2 3 Associations between Tooth Loss and Prognostic ...€¦ · 1 2 3 Associations between Tooth...
37
1 2 3 Associations between Tooth Loss and Prognostic Biomarkers and the Risk for 4 5 6 Cardiovascular Events in Patients with Stable Coronary Heart Disease 7 8 Short title: Vedin et al.: Tooth Loss and Biomarkers in CHD 9 10 11 12 Ola Vedin, MD, PhD 1,2 , Emil Hagström, MD, PhD 1,2 , Ollie Östlund, PhD 2 , Alvaro Avezum, 13 14 MD, PhD 3 , Andrzej Budaj, MD, PhD 4 , Marcus D. Flather, MBBS 5 , Robert A. Harrington, 15 16 MD 6 , Wolfgang Koenig, MD 7-9 , Joseph Soffer, MD 10 , Agneta Siegbahn, MD, PhD 2,11 , 17 18 Philippe Gabriel Steg, MD 12-15 , Ralph A. H. Stewart, MD 16 , Lars Wallentin, MD, PhD 1,2 , 19 20 Harvey D. White, MB, ChB, DSc 16 , Claes Held, MD, PhD 1,2 on behalf of the STABILITY 21 22 23 Investigators 24 25 26 27 1 Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden; 28 29 2 Uppsala Clinical Research Center (UCR), Uppsala University, Uppsala, Sweden; 3 Dante 30 31 Pazzanese Institute of Cardiology, São Paulo, Brazil; 4 Postgraduate Medical School, 32 33 Grochowski Hospital, Warsaw, Poland; 5 Norwich Medical School, University of East Anglia 34 35 and Norfolk and Norwich University Hospital, UK; 6 Department of Medicine, Stanford 36 37 University, Stanford, CA, USA; 7 Department of Internal Medicine II-Cardiology, University 38 39 40 of Ulm Medical Center, Ulm, Germany; 8 Deutsches Herzzentrum München, Technische 41 42 Universität München, Munich, Germany; 9 DZHK (German Centre for Cardiovascular 43 44 Research), partner site Munich Heart Alliance, Munich, Germany; 10 Metabolic Pathways and 45 46 Cardiovascular Therapeutic Area, GlaxoSmithKline, King of Prussia, PA, USA; 47 48 11 Department of Medical Sciences, Clinical Chemistry, Uppsala University, Uppsala, 49 50 Sweden; 12 INSERM-Unité 1148, Paris, France; 13 Assistance Publique-Hôpitaux de Paris, 51 52 Département Hospitalo-Universitaire FIRE, Hôpital Bichat, Paris, France; 14 Université Paris- 53 54 Diderot, Sorbonne-Paris Cité, Paris, France; 15 NHLI Imperial College, ICMS, Royal 55 56 57 58 1 59 60
Transcript of 2 3 Associations between Tooth Loss and Prognostic ...€¦ · 1 2 3 Associations between Tooth...

1
2 3
Associations between Tooth Loss and Prognostic Biomarkers and the Risk for 4 5
6 Cardiovascular Events in Patients with Stable Coronary Heart Disease 7
8 Short title: Vedin et al.: Tooth Loss and Biomarkers in CHD
9
10
11
12 Ola Vedin, MD, PhD1,2, Emil Hagström, MD, PhD1,2, Ollie Östlund, PhD2, Alvaro Avezum, 13
14 MD, PhD3, Andrzej Budaj, MD, PhD4, Marcus D. Flather, MBBS5, Robert A. Harrington, 15 16 MD6, Wolfgang Koenig, MD7-9, Joseph Soffer, MD10, Agneta Siegbahn, MD, PhD2,11, 17 18
Philippe Gabriel Steg, MD12-15, Ralph A. H. Stewart, MD16, Lars Wallentin, MD, PhD1,2, 19 20
Harvey D. White, MB, ChB, DSc16, Claes Held, MD, PhD1,2 on behalf of the STABILITY 21 22
23 Investigators
24
25
26
27 1Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden;
28
29 2Uppsala Clinical Research Center (UCR), Uppsala University, Uppsala, Sweden; 3Dante 30
31 Pazzanese Institute of Cardiology, São Paulo, Brazil; 4Postgraduate Medical School, 32
33 Grochowski Hospital, Warsaw, Poland; 5Norwich Medical School, University of East Anglia 34 35 and Norfolk and Norwich University Hospital, UK; 6Department of Medicine, Stanford 36 37
University, Stanford, CA, USA; 7Department of Internal Medicine II-Cardiology, University 38 39
40 of Ulm Medical Center, Ulm, Germany; 8Deutsches Herzzentrum München, Technische 41
42 Universität München, Munich, Germany; 9DZHK (German Centre for Cardiovascular 43
44 Research), partner site Munich Heart Alliance, Munich, Germany; 10Metabolic Pathways and 45
46 Cardiovascular Therapeutic Area, GlaxoSmithKline, King of Prussia, PA, USA; 47
48 11Department of Medical Sciences, Clinical Chemistry, Uppsala University, Uppsala, 49 50 Sweden; 12INSERM-Unité 1148, Paris, France; 13Assistance Publique-Hôpitaux de Paris, 51 52 Département Hospitalo-Universitaire FIRE, Hôpital Bichat, Paris, France; 14Université Paris- 53 54
Diderot, Sorbonne-Paris Cité, Paris, France; 15NHLI Imperial College, ICMS, Royal 55
56
57
58 1 59
60

61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
Brompton Hospital, London, UK; 16Green Lane Cardiovascular Service, Auckland City
Hospital and University of Auckland, Auckland, New Zealand
All authors take responsibility for all aspects of the reliability and freedom from bias of the
data presented and their discussed interpretation.
Address for correspondence: Dr. Ola Vedin; Uppsala Clinical Research Centre/MTC, Dag
Hammarskjölds väg 14B, 752 37, Uppsala, SWEDEN; Tel: + 46 18 6119500;
Fax: +46 18 515570; Email: [email protected]
ACKNOWLEDGEMENT OF GRANT SUPPORT
The STABILITY study was funded by GlaxoSmithKline. Roche Diagnostics, Rotkreuz,
Switzerland supported the research by providing GDF-15 assay free of charge.
CONFLICTS OF INTEREST
OV: institutional research grant from GlaxoSmithKline; expert committee member and lecture
fees from Boehringer Ingelheim, Fresenius Medicare, Novartis. EH: expert committee
member, lecture fees and institutional research grant from Sanofi; institutional research grant
and lecture fees from Amgen; institutional research grants from AstraZeneca,
GlaxoSmitKline; expert committee member for Ariad and Merck Sharp & Dohme. OÖ:
institutional research grants from GlaxoSmithKline. AA: personal fees from Boehringer
Ingelheim, Bristol-Myers Squibb, Pfizer, Bayer, AstraZeneca. AB: research
grants/investigator’s fees and honoraria for lectures from GlaxoSmithKline, AstraZeneca,
Bristol-Myers Squibb/Pfizer; research grants/investigator’s fees from Sanofi-Aventis,
Boehringer Ingelheim, Novartis, Eisai, Duke Research Institute. MDF: speaker's bureau and
2

121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
consultancy fees from AstraZeneca; grants from GlaxoSmithKline, Novartis, Menarini;
honoraria from Eli Lilly. RAH: research grants and consultant/advisory fees from Merck,
The Medicines Company; research grants from AstraZeneca, CSL Behrig, GlaxoSmithKline,
Portola, Regado, Sanofi; consultant/advisory fees from Amgen, Gilead, MyoKardia,
WebMD; stock ownership in Element Science, Scanadu, Signal Path. WK: lecture and
consultancy fees from Novartis, Amgen, AstraZeneca, Servier; lecture fees from Actavis;
consultancy fees from BioInvent, diaDexus, Cerenis, GlaxoSmithKline, The Medicines
Company, Genzyme, Pfizer, Merck Sharpe & Dohme; research grants from Roche
Diagnostics, Abbott, Singulex, Beckmann. JS: employee of and having stock ownership in
GlaxoSmithKline. AS: institutional research grants from AstraZeneca, Boehringer Ingelheim,
Bristol-Myers Squibb/Pfizer, GlaxoSmithKline. PGS: institutional research grants, honoraria
and non-financial support from Sanofi, Servier; honoraria and non-financial support from
AstraZeneca; honoraria from Amarin, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb,
Daiichi-Sankyo, Eli Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Medtronic, Janssen, The
Medicines Company, CSL-Behring, GlaxoSmithKline; stockholder in Aterovax. RAHS:
grants and non-financial support from GlaxoSmithKline. LW: institutional research grant,
consultancy and lecture fees, travel support and honoraria from GlaxoSmithKline;
institutional research grants, consultancy and lecture fees and travel support from
AstraZeneca, Bristol-Myers Squibb/Pfizer, Boehringer Ingelheim; institutional research grant
from Merck, Roche; consultancy fees from Abbott; holds two patents involving GDF-15.
HDW: research grants and advisory board for AstraZenecea; advisory board for The
Medicines Company; research grants from Sanofi Aventis, Eli Lilly and Company, National
Institute of Health, Merck Sharpe & Dohm, GlaxoSmithKline, Omthera Pharmaceuticals,
Pfizer New Zealand, Intarcia Therapeutics Inc, Elsai Inc., DalGen Products and Services,
Daiichi Sankyo Pharma Development. CH: institutional research grant and speaker’s bureau
3

181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
from AstraZeneca; institutional research grants from Bristol-Myers Squibb Merck & Co,
GlaxoSmithKline, Roche.
KEYWORDS
Tooth loss, periodontal disease, stable coronary heart disease, biomarkers, risk factors.
4

241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
ABSTRACT
BACKGROUND: Underlying mechanisms behind the hypothesized relationship between
periodontal disease (PD) and coronary heart disease (CHD) have been insufficiently
explored. We evaluated associations between self-reported tooth loss, a marker of PD, and
prognostic biomarkers in 15,456 (97%) patients with stable CHD in the global STABILITY
trial.
METHODS AND RESULTS: Baseline blood samples were obtained and patients reported
their number of teeth according to the following tooth loss levels: “26–32 (All)” [lowest
level], “20–25”, “15–19”, “1–14”, and “No Teeth” [highest level]. Linear and Cox regression
models assessed associations between tooth loss levels, biomarker levels and the relationship
between tooth loss levels and outcomes, respectively.
After multivariable adjustment, the relative biomarker increase between the
highest and the lowest tooth loss level was: high-sensitivity C-reactive protein 1.21 (95%
confidence interval, 1.14-1.29), interleukin 6 1.14 (1.10-1.18), lipoprotein-associated
phospholipase A2 activity 1.05 (1.03-1.06), growth differentiation factor 15 1.11 (1.08-1.14),
and N-terminal pro−B-type natriuretic peptide (NT-proBNP) 1.18 (1.11-1.25). No association
was detected for high-sensitivity troponin T 1.02 (0.98-1.05). Some attenuation of the
relationship between tooth loss and outcomes resulted from the addition of biomarkers to the
multivariable analysis, of which NT-proBNP had the biggest impact.
CONCLUSIONS: A graded and independent association between tooth loss and several
prognostic biomarkers was observed, suggesting that tooth loss and its underlying
mechanisms may be involved in multiple pathophysiological pathways also implicated in the
development and prognosis of CHD. The association between tooth loss and cardiovascular
5

301
302
303
304
305
306
307
308
309
310
death and stroke persisted despite comprehensive adjustment including prognostic
biomarkers.
Clinical trial registration: www.clinicaltrials.gov; NCT00799903
311 312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358 6 359 360

361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
1. INTRODUCTION
There is a growing body of evidence favouring an independent association between oral
health and coronary heart disease (CHD) [1–3]. We have recently reported an association
between tooth loss and cardiovascular (CV) outcomes, but not myocardial infarction (MI), in
a chronic CHD population [4]. In the literature, the hypothesized relationship between dental
disease and CV disease is often attributed to deleterious effects of periodontal disease (PD), a
highly prevalent chronic inflammatory condition ranging from early gingivitis to end-stage
tooth loss, on the atherosclerotic process but the specific mechanistic nature of such a
relationship remains elusive and debated [5].
Pathophysiological information on multiple aspects of etiology and progression
of CV disease is reflected by several biomarkers, many of which also have robust capabilities
of predicting prognosis [6–11]. Thus, associations between markers of PD, biomarkers and
CV outcomes could provide further insights about possible mechanisms connecting PD and
CV disease. However, such existing observations mainly stem from smaller populations and
are limited to selected inflammatory markers such as C-reactive protein and interleukin-6
[12,13], whereas reported associations with other important biomarkers are either scarce or
non-existent.
We evaluated associations between self-reported tooth loss, a marker of oral
disease and PD, and a wide range of prognostic biomarkers, including high-sensitivity
C-reactive protein (hs-CRP), interleukin-6 (IL-6), lipoprotein-associated phospholipase A2
activity (Lp-PLA2), growth differentiation factor 15 (GDF-15), high-sensitivity troponin T
(hs-Troponin T) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) in a large global
CHD population. Further, we assessed the influence of these biomarkers on the ability of
self-reported tooth loss to predict CV outcomes.
7

421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
2. METHODS
2.1. Study population
The STabilization of Atherosclerotic plaque By Initiation of darapLadIb TherapY
(STABILITY) study evaluated the efficacy of darapladib, an oral inhibitor of lipoprotein-
associated phospholipase A2 activity (Lp-PLA2) compared to placebo in addition to optimal
medical treatment in 15,828 participants from 39 countries with stable CHD, defined as prior
myocardial infarction (MI), prior coronary revascularization (percutaneous coronary
intervention or coronary artery bypass grafting), or multivessel CHD without
revascularization. At least one additional enrichment criterion was required: age ≥60 years;
diabetes mellitus requiring pharmacotherapy; high-density lipoprotein cholesterol
<1.03mmol/L; current or previous smoker defined as ≥5 cigarettes per day on average;
moderate renal dysfunction (estimated glomerular filtration rate ≥30 and <60mL/min/1.73 m2
or urine albumin:creatinine ratio ≥30mg albumin/g creatinine); or polyvascular disease (co-
existing disease in at least two arterial territories). Patients with an estimated glomerular
filtration rate <30mL/min/1.73 m2 were excluded [14]. After a median follow-up of 3.7 years,
no difference in major adverse cardiovascular events (MACE, i.e. first occurrence of CV
death, myocardial infarction or stroke) was observed for patients randomized to darapladib
compared to placebo [15]. The ethics committees of each participating country approved the
study and all patients provided written informed consent prior to inclusion. The STABILITY
trial was performed in accordance with the Declaration of Helsinki.
2.2. Data collection
At baseline, 15,456 (97%) patients reported their number of teeth according to the following
categories: “26–32 (All teeth)”, “20–25”, “15–19”, “1–14”, and “No Teeth”. For the purposes
8

481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
of this report, these categories are termed tooth loss levels with 26-32 teeth corresponding to
the lowest level and no teeth, the highest level.
Blood samples for routine laboratory tests and storage for later analyses were
obtained in all 15,456 patients at baseline and prognostic biomarker analyses were performed
in the majority of patients. Plasma aliquots were stored at -70°C until biochemical analysis.
All routine biochemical and hs-CRP analyses were performed at a central laboratory with
standardized methods (Quest Diagnostics Clinical Laboratories, Inc., Valencia, California,
USA). Plasma concentrations of hs-CRP were analyzed using a particle-enhanced
immunonephelometry assay, CardioPhase© hsCRP, Siemens Healthcare. Plasma
concentrations of high-sensitivity IL-6 were analyzed using an ELISA technique, R&D
Systems Inc., Minneapolis, MN, U.S.A. Lp-PLA2 activity was measured in an automated
enzyme assay system (PLAC® Test for Lp-PLA2 Activity, diaDexus, San Francisco, CA,
USA). The other biomarker assays were performed at the UCR Laboratory at Uppsala
University, Uppsala, Sweden, GDF-15 was measured with the GDF-15 precommercial assay
(Roche Diagnostics, Penzberg, Germany), composed of a monoclonal mouse antibody for
capture and a monoclonal mouse antibody fragment, [F(ab´)2], for detection in a sandwich
assay format. Detection was based on an electrochemiluminiscence immunoassay using a
ruthenium (II) complex label. Levels of hs-Troponin T and NT-proBNP were also determined
by electrochemiluminescence (Roche Diagnostics, Penzberg, Germany). The Cobas
Analytics e601 was used for the Roche immunoassays.
2.3. Statistical analysis
Baseline variables are presented as mean, standard deviation and percentages. Baseline
biomarker levels are presented as median and interquartile range. Baseline biomarker levels
by tooth loss level were compared using the Kruskal-Wallis tests.
9

541
542
543
544
545
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
To determine associations between tooth loss levels and biomarker levels, each
biomarker was modelled as a function of tooth loss level (five levels). All biomarkers were
analyzed on a log-transformed scale using linear models. Geometric mean ratios are presented
with 95% confidence intervals (CI) with the lowest tooth loss level (26-32 teeth) as
reference, and according to three adjustment models. Model 1 adjusted for randomized
treatment. Model 2 adjusted for Model 1 and prior MI, prior coronary revascularization,
multi-vessel CHD, age, sex, geographic region, diabetes mellitus, hypertension, renal
dysfunction, body mass index, smoking (current, former or never), systolic blood pressure
and polyvascular disease. Model 3 adjusted for Model 2 and estimated glomerular filtration
rate (according to The Chronic Kidney Disease Epidemiology Collaboration equation,
replacing significant renal dysfunction) [16], hemoglobin, white blood cells, low-density
lipoprotein cholesterol, high-density lipoprotein cholesterol and triglycerides. Cox
proportional hazards models were used to calculate hazard ratios for MACE, CV death and
stroke in relation to tooth loss levels, adjusting for biomarkers in addition to a previously
reported multivariable model [4], co-variables of which are also listed in Table 3. In these
models, all biomarkers except Lp-PLA2 activity were added after log-transformation. The
association between tooth loss and MI has previously been found to be absent in this cohort
and was not re-analysed in the present analysis.
A p-value <0.05 was considered statistically significant in all analyses. Analyses were
performed at the Uppsala Clinical Research Center, Uppsala, Sweden using SAS version 9.3
(SAS Institute, Inc., Cary, NC, USA). 587 588
589
590
591
592
593
594
595
596
597
598 10 599 600

601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
3. RESULTS
3.1. Baseline characteristics and associations with biomarkers
Patients with higher tooth loss levels were older, were more likely to be female and had a
greater CV risk factor burden, particularly a higher prevalence of smoking, diabetes mellitus,
hypertension and impaired renal function compared to those with lower tooth loss levels
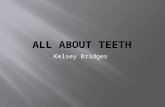
(Table 1). Patients with more tooth loss had progressively higher baseline levels of hs-CRP,
IL-6, Lp-PLA2 activity, GDF-15, hs-Troponin T and NT-proBNP (Table 2). As demonstrated
in Figure 1, higher tooth loss levels were associated with progressively greater relative
increases for all prognostic biomarkers in relation to the lowest tooth less level in Model 1.
After multivariable adjustment the association remained statistically significant for all
biomarkers, except for hs-Troponin T.
3.2. Tooth loss and outcomes
Table 3 demonstrates the association between a one-level increase in tooth loss and the risk
of MACE, CV death and stroke according to the three adjustment models after a median
follow-up of 3.7 years. The data up until Model 2 have been previously presented [4]
showing a relative risk increase of 1.06, 1.17 and 1.14 for MACE, CV death and for stroke,
respectively, for every one-level increase in tooth loss. The subsequent addition of
biomarkers, individually and in groups, only attenuated the results slightly. Nevertheless, the
addition of IL-6 and NT-proBNP rendered the association with MACE non-significant.
Despite adjustment for all biomarkers and other co-variables, the association between tooth
loss and CV death and stroke persisted. 652 653
654
655
656
657
658 11 659 660

661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719
720
4. DISCUSSION
We found that tooth loss, a marker of PD, was associated with higher levels of several CV
biomarkers indicating a potential relationship between tooth loss and several
pathophysiological mechanisms relevant to CV morbidity and mortality, including
inflammation, cellular integrity and myocardial dysfunction [6,7,9,17]. Adjustment for the
biomarkers somewhat attenuated the risk of adverse outcome, signalling a potential relevance
of the pathways they represent in the relationship between tooth loss and increased CV risk.
However, much of the risk increase remained, suggesting that other and presently unknown
mechanisms could be of importance, although confounding cannot be excluded.
The host-mediated inflammatory response to PD constitutes the most
commonly proposed mechanism linking oral disease with CHD and CV disease [18], mainly
based on evidence from smaller studies of moderate associations between various measures
of PD and elevation of inflammatory markers [12,13,19] and studies showing reductions of
CRP and IL-6 levels after PD treatment [20]. This is the first study to corroborate these
findings on a large scale in a global CHD population, including both upstream and
downstream inflammatory markers, with comprehensive adjustment and with tooth loss as
the exposure measure. Moreover, the association with Lp-PLA2 activity, previously only
assessed in small patient populations [21], could represent an additional alternative and
independent inflammatory link [22]. However, our findings could represent a challenge to the
inflammation hypothesis as the highest levels of inflammatory markers were observed among
the edentulous, who are most likely rid of oral substrates for inflammation. This could indicate
that intrinsic factors and not PD explain the inflammatory activity, for instance pro-
inflammatory genetic traits and epigenetic modifications common to both advanced PD and
CHD [23,24]. However, it is also conceivable that many years’ exposure to chronic oral
inflammation could instigate a secondary response in other locations, e.g.
12

721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
atherosclerosis in blood vessels, which in turn could promote or maintain an elevated
systemic inflammatory response.
Associations with biomarkers that reflect other than inflammatory processes
could suggest a relevance of alternative pathophysiological pathways in the tooth loss-CV
disease relationship. The association with GDF-15 for instance, has not been previously
described and could partly reflect a relationship between tooth loss and inflammation but also
other harmful mechanisms [17] of relevance to several cardiac afflictions, including MI and
heart failure, to which GDF-15 has been previously associated [25,26]. An independent
association with cardiac biomarkers could support a more specific link between tooth loss, its
antecedents, and cardiac pathology. This was previously investigated in a small study where
44 patients with clinical evidence of PD had higher levels of troponin and NT-proBNP
compared to controls, however these associations were unadjusted [27]. The association with
NT-proBNP in our study suggests a relationship between tooth loss and baseline cardiac
dysfunction that persisted after adjustment for traditional important heart failure determinants,
including prior MI, hypertension and diabetes. Cross-reactivity between periodontal
and myocardial antigens and chronic toll-like receptor activation have been
suggested as potential mechanisms linking chronic infection, e.g. PD, to heart failure [28].
Furthermore, a recent study demonstrated a greater burden of PD among patients with
advanced HF awaiting heart transplantation compared to controls without HF. However, the
observed differences were attenuated to non-significance after adjustment for markers of oral
hygiene, race and 25- hydroxyvitamin D levels [29]. Overall, data on the role of PD in the
pathophysiology of heart failure is largely lacking but the results from our present study and
other studies are interesting from a hypothesis generating perspective and should be explored
further.
Conversely to the association with NT-proBNP, tooth loss did not appear to be related to
13

781
782
783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
809
810
811
812
813
814
815
816
817
818
819
820
821
822
823
824
825
826
827
828
829
830
831
832
833
834
835
836
837
838
839
840
mechanisms generating elevated levels of troponin [30], which is an interesting finding
concurrent with the absent association between tooth loss and MI in this population [4].
In contrast to the absent MI association we recently reported a significant
association between tooth loss and MACE, CV death and stroke. Although the demonstrated
risk increases were relatively modest between adjacent tooth loss levels, they were more
substantial and likely to be clinically relevant when comparing patients with severe or
complete tooth loss to those with little or no tooth loss, particularly for CV death and stroke
[4]. In the present analysis, we added biomarkers to the previous outcomes model to assess
their influence on the demonstrated relationship between tooth loss and prognosis. Of the
inflammatory markers, IL-6, an upstream marker, attenuated the results the most and
eliminated the MACE association, supporting the hypothesis of inflammation as a mediator in
the PD-CV outcomes relationship further. However, for most of the biomarkers, resulting
attenuations were relatively small. The addition of NT-proBNP had the most pronounced
attenuating effect on the risk of adverse outcome, indicating a prognostic relevance of the
observed relationship between tooth loss and baseline myocardial dysfunction. The fact that a
significant portion of the increased risk for CV death and stroke persisted despite full
adjustment implies that alternate and presently unidentified pathways could be involved. The
observation of stronger associations for CV death and stroke compared to MI further suggests
that such pathways may be other than atherosclerotic and inflammatory, which is also
consistent with the associations to biomarkers reflecting other than primarily inflammatory
mechanisms, including GDF-15 and NT-proBNP. While the additional adjustment for
biomarkers could lead to underestimation of the true influence of tooth loss on prognosis by
removing effects of potential intermediate pathways, it also likely lessens the impact of
residual confounding, which is undoubtedly a considerable obstacle when assessing causality.
Nevertheless, as our findings are purely observational, causality cannot be inferred and they
14

841
842
843
844
845
846
847
848
849
850
851
852
853
854
855
856
857
858
859
860
861
862
863
864
865
866
867
868
869
870
871
872
873
874
875
876
877
878
879
880
881
882
883
884
885
886
887
888
889
890
891
892
893
894
895
896
897
898
899
900
may in fact be a product of long-term influence by causal factors common to both tooth loss
and CV disease.
From a prediction perspective and irrespective of causality, the observations
show promise for the potential use of self-reported tooth loss as a prognostication tool in
chronic CHD. Given its ability to predict several important outcomes combined with other
qualities, including its straightforward obtainability and affordability, the clinical predictive
utility of self-reported tooth loss should be explored further.
4.1. Study limitations
Self-reported tooth loss was the sole marker of PD in this analysis and the use of additional
exposure measures, e.g. clinical, could have provided better information regarding the
underlying etiology of tooth loss in the individual subjects. However, the literature generally
exhibits a lack of consistency in the use of PD definitions [5] and PD has been shown to be
the most common cause of tooth loss in older populations [31], although other causes, most
importantly caries, must be acknowledged. Moreover, self-reported tooth loss has been
validated against number of teeth on clinical examination with concurring results [32]. The
cross-sectional multivariable analysis of the association between tooth loss and biomarker
levels did not include markers of socioeconomic status, which could be important
confounders. Finally, the analysis does not specifically disclose the nature of the observed
associations, i.e. whether tooth loss and its underlying mechanisms increases CV risk or vice
versa, or if the two conditions are driven by a common etiology.
4.2. Conclusion
Self-reported tooth loss was associated with progressively higher levels of several prognostic
CV biomarkers suggesting possible involvement of tooth loss-generating mechanisms,
15

901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
929
930
931
932
933
934
935
936
937
938
939
940
941
942
943
944
945
946
947
948
949
950
951
952
953
954
955
956
957
958
959
960
including PD, in multiple pathophysiological pathways relevant to both CHD development
and prognosis. Adjustment for a wide range of CV risk factors, socioeconomic status and
biomarkers eliminated the association with MACE but the association with CV death and
stroke persisted.
ACKNOWLEDGMENTS
We thank all participants, study personnel and investigators in the STABILITY study. We
also thank Ebba Bergman, Susanna Thörnqvist, and Vendela Roos, Uppsala Clinical
Research Centre, for editorial support.
FUNDING
The STABILITY study was funded by GlaxoSmithKline. Roche Diagnostics, Rotkreuz,
Switzerland supported the research by providing GDF-15 assay free of charge.
16

961
962
963
964
965
966
967
968
969
970
971
972
973
974
975
976
977
978
979
980
981
982
983
984
985
986
987
988
989
990
991
992
993
994
995
996
997
998
999
1000
1001
1002
1003
1004
1005
1006
1007
1008
1009
1010
1011
1012
1013
1014
1015
1016
1017
1018
1019
1020
REFERENCES
[1] L.L. Humphrey, R. Fu, D.I. Buckley, M. Freeman, M. Helfand, Periodontal disease
and coronary heart disease incidence: a systematic review and meta-analysis, J. Gen.
Intern. Med. 23 (2008) 2079–86.
[2] A.A. Bahekar, S. Singh, S. Saha, J. Molnar, R. Arora, The prevalence and incidence of
coronary heart disease is significantly increased in periodontitis: a meta-analysis, Am.
Heart J. 154 (2007) 830–7.
[3] L. Rydén, K. Buhlin, E. Ekstrand, U. de Faire, A. Gustafsson, J. Holmer, B.
Kjellström, B. Lindahl, A. Norhammar, Å. Nygren, P. Näsman, N. Rathnayake, E.
Svenungsson, B. Klinge, Periodontitis Increases the Risk of a First Myocardial
Infarction: A Report From the PAROKRANK Study, Circulation. (2016).
[4] O. Vedin, E. Hagström, A. Budaj, S. Denchev, R.A. Harrington, W. Koenig, J. Soffer,
P. Sritara, A. Stebbins, R.H. Stewart, H.P. Swart, M. Viigimaa, D. Vinereanu, L.
Wallentin, H.D. White, C. Held, Tooth loss is independently associated with poor
outcomes in stable coronary heart disease, Eur. J. Prev. Cardiol. (2015)
2047487315621978-.
[5] P.B. Lockhart, A.F. Bolger, P.N. Papapanou, O. Osinbowale, M. Trevisan, M.E.
Levison, K. a Taubert, J.W. Newburger, H.L. Gornik, M.H. Gewitz, W.R. Wilson,
S.C. Smith, L.M. Baddour, Periodontal disease and atherosclerotic vascular disease:
does the evidence support an independent association?: a scientific statement from the
American Heart Association., Circulation. 125 (2012) 2520–44.
[6] S. Kaptoge, E. Di Angelantonio, G. Lowe, M.B. Pepys, S.G. Thompson, R. Collins, J.
Danesh, C-reactive protein concentration and risk of coronary heart disease, stroke,
17

1021
1022
1023
1024
1025
1026
1027
1028
1029
1030
1031
1032
1033
1034
1035
1036
1037
1038
1039
1040
1041
1042
1043
1044
1045
1046
1047
1048
1049
1050
1051
1052
1053
1054
1055
1056
1057
1058
1059
1060
1061
1062
1063
1064
1065
1066
1067
1068
1069
1070
1071
1072
1073
1074
1075
1076
1077
1078
1079
1080
and mortality: an individual participant meta-analysis., Lancet. 375 (2010) 132–40. [7]
J. Danesh, S. Kaptoge, A.G. Mann, N. Sarwar, A. Wood, S.B. Angleman, F. Wensley,
J.P.T. Higgins, L. Lennon, G. Eiriksdottir, A. Rumley, P.H. Whincup, G.D.O. Lowe,
V. Gudnason, Long-term interleukin-6 levels and subsequent risk of coronary heart
disease: Two new prospective studies and a systematic review, PLoS Med. 5 (2008)
0600–0610.
[8] A. Thompson, P. Gao, L. Orfei, S. Watson, E. Di Angelantonio, S. Kaptoge, C.
Ballantyne, C.P. Cannon, M. Criqui, M. Cushman, A. Hofman, C. Packard, S.G.
Thompson, R. Collins, J. Danesh, Lipoprotein-associated phospholipase A(2) and risk
of coronary disease, stroke, and mortality: collaborative analysis of 32 prospective
studies, Lancet. 375 (2010) 1536–1544.
[9] S. Blankenberg, M.J. McQueen, M. Smieja, J. Pogue, C. Balion, E. Lonn, H.J.
Rupprecht, C. Bickel, L. Tiret, F. Cambien, H. Gerstein, T. Münzel, S. Yusuf,
Comparative impact of multiple biomarkers and N-terminal pro-brain natriuretic
peptide in the context of conventional risk factors for the prediction of recurrent
cardiovascular events in the Heart Outcomes Prevention Evaluation (HOPE) study,
Circulation. 114 (2006) 201–208.
[10] T. Omland, J.A. de Lemos, M.S. Sabatine, C.A. Christophori, M. Rice, K.A. Jablonski,
S. Tjora, M.J. Domanski, B.J. Gersh, J.L. Rouleau, M.A. Pfeffer, E. Braunwald, A
Sensitive Cardiac Troponin T Assay in Stable Coronary Artery Disease, N Engl J Med.
361 (2009) 2538–2547.
[11] D.W. Schopfer, I.A. Ku, M. Regan, M.A. Whooley, Growth differentiation factor 15
and cardiovascular events in patients with stable ischemic heart disease (The Heart and
Soul Study), Am. Heart J. 167 (2014) 186–192.e1.
18

1081
1082
1083
1084
1085
1086
1087
1088
1089
1090
1091
1092
1093
1094
1095
1096
1097
1098
1099
1100
1101
1102
1103
1104
1105
1106
1107
1108
1109
1110
1111
1112
1113
1114
1115
1116
1117
1118
1119
1120
1121
1122
1123
1124
1125
1126
1127
1128
1129
1130
1131
1132
1133
1134
1135
1136
1137
1138
1139
1140
[12] S. Paraskevas, J.D. Huizinga, B.G. Loos, A systematic review and meta-analyses on
C-reactive protein in relation to periodontitis, J. Clin. Periodontol. 35 (2008) 277–90.
[13] B.G. Loos, J. Craandijk, F.J. Hoek, P.M. Wertheim-van Dillen, U. van der Velden,
Elevation of systemic markers related to cardiovascular diseases in the peripheral
blood of periodontitis patients, J. Periodontol. 71 (2000) 1528–34.
[14] H. White, C. Held, R. Stewart, D. Watson, R. Harrington, A. Budaj, P.G. Steg, C.P.
Cannon, S. Krug-Gourley, J. Wittes, T. Trivedi, E. Tarka, L. Wallentin, Study design
and rationale for the clinical outcomes of the STABILITY Trial (STabilization of
Atherosclerotic plaque By Initiation of darapLadIb TherapY) comparing darapladib
versus placebo in patients with coronary heart disease, Am. Heart J. 160 (2010) 655–
661.
[15] H.D. White, C. Held, R. Stewart, E. Tarka, R. Brown, R.Y. Davies, A. Budaj, R.A.
Harrington, P.G. Steg, D. Ardissino, P.W. Armstrong, A. Avezum, P.E. Aylward, A.
Bryce, H. Chen, M.-F. Chen, R. Corbalan, A.J. Dalby, N. Danchin, R.J. De Winter, S.
Denchev, R. Diaz, M. Elisaf, M.D. Flather, A.R. Goudev, C.B. Granger, L. Grinfeld,
J.S. Hochman, S. Husted, H.-S. Kim, W. Koenig, A. Linhart, E. Lonn, J. López-
Sendón, A.J. Manolis, E.R. Mohler, J.C. Nicolau, P. Pais, A. Parkhomenko, T.R.
Pedersen, D. Pella, M.A. Ramos-Corrales, M. Ruda, M. Sereg, S. Siddique, P.
Sinnaeve, P. Smith, P. Sritara, H.P. Swart, R.G. Sy, T. Teramoto, H.-F. Tse, D.
Watson, W.D. Weaver, R. Weiss, M. Viigimaa, D. Vinereanu, J. Zhu, C.P. Cannon, L.
Wallentin, Darapladib for Preventing Ischemic Events in Stable Coronary Heart
Disease, N. Engl. J. Med. 370 (2014).
[16] A.S. Levey, L.A. Stevens, C.H. Schmid, Y.L. Zhang, A.F. Castro, H.I. Feldman, J.W.
Kusek, P. Eggers, F. Van Lente, T. Greene, J. Coresh, A new equation to estimate
19

1141
1142
1143
1144
1145
1146
1147
1148
1149
1150
1151
1152
1153
1154
1155
1156
1157
1158
1159
1160
1161
1162
1163
1164
1165
1166
1167
1168
1169
1170
1171
1172
1173
1174
1175
1176
1177
1178
1179
1180
1181
1182
1183
1184
1185
1186
1187
1188
1189
1190
1191
1192
1193
1194
1195
1196
1197
1198
1199
1200
glomerular filtration rate, Ann. Intern. Med. 150 (2009) 604–12.
[17] T. Ago, J. Sadoshima, GDF15, a cardioprotective TGF-beta superfamily protein, Circ.
Res. 98 (2006) 294–7.
[18] M. Kebschull, R.T. Demmer, P.N. Papapanou, “Gum bug, leave my heart alone!”--
epidemiologic and mechanistic evidence linking periodontal infections and
atherosclerosis, J. Dent. Res. 89 (2010) 879–902.
[19] T. Nakajima, T. Honda, H. Domon, T. Okui, K. Kajita, H. Ito, N. Takahashi, T.
Maekawa, K. Tabeta, K. Yamazaki, Periodontitis-associated up-regulation of systemic
inflammatory mediator level may increase the risk of coronary heart disease, J.
Periodontal Res. 45 (2010) 116–22.
[20] M.S. Tonetti, F. D’Aiuto, L. Nibali, A. Donald, C. Storry, M. Parkar, J. Suvan, A.D.
Hingorani, P. Vallance, J. Deanfield, Treatment of periodontitis and endothelial
function, N. Engl. J. Med. 356 (2007) 911–20.
[21] W. Lösche, G.J. Marshal, D.A. Apatzidou, S. Krause, T. Kocher, D.F. Kinane,
Lipoprotein-associated phospholipase A2 and plasma lipids in patients with destructive
periodontal disease, J. Clin. Periodontol. 32 (2005) 640–4.
[22] F.D. Kolodgie, A.P. Burke, K.S. Skorija, E. Ladich, R. Kutys, A.T. Makuria, R.
Virmani, Lipoprotein-associated phospholipase A2 protein expression in the natural
progression of human coronary atherosclerosis, Arterioscler. Thromb. Vasc. Biol. 26
(2006) 2523–2529.
[23] A.S. Schaefer, G.M. Richter, B. Groessner-Schreiber, B. Noack, M. Nothnagel, N.-E.
El Mokhtari, B.G. Loos, S. Jepsen, S. Schreiber, Identification of a shared genetic
susceptibility locus for coronary heart disease and periodontitis, PLoS Genet. 5 (2009)
e1000378.
20

1201
1202
1203
1204
1205
1206
1207
1208
1209
1210
1211
1212
1213
1214
1215
1216
1217
1218
1219
1220
1221
1222
1223
1224
1225
1226
1227
1228
1229
1230
1231
1232
1233
1234
1235
1236
1237
1238
1239
1240
1241
1242
1243
1244
1245
1246
1247
1248
1249
1250
1251
1252
1253
1254
1255
1256
1257
1258
1259
1260
[24] S. Schulz, U.D. Immel, L. Just, H.-G. Schaller, C. Gläser, S. Reichert, Epigenetic
characteristics in inflammatory candidate genes in aggressive periodontitis, Hum.
Immunol. 77 (2016) 71–75.
[25] K.C. Wollert, T. Kempf, T. Peter, S. Olofsson, S. James, N. Johnston, B. Lindahl, R.
Horn-Wichmann, G. Brabant, M.L. Simoons, P.W. Armstrong, R.M. Califf, H.
Drexler, L. Wallentin, Prognostic value of growth-differentiation factor-15 in patients
with non-ST-elevation acute coronary syndrome, Circulation. 115 (2007) 962–971.
[26] T. Kempf, S. von Haehling, T. Peter, T. Allhoff, M. Cicoira, W. Doehner, P.
Ponikowski, G.S. Filippatos, P. Rozentryt, H. Drexler, S.D. Anker, K.C. Wollert,
Prognostic Utility of Growth Differentiation Factor-15 in Patients With Chronic Heart
Failure, J. Am. Coll. Cardiol. 50 (2007) 1054–1060.
[27] W.Y. Loo, Y. Yue, C. Fan, L. Bai, Y. Dou, M. Wang, H. Liang, M.N.B. Cheung,
L.W.C. Chow, J. Li, Y. Tian, L. Qing, Comparing serum levels of cardiac biomarkers
in cancer patients receiving chemotherapy and subjects with chronic periodontitis, J.
Transl. Med. 10 Suppl 1 (2012) S5.
[28] Z. Kaya, C. Leib, H. a. Katus, Autoantibodies in heart failure and cardiac dysfunction,
Circ. Res. 110 (2012) 145–158.
[29] U. Schulze-Späte, I. Mizani, K.R. Salaverry, J. Chang, C. Wu, M. Jones, P.J. Kennel,
D.L. Brunjes, T.-H. Choo, T.S. Kato, D. Mancini, J. Grbic, P.C. Schulze, Periodontitis
and bone metabolism in patients with advanced heart failure and after heart
transplantation, ESC Hear. Fail. 4 (2017) 169–177.
[30] H.D. White, Pathobiology of troponin elevations: do elevations occur with myocardial
ischemia as well as necrosis?, J. Am. Coll. Cardiol. 57 (2011) 2406–8.
[31] P.S. Hull, H. V Worthington, V. Clerehugh, R. Tsirba, R.M. Davies, J.E. Clarkson,
21

1261
1262
1263
1264
1265
1266
1267
1268
1269
1270
1271
1272
1273
1274
1275
1276
1277
1278
1279
1280
1281
1282
1283
1284
1285
1286
1287
1288
1289
1290
1291
1292
1293
1294
1295
1296
1297
1298
1299
1300
1301
1302
1303
1304
1305
1306
1307
1308
1309
1310
1311
1312
1313
1314
1315
1316
1317
1318
1319
1320
The reasons for tooth extractions in adults and their validation, J. Dent. 25 (1997) 233–
7.
[32] W. Pitiphat, R.I. Garcia, C.W. Douglass, K.J. Joshipura, Validation of self-reported
oral health measures, J. Public Health Dent. 62 (2002) 122–8.
22

1321
1322
1323
1324
1325
1326
1327
1328
1329
1330
1331
1332
1333
1334
1335
1336
1337
1338
1339
1340
1341
1342
1343
1344
1345
1346
1347
1348
1349
1350
1351
1352
1353
1354
1355
1356
1357
1358
1359
1360
1361
1362
1363
1364
1365
1366
1367
1368
1369
1370
1371
1372
1373
1374
1375
1376
1377
1378
1379
1380
FIGURE LEGENDS
Figure 1 legend. Geometric mean ratio of biomarker levels according to tooth loss level with
the lowest tooth loss level (26-32 teeth) as reference. Included biomarkers are high-sensitivity
C-reactive protein (hs-CRP), interleukin 6 (IL-6), lipoprotein-associated phospholipase A2
activity (Lp-PLA2), growth differentiation factor 15 (GDF-15), high-sensitivity troponin T
(hs-Troponin T), and N-terminal pro−B-type natriuretic peptide (NT-proBNP).
Adjusted for darapladib treatment, prior MI, prior revascularization, multi-vessel coronary
heart disease, age, sex, geographic region, diabetes mellitus, hypertension, body mass index,
smoking (current, former or never), systolic blood pressure, polyvascular disease, estimated
glomerular filtration rate, Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI),
hemoglobin, white blood cells, low-density lipoprotein (LDL) cholesterol, high-density
lipoprotein (HDL) cholesterol, and triglycerides.
23

1381
1382
1383
1384
1385
1386
1387
1388
1389
1390
1391
1392
1393
TABLES
Table 1. Demographic and baseline characteristics by tooth loss level
Tooth Loss Level
Lowest Highest
1394
1395
1396
Characteristics All Patients
(n=15456)
26-32 Teeth
(n=3310)
20-25 Teeth
(n=3680)
15-19 Teeth
(n=2167)
1-14 Teeth
(n=3785)
No Teeth
(n=2514)
p-value
1397
1398
1399
1400
Age, years 64.4 +/- 9.3 61.1 +/- 10.0 63.2 +/- 9.2 64.5 +/- 9.0 65.8 +/- 8.5 68.2 +/- 8.0 <0.0001
Sex <0.0001
1401
1402
1403
1404
1405
1406
1407
1408
1409
1410
1411
1412
1413
1414 1415
Female 18.6 13.7 15.1 19.9 21.6 24.9
Smoking status <0.0001
Never smoked 30.8 38.9 32.9 30.0 27.2 22.9
Former smoker 51.2 46.2 50.5 50.4 53.2 56.6
Current smoker 18.0 14.9 16.5 19.6 19.6 20.5
Diabetes 38.8 35.4 37.4 36.6 41.3 43.0 <0.0001
Chronic kidney disease 30.2 23.9 27.3 31.4 32.7 38.0 <0.0001
Prior MI 58.9 55.3 58.1 59.9 62.4 58.7 <0.0001
1416
1417 Prior revascularization 74.9 76.9 75.6 73.5 72.8 75.7 0.0078
1418 1419 24

1420 1421

1422
1423
1442
1424 Education
1425
1426 None 1427
3.6
3.5
2.6
3.1
3.8
5.2
<0.0001
1428 1-8 years 1429
19.2 14.7 15.5 16.8 23.1 27.1
1430 9-12 years 30.7 26.1 29.0 32.5 32.8 34.4
1431
1432 Trade school 18.2 14.5 17.8 19.7 20.7 18.6
1433
1434 College/university 28.3 41.2 35.0 27.9 19.7 14.7
1435
1436 Alcohol consumption/week
<0.0001
1437 None
1438
54.8 53.6 50.1 51.8 57.1 62.1
1439 1-4 drinks 1440
18.9 19.1 20.3 20.2 18.5 16.4
1441 5-14 drinks 15.8 16.3 18.0 16.4 14.9 12.9
1443 ≥15 drinks 10.5 11.0 11.6 11.7 9.5 8.7
1444
1445 Leisure time physical activity 0.0002
1446
1447 Sedentary 32.8 33.3 30.0 30.4 35.1 35.0
1448
1449 Mild exercise 44.6 44.4 45.1 45.5 43.0 45.4
1450 Moderate exercise 22.6 22.3 25.0 24.1 21.8 19.6 1451 1452 LDL cholesterol, mmol/L 2.2 ± 0.9 2.1 ± 0.8 2.2 ± 0.8 2.2 ± 0.8 2.3 ± 0.9 2.2 ± 0.8 <0.0001 1453 1454 HDL cholesterol, mmol/L 1.2 ± 0.3 1.2 ± 0.3 1.2 ± 0.3 1.2 ± 0.3 1.2 ± 0.3 1.2 ± 0.3 <0.0001
1455 1456 eGFR, mL/min/1.73m2
75.8 ± 18.1 78.7 ± 17.8 77.2 ± 17.8 75.3 ± 18.1 74.5 ± 18.2 72.3 ± 18.0 <0.0001
1457 1458 1459 1460 25 1461 1462

1463
1464
1465
1466
1467
1468
1469
1470
1471
1472
1473
1474
1475
1476
1477
1478
1479
1480
1481
1482
1483
1484
1485
1486
1487
1488
1489
1490
1491
1492
1493
1494
1495
1496
1497
1498
1499
1500
1501
1502
1503
Systolic BP, mmHg 131.5 ± 16.6 128.8 ± 16.0 131.3 ± 16.1 131.6 ± 17.0 132.6 ± 16.4 133.4 ± 17.3 <0.0001
Diastolic BP, mmHg 78.7 ± 10.4 78.4 ± 10.2 78.7 ± 10.3 78.8 ± 10.4 79.2 ± 10.3 78.2 ± 10.6 <0.0001
BMI, kg/m2 28.9 ± 5.0 28.5 ± 5.0 29.1 ± 5.1 28.9 ± 5.0 29.0 ± 4.8 29.3 ± 5.2 <0.0001
Data are percentages and mean ± SD
MI, myocardial infarction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; eGFR, estimated glomerular filtration
rate; BP, blood pressure; BMI, body mass index
26

1504
1505
1506
1507
1508
1509 1510
Table 2. Baseline biomarker levels by tooth loss level
Tooth Loss Level
1511 Lowest Highest
1512
1513
1514
1515
1516
1517
Biomarker All Patients
(n=15456)
hs-CRP, mg/L
26-32 Teeth
(n=3310)
20-25 Teeth
(n=3680)
15-19 Teeth
(n=2167)
1-14 Teeth
(n=3785)
No Teeth
(n=2514)
p-value
1518
1519
1520
1521
1522
1523
1524
1525
1526
1527
1528
1529
1530
n
Median (Q1; Q3)
IL-6, pg/mL
n
Median (Q1; Q3)
14076
1.3 (0.6; 3.1)
14263
2.1 (1.4; 3.2)
2977
1.1 (0.5; 2.6)
2974
1.8 (1.3; 2.8)
3389
1.3 (0.6; 2.8)
3400
2.0 (1.4; 2.9)
1972
1.4 (0.7; 3.0)
2007
2.1 (1.4; 3.3)
3467
1.5 (0.7; 3.3)
3545
2.2 (1.5; 3.4)
2271
1.7 (0.8; 4.0) < 0.0001
2337
2.4 (1.7; 3.8) < 0.0001
1531
1532
Lp-PLA2, μmol/min/L
1533
1534
1535
1536
1537
1538
1539
1540
1541
1542
1543
1544
n
Median
(Q1; Q3)
GDF-15,
pg/mL
14155
173 (143; 204)
2960
171 (140; 203)
3366
172 (143; 202)
1984
172 (143; 204)

27
3520
173 (144; 206)
2325
176 (148;
207)
< 0.0001

1545
1546
1547
1548
1549
1550
1557
1558
1559
1560
1561
1562
1563
1564
1565
1566
n
Median (Q1; Q3)
Median (Q1; Q3)
NT-proBNP, ng/L
14237
1254 (915; 1827)
9.3 (6.2; 14.2)
2974
1120 (824; 1615)
8.5 (5.7; 12.7)
3385
1181 (876; 1709)
8.7 (6.0; 13.3)
2011
1225 (907; 1792)
9.4 (6.2; 14.3)
3528
1314 (962; 1888)
9.8 (6.4; 14.8)
2339
1486 (1069; 2172)
10.4 (6.9; 16.2)
< 0.0001
< 0.0001
1567
1568
1569
1570
1571
1572
1573
1574
1575
1576
1577
1578
1579
1580
1581
1582
1583
1584
1585
n 14181 2960 3392 2003 3505 2321
Median (Q1; Q3) 173 (83; 377) 132 (64; 278) 152 (72; 328) 177 (88; 392) 202 (97; 450) 224 (108; 493) < 0.0001
1551 1552 1553 hs-Troponin T, ng/L
1554 1555 n 14147 2952 3386 1996 3497 2316
1556

hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; Lp-PLA2
, lipoprotein-associated phospholipase A2
activity; hs-Troponin T, high-sensitivity troponin
T;
NT-
proB
NP,
N-
termi
nal
pro−
B-
type
natri
uretic peptide; GDF-15, growth differentiation factor 15
28

1586
1587
1588
1589
1590
1591
1592
Table 3. Risk of major adverse cardiac events (MACE), cardiovascular (CV) death and stroke for one increase in tooth loss level after
adjustment for risk factors and biomarkers
1593
1594
1595
1596
1597
1598
Adjustment MACE
(HR [95% CI])
p-value CV death
(HR [95% CI])
p-value Stroke
(HR [95% CI])
p-value
1599
1600
1601
1602
1603
1604
1605
1606
1607
1608
1609
1610
1611
1612
1613
1614
1615
1616
1617
1618
1619
1620
1621
1622
1623
1624
1625
1626 Model 1
Model 2
Model 2 + hs-
CRP
Model 2 + IL-6
1.16
(1.12-
1.20)
1.06
(1.02-
1.10)
1.05
(1.00-
1.09)
1.04
(1.00-
1.09)
<0.0001
0.0041
0.0404
0.0581
1.30 (1.23-1.37)
<0.0001
1.17 (1.10-1.24)
<0.0001
1.16 (1.08-1.23)
<0.0001
1.14 (1.07-1.22)
<0.0001
1.22 (1.23-1.32)
1.14 (1.04-1.25)
1.14 (1.04-1.23)
1.12 (1.02-1.23)
Model 2 + Lp-PLA2 1.06 (1.01-1.10) 0.0091 1.16 (1.09-1.24) <0.0001 1.14 (1.04-1.26) 0.0057
Model 2 + GDF-15
1.05 (1.01-1.10)
0.0273
1.15 (1.08-1.23) <0.0001
1.12 (1.02-1.23)
0.0188
29

<
0
.
0
0
0
1
0
.
0
0
6
2
0
.
0
0
6
5
0
.
0
2
2
4

1627
1628
1629
1630
1631
1632
1633
1634
1635
1636
1637
1638
1639
1640
1641
1642
Model 2 + hs-Troponin T, NT-proBNP
1.03 (0.99-1.07)
0.1893
1.12 (1.05-1.19)
0.0006
1.10 (1.00-1.21)
0.0488
1643
1644
1645
1646
1647
HR, hazard ratio; CI, confidence interval; Model 1 is adjusted for study treatment only. Model 2 is adjusted for model 1 and age, systolic blood pressure, diastolic blood
pressure, BMI, LDL cholesterol, HDL cholesterol, history of diabetes, prior MI, sex, smoking status, waist hip ratio, eGFR, family history of coronary heart disease, alcohol
consumption, years of education, level of physical activity and country income level. Abbreviations as in Tables 1 and 2.
Model 2 + hs-CRP, IL-6, Lp-PLA2, 1.04 (0.99-1.08) 0.0973 1.13 (1.05-1.20) 0.0005 1.13 (1.03-1.25) 0.0146
GDF-15
Model 2 + hs-CRP, IL-6, Lp-PLA2,
GDF-15, hs-Troponin T, NT-proBNP
1.02 (0.98-1.07)
0.3335
1.10 (1.03-1.18)
0.0046
1.11 (1.00-1.23)
0.0406
1648 1649
1650
1651
1652
1653
1654
1655
1656
1657
1658
1659
1660
1661
1662
1663
1664
1665 30 1666 1667

1668
1669
1670
1671
1672
1673
1674
1675
1676
1677
1678
1679
1680
1681
1682
1683
1684
1685
1686
1687
1688
1689
1690
1691
1692
1693
1694
1695
1696
1697
1698
1699
1700
1701
1702
1703
1704
1705
1706
1707
1708
1709
1710
1711
1712
1713
1714
1715
1716
1717
1718
1719
1720
1721
1722
1723
1724
1725 31
1726

Biomarker
and tooth Mean (95%
loss level ratio Cl) P-value
0.9 0.95 1 1.05 1.1 1.15 1.2 1.25 1.3
• •
•

Author Agreement Form – International Journal of Cardiology
Manuscript Title: Associations between Tooth Loss and Prognostic Biomarkers and the Risk for
Cardiovascular Events in Patients with Stable Coronary Heart Disease
List of all Authors: Ola Vedin, MD, PhD; Emil Hagström, MD, PhD; Ollie Östlund, PhD; Alvaro
Avezum, MD, PhD; Andrzej Budaj, MD, PhD; Marcus D. Flather, MBBS; Robert A.
Harrington, MD; Wolfgang Koenig, MD; Joseph Soffer, MD; Agneta Siegbahn, MD, PhD;
Philippe Gabriel Steg, MD; Ralph A. H. Stewart, MD; Lars Wallentin, MD, PhD; Harvey D.
White, MB, ChB, DSc; Claes Held, MD, PhD.
Corresponding Author: Ola Vedin
This statement is to certify that all authors have seen and approved the manuscript
being submitted, have contributed significantly to the work, attest to the validity and legitimacy
of the data and its interpretation, and agree to its submission to the International Journal of
Cardiology.
We attest that the article is the Authors' original work, has not received prior publication and is
not under consideration for publication elsewhere. We adhere to the statement of ethical
publishing as appears in the International of Cardiology (citable as: Shewan LG, Rosano GMC,
Henein MY, Coats AJS. A statement on ethical standards in publishing scientific articles in the
International Journal of Cardiology family of journals. Int. J. Cardiol. 170 (2014) 253-254
DOI:10.1016/j.ijcard.2013.11).
On behalf of all Co-Authors, the corresponding Author shall bear full responsibility for the
submission. Any changes to the list of authors, including changes in order, additions or removals
will require the submission of a new author agreement form approved and signed by all the
original and added submitting authors.
All authors are requested to disclose any actual or potential conflict of interest including any
financial, personal or other relationships with other people or organizations within three years of
beginning the submitted work that could inappropriately influence, or be perceived to influence,
their work. If there are no conflicts of interest, the COI should read: “The authors report no
relationships that could be construed as a conflict of interest”.