2004 ISMRM E-poster Effect of Reduced Encoding Dynamic Data Size on Permeability-Surface Area...
6
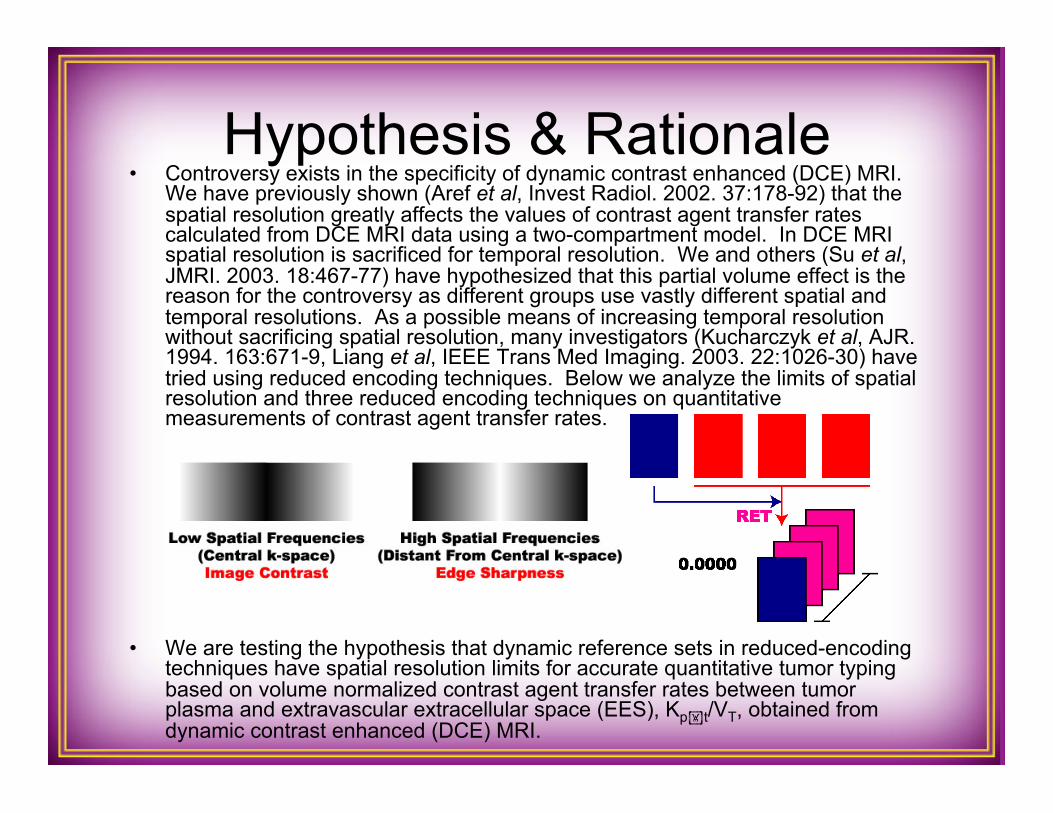
Hypothesis & Rationale • Controversy exists in the specificity of dynamic contrast enhanced (DCE) MRI. We have previously shown (Aref et al, Invest Radiol. 2002. 37:178-92) that the spatial resolution greatly affects the values of contrast agent transfer rates calculated from DCE MRI data using a two-compartment model. In DCE MRI spatial resolution is sacrificed for temporal resolution. We and others (Su et al, JMRI. 2003. 18:467-77) have hypothesized that this partial volume effect is the reason for the controversy as different groups use vastly different spatial and temporal resolutions. As a possible means of increasing temporal resolution without sacrificing spatial resolution, many investigators (Kucharczyk et al, AJR. 1994. 163:671-9, Liang et al, IEEE Trans Med Imaging. 2003. 22:1026-30) have tried using reduced encoding techniques. Below we analyze the limits of spatial resolution and three reduced encoding techniques on quantitative measurements of contrast agent transfer rates. • We are testing the hypothesis that dynamic reference sets in reduced-encoding techniques have spatial resolution limits for accurate quantitative tumor typing based on volume normalized contrast agent transfer rates between tumor plasma and extravascular extracellular space (EES), K pt /V T , obtained from dynamic contrast enhanced (DCE) MRI.
-
Upload
mike-aref -
Category
Health & Medicine
-
view
996 -
download
0
Transcript of 2004 ISMRM E-poster Effect of Reduced Encoding Dynamic Data Size on Permeability-Surface Area...
Hypothesis & Rationale • Controversy exists in the specificity of dynamic contrast enhanced (DCE) MRI.
We have previously shown (Aref et al, Invest Radiol. 2002. 37:178-92) that the spatial resolution greatly affects the values of contrast agent transfer rates calculated from DCE MRI data using a two-compartment model. In DCE MRI spatial resolution is sacrificed for temporal resolution. We and others (Su et al, JMRI. 2003. 18:467-77) have hypothesized that this partial volume effect is the reason for the controversy as different groups use vastly different spatial and temporal resolutions. As a possible means of increasing temporal resolution without sacrificing spatial resolution, many investigators (Kucharczyk et al, AJR. 1994. 163:671-9, Liang et al, IEEE Trans Med Imaging. 2003. 22:1026-30) have tried using reduced encoding techniques. Below we analyze the limits of spatial resolution and three reduced encoding techniques on quantitative measurements of contrast agent transfer rates.
• We are testing the hypothesis that dynamic reference sets in reduced-encoding techniques have spatial resolution limits for accurate quantitative tumor typing based on volume normalized contrast agent transfer rates between tumor plasma and extravascular extracellular space (EES), Kpt/VT, obtained from dynamic contrast enhanced (DCE) MRI.
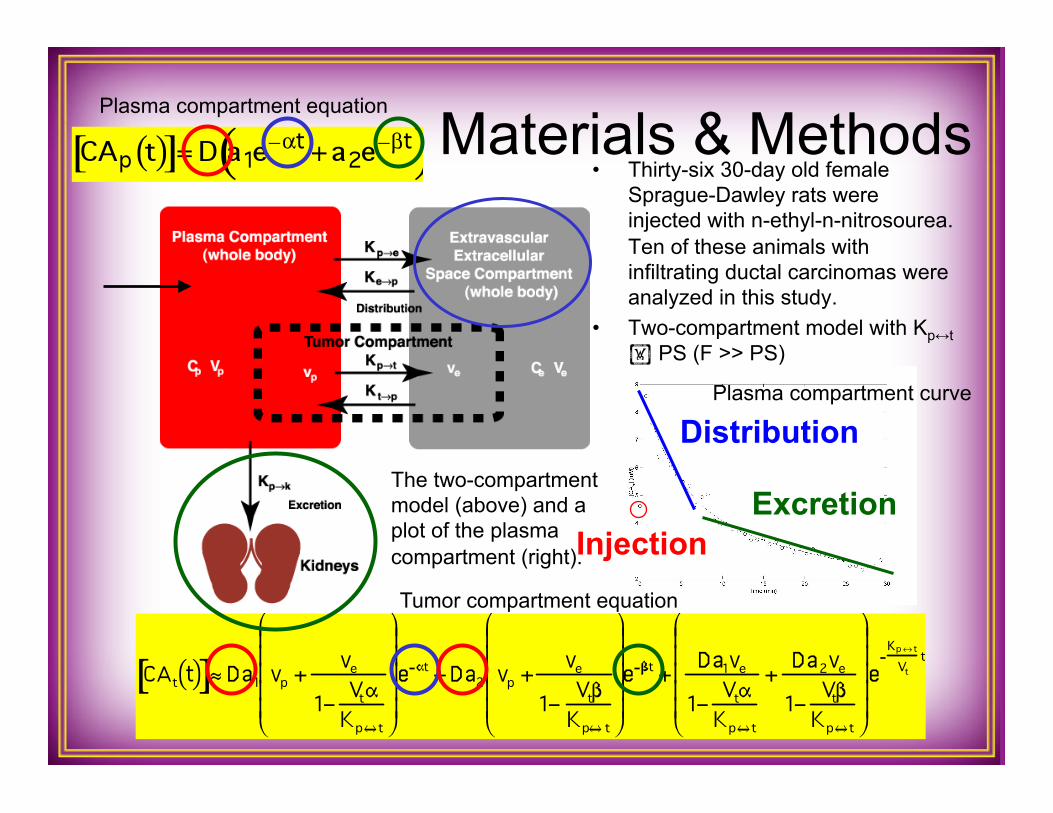
• Thirty-six 30-day old female Sprague-Dawley rats were injected with n-ethyl-n-nitrosourea. Ten of these animals with infiltrating ductal carcinomas were analyzed in this study.
• Two-compartment model with Kp↔t PS (F >> PS)
Materials & Methods
Distribution
Excretion Injection
The two-compartment model (above) and a plot of the plasma compartment (right).
Plasma compartment equation
Tumor compartment equation
Plasma compartment curve

Materials & Methods
Tumor
Heart
Liver
Bladder Image Ref.
Results Keyhole Difference Images TRIGR Difference Images
RIGR Difference Images
FFT
FFT
FFT
128 64 32 24 16 4
128 64 32 24 16 4
128 64 32 24 16 4
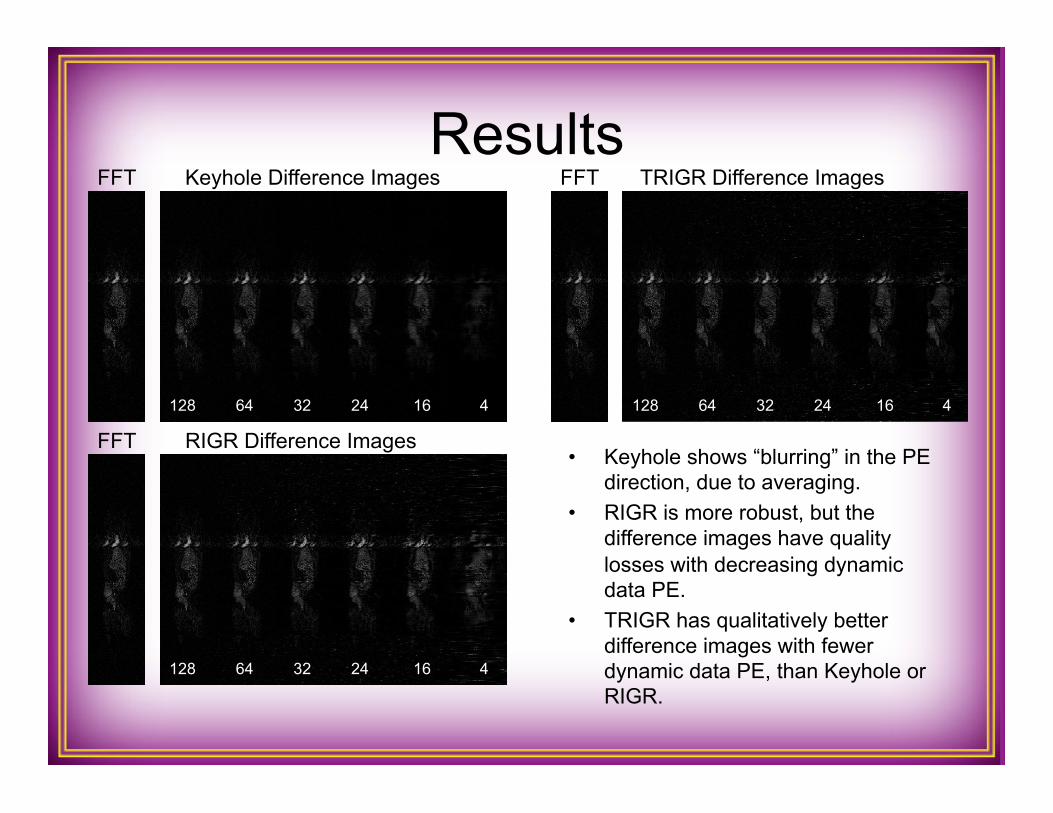
• Keyhole shows “blurring” in the PE direction, due to averaging.
• RIGR is more robust, but the difference images have quality losses with decreasing dynamic data PE.
• TRIGR has qualitatively better difference images with fewer dynamic data PE, than Keyhole or RIGR.
Results
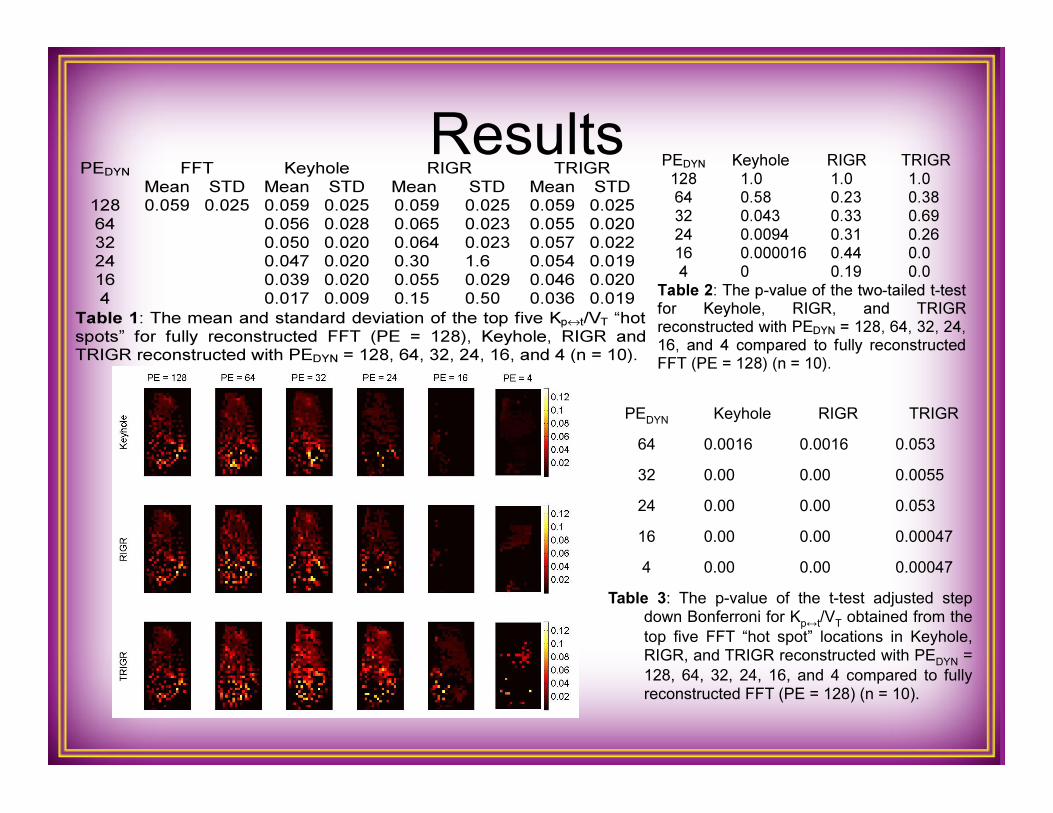
PEDYN Keyhole RIGR TRIGR 64 0.0016 0.0016 0.053 32 0.00 0.00 0.0055 24 0.00 0.00 0.053 16 0.00 0.00 0.00047 4 0.00 0.00 0.00047
Table 3: The p-value of the t-test adjusted step down Bonferroni for Kp↔t/VT obtained from the top five FFT “hot spot” locations in Keyhole, RIGR, and TRIGR reconstructed with PEDYN = 128, 64, 32, 24, 16, and 4 compared to fully reconstructed FFT (PE = 128) (n = 10).
Conclusions • Keyhole: the top five Kpt/VT “hot spots” from fully reconstructed FFT and
Keyhole are statistically the same only at PEDYN = 128 and 64. • RIGR: the top five Kpt/VT “hot spots” are statistically the same as FFT for all
PEDYN, as a result of very large standard deviations. • TRIGR: the top five Kpt/VT “hot spots” from TRIGR and FFT are the same at
PEDYN = 128, 64, 32, and 24. In addition, using reduced dynamic data, PEDYN = 64 and 24, TRIGR localizes statistically similar “hot spots” as those obtained from FFT maps.
• As PEDYN decreases the generalized-series techniques are better able to accurately estimate image data and hence provide more accurate quantitative dynamic contrast information than Keyhole.
• Although RIGR agrees with FFT at all PEDYN and appears statistically superior to TRIGR, RIGR has unrealistic outlier Kpt/VT “hot spots” and large standard deviations at lower PEDYN not seen with TRIGR. Furthermore, RIGR does not localize statistically similar “hot spots” as FFT.
• Keyhole has the most limited dynamic data threshold and TRIGR more accurately obtains clinical low-resolution dynamic data, PEDYN = 64, 32, and 24, and more accurately localizes “hot spots”, PEDYN = 64 and 24, than both Keyhole and RIGR.
• This implies that one can gain at least a fivefold (5.33) improvement in spatial resolution without sacrificing the necessary temporal resolution.