2007 Evidence Base for Newer Modes of Mechanical Ventilation
50
Evidence Base for Newer Modes of Mechanical Ventilation Charles B. Spearman, MSEd, RRT, Charles B. Spearman, MSEd, RRT, FAARC FAARC Assistant Professor Assistant Professor Respiratory Care Programs Respiratory Care Programs Department of Cardiopulmonary Department of Cardiopulmonary Sciences Sciences Loma Linda University Loma Linda University Loma Linda, California Loma Linda, California
-
Upload
vijay-gadagi -
Category
Documents
-
view
71 -
download
2
description
power point
Transcript of 2007 Evidence Base for Newer Modes of Mechanical Ventilation

Evidence Base for Newer Modes of Mechanical Ventilation
Charles B. Spearman, MSEd, RRT, FAARCCharles B. Spearman, MSEd, RRT, FAARC
Assistant ProfessorAssistant Professor
Respiratory Care ProgramsRespiratory Care Programs
Department of Cardiopulmonary SciencesDepartment of Cardiopulmonary Sciences
Loma Linda UniversityLoma Linda University
Loma Linda, CaliforniaLoma Linda, California

Evidence Base for Newer Modes of Mechanical Ventilation: Overview Background for evidence base levelsBackground for evidence base levels Dual modes of ventilationDual modes of ventilation Adaptive Support ventilation (ASV)Adaptive Support ventilation (ASV) Proportional Assist Ventilation (PAV)Proportional Assist Ventilation (PAV) Airway Pressure Release Ventilation (APRV)Airway Pressure Release Ventilation (APRV)

Evidence Base for Newer Modes of Mechanical Ventilation: Background Evidence-based medicine:Evidence-based medicine:
“…the integration of individual clinical expertise “…the integration of individual clinical expertise with the best available research evidence from with the best available research evidence from systematic research and the patient’s values and systematic research and the patient’s values and expectations.” expectations.” D. R. Hess, RC,2004;49:7, 730-741.D. R. Hess, RC,2004;49:7, 730-741.

Evidence Base for Newer Modes of Mechanical Ventilation: Background New Horizons Symposium: Integrating Evidence-based New Horizons Symposium: Integrating Evidence-based
Respiratory Care into PracticeRespiratory Care into PracticePublished in:Published in:Respiratory Care, July 2004 (49:7)Respiratory Care, July 2004 (49:7)
Topics covered:Topics covered:
-What is EBM-What is EBM -EB of New Modes-EB of New Modes
-RC Protocols-RC Protocols -COPD Manag.-COPD Manag.
-Asthma Manag.-Asthma Manag. -ALI/ARDS Manag.-ALI/ARDS Manag.
-NIPPV-NIPPV -Weaning-Weaning Also G. D. Rubenfeld’s article RCP role in EBM use Also G. D. Rubenfeld’s article RCP role in EBM use

Evidence Base for Newer Modes of Mechanical Ventilation: Background
Other sources for evidence :based practiceOther sources for evidence :based practice Clinical Practice GuidelinesClinical Practice Guidelines
AARC, ACCP, ATSAARC, ACCP, ATS Evidence based guidelinesEvidence based guidelines
Weaning, GOLD, Aerosol Task force, Weaning, GOLD, Aerosol Task force, Asthma training, etc.Asthma training, etc.

Evidence Base for Newer Modes of Mechanical Ventilation: Background
From: Branson & Johanningman, 2004:RC,49:7, 742-760.

New Modes of Mechanical Ventilation: Background
Introduction of the microprocessor-Introduction of the microprocessor-controlled ventilatorcontrolled ventilator Better control of flow & exhalation Better control of flow & exhalation
valvesvalves Increased monitoring capabilities Increased monitoring capabilities Increased pt-ventilator interactionIncreased pt-ventilator interaction ““Dual modes” of ventilation Dual modes” of ventilation
introducedintroduced
From Mosby’s R. C. Equip., 6th ed. 1999.

New Modes of Mechanical Ventilation: Examples of the first dual modes
Volume Assured Pressure Support (VAPS) Volume Assured Pressure Support (VAPS) & Pressure Augmentation& Pressure Augmentation
Pressure Regulated Volume Control Pressure Regulated Volume Control (PRVC) & similar modes(PRVC) & similar modes
Volume Support Ventilation (VS or VSV) Volume Support Ventilation (VS or VSV) & similar modes& similar modes

Pressure vs. Volume Ventilation(From Branson, R., Bird product literature)

Newer Methods of Ventilatory Support: dual modes 1st generation dual modes: VAPS, Press. 1st generation dual modes: VAPS, Press.
Aug., PRVC & VS Aug., PRVC & VS Allow variable flow delivery and pressure Allow variable flow delivery and pressure
“targeted” ventilation approach“targeted” ventilation approach Attempt to deliver a set tidal volume (TV)Attempt to deliver a set tidal volume (TV) Allow peak airway pressure to vary breath Allow peak airway pressure to vary breath
to breathto breath

VAPS: Volume Assured Pressure Support Combines volume ventilation & pressure supportCombines volume ventilation & pressure support
(for mech., vol. limited breaths only)(for mech., vol. limited breaths only) Uses TV, peak flow, and pressure sup./control settingsUses TV, peak flow, and pressure sup./control settings Targets PS level with Targets PS level with at leastat least set peak flow first set peak flow first Continues until flow decreases to set peak flow, then:Continues until flow decreases to set peak flow, then:
If TV not delivered, peak flow maintained If TV not delivered, peak flow maintained until vol. limituntil vol. limit
If TV or more delivered, breath endsIf TV or more delivered, breath ends

VAPS: Volume Assured Pressure Support
(From Branson, R., Bird product literature)(From Branson, R., Bird product literature)

VAPS: (and Pressure Augmentation) - Considerations
The set TV is the The set TV is the minimumminimum TV the patient TV the patient will receivewill receive
The set pressure support is the The set pressure support is the minimum minimum the patient will receivethe patient will receive
The set peak flow is the The set peak flow is the minimumminimum the the patient will receivepatient will receive
No ventilatory mechanics measuredNo ventilatory mechanics measured

Pressure Regulated Volume Control (Servo vents.)
Combines volume ventilation & pressure Combines volume ventilation & pressure controlcontrol (for mech., time-cycl. breaths only)(for mech., time-cycl. breaths only)
Set TV is “targeted”Set TV is “targeted” Ventilator estimates vol./press. relationship Ventilator estimates vol./press. relationship
each breatheach breath Ventilator adjusts level of pressure control Ventilator adjusts level of pressure control
breath by breathbreath by breath

Pressure Regulated Volume Control (Servo vents, example)
First breath = 5-10 cm H2O above PEEPFirst breath = 5-10 cm H2O above PEEP V/P relationship V/P relationship measuredmeasured Next 3 breaths, pressure increased to 75% Next 3 breaths, pressure increased to 75%
needed for set TVneeded for set TV Then up to +/- 3 cm H2O changes per Then up to +/- 3 cm H2O changes per
breathbreath Time ends inspirationTime ends inspiration

Pressure Regulated Volume Control (Siemens Servo 300)
From Siemens prod. literatureFrom Siemens prod. literature

Pressure Regulated Volume Control - Considerations
Assist-control modeAssist-control mode Like PC, flow varies automatically to Like PC, flow varies automatically to
varying patient demands varying patient demands Constant press. during each breath - Constant press. during each breath -
variable press. from breath to breathvariable press. from breath to breath Time is cycling method; delivered TV can Time is cycling method; delivered TV can
vary from setvary from set

First dual modes: VAPS, Press. Aug. vs. PRVC & VS
VAPS VAPS (& Press. (& Press. Augmentation)Augmentation)
Use the set TV as a Use the set TV as a minimumminimum
Normal cycling Normal cycling occurs at or above occurs at or above the set TVthe set TV
Mechanics not Mechanics not measuredmeasured
PRVC PRVC (& Vol. Support)(& Vol. Support)
Use the set TV as the Use the set TV as the “target” for each “target” for each breathbreath
Normal cycling may Normal cycling may stop insp. below stop insp. below oror above set TVabove set TV
Pressure used based Pressure used based on mechanics on mechanics measurements measurements

First dual modes: VAPS, Press. Aug. vs. PRVC & VS
Peak airway pressure can reach high levels:Peak airway pressure can reach high levels:
Set appropriate high pressure limitsSet appropriate high pressure limits
No settings for No settings for maximummaximum tidal volume tidal volume

Newer Ventilator Dual Modes:
AutoFlow:AutoFlow: Drager Drager ventilators Evita 4, ventilators Evita 4, Evita 2 duraEvita 2 dura
Adaptive Support Adaptive Support Ventilation (ASV): Ventilation (ASV): Hamilton GalileoHamilton Galileo

Newer Ventilator Dual Modes: Drager vent’s AutoFlow
First breath uses set First breath uses set TV & I-timeTV & I-time Pplateau measuredPplateau measured
Pplateau then usedPplateau then used V/P measured each V/P measured each
breathbreath Press. changed if Press. changed if
needed (+/- 3)needed (+/- 3) Then similar to PRVCThen similar to PRVC
From Drager & Mosby’s R. C. Equip., 6th ed. 1999.
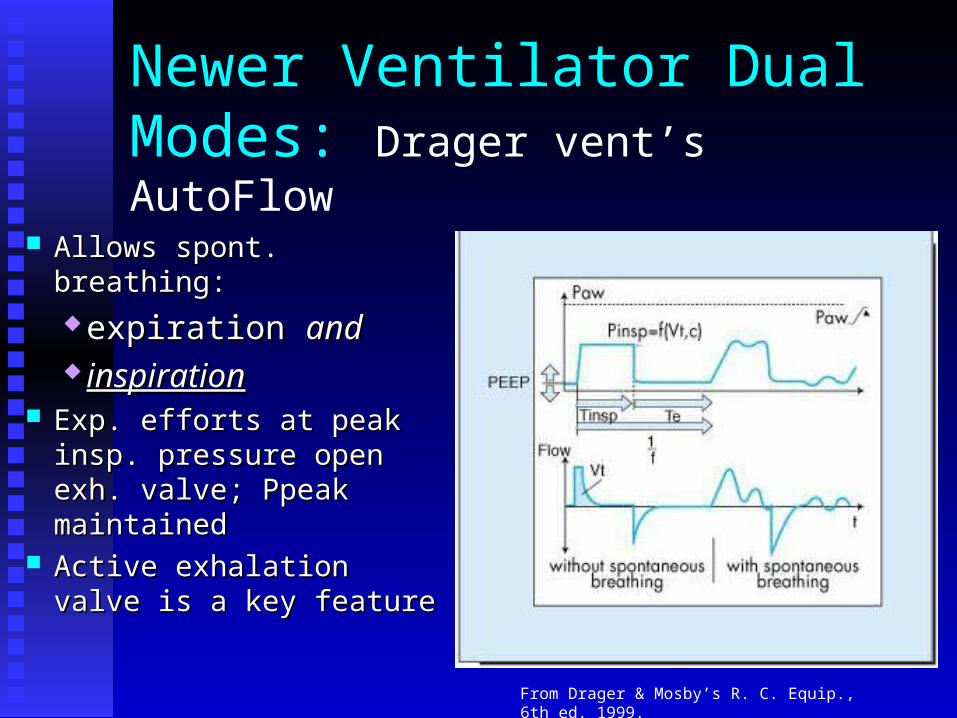
Newer Ventilator Dual Modes: Drager vent’s AutoFlow
Allows spont. breathing:Allows spont. breathing: expiration expiration andand inspirationinspiration
Exp. efforts at peak insp. Exp. efforts at peak insp. pressure open exh. pressure open exh. valve; Ppeak maintainedvalve; Ppeak maintained
Active exhalation valve Active exhalation valve is a key featureis a key feature
From Drager & Mosby’s R. C. Equip., 6th ed. 1999.

Newer Ventilator Dual Modes: Drager vent’s AutoFlow
Allows spont. breathing:Allows spont. breathing: expiration expiration andand inspirationinspiration
From Drager

Newer Ventilator Dual Modes: Drager vent’s AutoFlow - Considerations
Dual mode similar to PRVCDual mode similar to PRVC Targets vol., applies variable press. based on Targets vol., applies variable press. based on
mechanics measurementsmechanics measurements Allows highly variable inspiratory flows Allows highly variable inspiratory flows Time ends mandatory breathsTime ends mandatory breaths
Adds ability to freely exhale during mandatory Adds ability to freely exhale during mandatory inspiration (maintains pressure)inspiration (maintains pressure)
Adds high TV alarm & limitAdds high TV alarm & limit Can be used in CMV, SIMV and MMVCan be used in CMV, SIMV and MMV

Newer Ventilator Dual Modes: Hamilton Galileo’s ASV (adapt. sup. vent.)
Clinician enters pt. data & % supportClinician enters pt. data & % support Vent. calculates needed min. vol. & best Vent. calculates needed min. vol. & best
rate/TV to produces rate/TV to produces least work.least work. Targeted TV’s given as press. control or Targeted TV’s given as press. control or
press. support breathspress. support breaths Breath is: PC if time triggered, PS if pt. Breath is: PC if time triggered, PS if pt.
triggeredtriggered

Newer Ventilator Dual Modes: Hamilton Galileo’s ASV (adapt. sup. vent.)
Vent. measures & analyzes data & mechanics each Vent. measures & analyzes data & mechanics each breath for:breath for: compliancecompliance resistanceresistance inspiratory & expiratory time constantsinspiratory & expiratory time constants actual I-time, E-time, total f & min. vol. actual I-time, E-time, total f & min. vol. pressurespressures
Press. adjusts in +/- 2 cm HPress. adjusts in +/- 2 cm H22O to achieve TVO to achieve TV

Newer Ventilator Dual Modes: Hamilton Galileo’s ASV - Considerations
Mandatory breaths = PC, pt. triggered = PSMandatory breaths = PC, pt. triggered = PS both at same targeted TV and calculated both at same targeted TV and calculated
press.press.

ASV: Principle mode of ventilation
Pinsp
PEEP
no patient activity:* machine triggered+ time cycled
patient is active:* patient triggered+ flow cycled
Flow I
Flow E * *
+ +
From Hamilton Medical

Newer Ventilator Dual Modes: Hamilton Galileo’s ASV - Considerations
If pt.’s f > “set” by vent., mode is PSIf pt.’s f > “set” by vent., mode is PS If pt.’s f < “set” by vent., mode is PC-SIMV/PSIf pt.’s f < “set” by vent., mode is PC-SIMV/PS If patient is apneic, all breaths are PCIf patient is apneic, all breaths are PC
Mandatory breaths = PC, pt. triggered = PSMandatory breaths = PC, pt. triggered = PS both at same targeted TV and calculated press.both at same targeted TV and calculated press.

Newer Ventilator Dual Modes: Hamilton Galileo’s ASV: Considerations
Using “least work” as a criteria:Using “least work” as a criteria: calculation for needed rate may change,calculation for needed rate may change, therefore calculated TV may change, andtherefore calculated TV may change, and therefore calculated pressure needed for TV therefore calculated pressure needed for TV
may changemay change Both max. & min. TV limits are usedBoth max. & min. TV limits are used As patient improves,”support” is decreasedAs patient improves,”support” is decreased
pressure can be reduced to PEEP + 5 cm H2Opressure can be reduced to PEEP + 5 cm H2O

Newer Ventilator Dual Modes: Summary:
Combined methods of press. & volume Combined methods of press. & volume ventilation ventilation maymay replace standard volume replace standard volume ventilation.ventilation.
Prudent use of high pressure limits (and Prudent use of high pressure limits (and volume limits if available) and careful volume limits if available) and careful monitoring can decrease disadvantages of monitoring can decrease disadvantages of combined modes.combined modes.
Newer Ventilator Dual Modes: Evidence:
VAPS:VAPS: No randomized controlled trials (RCT)No randomized controlled trials (RCT) 2 observational studies, 1 bench study 2 observational studies, 1 bench study
with test lungwith test lung Lower level outcomes:Lower level outcomes:
Reduced workReduced work Evid. levels III, B & level V, CEvid. levels III, B & level V, C

Newer Ventilator Dual Modes: Evidence:
PRVC/VS PRVC/VS (also referred to as “adaptive PC”)(also referred to as “adaptive PC”):: 2 small randomized controlled trials (RCT): post-op 2 small randomized controlled trials (RCT): post-op
pts, no survival benefit, no diff or slightly shorter vent pts, no survival benefit, no diff or slightly shorter vent time, less interventions & blood gasestime, less interventions & blood gases
3 other randomized cross-over observational studies, & 3 other randomized cross-over observational studies, & 5 other cross-over short term obs. studies: safe, small 5 other cross-over short term obs. studies: safe, small differences in lower PIP, some shorter to extubationdifferences in lower PIP, some shorter to extubation
Lower level outcomes:Lower level outcomes: Small RCT trials: II, grade B evidenceSmall RCT trials: II, grade B evidence Small cross-over studies III, grade CSmall cross-over studies III, grade C

Newer Ventilator Dual Modes: Evidence:
ASV:ASV: 2 small randomized controlled trials (RCT): no survival 2 small randomized controlled trials (RCT): no survival
benefit, sub-group (10 infants) shorter vent time, less benefit, sub-group (10 infants) shorter vent time, less BPD; adult study showed only less PIP in PRVCBPD; adult study showed only less PIP in PRVC
3 other cross-over observational studies, lower PIP, 3 other cross-over observational studies, lower PIP, (better gas exchange in animal study only)(better gas exchange in animal study only)
Lower level outcomes:Lower level outcomes: Small RCT trials: II, grade B evidenceSmall RCT trials: II, grade B evidence Small cross-over studies III for humans, V for Small cross-over studies III for humans, V for
animal study, all grade Canimal study, all grade C

New Modes of Mechanical Ventilation: Bi-level ventilation methods Ventilation methods that allow spontaneous Ventilation methods that allow spontaneous
breathing at two airway pressures:breathing at two airway pressures: BiPAP (Drager E-4 & E-2 dura)BiPAP (Drager E-4 & E-2 dura) BiLevel (NPB 840)BiLevel (NPB 840) APRV (NPB 840, Drager E-4 & E-2 dura)APRV (NPB 840, Drager E-4 & E-2 dura)
Pressure targeted strategy & spont. Breathing Pressure targeted strategy & spont. Breathing can fit lung protective criteriacan fit lung protective criteria

Spontaneous Breaths
P
T
Spontaneous Breaths
BiLevel Ventilation: NPB 840BiLevel Ventilation: NPB 840
Uses two levels of pressure for two time periodsUses two levels of pressure for two time periods Mandatory breaths at the higher pressure are time Mandatory breaths at the higher pressure are time
cycledcycled Spontaneous breaths can be pressure supportedSpontaneous breaths can be pressure supported
From PB product lit.

P
T
Synchronized Transitions
PEEPHIGH
PEEPLOW
TLOW
THIGH
Synchronized Transitions
BiLevel Ventilation: NPB 840BiLevel Ventilation: NPB 840
Uses 2 pressure levels for 2 time periodsUses 2 pressure levels for 2 time periods PEEPPEEPlowlow & PEEP & PEEPhighhigh, T, Thighhigh and T and Tlow low
Patient triggering & cycling can change phasesPatient triggering & cycling can change phases
From PB product lit.

PEEPHigh + PS
P
PEEPL
PEEPH
Pressure Support
BiLevel Ventilation: NPB 840BiLevel Ventilation: NPB 840
Pressure support may be applied at both Pressure support may be applied at both pressures during a spont. breathpressures during a spont. breath If PS is set higher than PEEPIf PS is set higher than PEEPHH, the PS pressure is , the PS pressure is
applied to a spontaneous effort at upper pressureapplied to a spontaneous effort at upper pressure
From PB product lit.

Spontaneous Breaths
P Pressure Support
T
BiLevel Ventilation: NPB 840BiLevel Ventilation: NPB 840
If PS is set lower than PEEPIf PS is set lower than PEEPHH, PS is , PS is
applied to patient efforts at the lower applied to patient efforts at the lower pressure, PEEPpressure, PEEPLL
From PB product lit.

APRV (Drager ventilators)
Airway Pressure Release VentilationAirway Pressure Release Ventilation Like BiPAP/BiLevel but time at the lower Like BiPAP/BiLevel but time at the lower
pressure (“release time”) is usually short, pressure (“release time”) is usually short, 1-1.5 seconds1-1.5 seconds
Spontaneous breathing still allowed Spontaneous breathing still allowed throughout low & high pressuresthroughout low & high pressures

APRV (Drager ventilators)
Airway Pressure Release VentilationAirway Pressure Release Ventilation
From Mosby’s R. C. Equip. 6th ed. 1999.

Newer Methods of Ventilatory Support: Proportional Assist Ventilation
PAV - currently on PB 840 in US PAV - currently on PB 840 in US prototype/research ventilators, Drager Evita prototype/research ventilators, Drager Evita 4 & Respironics BiPAP Vision4 & Respironics BiPAP Vision
Allows free flow based on patient effortAllows free flow based on patient effort ““Targets” portion of patient’s Targets” portion of patient’s workwork during during
“spontaneous” breaths“spontaneous” breaths Automatically adjusts flow, volume and Automatically adjusts flow, volume and
pressure needed each breathpressure needed each breath

Methods of Ventilatory Support: PAV continued
““Vol. assist %” reduces work of elastanceVol. assist %” reduces work of elastance ““Flow assist%” reduces work of resistance'sFlow assist%” reduces work of resistance's Pressure adjusts during each breath to Pressure adjusts during each breath to
control work levelcontrol work level Increased patient effort causes increased Increased patient effort causes increased
applied pressure (and flow & volume)applied pressure (and flow & volume)

Methods of Ventilatory Support: PAV continued
From Younes, M: Ch.15, in Tobin, MJ From Younes, M: Ch.15, in Tobin, MJ Prin. & Pract. Of Mech. Vent.Prin. & Pract. Of Mech. Vent. 1994 1994 McGaw-Hill, Inc.McGaw-Hill, Inc.

Methods of Ventilatory Support: PAV continued
Other controls useful for PAV:Other controls useful for PAV: High pressure limitHigh pressure limit High volume limitHigh volume limit Back-up ventilation modeBack-up ventilation mode Typical alarms etc.Typical alarms etc.

Methods of Ventilatory Support: PAV - Considerations
Consistent level of support per breathConsistent level of support per breath Patient controls breathing patternPatient controls breathing pattern Patient triggered modePatient triggered mode
(Unless back-up mode present)(Unless back-up mode present) Reduced support with Auto-PEEPReduced support with Auto-PEEP Cannot compensate for leaks (prototypes)Cannot compensate for leaks (prototypes)
Methods of Ventilatory Support: PAV -Evidence
Huge number of studies since 1992.Huge number of studies since 1992. BUT, almost no large RCTs. Most were small, BUT, almost no large RCTs. Most were small,
short term observational comparing PAV to short term observational comparing PAV to pressure support.pressure support.
Largest trial in NIPPV for ARF: showed no Largest trial in NIPPV for ARF: showed no difference for intubation, stay, mortality. Better difference for intubation, stay, mortality. Better comfort for PAVcomfort for PAV
Most all other trials rated level III, grades or C.Most all other trials rated level III, grades or C.

New Modes of Mechanical Ventilation: Other neat stuff

New Modes of Mechanical Ventilation: Other neat stuff
Automatic tube Automatic tube compensation: compensation: Drager Evita 4Drager Evita 4
From Drager prod. lit.

New Modes of Mechanical Ventilation: Summary Older modes & ventilators:Older modes & ventilators:
passive, operator-dependant toolspassive, operator-dependant tools New modes on new generation ventilators:New modes on new generation ventilators:
adaptively interactiveadaptively interactive goal orientedgoal oriented patient centeredpatient centered
Adapted from John J. Marini, MD; AARC congress, Adapted from John J. Marini, MD; AARC congress, 11/9811/98





![Dual controlled modes of mechanical ventilation [onarılmış]](https://static.fdocuments.in/doc/165x107/5871a5ac1a28abda6a8b471f/dual-controlled-modes-of-mechanical-ventilation-onarilmis.jpg)




![2007 Evidence Base for Newer Modes of Mechanical Ventilation[1]](https://static.fdocuments.in/doc/165x107/5524dee34a7959f90c8b4606/2007-evidence-base-for-newer-modes-of-mechanical-ventilation1.jpg)