2. better control, better life dr. ko ko
114
Better control,Better Life Ko Ko Taunggyi MMA 15.2.13 UM 2
-
Upload
ko-ko-mg -
Category
Health & Medicine
-
view
733 -
download
2
Transcript of 2. better control, better life dr. ko ko

Better control,Better LifeKo Ko Taunggyi MMA 15.2.13
UM 2

What new in 2013
BP 140/80 rather than 130/80Patient centre apporoach

Conclusions from recent trialsTight control
-early on has long term benefit on CVD
-later in the disease has little impact on CVD
-later in the disease may CVD risk
Severe Hypo may be dangerous
BP <120/80 no better than <140/80
Multifactorial management saves lives
Early combination Therapy
Therapeutic Inertia


Do we need better control?YES

Are we achieving good control?Are we achieving good control?Are we achieving good control?Are we achieving good control?

Are We getting better control?
• Why?
• Diet and exercise(Life long)
• Therapeutic Inertia (Target not achieved)
• Not using better drugs,better combination,sup-optimal dose
• Poor compliance,Poor monitoring
• Not giving drug according to pathogenesis
• Secondary drug failure---Need insulin
• Stress,Infection,MI,
• Steroid
No

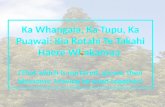
Treatment Strategies for Diabetes:Treatment Strategies for Diabetes:Are Patients Achieving Good Control?Are Patients Achieving Good Control?
Controlled
Uncontrolled
Hypertension Hyperlipidemia Diabetes
59%
41%
Harris MI et al. Diabetes Care. 2000;23:754
BP <140/90 mm Hg LDL-C <130 mg/dL A1C <7.0
59%
41%
58%
42%

Need SMBG 3 times per day in Type 1Type 2—depend on c ontrol,3,5,7 days/week
SMBG is associated with a better glycemic control in type 2 diabetes

- The pain: the ends of fingers are rich in nervous terminations (sensitivity +++)- Certain professions or certain leisures require a frequent use of the fingers:musicians (guitarists, pianists…), health workforces, plumbers, users of computer, hairdressers…
Obstacles with the self-monitoring at the end of the fingers

Self-monitoring Blood Glucose (SMBG) American Diabetes Association Recommendations
SMBG 3 or more times per day for type 1 diabetes
No specific frequency is recommended for type 2 diabetes
Standards of medical care in diabetes. Diabetes Care 2008

Measures to improve drug-Measures to improve drug-compliancecompliance
• Patient’s educationPatient’s education
• Promoting patient’s involvement in managementPromoting patient’s involvement in management
• Reducing pill load (Reducing pill load (long acting drugs eg.metformin long acting drugs eg.metformin XR,Gliclazide MR)XR,Gliclazide MR)
• Encouraging family involvement in patient’s careEncouraging family involvement in patient’s care

DRUGSDRUGS
• Correct DrugsCorrect Drugs
• Correct DosesCorrect Doses
• Correct TimingCorrect Timing
• Correct CombinationCorrect Combination
• ComplianceCompliance
• ?steroid?steroid

Correct DrugsCorrect Drugs• InsulinInsulin Type(1)DM/Type 2 DM with Stress/OHA FailureType(1)DM/Type 2 DM with Stress/OHA Failure
• TZD/MetforminTZD/Metformin Insulin ResistanceInsulin Resistance
• Postprandial HyperglycemiaPostprandial Hyperglycemia Glinites/Acarbose/voglibose/Soluble insulinGlinites/Acarbose/voglibose/Soluble insulin
• Insulin DeficiencyInsulin Deficiency SU/GliniteSU/Glinite
• Beta cell PreservationBeta cell Preservation TZDTZD

Correct Drugs
Insulin Resistance
Postprandial Hyperglycemic Insulin Deficiency
• Glinides
• Acarbose
• Voglibos
• Solube Insulin
• Thiazolidine diones
• Metformin
• Insulin Secretogogues
• Sulphonylurea Glinides

Correct CombinationCorrect Combination
• SU+MFMSU+MFM
• SU + AcarboseSU + Acarbose
• SU + ThiazolidinedionesSU + Thiazolidinediones
• MFM + ThiazolidinedionesMFM + Thiazolidinediones
• MFM + AcarboseMFM + Acarbose
• SU + MFM + AcarboseSU + MFM + Acarbose
• SU SU ++MFM + INSULATARDMFM + INSULATARD

• Clinical Inertia


901301802007Optimal Glycaemic Control
Is important to prevent death ,disability & complications of DM
-FBS -90-130mg% -2HPP -<180mg% -RBS -<200mg% -Bed time -110-150mg% -HbA1c -<7%

How Can we get good control of DM?How Can we get good control of DM?How Can we get good control of DM?How Can we get good control of DM?
?



Diabetes food pyramidDiabetes food pyramid
Cereals, whole Cereals, whole grains and starch: grains and starch:
6-11 servings6-11 servings
Fruits: 1- 2 Fruits: 1- 2 servingsservings
Vegetables:Vegetables:3-4 servings3-4 servings
Low fat milk and milkLow fat milk and milkproducts: 2-3 servingsproducts: 2-3 servings
Lean meat, fish, Lean meat, fish, poultry, pulses: poultry, pulses:
1-2 servings1-2 servings
Fats, oils, sugars, refined foods, Fats, oils, sugars, refined foods, fatty foods: eat sparinglyfatty foods: eat sparingly
Exercise for at least 30 minutes every dayExercise for at least 30 minutes every day
Therapeutic Lifestyle change
Fats, oils, sugars, refined foods, Fats, oils, sugars, refined foods, fatty foods: eat sparinglyfatty foods: eat sparingly
Vegetables:Vegetables:3-4 servings3-4 servings
Low fat milk and milkLow fat milk and milkproducts: 2-3 servingsproducts: 2-3 servings
Fats, oils, sugars, refined foods, Fats, oils, sugars, refined foods, fatty foods: eat sparinglyfatty foods: eat sparingly
Cereals, whole Cereals, whole grains and starch: grains and starch:
6-11 servings6-11 servings
Vegetables:Vegetables:3-4 servings3-4 servings
Low fat milk and milkLow fat milk and milkproducts: 2-3 servingsproducts: 2-3 servings
Fats, oils, sugars, refined foods, Fats, oils, sugars, refined foods, fatty foods: eat sparinglyfatty foods: eat sparingly

Plate modelPlate model
Vegetable
Milk/yoghurt
Fruit
Vegetable
Protein
Starch/cereal

Physical activityPhysical activity
RecommendationsRecommendations
• People with diabetes should be advised to perform People with diabetes should be advised to perform at at
least 150 min/weekleast 150 min/week of moderate-intensity aerobic of moderate-intensity aerobic
physical activity physical activity (50 – 70% of maximum heart rate).(50 – 70% of maximum heart rate). (A) (A)
• In the absence of contraindications, people with type 2 In the absence of contraindications, people with type 2
diabetes should be encouraged to perform resistance diabetes should be encouraged to perform resistance
training three times per week. (A)training three times per week. (A)
Standard of Medical Care in Diabetes 2010Standard of Medical Care in Diabetes 2010

Diabetes And Glycemic Control: A Rational Approach
• As low as possible
• As early as possible
• For as long as possible
• As safely as possible
• And as rationally as possible
Lifestyle +MET + TZD + SU
HbA1c < 6%

MedicationMedication RouteRoute YearYear Efficacy as monotherapy: % Efficacy as monotherapy: % in in HgbA1cHgbA1c
Insulin s.c. 1921 2.5
Sulfonylureas Oral 1946 1.5 -2
Glinides Oral 1997 1.0-1.5
Metformin Oral 1995 1.5-2
-glucosidase inhibitors OralOral 19951995 0.5-0.80.5-0.8
TZDs OralOral 19991999 0.8-1.00.8-1.0
GLP analogue s.c.s.c. 20052005 0.60.6
DPP-IV Inhibitors OralOral 20062006 0.5-0.80.5-0.8
Amylin analogue s.c.s.c. 20052005 0.60.6
Colesevelam OralOral 20082008 0.50.5
Bromocriptine mesylate OralOral 20092009 0.2-0.40.2-0.4
Type 2 Diabetes Medication ChoicesType 2 Diabetes Medication ChoicesExperience and PotencyExperience and Potency

Mechanisms of Action of Pharmacologic Mechanisms of Action of Pharmacologic Agents for Diabetes Agents for Diabetes
Improving Outcomes in Patients With Type 2 Diabetes Mellitus: Practical Solutions for Clinical ChallengesJames R. Gavin, III, MD, PhD; Mark W. Stolar, MD; Jeffrey S. Freeman, DO; Craig W. Spellman, DO, PhDJAOA • Vol 110 • No 5suppl6 • May 2010 • 2-14

Basic Steps in the Management of Type 2 DiabetesBasic Steps in the Management of Type 2 Diabetes
+ +
diet &exercise
Oral monotherapy
insulin
+
Oralcombination
Oral plusInsulin

• Fast onset of action
• To stimulate insulin secretion (including first phase)
• Decrease fasting and post prandial blood glucose
• Preservation of the beta cells
• Decrease insulin resistance
• Prevent complications
• Long duration of action (once daily administration)
An Ideal OHA should have…

• Control FPG & PPG effectively
• Lowest risk of hypoglycemia
• Should not produce hyperinsulinemia & weight gain
• Less drug interactions
An Ideal OHA should have…

No Single Class of Oral Antihyperglycemic Monotherapy Targets All Key Pathophysiologies
Alpha-Alpha-Glucosidase Glucosidase InhibitorsInhibitors1,21,2
MeglitinideMeglitinidess33 SUsSUs4,54,5 TZDsTZDs6,76,7
MetformiMetforminn88
DPP-4 DPP-4 InhibitorsInhibitors
Insulin deficiency Insulin resistance Excess hepatic glucose outputM
ajor
Pat
hoph
ysio
logi
es
1. Glyset [package insert]. New York, NY: Pfizer Inc; 2004. 2. Precose [package insert]. West Haven, Conn: Bayer; 2004.3. Prandin [package insert]. Princeton, NJ: Novo Nordisk; 2006. 4. Diabeta [package insert]. Bridgewater, NJ: Sanofi-Aventis; 2007.5. Glucotrol [package insert]. New York, NY: Pfizer Inc; 2006. 6. Actos [package insert]. Lincolnshire, Ill: Takeda Pharmaceuticals; 2004.7. Avandia [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2005.8. Glucophage [package insert]. Princeton, NJ: Bristol-Myers Squibb; 2004.
Intestinal glucose absorption

Early combination approach

When you saw a patient with DM• Glucose control?(glucose level)• Monitoring?• Compliance• Comobidities• Drugs• Stress –infection?MI,Pregnancy• Diet,exercise,body weight• Renal ,cardiac,liver• Economic status• Set the Target ----HbA1C,FBS,PPG

Glycaemic Indices : Present and Glycaemic Indices : Present and FutureFuture


HbA1C 7% in general HbA1C 7% in general
HbA1C Target <7% General
8% elderly6.5 to 7% in Young DM
HbA1C Target <7% General
8% elderly6.5 to 7% in Young DM


Effect SU and NSU Metformin TZA AGI
Mechanism Increase in insulin secretion
Decrease in HGO plus increases muscle sensitivity
Decrease in HGO plus increases muscle sensitivity
Decrease in glucose absorption
Decrease in FPG
60-70 mg% 60-70 mg% 35-40 mg% 20-30 mg%
Decrease in HbA
1.5-2.0% 1.5-2.0% 1.0-1.2% 0.7-1.0%
TG level No effect Decrease Decrease No effect
HDL level No effect Slight increase Increase No effect
LDL level No effect Decrease Increase No effect
Body weight Increase Decrease Increase No effect
Insulin level Increase Decrease Decrease No effect
Adverse effects
Hypoglycemia GI disturbances Anemia, hepatic GI disturbances

Initial Therapy with OHAs
Initial Add Add
Thin/normal Wt SU Metformin Insulin
Obese Metformin SU TZD/Insulin
Obese not tolerating MET TZD SU
MET contraindicated TZD SU
Severe IR Metformin TZD SU
Elderly SU Insulin
PPHG prominent MEG/AGI
PPHG prominent in Sec Failure
AGI/Exenatide

Combination Therapy with OHAs
• Drug combinations should be based on A. Therapeutic efficacy (“fire power”)B. Complementary mechanisms of actionC. Ancillary benefits (CVD risk factors)D. Safety and tolerabilityE. ? Compliance with multiple dosing regimens

Estimated Improvements with Combination Rx
Combination AIC% reduction FPG reduction
SU + MET 1.7% 65 mg/dl
SU + ROS 1.4% 60 mg/dl
SU + PIO 1.2% 50 mg/dl
SU + ACAR 1.3% 40 mg/dl
REP + MET 1.4% 40 mg/dl
MET + ROS/PIO 0.7-0.8% 40 mg/dl
INS + OHA Open to targets Open to targets
De Fronzo, NEJM 1995Horton, Diabetes Care 1998Coniff, Diabetes Care 1995Moses, Diabetes Care 1999Schneider, Diabetes 1999Egan, Diabetes 1999Fonseca, Diabetes 1999

Strategies for Antidiabetic Treatment
Oral Triple Combination Therapy plus Basal Insulin or plus GLP-1-Mimeticum
Oral Monotherapy
Oral Dual Combination Therapy
Oral Triple Combination Therapy
NPG, Glargine, Levemir
Metformin + Sulfonylureas + TZDs
Metformin + Sulfonylureas+DPP-4-Inhib.
Metformin
DPP-4 Inhibitors
Glinides
TZDs
Sulfonylureas
-Glucosidase-Inhibitors
Metformin + DPP-4-InhibitorsSulfonylureas + DPP-4-Inhibitors
Metformin + Sulfonylureas
Sulfonylureas + TZDsMetformin + TZDs
Exenatide, Liraglutide

Master Decision Path Master Decision Path Type 2 Diabetes Glycemic ControlType 2 Diabetes Glycemic Control
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan start monotherapystart monotherapy
Medical Nutrition TherapyMedical Nutrition Therapy&& Activity Plan Activity Plan start monotherapystart monotherapy
Oral combination treatment 2 drugsOral combination treatment 2 drugsIf target not reached after maximumIf target not reached after maximum
dose for 4 - 8 weeks - - start oral agentdose for 4 - 8 weeks - - start oral agent
Oral combination treatment 2 drugsOral combination treatment 2 drugsIf target not reached after maximumIf target not reached after maximum
dose for 4 - 8 weeks - - start oral agentdose for 4 - 8 weeks - - start oral agent
Insulin TherapyInsulin TherapyInsulin TherapyInsulin Therapy Oral Agent(s) + InsulinOral Agent(s) + InsulinOral Agent(s) + InsulinOral Agent(s) + Insulin
Oral Combination Rx 3 drugsOral Combination Rx 3 drugsIf target not reached after maximum If target not reached after maximum doses for 4 - 8 weeks -- start insulindoses for 4 - 8 weeks -- start insulin
Oral Combination Rx 3 drugsOral Combination Rx 3 drugsIf target not reached after maximum If target not reached after maximum doses for 4 - 8 weeks -- start insulindoses for 4 - 8 weeks -- start insulin
FPG < 200FPG < 200Casual < 250Casual < 250
FPG < 200FPG < 200Casual < 250Casual < 250
FPG 200-300FPG 200-300Casual 250-350Casual 250-350
FPG 200-300FPG 200-300Casual 250-350Casual 250-350
FPG > 350FPG > 350Casual > 400Casual > 400
FPG > 350FPG > 350Casual > 400Casual > 400
At Diagnosis(mg/dl)
Targets for Targets for Glycemic ControlGlycemic Control
HbA1c <7%HbA1c <7%
Targets for Targets for Glycemic ControlGlycemic Control
HbA1c <7%HbA1c <7%
FPG > 300-350FPG > 300-350Casual > 350-400Casual > 350-400
with severe symptomwith severe symptom
FPG > 300-350FPG > 300-350Casual > 350-400Casual > 350-400
with severe symptomwith severe symptom
KK/ESSENTIAL DRUG/3.4.11/tAUNGGHU

Practice GuidelinesPractice Guidelines

A1C 6.5 – 7.5%**
Monotherapy
MET +
GLP-1 or DPP4 1
TZD 2
Glinide or SU 5
TZD + GLP-1 or DPP4 1
MET +Colesevelam
AGI 3
2 - 3 Mos.***
2 - 3 Mos.***
2 - 3 Mos.***
Dual Therapy
MET +
GLP-1 or
DPP4 1+
TZD 2
Glinide or SU 4,7
A1C > 9.0%
No Symptoms
Drug Naive Under Treatment
INSULIN
± Other
Agent(s) 6
Symptoms
INSULIN
± Other
Agent(s) 6
INSULIN
± Other
Agent(s) 6
Triple Therapy
AACE/ACE Algorithm for Glycemic Control Committee
Cochairpersons:Helena W. Rodbard, MD, FACP, MACEPaul S. Jellinger, MD, MACE
Zachary T. Bloomgarden, MD, FACEJaime A. Davidson, MD, FACP, MACEDaniel Einhorn, MD, FACP, FACEAlan J. Garber, MD, PhD, FACEJames R. Gavin III, MD, PhDGeorge Grunberger, MD, FACP, FACEYehuda Handelsman, MD, FACP, FACEEdward S. Horton, MD, FACEHarold Lebovitz, MD, FACEPhilip Levy, MD, MACEEtie S. Moghissi, MD, FACP, FACEStanley S. Schwartz, MD, FACE
* May not be appropriate for all patients** For patients with diabetes and A1C < 6.5%,
pharmacologic Rx may be considered*** If A1C goal not achieved safely
† Preferred initial agent
1 DPP4 if PPG and FPG or GLP-1 if PPG
2 TZD if metabolic syndrome and/or nonalcoholic fatty liver disease (NAFLD)
3 AGI if PPG
4 Glinide if PPG or SU if FPG
5 Low-dose secretagogue recommended
6 a) Discontinue insulin secretagoguewith multidose insulin
b) Can use pramlintide with prandial insulin
7 Decrease secretagogue by 50% when added to GLP-1 or DPP-4
8 If A1C < 8.5%, combination Rx with agents that cause hypoglycemia should be used with caution
9 If A1C > 8.5%, in patients on Dual Therapy,insulin should be considered
MET +
GLP-1
or DPP4 1 ± SU 7
TZD 2
GLP-1
or DPP4 1 ± TZD 2
A1C 7.6 – 9.0%
Dual Therapy 8
2 - 3 Mos.***
2 - 3 Mos.***
Triple Therapy 9
INSULIN
± Other
Agent(s) 6
MET +
GLP-1 or DPP4 1
or TZD 2
SU or Glinide 4,5
MET +
GLP-1
or DPP4 1+ TZD 2
GLP-1
or DPP4 1 + SU 7
TZD 2
MET † DPP4 1 GLP-1 TZD 2 AGI 3
Available at www.aace.com/pub© AACE December 2009 Update. May not be reproduced in any form without express written permission from AACE

Mean Plasma Glucose Mean Plasma Glucose (mg/dl)(mg/dl)
A1C %A1C %
135135 66
170170 77
205205 88
240240 99
275275 1010
310310 1111
345345 1212
Correlation between A1c level & mean Correlation between A1c level & mean plasma glucose level on multiple testing plasma glucose level on multiple testing
over 2-3 months (Based on DCCT)over 2-3 months (Based on DCCT)
ADA 2010 Guidelines on Diagnosing diabetesADA 2010 Guidelines on Diagnosing diabetes

2. Juliana C. n. Chan; Vasanti Malik: Weiping Jia; et al. JAMA. 2009; 301 (20);2129-2140 (doi:10.1001/jama.2009.726)
SU – Sulphonylurea, SU – Sulphonylurea, MET – Metformin, MET – Metformin, TZD - ThiazolidinedioneTZD - Thiazolidinedione
HbA1c ≥6.5% after lifestyle interventionHbA1c ≥6.5% after lifestyle intervention
MET+ SUMET+ SU
HbA1c ≥7.5%HbA1c ≥7.5%
MetforminMetformin
HbA1c ≥6.5%HbA1c ≥6.5%
Insulin + MET + SUInsulin + MET + SU
HbA1c ≥7.5%HbA1c ≥7.5%
Increase InsulinIncrease InsulinDoseDose(or)(or)Insulin + PioglitazoneInsulin + Pioglitazone
SU (DIAMICRON MR)SU (DIAMICRON MR)- Not overweightNot overweight- MET not tolerated orMET not tolerated or is contraindicatedis contraindicated- Rapid therapeutic response- Rapid therapeutic response
HbA1c ≥6.5%HbA1c ≥6.5%
If MET is contraindicated or If MET is contraindicated or not toleratednot toleratedSU + DPP4 inhibitor or TZDSU + DPP4 inhibitor or TZD
If SU contraindicated If SU contraindicated or not toleratedor not toleratedMET + DPP4 inhibitorMET + DPP4 inhibitoror TZDor TZD
HbA1c ≥7.5%HbA1c ≥7.5%
Start InsulinStart Insulin
HbA1c ≥7.5%HbA1c ≥7.5%
If insulin is unacceptableIf insulin is unacceptableMET + SU + SitagliptinMET + SU + Sitagliptin
(or)(or)MET + SU + TZDMET + SU + TZD
(or)(or)MET + SU + ExenatideMET + SU + Exenatide
HbA1c ≥7.5%HbA1c ≥7.5%
NICE guideline for NICE guideline for Type 2 Diabetic Management, Type 2 Diabetic Management,
May 09May 09

1st line option in addition to lifestyle measures; start ONE OF
METMET SUSU (if intolerate of metformin or if weight loss/ osmotic symptoms)
1st line option in addition to lifestyle measures; start ONE OF
METMET SUSU (if intolerate of metformin or if weight loss/ osmotic symptoms)
2nd line options2nd line options
SUSU
(Usual approach)
SUSU
(Usual approach)
AlternativeAlternative
TZD or DPP-4 InhibitorTZD or DPP-4 Inhibitor
AlternativeAlternative
TZD or DPP-4 InhibitorTZD or DPP-4 Inhibitor
OralOral
MET/ SU + TZD (if no HF)MET/ SU + TZD (if no HF)
OralOral
MET/ SU + TZD (if no HF)MET/ SU + TZD (if no HF)
InjectableInjectable
MET/ SU + Insulin (before bed)MET/ SU + Insulin (before bed)(or)(or)
MET/ SU + GLP -1 agonistsMET/ SU + GLP -1 agonists
InjectableInjectable
MET/ SU + Insulin (before bed)MET/ SU + Insulin (before bed)(or)(or)
MET/ SU + GLP -1 agonistsMET/ SU + GLP -1 agonists
Review & if not reaching target move to 2nd line Review & if not reaching target move to 2nd line
Review & if not reaching target move to 3rd line Review & if not reaching target move to 3rd line
3rd line options3rd line options

ADA/EASD Consensus Algorithm for the Initiation and Adjustment of
Therapy Diabetes Care 2009; 32:193–203


1. Patient-Centered Approach“...providing care that is respectful of and responsive to individual patient preferences, needs, and values ensuring that patient values guide all clinical decisions.”
• Gauge patient’s preferred level of involvement.
• Explore, where possible, therapeutic choices.
• Utilize decision aids.
•Shared decision making – final decisions re: lifestyle choices ultimately lies with the patient.
Diabetes Care,Diabetes Care, Diabetologia. Diabetologia. 1919 April 2012 [Epub ahead of April 2012 [Epub ahead of print]print]
Diabetes Care,Diabetes Care, Diabetologia. Diabetologia. 1919 April 2012 [Epub ahead of April 2012 [Epub ahead of print]print]
ADA-EASD Position Statement: Management of Hyperglycemia in T2DM: A Patient-
Centered Approach

T2DM Anti-hyperglycemic Therapy: General Recommendations
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Avoid Hypoglycemia
Diabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Adapted Recommendations: When Goal is to Minimize CostsDiabetes Care, Diabetologia. 19 April 2012 [Epub ahead of print]

Patient Preference: EfficacyPatient Preference: Efficacy
metformin
sulfonylurea
TZD
glinide
DPP4 inhibitor
α -glucosidase inhibitors

Patient Preference: CostPatient Preference: Cost
metformin sulfonylurea
α-glucosidase
inhibitor
TZD
DPP4 inhibitor

Patient Preference: WeightPatient Preference: Weight
metforminDPP4
inhibitor
α -glucosidase inhibitor
TZD
sulfonylurea

Patient Preference: Patient Preference: Hypoglycemia AvoidanceHypoglycemia Avoidance
metformin
DPP4 inhibitor
TZD
α -glucosidase inhibitor
sulfonylurea
glinide


CASE 1
• 56 year male ,newly diagnosed DM,
• BMI 35
• RBS 350mg%
• BP 150/90
• Creatinine 100 mg%
• Total Cholesterol-250mg%
• ECG
Treatment?

Proplems
• DM,obese,hyperglycemia,IHD,increased cholesterol and TG,H/T
• Treatment• Metformin 500mg BD
• Gliclazide MR 60 mg 1 od
• Aspirin 1 od
• Atovastatin 10 mg
• Metoprolol 25 mg BD
• Ramipril 5 mg od
• Orlistat 120 mg 3 times
• Diet and exercise

Why I choose Metformin?

Metformin
• Obese
• Cardiac safe
• Reduced mortality
• First line drug in every guidelines
• Widely available
• Cheap-cost effective
• Powerful glucose lowering efffect
• 80% of Type 2 DM is due to Insulin Resistance
• Cannot use in advanced liver, renal and cardiac failure because of lactic acidosis

Metformin: Crucial Part of Metformin: Crucial Part of TherapyTherapy Metformin Effects on
Risk Factors
Hundal RS, Inzucchi SE. Metformin New Understandings, New Uses. Drugs 2003; 63(18): 1879-1894
Dose – 500 to 3000 mgCI - serum creatinine >1.5 mg%, Advanced Heart FailureSE - Reduce appetite, nausea, vomiting, diarrhoea

12 studies; ≥ 52 weeks; at least 1 CVD event
CVD outcomes: - fatal / non-fatal MI or stroke- PVD - other CVD death

Effect of Metformin on CVD Events

Why I choose Gliclazide (Diamicron MR 60 )
?

Rationale of Use of SU in T2DM
“Sulfonylureas are a rational choice to begin pharmacological intervention because almost all
patients with NIDDM [type 2 diabetes] are relatively insulin
deficient.”
ADA Consensus Statement 1996-1997

SulfonylureasSulfonylureas• Which ?
• When?
• Why?
1st line in underwt/normal wt type 2 patients
Along with insulin sensitizers: metformin or glitazones
Along with insulin to facilitate reduction/frequency of insulin dosing
1st line in underwt/normal wt type 2 patients
Along with insulin sensitizers: metformin or glitazones
Along with insulin to facilitate reduction/frequency of insulin dosing
All have same MOA
Require some viable β cell mass to work
Do not work in type 1 and after sec failure sets in type 2
Differential effects amongs SUs
All have same MOA
Require some viable β cell mass to work
Do not work in type 1 and after sec failure sets in type 2
Differential effects amongs SUs
• Can use in heart failure, renal failure• SE - Weight gain, hypoglycemia• Choice of SU – Newer SU to prevent cardiac side effect, prolong hypoglycemia

Sulfonylureas: How to Choose?
• Cardiac patients: Glimepiride/GLICLAZIDE
• Elderly patients: Glimepiride/GLICLAZIDE
• Economy: Glibenclamide
• Mild renal insufficiency: Glimepiride
• Severe Renal : Gliclazide and glipizide
• Require high potency: Glibenclamide
• Relatively younger patients: Glibenclamide

Glucose control therapy- Rationale

Mean HbA1c at final visit
Standard: 7.3%
Intensive: 6.5%
The ADVANCE Study
ADVANCE Collaborative Group. NEJM 2008

Combined primary outcomesMajor macro or microvascular event
Follow-up (months)
Cu
mu
lat i
ve i
nci
de
nce
(%
)
25
20
15
10
5
0
0 6 12 18 24 30 36 42 48 54 60 66
Standard
Intensive
Relative risk reduction10%: 95% CI: 2 to 18%
p=0.013
ADVANCE Collaborative Group. NEJM 2008

Any prevention of β cell dysfunction and failure (i.e. loss of β cell mass)
Initially correct glucotoxicity, lipotoxicity
some SU claims for reduction of ROS
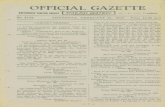
Some literature said :SU can even increase ROS ↑ apoptosis Esp in Glipizide,glimepride,glibenclamide ↓ROS *Gliclazide

Beta-cell apoptosis in islets: gliclazide vs glibenclamide
Islets pre-exposed for 5 days to - NG (5.5 mmol/L)- HG (alternating 5.5 & 16.7 mmol/L)
Groups differed significantly (p<0.01) by ANOVA: *p<0.05 vs NG;**p<0.005 vs HG and HG + glib after Bonferroni correction
S Del Guerra et al. Diabet Metab Res Rev 2007;23:234-8
HG +gliclazide
HG +glib
NG
HG

Effect of SU on MI Patients
Glipizide ,gliclazide and glimepiride are safer than glibenclamide b/c of more selective effect on pancreatic SU receptor



Relative risk of 1st-time MI according to OHA
0
0.5
1
1.5
2
2.5
C Glib Tolb Glicl Glimp
C
Glib
Tolb
Glicl
Glimp
(Johnsen SP, et al. Am J Ther. 2006;13:134-140.)
OR 2.08 [1.77-2.45]
OR 2.32 [1.48-2.64]
OR 1.37 [0.84-2.22]
OR 1.36 [0.93-1.99]

30-day post MI mortality according to 30-day post MI mortality according to OHAOHA
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Controls Glib/Tolb Glic/Glim
Controls
Glib/Tolb
Glic/Glim
(Johnsen SP, et al. Am J Ther. 2006;13:134-140.)
OR 1.29 [1.00-1.67]
OR 1.0[0.53-1.90]

Use of Sulfonylureas and mortality Use of Sulfonylureas and mortality after MI in diabetic patients:after MI in diabetic patients:
Danish nationwide population-based studyDanish nationwide population-based study
Thisted H, Thisted H, et alet al. EASD 2006. EASD 2006
old SHN
new SHN
1.08
0.81
0
0.4
0.8
1.2
old Sus new Sus
-25%


• Total mortality – Gliclazide - 67% (p<0.01), Total mortality – Gliclazide - 67% (p<0.01), Glimepiride - 40% Glimepiride - 40%
(p<0.01)(p<0.01)• CVD mortality – Gliclazide -71% (p<0.001)CVD mortality – Gliclazide -71% (p<0.001)

Cardiovascular death 253 289 12% (-4 to 26)
All deaths 498 533 7% (-6 to 17)
Non-cardiovascular death 245 244 0% (-20 to 16)
Number of patients with event
Intensive Standard(n=5,571) (n=5,569)
Relative riskreduction (95%CI)
FavoursIntensive
FavoursStandard
Hazard ratio0.5 1.0 2.0
ADVANCE study - trend to reduction in CV death with gliclazide MR based intensive control regimen
ADVANCE study - trend to reduction in CV death with gliclazide MR based intensive control regimen
ADVANCE Collaborative Group. NEJM 2008

ADVANCE is the only study to show a trend in favor of a reduction in cardiovascular death.
Control Group; Turnbull FM, Abraira C, Anderson RJ, et al. Diabetologia. 2009;52(11):2288-2298.

0.5 1.0 2.0
End stage kidney disease
Percent of patients with eventIntensive Standard(n=5,571) (n=5,569)
Relative riskreduction (95% CI)
FavoursIntensive
FavoursStandard
New microalbuminuria 23.7% 25.7%
Total renal events 26.9% 30.0%
9% (2 to 15)‡
11% (5 to 17)†
New macroalbuminuria 2.9% 4.1% 30% (15 to 43)†
New / worsening nephropathy 4.1% 5.2% 21% (7 to 34)***
Hazard ratio† P=<0.001
‡ P=0.02
*** P=0.006
*P=0.09
36% (-8 to 62)*0.4% 0.6%
ADVANCE Collaborative Group. NEJM 2008
ADVANCE: Reduction of Renal events
Less risk of dialysis, kidney transplantationand most of all death

Renal outcomes of the main morbidity-mortality trials in Renal outcomes of the main morbidity-mortality trials in diabetesdiabetes
1. UKPDS Group (33). Lancet. 1998;352(9131):837-853. 2. Duckworth W, Abraira C, Moritz T, et al; VADT Investigators. N Engl J Med. 2009;360(2):129-139. 3. Ismail-Beigi F, Craven T, Banerji MA, et al; ACCORD trial group. Lancet. 2010;376(9739):419-430. 4. Zoungas S, Lambers Heerspink HJ, Chalmers J, et al. Diabetologia. 2011;54(suppl 1):S23. 5. The ADVANCE Collaborative Group; Patel A, MacMahon S, Chalmers J, et al. N Engl J Med. 2008;358(24):2560-2572. * new or worsening nephropathy
*

ADVANCE Collaborative Group. EASD Congress 2010. Stockholm, Sweden. Oral communication
20 mg/l200 mg/lalbuminuria
Macroalbuminuria
Normal range of albuminuria
Majority of these
patients
*versus standard treatment group
Microalbuminuria
20% more patients regressed to normal range vs standard treatment
(P=0.0002)
ADVANCE: New renal results EASD 2010

ADVANCE is currently the only trial demonstrating protection of type 2 diabetic patients from end-stage kidney disease
Coca SG, Coca SG, Ismail-Beigi F, Haq N, Krumholz HM, Parikh CR. Arch Intern Med. 2012;172(10):761-769.

ACCORD2
ADVANCE3
Intensive Control
Standard Control
Pat
ien
ts e
xper
ien
cin
g a
t le
ast
on
e se
vere
hyp
og
lyce
mic
eve
nt
(%)
0
5
10
15
20
25
VADT1
2.7%2.7% 1.5%1.5%
16.2%16.2%
5.1%5.1%
21.2%21.2%
9.9%9.9%
P<0.001 P<0.001 P<0.001 P<0.001 HR=1.86(95% CI 1.40-2.40)
HR=1.86(95% CI 1.40-2.40)
% HbA1c at study end 7.36.46.9% change from baseline -0.2-1.7-2.5
8.4
-1.0
7.5
-0.6
6.5
-1.0
Comparison of severe hypoglycemia in morbimortality trials in diabetes
1. VADT Investigators. N Engl J Med. 2009;360:129-139. 2. Bonds DE, et al, BMJ. 2010;340:b4909. 3. ADVANCE Study Group. N Engl J Med. 2008;358(24):2560-2572.

• 1066 fasting patients
• Comparing incidence of hypos between SUs vs Sitagliptin
• Sponsored by MSD
Hypoglycemia in Ramadan: Sitagliptin vs SU
S. Al Sifri et al. Int J Clin Prac, Nov 2011;65,11: 1132–40

Hypoglycemia in Ramadan: Sitagliptin vs SU
S. Al Sifri et al. Int J Clin Prac, Nov 2011;65,11: 1132–40

0%
2%
4%
6%
8%
10%
Glimepiride Glibenclamide Gliclazide MR
(%)
of
pati
ents
wit
h >
one s
ym
pto
mati
c hypogly
cem
ia
Patient fasting Ramadan
2012 comparison
Patients’ Safety
9.1%9.1%
5.2%5.2%
1.8%1.8%

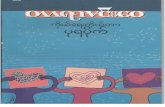
Hypoglycaemia with different Sulfonylureas
*<50 mg/dL. Tayek J. Diabetes Obes Metab. 2008;
10: 1128–1130.
0
5
10
15
20
25
30
Gliclazide0.85
Gliclazide0.85
Glipizide8.70
Glipizide8.70
Glimepiride0.86
Glimepiride0.86
Tolbutamide3.50
Tolbutamide3.50
Chlorpropamide
16.00
Chlorpropamide
16.00
Glyburide
16.00
Glyburide
16.00
Severe hypoglycemia*n/1000 person years
Severe hypoglycemia*n/1000 person years
Rela
tive R
isk (
%)
Rela
tive R
isk (
%)
SAFETY

Hypoglycemia in SU
OHARisk of
hypoglycemia
Glinide +
Gliclazide ++
Gliclazide MR +
Glimepride ++
Glibenclamide +++
All SU can give rise to hypoglycemia

HYPOGLYCEMIAHYPOGLYCEMIAGliclazide MR vs Glimepiride

Gliclazide MR
n=157
Gliclazide MR
n=226
Hypoglycaemia (blood glucose < 3.0 mmol/L) according to Creatinine Clearance (CCl)
Glimepiriden=25
Gliclazide MRn=17
0
6
12
18
24
50-80 ml/min
0
6
12
18
24
0
6
12
18
24
Num
ber o
f pati
ents
Glimepiriden=182
Glimepiriden=232
CCl > 80ml/minCCl < 50 ml/min
0% 12% 3.2% 12.6 % 4.4% 5.6%
(GUIDE-Study: Schernthaner G et al. Eur.J.Clin.Invest. 2004; 34:535-542)

50 year Male DM 12 yearson Metformin 500mg 2 TDSgliclazide MR 60 2 odPioglitazone 45 mg odHbA1C 8%,FBG-200,2hpp 350mg%Next Treatment?
CASE 2CASE 2

Uncontrolled DM
Check Diet Check Steroid Check Compliance Check Infection and Stress
3 drugs ,maximum dose for 3 monthsDrug Failure,Beta cell failure
Need INSULIN
3 drugs ,maximum dose for 3 monthsDrug Failure,Beta cell failure
Need INSULIN

Insulin Regimen for Type 2 Diabetes MellitusGuidelines for initiating insulin
0.15 units /kg /body wt /day
Chart G uidelines for Starting Insulin T herapy(Asia Pacific Type 2 D iabetes Policy group)
M orning 2 /3Pre-M ix-30/70
Evening 1 /3Pre-M ix-30/70
Pre-m ixed insulin 30/70
>30-40 iu --stopping OAD
T est FPG /Adjust 3-4 days
OAD + 10 iu NPH insulin (Bedtim e)

TWO basic INSULIN TWO basic INSULIN REGIMENSREGIMENS
SupplementarySupplementarySupplementarySupplementary SubstitutionSubstitutionSubstitutionSubstitution
(OHD +Bed time insulin)(OHD +Bed time insulin) ( No OHD +Only insulin)( No OHD +Only insulin)
Premixed/split mixedPremixed/split mixedPremixed/split mixedPremixed/split mixedBasal bolus insulinBasal bolus insulinBasal bolus insulinBasal bolus insulin

Insulin Regimen for Type 2 Diabetes Mellitus
Guidelines for Starting insulin therapy(Asia Pacific Type 2 Diabetes Policy group)
In normal person = 0.5 units /kg /BW /Day
Pre-mixed insulin 30/70Pre-mixed insulin 30/70
Morning 2/3
Pre-Mix 30/70
Morning 2/3
Pre-Mix 30/70
SubstitutionSubstitutionSubstitutionSubstitution
Evening 1/3
Pre-Mix 30/70
Evening 1/3
Pre-Mix 30/70

60
0
20
40
Insu
lin
PREMIX 30/70 PREMIX 30/706 AM 6 PM12 AM 12 PM
Insulin Regimen for Type 2 Diabetes Mellitus
PREMIXPREMIXPREMIXPREMIX

Basal Bolus Regimen Basal Bolus Regimen (Substitution)(Substitution)
106
• Mimics physiological insulin profile: starting dose- 40% daily dose as basal insulin (Intermediate-acting insulin- Insulatard or Humulin N) - 60% as short acting insulin (Actrapid or Humulin R) divided into
20% at breakfast 20% at lunch 20% at dinner
• Insulin dose adjusted if needed
• Requires highly motivated patients with constant monitoring

•Cardiac •Lipid Management•Smoking cessation •Vaccines •Transfer and
discharge
Cardiac •Lipid Management•Smoking cessation •Vaccines •Transfer and
discharge
Blood sugar control •Patient education •Nutrition counseling •Medication •Physical activity •Foot care •Retinopathy


Take Home Messages:Take Home Messages:Place of Sulfonylureas in T2DMPlace of Sulfonylureas in T2DM
• Are effective• Proven in OUTCOME trials Complications• ADVANCE (Gliclazide MR)
– weight gain NOT a given– hypoglycaemia can be minimised– effective irrespective of age, BMI or duration of DM
– renal failure / worsening of nephropathy• Not ALL Sulfonylureas are the same

CASE B
• 65 male with DM 10 years,IHD,Hypertension ,,Stroke
• HbAIC Target?• A. 7%• B.8%• C.6.5%

CASE c
• 45 female DM 3 year Thin ,RBS 230 ,creatinine 140,pedal oedema +
• Start with• A.Metformin• B.Metformin with Gliclazide MR• C.Gliclazide MR• D.Pioglitazone

CASE c
• 48 female DM 6 year ,RBS 350 ,• Start with• A.Metformin• B.Gliclazide MR• C.Metformin +Gliclazide MR

If RBS is >500mg%
•Poorly controlled DM•DKA•HHS(HONK)
•Admisssion is needed in patient with stressful conditions such as•Infection•Stroke•Myocardial infact.
•If there is no stressful condition
•Can be managed as OPD patient

Don't let the Don't let the situation situation confuse confuse you...you...

Thank you