2002 FRACP Written Examination Paediatrics & Child
54
2002 FRACP Written Examination Paediatrics & Child Health Paper 2 – Clinical Applications Introduction Format Paper 1 – Medical Sciences: 70 questions; time allowed: 2 hours Paper 2 – Clinical Applications: 100 questions; time allowed: 3 hours All questions are in the A-type multiple-choice format, that is, the single best answer of the five options given. In the questions, values appearing within [ ] refer to normal ranges. When visual material has been turned on its side, an arrow on the page indicates the orientation of the visual material. Questions do not necessarily appear in the order in which they were first printed. Answers A table of answers is located at the end of each paper. Scoring A correct answer will score one mark and an incorrect answer zero. There is no negative marking in the FRACP Written Examination. Queries Contact the Executive Officer, Examinations Section, Department of Training and Assessment via e- mail: [email protected]. Please note that with changes in medical knowledge, some of the information may no longer be current. Copyright © 2004 by The Royal Australasian College of Physicians All Written Examination papers are copyright. They may not be reproduced in whole or part without written permission from The Royal Australasian College of Physicians, 145 Macquarie Street, Sydney, Australia.
Transcript of 2002 FRACP Written Examination Paediatrics & Child
2002 FRACP Written Examination
Paediatrics & Child Health
Paper 2 – Clinical Applications
Introduction Format Paper 1 – Medical Sciences: 70 questions; time allowed: 2 hours Paper 2 – Clinical Applications: 100 questions; time allowed: 3 hours All questions are in the A-type multiple-choice format, that is, the single best answer of the five options given. In the questions, values appearing within [ ] refer to normal ranges. When visual material has been turned on its side, an arrow on the page indicates the orientation of the visual material. Questions do not necessarily appear in the order in which they were first printed. Answers A table of answers is located at the end of each paper. Scoring A correct answer will score one mark and an incorrect answer zero. There is no negative marking in the FRACP Written Examination. Queries Contact the Executive Officer, Examinations Section, Department of Training and Assessment via e-mail: [email protected]. Please note that with changes in medical knowledge, some of the information may no longer be current. Copyright © 2004 by The Royal Australasian College of Physicians All Written Examination papers are copyright. They may not be reproduced in whole or part without written permission from The Royal Australasian College of Physicians, 145 Macquarie Street, Sydney, Australia.
2 P202 QUESTION 1 Which one of the following, occurring in the first year of life, is most indicative of atopy? A. Chronic rhinitis. B. Chronic serous otitis media. C. Eczema. D. Recurrent wheeze. E. Urticaria. QUESTION 2 A universal neonatal hearing screening program targets children with congenital bilateral hearing impairment. The best indicator of the effectiveness of the program is: A. language ability of the target population at five years of age. B. median age of entry into early intervention services. C. median age of fitting hearing aids. D. number of deaf children detected by six months of age. E. proportion of population screened. QUESTION 3 A nine-year-old girl presents with obesity. Her height is on the 10th percentile, weight on the 97th percentile and she has a round face. Shortening of the fourth metacarpals bilaterally are found and confirmed by X-ray. Which finding would be most helpful in establishing a diagnosis of pseudohypoparathyroidism? A. Basal ganglia calcification. B. Increased fasting plasma insulin/glucose ratio. C. Increased plasma calcium. D. Increased serum alkaline phosphatase. E. Increased serum parathyroid hormone.
Copyright © 2004 by The Royal Australasian College of Physicians
3 P202 QUESTION 4 An 18-month-old girl presents with a history of persistent diarrhoea and poor weight gain since eight months of age. Her weight has progressively fallen from the 50th percentile to below the 3rd percentile. Over the past month her abdomen has become increasingly distended and on physical examination she has evidence of ascites. Faecal microscopy reveals large amounts of fat globules. Her laboratory findings are shown below. Haemoglobin 125 g/L [105-135] White cell count 7.1 x 109/L [6.0-18.0] differential: neutrophils 6.4 x 109/L [1.0-8.5] lymphocytes 0.4 x 109/L [4.0-10.0] eosinophils 0.3 x 109/L [0-0.8] Platelet count 355 x 109/L [150-400] Serum IgG 2.14 g/L [2.71-13.78] Serum IgM 0.42 g/L [0.35-1.35] Serum IgA <0.07 g/L [0.17-1.34] Which one of the following is the most likely diagnosis? A. Chronic liver disease. B. Coeliac disease. C. Common variable immunodeficiency. D. Congenital cytomegalovirus infection. E. Intestinal lymphangiectasia. QUESTION 5 A two-day-old neonate presents with copious purulent eye and nose discharge. Laboratory examination is performed to diagnose the organism involved. Which one of the following types of organism would carry the worst prognosis if not treated immediately? A. Gram-negative coccobacillus. B. Gram-negative diplococcus. C. Gram-positive bacillus. D. Gram-positive coccus. E. Intra-cytoplasmic inclusion bodies.
Copyright © 2004 by The Royal Australasian College of Physicians
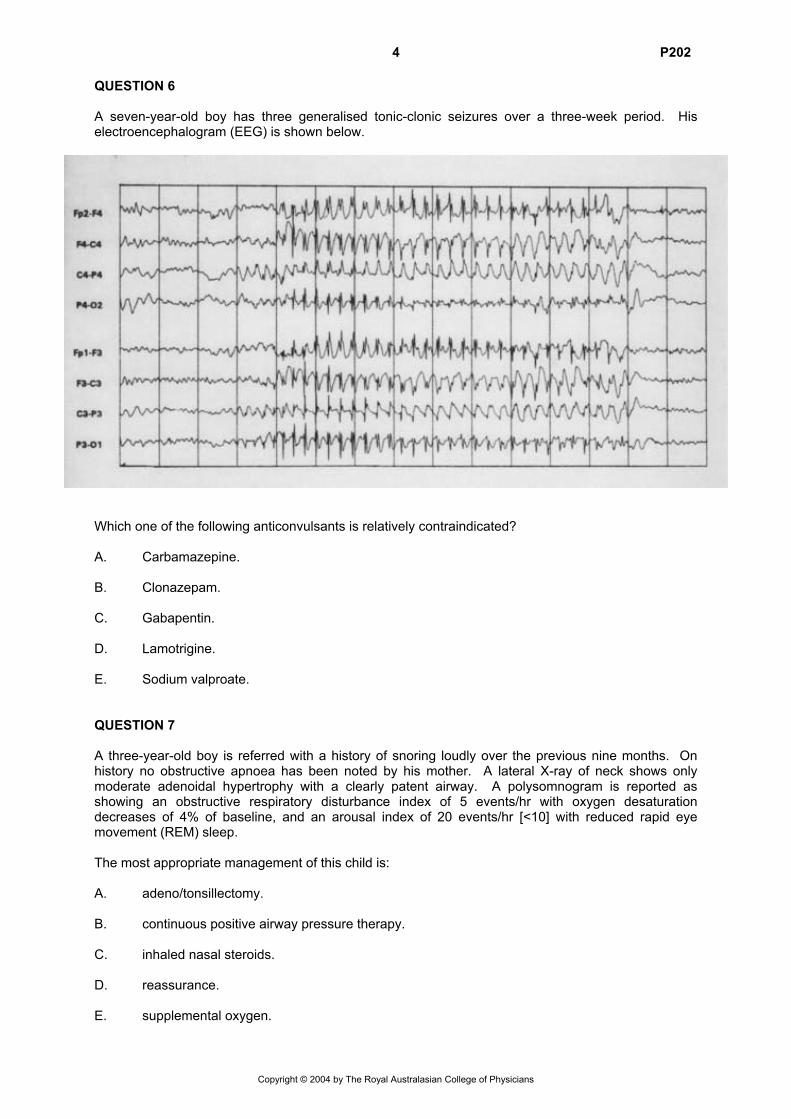
4 P202 QUESTION 6 A seven-year-old boy has three generalised tonic-clonic seizures over a three-week period. His electroencephalogram (EEG) is shown below.
Which one of the following anticonvulsants is relatively contraindicated? A. Carbamazepine. B. Clonazepam. C. Gabapentin. D. Lamotrigine. E. Sodium valproate. QUESTION 7 A three-year-old boy is referred with a history of snoring loudly over the previous nine months. On history no obstructive apnoea has been noted by his mother. A lateral X-ray of neck shows only moderate adenoidal hypertrophy with a clearly patent airway. A polysomnogram is reported as showing an obstructive respiratory disturbance index of 5 events/hr with oxygen desaturation decreases of 4% of baseline, and an arousal index of 20 events/hr [<10] with reduced rapid eye movement (REM) sleep. The most appropriate management of this child is: A. adeno/tonsillectomy. B. continuous positive airway pressure therapy. C. inhaled nasal steroids. D. reassurance. E. supplemental oxygen.
Copyright © 2004 by The Royal Australasian College of Physicians
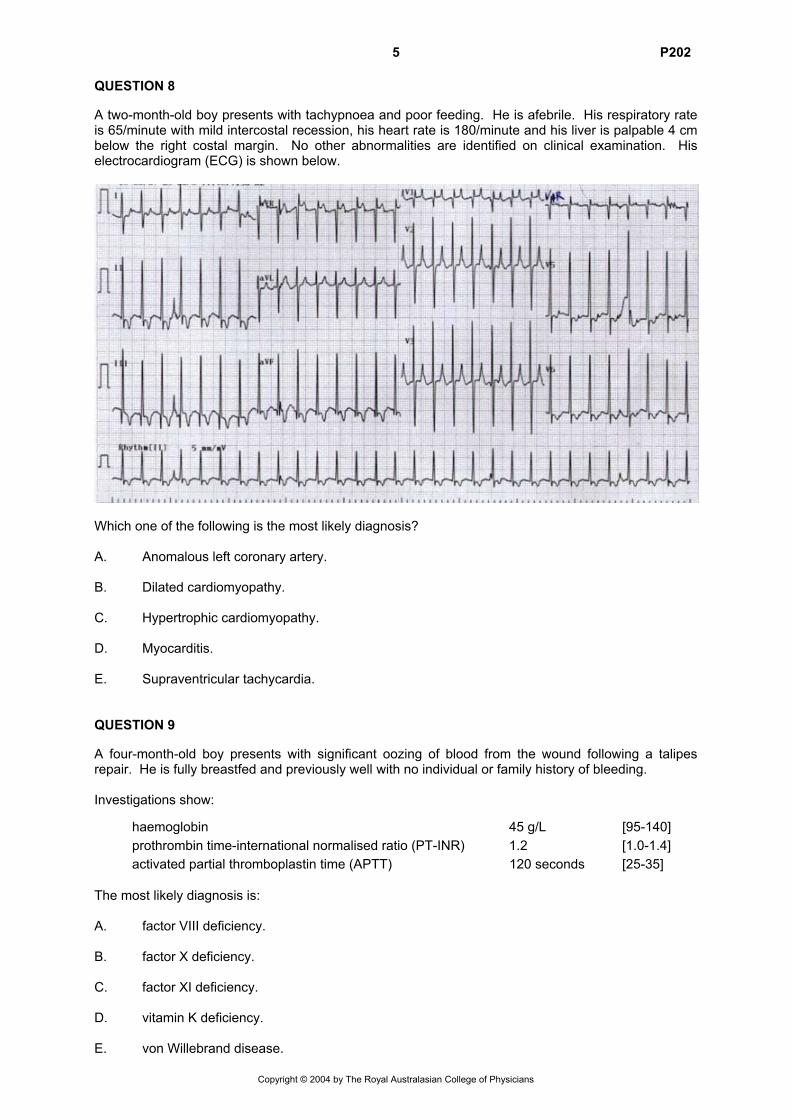
5 P202 QUESTION 8 A two-month-old boy presents with tachypnoea and poor feeding. He is afebrile. His respiratory rate is 65/minute with mild intercostal recession, his heart rate is 180/minute and his liver is palpable 4 cm below the right costal margin. No other abnormalities are identified on clinical examination. His electrocardiogram (ECG) is shown below.
Which one of the following is the most likely diagnosis? A. Anomalous left coronary artery. B. Dilated cardiomyopathy. C. Hypertrophic cardiomyopathy. D. Myocarditis. E. Supraventricular tachycardia. QUESTION 9 A four-month-old boy presents with significant oozing of blood from the wound following a talipes repair. He is fully breastfed and previously well with no individual or family history of bleeding. Investigations show:
haemoglobin 45 g/L [95-140] prothrombin time-international normalised ratio (PT-INR) 1.2 [1.0-1.4] activated partial thromboplastin time (APTT) 120 seconds [25-35] The most likely diagnosis is: A. factor VIII deficiency. B. factor X deficiency. C. factor XI deficiency. D. vitamin K deficiency. E. von Willebrand disease.
Copyright © 2004 by The Royal Australasian College of Physicians
6 P202 QUESTION 10 In which one of the following clinical settings is there the best evidence that prophylactic antibiotics protect against infection? A. Cerebrospinal fluid shunt insertion. B. Chest drain insertion for pneumothorax. C. Occipital skull fracture. D. Umbilical artery catheterisation. E. Urinary catheterisation. QUESTION 11 Severe congenital bilateral hearing loss is diagnosed in the first-born child of first cousin parents. Both parents are Caucasian. Which one of the following investigations is most likely to reveal the underlying cause of this child’s deafness? A. Electrocardiogram (ECG). B. Measurement of inner canthal distance. C. Polymerase chain reaction (PCR) for common Connexin 26 mutation. D. Rubella titres (IgG and IgM). E. Thyroid function testing.
Copyright © 2004 by The Royal Australasian College of Physicians
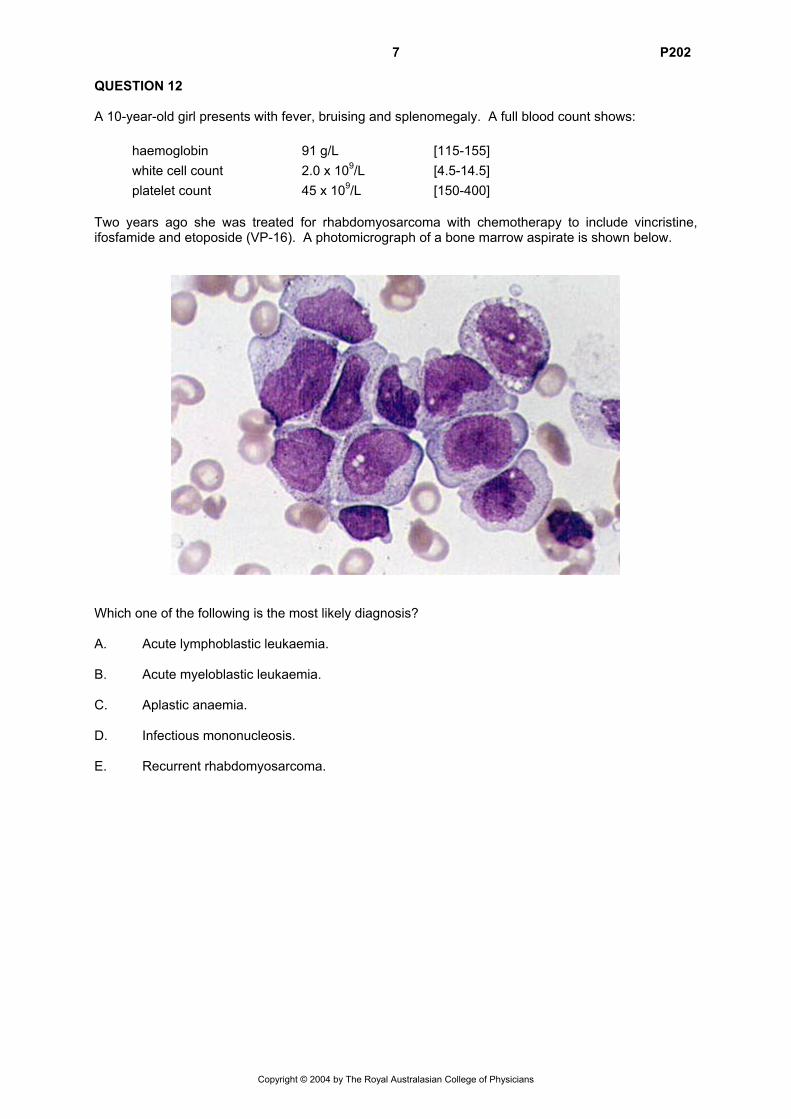
7 P202 QUESTION 12 A 10-year-old girl presents with fever, bruising and splenomegaly. A full blood count shows: haemoglobin 91 g/L [115-155] white cell count 2.0 x 109/L [4.5-14.5] platelet count 45 x 109/L [150-400] Two years ago she was treated for rhabdomyosarcoma with chemotherapy to include vincristine, ifosfamide and etoposide (VP-16). A photomicrograph of a bone marrow aspirate is shown below.
Which one of the following is the most likely diagnosis? A. Acute lymphoblastic leukaemia. B. Acute myeloblastic leukaemia. C. Aplastic anaemia. D. Infectious mononucleosis. E. Recurrent rhabdomyosarcoma.
Copyright © 2004 by The Royal Australasian College of Physicians
8 P202 QUESTION 13 A five-year-old boy presents to hospital with a four-day history of lethargy and dark coloured urine. On examination his blood pressure is 130/90 mmHg. He has mild periorbital oedema and his neck veins are easily visible. No neurological abnormalities are detected. His mid stream urine reveals >1000 red cells, few red and white cell casts and 3+ protein on albustix. His initial blood results show the following: haemoglobin 100 g/L [110-145] plasma sodium 136 mmol/L [135-146] plasma potassium 5.6 mmol/L [3.5-5.0] plasma urea 30.0 mmol/L [1.8-5.5] plasma creatinine 0.38 mmol/L [0.04-0.07] serum complement C3 0.15 g/L [0.80-1.80] Which one of the following is the most appropriate initial management? A. Albumin infusion. B. Fluid restriction. C. Glucose and insulin infusion. D. Intravenous diazoxide. E. Protein restriction. QUESTION 14 A six-year-old boy presents with a history of being difficult to manage in class because of fidgetiness and poor concentration that disturbs other class members, and outbursts of poor temper with apparently little provocation. His learning is progressing erratically, though there are periods where he appears to concentrate well. A medical history reveals that he has had ear infections in the past treated with drainage tubes, without hearing impairment. He snores at night and tends to wake up in a poor mood in the morning. He is on no current medication. The most appropriate next step in management is: A. behavioural modification. B. psychometric assessment with special education planning. C. refer for sleep studies. D. stimulant medication. E. stimulant medication and behavioural modification.
Copyright © 2004 by The Royal Australasian College of Physicians
9 P202 QUESTION 15 A 14-year-old girl presents to the emergency department with a 12-hour history of a blistering rash. The rash is extremely itchy and is spreading up her arm. She is otherwise well and afebrile. A history is obtained that she had been gardening on the day prior to the rash developing. A diagnosis of an allergic contact dermatitis is made. Which one of the following is the most appropriate initial therapy? A. Intravenous antihistamines. B. Oral antihistamines. C. Oral corticosteroids. D. Subcutaneous adrenaline. E. Topical corticosteroids. QUESTION 16 A two-year-old girl is referred because of breast development for the past six months. There is no history of a growth spurt and she has not been on any medications. Her height and weight are on the 25th percentile. She has Tanner stage 3 breast development, 3 cm in diameter, and pubic hair stage 1. There are no skin lesions and her neurological examination is normal. Relevant investigations show: luteinising hormone 0.3 U/L [0.1-1.0] follicle-stimulating hormone 1.1 U/L [0.3-1.1] oestradiol 40 pmol/L [30-60] bone age 2.5 years Pelvic ultrasound: uterus:cervix ratio 0.95 (prepubertal <1) left ovary 1.2 mL (prepubertal volume <3 mL) right ovary 2.5 mL with several 5 mm follicles The most likely diagnosis is: A. granulosa cell tumour of the ovary. B. idiopathic precocious puberty. C. idiopathic premature adrenarche. D. idiopathic premature thelarche. E. McCune-Albright syndrome.
Copyright © 2004 by The Royal Australasian College of Physicians
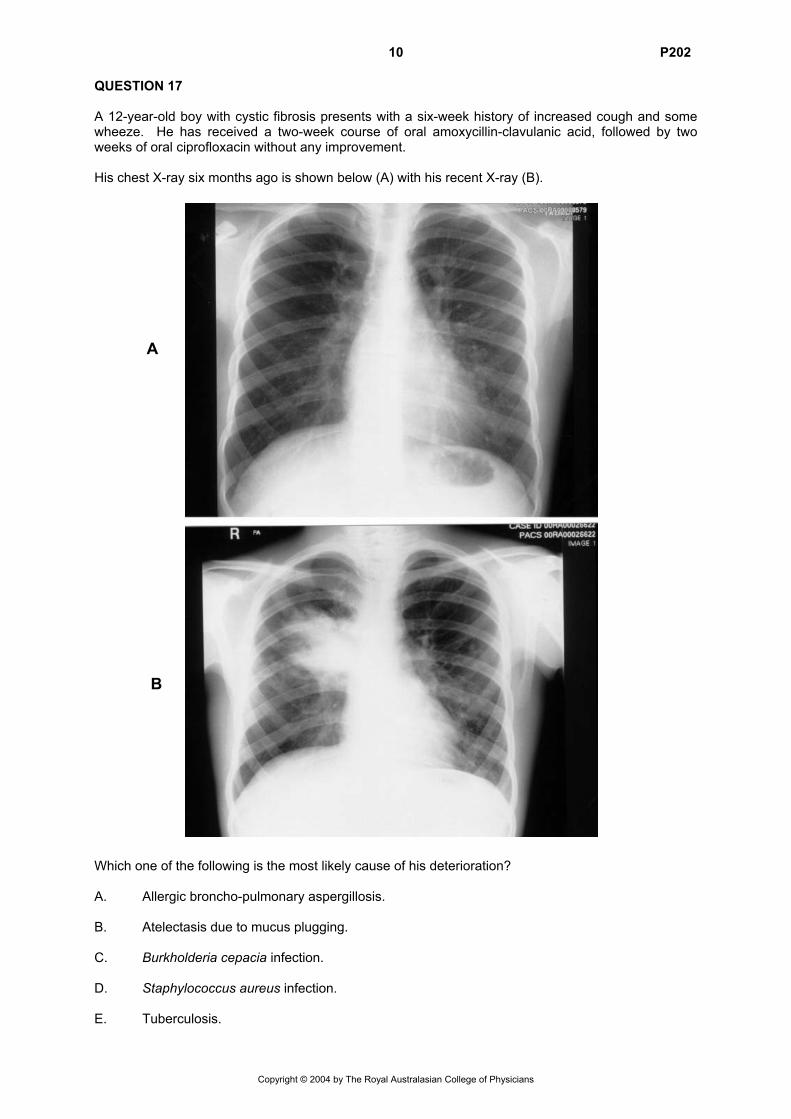
10 P202 QUESTION 17 A 12-year-old boy with cystic fibrosis presents with a six-week history of increased cough and some wheeze. He has received a two-week course of oral amoxycillin-clavulanic acid, followed by two weeks of oral ciprofloxacin without any improvement. His chest X-ray six months ago is shown below (A) with his recent X-ray (B).
A
B Which one of the following is the most likely cause of his deterioration? A. Allergic broncho-pulmonary aspergillosis. B. Atelectasis due to mucus plugging. C. Burkholderia cepacia infection. D. Staphylococcus aureus infection. E. Tuberculosis.
Copyright © 2004 by The Royal Australasian College of Physicians
11 P202 QUESTION 18 A three-month-old baby with vomiting and profuse watery diarrhoea presents 10% dehydrated. The following results are obtained: serum: sodium 160 mmol/L [135-145] potassium 3.9 mmol/L [3.5-4.5] urea 9.6 mmol/L [1.0-6.0] glucose 13.8 mmol/L [4.0-8.0] blood pressure 75 mmHg systolic A stool sample is positive for rotavirus. The most appropriate fluid management is: A. 0.18% sodium chloride plus 4.3% dextrose plus 20 mmol/L potassium chloride intravenously
(IV) to rehydrate over 48 hours. B. 0.45% sodium chloride plus 5.0% dextrose plus 20 mmol/L potassium chloride IV to rehydrate
over 24 hours. C. 0.45% sodium chloride plus 5.0% dextrose plus 20 mmol/L potassium chloride IV to rehydrate
over 48 hours. D. intensive breastfeeding. E. oral rehydration fluid given nasogastrically to rehydrate over 24 hours. QUESTION 19 An 18-month-old boy has recurrent blue breath-holding episodes, followed on one occasion by a 15-second generalised seizure. The investigation most likely to be useful in directing therapy is: A. electrocardiogram (ECG). B. electroencephalogram (EEG). C. iron studies. D. plasma calcium. E. plasma glucose.
Copyright © 2004 by The Royal Australasian College of Physicians
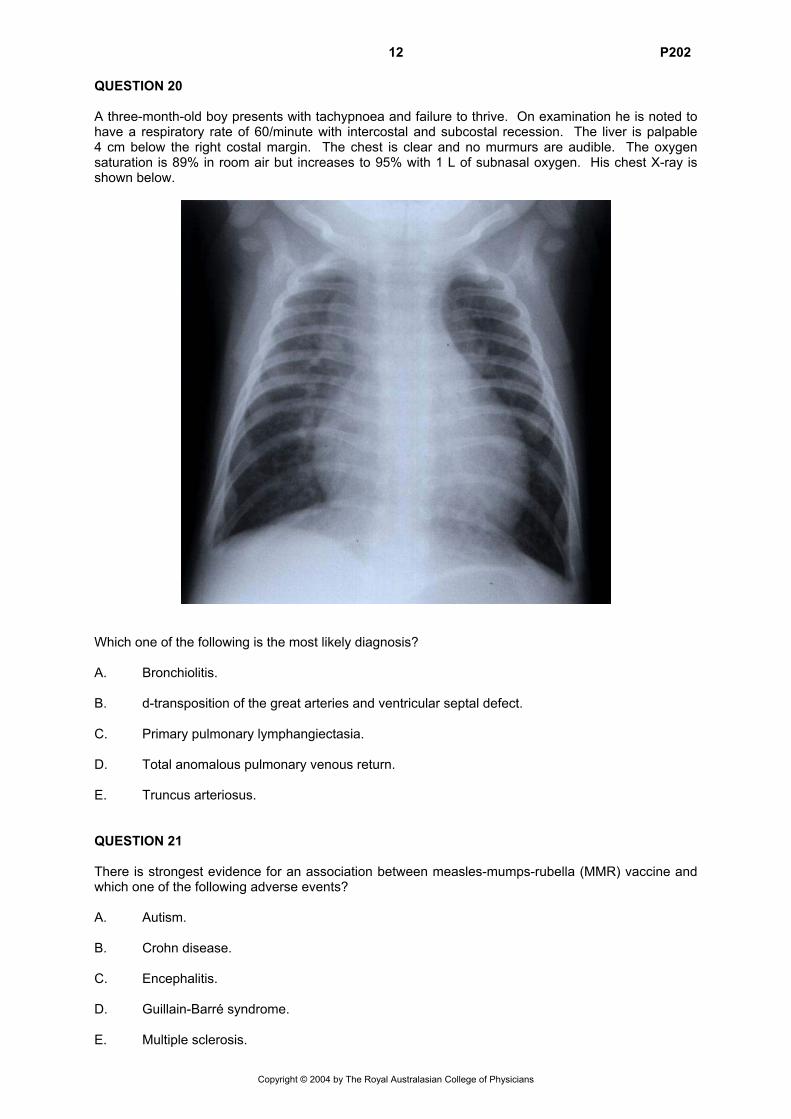
12 P202 QUESTION 20 A three-month-old boy presents with tachypnoea and failure to thrive. On examination he is noted to have a respiratory rate of 60/minute with intercostal and subcostal recession. The liver is palpable 4 cm below the right costal margin. The chest is clear and no murmurs are audible. The oxygen saturation is 89% in room air but increases to 95% with 1 L of subnasal oxygen. His chest X-ray is shown below.
Which one of the following is the most likely diagnosis? A. Bronchiolitis. B. d-transposition of the great arteries and ventricular septal defect. C. Primary pulmonary lymphangiectasia. D. Total anomalous pulmonary venous return. E. Truncus arteriosus. QUESTION 21 There is strongest evidence for an association between measles-mumps-rubella (MMR) vaccine and which one of the following adverse events? A. Autism. B. Crohn disease. C. Encephalitis. D. Guillain-Barré syndrome. E. Multiple sclerosis.
Copyright © 2004 by The Royal Australasian College of Physicians
13 P202 QUESTION 22 A 24-hour-old infant is found in the postnatal ward with poor perfusion and significant respiratory distress. Which one of the following would be the best indication to start a prostaglandin infusion? A. Active praecordium. B. Diminished pulses. C. Heart murmur. D. Hepatomegaly. E. Tachycardia. QUESTION 23 A three-year-old boy presents with a one-week history of bruising and severe, persistent epistaxis for 24 hours. Two weeks ago he had a mild illness consisting of a sore throat and low grade fever for which he took aspirin on one occasion. Clinical examination was unremarkable except for pallor, cutaneous bruising and fresh blood in the nasal antra. Full blood count shows: haemoglobin 80 g/L [110-145] white cell count 6 x 109/L [5-17] platelet count 8 x 109/L [150-400] Which one of the following is the most appropriate next step in management? A. Intravenous gamma globulin. B. Intravenous vincristine. C. Oral prednisolone. D. Platelet transfusion. E. No treatment. QUESTION 24 A 40-year-old pregnant woman and her partner choose to have an amniocentesis. The karyotype of the foetus is 47,XXY. Which one of the following is the most likely to occur in this condition? A. Gynaecomastia. B. Homosexuality. C. Infertility. D. Intellectual disability. E. Tall stature (>97th percentile).
Copyright © 2004 by The Royal Australasian College of Physicians
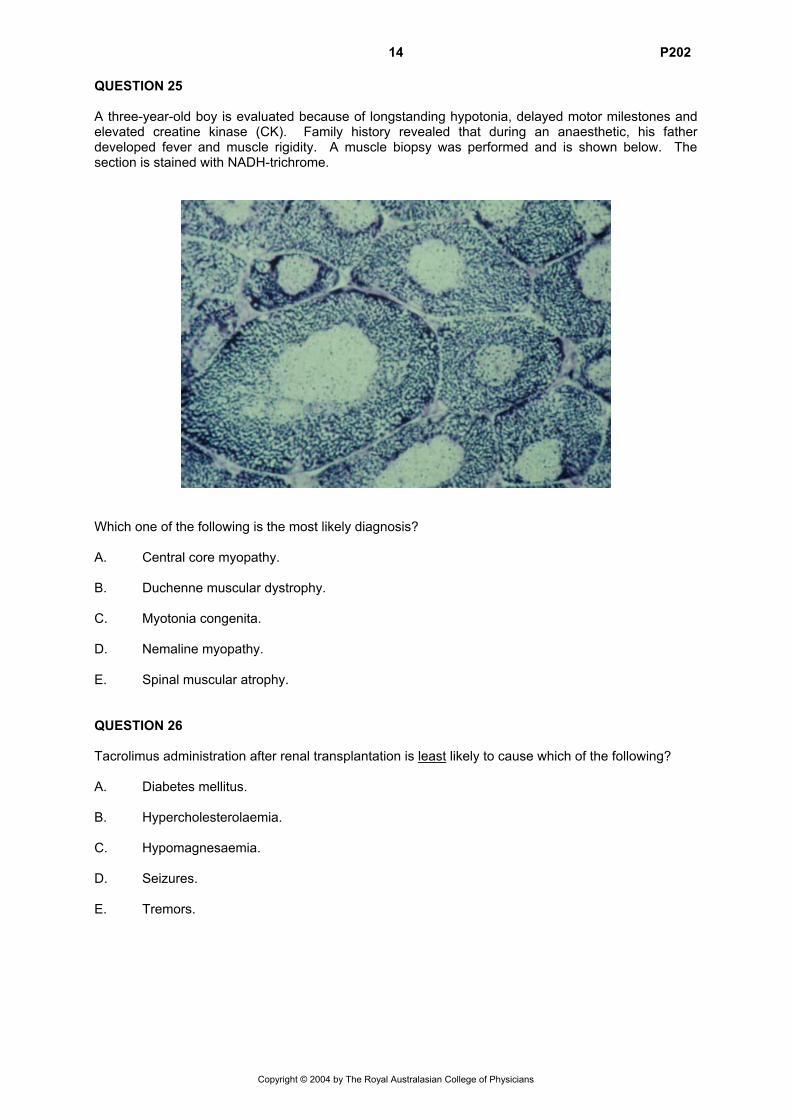
14 P202 QUESTION 25 A three-year-old boy is evaluated because of longstanding hypotonia, delayed motor milestones and elevated creatine kinase (CK). Family history revealed that during an anaesthetic, his father developed fever and muscle rigidity. A muscle biopsy was performed and is shown below. The section is stained with NADH-trichrome.
Which one of the following is the most likely diagnosis? A. Central core myopathy. B. Duchenne muscular dystrophy. C. Myotonia congenita. D. Nemaline myopathy. E. Spinal muscular atrophy. QUESTION 26 Tacrolimus administration after renal transplantation is least likely to cause which of the following? A. Diabetes mellitus. B. Hypercholesterolaemia. C. Hypomagnesaemia. D. Seizures. E. Tremors.
Copyright © 2004 by The Royal Australasian College of Physicians
15 P202 QUESTION 27 A seven-year-old girl is referred to the outpatients department for the evaluation of wheezing episodes which have occurred every month during the previous three months. She was born at 24 weeks gestation, ventilated for one month and was on supplemental oxygen for a further 12 weeks. Her clinical examination is normal. Her baseline lung function tests showed the following: forced vital capacity (FVC) 80% predicted forced expiratory volume in one second (FEV1) 70% predicted maximum mid-expiratory flow (MMEF) 30% predicted She was treated with prednisolone for two weeks (1 mg/kg/day). Repeat lung function tests post Ventolin were: FVC 83% predicted FEV1 75% predicted MMEF 40% predicted Her histamine challenge demonstrated a fall in FEV1 of 25%. Which one of the following is the most likely diagnosis? A. Asthma. B. Bronchial stenosis. C. Bronchomalacia. D. Bronchopulmonary dysplasia. E. Reflux aspiration. QUESTION 28 The mother of a seven-year-old boy on maintenance chemotherapy for acute lymphoblastic leukaemia telephones the oncology department to say that a child in her son’s class at school developed chickenpox yesterday. Her son has no history of having had chickenpox in the past. Which one of the following actions would you advise for her son? A. Admission for treatment with intravenous aciclovir. B. Immediate administration of varicella zoster immune globulin (ZIG). C. Immediate immunisation with varicella vaccine. D. Measurement of serum varicella antibody status and administration of ZIG if he is
seronegative. E. Observe and treat with intravenous aciclovir if chickenpox develops.
Copyright © 2004 by The Royal Australasian College of Physicians
16 P202 QUESTION 29 Infection with which one of the following organisms is best described as having its peak incidence in the first two years of life, with a secondary peak between age 15 and 24 years? A. Bordetella pertussis. B. Haemophilus influenzae type b. C. Influenza virus. D. Neisseria meningitidis. E. Streptococcus pneumoniae. QUESTION 30 An eight-month-old boy presents to the emergency room with a four-hour history of profound lethargy. When he woke that morning he was irritable and had episodes of unexplained crying. On examination he is a lethargic, pale infant. He has a temperature of 37.5°C. He is not clinically dehydrated. His cardiovascular and respiratory examination is normal. He has no focal neurological signs. His abdomen is slightly distended and there is fullness in the right upper quadrant. Bowel sounds are normal. The most likely cause for this infant’s condition is: A. allergic enterocolitis. B. constipation. C. intussusception. D. malrotation. E. Salmonella dysentery. QUESTION 31 A mother brings her one-year-old son to see you. For the past three months he has been waking every night, usually two hours after settling. He falls asleep at the start of the night with a bottle of milk. When he wakes during the night, he cries, stands up in the cot and drools. When his mother is unable to calm him with patting she gives him a bottle of 30 mL of formula. He settles back to sleep after drinking the formula. The mother says he is irritable during the day and this is ‘getting her down’. Physical examination is normal. Which one of the following is the most likely diagnosis? A. Hunger. B. Night terrors. C. Separation anxiety disorder. D. Sleep association disorder. E. Teething.
Copyright © 2004 by The Royal Australasian College of Physicians
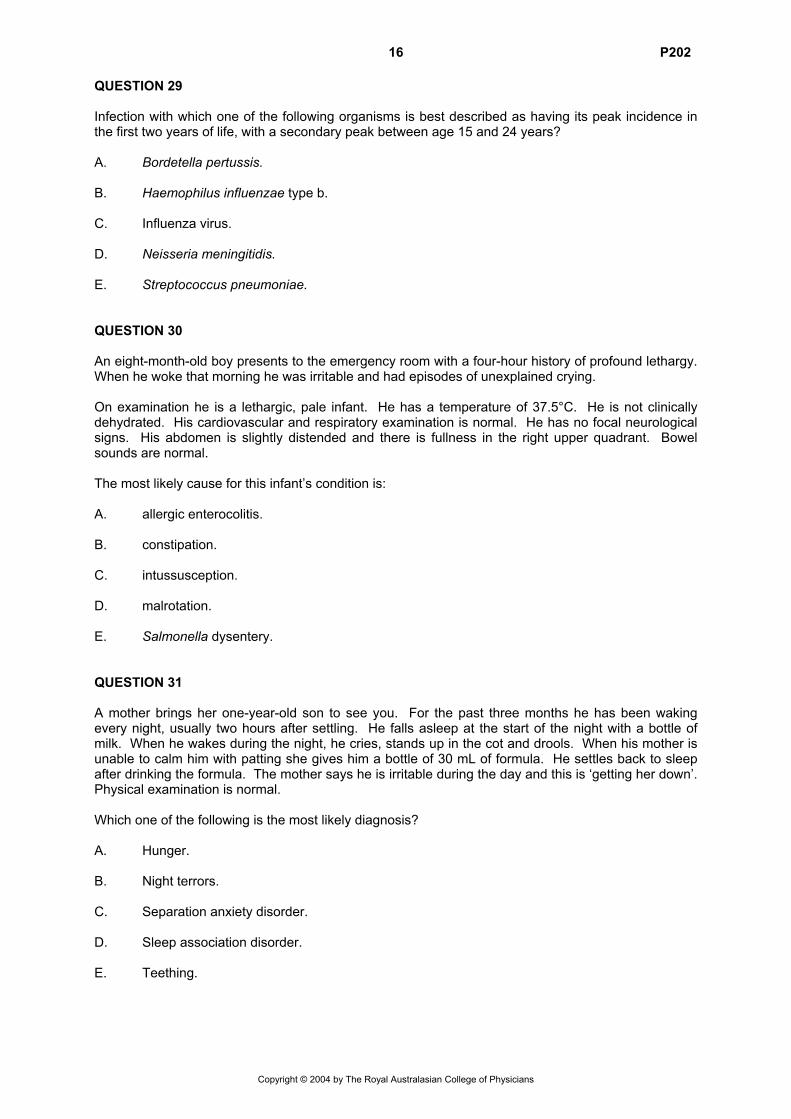
17 P202 QUESTION 32 A male infant was born at term and was well at birth. At four days of age he was discharged from hospital fully breastfed. Mild umbilical redness was noted at the discharge examination. He returned a day later with increasing peri-umbilical redness and was commenced on antibiotics. Over the next 24 hours he developed an erythematous rash starting around the perioral area and spreading rapidly to the face, trunk and flexural areas followed by marked bullous formation and desquamation as shown below. He was very irritable and had a mild fever.
Which one of the following is the most likely diagnosis? A. Bullous impetigo. B. Bullous varicella. C. Epidermolysis bullosa. D. Neonatal pemphigus. E. Staphylococcal scalded skin syndrome. QUESTION 33 A foetus is found to have an isolated echogenic focus in the left ventricle on a routine 18-week ultrasound. Which one of the following is the most likely explanation for this finding? A. A variant of normal. B. Down syndrome. C. Neurofibromatosis. D. Papillary muscle myxoma. E. Tuberous sclerosis (rhabdomyoma).
Copyright © 2004 by The Royal Australasian College of Physicians
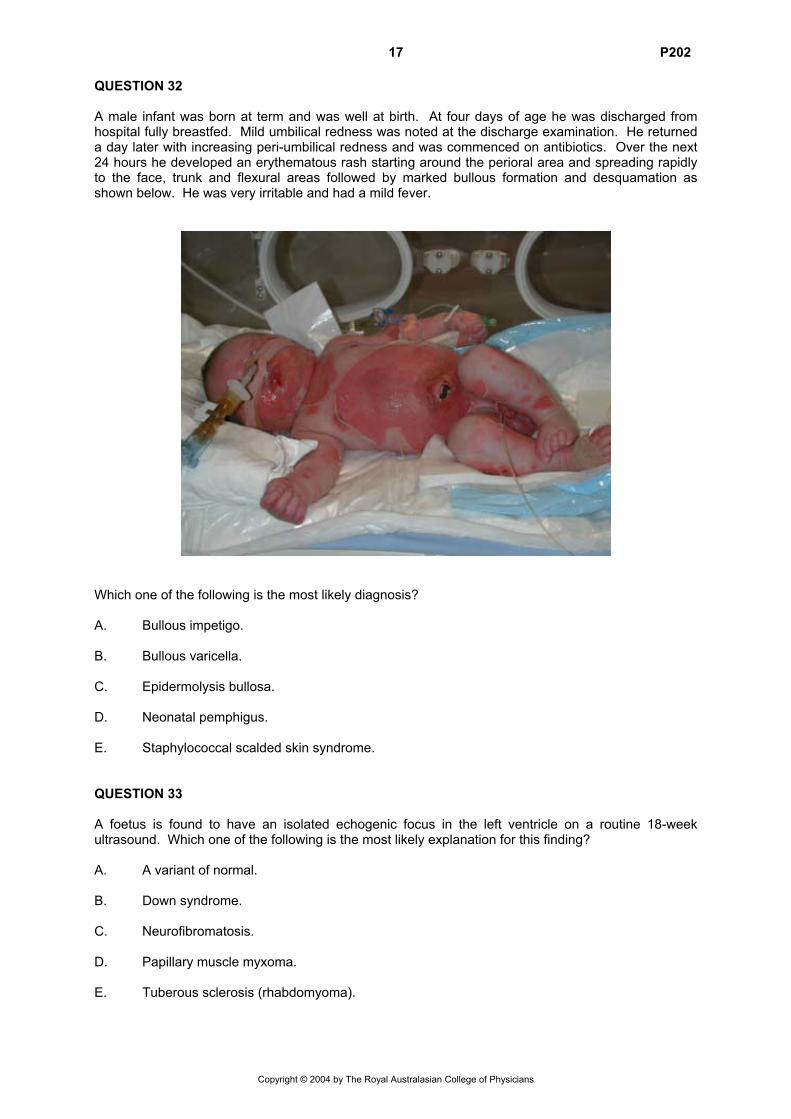
18 P202 QUESTION 34
A 10-month-old Lebanese boy presents to the emergency department with a five-day history of not moving his left upper arm. His X-ray is shown above. Which one of the following is the most likely diagnosis? A. Hypophosphatasia. B. Metaphyseal dysplasia. C. Non-accidental injury. D. Osteomyelitis. E. Rickets. QUESTION 35 A six-year-old boy with chronic granulomatous disease presents with a cough of three weeks duration. A chest X-ray shows right upper lobe consolidation. A computed tomography (CT) scan of the chest shows destruction of the right second rib. Infection with which one of the following is most likely to give this clinical picture? A. Aspergillus. B. Atypical mycobacteria. C. Candida albicans. D. Nocardia. E. Staphylococcus aureus.
Copyright © 2004 by The Royal Australasian College of Physicians
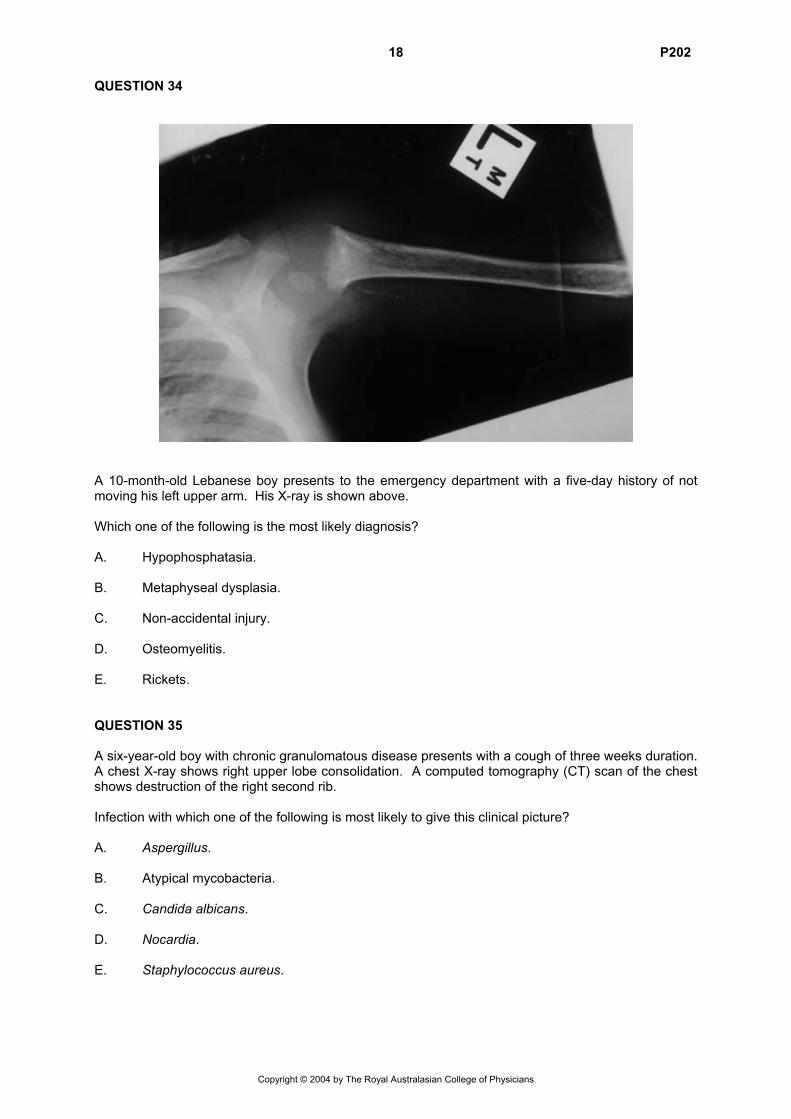
19 P202 QUESTION 36 A four-year-old girl with an unremarkable neonatal history presents with irritability, significant pallor and a palpable spleen. Full blood count shows: haemoglobin 40 g/L [110-150] white cell count 11.3 x 109/L [4.0-12.0] platelet count 383 x 109/L [150-450] A photograph of the peripheral blood film is shown below.
The most likely diagnosis is: A. autoimmune haemolytic anaemia. B. beta thalassaemia major. C. Blackfan-Diamond syndrome. D. megaloblastic anaemia. E. transient erythroblastopenia of childhood. QUESTION 37 The incidence of Grade 3 and 4 acute graft-versus-host disease is greatest when which one of the following sources of stem cells is utilised? A. Bone marrow from matched sibling. B. Bone marrow from matched unrelated donor. C. Cord blood from matched unrelated donor. D. Peripheral blood from related matched adult donor. E. T cell depleted bone marrow from mismatched sibling.
Copyright © 2004 by The Royal Australasian College of Physicians
20 P202 QUESTION 38 A 10-year-old girl has a history of muco-cutaneous candidiasis since age two years and hypoparathyroidism since age four years. She now has increasing tiredness but is clinically and biochemically euthyroid. Which one of the following would be the most useful next test to confirm a diagnosis of adrenal insufficiency? A. Adrenal autoantibodies. B. C26:C22 long chain fatty acid ratio. C. Plasma adrenocorticotrophic hormone. D. Plasma cortisol. E. Plasma renin activity. QUESTION 39 A seven-year-old boy with a history of frequent episodic asthma presents to his paediatrician with a six-month history of recurrent headaches with frequent school absences. The headaches are described as being frontal, “banging”, and associated with pallor. Sleep typically relieves the headaches. His neurologic examination is normal. A diagnosis of migraine is made and recommendations are made with regard to the use of abortive treatment and looking for specific triggers. On review, two months later his headaches continue unabated and a decision is made to recommend prophylactic therapy. Which one of the following prophylactic agents is least appropriate? A. Amitriptyline. B. Cyproheptadine. C. Pizotifen. D. Propranolol. E. Sodium valproate. QUESTION 40 An asymptomatic infant undergoing a routine discharge check on day two is noted to have a continuous murmur. His arterial oxygen saturation is 88% in room air. Which one of the following is the most likely diagnosis? A. Coronary artery fistula. B. Persistent ductus arteriosus. C. Pulmonary atresia and ventricular septal defect. D. Ruptured sinus of Valsalva. E. Transposition of the great arteries.
Copyright © 2004 by The Royal Australasian College of Physicians
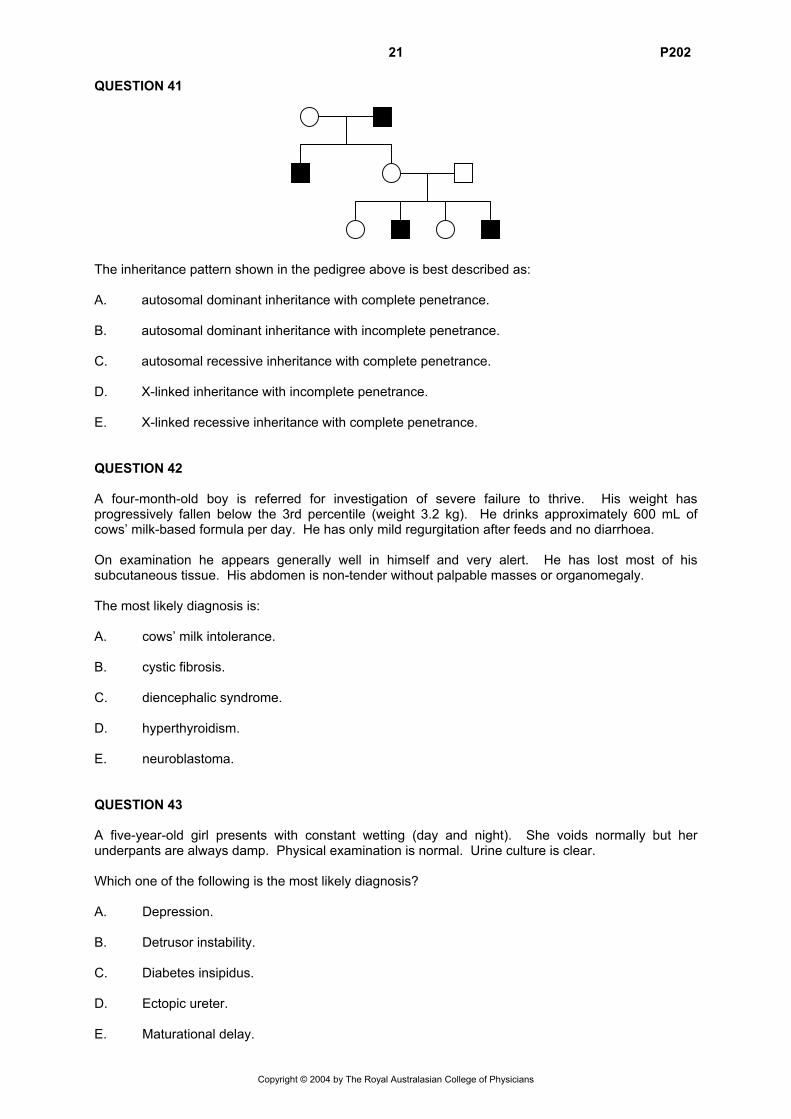
21 P202 QUESTION 41 The inheritance pattern shown in the pedigree above is best described as: A. autosomal dominant inheritance with complete penetrance. B. autosomal dominant inheritance with incomplete penetrance. C. autosomal recessive inheritance with complete penetrance. D. X-linked inheritance with incomplete penetrance. E. X-linked recessive inheritance with complete penetrance. QUESTION 42 A four-month-old boy is referred for investigation of severe failure to thrive. His weight has progressively fallen below the 3rd percentile (weight 3.2 kg). He drinks approximately 600 mL of cows’ milk-based formula per day. He has only mild regurgitation after feeds and no diarrhoea. On examination he appears generally well in himself and very alert. He has lost most of his subcutaneous tissue. His abdomen is non-tender without palpable masses or organomegaly. The most likely diagnosis is: A. cows’ milk intolerance. B. cystic fibrosis. C. diencephalic syndrome. D. hyperthyroidism. E. neuroblastoma. QUESTION 43 A five-year-old girl presents with constant wetting (day and night). She voids normally but her underpants are always damp. Physical examination is normal. Urine culture is clear. Which one of the following is the most likely diagnosis? A. Depression. B. Detrusor instability. C. Diabetes insipidus. D. Ectopic ureter. E. Maturational delay.
Copyright © 2004 by The Royal Australasian College of Physicians
22 P202 QUESTION 44 A 10-year-old obese boy presents with high fevers, shortness of breath, and he appears quite unwell. A chest X-ray reveals bilateral pleural effusions and a large heart. Ultrasound confirms a pericardial effusion. There is no pulsus paradoxus. He is started on intravenous cefotaxime. He becomes more short of breath and remains oxygen dependent after 24 hours, with his chest X-ray showing increased pleural effusions. There are no changes in blood pressure. The priority in his management is to: A. add intravenous flucloxacillin. B. insert large pleural chest drains. C. observe in intensive care unit. D. perform a thoracotomy to create a pericardial window. E. perform pleural and pericardial paracentesis. QUESTION 45 The parents of a 15-year-old boy telephone about his changing behaviour over the previous two weeks. His teachers have described poor concentration and disruptive behaviour at school and he has been truant for most of the past week. He has been very difficult to live with, arguing with his older brother, watching television all night and going out during the day. The parents of his girlfriend are also concerned as they believe the boy and their daughter have started having unprotected sex and he has encouraged her to leave school. The boy refuses to see you. Which one of the following diagnoses best explains these symptoms? A. Attention deficit/hyperactivity disorder. B. Bipolar affective disorder. C. Conduct disorder. D. Marijuana abuse. E. Schizophreniform disorder. QUESTION 46 Which one of the following is the least reliable predictor of neurodevelopmental outcome in term infants with hypoxic-ischaemic encephalopathy? A. Age at onset of seizures of less than 12 hours. B. An abnormal electroencephalogram (EEG) at seven days of age. C. Anuria or oliguria for more than 24 hours. D. Apgar score at 10 minutes. E. Neurological examination at 10 days of age.
Copyright © 2004 by The Royal Australasian College of Physicians
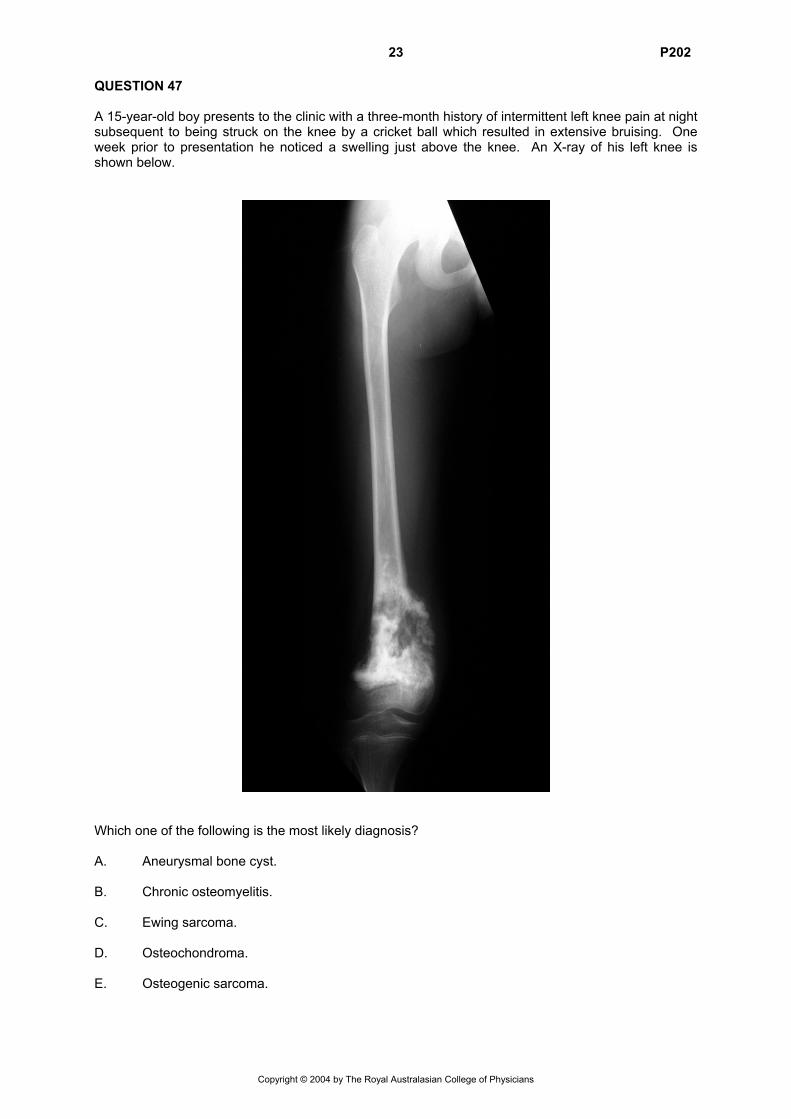
23 P202 QUESTION 47 A 15-year-old boy presents to the clinic with a three-month history of intermittent left knee pain at night subsequent to being struck on the knee by a cricket ball which resulted in extensive bruising. One week prior to presentation he noticed a swelling just above the knee. An X-ray of his left knee is shown below.
Which one of the following is the most likely diagnosis? A. Aneurysmal bone cyst. B. Chronic osteomyelitis. C. Ewing sarcoma. D. Osteochondroma. E. Osteogenic sarcoma.
Copyright © 2004 by The Royal Australasian College of Physicians
24 P202 QUESTION 48 A 13-month-old boy presented with a three-week history of daily fevers and persistent mouth ulcers, and two days of vomiting and diarrhoea. On examination he was miserable, febrile to 38.9ºC and drooling. The gingiva were red and friable with multiple shallow grey-coloured ulcers which did not involve the lips, palate or pharynx. He had multiple small cervical lymph nodes. Initial investigations revealed: haemoglobin 89 g/L [95-140] white cell count 11.3 x 109/L [5.0-17.0] neutrophils 0.2 x 109/L [1.0-8.0] lymphocytes 9 x 109/L [2-13] platelet count 614 x 109/L [150-500] erythrocyte sedimentation rate (ESR) 7 mm/hr [2-20] urine culture negative blood culture negative The ulcers were swabbed for viral culture, but no virus was isolated. The fever, vomiting and diarrhoea settled within three days, the mouth ulcers had healed after six days and the neutrophil count returned to normal after 10 days. A diagnosis of probable herpes simplex virus infection associated with viral-induced neutropenia was made. He re-presents two weeks later with a fever and erythema and swelling of the right eye, secondary to preseptal cellulitis. Serum immunoglobulin levels are: IgG <0.33 g/L [3.55-12.10] IgA <0.07 g/L [0.15-1.24] IgM 0.92 g/L [0.38-1.66] Antibodies to tetanus, diphtheria and Haemophilus influenzae type b are not detected despite his immunisations being up-to-date. T and B cell numbers are normal and T cell proliferation in response to concanavalin A is normal. This pattern of immunodeficiency fits best with: A. chronic granulomatous disease. B. hyper-IgM syndrome. C. severe-combined immunodeficiency. D. transient hypogammaglobulinaemia. E. X-linked hypogammaglobulinaemia.
Copyright © 2004 by The Royal Australasian College of Physicians
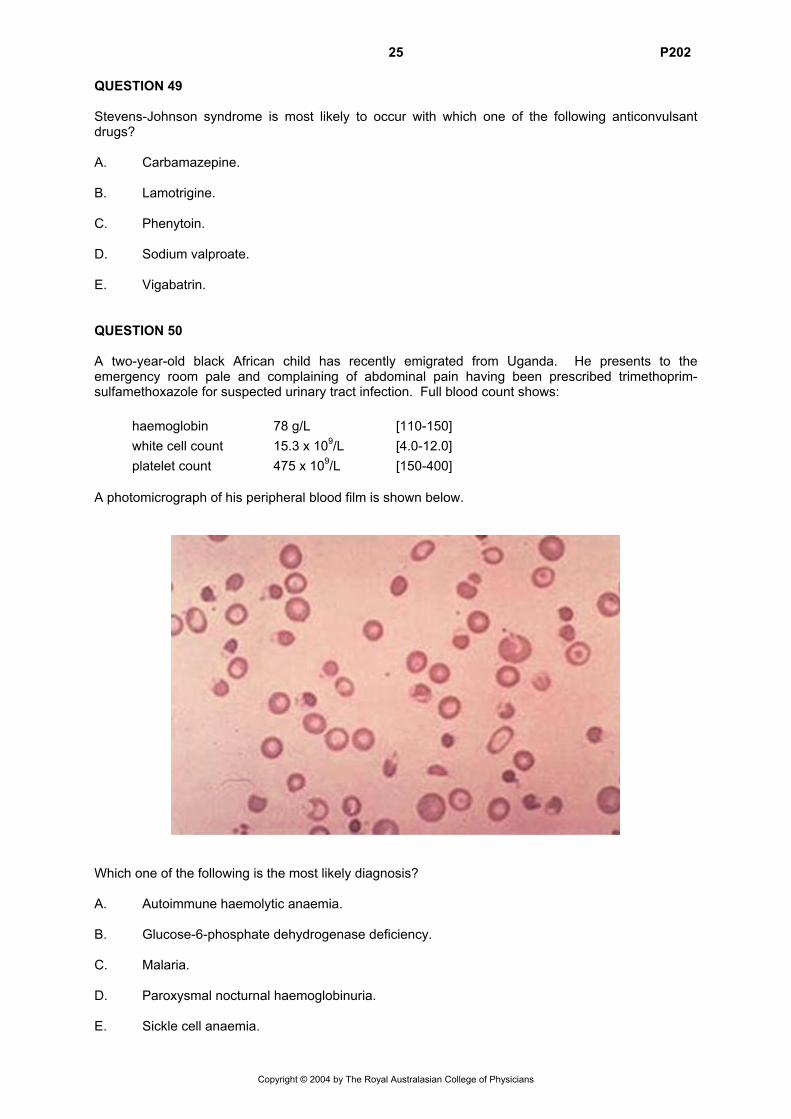
25 P202 QUESTION 49 Stevens-Johnson syndrome is most likely to occur with which one of the following anticonvulsant drugs? A. Carbamazepine. B. Lamotrigine. C. Phenytoin. D. Sodium valproate. E. Vigabatrin. QUESTION 50 A two-year-old black African child has recently emigrated from Uganda. He presents to the emergency room pale and complaining of abdominal pain having been prescribed trimethoprim-sulfamethoxazole for suspected urinary tract infection. Full blood count shows: haemoglobin 78 g/L [110-150] white cell count 15.3 x 109/L [4.0-12.0] platelet count 475 x 109/L [150-400] A photomicrograph of his peripheral blood film is shown below.
Which one of the following is the most likely diagnosis? A. Autoimmune haemolytic anaemia. B. Glucose-6-phosphate dehydrogenase deficiency. C. Malaria. D. Paroxysmal nocturnal haemoglobinuria. E. Sickle cell anaemia.
Copyright © 2004 by The Royal Australasian College of Physicians
26 P202 QUESTION 51 An 18-month-old girl develops fever and diarrhoea. Two days later she begins to vomit, develops a faint, generalised maculopapular rash, increasing tachypnoea and becomes obtunded. She is febrile 39.2°C, pale and poorly perfused. Her capillary refill time is 4 seconds. Her pulse is 140/minute and thready. Blood pressure is 90/60 mmHg. Her apex beat is difficult to feel but is in the mid-axillary line. She has a pansystolic murmur radiating to the axilla. Her respiratory rate is 52/minute and chest clear. Her liver is palpable 5 cm below the costal margin. She is drowsy and has moderate neck stiffness. Her generalised rash is truncal and is fine, maculopapular and blanches on pressure. Investigations show: haemoglobin 108 g/L [110-140] white cell count 11.4 x 109/L [4.0-11.0] neutrophils 5.2 x 109/L [1.0-4.0] platelet count 201 x 109/L [150-400] liver function tests normal cerebrospinal fluid (CSF) white cell count 420 x 106/L (300 polymorphs, 120 monocytes) red cell count 20 x 106/L sugar 2.2 mmol/L (blood sugar 4.2 mmol/L) protein 0.5 mmol/L [0.2-0.6] CSF Gram stain no organisms seen chest X-ray cardiomegaly with pulmonary congestion Which one of the following is the most likely causative organism? A. Coxsackie B virus. B. Enterovirus 71. C. Herpes simplex virus. D. Mycoplasma pneumoniae. E. Neisseria meningitidis. QUESTION 52 Abuse of which one of the following recreational drugs during pregnancy presents the greatest risk of birth defects to the foetus? A. Amphetamines. B. Cocaine. C. Heroin. D. THC (tetrahydrocannibol). E. Tobacco.
Copyright © 2004 by The Royal Australasian College of Physicians
27 P202 QUESTION 53
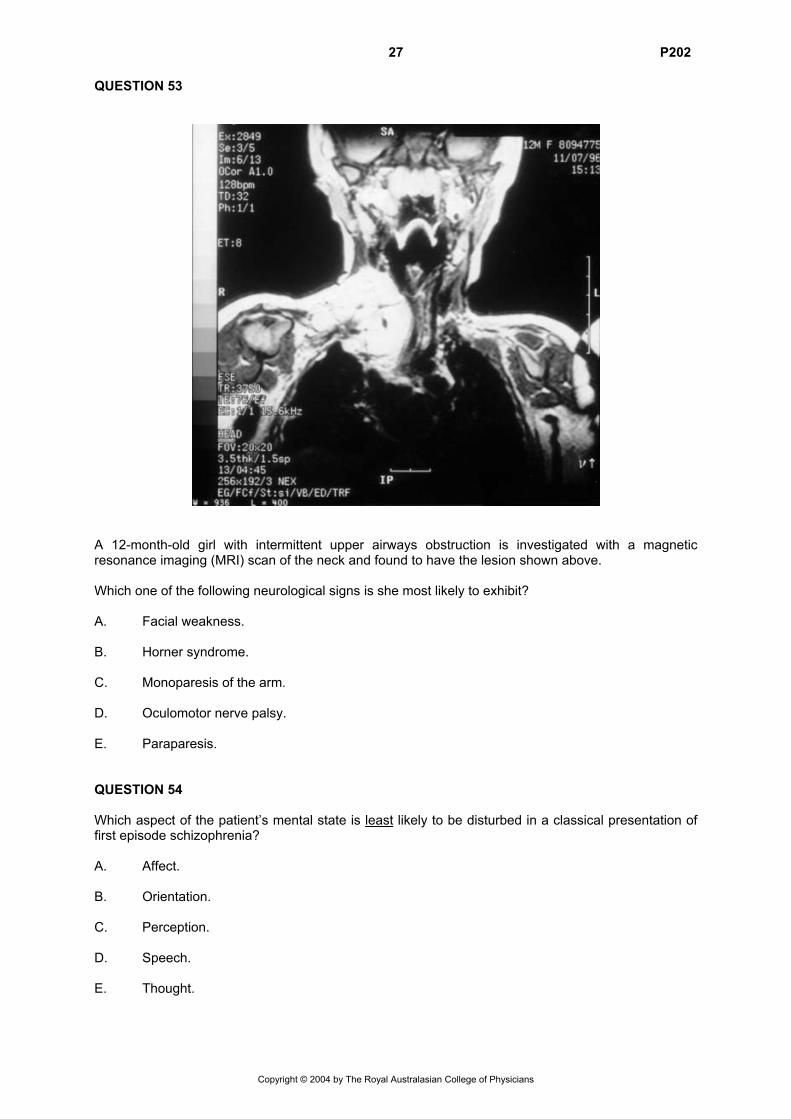
A 12-month-old girl with intermittent upper airways obstruction is investigated with a magnetic resonance imaging (MRI) scan of the neck and found to have the lesion shown above. Which one of the following neurological signs is she most likely to exhibit? A. Facial weakness. B. Horner syndrome. C. Monoparesis of the arm. D. Oculomotor nerve palsy. E. Paraparesis. QUESTION 54 Which aspect of the patient’s mental state is least likely to be disturbed in a classical presentation of first episode schizophrenia? A. Affect. B. Orientation. C. Perception. D. Speech. E. Thought.
Copyright © 2004 by The Royal Australasian College of Physicians
28 P202 QUESTION 55 Following an emergency caesarean section, a term male infant, birth weight 2800 g, required extensive resuscitation with endotracheal intubation, ventilation and cardiac massage. His Apgar scores were recorded as 0 at 1 minute, 3 at 5 minutes and 5 at 10 minutes. At 15 minutes of age he is noted to be bleeding from intravenous puncture sites and his umbilicus, and to develop widespread ecchymoses. Investigation of the cause of his bleeding reveals: prothrombin time (PT) 65 seconds [10-24] activated partial thromboplastin time (APTT) 150 seconds [31-55] fibrin degradation products 15 µg/mL [<10] platelet count 60 x 109/L [150-400] Which one of the following is the most appropriate treatment of the bleeding diathesis? A. Exchange transfusion. B. Intravenous cryoprecipitate. C. Intravenous fresh frozen plasma. D. Intravenous heparin. E. Intravenous platelets. QUESTION 56 A 12-year-old girl presents to the emergency department with swollen eyes and ankles for one week. She has been lethargic and complained of back and right flank pain for approximately 10 days. Examination reveals a well grown adolescent with blood pressure 120/84 mmHg. She has pitting oedema up to her thighs and her liver is palpable 2 cm below the right costal margin and is tender. Urine microscopy shows 400 red cells, red and white cell casts and 4+ protein. Blood tests show: haemoglobin 85 g/L [115-150] white cell count 4.62 x 109/L [4.40-12.50] segmented neutrophils 3.33 x 109/L [1.50-7.40] lymphocytes 1.02 x 109/L [1.50-4.70] platelet count 110 x 109/L [150-400] plasma creatinine 0.10 mmol/L [0.04-0.08] Which one of the following is the most likely diagnosis? A. Focal segmental glomerulosclerosis. B. IgA nephropathy. C. Lupus nephritis. D. Membranoproliferative glomerulonephritis. E. Post-streptococcal glomerulonephritis.
Copyright © 2004 by The Royal Australasian College of Physicians
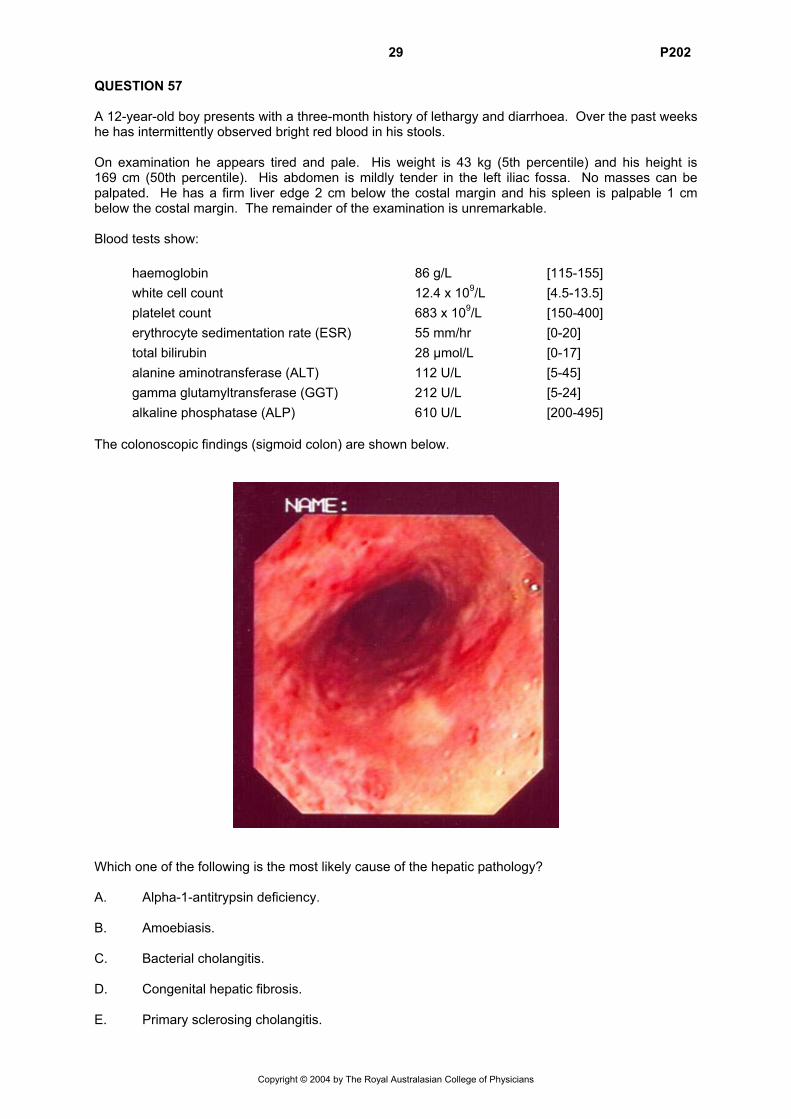
29 P202 QUESTION 57 A 12-year-old boy presents with a three-month history of lethargy and diarrhoea. Over the past weeks he has intermittently observed bright red blood in his stools. On examination he appears tired and pale. His weight is 43 kg (5th percentile) and his height is 169 cm (50th percentile). His abdomen is mildly tender in the left iliac fossa. No masses can be palpated. He has a firm liver edge 2 cm below the costal margin and his spleen is palpable 1 cm below the costal margin. The remainder of the examination is unremarkable. Blood tests show: haemoglobin 86 g/L [115-155] white cell count 12.4 x 109/L [4.5-13.5] platelet count 683 x 109/L [150-400] erythrocyte sedimentation rate (ESR) 55 mm/hr [0-20] total bilirubin 28 µmol/L [0-17] alanine aminotransferase (ALT) 112 U/L [5-45] gamma glutamyltransferase (GGT) 212 U/L [5-24] alkaline phosphatase (ALP) 610 U/L [200-495] The colonoscopic findings (sigmoid colon) are shown below.
Which one of the following is the most likely cause of the hepatic pathology? A. Alpha-1-antitrypsin deficiency. B. Amoebiasis. C. Bacterial cholangitis. D. Congenital hepatic fibrosis. E. Primary sclerosing cholangitis.
Copyright © 2004 by The Royal Australasian College of Physicians
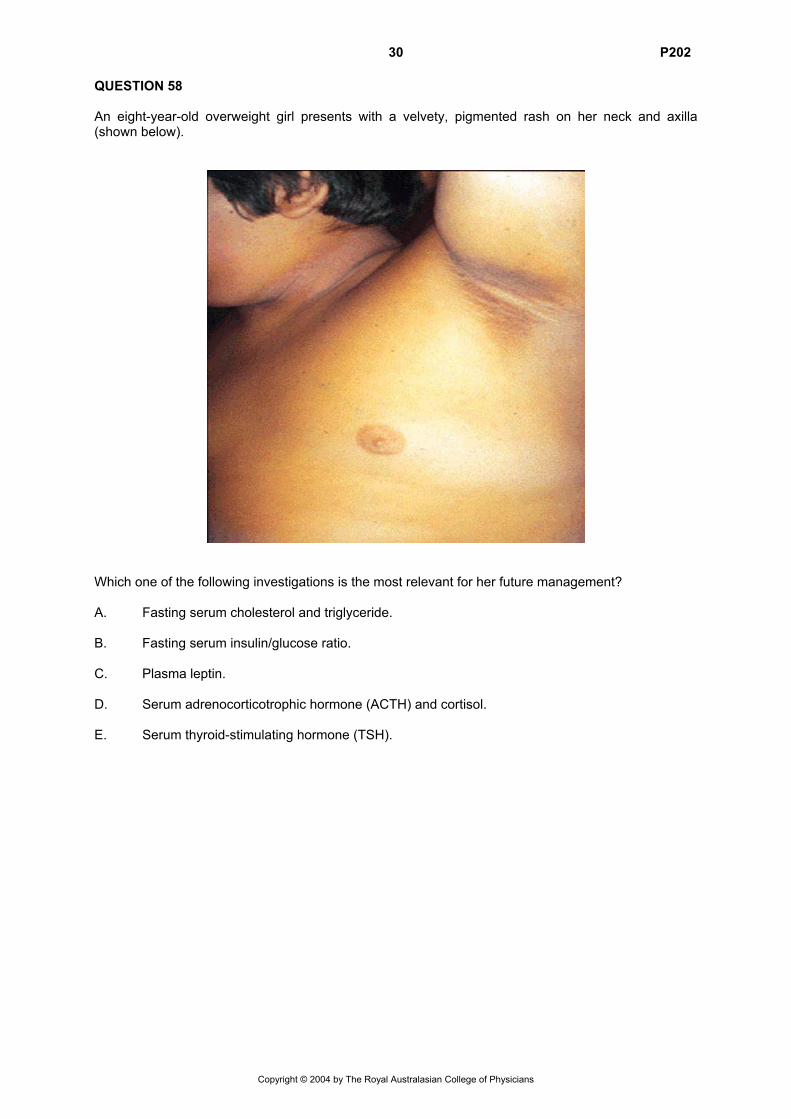
30 P202 QUESTION 58 An eight-year-old overweight girl presents with a velvety, pigmented rash on her neck and axilla (shown below).
Which one of the following investigations is the most relevant for her future management? A. Fasting serum cholesterol and triglyceride. B. Fasting serum insulin/glucose ratio. C. Plasma leptin. D. Serum adrenocorticotrophic hormone (ACTH) and cortisol. E. Serum thyroid-stimulating hormone (TSH).
Copyright © 2004 by The Royal Australasian College of Physicians
31 P202 QUESTION 59 A four-month-old infant known to have tetralogy of Fallot presents to the emergency department with cyanotic episodes associated with crying. Which one of the following is the most useful indicator of whether these episodes are representative of hypercyanotic (tetralogy) spells? A. Baseline arterial saturation. B. Echocardiographic gradient across the right ventricular outflow tract at rest. C. Echocardiographic gradient across the right ventricular outflow tract during a cyanotic episode. D. Intensity of the murmur during a cyanotic episode. E. Oxygen responsiveness during a cyanotic episode. QUESTION 60 A two-month-old girl, born at 30 weeks gestation, is referred by her family doctor as she had been noticed to stop breathing during sleep over the previous three nights. Two days previously she had developed an upper respiratory tract infection. She also has a history of vomiting which is being treated with ranitidine. Oximetry shows oxygen desaturation to the high 80’s. Which one of the following is the most likely diagnosis? A. Aspiration. B. Chlamydial pneumonia. C. Obstructive sleep apnoea. D. Respiratory syncytial virus infection. E. Seizure disorder. QUESTION 61 Which one of the following conditions is not associated with Wilms tumour? A. Aniridia. B. Beckwith-Wiedemann syndrome. C. Cryptorchidism. D. Hemihypertrophy. E. Fanconi anaemia.
Copyright © 2004 by The Royal Australasian College of Physicians
32 P202 QUESTION 62
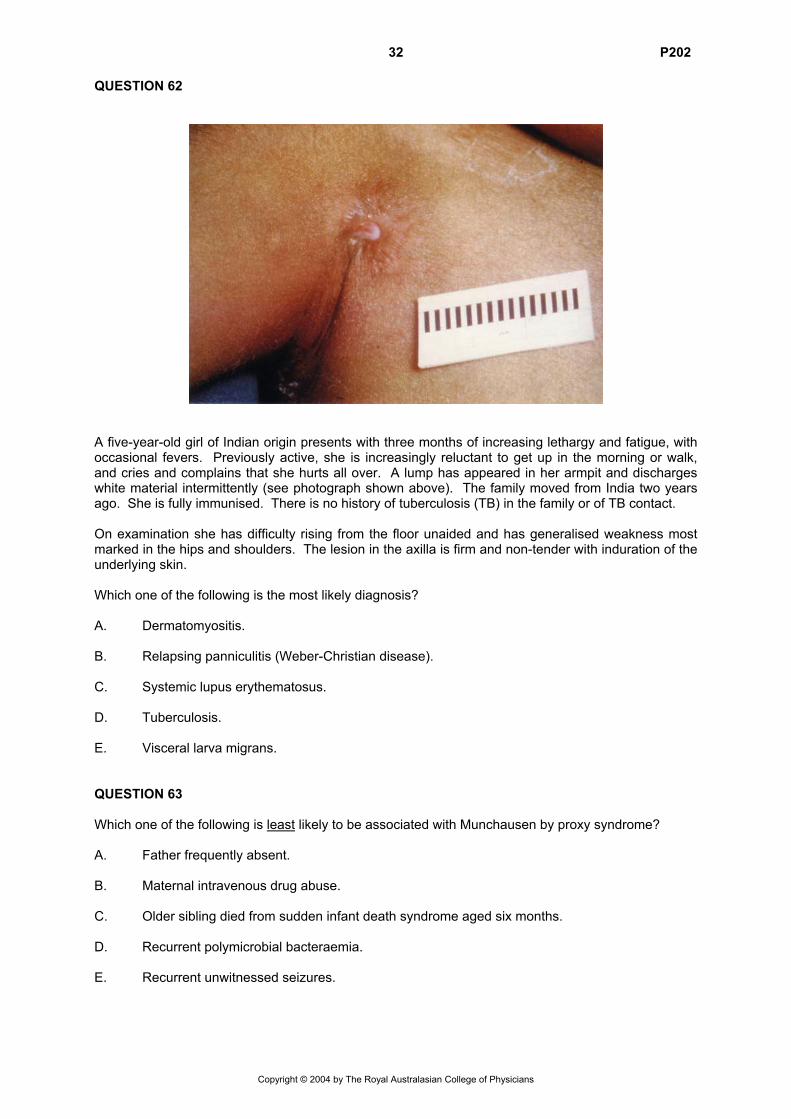
A five-year-old girl of Indian origin presents with three months of increasing lethargy and fatigue, with occasional fevers. Previously active, she is increasingly reluctant to get up in the morning or walk, and cries and complains that she hurts all over. A lump has appeared in her armpit and discharges white material intermittently (see photograph shown above). The family moved from India two years ago. She is fully immunised. There is no history of tuberculosis (TB) in the family or of TB contact. On examination she has difficulty rising from the floor unaided and has generalised weakness most marked in the hips and shoulders. The lesion in the axilla is firm and non-tender with induration of the underlying skin. Which one of the following is the most likely diagnosis? A. Dermatomyositis. B. Relapsing panniculitis (Weber-Christian disease). C. Systemic lupus erythematosus. D. Tuberculosis. E. Visceral larva migrans. QUESTION 63 Which one of the following is least likely to be associated with Munchausen by proxy syndrome? A. Father frequently absent. B. Maternal intravenous drug abuse. C. Older sibling died from sudden infant death syndrome aged six months. D. Recurrent polymicrobial bacteraemia. E. Recurrent unwitnessed seizures.
Copyright © 2004 by The Royal Australasian College of Physicians
33 P202 QUESTION 64 A one-year-old child arrives in the emergency department intubated and ventilated with high flow oxygen, following a motor vehicle accident. Observation reveals a child who is unconscious, cyanosed, pale and with limited chest expansion. Neck veins are slightly distended. Further examination demonstrates poor peripheral perfusion, a weak pulse and tachycardia at 160/minute. The child’s trachea is deviated to the right. Air entry is decreased bilaterally but with air entry on the left reduced compared with the right-hand side. There is hyperresonance over the left chest. The most appropriate next step is: A. chest drain insertion to the left chest. B. needle thoracocentesis of the left chest. C. repositioning of the endotracheal tube. D. suction of the endotracheal tube. E. urgent chest X-ray. QUESTION 65 The emergence of variant Creutzfeldt-Jakob disease (vCJD) in the United Kingdom has resulted in changes to the Australian Red Cross and New Zealand Blood Services’ procedures including a deferral of blood donations from people who have been in the United Kingdom for six months or more between 1980 and 1996. The main reason for this deferral is: A. blood from a sheep incubating bovine spongiform encephalopathy (BSE) was able to cause
the disease when transfused into another sheep. B. blood from experimentally infected primates with vCJD has been shown to transmit the
disease. C. blood from human beings with clinically evident vCJD has been reported to transmit the
disease after intracerebral inoculation into animals. D. there is evidence that a blood donor from the United Kingdom who was incubating vCJD has
transmitted the disease to a recipient. E. tonsils from patients with vCJD contain the prion protein which is thought to be a good index of
infectivity. QUESTION 66 Which one of the following sleep behaviours has the highest prevalence in primary school aged children? A. Bruxism. B. Enuresis. C. Night terrors. D. Sleep talking. E. Sleep walking.
Copyright © 2004 by The Royal Australasian College of Physicians
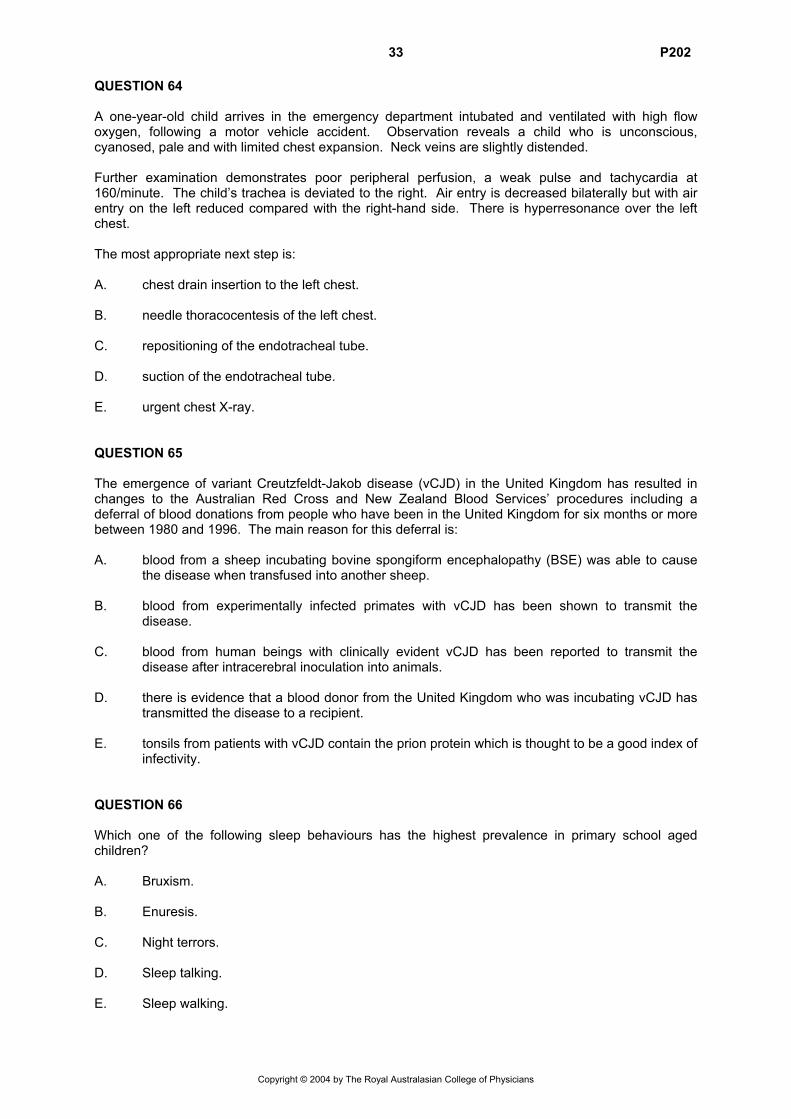
34 P202 QUESTION 67 An eight-week-old boy presents with a fever and a history of being unwell with poor feeding for two days. On enquiry he is noted to have had two similar episodes in the past two months. His urine shows 500 white cells and has a pure growth of >108/L Escherichia coli. His blood culture is negative and his renal function is normal. He is treated successfully with intravenous cefuroxime. A micturating cystourethrogram shows no reflux. Ultrasound of his left kidney is normal but his right kidney ultrasound is shown below.
The next most appropriate investigation is: A. a dimercaptosuccinic acid (DMSA) scan. B. a diuretic diethylene triamine pentaacetic acid (DTPA) scan. C. an antegrade pyelogram. D. an intravenous urogram. E. a retrograde pyelogram.
Copyright © 2004 by The Royal Australasian College of Physicians
35 P202 QUESTION 68
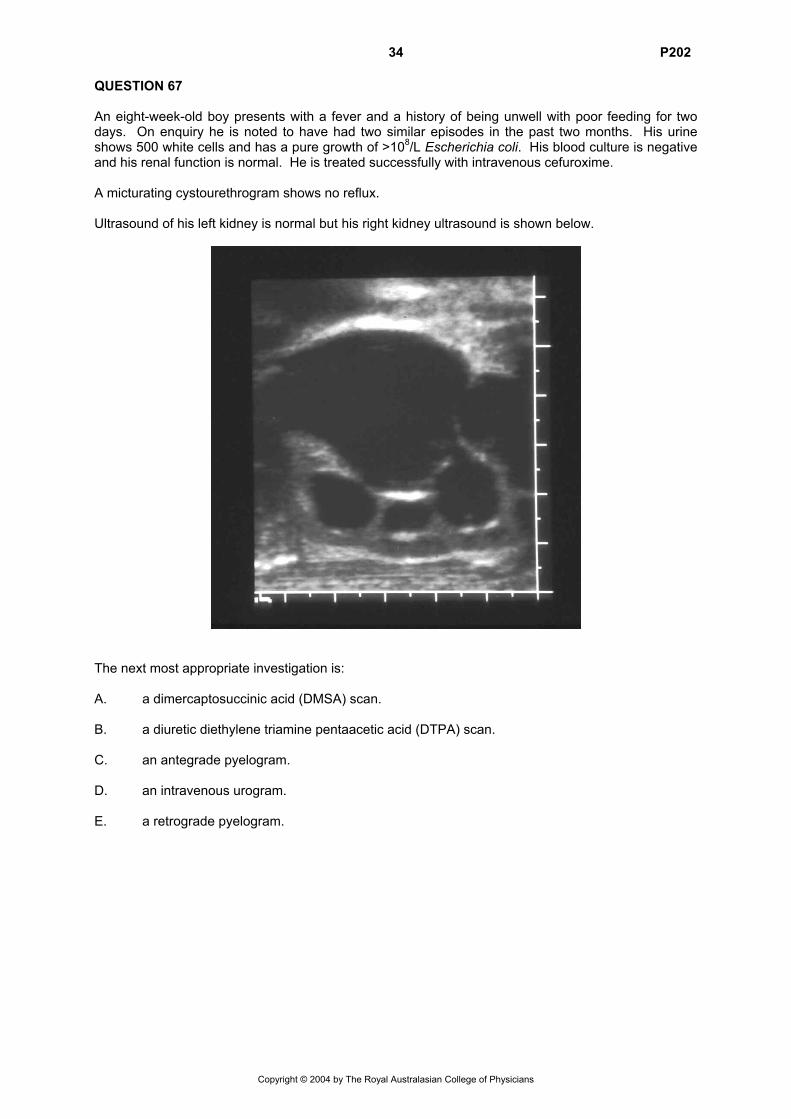
A 14-year-old girl presents with bitemporal hemianopia. Her magnetic resonance imaging (MRI) scan is shown above. She has grown poorly for five years and has a history of polydipsia and polyuria. Her height is <1st percentile, weight on the 3rd percentile and she has no signs of puberty. Investigations reveal: computed tomography (CT) scan of head mass as seen on MRI, no calcification free thyroxine (free T4) 8 pmol/L [10-20] thyroid-stimulating hormone (TSH) 2.50 mU/L [0.03-4.50] urea and electrolytes normal urine specific gravity 1.02 [1.05-1.25] beta human chorionic gonadotrophin detected Which one of the following is the most likely diagnosis? A. Craniopharyngioma. B. Germinoma. C. Glioma. D. Haemangioma. E. Hamartoma.
Copyright © 2004 by The Royal Australasian College of Physicians
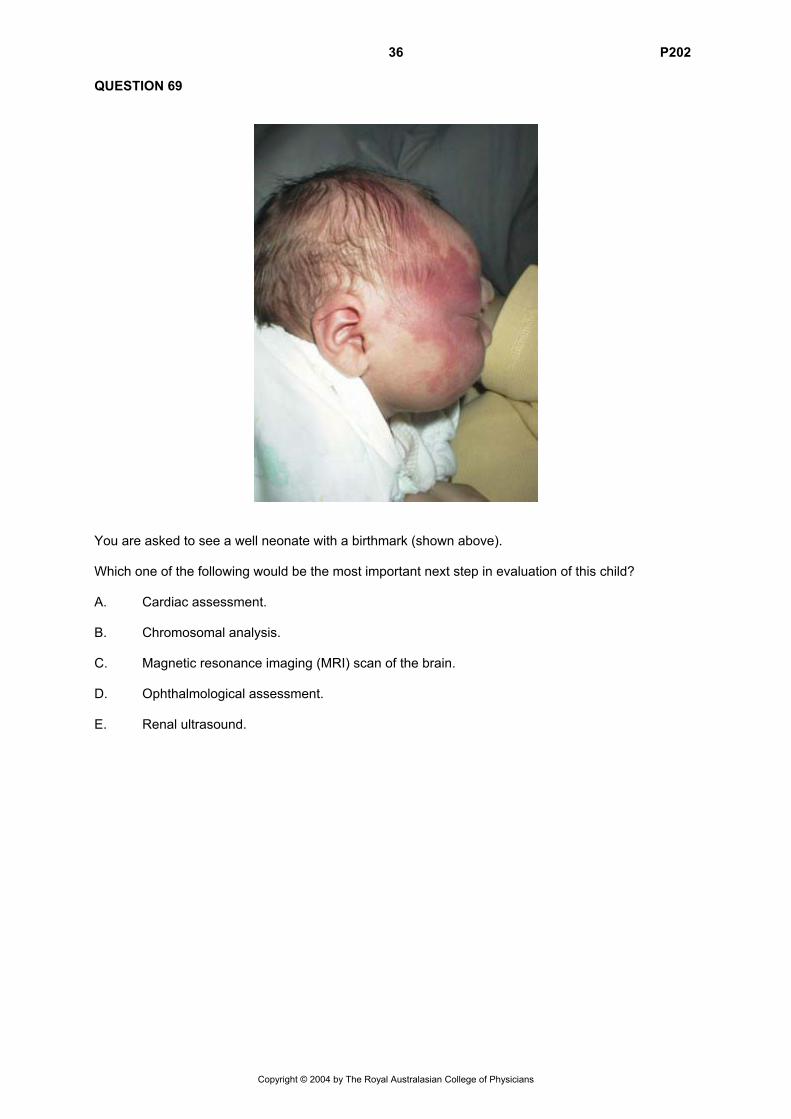
36 P202 QUESTION 69
You are asked to see a well neonate with a birthmark (shown above). Which one of the following would be the most important next step in evaluation of this child? A. Cardiac assessment. B. Chromosomal analysis. C. Magnetic resonance imaging (MRI) scan of the brain. D. Ophthalmological assessment. E. Renal ultrasound.
Copyright © 2004 by The Royal Australasian College of Physicians
37 P202 QUESTION 70 A 12-year-old male bone marrow recipient develops acute upper abdominal pain on day 10 after transplantation from a related donor. Over the following three days he develops increasing abdominal distension and jaundice. He has developed tender hepatomegaly and gained 4 kg in weight. His bowel sounds are sparse. His liver function tests reveal: alanine aminotransferase (ALT) 1850 U/L [5-45] gamma glutamyltransferase (GGT) 683 U/L [5-24] conjugated bilirubin 125.0 µmol/L [0-3.4] unconjugated bilirubin 12 µmol/L [0-17] albumin 30 g/L [40-53] total protein 55 g/L [66-82] His plain abdominal film shows marked ascites. The most likely diagnosis is: A. acute cholecystitis. B. graft-versus-host disease of the liver. C. hepatic veno-occlusive disease. D. primary peritonitis. E. transfusion-related acute hepatitis. QUESTION 71 A 14-year-old girl with cystic fibrosis is reviewed in clinic. It is two months since her last review and in that time she has lost 2 kg in weight, and has had a 10% reduction in forced expiratory volume in one second (FEV1) but has had no recent wet cough. She has had normal stools. On examination her chest is clear. Which one of the following is the most likely diagnosis? A. Diabetes mellitus. B. Gastro-oesophageal reflux. C. Inadequate pancreatic supplementation. D. Inadequate salt intake. E. Recurrent active bronchitis.
Copyright © 2004 by The Royal Australasian College of Physicians
38 P202 QUESTION 72 A four-year-old girl is diagnosed with Duchenne muscular dystrophy (DMD). She is of normal intelligence and is not dysmorphic. Her height is on the 3rd percentile. There is no family history of any similar disorder, but her mother has a high serum creatine kinase (CK) level. Which one of the following is the most likely mechanism for the expression of this X-linked recessive disorder in this girl? A. Father is mildly affected and mother is a carrier of the X-linked mutation. B. Mother is a carrier and a new mutation has occurred on the paternally derived allele. C. She has inherited an apparently balanced X/autosome translocation from her mother. D. She has inherited two copies of the X-linked mutation due to uniparental disomy. E. She has Turner syndrome as well as having inherited an X-linked mutation. QUESTION 73 A term infant was born by breech delivery with forceps assisted delivery of the head. Foetal heart rate decelerations (type 1) were noted towards the end of the second stage. The Apgar scores were 5 at 1 minute and 8 at 5 minutes. Over the next 18 hours the infant was drowsy but able to rouse for feeds and was afebrile. At 18 hours of age the infant develops apnoea and abnormal movements consistent with seizures. Which one of the following is the most likely diagnosis? A. Bacterial meningitis. B. Congenital malformation of the brain. C. Hypoxic-ischaemic encephalopathy. D. Intraventricular haemorrhage. E. Sub-arachnoid haemorrhage. QUESTION 74 A mother presents to you with her first child, aged two months. He has been crying most days for the last three weeks, up to two hours each day. He vomits after every second feed. He has 4-6 loose yellow bowel motions each day. He is currently on S26 formula and is gaining weight. Physical examination is normal. Which one of the following is the most appropriate next step? A. Change feeds to soy-based formula. B. Discuss normal crying patterns. C. Take stool sample for reducing substances. D. Trial of ranitidine. E. Urine culture.
Copyright © 2004 by The Royal Australasian College of Physicians
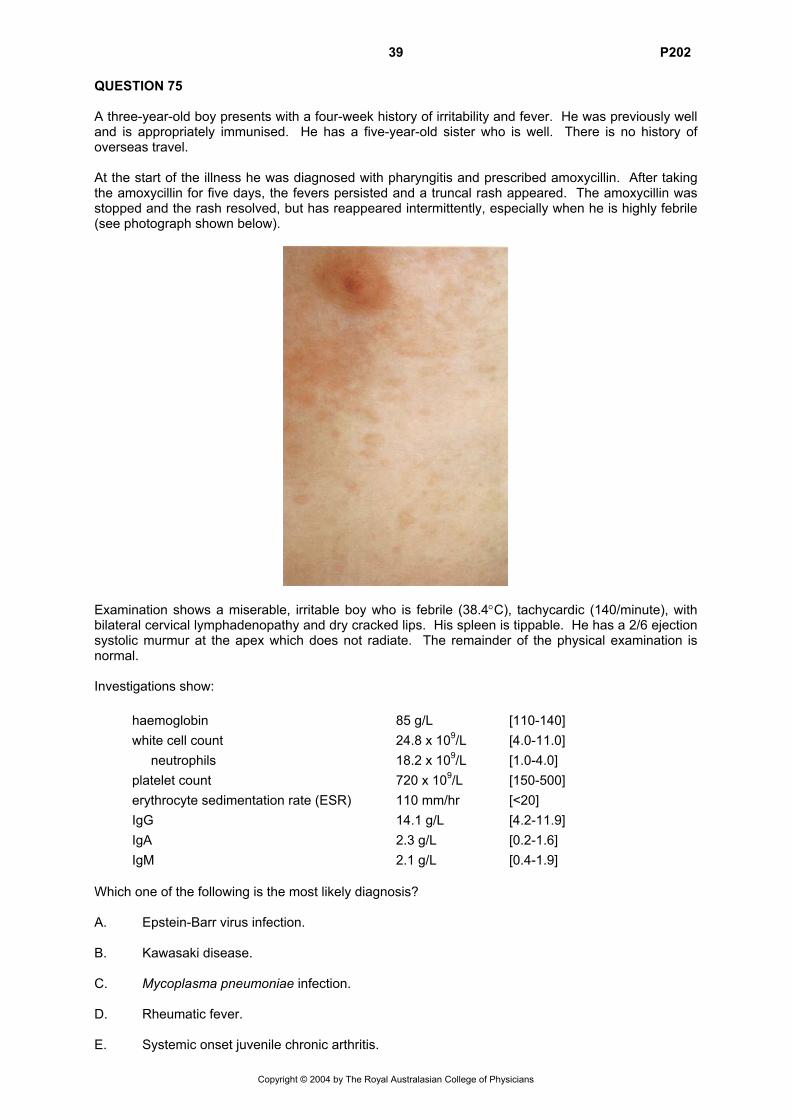
39 P202 QUESTION 75 A three-year-old boy presents with a four-week history of irritability and fever. He was previously well and is appropriately immunised. He has a five-year-old sister who is well. There is no history of overseas travel. At the start of the illness he was diagnosed with pharyngitis and prescribed amoxycillin. After taking the amoxycillin for five days, the fevers persisted and a truncal rash appeared. The amoxycillin was stopped and the rash resolved, but has reappeared intermittently, especially when he is highly febrile (see photograph shown below).
Examination shows a miserable, irritable boy who is febrile (38.4°C), tachycardic (140/minute), with bilateral cervical lymphadenopathy and dry cracked lips. His spleen is tippable. He has a 2/6 ejection systolic murmur at the apex which does not radiate. The remainder of the physical examination is normal. Investigations show: haemoglobin 85 g/L [110-140] white cell count 24.8 x 109/L [4.0-11.0] neutrophils 18.2 x 109/L [1.0-4.0] platelet count 720 x 109/L [150-500] erythrocyte sedimentation rate (ESR) 110 mm/hr [<20] IgG 14.1 g/L [4.2-11.9] IgA 2.3 g/L [0.2-1.6] IgM 2.1 g/L [0.4-1.9] Which one of the following is the most likely diagnosis? A. Epstein-Barr virus infection. B. Kawasaki disease. C. Mycoplasma pneumoniae infection. D. Rheumatic fever. E. Systemic onset juvenile chronic arthritis.
Copyright © 2004 by The Royal Australasian College of Physicians
40 P202 QUESTION 76 Anorexia nervosa has a highly variable outcome. Which one of the following factors is least predictive of a poor prognosis? A. Degree of weight loss at initial presentation. B. Frequent hospitalisations. C. Highly disturbed relationships with family members. D. Prepubertal onset. E. Poor premorbid functioning. QUESTION 77
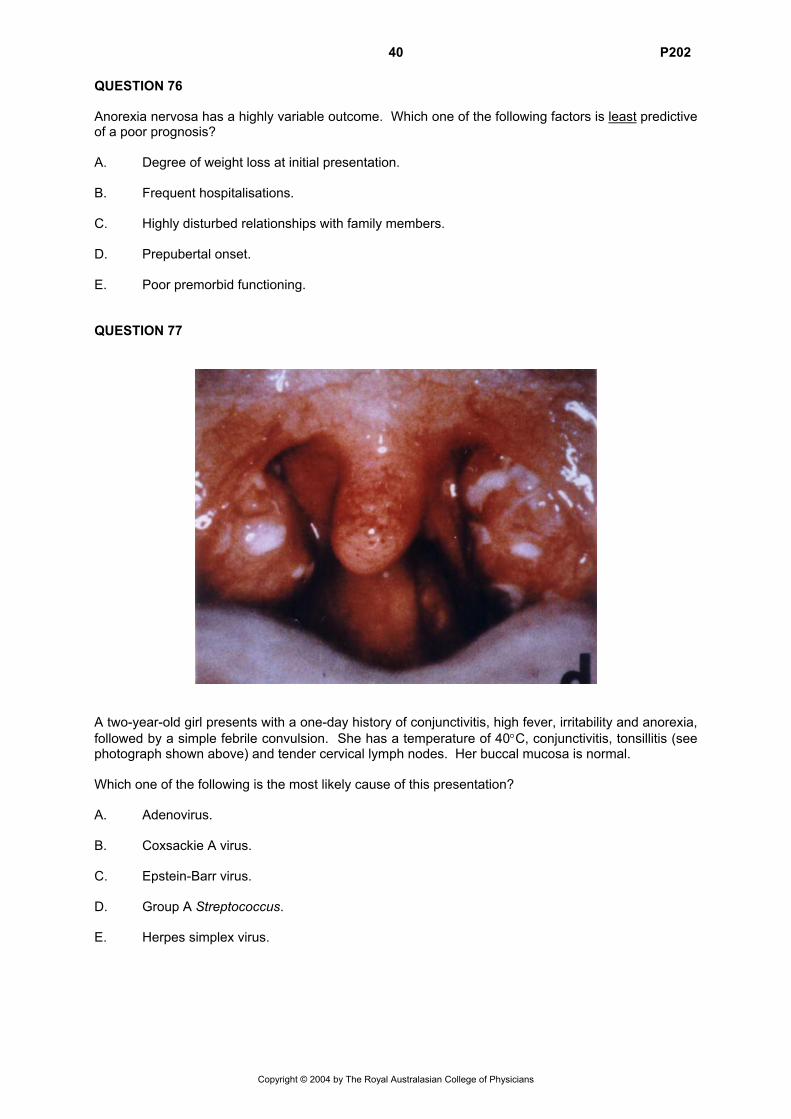
A two-year-old girl presents with a one-day history of conjunctivitis, high fever, irritability and anorexia, followed by a simple febrile convulsion. She has a temperature of 40°C, conjunctivitis, tonsillitis (see photograph shown above) and tender cervical lymph nodes. Her buccal mucosa is normal. Which one of the following is the most likely cause of this presentation? A. Adenovirus. B. Coxsackie A virus. C. Epstein-Barr virus. D. Group A Streptococcus. E. Herpes simplex virus.
Copyright © 2004 by The Royal Australasian College of Physicians
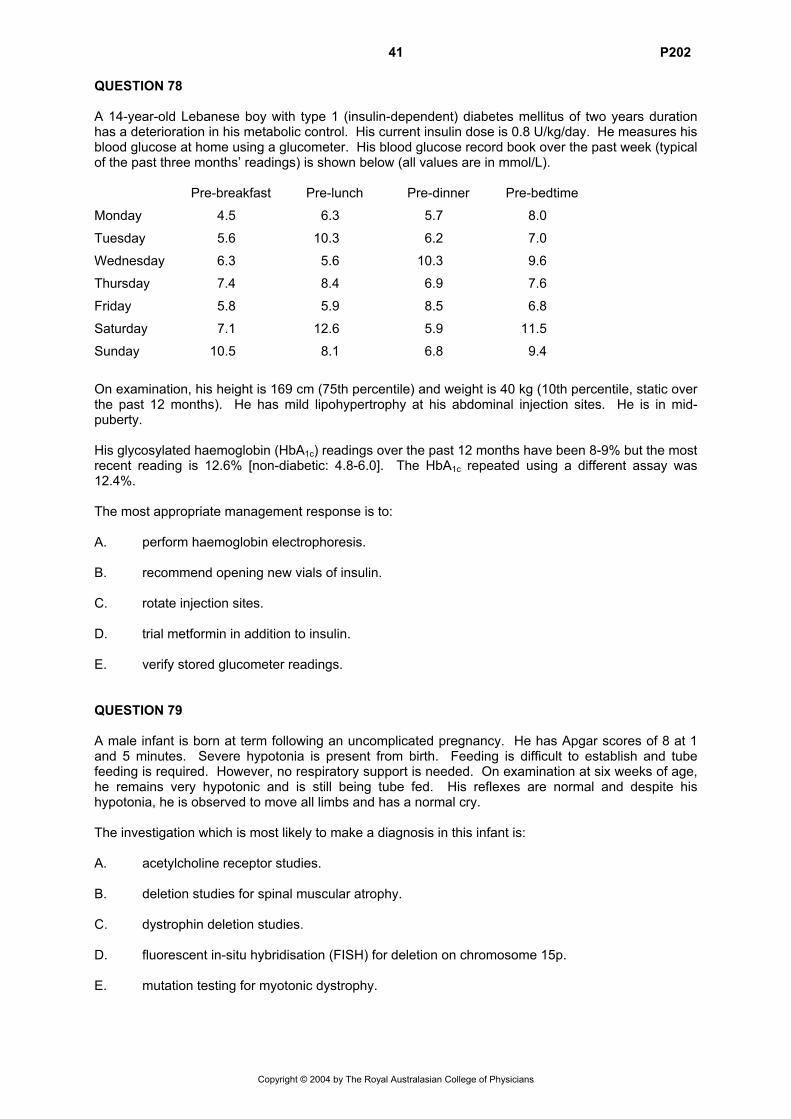
41 P202 QUESTION 78 A 14-year-old Lebanese boy with type 1 (insulin-dependent) diabetes mellitus of two years duration has a deterioration in his metabolic control. His current insulin dose is 0.8 U/kg/day. He measures his blood glucose at home using a glucometer. His blood glucose record book over the past week (typical of the past three months’ readings) is shown below (all values are in mmol/L). Pre-breakfast Pre-lunch Pre-dinner Pre-bedtime
Monday 4.5 6.3 5.7 8.0
Tuesday 5.6 10.3 6.2 7.0
Wednesday 6.3 5.6 10.3 9.6
Thursday 7.4 8.4 6.9 7.6
Friday 5.8 5.9 8.5 6.8
Saturday 7.1 12.6 5.9 11.5
Sunday 10.5 8.1 6.8 9.4
On examination, his height is 169 cm (75th percentile) and weight is 40 kg (10th percentile, static over the past 12 months). He has mild lipohypertrophy at his abdominal injection sites. He is in mid-puberty. His glycosylated haemoglobin (HbA1c) readings over the past 12 months have been 8-9% but the most recent reading is 12.6% [non-diabetic: 4.8-6.0]. The HbA1c repeated using a different assay was 12.4%. The most appropriate management response is to: A. perform haemoglobin electrophoresis. B. recommend opening new vials of insulin. C. rotate injection sites. D. trial metformin in addition to insulin. E. verify stored glucometer readings. QUESTION 79 A male infant is born at term following an uncomplicated pregnancy. He has Apgar scores of 8 at 1 and 5 minutes. Severe hypotonia is present from birth. Feeding is difficult to establish and tube feeding is required. However, no respiratory support is needed. On examination at six weeks of age, he remains very hypotonic and is still being tube fed. His reflexes are normal and despite his hypotonia, he is observed to move all limbs and has a normal cry. The investigation which is most likely to make a diagnosis in this infant is: A. acetylcholine receptor studies. B. deletion studies for spinal muscular atrophy. C. dystrophin deletion studies. D. fluorescent in-situ hybridisation (FISH) for deletion on chromosome 15p. E. mutation testing for myotonic dystrophy.
Copyright © 2004 by The Royal Australasian College of Physicians
42 P202 QUESTION 80 A seven-year-old boy has trodden on a bee and presents to the emergency department with swelling and redness of the foot spreading to mid-calf. He has been stung on one previous occasion with only minor redness and swelling. He has a history of mild intermittent asthma. There are no other symptoms. His mother is concerned about the size of the present reaction, its treatment and about consequences of future bee stings. What is your advice about management of the current reaction and prognosis for future stings? A. There is a moderate risk that this particular reaction will progress because of the background
of asthma and immediate administration of adrenaline is required with provision of adrenaline for future emergency use.
B. This is a large local reaction and requires treatment with oral corticosteroids as would any
future similar reactions. C. This reaction is a large local reaction and requires no immediate treatment but there is a high
risk that any future stings will result in a systemic reaction and adrenaline should be provided for emergency use.
D. This reaction requires treatment with oral antihistamines and any future stings should be
treated by the immediate administration of a fast-acting oral antihistamine. E. This reaction should be treated with intravenous corticosteroids and antihistamines and a
referral made for commencement of venom immunotherapy. QUESTION 81 A five-year-old boy has been rescued from a house fire. He is not cyanosed but has mild inspiratory stridor, a cough, burns to the face and carbon deposits around the mouth and nose. Cervical spine injury is excluded. An intravenous cannula has been inserted and he is being given oxygen by face mask. The most urgent next step in his management is to: A. administer adequate analgesia. B. administer nebulised adrenaline. C. administer nebulised steroids. D. administer volume replacement rapidly. E. prepare for endotracheal intubation.
Copyright © 2004 by The Royal Australasian College of Physicians
43 P202 QUESTION 82
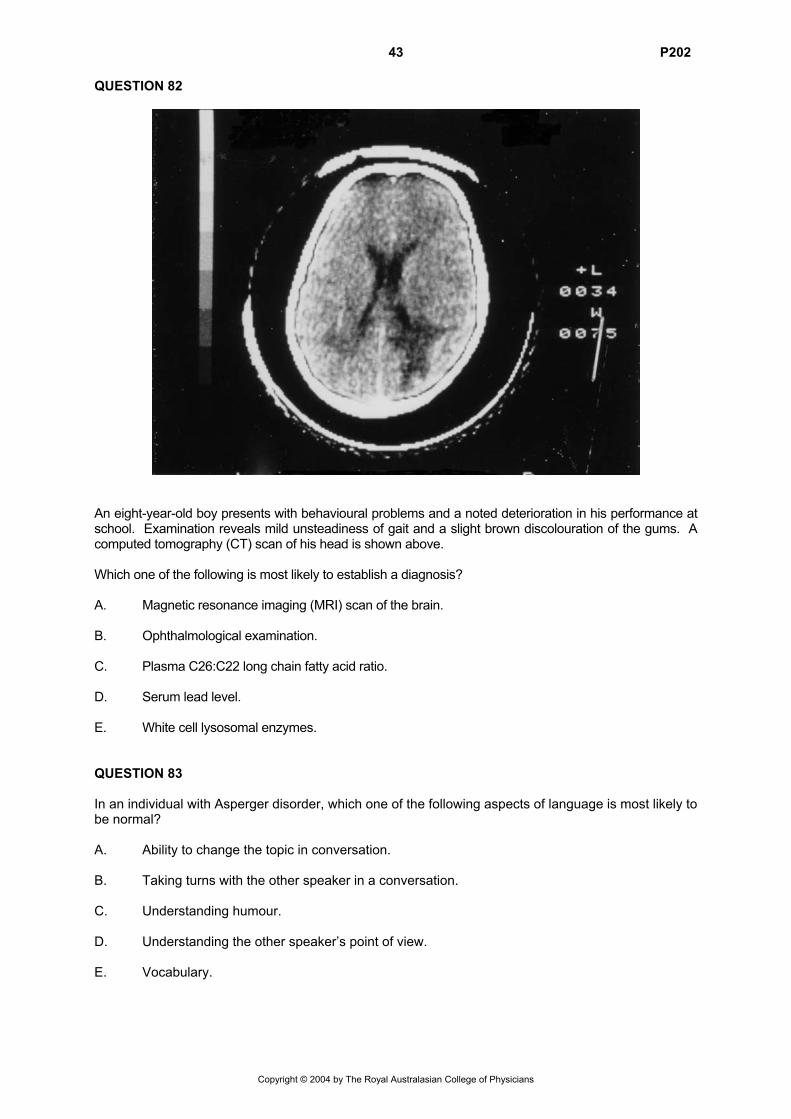
An eight-year-old boy presents with behavioural problems and a noted deterioration in his performance at school. Examination reveals mild unsteadiness of gait and a slight brown discolouration of the gums. A computed tomography (CT) scan of his head is shown above. Which one of the following is most likely to establish a diagnosis? A. Magnetic resonance imaging (MRI) scan of the brain. B. Ophthalmological examination. C. Plasma C26:C22 long chain fatty acid ratio. D. Serum lead level. E. White cell lysosomal enzymes. QUESTION 83 In an individual with Asperger disorder, which one of the following aspects of language is most likely to be normal? A. Ability to change the topic in conversation. B. Taking turns with the other speaker in a conversation. C. Understanding humour. D. Understanding the other speaker’s point of view. E. Vocabulary.
Copyright © 2004 by The Royal Australasian College of Physicians
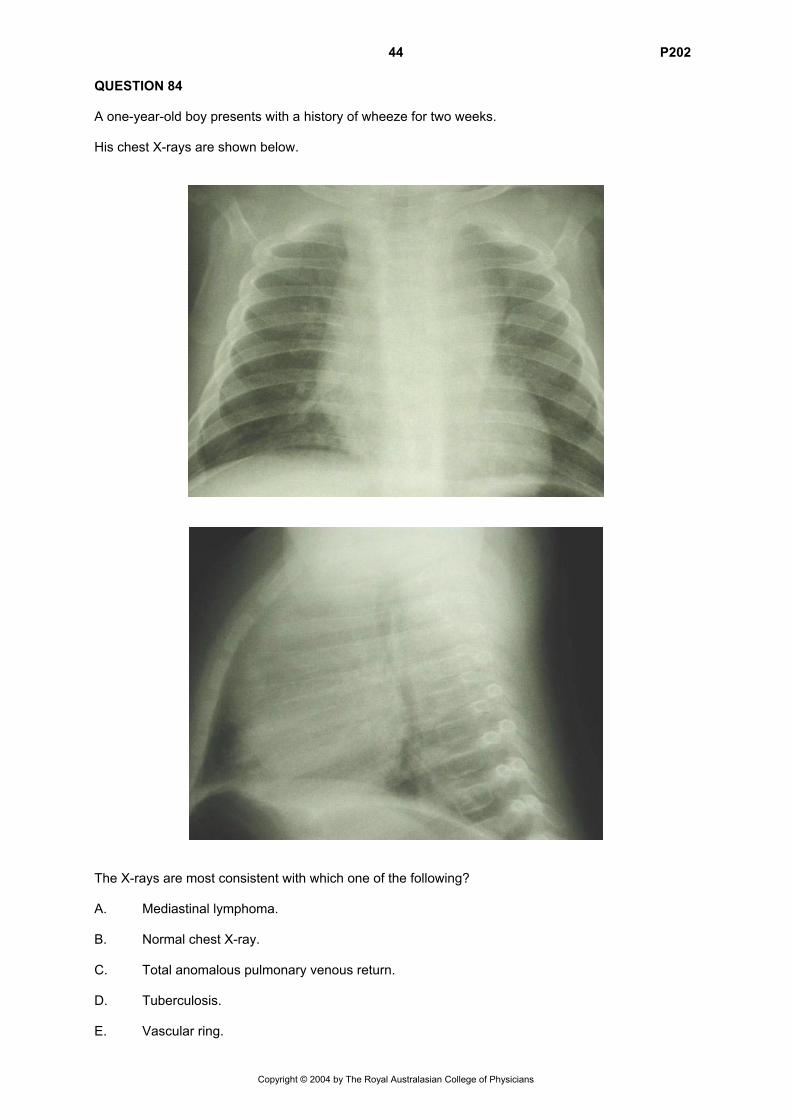
44 P202 QUESTION 84 A one-year-old boy presents with a history of wheeze for two weeks. His chest X-rays are shown below.
The X-rays are most consistent with which one of the following? A. Mediastinal lymphoma. B. Normal chest X-ray. C. Total anomalous pulmonary venous return. D. Tuberculosis. E. Vascular ring.
Copyright © 2004 by The Royal Australasian College of Physicians
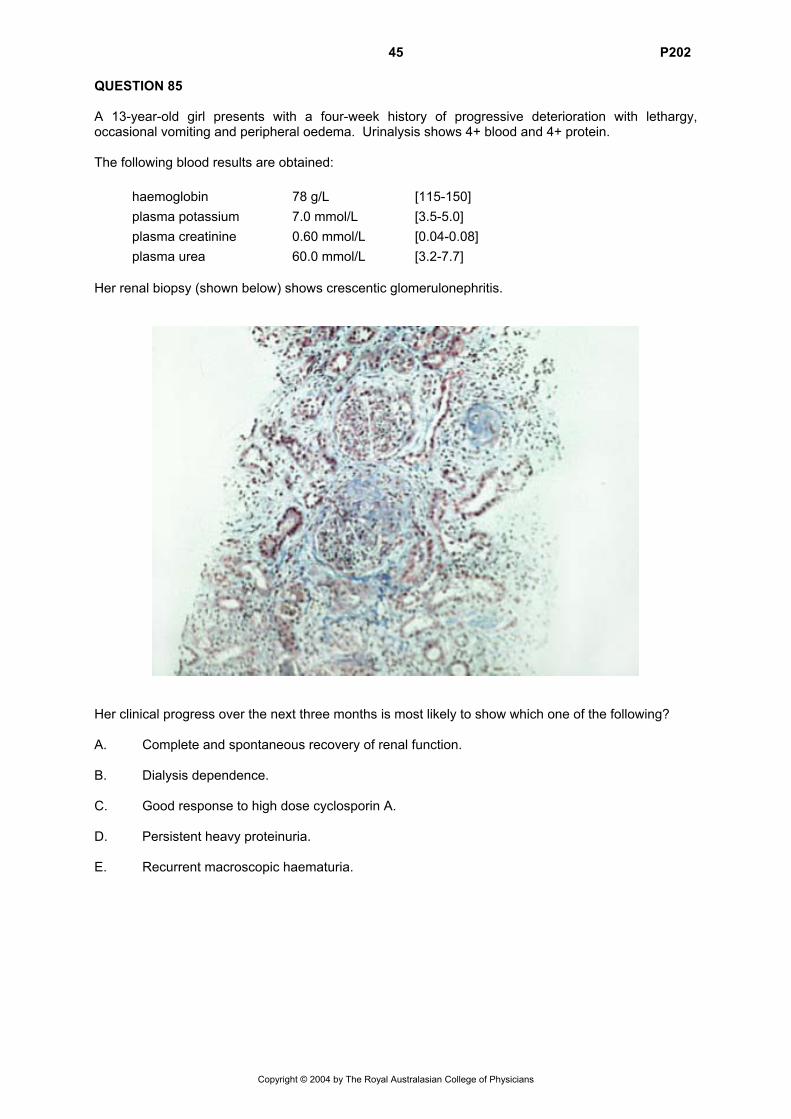
45 P202 QUESTION 85 A 13-year-old girl presents with a four-week history of progressive deterioration with lethargy, occasional vomiting and peripheral oedema. Urinalysis shows 4+ blood and 4+ protein. The following blood results are obtained: haemoglobin 78 g/L [115-150] plasma potassium 7.0 mmol/L [3.5-5.0] plasma creatinine 0.60 mmol/L [0.04-0.08] plasma urea 60.0 mmol/L [3.2-7.7] Her renal biopsy (shown below) shows crescentic glomerulonephritis.
Her clinical progress over the next three months is most likely to show which one of the following? A. Complete and spontaneous recovery of renal function. B. Dialysis dependence. C. Good response to high dose cyclosporin A. D. Persistent heavy proteinuria. E. Recurrent macroscopic haematuria.
Copyright © 2004 by The Royal Australasian College of Physicians
46 P202 QUESTION 86 A six-day-old breastfed female infant is taken to the emergency department by her mother because of bright red rectal bleeding, mild diarrhoea with mucus and persistent crying. On examination the baby is generally well and haemodynamically stable. The perianal region appears normal. Which one of the following is the most likely diagnosis? A. Allergic colitis. B. Colonic duplication. C. Juvenile polyp. D. Meckel diverticulum. E. Swallowed blood. QUESTION 87 Which one of the following is the most common among adolescent (13-17 years) girls in the community? A. Anorexia nervosa. B. Anxiety disorders. C. Attention deficit/hyperactivity disorder. D. Conduct disorder. E. Depressive disorders. QUESTION 88 A 16-year-old boy presents with a history of three episodes of low back pain over six months, each lasting for 10 days. The pain is worse later in the day, eased by rest, and is not associated with morning stiffness in the back. Investigations show: full blood examination within normal limits erythrocyte sedimentation rate (ESR) 19 mm/hr [2-20] HLA-B27 positive X-ray of lumbosacral spine and sacro-iliac joints normal The most likely diagnosis is: A. ankylosing spondylitis. B. discitis. C. non-specific low back pain. D. Scheuermann’s osteochondritis. E. spondylolysis.
Copyright © 2004 by The Royal Australasian College of Physicians
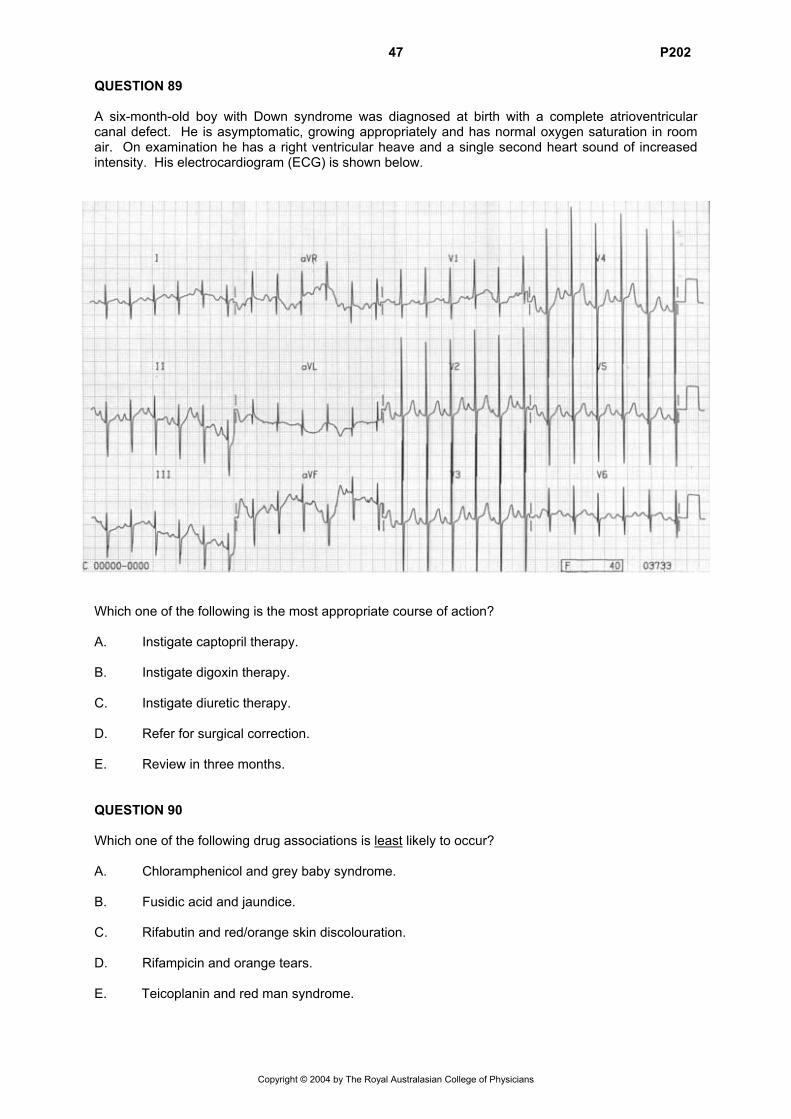
47 P202 QUESTION 89 A six-month-old boy with Down syndrome was diagnosed at birth with a complete atrioventricular canal defect. He is asymptomatic, growing appropriately and has normal oxygen saturation in room air. On examination he has a right ventricular heave and a single second heart sound of increased intensity. His electrocardiogram (ECG) is shown below.
Which one of the following is the most appropriate course of action? A. Instigate captopril therapy. B. Instigate digoxin therapy. C. Instigate diuretic therapy. D. Refer for surgical correction. E. Review in three months. QUESTION 90 Which one of the following drug associations is least likely to occur? A. Chloramphenicol and grey baby syndrome. B. Fusidic acid and jaundice. C. Rifabutin and red/orange skin discolouration. D. Rifampicin and orange tears. E. Teicoplanin and red man syndrome.
Copyright © 2004 by The Royal Australasian College of Physicians
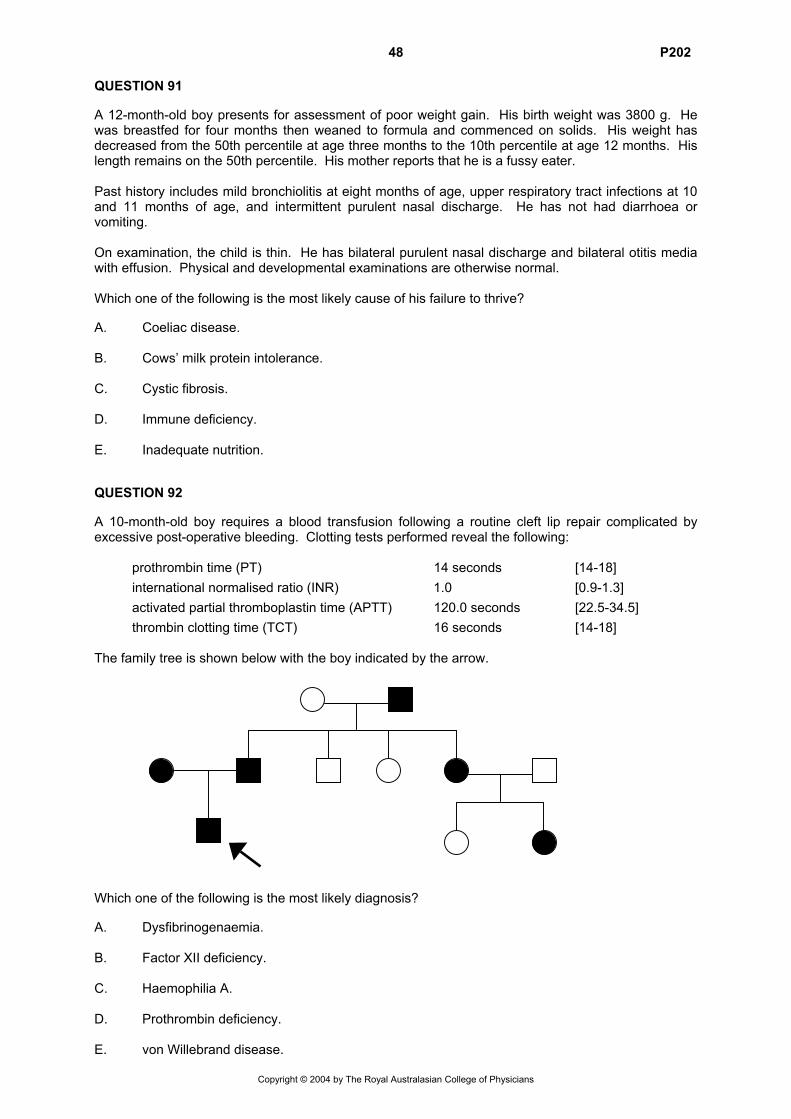
48 P202 QUESTION 91 A 12-month-old boy presents for assessment of poor weight gain. His birth weight was 3800 g. He was breastfed for four months then weaned to formula and commenced on solids. His weight has decreased from the 50th percentile at age three months to the 10th percentile at age 12 months. His length remains on the 50th percentile. His mother reports that he is a fussy eater. Past history includes mild bronchiolitis at eight months of age, upper respiratory tract infections at 10 and 11 months of age, and intermittent purulent nasal discharge. He has not had diarrhoea or vomiting. On examination, the child is thin. He has bilateral purulent nasal discharge and bilateral otitis media with effusion. Physical and developmental examinations are otherwise normal. Which one of the following is the most likely cause of his failure to thrive? A. Coeliac disease. B. Cows’ milk protein intolerance. C. Cystic fibrosis. D. Immune deficiency. E. Inadequate nutrition. QUESTION 92 A 10-month-old boy requires a blood transfusion following a routine cleft lip repair complicated by excessive post-operative bleeding. Clotting tests performed reveal the following: prothrombin time (PT) 14 seconds [14-18] international normalised ratio (INR) 1.0 [0.9-1.3] activated partial thromboplastin time (APTT) 120.0 seconds [22.5-34.5] thrombin clotting time (TCT) 16 seconds [14-18] The family tree is shown below with the boy indicated by the arrow. Which one of the following is the most likely diagnosis? A. Dysfibrinogenaemia. B. Factor XII deficiency. C. Haemophilia A. D. Prothrombin deficiency. E. von Willebrand disease.
Copyright © 2004 by The Royal Australasian College of Physicians
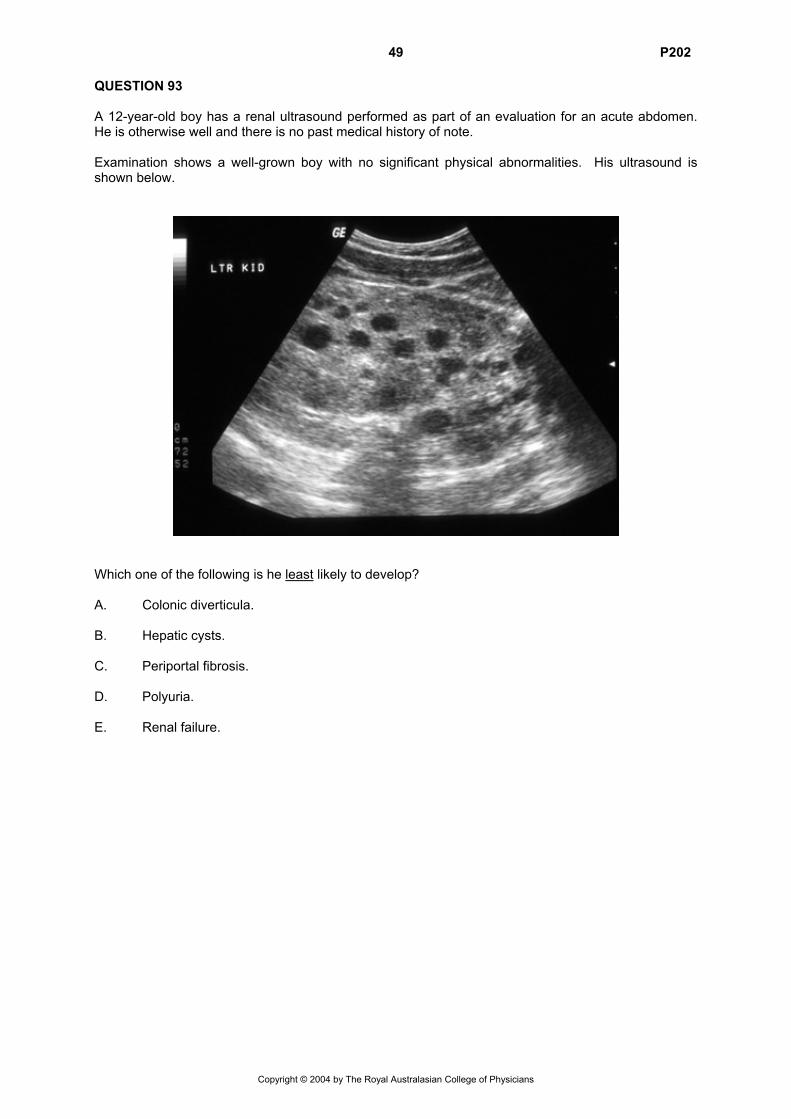
49 P202 QUESTION 93 A 12-year-old boy has a renal ultrasound performed as part of an evaluation for an acute abdomen. He is otherwise well and there is no past medical history of note. Examination shows a well-grown boy with no significant physical abnormalities. His ultrasound is shown below.
Which one of the following is he least likely to develop? A. Colonic diverticula. B. Hepatic cysts. C. Periportal fibrosis. D. Polyuria. E. Renal failure.
Copyright © 2004 by The Royal Australasian College of Physicians
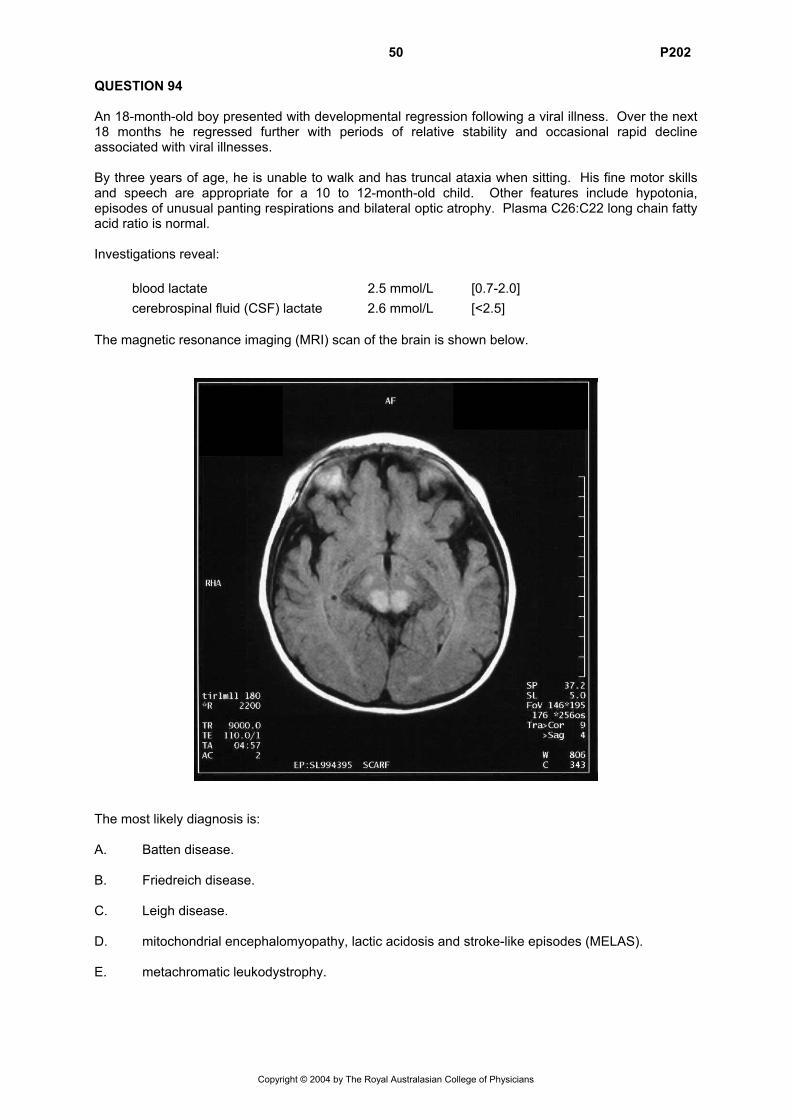
50 P202 QUESTION 94 An 18-month-old boy presented with developmental regression following a viral illness. Over the next 18 months he regressed further with periods of relative stability and occasional rapid decline associated with viral illnesses. By three years of age, he is unable to walk and has truncal ataxia when sitting. His fine motor skills and speech are appropriate for a 10 to 12-month-old child. Other features include hypotonia, episodes of unusual panting respirations and bilateral optic atrophy. Plasma C26:C22 long chain fatty acid ratio is normal. Investigations reveal: blood lactate 2.5 mmol/L [0.7-2.0] cerebrospinal fluid (CSF) lactate 2.6 mmol/L [<2.5] The magnetic resonance imaging (MRI) scan of the brain is shown below.
The most likely diagnosis is: A. Batten disease. B. Friedreich disease. C. Leigh disease. D. mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS). E. metachromatic leukodystrophy.
Copyright © 2004 by The Royal Australasian College of Physicians
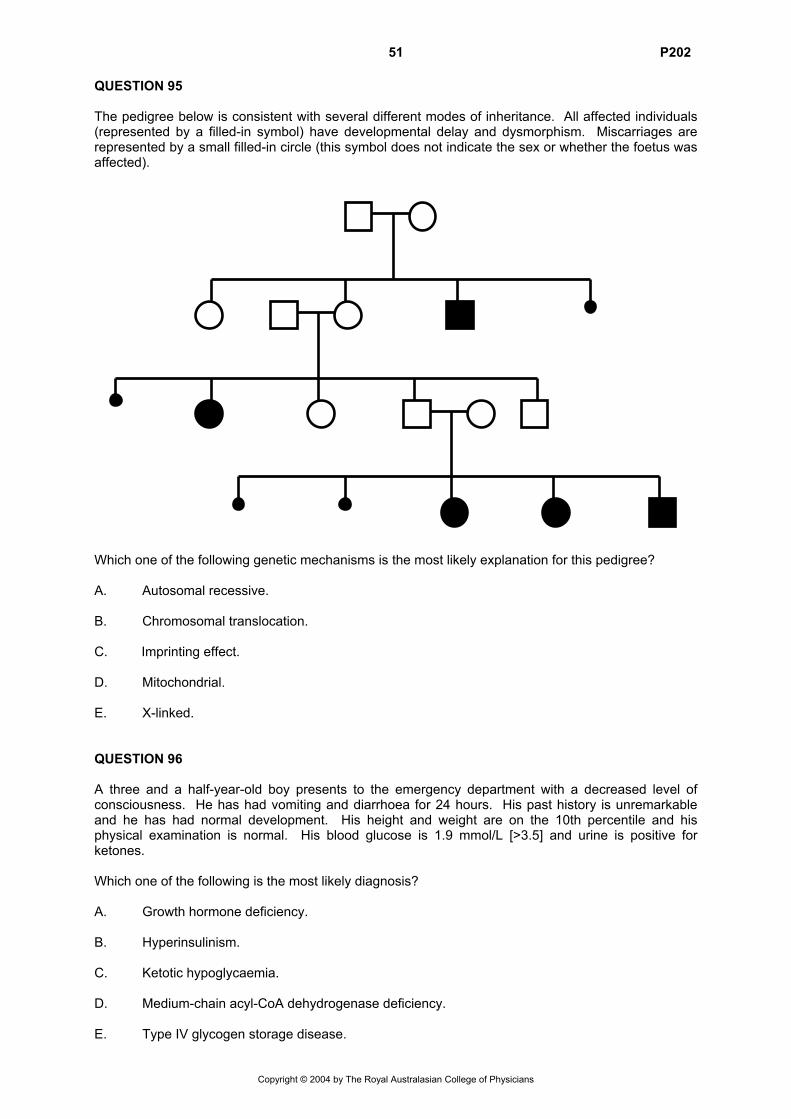
51 P202 QUESTION 95 The pedigree below is consistent with several different modes of inheritance. All affected individuals (represented by a filled-in symbol) have developmental delay and dysmorphism. Miscarriages are represented by a small filled-in circle (this symbol does not indicate the sex or whether the foetus was affected). Which one of the following genetic mechanisms is the most likely explanation for this pedigree? A. Autosomal recessive. B. Chromosomal translocation. C. Imprinting effect. D. Mitochondrial. E. X-linked. QUESTION 96 A three and a half-year-old boy presents to the emergency department with a decreased level of consciousness. He has had vomiting and diarrhoea for 24 hours. His past history is unremarkable and he has had normal development. His height and weight are on the 10th percentile and his physical examination is normal. His blood glucose is 1.9 mmol/L [>3.5] and urine is positive for ketones. Which one of the following is the most likely diagnosis? A. Growth hormone deficiency. B. Hyperinsulinism. C. Ketotic hypoglycaemia. D. Medium-chain acyl-CoA dehydrogenase deficiency. E. Type IV glycogen storage disease.
Copyright © 2004 by The Royal Australasian College of Physicians
52 P202 QUESTION 97
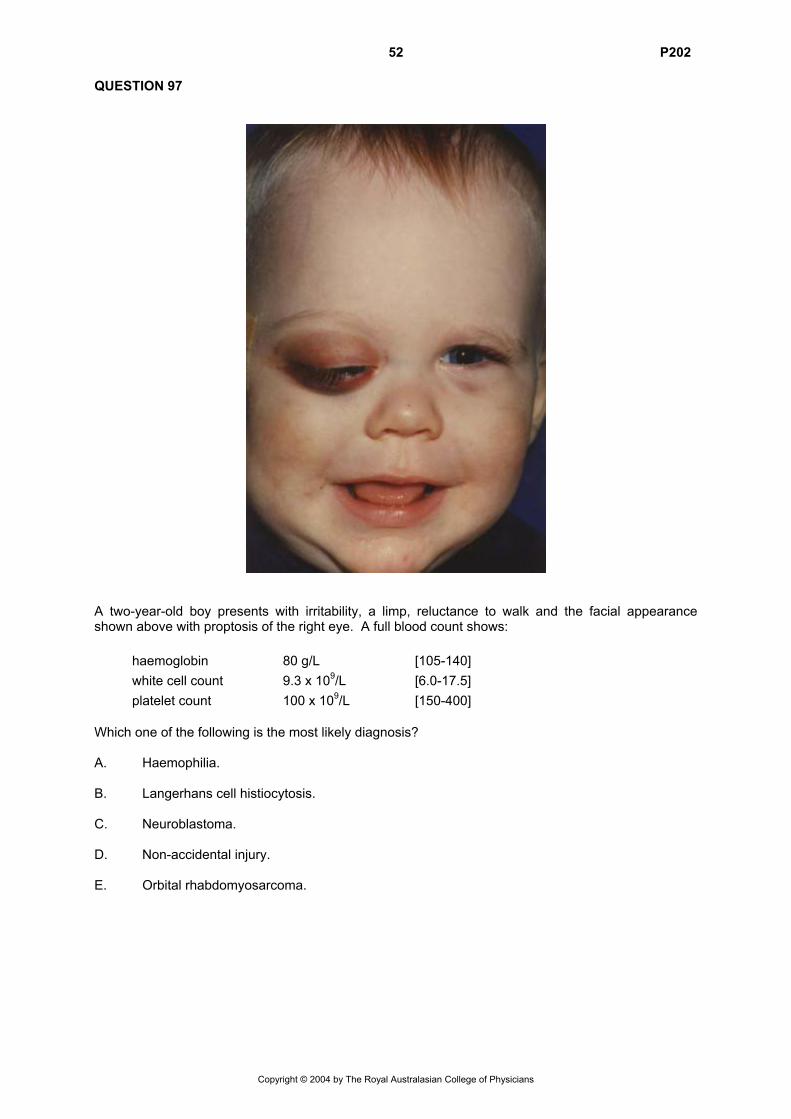
A two-year-old boy presents with irritability, a limp, reluctance to walk and the facial appearance shown above with proptosis of the right eye. A full blood count shows: haemoglobin 80 g/L [105-140] white cell count 9.3 x 109/L [6.0-17.5] platelet count 100 x 109/L [150-400] Which one of the following is the most likely diagnosis? A. Haemophilia. B. Langerhans cell histiocytosis. C. Neuroblastoma. D. Non-accidental injury. E. Orbital rhabdomyosarcoma.
Copyright © 2004 by The Royal Australasian College of Physicians
53 P202 QUESTION 98 A term baby is noted to be going blue during feeds on the second day of life. He seems to behave normally between feeds except for frequent small vomits. No abnormality is detected on physical examination. His chest X-ray shows patchy changes in the right upper lobe consistent with consolidation. Which one of the following is the most likely diagnosis? A. Choanal atresia. B. Congenital heart disease. C. Congenital laryngeal cleft. D. Gastro-oesophageal reflux. E. Tracheo-oesophageal fistula. QUESTION 99 For which one of the following conditions is there the best evidence of benefit from systemic corticosteriods? A. Acute disseminated encephalomyelitis. B. Cerebral malaria. C. Guillain-Barré syndrome. D. Meningococcal meningitis. E. Tuberculous meningitis. QUESTION 100 A four-month-old infant presents with biphasic stridor since day one of life and an unusual cry, which has been described as ‘quiet’. The infant sucks and swallows normally. Growth and development are also normal. The most likely cause of the stridor is: A. infantile larynx (laryngomalacia). B. lingual cyst. C. subglottic haemangioma. D. vascular ring. E. vocal cord lesion.
Copyright © 2004 by The Royal Australasian College of Physicians
54 P202
Copyright © 2004 by The Royal Australasian College of Physicians
2002 FRACP Written Examination
Paediatrics & Child Health
Paper 2 – Clinical Applications
Answers
1. C 34. E 67. B 2. A 35. A 68. B 3. E 36. A 69. D 4. E 37. B 70. C 5. B 38. C 71. A 6. A 39. D 72. E 7. A 40. C 73. E 8. E 41. B 74. B 9. A 42. C 75. E 10. A 43. D 76. A 11. C 44. B 77. A 12. B 45. B 78. E 13. B 46. D 79. D 14. C 47. E 80. B 15. C 48. B 81. E 16. D 49. B 82. C 17. A 50. B 83. E 18. C 51. A 84. B 19. C 52. B 85. D 20. D 53. B 86. A 21. C 54. B 87. B 22. B 55. C 88. C 23. A 56. C 89. D 24. C 57. E 90. E 25. A 58. B 91. E 26. B 59. D 92. E 27. D 60. D 93. C 28. B 61. E 94. C 29. D 62. A 95. B 30. C 63. B 96. C 31. D 64. B 97. C 32. E 65. A 98. E 33. A 66. D 99. E 100. E