
Advertising Direct Marketing. U.S. advertising expenditures ($ millions)
Upload
dominic-richCategory
view
216download
0
ALASKACARE HEALTH PLANS
STATE OF REFORMOCTOBER 4, 2013

State of Reform - October 4, 2013 2
HEALTH CARE SPENDING: US
Per Capita Total Current Health Care Expenditures, U.S. and Selected Countries, 2009
^OECD estimate.*Break in series.Notes: Amounts in U.S.$ Purchasing Power Parity, see http://www.oecd.org/std/ppp; includes only countries over $2,500. OECD defines Total Current Expenditures on Health as the sum of expenditures on personal health care, preventive and public health services, and health administration and health insurance; it excludes investment. Source: Organisation for Economic Co-operation and Development. “OECD Health Data: Health Expenditures and Financing”, OECD Health Statistics
State of Reform - October 4, 2013 3
HEALTH CARE SPENDING: US
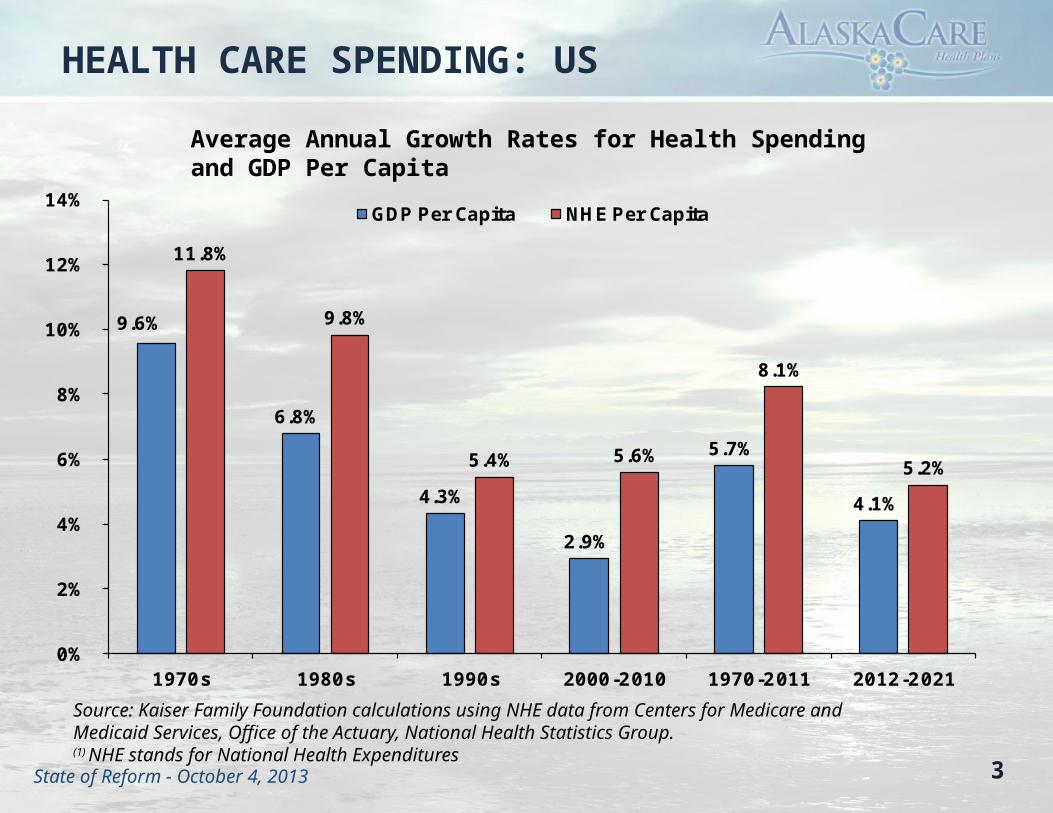
Average Annual Growth Rates for Health Spending and GDP Per Capita
9.6%
6.8%
4.3%
2.9%
5.7%
4.1%
11.8%
9.8%
5.4% 5.6%
8.1%
5.2%
0%
2%
4%
6%
8%
10%
12%
14%
1970s 1980s 1990s 2000-2010 1970-2011 2012-2021
GDP Per Capita NHE Per Capita
Source: Kaiser Family Foundation calculations using NHE data from Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group.(1) NHE stands for National Health Expenditures

State of Reform - October 4, 2013 4
STATE HEALTH CARE SPENDING
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011$0.00
$200.00
$400.00
$600.00
$800.00
$1,000.00
$1,200.00
$1,400.00
$1,600.00
$1,800.00
$2,000.00
$2,200.00Union
JRS
Corrections
Medicaid
Workers Comp
TRS
PERS
AlaskaCare

State of Reform - October 4, 2013
ALASKACARE GOALS
Provide high-quality, high-value, fiscally sustainable care to AlaskaCare members through: • Increasing member engagement• Supporting evidence-based medicine and
promoting data-driven decision making• Collaborating with providers to transform the
Alaska health care market
5

State of Reform - October 4, 2013 6
STATE COSTS FOR ACTIVE EMPLOYEE HEALTH INSURANCE
• State employee health insurance costs have more than doubled in the past decade, from $117mm in 2003 to $256mm in 2012.
• The population-adjusted increase is approximately 7%/year.

State of Reform - October 4, 2013
STATE OF ALASKAEMPLOYEE HEALTH INSURANCE
7
AlaskaCare Health Plan Union Health TrustsEmployees: 6,700* Employees: 10,500*
AVTEC General Government (GGU/ASEA)
Confidential Employees Labor, Trades and Crafts
Correctional Officers Public Safety Employees Association
Marine Engineers Masters, Mates & Pilots
Mt. Edgecumbe Teachers
Supervisory
Inland Boatmen’s Union
Exempt/Partially Exempt Employees
*Population counts are approximate

State of Reform - October 4, 2013
BENEFIT CREDIT
8
• Amount State contributes per employee per month
• Subject to negotiations
• Historically based on AlaskaCare premiums and plan experience
• FY 14 benefit credit:– $1,389 per month
– $16,668 per year (medical & dental)
FY 01 FY 14$0
$200
$400
$600
$800
$1,000
$1,200
$1,400
$1,600
$525
$1,389
Benefit Credit

State of Reform - October 4, 2013
US EMPLOYER & EMPLOYEE CONTRIBUTIONS
9
Private Employers Public Employers AlaskaCare (FY13) $0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
$18,000
$4,495 $3,368
$10,704 $12,381
$15,960
Worker Contribution (Yearly) Employer Contribution (Yearly)Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2012.
Worker and Employer Premium Contributions for Family Coverage / Economy Plans (2012)
Participants in the economy plan don’t make
any contribution.

State of Reform - October 4, 2013 10
PLAN DEMOGRAPHICS: ACTIVE
Demographic information:• Average number of members (plus dependents) is around 17,000 • Almost even distribution of men and women• Average age is 35 • 0.18% of our membership (31 people) accounted for 14% of the cost of medical claims paid
out• Highly prevalent conditions are:
– Psychiatric disorders– Metabolic disorders– Gastrointestinal disorders– Diabetes

State of Reform - October 4, 2013 11
ACTIVE HEALTH PLAN CHALLENGES
• Recent plan experience: spike in high-cost claimants (up approximately 20% in 2012)
• State of Alaska culture• Traditional plan structure• Geography/dispersed population• Network development/access• Cost of services
State of Reform - October 4, 2013 12
COSTS FOR RETIREE HEALTH INSURANCE
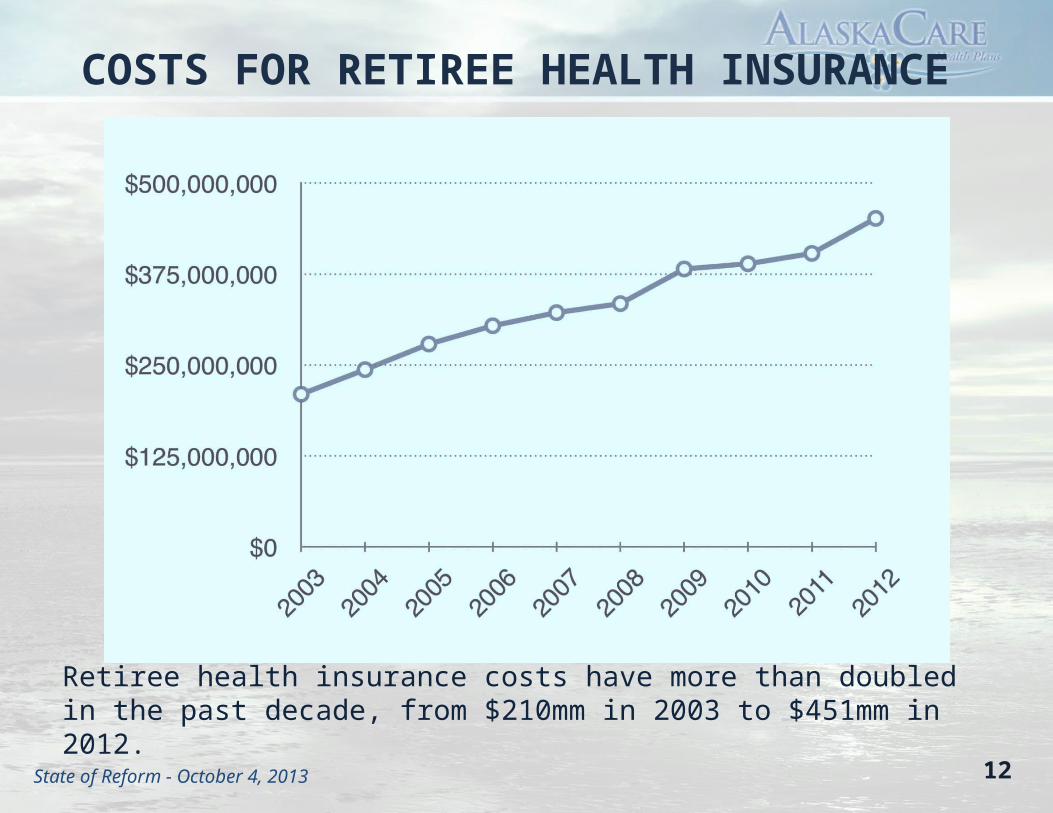
Retiree health insurance costs have more than doubled in the past decade, from $210mm in 2003 to $451mm in 2012.

State of Reform - October 4, 2013 13
BENEFITS: PERS/TRS
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
FY08
FY09
FY10
FY11
FY12
FY13
Propose
d FY14
$0
$200,000,000
$400,000,000
$600,000,000
$800,000,000
$1,000,000,000
$1,200,000,000
PERS/TRS GF State Assistance (SB125)
Projected GF State Assistance (Level Dollar)

State of Reform - October 4, 2013 14
PROJECTED RETIREMENT SYSTEM GROWTH
2010 2012 2014 2016 2018 2020 2022 2024 2026 2028 20300
10,000
20,000
30,000
40,000
50,000
60,000
70,000

State of Reform - October 4, 2013 15
PLAN DEMOGRAPHICS: RETIREE
Demographic information:• Average number of members (plus dependents) is around 65,000• Slightly higher distribution of women (54%)• Average age is 63• 0.20% of our membership (129 people) accounted for 17.5% of the cost of medical claims
paid out. • Highly prevalent conditions are:
– Degenerative ortho – Diabetes– Metabolic disorders– Hypertension– Gastrointestinal disorders– Coronary artery related conditions– Psychological disorders
State of Reform - October 4, 2013 16
RETIREE PLAN CHALLENGES
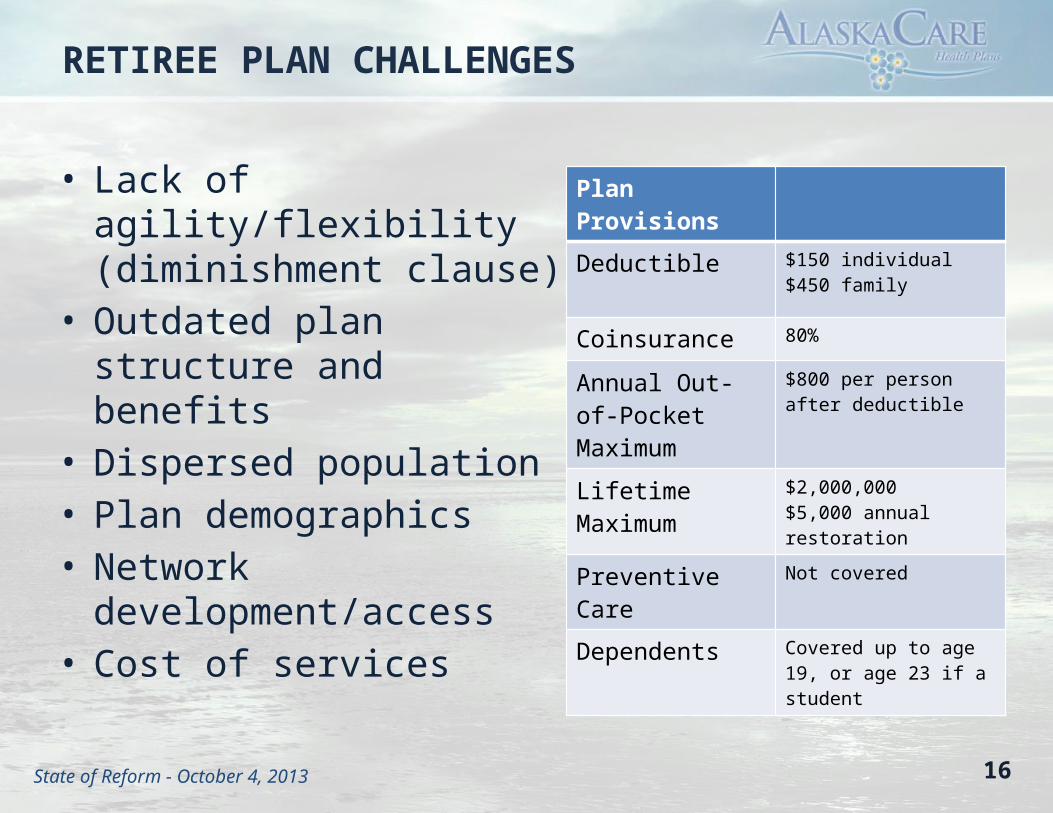
• Lack of agility/flexibility (diminishment clause)
• Outdated plan structure and benefits
• Dispersed population• Plan demographics• Network development/access• Cost of services
Plan Provisions
Deductible $150 individual$450 family
Coinsurance 80%
Annual Out-of-PocketMaximum
$800 per person after deductible
Lifetime Maximum $2,000,000$5,000 annual restoration
Preventive Care Not covered
Dependents Covered up to age 19, or age 23 if a student

State of Reform - October 4, 2013 17
SOLUTIONS

State of Reform - October 4, 2013
ALASKACARE GOALS
Provide high-quality, high-value, fiscally sustainable care to AlaskaCare members through: • Increasing member engagement• Supporting evidence-based medicine and
promoting data-driven decision making• Collaborating with providers to transform the
Alaska health care market
18

State of Reform - October 4, 2013
NEW PARTNERS: AETNA & MODAHEALTH
We have new health care partners.
As of January 1, 2014 we’ll be transitioning to Aetna, ActiveHealth Management and ModaHealth.
19

State of Reform - October 4, 2013 20
INCREASE MEMBER ENGAGEMENT: WELLNESSThe aim: move the population to the left
State of Reform - October 4, 2013 21
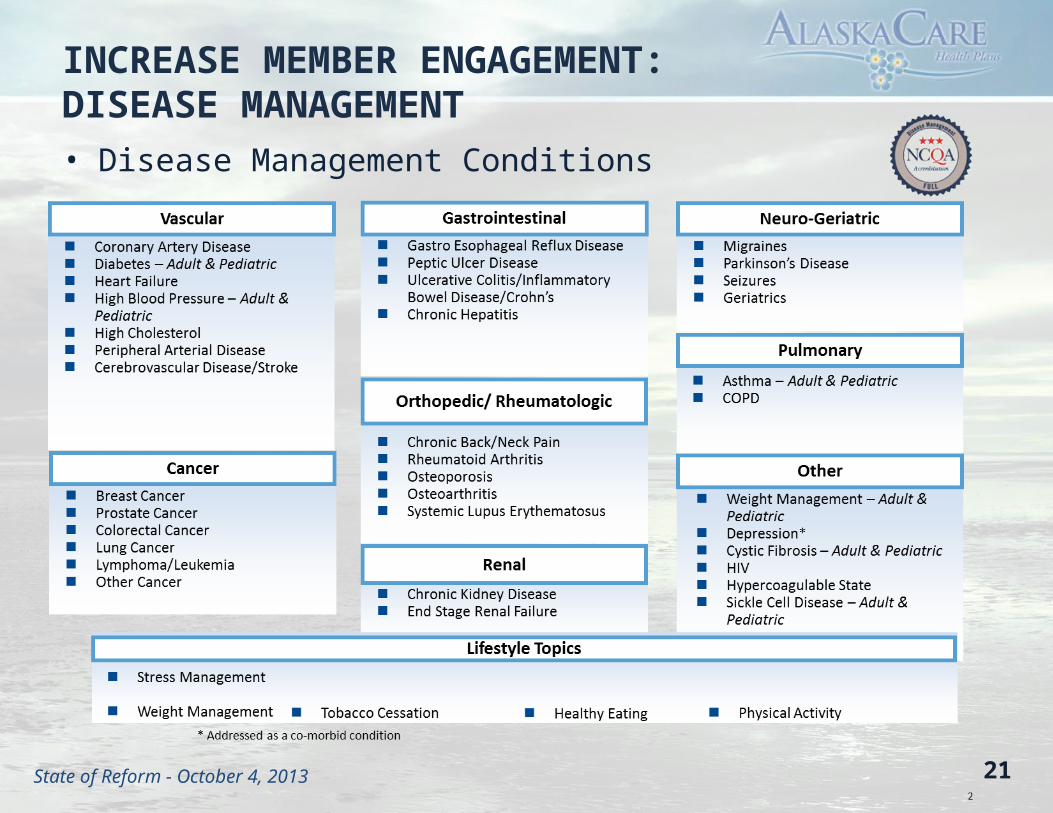
INCREASE MEMBER ENGAGEMENT:DISEASE MANAGEMENT• Disease Management Conditions

State of Reform - October 4, 2013 22
INCREASED MEMBER ENGAGEMENT: CDHP (ACTIVE)
• In 2006, the State of Indiana implemented a Consumer-Driven Health Plan (CDHP)– Individual deductible $2,500, family deductible $5,000– State contributed 45% of deductible to Health Savings Account
• In 2007, a second CDHP plan was implemented with lower deductibles but higher premiums
• Indiana saved money: CHDP 2010 savings were 10.7% or $17-$23 million• Employees saved money
– 2010 employees saved $7-$10 million– Unused funds were $30 million– Average of $2,000 per employee
• 2012 CDHP participation above 90%• CDHP participants did not put off or avoid using important health care
services

State of Reform - October 4, 2013 23
INCREASED MEMBER ENGAGEMENT: CONCIERGE SERVICES
• A dedicated concierge team - State of Alaska members will have a single point of contact for health care needs
• What is a concierge: A go-to, real, live person who is on-call and on-chat to answer any real-world questions from our members
• Concierges: – Take the time to guide members through their health care journeys– Empower members with tools and resources – Are uniquely equipped with member call history, preferences, clinical alerts and
detailed personal information at hand– Provide a warm transfer if a transfer is necessary
• Personalized guidance and advocacy

State of Reform - October 4, 2013 24
INCREASED MEMBER ENGAGEMENT: ITRIAGE
1 iTriagehealth.com2 January, 2012 edition. Aetna is the brand name used for products and services provided by one or more of the Aetna group of subsidiary companies, including Aetna Life Insurance Company and its affiliates (Aetna). Apple, iPad, iPod and iPhone are trademarks of Apple Inc., registered in the U.S. and other countries. ©2012 Aetna Inc.

State of Reform - October 4, 2013 25
EVIDENCE-BASED MEDICINE: PLAN STRUCTURE
• Align plan structure around best practices– Expand pre-certification list– Adopt Aetna’s clinical policy bulletins– Rigorous review of our plan provisions– Consider plan design changes to support evidence
based medicine: e.g. three-tier formulary, etc.• Use concierge services as opportunity for decision-
support

State of Reform - October 4, 2013 26
EVIDENCE-BASED MEDICINE: CAREENGINE
26
Assesses health opportunities: continuous data-driven evidence-based medicine

State of Reform - October 4, 2013 27
EVIDENCE-BASED MEDICINE: DATA-DRIVEN DECISION-MAKING
• Identify trends early and address them, before they become cost-drivers• Uncover “hidden cost drivers” that can address the root cause of a problem

State of Reform - October 4, 2013 28
COLLABORATE WITH PROVIDERS TO TRANSFORM MARKET
Network Strategy and Priorities
o Improve access to contracting physicians and providers
o Improve predictability and performance (cost) of contracts
o Address egregious charges/rates for targeted high volume procedureso Collaborate with Aetna to identify and engage delivery system partners
committed to designing transformative solutions
o Encourage delivery system investment in integrated care delivery
Comprehensive care models such as PCMH and ACOs
Procedure-based integration opportunities such as bundled payments
State of Reform - October 4, 2013 29
THINGS WE’RE WATCHING
• Onsite clinics (State of Montana, HCCMCA)• Centers of Excellence• Narrow networks• Reference pricing (CalPERS)• Private exchanges• Consumerism and transparency tools• Impact of public plans on health care market

State of Reform - October 4, 2013
ANY QUESTIONS?
Retirement and Benefits 6th Floor State Office Building,P.O. Box 110203Juneau, AK 99811-0203
DRB Call Centers:Outside Juneau: (800) 821-2251Juneau: (907) 465-4460Office Hours of Operation: 8 a.m. to 5 p.m. AKST
DOA Commissioner’s Office:Juneau: (907) 465-2200Anchorage: (907) 269-6293
30
www.AlaskaCare.govState of Alaska, Division of









![THOMAS, WILSON, RAGUSA, UFTTMAN & CO.app1.lla.la.gov/PublicReports.nsf/76F1D9C1A8BF37E...Public safety 780,047 Debt service 209,760 Capita] expenditures 161.636 Total Expenditures](https://static.fdocuments.in/doc/165x107/60070709e302ab04af4a4a82/thomas-wilson-ragusa-ufttman-coapp1llalagov-public-safety-780047.jpg)






