2012 oe booklet national
19
1 2012 Employee Benefits Booklet National No matter how you slice it, GOOD HEALTH IS THE BEST CHOICE.
-
Upload
sandra-duncan -
Category
Business
-
view
79 -
download
0
Transcript of 2012 oe booklet national

1
2012 Employee Benefits BookletNational
No matter how you slice it,GOOD HEALTH IS THE BEST CHOICE.

2012-2013 Open Enrollment

The Benefits of Working at ReachLocal
At ReachLocal, we know that to succeed we need employees who are committed to excellence. We acknowledge your important contributions to our success by providing a competitive total rewards package consisting of pay, benefits and development opportunities.
This brochure gives you an overview of the benefits program at ReachLocal. Please review it, share it with your family and be sure to enroll by the deadline to ensure coverage.
If you have any questions about your benefits, please contact Human Resources at [email protected].

Contents
About 2012-2013 Open Enrollment ....................................................... 1
Medical Plans .......................................................................................... 2 Anthem Blue Cross Base PPO Plan Anthem Blue Cross Base Plus PPO Plan Anthem Blue Cross Buy Up PPO Plan
Dental Plans ............................................................................................ 5 Guardian Dental HMO Plan Guardian Dental Base PPO Plan Guardian Dental Buy Up PPO Plan
Vision Plan .............................................................................................. 8 Anthem Blue Cross Vision PPO Plan
Term Life, Accidental Death& Dismemberment (AD&D) and Disability Plans ................................. 9 Anthem Blue Cross Group Term Life Anthem Blue Cross Voluntary Life Anthem Blue Cross STD & LTD
Flexible Spending Account .................................................................. 11
401K Retirement Plan............................................................................ 11
Employee Assistance Program (EAP) ................................................. 12
Medical and Emergency Information ................................................... 13
Contact Information

1
THIS IS THE TIME YOU CAN• Change the benefits plans you’re enrolled in• Change who you cover by adding or dropping dependents• Increase your voluntary life and/or disability coverages
WHAT YOU NEED TO DOTo make sure you have the benefits coverage you want during 2012-2013:
• Attend a webinar• Discuss your benefit needs with your family• Go online www.vbas.com and confirm or change current elections
WHO IS ELIGIBLEYou are eligible for the ReachLocal benefits program if you are:
• A full time employee who is regularly scheduled to work at least 30 hours each week and have completed at least 30 days of employment
• You may also elect medical, dental, vision, life and/or disability coverage(s) for your:
• Legal husband or wife• Dependent children until they turn age 26• Unmarried dependent children over age 26 who are physically or
mentally incapable of self support.
QUALIFYING EVENTSDuring the year, you can change your benefit elections only if you experience a qualifying event. Examples of qualifying events include changes in:
• Marital status (marriage, divorce, legal separation)• Adding dependent(s) – birth, adoption, placement for adoption, being
named legal guardian• Dependent status (child reaches maximum age)• Eligibility status (you or your spouse experience a change in hours,
job loss, getting a new job, become entitled to Medicare or Medicaid).
You have 31 days from the time of the qualifying event to notify Human Resources to change your benefits.
About 2012-2013 Open EnrollmentEach year ReachLocal holds Open Enrollment
nycosmogirl
Typewritten Text
nycosmogirl
Typewritten Text

2
In-Network Out-of-Network
Annual Plan Deductible Individual: $1500Family: $3,000
Individual: $1,500Family: $3,000
Maximum Out-of-Pocket Individual: $3,000Family: $6,000
Individual: $6,000Family: $12,000
Lifetime Maximum Unlimited Unlimited
In-Patient Hospitalization 10% (after deductible) 30% (after out-of-network
deductible)
Out-Patient Hospitalization 10% (after deductible) 30% (after deductible)
Emergency Room 10% (after deductible) 30% (after deductible)
Office Visit 10% (after deductible) 30% (after deductible)
Preventative Care No charge 30% (after deductible)
Chiropractic 10% (after deductible)24 visits
30% (after deductible)24 visits
Prescription Drugs Generic Preferred Brand Non-Preferred Brand Self-Injectable
$10 copay (after deductible)$30 copay (after deductible)$50 copay (after deductible)
30%
Member pays retail copay plus 30% of the remaining
covered expenses in excess of the maximum allowed
amount
Anthem Blue Cross Base PPO PlanOption PPO LHSA 86
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Enrollment Deduction per Paycheck
Employee Only $0.00
Two Party (Employee + one dependent) $88.00
Family (Employee + two or more dependents) $125.72
3
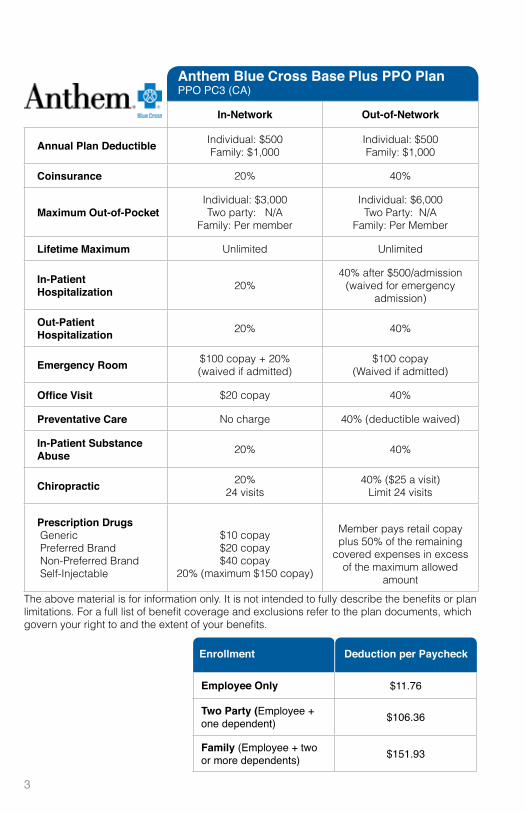
In-Network Out-of-Network
Annual Plan Deductible Individual: $500Family: $1,000
Individual: $500Family: $1,000
Coinsurance 20% 40%
Maximum Out-of-Pocket Individual: $3,000Two party: N/A
Family: Per member
Individual: $6,000Two Party: N/A
Family: Per Member
Lifetime Maximum Unlimited Unlimited
In-Patient Hospitalization 20%
40% after $500/admission(waived for emergency
admission)
Out-Patient Hospitalization 20% 40%
Emergency Room $100 copay + 20%(waived if admitted)
$100 copay(Waived if admitted)
Office Visit $20 copay 40%
Preventative Care No charge 40% (deductible waived)
In-Patient Substance Abuse 20% 40%
Chiropractic 20%24 visits
40% ($25 a visit)Limit 24 visits
Prescription Drugs Generic Preferred Brand Non-Preferred Brand Self-Injectable
$10 copay$20 copay$40 copay
20% (maximum $150 copay)
Member pays retail copay plus 50% of the remaining
covered expenses in excess of the maximum allowed
amount
Anthem Blue Cross Base Plus PPO PlanPPO PC3 (CA)
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Enrollment Deduction per Paycheck
Employee Only $11.76
Two Party (Employee + one dependent) $106.36
Family (Employee + two or more dependents) $151.93

4
Employee Only $11.76
Two Party (Employee + one dependent) $106.36
Family (Employee + two or more dependents) $151.93
In-Network Out-of-Network
Annual Plan Deductible Individual: $250Family: $750
Individual: $250Family: $750
Coinsurance 10% 30%
Maximum Out-of-Pocket Individual: $2,000Two party: N/A
Family: Per member
Individual: $6,000Two Party: N/A
Family: Per Member
Lifetime Maximum Unlimited Unlimited
In-Patient Hospitalization 10%
30% after $500/admission(waived for emergency
admission)
Out-Patient Hospitalization 10% 30%
Emergency Room $100 copay + 10%(waived if admitted)
$100 copay(Waived if admitted)
Office Visit $10 copay 30%
Preventative Care No charge 40% (deductible waived)
In-Patient Substance Abuse 10% 30%
Chiropractic 10%24 visits
30% ($25 a visit)Limit 24 visits
Prescription Drugs Generic Preferred Brand Non-Preferred Brand Self-Injectable
$10 copay$20 copay$40 copay
20% (maximum $150 copay)
Member pays retail copay plus 50% of the remaining
covered expenses in excess of the maximum allowed
amount
Anthem Blue Cross Buy Up PPO PlanPPO PC6 (CA)
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Deduction per PaycheckEnrollment
Employee Only $43.94
Two Party (Employee + one dependent) $174.94
Family (Employee + two or more dependents) $249.89

5
Network Only*
Preventive Deductible N/A
Basic & Major Deductible N/A
Annual Maximum Individual: Unlimited
DPPO Coinsurance Diagnostics (exams) Preventive (teeth cleaning) Basic (fillings) Scaling & Root Planning (per quadrant)
No chargeNo chargeNo charge($15-$25)
Cleanings per year 2 (regular only)
Services Root Canal Prior Surgery Single Crown
$70-$140$60-$155
$100
OrthodonticsDental ImplantsCosmetic Care - Bleaching
Child/Adult: $2,500-$2,800N/A
$165
Guardian Dental HMO PlanDental HMO Plan
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
*DHMO Plans are available in California, Florida, Illinois, Indiana, Michigan, Missouri, New Jersey, New York and Texas.
Enrollment Deduction per Paycheck
Employee Only $0.00
Employee + Spouse $1.00
Employee + Child(ren) $1.00
Employee + Family $2.00

6
Employee Only $0.00
Employee + Spouse $1.00
Employee + Child(ren) $1.00
Employee + Family $2.00
In-Network Out-of-Network
Preventive Deductible Individual: N/A Individual: N/A
Basic & Major Deductible
Individual: $50Family: $150
Individual: $50Family: $150
Annual Maximum Individual: $2,000 Individual: $2,000
DPPO Coinsurance Diagnostics (exams) Preventive (teeth cleaning) Basic (fillings) Major (oral surgery, extractions, implants)
No chargeNo charge
10%40%
No chargeNo charge
20%50%
Cleanings per year 2 (regular only) 2 (regular only)
Dental Maximum Roll Over Annual Threshold Annual Roll Over Amount Annual Roll Over In-Net-Work Bonus
$800$400$600
$800$400$600
Orthodontics N/A N/A
Non-Network Reimbursement 90th percentile of UCR 90th percentile of UCR
Guardian Dental Base PPO PlanDPPO Base without Ortho
Enrollment
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Deduction per Paycheck
Employee Only $1.91
Employee + Spouse $20.51
Employee + Child(ren) $18.86
Employee + Family $32.30

7
In-Network Out-of-Network
Preventive Deductible Individual: N/A Individual: N/A
Basic & Major Deductible
Individual: $50Family: $150
Individual: $50Family: $150
Annual Maximum Individual: $3,000 Individual: $3,000
DPPO Coinsurance Diagnostics (exams) Preventive (teeth cleaning) Basic (fillings) Major (oral surgery, extractions)
No chargeNo charge
10%40%
No chargeNo charge
20%50%
Cleanings per year 2 (regular only) 2 (regular only)
Dental Maximum Roll Over Annual Threshold Annual Roll Over Amount Annual Roll Over In-Net-Work Bonus
$1,000$500$750
$1,000$500$750
Orthodontics Lifetime Maximum Age Limitation
50%Child/Adult: $2,000
N/A
50%Child/Adult: $2,000
N/A
Non-Network Reimbursement 90th percentile of UCR 90th percentile of UCR
Guardian Dental Buy Up PPO PlanDPPO Buy Up with Ortho
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Enrollment Deduction per Paycheck
Employee Only $5.43
Employee + Spouse $28.16
Employee + Child(ren) $25.89
Employee + Family $44.35
8
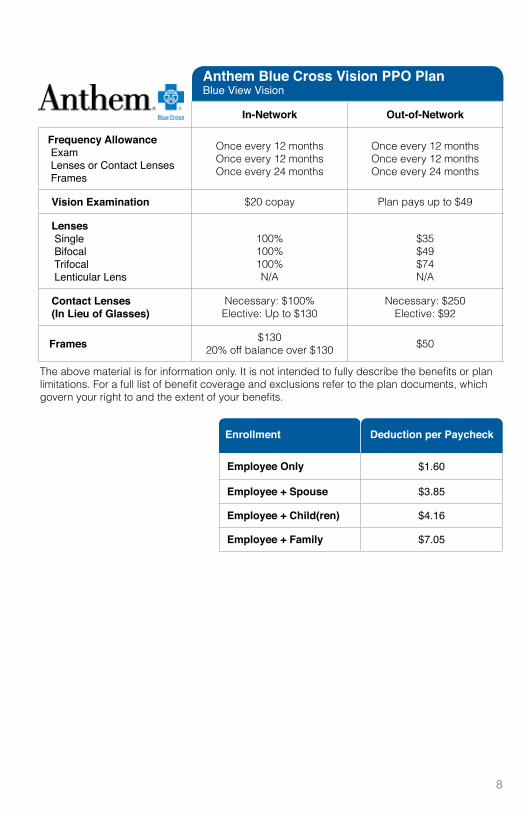
In-Network Out-of-Network
Frequency Allowance Exam Lenses or Contact Lenses Frames
Once every 12 monthsOnce every 12 monthsOnce every 24 months
Once every 12 monthsOnce every 12 monthsOnce every 24 months
Vision Examination $20 copay Plan pays up to $49
Lenses Single Bifocal Trifocal Lenticular Lens
100%100%100%N/A
$35$49$74N/A
Contact Lenses(In Lieu of Glasses)
Necessary: $100%Elective: Up to $130
Necessary: $250Elective: $92
Frames $13020% off balance over $130 $50
Anthem Blue Cross Vision PPO PlanBlue View Vision
The above material is for information only. It is not intended to fully describe the benefits or plan limitations. For a full list of benefit coverage and exclusions refer to the plan documents, which govern your right to and the extent of your benefits.
Enrollment Deduction per Paycheck
Employee Only $1.60
Employee + Spouse $3.85
Employee + Child(ren) $4.16
Employee + Family $7.05

9
Age Employee or Spouse Child(ren)
< 25 $0.050 $0.03
25-29 $0.057
30-34 $0.071
35-39 $0.101
40-44 $0.144
45-49 $0.229
50-54 $0.365
55-59 $0.561
60-64 $0.875
65-69 $1.518
70-74 $2.709
75+ $5.309
Voluntary LifeMonthly rate per $1,000 of Benefit
Example: The cost for $100,000 Voluntary Life insurance for a 30 year-old employee: Per Month: $7.10 + 3.61
Per Pay Period: $5.36
Group Term Life and AD&DAll full time benefit eligible employees receive term Life and AD&D benefits equal to one times annual salary to a maximum of $400,000. This is fully paid for by ReachLocal.
Voluntary LifeYou can purchase additional term life/AD&D benefits for yourself, your spouse, and dependent child(ren) on a voluntary basis at cost effective group pricing.
Voluntary AD&DMonthly rate
per $1,000 of benefit
Employee Only $0.0361
Employee + Family $0.051

10
Example: 30 year-old employee to cover $60,000 salary (60% disability benefits):
Long-Term Disability $36,000/year benefit up to Social Security Normal Retirement Age
Cost: $4.25/pay period
Short-Term Disability • $692.3/week benefit up to 12 weeks
Cost: $9.00/pay period
Short-Term & Long-Term DisabilityShort-Term and Long-Term Disability benefits offer protection for your salary when you are unable to work due to illness or a non-work related injury.
Short-Term Disability benefit replaces 60% of your pre-disability earnings to a max weekly benefit of $1,500 for 12 weeks. The elimination period is 8 days due to accident/sickness.
Long-Term Disability benefit replaces 60% of your pre-disability earnings to a maximum benefit of $6,000 per month and continues for 2 years if you cannot perform your own occupation, up to the Social Security Normal Retirement Age if you cannot perform any occupation.
Age Rate
< 25 $0.27
25-29 $0.29
30-34 $0.26
35-39 $0.23
40-44 $0.25
45-49 $0.27
50-54 $0.32
55-59 $0.43
60-64 $0.51
65-69 $0.55
70+ $0.55
Voluntary STD RatesMonthly rate per $10 of Weekly Benefit
Age Rate
< 25 $0.09
25-29 $0.11
30-34 $0.17
35-39 $0.25
40-44 $0.36
45-49 $0.52
50-54 $0.72
55-59 $0.93
60-64 $0.87
65-69 $0.95
70+ $0.98
Voluntary LTD RatesRate per $100 of Covered Salary

11
Flexible Spending Account (FSA)Take Advantage of Tax Savings to set aside funds for child care and medical expenses tax free.
Employees can elect to participate in either Dependent Care Account or Health Care account. You will have money deducted from your paychecks on a pretax basis to use later to pay for qualified health care or dependent care related expenses.
The advantage is that the employee’s taxable income is reduced by the amount that is deducted, resulting in a lesser amount of tax being taken from the employee’s pay check.
Maximum/Minimum Annual DeductionDependent Care: $5,000/$300Health Care: $3600/$300
Use it or Lose It. Qualified expenses must incur during the plan year from July 1 to June 30. You have 90 days to submit claims for reimbursement. If you fail to claim the money set aside in the FSA account, the funds will be forfeited as required by law.
401K Retirement PlanStart saving for your future and watch your savings grow.
Contribute pre-tax dollars towards your retirement. Your contributions are with pre-tax dollars and your earnings grow tax deferred.
• You can sign up at www.mykplan.com anytime after your first paycheck• Contribute 1% to 90% of your gross wages on a pre-tax basis• The money you contribute is always yours
- You can take a loan distribution- You can rollover money from a previous employer into our plan- If you leave ReachLocal, you can take the money with you

12
Employee Assistance ProgramResource Advisor provided by Anthem Blue Cross
• Providing guidance and support to manage your emotional, legal and financial issues 24/7 on the phone and/or online
• Professional legal and financial advisor visits on the phone or in person
• Beneficiary Services
• Identity Theft Victim Recovery Services
13
Medical & Emergency Information
Family Physcian
Dentist
Pediatrician
Pharmacy
Urgent Care
Hospital
Police Department
Fire Department
Notes

Contact Information
ReachLocal HR Contact [email protected] x1149
Guardian Dental Plan www.glic.com1.800.541.7846
DPPO1.800.541.7846
DMO1.888.618.2016
BRMS (FSA) www.vbas.comwww.brmsclaims.com1.888.326.2555
Anthem Blue Cross Medical PPO www.anthem.com/ca1.800.765.2588
Anthem Blue Cross Vision PPOwww.anthem.com/ca1.866.723.0515
Anthem EAP www.resourceadvisor.anthem.ca1.888.209.7840
Dickerson Employee Benefits 1.800.457.6116 x243
ADP Retirement Serviceswww.mykplan.com1.800.695.7526

Employee Benefits Consultant