2 uti
56
URINARY TRACT INFECTION
-
Upload
nuramalina-yahaya -
Category
Documents
-
view
26 -
download
0
Transcript of 2 uti

URINARY TRACT
INFECTION

Definitions
UTI : Inflammatory response of urothelium to bacterial invasion associated with bacteriuria &
Pyuria.
Bacteriuria: Presence of bacteria in urine which is normally free of bacteria.It may be due to contamination.
Pyuria: Presence of WBCs in urine.
Bacteriuria without pyuria: Colonization with no infection.
Pyuria without bacteriuria: T.B, stones, cancer.
Sterile culture, pus but no bacteria

Uncomplicated UTI: Inf. in normal U.T both structurally & functionally.
Complicated UTI: U.T is functionally or structurally
abnormal, host is compromised, increased virule-
nce of bacteria (pregnancy, elderly, DM, instrume-
ntation).
First or isolated: Never had inf. before or since a
long time.
Unresolved inf.: not responded to antimicrobials.
Recurrent inf.: occur after successful resolution of inf.

Incidence & Epidemiology
-UTIs are the most common bacterial inf.
-1.2% of office visits by females & 0.6% by males.
-50% of females will experience UTI during life.
-Once a pt. has inf., is likely to develop subseque-
nt infections.

Pathogenesis:
Routes of infection:
1-Ascending route:
-Bowel reservoir----urethra----bladder
e.g: perineum soiled with faeces.
indwelling catheter
-Cystitis may ascend to kidney by VUR.
2-Haematogenous route:
-Renal infection with staph. from a septic focus.
3-Lymphatic route:
-Not common.
-From adjacent organs (severe bowel inf. – RP abscess).
Most common
Skin carbuncle

Urinary Pathogens:
E. Coli : 85% of community acquired
50% of hospital acquired
Proteus, klebsiella, gm +ve (E. faecalis): remain.
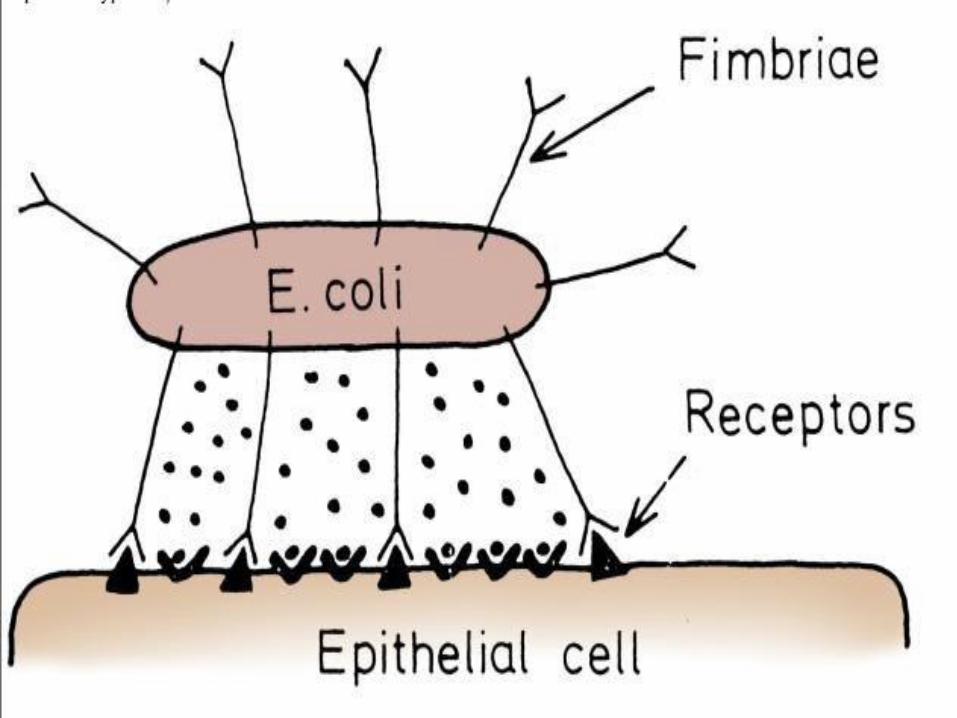
Bacterial adherence:
Bacterial adhesins:
-UP expresses a number of adhesins that allow it
to attach to U.T tissues.
Bacteria should adhere to urothelium

Natural defenses of U.T:
1- Periurethral & urethral region:
- Normal flora of introitus & urethra contain orga-
- nisms as lactobacilli & streptococci forming a
- barrier against UP.
- - Flow of urine.
2- Urine:
- Organisms normally colonizing the urethra do
not multiply in urine.
- Bacterial growth is inh. by dilute urine or high osmolality assoc. with low PH.
- Tamm-Horsfall ptn. (1000ng/ml) block bacterial
binding to urothelial receptors.
3- bladder emptying.
4- General immunity.

Diagnosis
- -Urine & U.T are normally free of bacteria & infl.
Urine collection:
-Mid stream.
-How to collect ?
voided or catheterized
Suprapubic aspiration: highly accurate,
useful in newborn
pts who can not void
-Non circumcised: prepuce retracted, glans washed
-In females: spread labia, wash introitus, mid str.
Urine analysis:
5-10 ml centrifuged for 5 min. at 2000 rpm.
Bacteriuria found in 90% of infs. with counts
>100000 CFU/ml.
2 WBCs/HPF in centrifuged specimen= 10 in an
unspined specimen & both correlates with bacte-
ruria.
Imaging techniques:
-Not required in most cases.
-Indications: fever- failure to respond to treatment
recurrent infs.- D.M- history of stones or surgery.
-Plain, IVU, VCUG, U/S, CT.
Centrifugal > concentrated > ⬆️number
To find the cause
Infection > immunity not very good

Principles of antimicrobial treatment:
-Efficacy is dependent on drug level in urine &
duration this level remains above MIC of inf.
organism.
-Concentration in blood is not important as in
urine, except in septicemia or bacterimia.
-Patients with renal failure:
Dose modification are necessary for drug cleared
only by kidneys.
Conc. power is impaired ---difficult eradication of
infection.
⬇️dose

Bladder infections
Uncomplicated cystitis:
-Most caes in females.
-25% between 20-40 yrs.
Risk factors:
-Weak urine flow.
-Promote colonization: sexual activity.
-Facilitate ascent: catheter, fecal incontinence.
Clinical presentation:
-Burning, frequency, urgency, S.P pain.
-Haematuria, foul smelling urine.
-Fever & chills usually absent (superficial mucosal infection).
Causative organism: E. coli 80-90%
Short & straight urethra
Due to obstruction, ⬆️residual urine > ⬆️risk of infection
Lab diagnosis:
-urine analysis: pyuria, bacteriuria, hematuria.
-urine culture: often not necessary.
Treatment:
-TMP-SMX, quinolones, floroquinolones
-Duration: 3 days.
Complicated cystitis:
-Occur in compromised U.T or by resistant org.
-mild cystitis----life threatening renal inf. & urosepsis.
-Urine culture is mandatory.
-treatment of cause.
Empirical rx, no need culture
BPH

Kidney Infections
Acute Pyelonephritis:
-Inflammation of both renal parenchyma & pelvis.
Causative organism:
-E. coli (80%), proteus, klebsiella, pseudomonas
-Rarely, gm +ve.
Pathology:
-Renal enlargement, capsule strips easily, small
yellowish white cortical abscesses with parench-
ymal hyperemia.
-Glomeruli usually spared, neutrophil infiltrate.

Clinical picture:
-Chills, fever (100F or >), flank pain.
-LUTS (dysuria, urgency, frequency).
-GIT symptoms.
Lab diagnosis:
-CBC: leucocytosis with predominance of
neutrophils, inc.ESR & C- reactive ptn.
U.A: WBCs in clumps, bacterial rods.
WBC casts
Specific casts (bacteria in ptn matrix).
U.C:
Blood culture:
Triad
Infection in kidney > pus cell come down > cystitis

Radiology:
IVU: renal enlargement (1.5 cm greater in length).
focal ― (focal bacterial nephritis)
disappear with treatment.
calyceal & ureteral dilatation (endotoxins)
U/S & CT: to diagnose complicated PN
to reevaluate pts not responding after
72 hours treatment.
Treatment: Antibiotics for 7 days.
Bed rest – antipyretics.
Hospitalize or not ?
Fever return to N within 2-3d after rxIf no response > imaging > US, CT


Emphysematous PN:
-Acute necrotising parenchymal & perirenal infn.
caused by gas forming UP.
-Organism cause fermentation of glucose ----CO2.
-However, not common in diabetics.
Should be considered compl. of severe PN.
-Mortality rate 20-40%
Causative organism:
-E. coli (commonest), klebsiella, proteus.
Clinical picture:
-Triad of fever, vomiting, flank pain.
-Pneumaturia, when infn. involves collecting system.
Triad, same as pyelonephritis, but more severe
Air in urine, frothy

Imaging:
-Plain KUB: crescentic gas shaddow (in renal
space) & loculated ― ― (in parench.)
-IVU: rare of value (NF or poorly functioning K.)
U/S: gas.
CT: procedure of choice.
Treatment: surgical emergency
-Fluid resuscitation & broad spectrum antibiotics.
-Nephrectomy if no improvement after few days.
Can be deferred if condition improved.
May die
Gas inside & around the kidney


Renal Abscess:
-Collection of purulent material confined to renal
parenchyma.
-Usually due to VUR in an obstructed kidney.
-Causative organism: g +Ve or –Ve.
Clinical picture:
-Triad------cystitis
-History of g +Ve source of inf.(1-8 weeks) before
onset of symptoms. e.g: skin carbuncle.
Lab diagnosis:
-Leucocytosis, pyuria, bacteriuria (if communicat).
-Urine culture: no or different organism (bld borne).
Diagnosis-

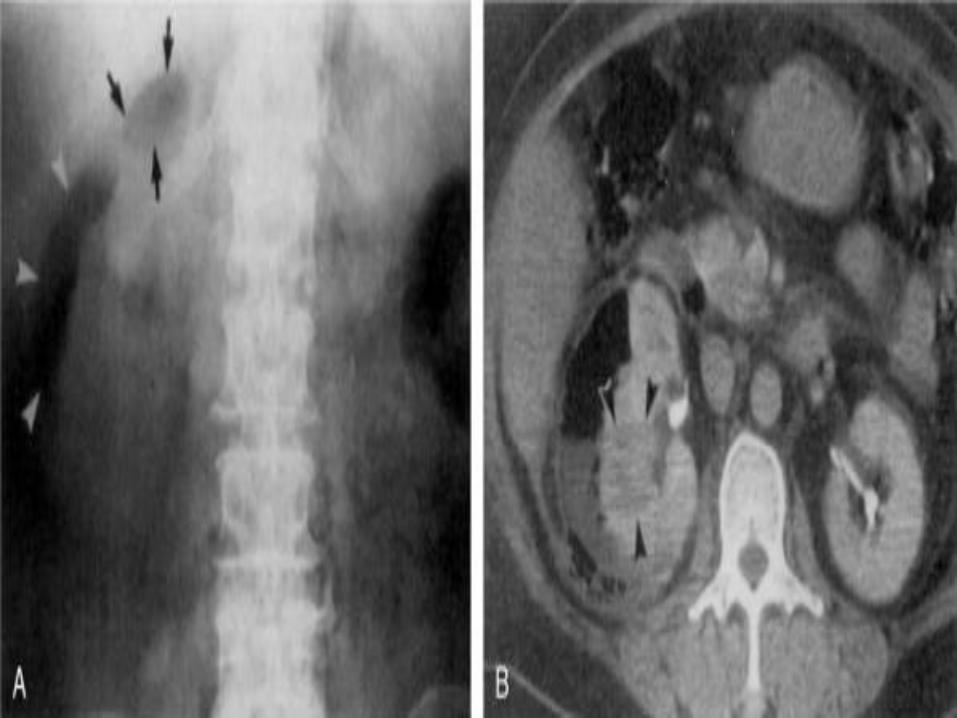
Radiology:
-Renal enlargement & distortion of renal contour.
-Renal fixation on insp. & exp. films.
-Obliteration of psoas shadow & scoliosis.
-CT is the procedure of choice
Renal enlargement & area of low attenuation.
Thickening of perinephric fascia.
Treatment:
-PC or open drainage (DD. Renal tumor).
-I.V antibiotics & observation, if <3cm.-----good response.
-Follow up with U/S or CT till complete resolution.
Normally mobile Fix to the muscle at the back
Shadow not apparent Occur in Perinephric collection & enlargement
Due to contraction of psoas muscle
Per cutaneous
> 3cm


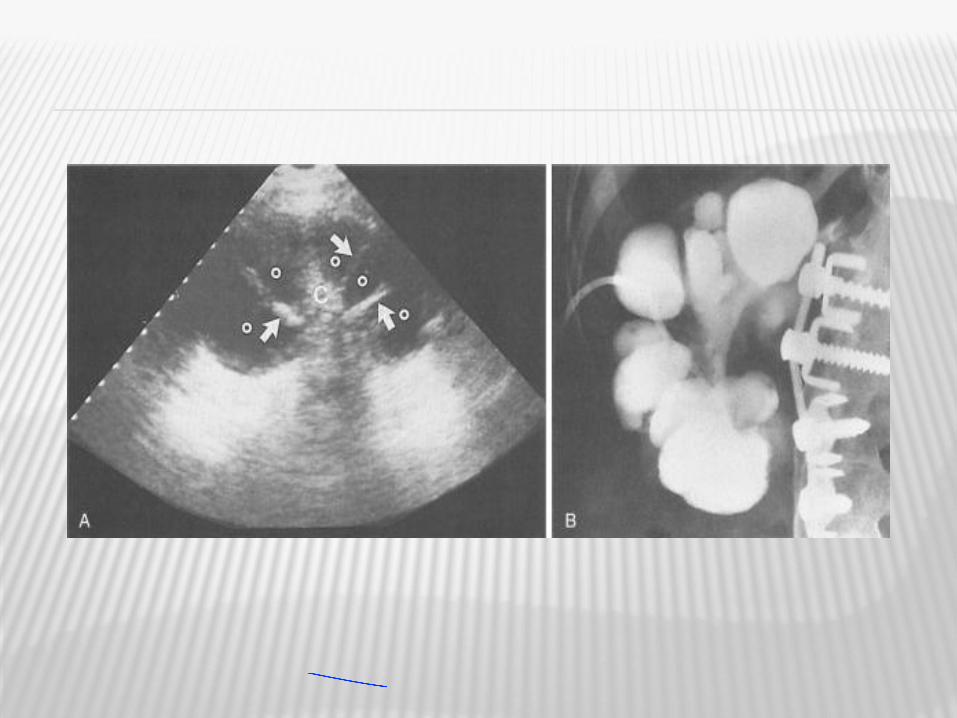
Infected Hydronephrosis & Pyonephrosis:
Infected HN: bacterial inf. in a hydronephrotic k.
Pyonephrosis:inf. HN associated with suppuration
of renal parenchyma----partial or total loss of renal function.
Differentiation not always easy.
Clinical picture:
-Triad.
-Bacteria may not be present if ureter completely
obstructed.
Radiology: internal ecchoes in dilated P.C system.
Treatment: drainage &antibiotics.
First obstruction then infection on top
Infection from start
More severe , due to obstruction + infection
PC & double j stents
Perinephric fat
Capsule
Renal capsule
Perinephric space

Perinephric abscess:
Etiology:
-Rupture of a cortical abscess into perinephric sp.
-Infected perirenal hematoma or urinoma.
-Spread of osteomyelitis from T.B lumbar spine.
When it rupture through renal fascia ---paraneph.
abscess.
Clinical picture: insidious onset, 1/3 afebrile.
Local signs of infl. (hotness, redness, oedema,
loin mass may be pointing)
No response to antibiotics.

Radiology:
-Absent psoas shaddow, elevated or immobile
diaphram.
-U/S & CT: ecchogenic collection.
Treatment:
-Surgical drainage (if large)
-PC ― (if small)
Same sign as renal abscess

PROSTATITIS
Etiology:
1- G –Ve: E. coli (80%), kleb., pseudomonas,….
2- G +Ve: staph aureus (5-10%)
3- Chlamydia & U. urealyticum: minor role.
Risk factors:
1- Intra-prostatic ductal reflux.
2- Immunologic alteration inside prostate.
3- Acute epididymitis, indwelling catheter, TURP
especially with infected urine.
Prostate = exocrine, has duct, open into prostatic urethra

Pathology:
-Increase no. of infl. cells within parenchyma.
-Lymphocytic infil. in stroma adjacent to acini
(most common pattern).
-Corpora amylacea (deposition of pr. secretion
around a sloughed epithelial cell) may obstruct
pr. gland.
Classification: ―Traditional classification system‖
Type s. of UTI bacteria infl. cells
1-ABP: severe + +
2-CBP: mild + +
3-NBP: ----- - +
4-Prostatodynia: ----- - -
Infection > prostate compressed acini > itis > epithelium get shredded/slough > around the slough epithelium > prostatic secretion collected ( slough acini surround prostate secretion )
Acute bacterial prostatitis
Chronic
Non
Spasm in muscle of pelvic floor
Symptoms

Clinical picture:
1- ABP: fever, severe irritative & obstructive C/O.
5%------- CBP
2- CBP: asymptomatic
irritative & obstructive C/O
3- NBP: pain (predominant C/O) in perineum,S.P,
penis, testis, low back.
4- Prostatodynia: painful ejaculation (50%)
symptoms tend to wane & wax over time
1/3 improve over one year.
Severest, may end by complete @ acute retention
When not properly rx
Not as severe as ABP
May disappear without rx

Diagnosis:
1- Physical examination:
-Important but not helpful for diagnosis or classificat
ABP: prostate is hot, boggy, very tender
Other types: prostate is normal.
2- Cytology & culture:
- Stamey 4 glass urine collection
Treatment:
1- Antibiotics: for ABP & CBP.
2- Alpha adr. blockers: for NBP & prostatodynia
with poor relaxation of B.N -----increase ur. flow &
decrease IPR.
Soft due to pus & breakdown of tissues
In CBP, N prostate
DRE, in ABP only, but sometimes can't due to severe pain & tenderness

1st gushing of urineUrethra+ve in urethritis
Midstream BladderCystitis @ pyelonephritis
Do prostatic massage
Express prostatic secretions Too little, so need to void
Voiding bladder Prostatic urethraProstatitis

3- Anti-inflammatory:
NSAIDs- cortisone.
4- Ms. relaxants:
NBP & prostatodynia may be due to smooth & skeletal ms dysregulation of pelvis
& perineum.
5- Phytotherapy:
Some plant extracts show 5 alpha- reductase
activity, alpha blocker, anti- inflammatory.
6- Allopurinol:
IPR---inc. metabolites containing purine & pyrimidine in pr. ducts-----inflammation.

Orchitis:
Definition:
-Inflammation of testis, & also describe testicular
pain without evidence of infl.
Etiology:
-Isolated orchitis is relatively rare & usually viral
due to blood spread.
-Orchitis of bacterial origin usually occur due to
local spread from ipsi. epididymis (E. coli, pseud.,
Staph, strept.,N. gonorrhea).
Presentation:
-Pain- fever- nausea & vomiting- tenderness- secondary hydrocele (mild).
Dt itis
Most common mumps
Usually both, testis & epididymis
Severe
Diagnosis:
Urine analysis- urethral swab
U/S: to rule out malignancy & torsion
Treatment:
- Rest- scrotal support- hydration- antipyretics- AI
- Antibiotics.
Chronic orchitis:
-Inflammation & pain in testis, without swelling
for >6 weeks.
-Self limited & may take years to resolve.
Rx- assure, no complications - rx only analgesic
Epididymitis:
-Acute : sudden pain, swelling.
-Chronic: pain & infl. with no swelling >6 weeks.
may be due to inadequate treatment.
-Spread from bladder, urethra & prostate.
-Starts in tail-----body-----head.
-Testis is involved in most cases-----epididymo-orchitis.
Treatment:
-antibiotics for 4-6 weeks.
-Chronic: self-limiting taking long duration.
-Epididymectomy: with treatment failure & to cure
pain.
Slowly resolve

Tuberculosis (T.B)
-Always considered in a pt. with vague long
standing urinary C/O with no obvious cause.
-Age: 20-40 yrs, uncommon in children.
When to suspect?
-Following presentation without obvious etiology.
Frequency—recurrent cystitis not responding to
treatment---gross or microscopic hematuria---
sterile pyuria.
Sterile culture, there is pus but no bacteria
UT TB 2ry to 1ry TB of chest @ GIT, never 1ry

T.B of kidney:
-Organism settle in blood v. close to glomeruli.
-Caseating granulomas develop & consist of giant
cells (Langhans) surrounded by lymphocytes &
fibroblasts.
-Caseous material open through calyces---cavities
of moth-eaten appearance.
-Course depends on virulence & resistance.
-If pathology progress + obst.---autonephrectomy.
-If healing occur---fibrosis & calcification---stricture
in calyces or PUJ.
-Mycobacterium may remain viable in calcific lesions.
Cause renal parenchyma destruction
Bilateral kidney affection, even by imaging show 1 kidney affection, the other are already infected but not manifest yet





T.B of ureter:
-T.B ureteritis---fibrosis---str. usually at UVJ
-Whole ureter may be affected---multiple levels
ureteric stricture.
T.B of bladder:
-Starts around U.O---infl. & edema---T.B granuloma
-T.B ulcers is rare, occasionally whole bladder is
covered by infl. velvety granulation---bladder fibr-
osis & contraction.

KUB, calcification in bladder wall
US, calcification
Black = urine


T.B of epididymis & testis:
-Painful & infl. scrotal swelling. D.D: ep.orchitis.
-Globus minor affected alone in 40%.
-Testicular affection without ep. is very rare.
-Scrotal sinus.
T.B of penis----superficial glanular ulcer. D.D:Tr.
T.B of urethra ---urethral stricture.
Tail
TB = epididymis but spare the testisSyphilis = testis but spare epididymis
Epididymis place behind the testis> sinus > discharge at back of scrotum> sinus
Diagnosis:
1-Tuberculin test:
-M.T.B complex (M.T.B—M. bovis—M. microti—M.
africanum).
-Intradermal inj. of a PPD of tuberculin.
-Infl. condition reaching max.between 48-72 hrs.
-Central indurated zone surrounded by erythema.
-+Ve reaction =inf., but not indication of active
T.B or C/O due to T.B.
2-Urine examination:
-Sterile pyuria-2ry inf.(20%)-microhematuria(50%)
3-Urine culture:
-Lowenstein-Jensen.
-Takes 6-8 weeks (slowly growing).
-3-5 consequetive early morning samples
(org. is intermittently excreted).
4-Imaging:
-Plain KUB:
-Calcification in kidney, ureter, bladder, seminal
vesicle.
-Plain chest & spine.
-IVU:
-Fibrosed & occluded calyx (lost calyx).
-Moth-eaten cavities, HUN, contracted bladder.

Treatment
First line drugs:
1-Isoniazid (INH): hepatotoxicity, peripheral neuritis.
5 mg/kg maximum 300 mg
2-Rifampicin: hepatotoxicity
10 mg/kg max. 600 mg
3-Pyrazinamide: hepatotoxicity
20-25 mg/kg
4-Streptomycin: ototoxicity
5-Ethambutol: retrobulbar neuritis
15-25 mg/kg

Cornerstone is multidrug treatment to decrease
duration of treatment & drug resistant developm-
ent.
Second line drugs:
-kanamycin—amikacin—ciprofloxacin……
Guidelines:
-Short course 6 months regimen.
-All drugs given in a single dose.
-Followup with urine culture at 3, 6, 12 months
after treatment finished.
Surgery: delayed until medical treatment adminis- tered for 4-6 weeks.
- nephrectomy- stricture ureter- contracted bladder ( ⬆️size, augmentation )
Parasitic diseases
Urinary schistosomiasis:
Caused by S. haematobium.
Pathology & pathogenesis:
-Worms in pelvic v. plexus----eggs in lower UT.
-Granulomas formed in response to egg Ag------
large,bulky, hyperemic polypoid masses. As egg
laying ceases, eggs are destroyed or calcified &
infl. wanes & replaced by f.t. (inactive form). Acute
& chronic bladder ulcers
-Obstructive uropathy occur due to chronic dis.
Usually bilateral asymmetrical (JV & lower ureter)
-Bladder cancer is a sequalae:early, sq.c.c (60-90%).
Fibrous tissue
Egg in lamina propria ( submucosa ) layer > chronic, inactive > blood supply to mucosa ⬇️ > ulcer ( in acute & chronic )
Usually lower ureter, bladder, urethra
Dt chronic irritation, usually squamous cell carcinoma, not TCC
Presentation:
Acute:‖ Katayama fever‖
-fever, lymphadenopathy, splenomegaly, urticaria
-occur 3-9 weeks after inf.
-terminal hematuria & burning.
Chronic:
-HUN—contracted bladder
Diagnosis:
1-Presence of eggs with terminal spikes is diagn-
ostic of & only possible during active inf.
2-Serologic tests: do not diff. between acute & ch
inf.
3-Plain & IVU.
50% urine ( acute only )50% deposited
Hydronephrosis
> frequency

Treatment:
Medical:
Praziquentel: drug of choice
cure rate 80-100%
dose:2 oral doses of 40mg/kg in 24 hrs
No serious side effects.
Surgical: nephrectomy—ureteric implantation

Filariasis
Lymphatic filariasis:
-Causative organism: W. bancrofti
-Cycle proceeds from human---mosquito---human.
-Acute lymphatic infiltration----fever, lymphangitis &
lymphadenitis---chronic lymphatic obstruction
& dilation----hydrocele, elephantiasis of limbs &
chyluria.
-Diagnosis: C.p & Giemsa stain for blood.
-Treatment:
Diethylcarbamazine (DEC), ivermectin, albendazole.
Very rare

Nonlymphatic Filariasis:
-Transmitted by black flies (Simulum species).
-Adult worms inhibit S.C tissues----f. nodules in which it is encapsulated.
-Microfilaria travel through dermis & eye ----------blindness.
-Diagnosis:
Microscopic exam. of skin snips under normal saline or Giemsa stain.
Treatment:
-Ivermectin. DEC not used due to severe allergic
immune response to microfilaria dying in skin.