocycline 1 Susceptible
Tobramycin 1 Susceptible
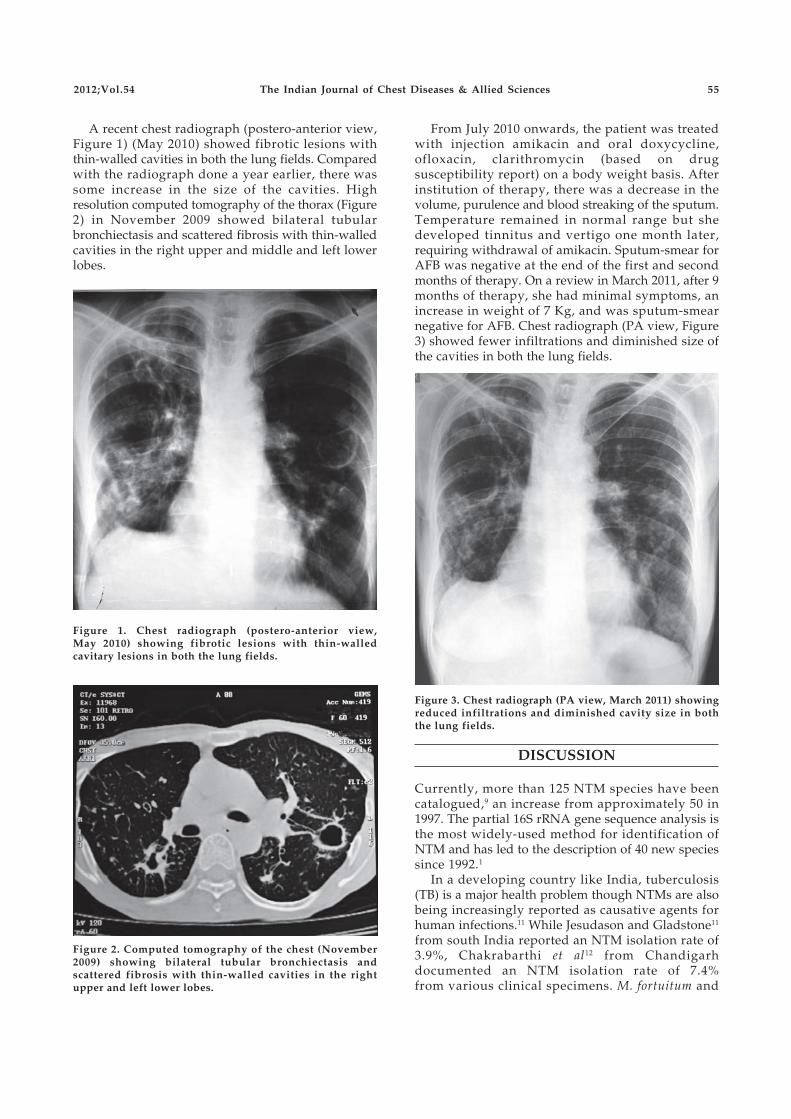
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 55
A recent chest radiograph (postero-anterior view,Figure 1) (May 2010) showed fibrotic lesions withthin-walled cavities in both the lung fields. Comparedwith the radiograph done a year earlier, there wassome increase in the size of the cavities. Highresolution computed tomography of the thorax (Figure2) in November 2009 showed bilateral tubularbronchiectasis and scattered fibrosis with thin-walledcavities in the right upper and middle and left lowerlobes.
From July 2010 onwards, the patient was treatedwith injection amikacin and oral doxycycline,ofloxacin, clarithromycin (based on drugsusceptibility report) on a body weight basis. Afterinstitution of therapy, there was a decrease in thevolume, purulence and blood streaking of the sputum.Temperature remained in normal range but shedeveloped tinnitus and vertigo one month later,requiring withdrawal of amikacin. Sputum-smear forAFB was negative at the end of the first and secondmonths of therapy. On a review in March 2011, after 9months of therapy, she had minimal symptoms, anincrease in weight of 7 Kg, and was sputum-smearnegative for AFB. Chest radiograph (PA view, Figure3) showed fewer infiltrations and diminished size ofthe cavities in both the lung fields.
Figure 1. Chest radiograph (postero-anterior view,May 2010) showing fibrotic lesions with thin-walledcavitary lesions in both the lung fields.
Figure 2. Computed tomography of the chest (November2009) showing bilateral tubular bronchiectasis andscattered fibrosis with thin-walled cavities in the rightupper and left lower lobes.
Figure 3. Chest radiograph (PA view, March 2011) showingreduced infiltrations and diminished cavity size in boththe lung fields.
DISCUSSION
Currently, more than 125 NTM species have beencatalogued,9 an increase from approximately 50 in1997. The partial 16S rRNA gene sequence analysis isthe most widely-used method for identification ofNTM and has led to the description of 40 new speciessince 1992.1
In a developing country like India, tuberculosis(TB) is a major health problem though NTMs are alsobeing increasingly reported as causative agents forhuman infections.11 While Jesudason and Gladstone11
from south India reported an NTM isolation rate of3.9%, Chakrabarthi et al12 from Chandigarhdocumented an NTM isolation rate of 7.4%from various clinical specimens. M. fortuitum and

56 Mycobacterium massiliense Pulmonary Disease Subhra Mitra et al56
M. chelonae were the commonest isolates in thesestudies.
Chronic pulmonary disease is the most commonclinical manifestation of NTM and it reflects the formof disease and co-morbidities rather than the speciesof NTM involved.13 Our patient, an elderly thin-builtwoman, had prior TB, bronchiectasis and possiblygastro-oesophageal reflux disease as facilitating co-morbidities and presented clinico-radiologically aschronic pulmonary TB.
The radiographic features of NTM may beprimarily fibrocavitary, similar to pulmonary TB, orcharacterised by nodules and bronchiectasis.8 Thecavities are thin-walled with greater pleural reactionand lesser surrounding parenchymal opacities thanthat seen in classic pulmonary TB.9,13
Isolation of NTM in culture is essential for thediagnosis of NTM lung disease. However, since theNTM are ubiquitous and may contaminaterespiratory specimens, two or more positive cultureresults for NTM from separate expectorated sputumsamples are required to make the microbiologicdiagnosis clinically significant as per the AmericanThoracic Society guidelines.9 In our patient, sputumculture was thrice positive for NTM and DNAspeciation done twice yielded M. massiliense.
Colonisation without infection (i.e., no tissueinvasion) is an unproven condition for NTM,9 somepreferring the term ‘indolent disease’ in that it maynot be evident that NTM are causing progressivedisease unless the patient is followed up for severalyears. The significance of NTM isolation from apatient during therapy for pulmonary TB isuncertain.9 Co-existence of M. tuberculosis and NTMhas been reported in both HIV-1 infected and non-infected patients.14 In these situations NTM may bepresent only as a saprophyte (coloniser),14 but bothmay also simultaneously cause disease requiringspecific treatments for the two mycobacteria.15
Persistent symptoms with repeated isolation of thesame pathogenic NTM species from respiratoryspecimens and progressive radiologic changessuggested disease rather than colonisation,16
prompting us to treat our patient after a year ofobservation.
Rapidly growing mycobacteria are uniformlyresistant to the “standard” anti-tuberculosis drugsand antibiotic susceptibility testing is, therefore,recommended for all clinically significant isolates.The treatment of the present patient was based on thedrug-susceptibility report.
Koh et al17 compared the clinical features andtreatment outcomes between patients with M.abscessus and those with M. massiliense lung disease.The clinical and radiographic manifestations ofdisease caused by both species were similar. Responserates to combination antibiotic therapy including
clarithromycin were higher in patients with M.massiliense than in those with M. abscessus lungdisease.17 Inducible resistance to clarithromycin foundin M. abscessus isolates may explain this lack ofefficacy.17
In our patient, sputum-smear conversion occurredafter one month of therapy and has remainednegative at eight months follow-up with a significantclinico-radiologic improvement.
Non-tuberculosis mycobacteria may be an under-recognised cause of AFB sputum positivity, especiallyin patients who have received treatment several timesor have developed MDR-TB.
ACKNOWLEDGEMENTS
Authors are thankful for the assistance provided by Dr B.R.Das, Executive Director, Research and Development, and HeadMolecular Diagnostics, Religare SRL Diagnostics, Mumbai andDr Vidya Nerurkar, Senior Microbiologist, Religare SRLDiagnostics, Mumbai.
REFERENCES
1. Adékambi T, Reynaud-Gaubert M, Greub G, GevaudanMJ, La Scola B, Raoult D, et al. Amoebal coculture of“Mycobacterium massiliense” sp. nov. from the sputumof a patient with hemoptoic pneumonia. J Clin Microbiol2004;42:5493-501.
2. Simmon KE, Pounder JI, Greene JN, Walsh F, AndersonCM, Cohen S, et al. Identification of an emergingpathogen, Mycobacterium massiliense, by rpoBsequencing of clinical isolates collected in the UnitedStates. J Clin Microbiol 2007;45:1978-80.
3. Tortoli E, Gabini R, Galanti I, Mariottini A. LethalMycobacterium massiliense sepsis, Italy (Letter to theEditor). Emerg Infect Dis 2008;14:984-5.
4. Kim HY, Yun YJ, Park CG, Lee BH, Cho YK, Park BJ, et al.Outbreak of Mycobacterium massiliense infectionassociated with intramuscular injections. J Clin Microbiol2007;45:3127-30.
5. Viana-Niero C, Lima KV, Lopes ML, da Silva RabelloMC, Marsola LR, Brilhante VC, et al. Molecularcharacterization of Mycobacterium massiliense andMycobacterium bolletii in outbreaks of infections afterlaparoscopic surgeries and cosmetic procedures. J ClinMicrobiol 2008;46:850-5.
6. Shrestha NK, Tuohy MJ, Hall GS, Reischl U, Gordon SM,Gary W, et al. Detection and differentiation ofmycobacterium tuberculosis and nontuberculousmycobacterial isolates by real-time PCR. J Clin Microbiol2003;41:5121-6.
7. Park H, Jang H, Song E, Chang CL, Lee M, Jeong S, et al.Microbiology, detection and genotyping ofmycobacterium species from clinical isolates andspecimens by oligonucleotide array. J Clin Microbiol 2005;43:1782-8.
8. Telenti A, Marchesi F, Balz M, Bally F, Bottger E, Bodmer T.Rapidly growing mycobacteria to the species level bypolymerase chain reaction and restriction enzymeanalysis. J Clin Microbiol 1993;31:175-8.
9. American Thoracic Society/Infectious Disease Society ofAmerica. An official ATS/IDSA statement: diagnosis,
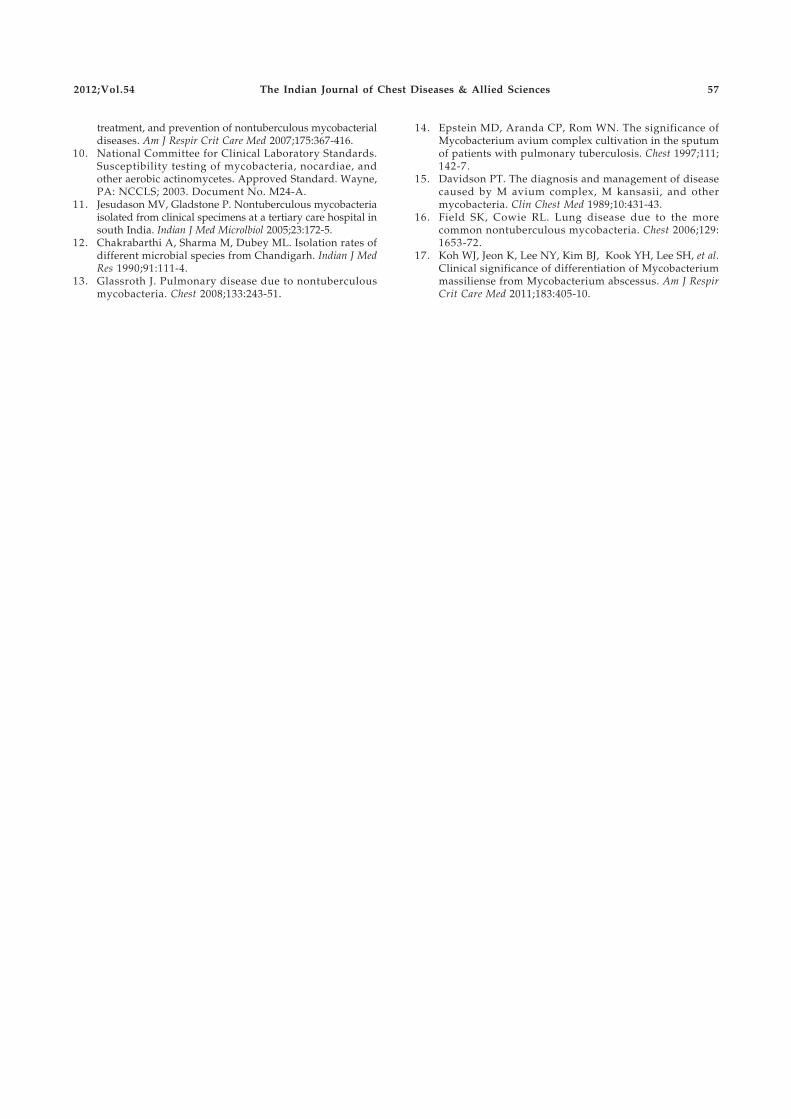
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 57
treatment, and prevention of nontuberculous mycobacterialdiseases. Am J Respir Crit Care Med 2007;175:367-416.
10. National Committee for Clinical Laboratory Standards.Susceptibility testing of mycobacteria, nocardiae, andother aerobic actinomycetes. Approved Standard. Wayne,PA: NCCLS; 2003. Document No. M24-A.
11. Jesudason MV, Gladstone P. Nontuberculous mycobacteriaisolated from clinical specimens at a tertiary care hospital insouth India. Indian J Med Microlbiol 2005;23:172-5.
12. Chakrabarthi A, Sharma M, Dubey ML. Isolation rates ofdifferent microbial species from Chandigarh. Indian J MedRes 1990;91:111-4.
13. Glassroth J. Pulmonary disease due to nontuberculousmycobacteria. Chest 2008;133:243-51.
14. Epstein MD, Aranda CP, Rom WN. The significance ofMycobacterium avium complex cultivation in the sputumof patients with pulmonary tuberculosis. Chest 1997;111;142-7.
15. Davidson PT. The diagnosis and management of diseasecaused by M avium complex, M kansasii, and othermycobacteria. Clin Chest Med 1989;10:431-43.
16. Field SK, Cowie RL. Lung disease due to the morecommon nontuberculous mycobacteria. Chest 2006;129:1653-72.
17. Koh WJ, Jeon K, Lee NY, Kim BJ, Kook YH, Lee SH, et al.Clinical significance of differentiation of Mycobacteriummassiliense from Mycobacterium abscessus. Am J RespirCrit Care Med 2011;183:405-10.
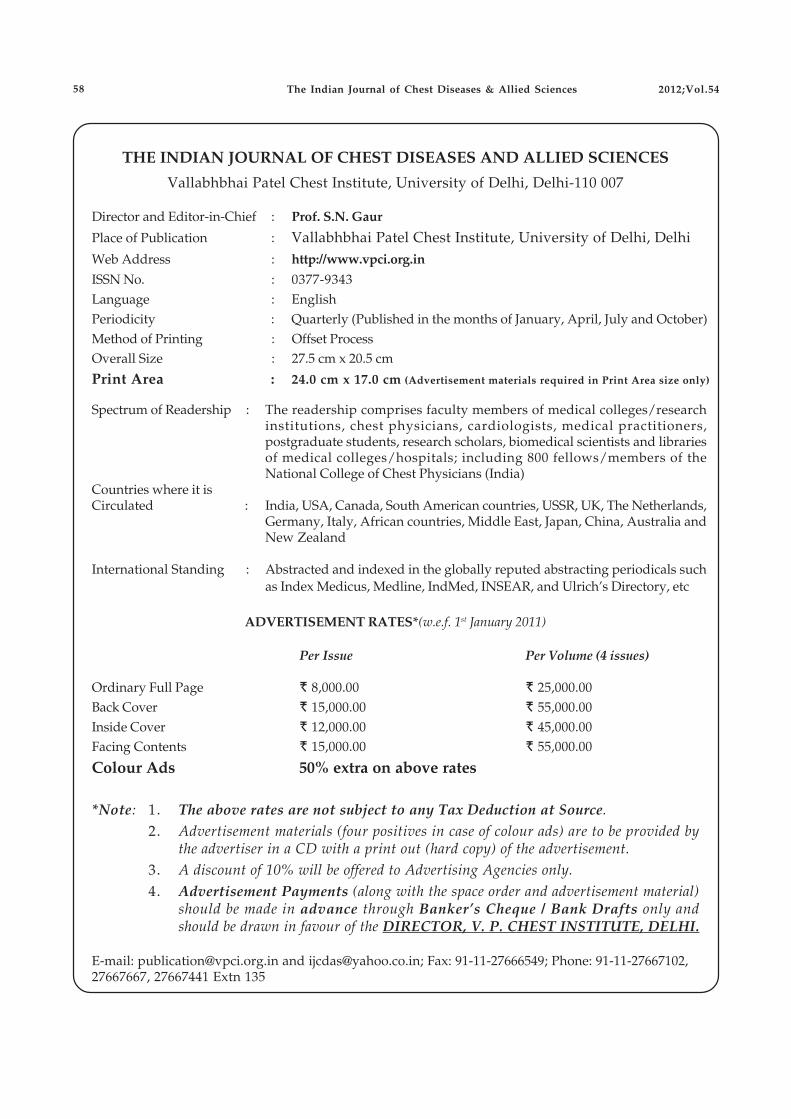
THE INDIAN JOURNAL OF CHEST DISEASES AND ALLIED SCIENCES
Vallabhbhai Patel Chest Institute, University of Delhi, Delhi-110 007
Director and Editor-in-Chief : Prof. S.N. Gaur
Place of Publication : Vallabhbhai Patel Chest Institute, University of Delhi, DelhiWeb Address : http://www.vpci.org.in
ISSN No. : 0377-9343Language : EnglishPeriodicity : Quarterly (Published in the months of January, April, July and October)Method of Printing : Offset ProcessOverall Size : 27.5 cm x 20.5 cm
Print Area : 24.0 cm x 17.0 cm (Advertisement materials required in Print Area size only)
Spectrum of Readership : The readership comprises faculty members of medical colleges/researchinstitutions, chest physicians, cardiologists, medical practitioners,postgraduate students, research scholars, biomedical scientists and librariesof medical colleges/hospitals; including 800 fellows/members of theNational College of Chest Physicians (India)
Countries where it isCirculated : India, USA, Canada, South American countries, USSR, UK, The Netherlands,
Germany, Italy, African countries, Middle East, Japan, China, Australia andNew Zealand
International Standing : Abstracted and indexed in the globally reputed abstracting periodicals suchas Index Medicus, Medline, IndMed, INSEAR, and Ulrich’s Directory, etc
ADVERTISEMENT RATES*(w.e.f. 1st January 2011)
Per Issue Per Volume (4 issues)
Ordinary Full Page R 8,000.00 R 25,000.00Back Cover R 15,000.00 R 55,000.00Inside Cover R 12,000.00 R 45,000.00Facing Contents R 15,000.00 R 55,000.00
Colour Ads 50% extra on above rates
*Note: 1. The above rates are not subject to any Tax Deduction at Source.2. Advertisement materials (four positives in case of colour ads) are to be provided by
the advertiser in a CD with a print out (hard copy) of the advertisement.3. A discount of 10% will be offered to Advertising Agencies only.4. Advertisement Payments (along with the space order and advertisement material)
should be made in advance through Banker’s Cheque / Bank Drafts only andshould be drawn in favour of the DIRECTOR, V. P. CHEST INSTITUTE, DELHI.
E-mail: [email protected] and [email protected]; Fax: 91-11-27666549; Phone: 91-11-27667102,27667667, 27667441 Extn 135
The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.5458

Short Communication
Regression Equations for Spirometry in Children Aged 6 to17 Years in Delhi Region
S.K. Chhabra1, V.K. Vijayan2, M. Rahman3, V. Mittal1 and P.D. Singh1
Departments of Cardio-respiratory Physiology1, Former Director2 and Biostatistics3, Viswanathan Chest Hospital,Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India
ABSTRACT
Background. Most of the studies carried out in India to develop regression equations for spirometry in children are nowseveral years-to-decades old and had used equipment and measurement protocols that have since changed. Predictionequations using the current standardisation protocols for spirometry are not available. The lung health of the populationmay have changed too.
Objective. To develop regression equations for spirometry for children aged 6 to 17 years of north Indian origin in Delhi region.
Methods. School children of north Indian origin, as determined by mother tongue and parentage, aged 6 to 17 years werescreened by a health questionnaire and physical examination and those found “normal” underwent spirometry accordingto the standardised procedure recommended by the American Thoracic Society/ European Respiratory Society (ATS/ERS)task force in 2005. Pearson’s correlation analysis was carried out to identify the predictor variables for spirometricparameters. Prediction equations were developed using the multiple linear regression procedure. The independent variableswere entered in sequence of height, age and weight. R2, adjusted R2 and R2 change, standard errors of the estimate (SEE),and estimates of regression coefficients were obtained and the goodness of fit was examined.
Results. Data was obtained in 365 boys and 305 girls. Forced vital capacity (FVC), forced expiratory volume in one second(FEV1), peak expiratory flow rate (PEFR), forced expiratory flow rate at 50% and 75% exhalation of vial capacity (F50 andF75) and mean forced expiratory flow rate over the middle 50% of the vital capacity (F25-75) showed moderate to strongcorrelations with age, height and weight in both boys and girls. In both genders, the equations explained very highvariability of FVC, FEV1 and PEFR as shown by the R2 values. The explained variability for flow rates was lesser, with thatfor F75 being the least.
Conclusions. Regression equations for spirometry variables for children of north Indian origin in Delhi region have beendeveloped. These represent the first such effort from India after the publication of the ATS/ERS task force 2005 guidelineson standardisation of spirometry. [Indian J Chest Dis Allied Sci 2012;54:59-63]
Key words: Pulmonary function, Spirometry, Normals, Children, Delhi, Regression equations.
[Received: September 5, 2011; accepted after revision: December 20, 2011]
Correspondence and reprint requests: Dr S.K. Chhabra, Professor and Head, Department of Cardio-respiratory Physiology,Vallabhbhai Patel Chest Institute, University of Delhi, Delhi - 110 007, India; E-mail: [email protected]
from age, weight and some other physicalmeasurements.
Technological advancements have resulted ingreater automation and newer methods of electronicmeasurements. The measurement protocols have beenrevised over time. The latest standardisation ofspirometry was carried out by a joint task force of theAmerican Thoracic Society and the EuropeanRespiratory Society (ATS/ERS) and published in theyear 2005.10 Most of the above Indian studies werecarried out several years-to-decades ago withequipment and measurement protocols that havechanged. Thus, these may no longer be valid. This islikely to affect interpretation of data. Correctinterpretation of pulmonary function data requires
INTRODUCTION
Pulmonary function is influenced by anthropometric,gender, environmental, genetic, socio-economic andtechnical factors. To predict pulmonary function,variations with anthropometric variables, sex andrace have been studied extensively and documentedin the western literature. A few studies from differentparts of India1-9 have provided information onpulmonary function in children and its determinantsand prediction equations have been described. Thestudies have varied in sample size, instrumentationand results. In general, boys have been found to havelarger vital capacities and height is the mostimportant determinant with variable contributions

60
use of locally developed prediction equations.Equations using the current standardisationprotocols for spirometry have not been developed inIndia. Ethnic variations in pulmonary function arewell known. This precludes development of a singleequation for all Indians. There is an urgent need todevelop these equations for different regions of thecountry. Delhi is a cosmopolitan city in the northernregion of the country. We, therefore, carried out astudy to develop regression equations for spirometryin children aged 6 to 17 years of north Indian originin Delhi region. We present here a briefcommunication of the study carried so that these canbe applied in practice at the earliest. A detailedevaluation and comparative analysis with previousIndian studies as well as with equations from othercountries will be presented subsequently.
MATERIAL AND METHODS
The study was approved by the Institutional EthicsCommittee. It was carried out in children in a schoolselected randomly from a list of schools in Delhi. Theschool caters to a wide area of Delhi and the childrenare drawn from a very wide socio-economicspectrum. Hence, it approximates a representativesample. All the children from ages 6 to 17 years wereeligible for inclusion provided they had been in Delhifor more than half of their life. Additionally, themother tongue was required to be Hindi, Urdu orPunjabi, the predominant languages in this region,and both parents had to be of north Indian origin tolimit the confounding effects of ethnic variation. Ademonstration of the testing procedure was given tofamiliarise the children with pulmonary functiontesting. For each age, a target of 15 to 20 boys and girlswith technically acceptable tests was set andconsecutive eligible children were included till thesample requirement was met. This number was basedon statistical considerations of numbers required forlinear regression procedures, previously publishedstudies1-9 and feasibility.
A questionnaire was designed in English andHindi was answered by either parent. It had severalsections as follows: cover letter from Principal,information sheet, consent form and questionnaireabout the health status. Children with completelyfilled-up questionnaires with written consent forparticipation were included. Those judged to be“normal” from the questionnaire responses wereagain examined by the investigators in the school toconfirm that they were eligible for inclusion. Theexclusion criteria included current or past history ofany chronic respiratory, cardiac or other systemdisease, thoracic cage abnormality, any current acuteillness, recent chest infection (within 6 weeks),current smokers or with environmental tobacco
smoke exposure, and unwilling parents/children.Age in completed years, gender, standing height to
the nearest centimeter without shoes and weightrounded off to the nearest kilogram were recorded atthe time of the testing. Weight was measured wearinglight clothing and no footwear to the nearest 0.5 Kgusing an electronic scale that was calibrated on aweekly basis with known weights. Height wasmeasured with the children standing erect with headin the Frankfurt plane and ankles pressed against awall on which a measuring tape had been fixed.
Spirometry was carried out in accordance with therecommendations of the ATS/ERS task force.10 Thespirometer with a heated Lily screen pneumotach(Medisoft Micro 5000, Belgium) was calibrated daily.The manoeuvers were performed in the sittingposition with a nose-clip applied. The children wasasked to inhale completely and rapidly with a pauseof <1 s at total lung capacity (TLC) and exhale withmaximum force until no more air was expelled outwhile maintaining an upright posture. At thecompletion of expiration and on signal from thetechnician, the subject was asked to inhalecompletely. The manoeuvers was monitored on thecomputer screen. Throughout the procedure, loudverbal encouragement was given to obtain theexpiratory and inspiratory manoeuvers completelywith maximal force. The procedure was monitored forcompliance with the acceptability and repeatabilitycriteria recommended by the ATS/ERS task Force.10
At least three acceptable and two repeatable effortswere obtained.
The highest values of FVC, FEV1 and PEFR wereselected. The flow rates, forced expiratory flow rate at50% and 75% exhalation of vital capacity (F50 and F75)and mean forced expiratory flow rates over themiddle 50% of the vital capacity(F25-75) were obtainedfrom the “best” curve, i.e. the one with the highestsum of FVC and FEV1.
Statistical Analysis
Statistical analysis was carried out using statisticalpackage for the social sciences (SPSS) 16.0 andGraphPad Prism 4.01 softwares. Analysis wascarried out separately in boys and girls. In the presentstudy, the dependent variables were FVC, FEV1, PEFR,F50, F75 and F25-75. Pearson’s correlation analysis wascarried out to identify the predictor variables.Prediction equations were developed using themultiple linear regression procedure. Linear and non-linear models were developed and the former wasselected based on criteria of simplicity and ease ofclinical application, high predictive capability (R2)and yield of smallest residuals.
The independent variables were entered in thesequence of height, age and weight. Models wereconstructed including one (height), two (height and
Regression Equations for Spirometry in Children S.K. Chhabra et al
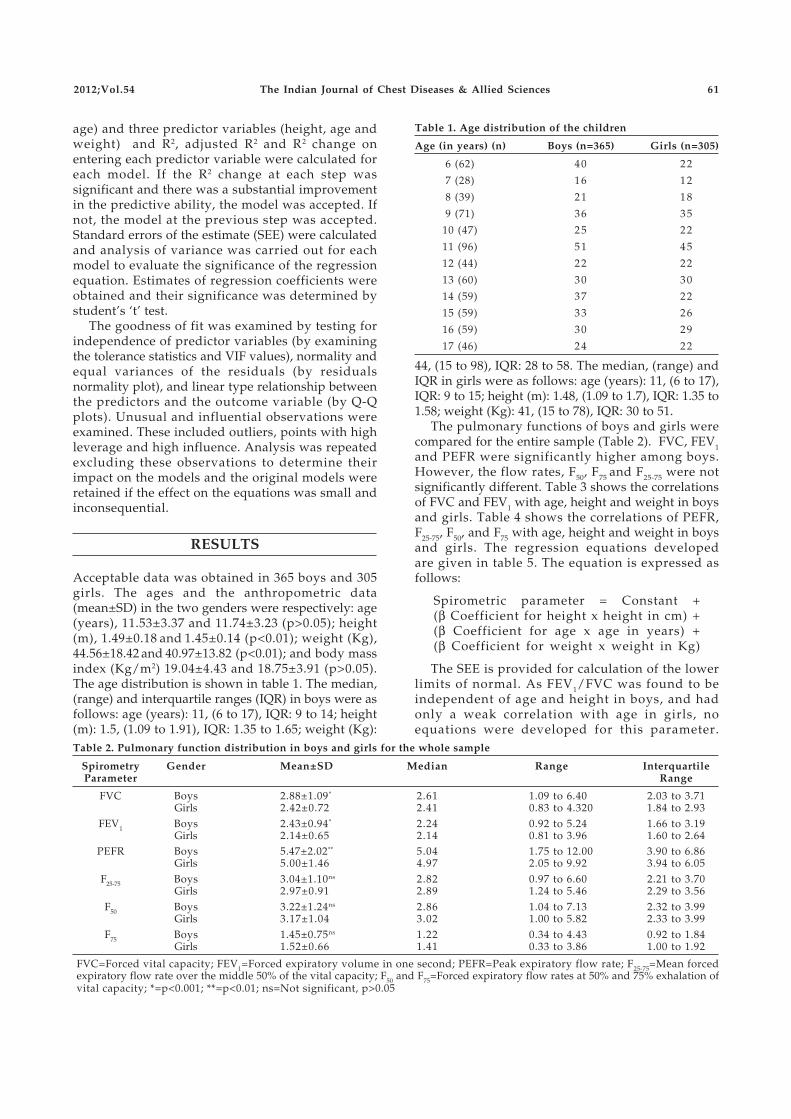
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 61
age) and three predictor variables (height, age andweight) and R2, adjusted R2 and R2 change onentering each predictor variable were calculated foreach model. If the R2 change at each step wassignificant and there was a substantial improvementin the predictive ability, the model was accepted. Ifnot, the model at the previous step was accepted.Standard errors of the estimate (SEE) were calculatedand analysis of variance was carried out for eachmodel to evaluate the significance of the regressionequation. Estimates of regression coefficients wereobtained and their significance was determined bystudent’s ‘t’ test.
The goodness of fit was examined by testing forindependence of predictor variables (by examiningthe tolerance statistics and VIF values), normality andequal variances of the residuals (by residualsnormality plot), and linear type relationship betweenthe predictors and the outcome variable (by Q-Qplots). Unusual and influential observations wereexamined. These included outliers, points with highleverage and high influence. Analysis was repeatedexcluding these observations to determine theirimpact on the models and the original models wereretained if the effect on the equations was small andinconsequential.
RESULTS
Acceptable data was obtained in 365 boys and 305girls. The ages and the anthropometric data(mean±SD) in the two genders were respectively: age(years), 11.53±3.37 and 11.74±3.23 (p>0.05); height(m), 1.49±0.18 and 1.45±0.14 (p<0.01); weight (Kg),44.56±18.42 and 40.97±13.82 (p<0.01); and body massindex (Kg/m2) 19.04±4.43 and 18.75±3.91 (p>0.05).The age distribution is shown in table 1. The median,(range) and interquartile ranges (IQR) in boys were asfollows: age (years): 11, (6 to 17), IQR: 9 to 14; height(m): 1.5, (1.09 to 1.91), IQR: 1.35 to 1.65; weight (Kg):
44, (15 to 98), IQR: 28 to 58. The median, (range) andIQR in girls were as follows: age (years): 11, (6 to 17),IQR: 9 to 15; height (m): 1.48, (1.09 to 1.7), IQR: 1.35 to1.58; weight (Kg): 41, (15 to 78), IQR: 30 to 51.
The pulmonary functions of boys and girls werecompared for the entire sample (Table 2). FVC, FEV1and PEFR were significantly higher among boys.However, the flow rates, F50, F75 and F25-75 were notsignificantly different. Table 3 shows the correlationsof FVC and FEV1 with age, height and weight in boysand girls. Table 4 shows the correlations of PEFR,F25-75, F50, and F75 with age, height and weight in boysand girls. The regression equations developedare given in table 5. The equation is expressed asfollows:
Spirometric parameter = Constant +(β Coefficient for height x height in cm) +(β Coefficient for age x age in years) +(β Coefficient for weight x weight in Kg)
The SEE is provided for calculation of the lowerlimits of normal. As FEV1/FVC was found to beindependent of age and height in boys, and hadonly a weak correlation with age in girls, noequations were developed for this parameter.
Table 2. Pulmonary function distribution in boys and girls for the whole sample
Spirometry Gender Mean±SD Median Range InterquartileParameter Range
FVC Boys 2.88±1.09* 2.61 1.09 to 6.40 2.03 to 3.71Girls 2.42±0.72 2.41 0.83 to 4.320 1.84 to 2.93
FEV1 Boys 2.43±0.94* 2.24 0.92 to 5.24 1.66 to 3.19Girls 2.14±0.65 2.14 0.81 to 3.96 1.60 to 2.64
PEFR Boys 5.47±2.02** 5.04 1.75 to 12.00 3.90 to 6.86Girls 5.00±1.46 4.97 2.05 to 9.92 3.94 to 6.05
F25-75 Boys 3.04±1.10ns 2.82 0.97 to 6.60 2.21 to 3.70Girls 2.97±0.91 2.89 1.24 to 5.46 2.29 to 3.56
F50 Boys 3.22±1.24ns 2.86 1.04 to 7.13 2.32 to 3.99Girls 3.17±1.04 3.02 1.00 to 5.82 2.33 to 3.99
F75 Boys 1.45±0.75ns 1.22 0.34 to 4.43 0.92 to 1.84Girls 1.52±0.66 1.41 0.33 to 3.86 1.00 to 1.92
FVC=Forced vital capacity; FEV1=Forced expiratory volume in one second; PEFR=Peak expiratory flow rate; F25-75=Mean forcedexpiratory flow rate over the middle 50% of the vital capacity; F50 and F75=Forced expiratory flow rates at 50% and 75% exhalation ofvital capacity; *=p<0.001; **=p<0.01; ns=Not significant, p>0.05
Table 1. Age distribution of the children
Age (in years) (n) Boys (n=365) Girls (n=305)
6 (62) 40 22
7 (28) 16 12
8 (39) 21 18
9 (71) 36 35
10 (47) 25 22
11 (96) 51 45
12 (44) 22 22
13 (60) 30 30
14 (59) 37 22
15 (59) 33 26
16 (59) 30 29
17 (46) 24 22
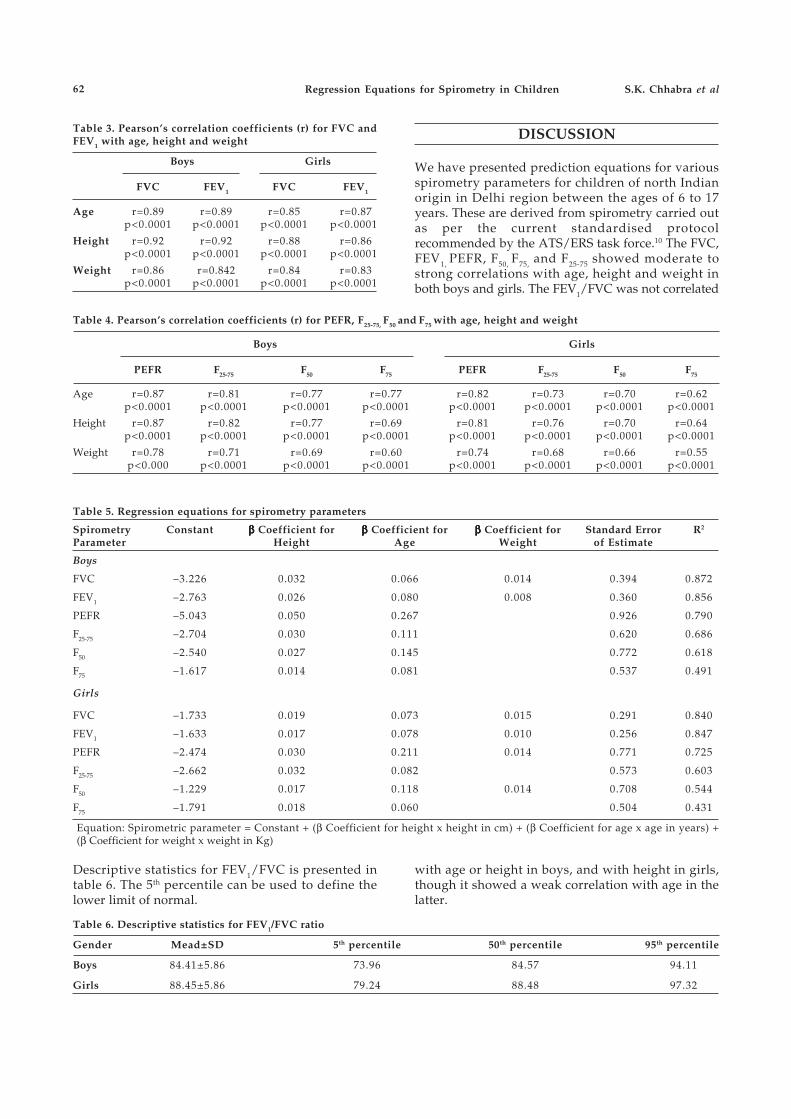
62 Regression Equations for Spirometry in Children S.K. Chhabra et al
Table 3. Pearson’s correlation coefficients (r) for FVC andFEV1 with age, height and weight
Boys Girls
FVC FEV1 FVC FEV1
Age r=0.89 r=0.89 r=0.85 r=0.87p<0.0001 p<0.0001 p<0.0001 p<0.0001
Height r=0.92 r=0.92 r=0.88 r=0.86p<0.0001 p<0.0001 p<0.0001 p<0.0001
Weight r=0.86 r=0.842 r=0.84 r=0.83p<0.0001 p<0.0001 p<0.0001 p<0.0001
Table 4. Pearson’s correlation coefficients (r) for PEFR, F25-75, F50 and F75 with age, height and weight
Boys Girls
PEFR F25-75 F50 F75 PEFR F25-75 F50 F75
Age r=0.87 r=0.81 r=0.77 r=0.77 r=0.82 r=0.73 r=0.70 r=0.62p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001
Height r=0.87 r=0.82 r=0.77 r=0.69 r=0.81 r=0.76 r=0.70 r=0.64p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001
Weight r=0.78 r=0.71 r=0.69 r=0.60 r=0.74 r=0.68 r=0.66 r=0.55p<0.000 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001 p<0.0001
Table 5. Regression equations for spirometry parameters
Spirometry Constant βββββ Coefficient for βββββ Coefficient for βββββ Coefficient for Standard Error R2
Parameter Height Age Weight of Estimate
Boys
FVC –3.226 0.032 0.066 0.014 0.394 0.872
FEV1 –2.763 0.026 0.080 0.008 0.360 0.856
PEFR –5.043 0.050 0.267 0.926 0.790
F25-75 –2.704 0.030 0.111 0.620 0.686
F50 –2.540 0.027 0.145 0.772 0.618
F75 –1.617 0.014 0.081 0.537 0.491
Girls
FVC –1.733 0.019 0.073 0.015 0.291 0.840
FEV1 –1.633 0.017 0.078 0.010 0.256 0.847
PEFR –2.474 0.030 0.211 0.014 0.771 0.725
F25-75 –2.662 0.032 0.082 0.573 0.603
F50 –1.229 0.017 0.118 0.014 0.708 0.544
F75 –1.791 0.018 0.060 0.504 0.431
Equation: Spirometric parameter = Constant + (β Coefficient for height x height in cm) + (β Coefficient for age x age in years) +(β Coefficient for weight x weight in Kg)
Table 6. Descriptive statistics for FEV1/FVC ratio
Gender Mead±SD 5th percentile 50th percentile 95th percentile
Boys 84.41±5.86 73.96 84.57 94.11
Girls 88.45±5.86 79.24 88.48 97.32
Descriptive statistics for FEV1/FVC is presented intable 6. The 5th percentile can be used to define thelower limit of normal.
DISCUSSION
We have presented prediction equations for variousspirometry parameters for children of north Indianorigin in Delhi region between the ages of 6 to 17years. These are derived from spirometry carried outas per the current standardised protocolrecommended by the ATS/ERS task force.10 The FVC,FEV1, PEFR, F50, F75, and F25-75 showed moderate tostrong correlations with age, height and weight inboth boys and girls. The FEV1/FVC was not correlated
with age or height in boys, and with height in girls,though it showed a weak correlation with age in thelatter.

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 63
In both boys and girls, the equations explained veryhigh variability of FVC, FEV1 and PEFR as shown bythe R2 values. However, the explained variability forflow rates was lesser, with that for F75 being the least.The very high values for R2 for FVC and FEV1 are alsothe reason why the interpretation algorithms forspirometry are based exclusively on these twoparameters. The FVC and FEV1 are the only parametersfor which reproducibility criteria have been defined10
and the flow rates have less precision. Effects ofenvironmental exposures including environmentaltobacco smoke and outdoor air pollution, physicalactivity and conditioning, nutritional factors, geneticsand respiratory infections are extremely difficult tocapture and therefore never factored in any model. Inaddition, pulmonary function has inherent variabilityon repeated testing. Therefore, pulmonary functionparameters usually have a high standard deviationand consequently wide range of 95% confidence limitsfor defining normalcy.
It is remarkable that among all the predictors,height alone explained a major part of variability.Inclusion of age, and weight in some equations,explained a small additional variability as shown bythe R2 change. Thus, in boys, for FVC and FEV1, allthe three predictor variables were retained in theequations while for PEFR, F50, F75 and F25-75, onlyheight and age were included. For girls, weight wasretained in the equations for FVC, FEV1, PEFR and F50.For all the parameters, the adjusted R2 values werevery close to R2 implying that if the equation wasderived from the population rather than the sample,we would get similar results.
These equations are the first effort from India afterthe recent standardisation of spirometry10 and indeedone of the few available globally. Revision ofprediction equations was long overdue as technologyand measurement protocols have changed and also todetermine if lung health in population is changingdue to changes in nutritional status, environmentalexposures and rates of early childhood respiratoryinfections. The previous studies from India, withcity and year, were: Bhattacharya and Banerjee1
(Delhi, 1966), Jain and Ramiah2 (Delhi, 1967), Vohraet al3 (Ahmedabad, 1984), Malik and Jindal4
(Chandigarh, 1985), Kumar et al5 (Patiala, 1992),Gupta et al6 (Delhi, 1993), Chowgule et al7 (Mumbai,1995), RajKappor et al8 (Rohtak, 1997) and Vijayan etal9 (Chennai, 2000).
The present study has a few limitations. A widerselection from several schools would have provided amore representative sample. However, the selectedschool caters to a very wide socio-economicspectrum, and therefore, may be viewed as beingfairly representative of Delhi. In order to ensure ethnichomogeneity, we included only children whoseparents were of north Indian origin. A multicentricstudy with participation of other cities of the region
was not feasible because of limited resources.Therefore, while the equations predict pulmonaryfunction of children of north Indian origin, wesuggest that the equations may also be validated inother north Indian states in further studies. A chestradiograph would have confirmed normalcy.However, this was not feasible in a field study. Acareful and detailed history and examination by thephysicians, however, ensured that only normalchildren were included.
These equations should be helpful ininterpretation of spirometric data, and thus, in themanagement of respiratory diseases such as asthmain children. Equipments used in most pulmonaryclinics use softwares that carry western predictionequations and are not valid for Indian population.These equations would allow manufacturers toprovide Indian equations in the softwares. Theequations described by us have been developed fornorthern parts of the country. As ethnic differencesare important, each region needs to develop suchequations following the standardised protocols andstrict quality control.
ACKNOWLEDGEMENTS
The project titled “Pulmonary Function in Normal Children inDelhi Region: Development of Reference Standards forSpirometry” was approved and funded by the Indian Councilof Medical Research. The support of the Council is gratefullyacknowledged.
REFERENCES
1. Bhattacharya AK, Banerjee S. Vital capacity in children andyoung adults of India. Indian J Med Res 1966;54:62-71.
2. Jain SK, Ramiah TJ. Prediction of ventilatory norms in healthyboys 7-14 years age. Indian J Med Res 1967;55:69-79.
3. Vohra RS, Shah SC, Shah GS. Pulmonary functions innormal children. Indian Pediatr 1984;21:785-90.
4. Malik SK, Jindal SK. Pulmonary function tests in healthychildren. Indian Pediatr 1985;22:677-81.
5. Kumar A, Pannu BK, Manchanda KC, Singh KD, LahalSS. Pulmonary function tests in healthy male Punjabichildren. Indian J Chest Dis Allied Sci 1992;34:191-5.
6. Gupta CK, Mishra G, Mehta SC, Prasad J. On thecontribution of height to predict lung volumes, capacitiesand diffusion in healthy schoolchildren of 10-17 years.Indian J Chest Dis Allied Sci 1993;35:167-77.
7. Chowgule RV, Shetye VM, Parmar JR. Lung function testsin normal Indian children. Indian Pediatr 1995;32:185-91.
8. RajKappor, Mahajan KK, Mahajan A. Ventilatory lungfunction tests in schoolchildren of 6-13 years. Indian J ChestDis Allied Sci 1997;39:97-105.
9. Vijayan VK, Reetha AM, Kuppurao KV, Venkatesan P,Thilakavathy S. Pulmonary function in normal southIndian children aged 7 to 19 years. Indian J Chest Dis AlliedSci 2000;42:147-56.
10. Miller MR, Hankinson J, Brusasco V, Burgos F, CasaburiR, Coates A, et al. Standardisation of spirometry. EurRespir J 2005;26:319-38.

64Correspondence
To the Editor: I read with interest the article byMukherjee A et al.1High sputum grade indicate that thepatient is harboring large bacillary load which alsoindicate severity of the disease and presence of naturaldrug resistant strain. The authors had added alloutcomes (i.e., default, failure and death) to compare theunfavourable outcome between high and low gradesputum positive patients. However, the risk for deathand default rate are not related to category of patients ortheir treatment.2 In the present study, no significantdifference in failure rate among low-grade and high-grade sputum positive patient was observed (2.1% vs2.5%, p>0.37). So the authors’ advocacy to add anotheranti-tuberculosis drug in the current regimen of RevisedNational Tuberculosis Control Programme (RNTCP) forinitial higher grade of sputum positive patient is notjustifiable. Other than fluoroquinolone, we have noother effective and less toxic oral medicine to add in thecurrent regimen. However, fluoroqinolones arerampantly used for various common diseases and thehigh prevalence of resistance to ofloxacin has beenreported from India.3 The authors have not discussed thereason behind relatively high death rate among scantypositive patients.
Irrespective of smear report, RNTCP guidelineshave recommended to start continuation phase aftercompletion of prolongation of intensive phase of thetreatment. As per Directly Observed Treatment, shortcourse-Plus (DOTS-PLUS) guidelines, a multidrug-resistant tuberculosis (MDR) suspect is a new smearpositive patient who remain smear positive at the endof five months of the treatment. The outcome analysisof new smear positive patients who remained positiveat the end of prolongation of intensive phase of thetreatment may be helpful to recommend sputumculture for the early detection of MDR.
REFERENCES
1. Mukherjee A, Singla R, Saha I, Sarkar A, Bhattacharyya P.Difference in the outcome of patients with different gradesof initial sputum positivity under the Revised NationalTuberculosis Control Programme. Indian J Chest Dis AlliedSci 2011;53:241-2.
2. Chandrasekaran V, Gopi PG, Subramani R, Thomas A,Jaggarajamma K, Narayanan PR. Default during theintensive phase of treatment under DOTS programme.Indian J Tuber 2005;52:197-202.
3. Singh M, Chauhan DS, Gupta P, Das K, Srivastav RK,Upadhyay P, et al. In vitro effect of fluoroquinolonesagainst Mycobacterium tuberculosis isolates from Agra and
Difference in the Outcome of Patients with Different Grades ofInitial Sputum Positivity under the Revised NationalTuberculosis Control Programme1
[Indian J Chest Dis Allied Sci 2012;54:64-65]
Kanpur regions of north India. Indian J Med Res2009;129:542-7.
Sajal DeQr No.-8 , Vivekananda Colony
MGIMS CampusSevagram - 442 102 [Maharashtra]
E-Mail: [email protected]
The Authors’ Reply: We would like to thank thereader for showing interest in our article.1 Death,default and failure have been included underunfavourable outcomes in several studies on theRNTCP in the past,2 and hence were used by theauthors.
Rajpal et al3 in their study on patients notifiedunder the RNTCP found that the proportion ofdefaulters was higher in 3+ patients. The authors goon to say that from the practical point of view, itwould appear that grading of sputum need not bemerely an academic exercise but instead helppinpoint a group of patients who are likely to defaultoftener than others.3 Even studies from Gambia4 haverecommended that patients with high bacterial loadin initial sputum smears need to be closelysupervised, as they are more likely to default fromtreatment.
Singla et al5 have shown significantly highfailure rates among patients with 3+ TB patients.The present study also shows a higher failure rate(2.1% vs 2.5%) among the groups although thedifference is not statistically significant. Given thelarge number of patients suffering from tuberculosiseven a small decrease in the rates of failure willhave a huge impact in terms of the absolute numberof patients with failure. Studies with a largersample may be able to bring out the statisticalsignificance.
The authors would like to suggest the use ofstreptomycin and not fluoroquinolones as theadditional drug for the patients with higher grades ofinitial sputum positivity. A regimen similar toCategory II may be used in patients with 3+ initialsputum smear grades.
REFERENCES
1. Mukherjee A, Singla R, Saha I, Sarkar A, Bhattacharyya P.Difference in the outcome of patients with different gradesof initial sputum positivity under the Revised NationalTuberculosis Control Programme. Indian J Chest Dis AlliedSci 2011;53:241-2.
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 65
2. Vijay S, Balasangameshwara VH, Jagannatha PS, SarojaVN, Shivashankar B, Jagota P. Re-treatment outcome ofsmear positive tuberculosis cases under DOTS inBangalore city. Indian J Tuber 2002;49:195-203.
3. Rajpal S, Dhingra VK, Aggarwal JK. Sputum grading aspredictor of treatment outcome in pulmonarytuberculosis. Indian J Tuber 2002;49:139-41.
4. Lienhardt C, Manneh K, Bouchier V, Lahai G, MilliganPJM, Mc Adam KPWJ. Factors determining the outcomeof treatment of adult smear positive tuberculosis cases inthe Gambia. Int J Tuberc Lung Dis 1998;2:712-8.
5. Singla R, Singla N, Sarin R, Arora V.K. Influence of
pretreatment bacillary Load on treatment outcome ofpulmonary tuberculosis patients receiving DOTS underthe Revised National Tuberculosis Control Programme.Indian J Chest Dis Allied Sci 2005;47:19-23.
Abhijit Mukherjee34, S.N. Banerjee Road
New BarrackporeKolkata - 700 131 (West Bengal), India
E-mail: [email protected]
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 65
Abstracts’ Service
[Indian J Chest Dis Allied Sci 2012;54:66-69]
Policy transfer occurs regularly. In essence, a strategydeveloped elsewhere is taken up and applied inanother policy context. Yet what precisely is policytransfer and, more importantly, under whatconditions does it occur? This paper describes policytransfer and addresses three main questions,exploring what perspectives of policy transfer mightcontribute to operational research (OR) efforts. First,what facilitates the transfer of OR results into policyand practice? Second, what facilitates effectivelesson-drawing about OR results and processesbetween and within countries? And third, whatwould increase the amount of OR being carried out bylow- and middle-income countries and used to informpolicy and practice at local and global levels?
Mexico’s adoption and adaptation of the DOTSstrategy is used here as an example of policy transfer.
Analysing Policy Transfer: Perspectives for Operational Research
K. Bissell, K. Lee and R. Freeman
International Journal of Tuberculosis and Lung Disease 2011;15:1140-1148
Policy transfer is relevant to all countries, levels andarenas of people, institutions and organisationsinvolved in health. With a more systematic analysis oflearning and policy processes, OR policy and practiceoutcomes could be improved at all levels, from local toglobal.
Policy transfer offers theory and concepts foranalysing OR from a new perspective. The presentpaper proposes a model of the policy transfer processfor qualitative research use. Comprehensive policytransfer research, given its length, complexity andneed for qualitative researchers, should not beenvisaged for all OR projects. All OR projects could,however, incorporate some concepts and practicaltools inspired from this model. This should help toplan, evaluate and improve OR processes and theresulting changes in policy and practice.
Objective. A new loop-mediated isothermalamplification (LAMP) test kit, including a simpleDNA extraction device for the detection ofMycobacterium tuberculosis complex, was developed forcommercial use and evaluated for its usefulness indiagnosing tuberculosis (TB).
Design. The LAMP test was performed usinguntreated and N-acetyl-L-cysteine (NALC) NaOH-treated sputum specimen. The efficiency of the kit wascompared with other conventional laboratoryexaminations, including other nucleic acidamplification (NAA) tests.
Results. The sensitivity of LAMP using raw sputum(direct LAMP) in smear- and culture-positivespecimens was 98.2% (95% CI 94.9-99.4), while thesensitivity in smear-negative, culture-positive
Evaluation of a Simple Loop-mediated Isothermal Amplification Test Kit forthe Diagnosis of Tuberculosis
S. Mitarai, M. Okumura, E. Toyota, T. Yoshiyama, A. Aono, A. Sejimo, Y. Azuma, K. Sugahara,T. Nagasawa, N. Nagayama, A. Yamane, R. Yano, H. Kokuto, K. Morimoto, M. Ueyama,M. Kubota, R. Yi, H. Ogata, S. Kudoh and T. Mori
International Journal of Tuberculosis and Lung Disease 2011;15:1211-1217
specimens was 55.6% (95% CI 43.4-68.0). Thediagnostic sensitivity of direct LAMP for thediagnosis of individuals with TB was 88.2% (95% CI81.4-92.7). The sensitivity values of direct LAMP wereslightly, but not statistically significantly lower thanthose of Cobas Amplicor MTB and TRC Rapid MTB,while the sensitivity of the LAMP test using NALC-NaOH treated sputum was significantly lower thanother NAA tests (P<0.05) for smear-negative, culture-positive specimens. The new commercial version ofthe LAMP kit was easy to handle and yielded resultswithin 1 h of receiving sputum specimens.
Conclusions. This test is considered a promisingdiagnostic tool for TB, even for peripherallaboratories with limited equipment, such as those indeveloping countries.
Background. The severity of obstructive pulmonarydisease is determined by the FEV1 % predicted basedon the American Thoracic Society/EuropeanRespiratory Society (ATS/ERS) guidelines. In patientswith coexisting restrictive lung disease, the decreasein FEV1 can overestimate the degree of obstruction. Wehypothesize that adjusting the FEV1 for the decreasein total lung capacity (TLC) results in a moreappropriate grading of the severity of obstruction.
Methods. We examined a large pulmonary functiontest database and identified patients with bothrestrictive (TLC <80% predicted) and obstructive(FEV1/FVC < the lower limit of normal) lung disease.FEV1 % predicted was adjusted for the degree ofrestriction by dividing it by TLC % predicted. Wecompared the distribution of severity grading betweenadjusted and unadjusted values according to ATS/ERS criteria and determined how the distribution of
severity would change based on asthma and COPDguidelines.Results. We identified 199 patients with coexistingrestrictive and obstructive lung disease. By ATS/ERSgrading, the unadjusted data categorized 76% ofpatients as having severe or very severe obstructionand 11% as having mild or moderate obstruction. Theadjusted data classified 33% with severe or very severeobstruction and 44% with mild or moderateobstruction. Of the corrected values, 83% resulted in achange to less severe obstruction by ATS/ERSguidelines, and 44% and 70% of patients, respectively,would be reclassified as having less severe obstructionby current asthma and COPD guidelines.Conclusions. This method results in a moreappropriate distribution of severity of obstruction,which should lead to more accurate treatment ofobstruction in these patients.
Grading the Severity of Obstruction in Mixed Obstructive-Restrictive LungDisease
Zechariah S. Gardner, Gregg L. Ruppel and David A. Kaminsky
Chest 2011;140:598-603
Context. Immunochemical staining of sentinel lymphnodes (SLNs) and bone marrow identifies breastcancer metastases not seen with routine pathologicalor clinical examination.
Objective. To determine the association betweensurvival and metastases detected by immunochemicalstaining of SLNs and bone marrow specimens frompatients with early-stage breast cancer.
Design, Setting, and Patients. From May 1999 to May2003, 126 sites in the American College of SurgeonsOncology Group Z0010 trial enrolled women withclinical T1 to T2N0M0 invasive breast carcinoma in aprospective observational study.
Interventions. All 5210 patients underwent breast-conserving surgery and SLN dissection. Bone marrowaspiration at the time of operation was initiallyoptional and subsequently mandatory (March 2001).Sentinel lymph node specimens (hematoxylin-eosin
negative) and bone marrow specimens were sent to acentral laboratory for immunochemical staining;treating clinicians were blinded to results.Main Outcome Measures. Overall survival (primaryend point) and disease-free survival (a secondary endpoint).Results. Of 5119 SLN specimens (98.3%), 3904(76.3%) were tumor-negative by hematoxylin-eosinstaining. Of 3326 SLN specimens examined byimmunohistochemistry, 349 (10.5%) were positivefor tumor. Of 3413 bone marrow specimensexamined by immunocytochemistry, 104 (3.0%)were positive for tumors. At a median follow-upof 6.3 years (through April 2010), 435 patients haddied and 376 had disease recurrence. Immunohisto-chemical evidence of SLN metastases was notsignificantly associated with overall survival (5-yearrates: 95.7%; 95% confidence interval [CI], 95.0%-96.5% for immunohistochemical negative and 95.1
Association of Occult Metastases in Sentinel Lymph Nodes and Bone MarrowWith Survival Among Women With Early-Stage Invasive Breast Cancer
Armando E. Giuliano, Debra Hawes, Karla V. Ballman, Pat W. Whitworth, Peter W. Blumencranz,Douglas S. Reintgen, Monica Morrow, A. Marilyn Leitch, Kelly K. Hunt, Linda M. McCall,Andrea Abati and Richard Cote
JAMA 2011;306:385-393
2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 67

68
The safety of talc pleurodesis is under disputefollowing reports of talc-induced acute respiratorydistress syndrome (ARDS) and death. We investigatedthe safety of large-particle talc for thoracoscopicpleurodesis to prevent recurrence of primaryspontaneous pneumothorax (PSP).
418 patients with recurrent PSP were enrolledbetween 2002 and 2008 in nine centres in Europe andSouth Africa. The main exclusion criteria wereinfection, heart disease and coagulation disorders.Serious adverse events (ARDS, death or other) wererecorded up to 30 days after the procedure. Oxygensaturation, supplemental oxygen use and temperaturewere recorded daily at baseline and after
thoracoscopic pleurodesis (2 g graded talc).During the 30-day observation period following talcpoudrage, no ARDS (95% CI 0.0-0.9%), intensive careunit admission or death were recorded. Seven patientspresented with minor complications (1.7%, 95% CI0.7-3.4%). After pleurodesis, mean body temperatureincreased by 0.41°C (95% CI 0.33-0.48 °C; p<0.001) atday 1 and returned to baseline value at day 5. Pleuraldrains were removed after day 4 in 80% of patients.Serious adverse events, including ARDS or death, didnot occur in this large, multicentre cohort.Thoracoscopic talc poudrage using larger particletalc to prevent recurrence of PSPs can be consideredsafe.
Short-term Safety of Thoracoscopic Talc Pleurodesis for Recurrent PrimarySpontaneous Pneumothorax: A Prospective European Multicentre Study
P-O. Bridevaux, J-M. Tschopp, G. Cardillo, C-H. Marquette, M. Noppen, P. Astoul, P. Driesen,C.T. Bolliger, M.E. Froudarakis and J.P. Janssen
European Respiratory Journal 2011;38:770-773
%; 95% CI, 92.7%-97.5% for immunohistochemicalpositive disease; P=.64; unadjusted hazard ratio[HR], 0.90; 95% CI, 0.59-1.39; P=.64). Bone marrowmetastases were associated with decreased overallsurvival (unadjusted HR for mortality, 1.94; 95% CI,1.02-3.67; P=.04), but neither immunohistochemicalevidence of tumor in SLNs (adjusted HR, 0.88; 95%CI, 0.45-1.71; P=.70) nor immunocytochemicalevidence of tumor in bone marrow (adjusted HR,1.83; 95% CI, 0.79-4.26; P=.15) was statistically
significant on multivariable analysis.
Conclusion. Among women receiving breast-conserving therapy and SLN dissection,immunohistochemical evidence of SLN metastasis wasnot associated with overall survival over a median of6.3 years, whereas occult bone marrow metastasis,although rare, was associated with decreased survival.
Trial Registration clinicaltrials.gov Identifier:NCT00003854
Context. Combining foods with recognizedcholesterol-lowering properties (dietary portfolio) hasproven highly effective in lowering serum cholesterolunder metabolically controlled conditions.
Objective. To assess the effect of a dietary portfolioadministered at 2 levels of intensity on percentagechange in low-density lipoprotein cholesterol (LDLC)
among participants following self-selected diets.
Design, Setting, and Participants. A parallel-designstudy of 351 participants with hyperlipidemia from 4participating academic centers across Canada(Quebec City, Toronto, Winnipeg, and Vancouver)randomized between June 25, 2007, and February 19,2009, to 1 of 3 treatments lasting 6 months.
Effect of a Dietary Portfolio of Cholesterol-Lowering Foods Given at 2 Levelsof Intensity of Dietary Advice on Serum Lipids in Hyperlipidemia: ARandomized Controlled Trial
David J.A. Jenkins, Peter J.H. Jones, Benoit Lamarche, Cyril W.C. Kendall, Dorothea Faulkner,Luba Cermakova, Iris Gigleux, Vanu Ramprasath, Russell de Souza, Chris Ireland,Darshna Patel, Korbua Srichaikul, Shahad Abdulnour, Balachandran Bashyam, Cheryl Collier,Sandy Hoshizaki, Robert G. Josse, Lawrence A. Leiter, Philip W. Connelly and Jiri Frohlich
JAMA 2011;306:831-839
Abstracts’ Service

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 69
Intervention. Participants received dietary advice for6 months on either a low-saturated fat therapeuticdiet (control) or a dietary portfolio, for whichcounseling was delivered at different frequencies, thatemphasized dietary incorporation of plant sterols, soyprotein, viscous fibers, and nuts. Routine dietaryportfolio involved 2 clinic visits over 6 months andintensive dietary portfolio involved 7 clinic visits over6 months.
Main Outcome Measures. Percentage change inserum LDL-C.
Results. In the modified intention-to-treat analysisof 345 participants, the overall attrition rate was notsignificantly different between treatments (18% forintensive dietary portfolio, 23% for routine dietaryportfolio, and 26% for control; Fisher exact test,P=.33). The LDL-C reductions from an overall meanof 171 mg/dL (95% confidence interval [CI], 168-174mg/dL) were –13.8% (95% CI, –17.2% to –10.3%; P<.001) or –26 mg/dL (95% CI, –31 to –21 mg/dL;
P<.001) for the intensive dietary portfolio; –13.1%(95% CI, –16.7% to –9.5%; P<.001) or –24 mg/dL(95% CI, –30 to –19 mg/dL; P<.001) for the routinedietary portfolio; and –3.0% (95% 0, –6.1% to 0.1%;P=.06) or –8 mg/dL (95% CI, –13 to –3 mg/dL;P=.002) for the control diet. Percentage LDL-Creductions for each dietary portfolio weresignificantly more than the control diet (P< .001,respectively). The 2 dietary portfolio interventionsdid not differ significantly (P= .66). Amongparticipants randomized to one of the dietaryportfolio interventions, percentage reduction inLDL-C on the dietary portfolio was associated withdietary adherence (r=–0.34, n=157, P<.001).
Conclusion. Use of a dietary portfolio compared withthe low-saturated fat dietary advice resulted ingreater LDL-C lowering during 6 months of follow-up.
Trial Registration clinicaltrials.gov Identifier:NCT00438425
11th NCCP RAJPULMOCON-2012(Rajasthan State Conference)
on
March 3-4, 2012
at
RNT Medical CollegeUdaipur (Rajasthan)
For further information and details, please contact:
Secretary, Organising Committee Chairman, Organising CommitteeDr Mahendra Kumar Dr N.K. GuptaConference Secretariate: Q-2. TB Hospital, Bari Mobile: 09829136089E-mail: [email protected]: 0294-2450733Mobile: 08769153850
70 The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.54
A.K. Agarwal(New Delhi)
Ritesh Agarwal(Chandigarh)
A.N. Aggarwal(Chandigarh)
Gautam Ahluwalia(Chandigarh)
Naveen Arora(Delhi)
Rajinder Singh Bedi(Patiala)
Arati Bhatia(Delhi)
S.K. Chhabra(Delhi)
Debashis Dhar(New Delhi)
Nitin Goel(Delhi)
Dheeraj Gupta(Chandigarh)
K.B. Gupta(Rohtak)
M.L. Gupta(Jaipur)
Anand Jaiswal(New Delhi)
A.K. Janmeja(Chandigarh)
M.S. Jawahar(Chennai)
S.K. Jindal(Chandigarh)
Panel of Reviewers—2011
J.M. Joshi(Mumbai)
T. Kadhiravan(Puducherry)
Ritu Kulshrestha(Delhi)
Raj Kumar(Delhi)
T.K. Lahiri(Varanasi)
Balakrishnan Menon(Delhi)
Alladi Mohan(Tirupati)
P.R. Mohapatra(Chandigarh)
R. Prasad(Lucknow)
H.S. Randhawa(Delhi)
J.K. Samaria(Varanasi)
Ashok Shah(Delhi)
S.K. Sharma(New Delhi)
Virendra Singh(Jaipur)
Rupak Singla(New Delhi)
Manish Soneja(New Delhi)
Vijayalakshmi Thanasekaraan(Chennai)
Mandira Varma-Basil(Delhi)

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 71
Form IV
Statement about ownership and other particulars of the Indian Journal of Chest Diseases and AlliedSciences under Rule 8 of the Registration of Newspapers (Central), Rules, 1956.
1. Place of Publication : Vallabhbhai Patel Chest InstituteUniversity of Delhi, Delhi-110 007
2. Periodicity : Quarterly
3. Printer’s name : Prof. S.N. GaurV.K. Vijayan(i) Whether citizen of India? : Yes(ii) Address : Director (Actg)
Vallabhbhai Patel Chest InstituteUniversity of Delhi, Delhi-110 007
4. Publisher’s name : Prof. S.N. GaurVK. Vijayan(i) Whether citizen of India? : Yes(ii) Address : Director (Actg)
Vallabhbhai Patel Chest InstituteUniversity of Delhi, Delhi-110 007
5. Editor-in-Chief's name : Prof. S.N. GaurVK.(i) Whether citizen of India? : Yes(ii) Address : Director (Actg)
Vallabhbhai Patel Chest InstituteUniversity of Delhi, Delhi-110 007
6. Names and address as of individuals : Vallabhbhai Patel Chest Institutewho own the newspapers and partners or University of Delhishareholder holding more than one percent Delhi-110 007of the total capital
I, Professor S.N. Gaur, hereby declare that the particulars given above are true to the best of myknowledge and belief.
Sd/-Dated: January 18, 2012 Prof. S.N. Gaur
(Signature of Publisher)

The Indian Journal of Chest Diseases & Allied Sciences 2012;Vol.5472
ATTENTION SUBSCRIBERS
Subscription Rates[w.e.f. Ist January, 2011]
Individual Institutes/Hospitals/Colleges, etc.India Overseas (Airmail) India Overseas (Airmail)(in R) (in US $) (in R) (in US $)
Single Issue 400.00 60.00 500.00 100.00
Per Volume(4 issues) 1300.00 200.00 1800.00 350.00____________________________________________________________________________________________
1. Overseas subscription rates include airmail postal charges.
2. Subscription Agencies are eligible for a 10% discount on annual rates for institutional subscriptiononly. Agencies must provide complete address of the institution for which subscription is sent intheir subscription order.
3. Payments should be made only by Banker’s Cheque/Demand Draft; drawn in favour of TheDirector, V.P. Chest Institute, Delhi.
4. Subscription rates are not subject to any Tax Deduction at Source.
5. Subscribers are advised to get their copies by “Registered Post” by making an advance payment ofR400/- per year in addition to Subscription rates, if subscription is made for one year (in case of asingle copy, R100/- to be added).
6. The rates are subject to revision at any time by announcement in the Journal.
7. Subscription can be enrolled only on receipt of full payment in advance. Copies will not be sent ifpart payment is received.
8. Our responsibility ceases once we hand over the copies to the Post/Courier Office. We are notresponsible for any delay/loss/damage in transit. We hold the receipt from the Post/Courier Officeas proof. The Journal Office is not liable to replace copies lost in transit.
9. Requests for missing issues will be considered if made within one month of the publication of aparticular issue (i.e. for January-March issue ➔ upto April, for April-June issue ➔ upto July, for July-September issue ➔ upto October and for October-December issue ➔ upto January). Supply ofreplacement copy will be subject to availability.
Director/Editor-in-Chief

[Indian J Chest Dis Allied Sci 2012;54:73-78]
The Indian Journal of Chest Diseases and Allied Sciencesconsiders for publication original articles dealing withrespiratory and cardiovascular diseases and in the fieldsof anatomy, biochemistry, microbiology, mycology,pathology, pharmacology, physiology, ultra-structureand virology of respiratory, and cardiovascular systems.However, only papers that make a significant contribu-tion to the existing state of knowledge in a particularfield will be published. The journal publishes originalarticles, review articles (invited) case reports, radiologyforum, short communications and book reviews.
Submission of Manuscripts. Manuscripts shouldbe submitted in a CD in MS word (in addition to hardcopies). Typescript including figures (in triplicate)should be sent to The Editor–in–Chief, The IndianJournal of Chest Diseases and Allied Sciences, C/oPublication Division, V.P. Chest Institute, Universityof Delhi, Delhi-110007, Post Box No. 2101.
Articles can also be submitted on our e-mail at:[email protected]
Manuscripts should be submitted with theundertaking that they are not under considerationelsewhere and have not been reported earlier partly/totally. Submission of a manuscript indicates tacitacknowledgement that all authors have made significantcontributions to the study and have read and approvedthe contents. Any change in authorship following theoriginal submission must be justified and agreed to inwriting by the affected author(s). Manuscripts areacknowledged upon receipt.
When inquiring about a manuscript, please refer tothe article accession number assigned to the manuscriptby the Publication Office of the IJCDAS.
Manuscripts are evaluated critically by the EditorialBoard with the help of Experts. Acceptance ofmanuscripts for publication is based on: (a) originalityof contribution; (b) proper analysis of scientific data; (c)clarity of presentation; and (d) ethically acceptabledesign of the study. All accepted manuscripts aresubject to manuscript editing. Only one copy ofrejected manuscripts will be returned.
Preparation of Manuscript
Presentation of manuscripts should conform withthe uniform requirements for manuscripts submitted tobiomedical journals.
Authors are advised to see a recent issue of theJournal to get familiar with the format adopted onvarious elements of a paper. All the manuscripts shouldbe submitted in the order set forth below. Failure to followthese instructions may result in the manuscript being
Guidelines to Authorsreturned to the author(s) for revision before it will bereviewed.
General. Manuscripts must be typewritten, double-spaced with wide margin on A-4 size good qualitybond paper. Each of these segments of the manuscriptshould begin on a new page: title page; abstract;introduction; references; legends; tables.
I. Title Page. This should be as concise and asinformative as possible. List (i) title; (ii) the initialsfollowed by the last name of each author; (iii) the nameof the department(s) and institution(s) to which thework should be attributed; (iv) the name and address(including e-mail) of the author to whom queries,proofs and requests for reprints should be sent; and (v)a short running title (not exceeding 5-6 words).
II. Abstract and Key Words. The second page shouldcarry a structured abstract of not more than 200 wordswith subheadings of Background and objectives,Methods, Results and Conclusions (unstructuredabstract for case reports). It should be written for thereadership of both clinicians and basic investigatorsand should state the hypothesis or central question ofthe study or investigation, the study subjects orexperimental animals, observational and analyticalmethods, the main findings, and a final statement of theprincipal conclusions. Three to six key words using,where possible terms of medical subjects headingslist from Index Medicus.
III. Introduction. It should commence on separatepage and should briefly review the current state ofknowledge strictly concerning the topic of the paper. Itshould also make a clear statement on the reasons forundertaking the study being reported and what ithoped to achieve. No mention should be made of theresults obtained or conclusions drawn.
IV. Material and Methods. The material (patients,experimental animals, etc.) used for makingobservations must be described along with all otherrelevant information. The methods used in the studyshould be described, giving sufficient information topermit the work to be repeated. If a generally acceptedtechnique has been used, only a reference to that isenough. If, however, such a technique has beenmodified by the workers, the manner in which this hasbeen done should be clearly stated. If statisticalanalysis of the data has been done, the methods usedfor analysis should be specified.
V. Results. This section should not include materialssuitable for inclusion in “Material and Methods” or“Discussion”. The results should be presented in

74
logical sequence in the text, tables and illustrations. Thedata presented in the tables or figures should not berepeated in the text. Only important and significantobservations should be included.
VI. Discussion. This should be limited to significanceof results obtained and what can and what cannot beconcluded and why. It should not be a repetition of thefindings already given under ‘Results’. Results shouldbe discussed in the light of others’ work in the field.Speculative and purely theoretical discussion to whichresults presented are not related will not be accepted.
VII. Acknowledgements. Acknowledgement should bebrief and made specific for scientific/technicalassistance and financial supports in the form ofgrants/drugs/equipment only and for not providingroutine departmental facilities and for help in thepreparation of manuscript (including typing/secretarial assistance).
VIII. References. References should be typed on aseparate page after the text and these should benumbered consecutively in the order in which they arefirst mentioned in the text. Identify references in text,tables, and legends by Arabic numerals in parentheses.References cited only in tables or figure legends shouldbe numbered in accordance with the sequenceestablished by the first identification in the text of theparticular table or figure. The titles of journals should beabbreviated according to the style used in Index Medicus.Consult the List of Journals Indexed in Index Medicus,published annually as a separate publication by thelibrary and as a list in the January issue of Index Medicus.The list can also be obtained through the library’s website (http://www.nlm.nih.gov). Unpublished workshould not be cited in references, but may be cited fullyparenthetically within the text. List all the authors whenthere are six or fewer; but when there are seven or more,list the first six, then ‘et al’. Examples of correct form ofreferences are given here :
Articles in Journals
1. Standard journal article
Halpern SD, Ubel PA, Caplan AL. Solid-organ trans-plantation in HIV-infected patients. N Engl J Med 2002;347: 284-7.
More than six authors:
Rose ME, Huerbin MB, Melick J, Marion DW, PalmerAM, Schiding JK, et al. Regulation of interstitial excita-tory amino acid concentrations after cortical contu-sion injury. Brain Res 2002; 935 (1-2): 40-6.
2. Article published electronically ahead of the print version
Yu WM, Hawley TS, Hawley RG, Qu CK. Immortal-ization of yolk sac-derived precursor cells. Blood 2002Nov 15; 100(10): 3828-31. Epub 2002 July 5.
3. Volume with supplement
Geraud G, Spierings EL, Keywood C. Tolerability andsafety of frovatriptan with short-and long-term usefor treatment of migraine and in comparison withsumatriptan. Headache 2002; 42 Suppl 2: S93-9.
4. Issue with supplement
Glauser TA. Integrating clinical trial data into clinicalpractice. Neurology 2002; 58 (12 Suppl 7): S6-12.
5. Type of article indicated as needed
Tor M, Turker H. International approaches to the pre-scription of long-term oxygen therapy [letter]. EurRespir J 2002; 20(1): 242.
Lofwall MR, Strain EC, Brooner RK, Kindbom KA,Bigelow GE. Characteristics of older methadone main-tenance (MM) patients [abstract]. Drug Alcohol Depend2002; 66 Suppl 1: S105.
6. Volume with part
Abend SM, Kulish N. The psychoanalytic methodfrom an epistemological viewpoint. Int J Psychoanal2002; 83 (Pt 2): 491-5.
7. Issue with part
Ahrar K, Madoff DC, Gupta S, Wallace MJ, Price RE,Wright KC. Development of a large animal model forlung tumours. J Vasc Interv Radiol. 2002; 13(9 Pt 1):923-8.
8. Issue with no volume
Banit DM, Kaufer H, Hartford JM. Intraoperative fro-zen section analysis in revision total joint arthroplasty.Clin Orthop 2002; (401): 230-8.
9. No volume or issue
Outreach: bringing HIV-positive individuals into care.HRSA Careaction 2002 Jun: 1-6.
10. Pagination in roman numerals
Chadwick R, Schuklenk U. The politics of ethical con-sensus finding. Bioethics 2002; 16(2): iii-v.
11. Organization as author
Diabetes Prevention Program Research Group. Hyper-tension, insulin, and proinsulin in participants withimpaired glucose tolerance. Hypertension 2002; 40(5):679-86.
12. Both personal authors and an organization as author(This example does not conform to NISO standards).
Vallancien G, Emberton M, Harving N, van MoorselaarRJ; Alf-One Study Group. Sexual dysfunction in 1,274European men suffering from lower urinary tractsymptoms. J Urol 2003; 169(6): 2257-61.
Guidelines to Authors 2012;Vol.53

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 75
13. No author given
21st century heart solution may have a sting in thetail. BMJ 2002; 325(7357): 184.
14. Article containing retraction
Feifel D, Moutier CY, Perry W. Safety and tolerabilityof a rapidly escalating dose-loading regimen forrisperidone. J Clin Psychiatry 2002; 63(2): 169. Retrac-tion of: Feifel D, Moutier CY, Perry W. J Clin Psychiatry2000; 61(12): 909-11.
15. Article retracted
Feifel D, Moutier CY, Perry W. Safety and tolerabilityof a rapidly escalating dose-loading regimen forrisperidone. J Clin Psychiatry 2000; 61(12): 909-11. Re-traction in: Feifel D, Moutier CY, Perry W. J Clin Psy-chiatry 2002; 63(2): 169.
16. Article republished with corrections
Mansharamani M, Chilton BS. The reproductive im-portance of P-type ATPases. Mol Cell Endocrinol 2002;188(1-2): 22-5. Corrected and republished from: MolCell Endocrinol 2001; 183(1-2): 123-6.
17. Article with published erratum
Malinowski JM, Bolesta S. Rosiglitazone in the treat-ment of type 2 diabetes mellitus: a critical review. ClinTher 2000; 22(10): 1151-68; discussion 1149-50. Erra-tum in : Clin Ther 2001; 23(2): 309.
18. Article not in English
(Note: NLM translates the title into English, enclosesthe translation in square brackets, and adds an abbre-viated language designator.)
Ellingsen AE, Wilhelmsen I. Sykdomsangst blantmedisin-og jusstudenter. Tidsskr Nor Laegeforen 2002;122(8): 785-7.
Personal Communication
Name of the person and date of communication shouldbe cited in parentheses in the text. For scientific ar-ticles, authors should obtain written permission andconfirmation of accuracy from the source of a personalcommunication.
Unpublished Material
19. In press
(Note: NLM prefers “forthcoming” because not allitems will be printed.)
Tian D, Araki H, Stahl E, Bergelson J, Kreitman M.Signature of balancing selection in Arabidopsis. ProcNatl Acad Sci USA. In press 2002.
Books and Other Monographs
20. Chapter in a book
Meltzer PS, Kallioniemi A, Trent JM. Chromosomealterations in human solid tumours. In: Vogelstein B,Kinzler KW, editors. The Genetic Basis of Human Cancer.New York: McGraw-Hill. 2002; pp 93-113.
21. Conference paper
Christensen S, Oppacher F. An analysis of Koza’scomputational effort statistic for genetic programming.In : Foster JA, Lutton E, Miller J, Ryan C, TettamanziAG, editors. Genetic programming. EuroGP 2002: Pro-ceedings of the 5th European Conference on Genetic Pro-gramming; 2002 Apr 3-5; Kinsdale Ireland. Berlin:Springer. 2002; pp 182-91.
22. Personal author(s)
Murray PR, Rosenthal KS, Kobayashi GS, Pfaller MA.Medical Microbiology; 4th ed. St. Louis: Mosby. 2002.
23. Editor(s), compiler(s) as author
Gilstrap LC (3rd), Cunningham FG, VanDorsten JP,editors. Operative Obstetrics. 2nd ed. New York:McGraw-Hill. 2002.
24. Author(s) and editor(s)
Breedlove GK, Schorfheide AM. Adolescent Pregnancy.2nd ed. Wieczorek RR, editor. White Plains (NY):March of Dimes Education Services; 2001.
25. Organization(s) as author
Royal Adelaide Hospital; University of Adelaide, De-partment of Clinical Nursing. Compendium of NursingResearch and Practice Development, 1999-2000. Adelaide(Australia): Adelaide University; 2001.
26. Conference proceedings
Harnden P, Joffe JK, Jones WG, editors. Germ celltumours V. Proceedings of the 5th Germ Cell TumourConference; 2001 Sep 13-15; Leeds, UK. New York:Springer; 2002.
27. Scientific or technical report
Issued by funding/sponsoring agency:
Yen GG (Oklahoma State University, School of Elec-trical and Computer Engineering, Stillwater, OK).Health monitoring on vibration signatures. Final re-port. Arlington (VA): Air Force Office of Scientific Re-search (US), Air Force Research Laboratory; 2002 Feb.Report No.: AFRLSRBLTR020123. Contract No.:F496209810049.
Issued by performing agency:
Russelll ML, Goth-Goldstein R, Apte MG, Fisk WJ.Method for measuring the size distribution of airborneRhinovirus. Berkeley (CA): Lawrence Berkeley Na-
76
tional Laboratory, Environmental Energy Technolo-gies Division; 2002 Jan. Report No.: LBNL49574. Con-tract No.: DEAC0376SF00098. Sponsored by the De-partment of Energy.
28. Dissertation
Borkowski MM. Infant sleep and feeding: a telephonesurvey of Hispanic Americans [dissertation]. MountPleasant (MI): Central Michigan University; 2002.
29. Patent
Pegedas AC, inventor; Ancel Surgical R& D Inc., as-signee. Flexible endoscopic grasping and cutting de-vice and positioning tool assembly. United Statespatent US 20020103498. 2002 Aug 1.
Other Published Material
30. Newspaper article
Tynan T. Medical improvements lower homicide rate:study sees drop in assault rate. The Washington Post.2002 Aug 12; Sect. A:2 (col. 4).
31. Audiovisual material
Chason KW, Sallustio S. Hospital preparedness forbioterrorism [videocassette]. Secaucus (NJ): Networkfor Continuing Medical Education; 2002.
32. Legal Material
Public law:
Veterans Hearing Loss Compensation Act of 2002,Pub.L.No. 107-9, 115 Stat. 11 (May 24, 2001).
Unenacted bill:
Healthy Children Learn Act, S. 1012, 107th Cong., 1stSess. (2001).
Code of Federal Regulations:
Cardiopulmonary Bypass Intracardiac Suction Con-trol, 21 C.F.R. Sect. 870.4430 (2002).
Hearing:
Arsenic in Drinking Water: An Update on the Science,Benefits and Cost: Hearing Before the Subcomm. onEnvironment, Technology and Standards of the HouseComm. on Science, 107th Cong., 1st Sess. (Oct. 4, 2001).
33. Map
Pratt B, Flick, P, Vynne C, cartographers. Biodiversityhotspots [map]. Washington: ConservationInternational; 2000.
34. Dictionary and similar references
Dorland’s Illustrated Medical Dictionary. 29th ed. Phila-delphia: W.B. Saunders; 2000. Filamin; p. 675.
Electronic Material
35. CD-ROM
Anderson SC, Poulsen KB. Anderson’s Electronic Atlasof Hematology [CD-ROM]. Philadelphia: LippincottWilliams & Wilkins; 2002.
36. Journal article on the Internet
Abood S. Quality improvement initiative in nursinghomes: the ANA acts in an advisory role. Am J Nurs[serial on the Internet]. 2002 Jun [cited 2002 Aug 12];102(6) : [about 3 p.]. Available from: http://www.nursingworld. org/AJN/2002/june/Wawatch.htm
37. Monograph on the Internet
Foley KM, Gelband H, editors. Improving palliativecare for cancer [monograph on the Internet].Washington: National Academy Press; 2001 [cited2002 Jul 9]. Available from: http://www.nap.edu/books/0309074029/html/.
38. Homepage/Web site
Cancer-Pain.org [homepage on the Internet]. NewYork: Association of Cancer Online Resources, Inc.;c2000-01 [updated 2002 May 16; cited 2002 Jul 9].Available from: http://www.cancer-pain.org/.
39. Part of a homepage/Web site
American Medical Association [homepage on theInternet]. Chicago: The Association; c1995-2002 [up-dated 2001 Aug 23; cited 2002 Aug 12]. AMA Office ofGroup Practice Liaison; [about 2 screens]. Availablefrom: http//www.ama-assn.org/ama/pub/category1736.html.
40. Database on the Internet
Open database:Who’s Certified [database on the Internet]. Evanston(IL): The American Board of Medical Specialists. c2000-[cited 2001 Mar 8]. Available from: http://www.abms.org/newsearch.asp
Closed database:Jablonski S. Online Multiple Congential Anomaly/Mental Retardation (MCA/MR) Syndromes [databaseon the Internet]. Bethesda (MD): National Library ofMedicine (US). c1999 [updated 2001 Nov 20; cited 2002Aug 12]. Available from: http://www.nlm.nih.gov/mesh/jablonski/syndrome_title.html
41. Part of a database on the Internet
MeSH Browser [database on the Internet]. Bethesda(MD): National Library of Medicine (US); 2002 - [cited2003 Jun 10]. Meta-analysis; unique ID: D015201;[about 3 p.]. Available from: http://www.nlm.nih.gov/mesh/MBrowser.html Files updated weekly.
MeSH Browser [database on the Internet]. Bethesda(MD): National Library of Medicine (US); 2002 - [cited
Guidelines to Authors 2012;Vol.53

2012;Vol.54 The Indian Journal of Chest Diseases & Allied Sciences 77
2003 Jun 10]. Meta-analysis; unique ID: D015201;[about 3 p.]. Available from: http://www.nlm.nih.gov/mesh/MBrowser.html Files updated weekly.
Correctness of the reference list is the entireresponsibility of the author (s).
Figures and Tables
Figures. Glossy print photographs (in triplicate) arerequired (usually 10 cm × 8 cm); good black and whitecontrast is essential for good reproduction. Allillustrations must be numbered and cited in the text.Legends should be provided for each illustration, listedon a separate page. All lettering must be doneprofessionally. Freehand or typed lettering is notacceptable. All figures should bear author’s name,short title and an arrow indicating top of the figure inpencil on the back of the photographs.
Colour illustrations must be paid by the authors.Please ask rates/charges from the Publication Office ofthe IJCDAS.
Tables. Each table should be typed double-spacedon a separate sheet. They should have an underlinedtitle followed by a legend, if any. Explanatory mattershould be in a footnote, not in the title. The approxi-mate position of each table in the text should beindicated in the margin of the manuscript.
Page Proofs and Reprints. A galley proof will be sentto the corresponding author which should be returnedwithin four days. Corrections should be limited toprinters errors only and no substantial additions/deletions should be made. No change in the names ofauthors (by way of additions and/or deletions) ispermissible at the proof stage. Twenty-five reprints of thearticle will be sent free of cost to the corresponding author.
Papers which have been accepted/published become theproperty of the Indian Journal of Chest Diseases and AlliedSciences and permission to re-publish them must be obtainedfrom the Editor.
CHECKLIST FOR SUBMISSION OF MANUSCRIPT
— Covering letter including copy-right release
— Three copies of typescript of the article on A-4 size paper
— Name and address of author responsible for correspondence about the manuscript, includinghighest degree and affiliations of each author.
— Abstract (upto 150 words) along with 3-6 key words
— Running title (5-6 words)
— Three glossy prints for each illustration (10 cm × 8 cm), appropriately labelled and eachillustration is cited in the text. Submit the legends on a separate sheet in the manuscript.
— Check all references for accuracy and completeness. Put references in proper format in numericalorder, making sure each is cited in the text.
The Indian Journal of Chest Diseases and Allied SciencesPublication DivisionV.P. Chest InstituteUniversity of Delhi
Delhi - 110 007
UNDERTAKING BY AUTHORS
We, the undersigned, give an undertaking to the following effect with regard to our article entitled
submitted for publication in the Indian Journal of Chest Diseases and Allied Sciences:
1. The article mentioned above has not been published or submitted to or accepted for publication in any form,in any other journal;
2. We also vouchsafe that the authorship of this article will not be contested by anyone whose name(s) is/are notlisted by use here; and
3. We also agree to the authorship of the article in following sequence:
Author’s Name(s) (in sequence) Signature of Author(s)1.
2.
3.
4.
5.
6.
7.
8.
IMPORTANT
1. All the authors are required to sign this form independently in the sequence given above.
2. Each author should have generated at least a part of the intellectual content of the paper.
3. Each author should be able to defend publicly in the scientific community, that intellectual content of the paperfor which he/she can take responsibility.
4. No addition/deletion/or any change in the sequence of the authorship will be permissible at a later stage.
Guidelines to Authors 2012;Vol.5478