2012/13 QOF QP Pathways Overview - Ipswich and East ... Area... · and attracts a £50 per plan...
35
1 2012/13 QOF QP Pathways For further information, please contact a member of the Commissioning Implementation Team: Clare Banyard, Head of Commissioning Implementation [email protected] , 01473 770011 or 07947 961753 Lorraine Parr, Commissioning Implementation Manager [email protected] , 01473 770141 or 07904 548855 Sarah Slade, Commissioning Implementation Manager Sarah.Slade @nhs.net 01473 770278 Emily Thurston, Commissioning Implementation Officer [email protected] , 01473 770246
Transcript of 2012/13 QOF QP Pathways Overview - Ipswich and East ... Area... · and attracts a £50 per plan...

1
2012/13 QOF QP Pathways
For further information, please contact a member of the Commissioning Implementation Team: Clare Banyard, Head of Commissioning Implementation [email protected] , 01473 770011 or 07947 961753
Lorraine Parr, Commissioning Implementation Manager
[email protected] , 01473 770141 or 07904 548855
Sarah Slade, Commissioning Implementation Manager Sarah.Slade @nhs.net 01473 770278
Emily Thurston, Commissioning Implementation Officer [email protected] , 01473 770246

2
2012/13 QOF QP Pathways Overview QP Indicator Pathway Overview of Pathway
QP8 Outpatient Referrals
Advice Letter Listing (ALL) and Clinical Management Service (CMS)
Advice Letter Listing applied to seven specialities in 2011/12 (gynaecology, urology, ENT, colorectal, pain management, rheumatology and cardiology). Amendments have been made to rheumatology pre-referral guidance. To roll out to other pathways during 2012/13, initially nephrology in the autumn. Clinical Management Service is a unique referral route for ENT, Endocrine (Lipids), GI & Liver (Gastroenterology), Gynaecology, Haematology and Urology at West Suffolk Hospital and has been running since October 2011. Paediatrics will be rolled out during October 2012.
Community Endoscopy
Community Endoscopy is a direct access non-two week wait community based gastroscopy (including transnasal endoscopy), flexible sigmoidoscopy and colonoscopy and was launched May 2012. The revised referral form was issued in September 2012.
OA Knees
The East Suffolk OA Knee Service is a Physio-led service for all patients with moderate or severe osteoarthritis (OA) of the knee. The service aims to ensure that patients get rapid access to the best conservative management, information and preparation prior to any surgery, to help them manage their symptoms and recover faster after surgery.
QP11 Emergency Admissions
Admission Prevention Pathways
A fast response to support patients who requires urgent health and/or social care within their own home. There are four services within this pathway; EAU, APS, COPD and DIST.
End of Life Care Advance Care Planning
In addition to the EOL Advance Care Planning Pilot which supports residential care/nursing homes and attracts a £50 per plan payment, the QOF QP pathway focuses on patients who reside in their own home (launched in August 2012), the same principles apply, however the £50 per plan payment is excluded.
Fall Assessments from East of England Ambulance Service
Focuses on patients identified by the East of England Ambulance Service Trust (EEAST) who have fallen. Fall notification forms are completed by EEAST and faxed to the GP practice. Practices are required to create a falls register, add the patient and discuss them if appropriate at their monthly Multi Disciplinary Team (MDT) meeting to ascertain if intervention from health and social care is appropriate.
QP14 A&E Attendances
Paediatric Acute Asthma/Wheeze Discharge Pilot
The pilot commenced on 20th August with Ipswich Hospital, providing a detailed management plan for patients who are discharged from hospital following admission for acute asthma/wheeze. Parents/guardians will leave with a copy of the plan and the practices will receive a faxed copy (the original will be posted). Upon receipt of this information practices are required to make an appointment if indicated with the parent for their child within a given timescale suggested by Ipswich Hospital in order for them to be followed up and managed in primary care with the Asthma Nurse.
Referral of Fall Assessments from Ipswich Hospital A&E (over 65’s)
Focuses on patients identified by Ipswich Hospital and West Suffolk Hospital A&E departments who have fallen and received a stage 2 risk assessment and practices will be notified through the discharge summary. Practices to add the patient to the falls register, discussing them if appropriate at their monthly MDT meeting to ascertain if intervention from health and social care is appropriate.
Referral of A&E Frequent Attenders
NHS Suffolk will provide monthly MDT information. This information will highlight patients who have attended A&E more than 4 times since January 2012. Practices will be required to review these patients and add them onto their monthly MDT meeting to ascertain if intervention from health and social care is appropriate. Practices will be able to invite Out Of Hours or EEAST to meetings if they feel there is sufficient need.

3
QOF QP8 Outpatient Referrals
Advice Letter Listing Page 4 - Nephrology Pre-Referral Guidance Community Endoscopy Page 6 - Referral form OA Knees Page 9
4
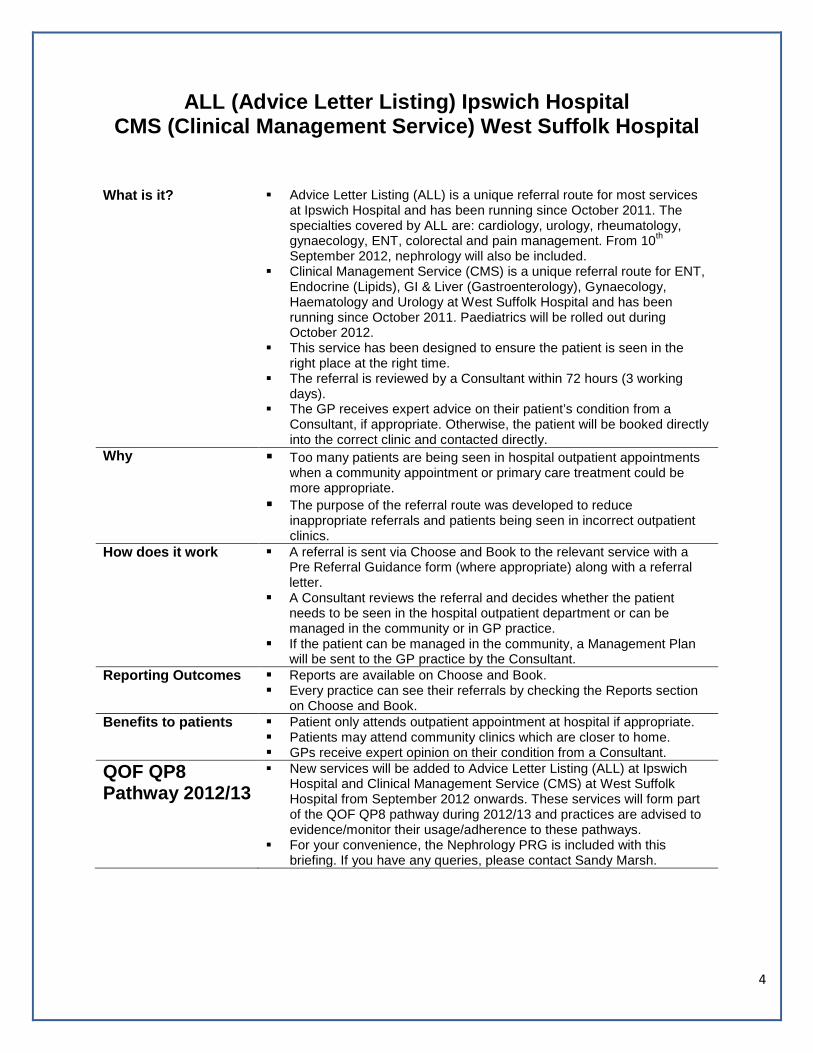
ALL (Advice Letter Listing) Ipswich Hospital
CMS (Clinical Management Service) West Suffolk Hospital
What is it? Advice Letter Listing (ALL) is a unique referral route for most services
at Ipswich Hospital and has been running since October 2011. The specialties covered by ALL are: cardiology, urology, rheumatology, gynaecology, ENT, colorectal and pain management. From 10th September 2012, nephrology will also be included.
Clinical Management Service (CMS) is a unique referral route for ENT, Endocrine (Lipids), GI & Liver (Gastroenterology), Gynaecology, Haematology and Urology at West Suffolk Hospital and has been running since October 2011. Paediatrics will be rolled out during October 2012.
This service has been designed to ensure the patient is seen in the right place at the right time.
The referral is reviewed by a Consultant within 72 hours (3 working days).
The GP receives expert advice on their patient’s condition from a Consultant, if appropriate. Otherwise, the patient will be booked directly into the correct clinic and contacted directly.
Why Too many patients are being seen in hospital outpatient appointments when a community appointment or primary care treatment could be more appropriate.
The purpose of the referral route was developed to reduce inappropriate referrals and patients being seen in incorrect outpatient clinics.
How does it work A referral is sent via Choose and Book to the relevant service with a Pre Referral Guidance form (where appropriate) along with a referral letter.
A Consultant reviews the referral and decides whether the patient needs to be seen in the hospital outpatient department or can be managed in the community or in GP practice.
If the patient can be managed in the community, a Management Plan will be sent to the GP practice by the Consultant.
Reporting Outcomes
Reports are available on Choose and Book. Every practice can see their referrals by checking the Reports section
on Choose and Book. Benefits to patients Patient only attends outpatient appointment at hospital if appropriate.
Patients may attend community clinics which are closer to home. GPs receive expert opinion on their condition from a Consultant.
QOF QP8 Pathway 2012/13
New services will be added to Advice Letter Listing (ALL) at Ipswich Hospital and Clinical Management Service (CMS) at West Suffolk Hospital from September 2012 onwards. These services will form part of the QOF QP8 pathway during 2012/13 and practices are advised to evidence/monitor their usage/adherence to these pathways.
For your convenience, the Nephrology PRG is included with this briefing. If you have any queries, please contact Sandy Marsh.

5
Please tick the reason for referral and that the pre-referral tasks have been completed Reason for referral (tick boxes)
Stage 4 and 5 CKD (with or without diabetes) Proteinuria (ACR >70mg/mmol or PCR >100mg/mmol) unless known to be due to diabetes and appropriately treated Proteinuria (ACR >30mg/mmol or PCR >50mg/mmol) together with dipstix positive haematuria Rapidly declining eGFR (for those patients with CKD3 or worse, >5ml/min in 1 year, or >10ml/min within 5 years) Poorly controlled hypertension despite at least 3 antihypertensive agents and abnormal renal function or +ve urine findings People with, or suspected of having, rare or genetic causes of CKD Suspected renal artery stenosis (this may include asymmetrical kidneys of >1.5cm, significant deterioration of renal function
on starting ACEi or ARB i.e eGFR decrease of >25% or plasma creatinine increase >30%)
Work to be completed before referral (tick boxes) Blood tests FBC Renal function Bone profile LFT Glucose Urine tests Urine dipstick ACR or PCR on a spot urine sample MSU Renal USS Report must be attached to referral
Offer a renal U/S to all people with CKD who have • Progressive CKD • Visible or persistent invisible haematuria • Symptoms of urinary tract obstruction • Family history of polycystic kidney disease and aged more over 20 • Stage 4 or 5 CKD
If you feel it might be useful
Vasculitis screen (ANA, ANCA, C3, C4, GBM)
Myeloma screen (serum protein electrophoresis, urine for Bence Jones protein)
Clinical Indication/Problem (attached)
Relevant Past Medical History - include previous & current treatment/medication where relevant (attached)
Current Medication (attached)
Allergies (attached)
ALL Suffolk Pre-Referral Guidance Nephrology
This form should be attached electronically to your referral letter and any investigations (see below) and submitted via C&B to the IHT Advice Letter Listing Nephrology Clinic
Patient Information
Name: ………………………………………………………………. Address: ……………………………………………………………. ………………………………………………………………….…….. ………………………………………………………………….…….. Tel (Home): …………………….. (Mbl): ………………………... NHS No: ………………………. DOB: ………………………... Gender: ……………………….. UBRN: ……………………….
GP Information GP Name: ………………………………………………………… Practice address: ………………………………………………….. ………………………………………………………………….… ………………………………………………………………….… Tel: ……………….…….……….. Fax:……………..……..…... Referral date:……………………………………………………….. Referrer name: …………………………………………………… Referrer signature: …………………………………………………

6
Community Endoscopy Service
What is it? Direct access non-two week wait community based gastroscopy (including transnasal endoscopy), flexible sigmoidoscopy and colonoscopy.
Delivered from a new dedicated unit at Ravenswood (next to the GP practice) – starting Mid-May 2012.
Waiting times 2-4 weeks, daily sessions and 14% less expensive than a secondary care referral.
Integrated with IHT for onward referral (e.g. MDTs) and provides additional capacity
Scope of service Included Lower GI conditions (which do not full fill 2 WW criteria):
Persistent diarrhoea with or without bleeding Anal symptoms/ rectal bleeding Left sided abdominal pain Persistent change in bowel habit Surveillance of long term conditions and polyp disease Unexplained anaemia
Upper GI conditions (which do not full fill 2 WW criteria): Patients who have resistant H.pylori infection and/or worsening
dyspepsia in spite of appropriate treatment Post-treatment (6-8 weeks) for gastric or oesophageal ulcer and
bleeding duodenal ulcer Coeliac disease for confirmatory biopsy Barrett’s oesophagus surveillance Follow up of oesophageal and gastric ulcers Unexplained anaemia Dyspepsia Reflux symptoms, where appropriate Patients 6 weeks after oesophageal ulceration or histological
evidence of dysplasia Banding of Haemorrhoids
Persistent, troublesome, rectal bleeding Diagnostic Endoscopy
Trans nasal endoscopy (including biopsy) Oral upper endoscopy (including biopsy) Flexible Sigmoidoscopy (including biopsy and polypectomy) Colonoscopy (including biopsy and polypectomy)
Therapeutic Endoscopy Polypectomy including tattooing
Excluded Significant acute GI bleeding – immediate referral to secondary care Children
The provider ‘Prime Diagnostics’
Founded by a GP and with a full understanding of the needs of primary care. Pioneered community based endoscopy from Braintree in 2004.
Now runs 11 dedicated units delivering >10,000 scopes per annum and initiatives to reduce waiting lists e.g. IHT & Guys & St. Thomas’.
Quality features: o All units are JAG compliant (Joint Advisory Group for
endoscopy). o High scores (A’s and B’s) on the Global Rating Scale. o All endoscopists training to British Society of Gastroenterology
(BSG) standards. o Pioneered the use of transnasal which reduces sedation rates
Preferred Hospital if Referral to Secondary Care is Necessary: ………………………………………………………………….
7
and generates high patient satisfaction. Fully integrated with IHT e.g. MDTs
How to refer? C&B using the referral form attached (which will be on your clinical system). Please telephone the number below if you need telephone advice before referring.
All referrals triaged by an endoscopist to ensure they are clinically appropriate. If the referral needs to be seen in secondary care it will be forwarded directly and the GP practice informed.
Patients have choice and can be referred to IHT directly Reporting All Endoscopies will be fully reported:
o If no suspected serious pathology found report back to the practice, via NHS email, on the day of the scope. If relevant the endoscopists will provide management advice and arrange follow ups.
o If serious suspected pathology during is found during the procedure, the endoscopists will advise the patient, contact the GP by telephone and make a two week referral to the patient’s choice of hospital.
o If serious pathology is found at histology the patient will be given an appointment at the next session and then referred to the hospital of their choice on a two week wait.
o For those patients requiring follow up, e.g. patients with polyps, the service will actively manage their surveillance needs in accordance with BSG guidelines
o If a serious condition, such as Crohn’s disease, is found on scoping; a management plan and the results will be reported back to the GP practice on the same day.
Benefits to patients Short waiting times. Dedicated brand new unit designed for patient comfort. Easy to park – no charges. Generous timeslots - most patients seen on time as only routine
referrals accepted. Integrated onward pathways with secondary care.
Contact details Unit address - 1st Floor, 22 Hening Avenue, Ravenswood, Ipswich IP3 9QJ
Admin team 01449 776008 (Fax 01449 776009) [email protected] www.primediagnostics.co.uk

8
COMMUNITY ENDOSCOPY REFERRAL Unit address - 1st Floor, 22 Hening Avenue, Ravenswood, Ipswich IP3 9QJ Admin team 01449 776008 (Fax 01449
776009) [email protected]
Patient ID Name: Date of birth: NHS number: Address: Post code Telephone: Mobile No: Gender: Physical/communication difficulties (specify if any e.g poor vision/loss of hearing): If Interpreter required, language?
Referring Clinician GP Name: Practice Address: Urgent Telephone *: Fax *: * for clinical enquiries use only Date of Referral : Referrer’s Signature:
Presenting Problem: Relevant Past Medical History: PLEASE TICK BOX(ES)
Type of Scope required
Anaemia
Rectal Bleeding
Anticoagulants
Known Bowel Disease
Unintentional Weight Loss
Dysphagia
Renal Disease
Respiratory Disease
Heart Disease
Diabetes Mellitus Current Medication: Blood test results:
Upper Lower
If YES please tick relevant boxes:
Bright red Mixed with stool Pain No Pain
If YES, latest INR and date:
If YES please state here:
If YES please state here how much/duration:

9
Allergies:
East Suffolk OA Knee Service
What is it? A physiotherapist-led service for all patients with moderate or advanced
osteoarthritis of the knee. The service is provided by either Allied Health Professionals Suffolk (AHPS) or Ipswich Hospital Trust (IHT).
Aims are to improve access earlier to pre-operative information, prepare patients to manage their condition, offer alternatives to surgery and improve post-operative recovery.
Referral process
Patients with suspected malignancy must be referred directly to acute care using the 2 week wait pathway
GP completes a referral form along with the Oxford Knee Score questionnaire which is completed by the patient. Both documents need to be sent to either: - AHPS via fax to 01379 873738 or IHT via Choose and Book clinic East
Suffolk OA Knee Service Please attach any relevant X-Ray reports if applicable For adults with acute knee pain, be alert for ‘red flags’ that may indicate a more
serious medical condition as the source of pain. Please refer these patients directly to secondary care for immediate investigation.
10
Service Delivery - The providers will determine the severity of the OA knee from the Oxford Knee Score questionnaire and will contact the patient to issue an appointment.
- Patients classed as moderate will be assessed by an experienced physiotherapist within 4 weeks of referral and within 2-4 weeks if classed as severe.
- Physio sessions will start within four weeks of the first Physio-led Assessment - The Service includes the following: - Stage 1 Programme up to 5 group physio sessions for those with moderate
or advanced OA (these sessions cover education and advice around OA knee, total knee replacement surgery, pain management, exercise, weight management and the benefit of aids. Patients will also be taken through an exercise programme specifically aimed at improving their strength, flexibility and mobility).
- Stage 2 Programme up to 3 individual (1:1) physio sessions for advanced or severe OA (these sessions also cover advice and education around pain management, exercise therapy and aids, but we also aim to fully prepare patients for surgery prior to referral to secondary care).
- The 1:1 sessions may be substituted for group sessions at the discretion of Ipswich Hospital Trust or AHPS.
- Stage 1 and Stage 2 Programmes are both able to :- - The physios will make urgent consultant referrals where necessary. - Any patient assessed and deemed to be in the early/mild stages of OA will be
referred into routine musculoskeletal physiotherapy. - If early/mild stage of OA, patient referred back to GP with advice & guidance. - Physiotherapists will provide written notification to the referring GP once the
patient enters the Physio part of the pathway and when a patient is discharged or referred on for an urgent consultant appointment.
- Patients referred to IHT will be seen at IHT Physiotherapy Department - IHT sessions will be held weekly.
- Patients referred to AHPS will be seen at one the following locations convenient to the patients location: Ipswich (Riverside Clinic) Stowmarket, Woodbridge, Felixstowe, Aldeburgh, Hartismere Health Centre and Hadleigh Health Centre - AHPS sessions will be held weekly.
Benefits The pathway empowers patients to make informed decisions about their care and the timing of their surgery (if surgery is applicable) as well as providing support and guidance throughout the patient journey.
The evidence suggests that patients who are provided with pre-operative education and exercise have significantly greater benefits from surgery with fewer complications.
Launch details 13 practices across Ipswich and East Suffolk will commence with a ‘soft launch’ with effect from 12th November 2012.
The remaining practices will commence from 22nd November 2012 following the T&O Training and Education afternoon.
Contact details AHPS Riverside Clinic, Landseer Road, Ipswich IP3 0AZ Tel: 01473 301064 Mob: 07940 471604 – Grace Allston
IHT, Musculoskeletal Physiotherapy Outpatients, Heath Road, Ipswich, IP4 5PD Tel: 01473 703312 - Sue Voules
11
East Suffolk Knee Service Referral Form
SUSPECTED CANCER PLEASE NOTE THAT ALL SUSPECTED CANCER CASES SHOULD BE REFERRED DIRECTLY TO HOSPITAL IN LINE WITH THE TWO WEEK WAIT ARRANGEMENTS CURRENTLY IN PLACE Date of referral: Service provider required (please tick one box):
AHPS – Allied Health Professionals Suffolk Riverside Clinic, Ipswich Stowmarket Woodbridge Felixstowe Aldeburgh Hadleigh Hartismere HC
Ipswich Hospital Trust, Heath Road, Ipswich
Referral to be sent via Choose and Book to clinic:
12
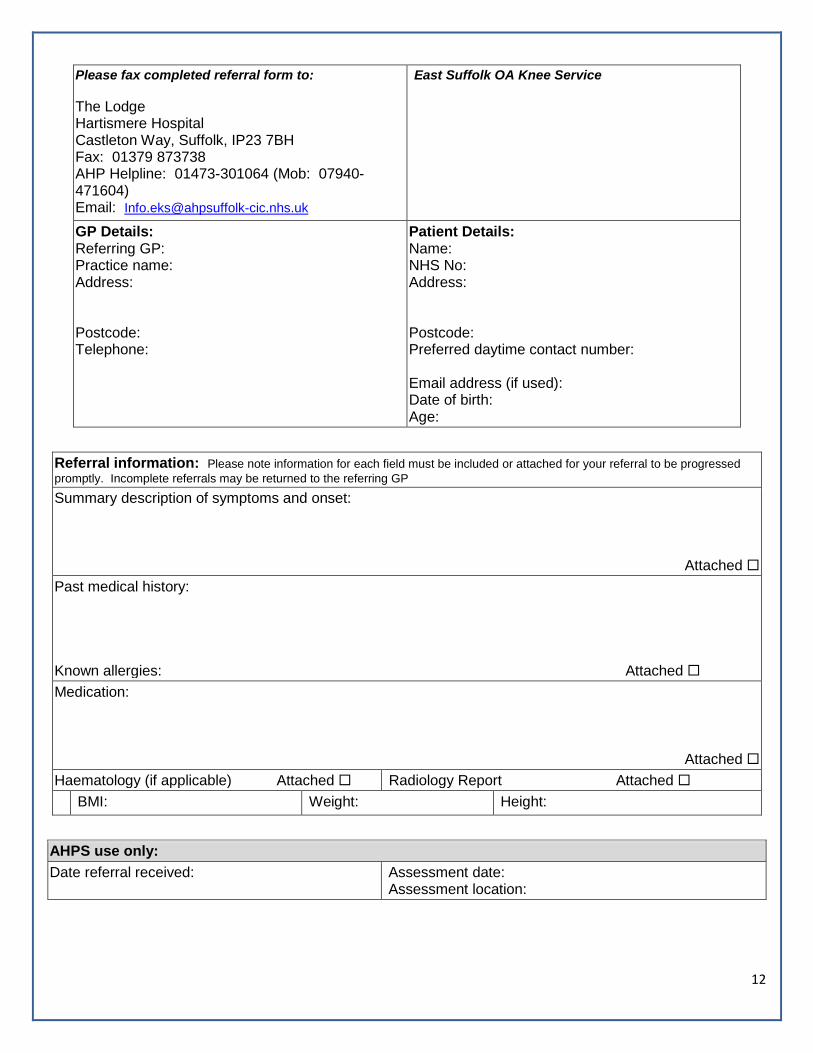
Please fax completed referral form to: The Lodge Hartismere Hospital Castleton Way, Suffolk, IP23 7BH Fax: 01379 873738 AHP Helpline: 01473-301064 (Mob: 07940-471604) Email: [email protected]
East Suffolk OA Knee Service
GP Details: Referring GP: Practice name: Address: Postcode: Telephone:
Patient Details: Name: NHS No: Address: Postcode: Preferred daytime contact number: Email address (if used): Date of birth: Age:
Referral information: Please note information for each field must be included or attached for your referral to be progressed promptly. Incomplete referrals may be returned to the referring GP Summary description of symptoms and onset:
Attached Past medical history: Known allergies: Attached Medication:
Attached Haematology (if applicable) Attached Radiology Report Attached BMI: Weight: Height:
AHPS use only: Date referral received: Assessment date:
Assessment location:
13
Outcome:
Stage 1 Stage 2 Community MSK Ipswich Hospital Trust use only: Date referral received: Assessment date:
Assessment location: Outcome:
Stage 1 Stage 2 Community MSK
14
Admission Prevention Pathways
Services Delivered There are a number of admission prevention initiatives across the
county. The aims of all of these admission prevention initiatives are aligned to the principles of ‘the right care in the right place, at the right time’ and ‘care closer to home’. Admission Prevention Service (APS) Coordination of health and/or social care in the community in order
to prevent an unnecessary admission and referral to Specialist Services.
Administration of IV Antibiotics and Sub-Cut Infusions in the community.
Anti-coagulation management including administration of oral vitamin K, monitoring of unstable INR in the community.
QOF QP11 Emergency Admissions
Admission Prevention Pathways Page 14
- Overview of pathways End of Life Advance Care Planning Page 17
- Claim form Fall Assessments from East of England Ambulance Services Page 21
- Falls Notification Form
15
First catheterisations in the community following medical assessment and management of blocked catheters (out of hours) on behalf of community nursing teams.
Emergency Assessment Unit (EAU) Acute hospital consultant-led service for advice regarding
emergency admissions and the arrangement of urgent appointments (same day or next day) in order to prevent an unnecessary admission.
Where onward referral to APS is recommended, the overarching clinical accountability remains with EAU.
Chronic Obstructive Pulmonary Disease Service (COPD) Admission avoidance service through same day assessment within
the community for people experiencing acute exacerbation of COPD.
Undertaking community pulmonary rehabilitation. Undertaking home oxygen assessments for all conditions. Dementia Intensive Support Team (DIST) Providing assessment, advice and support where there is acute
exacerbation of dementia in order to prevent an unnecessary admission.
How to Refer GPs can telephone each admission prevention service directly to make a referral. APS – Hours 24/7 Ipswich & East Office – 01473 704259 Mobile – 07970847449 Fax – 01473 704152 West Office – 01284 718250 Mobile – 07985 365544 Fax – 01284 718275 EAU – Hours Mon-Fri 0900-1900 Ipswich & East EAU Consultant – 01473 712233 and ask to bleep 620 West EAU Consultant - 01284 712712 COPD Office – 01284 712705 Fax – 01284 712557 Hours – Mon-Fri, 0800 – 1830 & Sat-Sun, 0800 – 1600 DIST Ipswich & East Hours Mon-Fri 0900-1700 Mobile – 07852 769172 West Hours Mon-Fri 0800-1800 Office - 01284 733260 Fax - 01284 733278
Action for Practices
To use the APS, EAU, DIST and COPD services for patients who are clinically appropriate within practice opening hours for referrals in order to prevent unnecessary emergency admissions.
To display Admission Prevention Pathways chart in all appropriate consulting rooms (laminated copies are available via the Commissioning Implementation Team).
Contact Details Mark Cooke, Transformational Lead. [email protected] or Tel: 01473 770292 Mob: 07940 477270
16
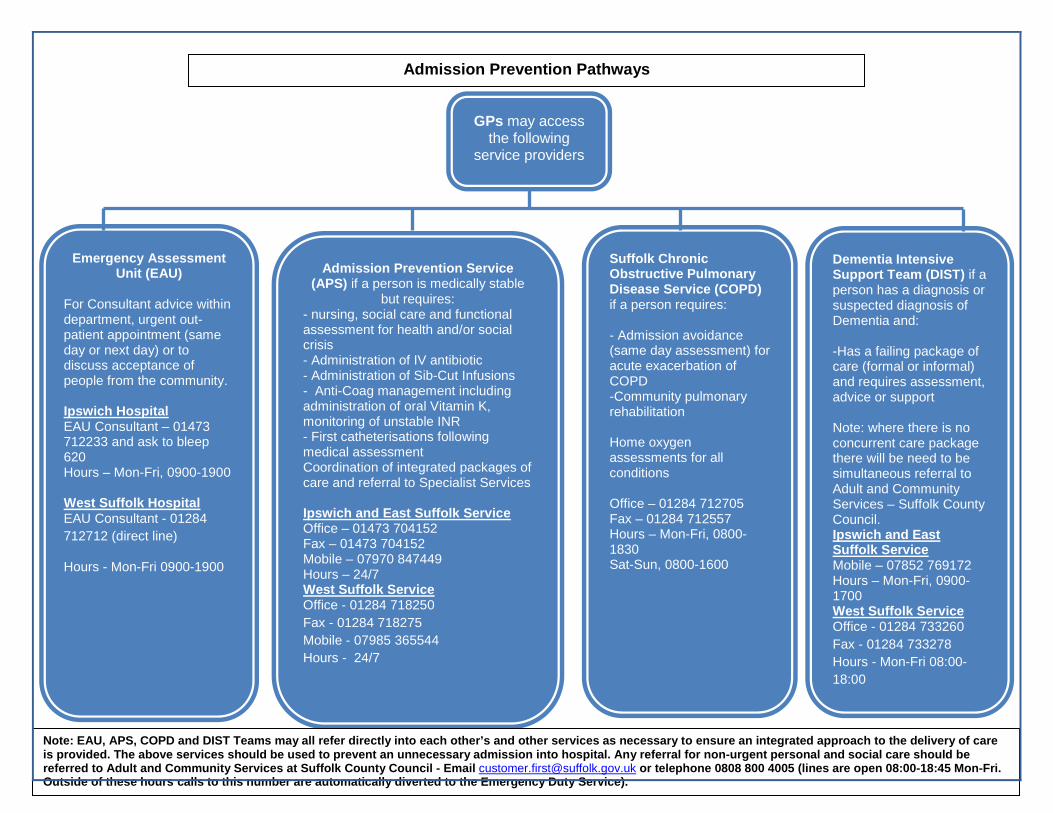
Admission Prevention Pathways
GPs may access the following
service providers
Emergency Assessment Unit (EAU)
For Consultant advice within department, urgent out-patient appointment (same day or next day) or to discuss acceptance of people from the community. Ipswich Hospital EAU Consultant – 01473 712233 and ask to bleep 620 Hours – Mon-Fri, 0900-1900 West Suffolk Hospital EAU Consultant - 01284 712712 (direct line)
Hours - Mon-Fri 0900-1900
Admission Prevention Service (APS) if a person is medically stable
but requires: - nursing, social care and functional assessment for health and/or social crisis - Administration of IV antibiotic - Administration of Sib-Cut Infusions - Anti-Coag management including administration of oral Vitamin K, monitoring of unstable INR - First catheterisations following medical assessment Coordination of integrated packages of care and referral to Specialist Services Ipswich and East Suffolk Service Office – 01473 704152 Fax – 01473 704152 Mobile – 07970 847449 Hours – 24/7 West Suffolk Service Office - 01284 718250 Fax - 01284 718275 Mobile - 07985 365544 Hours - 24/7
Dementia Intensive Support Team (DIST) if a person has a diagnosis or suspected diagnosis of Dementia and: -Has a failing package of care (formal or informal) and requires assessment, advice or support Note: where there is no concurrent care package there will be need to be simultaneous referral to Adult and Community Services – Suffolk County Council. Ipswich and East Suffolk Service Mobile – 07852 769172 Hours – Mon-Fri, 0900-1700 West Suffolk Service Office - 01284 733260 Fax - 01284 733278 Hours - Mon-Fri 08:00-18:00
Suffolk Chronic Obstructive Pulmonary Disease Service (COPD) if a person requires: - Admission avoidance (same day assessment) for acute exacerbation of COPD -Community pulmonary rehabilitation Home oxygen assessments for all conditions Office – 01284 712705 Fax – 01284 712557 Hours – Mon-Fri, 0800-1830 Sat-Sun, 0800-1600
Note: EAU, APS, COPD and DIST Teams may all refer directly into each other’s and other services as necessary to ensure an integrated approach to the delivery of care is provided. The above services should be used to prevent an unnecessary admission into hospital. Any referral for non-urgent personal and social care should be referred to Adult and Community Services at Suffolk County Council - Email [email protected] or telephone 0808 800 4005 (lines are open 08:00-18:45 Mon-Fri. Outside of these hours calls to this number are automatically diverted to the Emergency Duty Service).

17
End of Life Advance Care Planning
What is it? An End of Life Advanced Care Planning pilot commenced in 2011 with East Suffolk practices.
The evaluation of the pilot has proved successful and a decision has been made by the CCG to continue the pilot until March 2013 with East Suffolk practices.
Ipswich practices are being invited to participate in the pilot with effect from September 2012 until March 2013.
The pilot requires practices to identify patients in residential care and nursing homes for whom end of life care planning is appropriate, prepare plans/Yellow Folders which includes completing key documents such as DNACPR, and notify the Ambulance and OOH services. The payment for this is £50 per plan.
For patients whose place of residence is not a residential care/nursing home, i.e. their own home, the CCG agreed that it would be sensible to extend the End of Life Advanced Care Planning pilot as a QOF QP11 pathway.
Why The End of Life pilot was designed and initiated by Dr Paul Driscoll at Haven Health Practice in July 2011. The pilot aimed to use Advance Care Planning (ACP) within practices in East Suffolk.
Patients at the end of life are often admitted to hospital to die causing unnecessary distress, use of services and cost. A key objective of the pilot is therefore to shift the place of death from hospital to hospices or care homes by 10% through the implementation of ACP.
How does it work Practices are asked to: Identify patients likely to die within 12 months and, where a GP feels
appropriate, initiate a discussion about their end of life care wishes with patient/family/carers.
The patients’ wishes are used to develop a care plan and this is recorded in the patient notes, which is held in a Yellow Folder and kept with the patient.
If applicable, an EoE DNACPR form is completed and faxed to the Ambulance Service on 01234 215399.
A Harmoni OOH form/Special Patients Notes is completed, preferably via Adastra.
If applicable, patient is added to the practice Palliative Care Register and (when available) patient is added to the Electronic Palliative Care Coordinating System (EPCCS).
Attend relevant GP training sessions on end of life care planning. This training is also provided to ambulance, residential care/nursing homes and Harmoni staff.
Practices are paid £50 per care plan for patients who reside in a residential care/nursing home. For those patients who reside in other abodes, a £50 payment will not be made however practices can use the claim form to support their evidence for QOF QP11.
Practices are asked to complete and send their claim forms to: Emily Thurston, Ipswich and East Suffolk CCG, Rushbrook House, Paper Mill Lane, Bramford IP8 4DE on a monthly basis.
Reporting Outcomes
Upon receipt of any claim forms, information will be recorded on a database. The forms will be forwarded on to the Finance team to initiate a payment.
With effect from October 2012, a monthly update will be provided to practices detailing their activity. This will be split between patients who reside in a residential care/nursing home (and have received a payment), and patients who reside in another abode (which practices can consider using as part of their QPF QP11 evidence).
18
Benefits to patients Improves the quality of end of life care for patients and their families by improving communication, the coordination of care and their overall experience and satisfaction.
The pilot will also have a positive impact on utilisation of clinical services by reducing emergency admissions, length of stay, use of unnecessary treatments and healthcare costs.

19
End of Life Advanced Care Planning Claim Form A national read-code has been requested for: ‘Patient Held Palliative Care Record’. Once this is available practices will be notified.
Practice Name NHS Number Patient Residence (Please tick) Own Home [ ] Please note this relates to QOF QP11 and no additional claim Residential Care/Nursing Home [ ] Please note payment will only be made for those patients in a Residential care/Nursing home Residential Care/Nursing Home Address (if applicable)
Medical Condition/s (Please tick)
Cancer [ ] Chronic Condition [ ] Dementia/Frailty [ ]
Choice of place of death Note: this is captured at the time of completing this form and is subject to change
GP discussed end of life issues with Residential Care/Nursing Home MDT meeting (if applicable) GP discussed resuscitation status, end of life issues, and place of care/death with patient/family/carers End of life plan completed & yellow folder in place EoE DNACPR form completed (if applicable) (and faxed to 01234 215399)
Tick: [ ] Date: Date: Date:
Harmoni OOH form/Special Patient Notes completed (via Adastra) (if applicable) End of life drugs package arranged (if applicable) (Please see reverse of form and note this is an aide memoir only and is to help GPs and will not necessarily be needed) Patient added to practice palliative care register (if applicable) Patient added to electronic palliative care coordinating system (EPCCS) when available (if applicable)
Tick: [ ] Tick: [ ] Date: Date:
Useful Contacts Admission Prevention Service 01473 704259
One Call 0800 567011 or;
OOH 0300 130 3066 www.stelizabethhospice.org.uk
Please return completed claim form for the attention of Emily Thurston at Rushbrook House, Paper Mill Lane, Ipswich, IP8 4DE for payment purposes

20
“JUST IN CASE” DRUGS – LIST FOR END OF LIFE
Diamorphine Haloperidol Levomepromazine Midazolam Hyoscine Butyl Bromide Water for Injection
5 MG x 5 AMPS 5 MG/ML 5 AMPS 25 MG/ 5 ML 5 AMPS 10 MG / 2 ML 5 AMPS 20 MG / MP 5 AMPS 10 ML 10 AMPS
*(CD) *(CD)
To access the DNACPR (Do Not Attempt Cardiopulmonary Resuscitation) documents, go to: www.suffolk.nhs.uk/palliativecare To access the e-learning programme:
• Go to www.eoe.nhs.uk • Scroll down the left hand side to a purple box called “Changing Our NHS Together” • Select work stream “End of Life Care” and click “GO” • Select “DNACPR” in the left column where all the documents can be found • The documents that can be found on the webpage are: DNACPR Form & flowchart, DNACPR Patient
Leaflet, DNACPR East of England Policy & Frequently Asked Questions sheet • At the bottom of this page is a link to access the e-learning programme • NB-You may have to register with EOE to access the e-learning programme. On completion of the
training a certificate can be printed off for each staff member

21
Fall Assessments from East of England Ambulance Services
What is it? A process to ensure that falls assessments carried out by East of England
Ambulance Services Trust (EEAST) are included in the monthly practice MDT meetings for discussion (if appropriate) by adding them to a falls register.
These patients are discussed to decide if any further action is required to help prevent future falls and/or a potential emergency admission.
The process will commence from 1st October 2012 and falls data will be issued to practices from the end of September 2012.
The process Every time the ambulance service is called out to see a patient who has fallen, regardless of whether that patient is conveyed to hospital or not, EEAST complete a falls notification.
The falls notification captures not only the patient’s demographics but also key clinical information about the event.
The ambulance crew ask the patient a variety of questions and the answers provide valuable information along with why the patient may have fallen:
Is the patient taken to hospital? Which hospital? Does the patient live alone? Has the patient had a fall in the previous year? How many (estimated)? Where did the fall occur? Do they take 4 or more medications daily? Does the patient have a history of Stroke or Parkinson’s? Does the patient have problems with balance? Any difficulty in rising from a chair of knee height? Has the patient complained of blackouts/loss of consciousness? Was the AMT score normal or reduced? Does the patient have suspected Atrial Fibrillation? Have you notified any other service about this patients fall? Which
service? EEAST fax the falls notification to the GP practice for their information. The practice adds the details from the falls notification to their falls
register. EEAST will send a list of all patients who have fallen each month to NHS
Suffolk. The patients will be added to the monthly PARR++ data and is sent out to the practice so they can include this in their MDT meetings for discussion.
Action for practices Upon receipt of either the Falls Notification from EEAST or the monthly falls MDT data, practices are to create a falls register for these patients.
The register should include the following as a minimum: - Name - NHS Number - DOB - EMIS/SystmOne number (if applicable) - Fall date (as per either the EEAST Falls Notification or A&E discharge
summary) - Source of information (e.g. EEAST or A&E) - Date discussed at MDT

22
The practice to use the register, along with the monthly MDT data and gather any other relevant information needed to enable these patients to be discussed at their MDT meetings.
The practice will take brief notes/actions points from these discussions.
Launch details The process will start from 1st October 2012 EEAST falls data will be included as part of the monthly MDT data sent to
practices from the end of September 2012
Contact details For any queries on the process, please contact [email protected] For any queries on the data, please contact
23
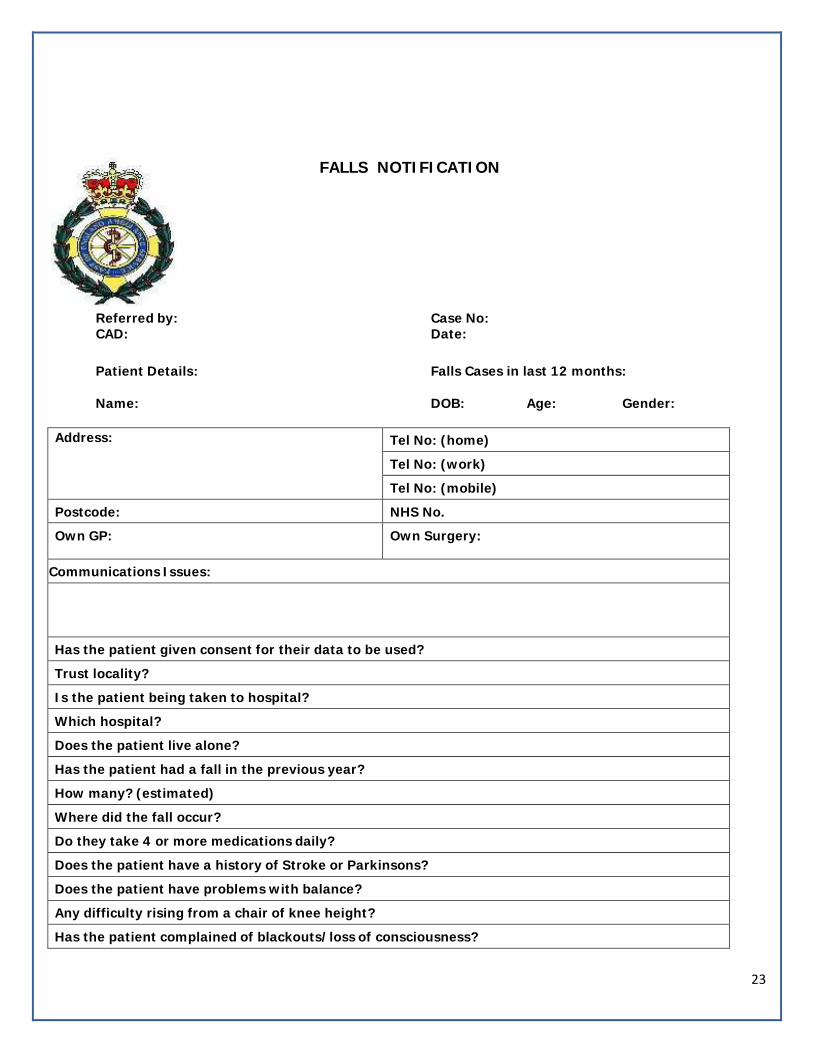
FALLS NOTIFICATION
Referred by: Case No: CAD: Date:
Patient Details: Falls Cases in last 12 months:
Name: DOB: Age: Gender:
Address: Tel No: (home) Tel No: (work) Tel No: (mobile)
Postcode: NHS No. Own GP: Own Surgery:
Communications Issues:
Has the patient given consent for their data to be used? Trust locality? Is the patient being taken to hospital? Which hospital? Does the patient live alone? Has the patient had a fall in the previous year? How many? (estimated) Where did the fall occur? Do they take 4 or more medications daily? Does the patient have a history of Stroke or Parkinsons? Does the patient have problems with balance? Any difficulty rising from a chair of knee height? Has the patient complained of blackouts/loss of consciousness?
24
Was the AMT score normal or reduced Does the patient have suspected AF? Have you notified any other service about this patients fall?
Which Service? Additional Information
QOF QP14 A&E Attendances
Paediatric Acute Asthma/Wheeze Discharge Pilot Page 25
- Discharge Management Plan - Monitoring form
Falls Assessments from Ipswich Hospital A&E Page 29
- Example of wording on A&E electronic discharge summary - Ipswich Hospital Falls Screening Assessment
A&E Frequent Attenders Page 32 - Example of data pack with explanatory text

25
Paediatric Acute Asthma/Wheeze Discharge Pilot
What is it? A management plan for paediatric patients who are discharged from hospital following admission for acute asthma/wheeze.
The plan aims to ensure all patients discharged are followed up by either their GP practice or Ipswich Hospital.
The pilot will enable GP practices to robustly monitor where patients should be followed up, provide a safety net to ensure appropriate follow up and capture data for evaluation purposes.
The management plan has been created in partnership with Ipswich Hospital and GPs in the Ipswich and East Suffolk CCG.
This pilot is due to commence on 20th August until the end of October 2012 to enable the process to be tested and amended if required.
Why NICE guidance states that paediatric patients suffering from acute asthma/wheeze should be seen in 24/48 hours following discharge. In reality this is a small number of patients who, for clinical reasons, need to be seen urgently.
The purpose of the pilot is to identify when and where patients need to be followed up and the timescales involved.
To increase self-care and education for patients and their parents/guardians .
Managing patients in the most appropriate environment – only using Ipswich Hospital services when clinically necessary.
How does it work Upon discharge, Ipswich Hospital will complete the Management Plan, which includes actions required by Practice staff. The plan will state whether; - The patient is to be seen urgently by Ipswich Hospital and include a
date and time of the appointment - The patient is to be seen by staff in their GP practice within a given
timescale i.e. between xx to xx no. of days or weeks depending on the urgency
- The patient is to be seen routinely by Ipswich Hospital and include a date and time of appointment
The management plan and actions which will include medication will be sent to the practice electronically as per other hospital discharge summaries.
A copy of the management plan and actions will be given to the patient’s parent/guardian for their information and action.
There is self care information included on the bottom of the management plan for parents/guardians to use based upon their child’s symptoms.
It is expected that the patient’s parent/guardian will contact their GP practice to arrange a follow up appointment if required, stating the timescale required, as indicated above (between xx to xx no. of days or weeks).
So patients are not missed, practice staff are asked to contact the

26
parent/guardian if no appointment is made. Reporting Outcomes
Pilot practices are required to complete a Monitoring Form for every patient where a hospital management plan is received and fax to 01473 770201 at the end of every month
For the pilot, Ipswich Hospital will provide a list of patients discharged with asthma/wheeze who are registered with the practices
The CCG will evaluate the pilot to establish if any changes need to be made
The final version will be rolled out to all practices in within Ipswich and East Suffolk CCG and will form part of the 2012/13 QOF QP14 pathway
Benefits to patients All patients and parents/guardians will leave the hospital with either an urgent follow up appointment or details of how to book a routine follow up appointment with their GP practice or Ipswich Hospital
Parents/guardians will know clearly what they should do if their children’s health/condition changes
Re-admissions to hospital should reduce as follow up care will be managed in a more timely manner, with patients being seen by the right service and at the right time
Patients and parents/guardians will be better informed about their care

27
Management plan and actions required upon discharge of paediatric patients with Acute Asthma/ wheeze
Name: Hospital Number: Dob: Admission date: NHS number: Discharge date: Named Consultant: Diagnosis: Follow up at Ipswich Hospital (if required)
An appointment has been made on xxx/xxx (date/time) for the patient to be followed up Ipswich Hospital
Routine follow up arrangements with your GP Practice Staff Patient to be seen in xxx to xxx working days with GP Practice Staff (Dear Parent/Guardian, please contact your GP practice as soon as possible to arrange an appointment for your child to be seen with the asthma nurse) Patient to be seen in xxx to xxx weeks with GP Practice Staff (Dear Parent/Guardian, please contact your GP practice as soon as possible to arrange an appointment for your child to be seen with the asthma nurse)
Routine follow up arrangements at Ipswich Hospital (if required) Follow up with Dr XXX in XXX week’s time Medication Plan
*Take salbutamol 2 puffs every two minutes, up to 10 via spacer, up to 4 hourly. If needing to use more frequently then seek medical attention.
Medication Name and Strength of medication No. of puffs per day
Times per day
Salbutamol (reliever) blue inhaler* Steroid/combination inhaler (preventer)
Prednisolone (steroids) Leukotriene antagonist (Montelukast) Other treatments:
If your child’s symptoms are improving then discuss with Asthma practice nurse and keep follow up appointments in the hospital
Keep your review appointment in the hospital

28
If your child’s symptoms are not improving and your child is needing to use more blue reliever inhaler frequently
If your child’s symptoms worsen e.g.: -The child’s blue reliever inhaler is not helping -The child’s breathing is hard and fast -The child can’t talk or walk easily - The child is getting tired
Need to seek medical attention
Please phone 999
What to do in an emergency whilst waiting for 999: 1. The child to take 2 puffs of their reliever inhaler (usually blue) through spacer. 2. Sit the child down and get them to take slow, steady breaths 3. If no immediate improvement, get your child to continue to take two puffs (one puff at a time) of reliever inhaler every two minutes. They can take up to
ten puffs. 4. If ambulance does not arrive in ten minutes and you are still feeling unwell, repeat step 3.
After an emergency you should call your doctor or asthma nurse and ask for an urgent appointment—even if they feel better. Do not ignore worsening asthma. Get medical help immediately. Day or night.

29
PRACTICE NAME: Pilot Management Plan and Actions Required Upon Discharge of Ipswich Hospital Paediatric Patients with Acute Asthma/Wheeze
Monitoring Form – IDEALLY TO BE COMPLETED BY ALL PRACTICES PARTICIPATING IN THE 3 MONTH PILOT (NB – THIS DOCUMENT COULD ALSO BE USED BY PRACTICES TO SUPPORT EVIDENCING USE OF THE QOF QP14 PATHWAY)
This monitoring form supports the 3 month pilot with Ipswich Hospital for patients who are discharged from paediatrics with acute asthma/wheeze.
• It is expected that the parent/guardian will contact their GP practice to arrange a follow up appointment if required, stating the timescale required. • So patients are not missed, practice staff are asked to contact the parent/guardian if no appointment is made. • Practices are asked to record the data on discharge management plans received using this monitoring form in order to capture any areas for improvement
in the future.
Once a month practices are asked to update the asthma clinic data and fax back to 01473 770201
NHS Number Discharge Date
Date discharge form received
Follow-Up Outcome: -Follow up at IHT -Routine follow up at IHT -Routine follow up at GP practice
Timescale indicated by IHT for routine follow-up in GP practice
Was contact made by parent/guardian? (Y/N)
If no, date practice contacted parent/guardian
Comments
Example: 454423465
15/06/2012 17/06/2012 Routine follow up at GP practice
2 weeks No 25/06/2012
30
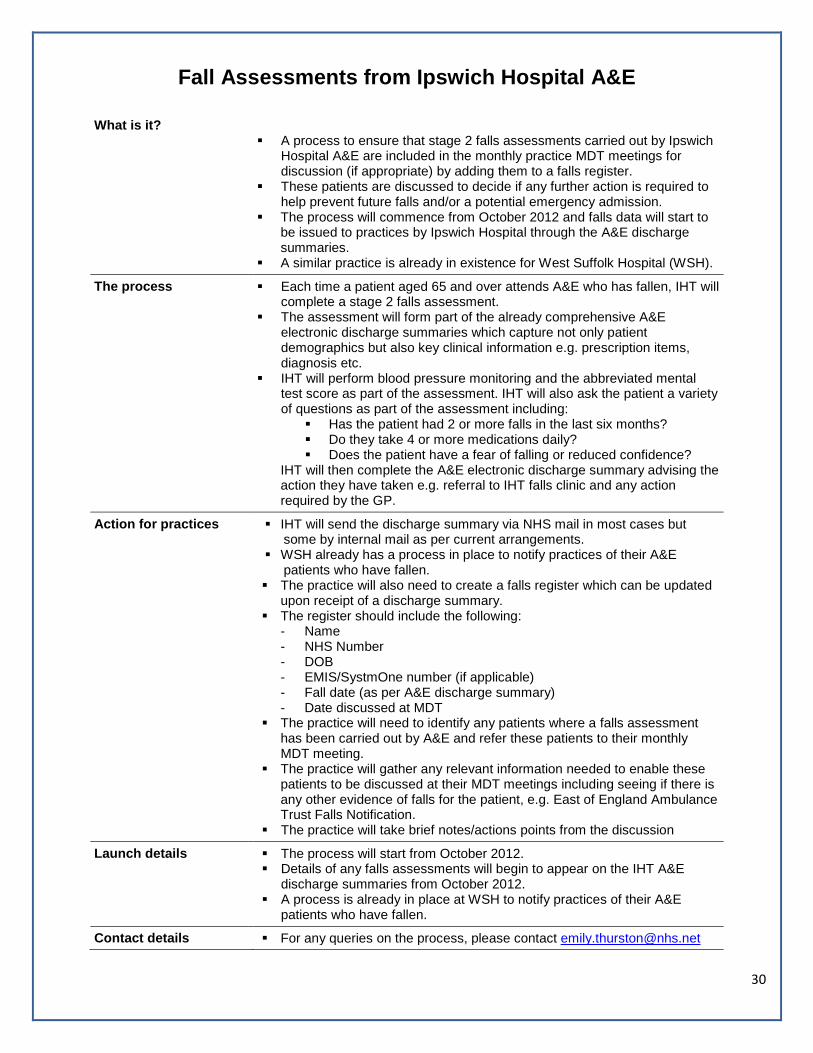
Fall Assessments from Ipswich Hospital A&E
What is it?
A process to ensure that stage 2 falls assessments carried out by Ipswich Hospital A&E are included in the monthly practice MDT meetings for discussion (if appropriate) by adding them to a falls register.
These patients are discussed to decide if any further action is required to help prevent future falls and/or a potential emergency admission.
The process will commence from October 2012 and falls data will start to be issued to practices by Ipswich Hospital through the A&E discharge summaries.
A similar practice is already in existence for West Suffolk Hospital (WSH).
The process
Each time a patient aged 65 and over attends A&E who has fallen, IHT will complete a stage 2 falls assessment.
The assessment will form part of the already comprehensive A&E electronic discharge summaries which capture not only patient demographics but also key clinical information e.g. prescription items, diagnosis etc.
IHT will perform blood pressure monitoring and the abbreviated mental test score as part of the assessment. IHT will also ask the patient a variety of questions as part of the assessment including:
Has the patient had 2 or more falls in the last six months? Do they take 4 or more medications daily? Does the patient have a fear of falling or reduced confidence?
IHT will then complete the A&E electronic discharge summary advising the action they have taken e.g. referral to IHT falls clinic and any action required by the GP.
Action for practices IHT will send the discharge summary via NHS mail in most cases but some by internal mail as per current arrangements.
WSH already has a process in place to notify practices of their A&E patients who have fallen.
The practice will also need to create a falls register which can be updated upon receipt of a discharge summary.
The register should include the following: - Name - NHS Number - DOB - EMIS/SystmOne number (if applicable) - Fall date (as per A&E discharge summary) - Date discussed at MDT
The practice will need to identify any patients where a falls assessment has been carried out by A&E and refer these patients to their monthly MDT meeting.
The practice will gather any relevant information needed to enable these patients to be discussed at their MDT meetings including seeing if there is
any other evidence of falls for the patient, e.g. East of England Ambulance Trust Falls Notification.
The practice will take brief notes/actions points from the discussion
Launch details The process will start from October 2012. Details of any falls assessments will begin to appear on the IHT A&E
discharge summaries from October 2012. A process is already in place at WSH to notify practices of their A&E
patients who have fallen.
Contact details For any queries on the process, please contact [email protected]

31
Example of wording on A&E Electronic Discharge Summary
32
Ipswich Hospital Falls Screening Assessment

33
Ipswich Hospital Modified Falls Screening Assessment checklist - Adult
Name…………………………………………DOB………………………….NHS No…………………………………………………….
GP…………………………………….Address………………………………………………………………………………….…………….
Tel……………………………………………………..
(To save time, lay patient on couch at beginning of assessment so postural BP can be done at the end)
Please circle appropriate box
Refer to Date of referral
Comments including “no action”
Postural BP* Giddiness
Lying Standing Immed 1 min
3 min
Y N Not Known
GP and Local Healthcare
Teams
2 or more falls in last 6 months Y N Not Known
Currently on 4 or more medications Y N Not Known
Fear of falling / reduced confidence Y N Not Known
AMTS * less than 8/10 Y N Not Known
Excess alcohol problems Y N Not Known
ECG Y N Not Known
Give advice and treat as necessary. If appropriate, refer as suggested with copy of assessment form. Where no cause of fall can be clearly identified, or medical review is required, please refer to Rapid Assessment Unit, IHT (East Suffolk only) via the GP or to the GP for medical review. If falls and fracture intervention & rehabilitation is indicated – refer to Local Healthcare Teams via SPA. In ALL referrals indicate 1) reasons for referral, 2) gain consent from client/patient.
Name………………………………………………………………...Designation…………………………………………….……………
Signature………………………………………………….………..Date………………………….…………………………………………
A&E Frequent Attenders

34
What is it? A process to ensure that any patients who attend A&E frequently are referred to practice MDT meetings for discussion where appropriate.
These patients are to be discussed to decide if any action can be taken to help prevent future A&E attendances.
The process will start from 1st October 2012.
The process
Every month the SUS data is submitted to NHS Suffolk which will include details of all attendances to hospitals.
The data will be analysed and issued to practices as part of a monthly A&E Data pack which is being issued as stated in the BMA Quality and Outcomes Framework for 2012/13 guidance. Please note: in order to provide timely information to practices, this data is un-validated.
The data will include an overview of numbers of patients attending more than once each month, and a list of NHS numbers for patients who have attended more than 4 times since January 2012.
For ease, the monthly MDT data will also include patients who have attended A&E more than 4 times since January 2012.
If appropriate, the patients are to be discussed at the practice monthly MDT meeting to establish if there is any action from a health and social perspective that can be taken to help prevent future A&E attendances.
Action for practices NHS Suffolk will send the monthly A&E data pack to practices via NHS.net mail by the 25th of each month. Practices can either use this pack or the monthly MDT data.
The practice will need to review any patients who are identified as a ‘frequent attender’ (patients who have attended more than 4 times since January 2012) and ascertain if they would benefit from being discussed at the MDT meeting.
For practices which do not have patients who have attended A&E more than 4 times since January 2012, they may wish to consider reviewing those patients who have attended A&E more than 3 times (this information is available and will be highlighted to practices in the monthly A&E data pack)
The practice will need to gather any relevant information needed to enable these patients to be discussed at their MDT meetings.
Other attendees may be invited to MDT meetings by the practice, which may help aid discussion i.e. Adult Community Services, OOH etc.
Brief notes/actions points from the discussion should be taken.
Launch details The process will start from 1st October 2012.
Contact details For any queries on the process, please contact [email protected] For any queries on the data, please contact

35
The table below appears towards the end of the monthly A&E data pack and features those patients who have attended A&E more than 4 times since January 2012.
Multiple A&E Attendances Summary - D8123 Example practice - Aug-12 Summary of patients who have attended A&E more than 4 times since Jan-12 (highlight shows when number of attends exceeds 4)
NHS Number Cohort Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Grand Total
Patient 1 16-64 3 6 1 1 11
Patient 2 65 and Over 1 2 2 3 2 10
Patient 3 65 and Over 1 2 3 6
Patient 4 65 and Over 1 4 5
Patient 5 65 and Over 1 3 1 5
Patient 6 65 and Over 1 3 1 5 Patient 7 15 and Under 2 1 1 1 5
Patient 8 65 and Over 2 1 2 5
Total 5 9 6 10 11 3 8 52
This row shows the total number of attendances per month for patients identified. In this example, the practice might want to look at why attendances increased in April and May.
This column will be populated with those patients who have attended A&E more than 4 times since January 2012. These are the patients which you will need to discuss at your MDT.
The rows will turn yellow when the number of A&E attendances for the patient reaches 4. For example, patient number 3 reached 4 A&E attendances in May 2012.
This column shows the total number of attendances for each patient. The grand total (in this case 52) is the total number of attendances for all patients identified.