1SFQBSFE &/5 - Prepared 4 ENT · 2018. 8. 19. · Salivary Stones ... This is a collection of pus...
12
Transcript of 1SFQBSFE &/5 - Prepared 4 ENT · 2018. 8. 19. · Salivary Stones ... This is a collection of pus...

Contributors
Vik Veer Naveed Kara Anja Lieder Adam Shakir Natasha Thandrayen 1st Edition 2011
Resource materials to accompany course
Prepared 4 ENTA Practical One Day Course


2 | P a g e
CONTENTS
Preface ........................................................................................................................................ 6
PREPARED FOR OTOLOGY ..................................................................................................................... .7
Taking a History in Otology........................................................................................................... 8
Examination of the Ear ................................................................................................................. 9
Tests for Vertigo ........................................................................................................................ 12
Romberg’s test .................................................................................................................................................. 12
Unterberger’s Stepping test ............................................................................................................................. 13
Dix-Hallpike’s test ............................................................................................................................................. 13
Tuning Fork Tests ....................................................................................................................... 14
Weber’s Test ..................................................................................................................................................... 14
Rinne’s Test ....................................................................................................................................................... 15
Infections of the Ear ................................................................................................................... 16
Otitis Externa .................................................................................................................................................... 16
Otitis Media ...................................................................................................................................................... 18
Mastoiditis ........................................................................................................................................................ 21
Hearing Loss .............................................................................................................................. 22
Causes of Sensorineural hearing loss ............................................................................................................... 22
Presbyacusis ..................................................................................................................................................... 23
Traumatic injury ................................................................................................................................................ 24
Acoustic Trauma ............................................................................................................................................... 24
Ototoxic drugs .................................................................................................................................................. 25
Infections of the Inner ear ................................................................................................................................ 25
Cerebellopontine Angle Tumours ..................................................................................................................... 25
Ménière's disease ............................................................................................................................................. 26
Idiopathic Sudden Sensorineural Hearing loss ................................................................................................. 27
Causes of Conductive hearing loss ................................................................................................................... 27
Wax / Cerumen ................................................................................................................................................. 28

3 | P a g e
Tympanic Perforation ....................................................................................................................................... 29
Cholesteatoma .................................................................................................................................................. 30
Otosclerosis ...................................................................................................................................................... 31
Vertigo ...................................................................................................................................... 32
Causes of Vertigo .............................................................................................................................................. 32
BPPV - Benign Paroxysmal Positional Vertigo ................................................................................................... 32
Epley’s manoeuvre ........................................................................................................................................... 34
Ménière's disease ............................................................................................................................................. 35
Labyrinthitis ...................................................................................................................................................... 36
Acoustic Neuroma ............................................................................................................................................ 37
Facial Nerve Palsy ...................................................................................................................... 38
Causes of Facial Nerve Palsy ............................................................................................................................. 38
Classification Systems for Facial Nerve Palsy.................................................................................................... 39
PREPARED FOR RHINOLOGY ....................................................................................................... 40
Anatomy of the nasal cavity ....................................................................................................... 41
CT Imaging of the Paranasal Sinuses ................................................................................................................ 43
Examination of the Nose ............................................................................................................ 44
The Blocked Nose....................................................................................................................... 46
Causes of a blocked nose .................................................................................................................................. 46
Allergic Rhinitis ................................................................................................................................................. 46
Nasal Polyps ...................................................................................................................................................... 51
Rhinosinusitis .................................................................................................................................................... 54
Peri-Orbital Cellulitis ......................................................................................................................................... 56
Potts Puffy Tumour ........................................................................................................................................... 57
Structural Blockage of the Nose ....................................................................................................................... 58
Neoplasms of the Nose ..................................................................................................................................... 60
Epistaxis .................................................................................................................................... 62
Nasal Fractures .......................................................................................................................... 69
Foreign Bodies in the Nose ......................................................................................................... 70

4 | P a g e
PREPARED FOR HEAD & NECK .................................................................................................... 71
Taking a Head & Neck History ..................................................................................................... 72
Examination of the Head & Neck ................................................................................................ 74
Examination of a Neck lump ............................................................................................................................. 76
Examination of Ulcers ....................................................................................................................................... 77
Examination of the Thyroid .............................................................................................................................. 78
Flexible Nasendoscopy ..................................................................................................................................... 80
Diseases of the Tonsils ............................................................................................................... 83
Acute Tonsillitis ................................................................................................................................................. 83
Quinsy / Peritonsillar Abscess ........................................................................................................................... 86
Draining a Quinsy .............................................................................................................................................. 88
Deep Neck Space Infections ............................................................................................................................. 92
Tonsillectomy .................................................................................................................................................... 94
Post-Tonsillectomy / Adenoidectomy Haemorrhage ....................................................................................... 96
Oesophageal Food Bolus and Foreign Bodies .............................................................................. 98
Oesophageal Food Bolus .................................................................................................................................. 98
Foreign Bodies in Children .............................................................................................................................. 100
Foreign Bodies in adults.................................................................................................................................. 100
Diseases Affecting the Larynx ................................................................................................... 101
Causes of Hoarseness ..................................................................................................................................... 101
Laryngitis ......................................................................................................................................................... 101
Epiglottitis ....................................................................................................................................................... 102
Reflux Laryngitis .............................................................................................................................................. 103
Vocal Cord Palsy ............................................................................................................................................. 104
Muscle Tension Dysphonia ............................................................................................................................. 105
Reinke’s Oedema (Polypoid degeneration) .................................................................................................... 105
Neoplasms of the Vocal Cords ........................................................................................................................ 105
Benign Lesions of the Vocal Cords .................................................................................................................. 106
Other Causes of Hoarseness ........................................................................................................................... 107

5 | P a g e
Stridor & Stertor ...................................................................................................................... 108
The Snoring Patient .................................................................................................................. 111
Salivary Gland Diseases ............................................................................................................ 113
Salivary Gland Enlargement ............................................................................................................................ 114
Infections of the Salivary Glands .................................................................................................................... 114
Salivary Stones ................................................................................................................................................ 115
Salivary Gland Tumours .................................................................................................................................. 115
Dysphagia ................................................................................................................................ 117
Head & Neck Cancer ................................................................................................................. 118
Risk Factors ..................................................................................................................................................... 118
Staging ............................................................................................................................................................ 119
Anatomy ......................................................................................................................................................... 120
TNM 7th
Edition ............................................................................................................................................... 121
Investigations .................................................................................................................................................. 127
Treatment ....................................................................................................................................................... 127
Consenting Guidelines .............................................................................................................. 134
Tonsillectomy .................................................................................................................................................. 134
Adenoidectomy .............................................................................................................................................. 135
Myringotomy and insertion of Grommets ...................................................................................................... 136
Other Ear Operations ...................................................................................................................................... 137
FESS – Functional Endoscopic Sinus Surgery +/- Polypectomy ....................................................................... 138
Septoplasty / Rhinoplasty ............................................................................................................................... 138
Panendoscopy +/- Biopsy ............................................................................................................................... 139
APPENDIX
SIGN Guidance – Management of sore throat and indications for tonsillectomy
NICE Guidance – Surgical management of otitis media with effusion in children
SIGN Guidance – Diagnosis and management of childhood otitis media in primary care
SIGN Guidance – Management of obstructive sleep apnoea / hypopnoea syndrome (OSAHS)
SIGN Guidance – Diagnosis and management of head and neck cancer
BSACI guidelines for the management of allergic and non-allergic rhinitis
BSACI guidelines for the management of rhinosinusitis and nasal polyposis

86 | P a g e
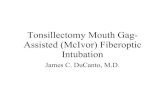
QUINSY / PERITONSILLAR ABSCESS
This is a collection of pus between the tonsil and the lateral wall of the oropharynx. It continues to expand in size to give the characteristic symptoms and signs of a quinsy.
Clinical photograph of a left quinsy
A quinsy is a recognised complication of partially or untreated bacterial tonsillitis. While tonsillitis is
predominantly a disease of childhood, developing a quinsy is rarely seen in very young children, and young
adults are most commonly affected by these abscesses. It can involve aerobic and/or anaerobic flora.
Streptococci, Staphylococci and Haemophilus species are most commonly responsible.
CLINICAL FEATURES
Patients will present similarly to those who have tonsillitis, with odynophagia, pyrexia and malaise. However,
they will also have a definite muffled change to their voice (often described as a ‘hot potato’ voice). They may
also have lateralising symptoms, such as pain worse on one particular side, and unilateral otalgia. They will
nearly always present with trismus (this is an inability to open the mouth, caused by irritation of the pterygoid
muscles resulting in spasm). You would be question the diagnosis of quinsy in anyone who did not have the
classic triad of a hot potato voice, unilateral pain and trismus.
Clinical findings are that of a swollen oedematous soft palate, predominantly one-sided, and a displaced uvula
away from the side of the abscess. Patients will often have an infected appearance of both tonsils, and
examination can be limited due to the restricted mouth opening.

87 | P a g e
DIFFERENTIAL DIAGNOSES
A quinsy can be confused with several other conditions, and one must always bear in mind the triad of
symptoms described above.
Severe tonsillitis – is nearly always bilateral and does not normally result in a muffled voice
(particularly after adequate analgesia).
Peritonsillitis – this is normally considered a pre-cursor to quinsy, and you will see spreading
inflammation to the anterior tonsillar pillar or palatoglossal fold (see image under examination of the
head and neck). Peritonsillitis does not result in the swelling or displacement of the uvula as seen in
quinsy.
Haematological malignancies – lymphomas may present acutely this way, particularly in children.
Typically the child presents with the appearance of a florid quinsy, but seems too well with it. They
are not septic, and do not have as much pain as one would suspect with such a large mass in the
throat. This should be considered an emergency and the child should be immediately referred to the
Paediatric team. An LDH level will be very high, and a chest x-ray should be performed (mediastinal

88 | P a g e
mass may be seen which could complicate any attempt at intubation). The child should be reviewed
frequently as they may develop airway compromise very quickly.
Oropharyngeal malignancies – squamous cell carcinoma is the most common malignancy of this area,
and patients (who are typically older than your average quinsy patient) may present with what
appears to be a quinsy. These masses however tend to be less painful and the patient is not normally
septic (unless secondarily infected).
MANAGEMENT
As with all abscesses, a quinsy needs to be drained. This is performed under local anaesthetic by the bedside
or in a treatment room, and involves either aspiration with a large gauge needle or incision with a scalpel.
Firstly you should treat the patient as you would for any tonsillitis, with adequate analgesia, fluids and
antibiotics. Most hospitals would give Benzylpenicillin 1.2g QDS IV +/- Metronidazole 500mg TDS IV (as most
of these abscesses have been found to contain anaerobic bacteria within them).
Draining a quinsy is difficult, so do not try this without being guided by an experienced ENT doctor first. A
description of the technique is provided below.
DRAINING A QUINSY
There are two schools of thought on the management of a quinsy, being either to aspirate only or to incise and
drain. Either way, the underlying principle remains; “if there is pus about, let it out”.
There is increasing evidence that a quinsy can be managed safely on an outpatient basis, by draining it and
discharging the patient after a short period of observation. However common practice in the UK is still to
drain the abscess and to admit the patient to hospital overnight for intravenous antibiotics.
There is no single correct method for draining a quinsy. The patient will inevitably be apprehensive, and will
require constant reassurance. It should be done cautiously with a steady hand, and if inexperienced, never
unsupervised.
To prepare the patient they should first have xylocaine sprayed into their mouth to provide some limited
analgesia. Then inject the surface mucosa overlying the quinsy with 1-2% lignocaine using the smallest needle
you can find (orange or dental needles). You will notice the mucosa blanching as you inject, and you should
give it a few minutes to take effect. Although this achieves the best analgesia, some clinicians will merely
spray topical anaesthetic instead, the argument being that it spares the patient two needles. If incising, then
local anaesthetic should be injected.
A good headlight should be used to allow two functional hands, and an assistant is advisable for patient
reassurance and as an extra pair of hands. A tongue depressor will also be required, in addition to a syringe
and needle, or a scalpel and some sticky tape (which will be used to prevent the needle from going in too
deep). Suction should also be available as sometimes an incision will release a large quantity of pus, hence
posing a risk of aspiration. Patients should always warned beforehand that there will often be quite a lot of
blood and pus in the mouth during this procedure.

89 | P a g e
Regardless of which method is used, even if no pus is obtained, then the patient should be admitted and
treated as quinsy, pending further senior review.
The role of swabs taken for microbiology is unclear, and practice varies from unit to unit. Most patients have
usually improved and been discharged home before the results are available, however they can prove useful in
those cases that fail to respond to treatment.
ASPIRATION TECHNIQUE
Whilst the anaesthetic is working, get the largest cannula you can find (brown) and remove everything (plastic
cannula, and other attachments), leaving only the needle, which can now be attached to a 10ml or 20ml
syringe. Alternatively, a standard large gauge needle may be used.
Over this needle wrap sticky tape around until only the top 1.5 – 2cm of the needle tip is exposed. This will
prevent you from going too deep with your needle (see the picture steps below on the left). A different
method to make a safe quinsy aspiration kit would be to cut off the cannula protector at the appropriate level
and leave it on so that you may use this to stop the needle from diving in too deep (see picture below right).
Using a headlight and a tongue depressor, insert the needle deep into the quinsy where it looks the most
prominent, staying as horizontal and straight as possible. Classically you place the needle at the point where a
vertical line up from the molar teeth and a horizontal line parallel to the base of the uvula meet. A diagram is
describing this is on the next page.
The abscess can sometimes recur, and it is not uncommon for the procedure to be repeated the next day.

90 | P a g e
Unfortunately photographing a
quinsy is extremely difficult due
to trismus. These images
should you give you an idea of
where to aspirate a quinsy.
The horizontal black lines (A)
show the level of the base of
the uvula, and the almost
vertical lines (B) show the line
drawn from the teeth.
The point at which these two
lines meet is the place where to
aspirate first - see central white
star indicating the aspiration
point.
To inexperienced eyes, it may
look far too high in the palate to
aspirate, and you may feel you
should aim a bit lower to get
the most ‘bulgy’ point.
Remember that you are trying
to drain pus from around the
tonsil, and placing the needle
too low will mean that you will
be entering the tonsil, rather
than the abscess.
The other points (left and right
white stars), show the second
and third possible points where
you could try and aspirate.
These should be used if you
were unsuccessful on your first
attempt.
A
A
B
B

91 | P a g e
INCISION TECHNIQUE
This is roughly the same technique, however this time a scalpel is used. A disposable blade should be used,
and all of the blade except the distal 1.5cm should be covered with sticky tape. The incision should be made in
the same location as the aspiration points shown above, but the three white stars are joined together in a
single incision.
You should use a ‘sawing’ motion with the blade rather than slicing across, this makes the incision more
controlled and you are less likely to cause unnecessary trauma. With properly delivered local anaesthetic, this
is normally painless.
After you have incised, normally quite a lot of pus pours into the mouth. Allow the patient to spit this out. A
lot blood will also be produced, this is normal, and will stop in a minute or so.
Once the patient and the bleeding has settled, you should try and break down the loculations within the
abscess by opening the cavity with a Tilley’s dressing forceps. Compared to the actual incision, this stretching
of the cavity is rather painful, and the patient should be warned of this.
Once the procedure has been performed, the patient will still be spitting out blood, and can be given either
diluted hydrogen peroxide or another antiseptic mouthwash to gargle. The bleeding will completely settle
with time. Often when a large quantity of pus has been obtained, the patient will report an immediate
improvement in their symptoms, presumably as a result of the release of the pressure.
Appearance of oral cavity after draining a right sided quinsy with an incision





![The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://static.fdocuments.in/doc/165x107/5e9dc57b42f70b199c246bec/the-technique-of-tonsil-enucleation-semantic-scholar-dec-1936-technique.jpg)



![Smoking, Periodontitis and Vascular Disease -Collaboration ... · disease sufferers showed periodontal infection and 80% showed tonsil enlargement or pus attachment [9]. Allen believed](https://static.fdocuments.in/doc/165x107/5f37c4354da5c84b564be66e/smoking-periodontitis-and-vascular-disease-collaboration-disease-sufferers.jpg)