2. Leukemia
3
AML ALL CML CLL General Rapid onset & Rapid progression High Mortality Plenty of Blasts >20% (in PS or BM) low RBC, low WBC, low PLT, leukemic infiltration Indolent course. More mature forms are seen in the PS like lymphocyte and neutrophils Blasts in PS or BM is less than 20% (5-10%) WBC counts are very high Age Young adults Children Older adults Old age Clinical feature Palor, fatigue, weakness, anaemia Bleeding, bruising, petechial hemorrhages Infections, pneumonia, meningitis Hepatosplenomegaly Growth failure, fever, anaemia Bleeding Lymphadenopathy Hepatosplenomegaly Fever, anaemia Bleeding Hepatosplenomegaly Weight loss 3 phases: Chronic, Accelerated, Blast crisis Insidious onset May be asymptomatic. Lymphadenopathy No need aggressive therapy Diagnosis High clinical suspicion Family history, past history Simple PS examination. Other lab tests: Serum uric acid, LDH, RFT, Sr.Ca, electrolytes PS examination RBC normocytic normochromic WBC count increased, rarely decreased or normal. Majority of cells are Immature cells- Blasts PS shows > 20% Myeloblasts Mature neutrophils are less Morphology of AML M0- M7 type Low platelets Bone marrow examination Hypercellular Marrow Blasts are > 20% Blasts with intracytoplasmic rods- Auer Rods Increased M: E ratio Less of Megakaryocytes Cytochemistry High clinical suspicion PS & BM study (morphological diagnosis) Morphology of ALL L1, L2, L3 Lymph node aspiration & biopsy Immunophenotyping Cytogenetics Imaging (USG scan, CT) Neoplastic cells are CD10 +ve & most are Pre B cell type. 2% of child ALL & 20-30% of adult onset ALL has t(9;22) Philadelphia chromosome, t(9:22) Leucocytosis Clonal B cells are seen with arrest in maturation (arrested in between Pre-B cell & Mature B cell) All neoplastic cells show surface CD 5 +ve Mature lymphocyte markers like CD 19, 20, 21 PS examination o Total count increased, majority are mature lymphocytes, smudge cells, (smear cells, basket cells), less of neutrophils Some prolymphocytes + Identical tumor of lymph node SLL (small lymphocytic lymphoma) Autoimmune HA, Autoimmune Thrombocytopenia is common (10% of cases) May progress to aggressive types o Prolymphocytic leukemia
Transcript of 2. Leukemia

AML ALL CML CLLGeneral Rapid onset & Rapid progression
High MortalityPlenty of Blasts >20% (in PS or BM)low RBC, low WBC, low PLT, leukemic infiltration
Indolent course.More mature forms are seen in the PS like lymphocyte and neutrophilsBlasts in PS or BM is less than 20% (5-10%)WBC counts are very high
Age Young adults Children Older adults Old ageClinical feature
Palor, fatigue, weakness, anaemia Bleeding, bruising, petechial
hemorrhages Infections, pneumonia, meningitis Hepatosplenomegaly
Growth failure, fever, anaemia
Bleeding Lymphadenopathy Hepatosplenomegaly
Fever, anaemia Bleeding Hepatosplenomegaly Weight loss 3 phases: Chronic, Accelerated,
Blast crisis Insidious onset
May be asymptomatic. Lymphadenopathy No need aggressive therapy
Diagnosis High clinical suspicion Family history, past history Simple PS examination. Other lab tests: Serum uric acid,
LDH, RFT, Sr.Ca, electrolytes
PS examination RBC normocytic normochromic WBC count increased, rarely
decreased or normal. Majority of cells are Immature
cells- Blasts PS shows > 20% Myeloblasts Mature neutrophils are less Morphology of AML M0- M7 type Low platelets
Bone marrow examination Hypercellular Marrow Blasts are > 20% Blasts with intracytoplasmic rods-
Auer Rods Increased M: E ratio Less of Megakaryocytes
Cytochemistry Myeloblasts are +ve for Sudan
black B & Myeloperoxidase (MPO) Lymphoblasts are +ve for Periodic
acid schiff (PAS) AML M4 & M5 blasts are +ve for
Non- specific esterase (NSE)Immunophenotyping
Identify cells by surface markers using antibodies
Cytogenetics t(8;21) in AML M2 t(15;17) in AML M3 inv16 in AML M4
High clinical suspicion PS & BM study
(morphological diagnosis) Morphology of ALL L1, L2, L3 Lymph node aspiration &
biopsy Immunophenotyping Cytogenetics Imaging (USG scan, CT) Neoplastic cells are CD10 +ve
& most are Pre B cell type. 2% of child ALL & 20-30% of
adult onset ALL has t(9;22)
Philadelphia chromosome, t(9:22)
Leucocytosis
Clonal B cells are seen with arrest in maturation (arrested in between Pre-B cell & Mature B cell)
All neoplastic cells show surface CD 5 +ve
Mature lymphocyte markers like CD 19, 20, 21
PS examinationo Total count increased,
majority are mature lymphocytes, smudge cells, (smear cells, basket cells), less of neutrophils
Some prolymphocytes + Identical tumor of lymph node
SLL (small lymphocytic lymphoma)
Autoimmune HA, Autoimmune Thrombocytopenia is common (10% of cases)
May progress to aggressive typeso Prolymphocytic leukemiao Diffuse large B cell
lymphoma (Richter syndrome)

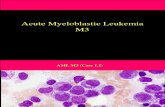
Morphology of AML (M0-M7 types)
M0 UndifferentiatedM1 Without maturationM2 With maturationM3 Promyelocytic
Numerous cytoplasmic granules- promyelocytesAuer rods are plentyComplication of DIC seen in most casesClassical t(15;17)Treated with ATRA (all trans retinoic acid)
M4 Myelomonocytic
M5 Acute monocytic leukemiaCommonly present with gingival swellings & skin nodules
M6 Acute ErythroleukemiaDi Guglielmo diseaseBinucleated & megaloblastic erythroid precursors are in excess
M7 Megakaryocytic
Differences between CML & Leukemoid Reaction
Peripheral B cell neoplasm
These are Chronic Lymphocytic Leukemia (CLL) & Small Lymphocytic Lymphoma (SLL) Identical in morphology, genoptype & phenotype Degree of PS lymphocytosis is different (higher in CLL) CLL Blood phase of neoplasm SLL Tissue phase of neoplasm Both can co exist in same patient
Myeloproliferative disorder
1. Chronic myeloid leukemia (CML)
2. Polycythaemia vera → Marrow fibrosis (cytopenias) → Acute leukemia
3. Essential thrombocytosis
4. Myelofibrosis.
Staging of CLL
Modified Rai staging (USA) Binet staging (Europe)o Low risk– Lymphocytosis in
the blood and marrow onlyo Intermediate risk –
Lymphocytosis with Lymphadenopathy / splenomegaly or hepatomegaly
o High risk– Lymphocytosis with Anemia or thrombocytopenia
o Stage A – Hb >/=10 g/dL, Platelets >/= 100 X 109/L, and fewer than 3 lymph node areas involved.
o Stage B – Hb and Platelet levels as in stage A and 3 or more lymph node areas involved.
o Stage C – Hb < 10 g/dL or Platelets < 100 X 109/L, or both
CML Leukemoid reactionMalignancyHepatosplenomegalyLarge spleenSlow courseTotal count IncreasedThrombocytosisLAP decreasedPh chromosomeBasophilia
Inflammatory lesionHepatomegalyMild spleen if presentShort durationIncreased but not muchPlatelets- NormalLAP increasedNo Ph chromosomeAntibiotics