
1H nuclear magnetic resonance based metabolic …chemistry.skku.edu/dhryu/publication/2011-...
7
1 H nuclear magnetic resonance based metabolic urinary profiling of patients with ischemic heart failure Seok-Min Kang a , Jong-Chul Park b,c , Min-Jeong Shin d , Hyeran Lee d , Jaewon Oh a , Do Hyun Ryu e , Geum-Sook Hwang b,c, ⁎, Ji Hyung Chung a,f, ⁎ a Cardiology Division, Yonsei Cardiovascular Hospital and Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul 120-752, Republic of Korea b Korea Basic Science Institute, Seoul 136-713, Republic of Korea c Graduate School of Analytical Science and Technology, Chungnam National University, Daejeon 305-764, Republic of Korea d Department of Food and Nutrition, Korea University, Seoul 136-703, Republic of Korea e Department of Chemistry, Sungkyunkwan University, Gyeonggi-do 440-746, Republic of Korea f Severance Integrative Research Institute for Cerebral and Cardiovascular Disease, Yonsei University Health System, Seoul 120-752, Republic of Korea abstract article info Article history: Received 31 August 2010 Received in revised form 24 November 2010 Accepted 30 November 2010 Available online 15 December 2010 Keywords: Heart failure Citric acid cycle Metabolism Methylmalonic acid Phenylacetylglycine Objectives: We sought to identify metabolic pathways characterizing human heart failure (HF) using 1 NMR based urinary metabolomic analysis in conjunction with multivariate statistics. Design and methods: Patients with systolic HF of ischemic origin (n = 15) and healthy controls (n = 20) participated in this study. Patients with type 2 diabetes mellitus were excluded. Results: The results showed that the urine of the HF patients had higher levels of metabolites for acetate (p b 0.05) and acetone (p b 0.01) compared to the healthy controls. In addition, there was a perturbation in methylmalonate metabolism as shown by increased urinary levels of methylmalonic acid (p b 0.001) in the HF patients. HF patients also had increased urinary levels of cytosine (p b 0.01) and phenylacetylglycine (p b 0.01) and decreased 1-methylnicotinamide (p b 0.05) compared to healthy controls. Conclusions: TCA cycle metabolites and fatty acid metabolism were modified in the HF patients, indicating altered energy metabolism. Moreover, perturbations of metabolism in nucleotide and methylma- lonate were observed. © 2010 The Canadian Society of Clinical Chemists. Published by Elsevier Inc. All rights reserved. Introduction The prevalence of heart failure (HF) is increasing despite major therapeutic advances, and HF is now considered as one of the major public health burdens both in developed and developing countries [1]. It has been well known that HF is, in part, the result of the progression of chronic hypertension as well as acute and chronic cardiac injury including myocardial infarction [2]. Considering the aging of popula- tions and the pandemic of cardiovascular disease (CVD) all over the world, the importance of its prevention is magnified [3]. As such, the prevention of HF is an urgent public health need with national and global implications that deserves high priority. The etiology of HF is very complex and correspondingly numerous studies have aimed to define the underlying pathophysiology of HF using recent advances in the systems biology approach, which enables the diagnosis of disease state [4]. Metabolomic analysis is a com- prehensive tool for simultaneously measuring the amounts of metab- olites of multiple metabolic pathways. Global metabolite profiles of complex samples are used to identify potential biomarkers, which can provide new and unexpected insights into biological processes [5]. Indeed, emerging data have been reported by studies of metabolomics to define perturbations in metabolic pathways and networks in human disease including diabetes [6], cancer [7], and neurodegenerative disorders [8,9]. In the application of metabolomics to cardiovascular pathway discoveries, there have been several attempts to identify metabolic phenotypes differentiating the meta- bolic pathways of myocardial ischemia [10], planned myocardial infarction [11], and a reperfusion model [12]. However, metabolic investigations into urinary metabolites in human heart failure have not been performed. In the present study, we attempted to determine the differences in urinary metabolites of HF patients versus healthy controls. Clinical Biochemistry 44 (2011) 293–299 Abbreviations: NMR, nuclear magnetic resonance; TCA, tricarboxylic acid; BNP, B-type natriuretic peptide; NYHA, New York Heart Association; PAG, phenylacetylglycine; MNM amide, methylnicotinamide; TMAO, trimethylamine N-oxide; MMA, methylmalonate; DRI, dietary reference intake. ⁎ Corresponding authors. G.-S. Hwang is to be contacted at Korea Basic Science Institute, Seoul 136-713, Republic of Korea. Fax: + 82 2 920 0779. J.H. Chung, Severance Integrative Research Institute for Cerebral and Cardiovascular Disease, Yonsei University Health System, Seoul 120-752, Republic of Korea. Fax: +82 2 2227 7869. E-mail addresses: [email protected] (G.-S. Hwang), [email protected] (J.H. Chung). 0009-9120/$ – see front matter © 2010 The Canadian Society of Clinical Chemists. Published by Elsevier Inc. All rights reserved. doi:10.1016/j.clinbiochem.2010.11.010 Contents lists available at ScienceDirect Clinical Biochemistry journal homepage: www.elsevier.com/locate/clinbiochem
Transcript of 1H nuclear magnetic resonance based metabolic …chemistry.skku.edu/dhryu/publication/2011-...

Clinical Biochemistry 44 (2011) 293–299
Contents lists available at ScienceDirect
Clinical Biochemistry
j ourna l homepage: www.e lsev ie r.com/ locate /c l inb iochem
1H nuclear magnetic resonance based metabolic urinary profiling of patients withischemic heart failure
Seok-Min Kang a, Jong-Chul Park b,c, Min-Jeong Shin d, Hyeran Lee d, Jaewon Oh a, Do Hyun Ryu e,Geum-Sook Hwang b,c,⁎, Ji Hyung Chung a,f,⁎a Cardiology Division, Yonsei Cardiovascular Hospital and Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul 120-752, Republic of Koreab Korea Basic Science Institute, Seoul 136-713, Republic of Koreac Graduate School of Analytical Science and Technology, Chungnam National University, Daejeon 305-764, Republic of Koread Department of Food and Nutrition, Korea University, Seoul 136-703, Republic of Koreae Department of Chemistry, Sungkyunkwan University, Gyeonggi-do 440-746, Republic of Koreaf Severance Integrative Research Institute for Cerebral and Cardiovascular Disease, Yonsei University Health System, Seoul 120-752, Republic of Korea
Abbreviations: NMR, nuclearmagnetic resonance; TCAnatriuretic peptide; NYHA, New York Heart Association; Pamide, methylnicotinamide; TMAO, trimethylamine N-DRI, dietary reference intake.⁎ Corresponding authors. G.-S. Hwang is to be con
Institute, Seoul 136-713, Republic of Korea. Fax: +82 2 9Integrative Research Institute for Cerebral and CaUniversity Health System, Seoul 120-752, Republic of K
E-mail addresses: [email protected] (G.-S. Hwang)
0009-9120/$ – see front matter © 2010 The Canadian Sdoi:10.1016/j.clinbiochem.2010.11.010
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 31 August 2010Received in revised form 24 November 2010Accepted 30 November 2010Available online 15 December 2010Keywords:Heart failureCitric acid cycleMetabolismMethylmalonic acidPhenylacetylglycine
Objectives: We sought to identify metabolic pathways characterizing human heart failure (HF) using1NMR based urinary metabolomic analysis in conjunction with multivariate statistics.
Design and methods: Patients with systolic HF of ischemic origin (n=15) and healthy controls (n=20)participated in this study. Patients with type 2 diabetes mellitus were excluded.
Results: The results showed that the urine of the HF patients had higher levels of metabolites for acetate(pb0.05) and acetone (pb0.01) compared to the healthy controls. In addition, there was a perturbation inmethylmalonate metabolism as shown by increased urinary levels of methylmalonic acid (pb0.001) in the HFpatients. HF patients also had increased urinary levels of cytosine (pb0.01) and phenylacetylglycine (pb0.01)and decreased 1-methylnicotinamide (pb0.05) compared to healthy controls.
Conclusions: TCA cycle metabolites and fatty acid metabolism were modified in the HF patients,indicating altered energy metabolism. Moreover, perturbations of metabolism in nucleotide and methylma-
lonate were observed.© 2010 The Canadian Society of Clinical Chemists. Published by Elsevier Inc. All rights reserved.
Introduction
The prevalence of heart failure (HF) is increasing despite majortherapeutic advances, and HF is now considered as one of the majorpublic health burdens both in developed and developing countries [1].It has been well known that HF is, in part, the result of the progressionof chronic hypertension as well as acute and chronic cardiac injuryincluding myocardial infarction [2]. Considering the aging of popula-tions and the pandemic of cardiovascular disease (CVD) all over theworld, the importance of its prevention is magnified [3]. As such, the
, tricarboxylic acid; BNP, B-typeAG, phenylacetylglycine; MNMoxide; MMA, methylmalonate;
tacted at Korea Basic Science20 0779. J.H. Chung, Severancerdiovascular Disease, Yonseiorea. Fax: +82 2 2227 7869., [email protected] (J.H. Chung).
ociety of Clinical Chemists. Publish
prevention of HF is an urgent public health need with national andglobal implications that deserves high priority.
The etiology of HF is very complex and correspondingly numerousstudies have aimed to define the underlying pathophysiology of HFusing recent advances in the systems biology approach, which enablesthe diagnosis of disease state [4]. Metabolomic analysis is a com-prehensive tool for simultaneously measuring the amounts of metab-olites of multiple metabolic pathways. Global metabolite profiles ofcomplex samples are used to identify potential biomarkers, whichcan provide new and unexpected insights into biological processes[5]. Indeed, emerging data have been reported by studies ofmetabolomics to define perturbations in metabolic pathways andnetworks in human disease including diabetes [6], cancer [7], andneurodegenerative disorders [8,9]. In the application of metabolomicsto cardiovascular pathway discoveries, there have been severalattempts to identify metabolic phenotypes differentiating the meta-bolic pathways of myocardial ischemia [10], planned myocardialinfarction [11], and a reperfusion model [12]. However, metabolicinvestigations into urinary metabolites in human heart failure havenot been performed.
In the present study, we attempted to determine the differencesin urinary metabolites of HF patients versus healthy controls.
ed by Elsevier Inc. All rights reserved.

294 S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299
Materials and methods
Subjects
For this study, 15 chronic stable HF patients from Yonsei Cardio-vascular Hospital and 20 age- and gender-matched healthy controlsparticipated in the study. The inclusion criteria for HF were: (1) adiagnosis of systolic HF of ischemic origin and a left ventricularejection fraction (LVEF)≤50%, (2)≤80 years of age, and (3) stable HF(New York Heart Association Classes I–II) with medication for atleast 1 month prior to inclusion. The exclusion criteria were: (1) adiagnosis of HF with a preserved ejection fraction (N50%) or non-ischemic origin, (2) diagnosed type 2 diabetes mellitus and acutemyocardial infarction 3 months prior to inclusion, and (3) severecognitive impairment. At the time of initial enrollment, HF patientsunderwent a complete physical examination including blood pres-sure and heart rate and laboratory assessment. Body mass index(BMI) was calculated as weight in kg divided by height in meterssquared. Medical history, including diagnosis, underlying disease,etiology of HF, and drug use were obtained. All patients were givenwritten informed consent, and the Institutional Review Board atYonsei University Medical Center approved the study protocol.Venous bloods were collected for further analysis after a fastingperiod. Urine was collected in polyethylene tubes in the morningafter 12 h of fasting. The tubes were immediately stored at −70 °Cuntil analysis.
Biochemical measurements
Biochemical measurements including total cholesterol, triglycer-ide, HDL-cholesterol, LDL-cholesterol, free fatty acid, creatinine, uricacid and glucose were analyzed by enzymatic methods with com-mercially available kitswith automatic analyzer (Advia 1650, Siemens,Germany). Plasma B-type natriuretic peptide (BNP) concentrationswere measured with a Triage BNP test kit (Biosite Diagnositics, SanDiego, CA, USA).
NMR spectroscopic measurement of urine
The urine samples were thawed, vortexed, and allowed to standfor 10 min prior to mixing aliquots (540 μL) with an internal stan-dard solution [60 μL, consisting of 5 mM sodium 2,2-dimethyl-2-silapentane-5-sulfonate (DSS), 0.2% sodium azide in 99% deuteriumwater (D2O)], and then centrifuged at 12,000 rpm for 10 min. Thesupernatant from each urine sample was adjusted to pH 7.0 and analiquot of the prepared urine sample (600 μL) was transferred into a5-mm NMR tube (Wilmad, Buena, NJ). D2O and DSS provided a fieldfrequency lock and chemical shift reference (1H, δ 0.00), respectively.The 1H NMR spectra were acquired on a Varian VNMRS-600 MHzNMR spectrometer (Varian Inc., Palo Alto, CA) operating at a599.84 MHz 1H frequency and a temperature of 298 K, using a tripleresonance 5-mm HCN salt tolerant cold probe. A noesypresat pulsesequence was applied to suppress the residual water signal. For eachsample, FIDs were collected with 64 transients into 32 K data points,using a spectral width of 9615.4 Hz with a relaxation delay of 2 s, anacquisition time of 4 s, and a mixing time of 400 ms. All spectra weremultiplied by an exponential weighting function corresponding to aline-broadening of 0.5 Hz.
NMR data preprocessing and multivariate statistical analysis
All NMR spectra were phased and baseline corrected usingChenomx NMR suite 4.6 software, professional edition (ChenomxInc.). The NMR spectral data were reduced into 0.005 ppm spectralbuckets and the regions corresponding to water/HOD and urea (4.32–6.32) were removed from all the spectra. The spectral data were then
normalized to the total spectral area and converted to the ASCIIformat. The ASCII format files were imported into MATLAB (R2006a,Mathworks, Inc., Natick, MA), and all spectra were aligned using theCorrelation Optimized Warping (COW) method [13]. The resultingdata sets were then imported into SIMCA-P version 12.0 (Umetrics,Umeå, Sweden) and Pareto scaled for multivariate statistical analysis.Principal components analysis (PCA), an unsupervised patternmethod, was performed to examine the intrinsic variation in thedataset. To maximize the separation between samples, the orthogonalprojections to latent structures method or an orthogonal partial least-squares discriminant analysis (OPLS-DA) model was applied tomaximize the covariance between the measured data (X variable,peak intensities in the NMR spectra) and the response variable(Y variable, predictive classifications), and simultaneously to removenon-correlated variation in X variables to Y variables or variability inX that is orthogonal to Y [14]. Hotelling's T2 region [15], shown as anellipse in the scores plot, defines the 95% confidence interval of themodeled variation. The quality of the models was described by R2 andQ2 values. R2 is defined as the proportion of variance in the dataexplained by the models and indicates goodness of fit, and Q2 isdefined as the proportion of variance in the data predictable by themodel, and indicates predictability.
Quantification of urinary metabolites
Quantification of the metabolite concentrations was achievedusing Chenomx NMR Suite 5.1 (Chenomx Inc. Edmonton, Canada)[15]. A reference compound (DSS) was used as an internal standardfor the chemical shifts (set to 0 ppm) as well as a reference signal forquantification. Quantification was done by comparing the integral ofa known reference signal (DSS-d6) with the signals derived from alibrary of compounds containing chemical shifts and peak multi-plicities. Identifiable metabolites were chosen for quantification bymatching to the Chenomx 600 MHz Library. Each urinary metaboliteconcentration was normalized to creatinine (μM/mM creatinine) ineach urine samples. The metabolite concentration data sets werethen imported into Spotfire Decision site 9.2 software (Tibcosoftware, CA, USA). For pattern detection, heat-map analysis wasperformed to characterize and to verify the metabolite concentra-tions of the urinary metabolites. Differences in metabolite concen-tration and blood parameters were evaluated using Student's t-testwith GraphPad Prism version 5.01 (GraphPad Software, San Diego,CA). A two-tailed value of Pb0.05 was considered statisticallysignificant.
Results
This study consisted of 15 patients with HF of ischemic origin (12NYHA I and 3 NYHA II) and 20 age- and gender-matched healthycontrols. The mean ejection fraction, systolic blood pressure, diastolicblood pressure and heart rate were 37.1±8.7%, 121.7±15.9 mmHg,76.0±8.9 mmHg and 74.8±9.1 beats/min in the HF patients, respec-tively. Medical treatment for the HF patients consisted of diuretics(53.3%), digitalis (0%), β-blocker (53.3%), angiotensin convertingenzyme inhibitors and/or angiotensin II receptor blocker (69.2%),anti-platelet agents (100.0%), and hypolipidemic agents (80.0%). Theproportions of HF patients with hypertension, hyperlipidemia, andchronic renal failure were 40.0%, 33.3% and 13.3%, respectively.Table 1 presents baseline characteristics and biochemical parametersof the subjects. Age, gender distributions and BMI were not sta-tistically different between the two groups. Serum levels of totalcholesterol and LDL-cholesterol were lower in HF patients than inhealthy controls, whereas creatinine, uric acid and BNP levels werehigher in HF patients than in healthy controls.
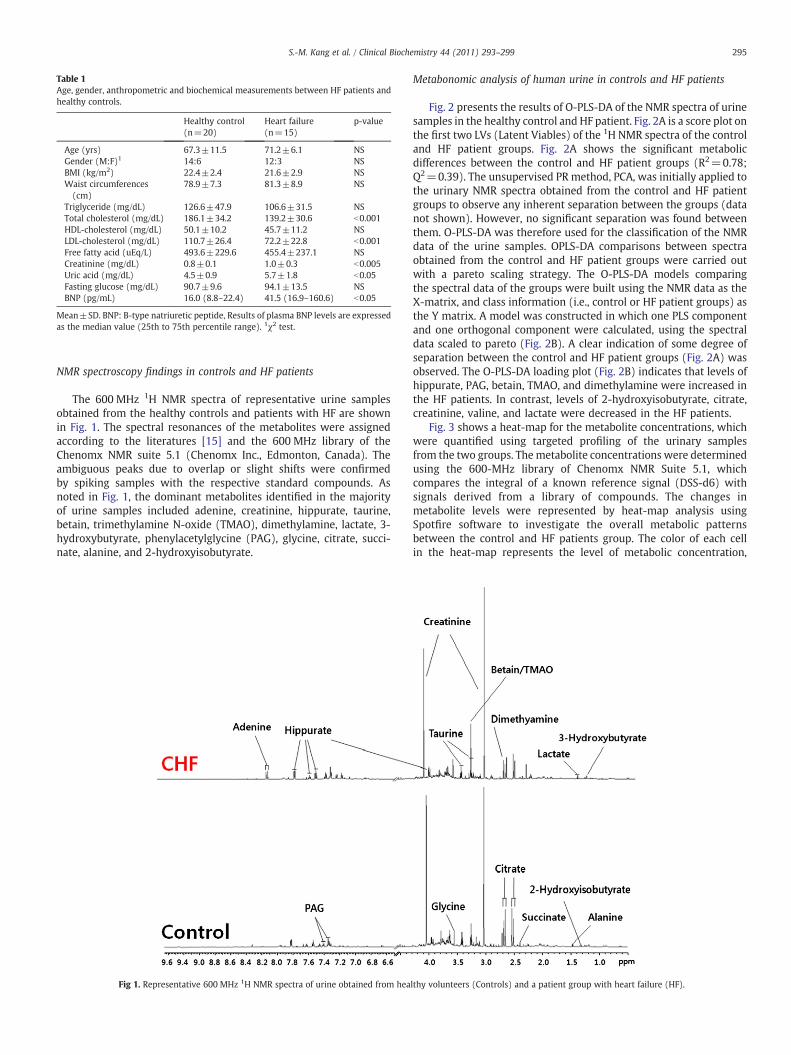
Table 1Age, gender, anthropometric and biochemical measurements between HF patients andhealthy controls.
Healthy control(n=20)
Heart failure(n=15)
p-value
Age (yrs) 67.3±11.5 71.2±6.1 NSGender (M:F)1 14:6 12:3 NSBMI (kg/m2) 22.4±2.4 21.6±2.9 NSWaist circumferences(cm)
78.9±7.3 81.3±8.9 NS
Triglyceride (mg/dL) 126.6±47.9 106.6±31.5 NSTotal cholesterol (mg/dL) 186.1±34.2 139.2±30.6 b0.001HDL-cholesterol (mg/dL) 50.1±10.2 45.7±11.2 NSLDL-cholesterol (mg/dL) 110.7±26.4 72.2±22.8 b0.001Free fatty acid (uEq/L) 493.6±229.6 455.4±237.1 NSCreatinine (mg/dL) 0.8±0.1 1.0±0.3 b0.005Uric acid (mg/dL) 4.5±0.9 5.7±1.8 b0.05Fasting glucose (mg/dL) 90.7±9.6 94.1±13.5 NSBNP (pg/mL) 16.0 (8.8–22.4) 41.5 (16.9–160.6) b0.05
Mean±SD. BNP: B-type natriuretic peptide, Results of plasma BNP levels are expressedas the median value (25th to 75th percentile range). 1χ2 test.
295S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299
NMR spectroscopy findings in controls and HF patients
The 600 MHz 1H NMR spectra of representative urine samplesobtained from the healthy controls and patients with HF are shownin Fig. 1. The spectral resonances of the metabolites were assignedaccording to the literatures [15] and the 600 MHz library of theChenomx NMR suite 5.1 (Chenomx Inc., Edmonton, Canada). Theambiguous peaks due to overlap or slight shifts were confirmedby spiking samples with the respective standard compounds. Asnoted in Fig. 1, the dominant metabolites identified in the majorityof urine samples included adenine, creatinine, hippurate, taurine,betain, trimethylamine N-oxide (TMAO), dimethylamine, lactate, 3-hydroxybutyrate, phenylacetylglycine (PAG), glycine, citrate, succi-nate, alanine, and 2-hydroxyisobutyrate.
Fig 1. Representative 600 MHz 1H NMR spectra of urine obtained from hea
Metabonomic analysis of human urine in controls and HF patients
Fig. 2 presents the results of O-PLS-DA of the NMR spectra of urinesamples in the healthy control and HF patient. Fig. 2A is a score plot onthe first two LVs (Latent Viables) of the 1H NMR spectra of the controland HF patient groups. Fig. 2A shows the significant metabolicdifferences between the control and HF patient groups (R2=0.78;Q2=0.39). The unsupervised PR method, PCA, was initially applied tothe urinary NMR spectra obtained from the control and HF patientgroups to observe any inherent separation between the groups (datanot shown). However, no significant separation was found betweenthem. O-PLS-DA was therefore used for the classification of the NMRdata of the urine samples. OPLS-DA comparisons between spectraobtained from the control and HF patient groups were carried outwith a pareto scaling strategy. The O-PLS-DA models comparingthe spectral data of the groups were built using the NMR data as theX-matrix, and class information (i.e., control or HF patient groups) asthe Y matrix. A model was constructed in which one PLS componentand one orthogonal component were calculated, using the spectraldata scaled to pareto (Fig. 2B). A clear indication of some degree ofseparation between the control and HF patient groups (Fig. 2A) wasobserved. The O-PLS-DA loading plot (Fig. 2B) indicates that levels ofhippurate, PAG, betain, TMAO, and dimethylamine were increased inthe HF patients. In contrast, levels of 2-hydroxyisobutyrate, citrate,creatinine, valine, and lactate were decreased in the HF patients.
Fig. 3 shows a heat-map for the metabolite concentrations, whichwere quantified using targeted profiling of the urinary samplesfrom the two groups. Themetabolite concentrations were determinedusing the 600-MHz library of Chenomx NMR Suite 5.1, whichcompares the integral of a known reference signal (DSS-d6) withsignals derived from a library of compounds. The changes inmetabolite levels were represented by heat-map analysis usingSpotfire software to investigate the overall metabolic patternsbetween the control and HF patients group. The color of each cellin the heat-map represents the level of metabolic concentration,
lthy volunteers (Controls) and a patient group with heart failure (HF).

Fig 2. OPLS-DA score plot (A) and loadings plot (B) of urinary NMR spectra obtained from healthy controls and patients with HF. The loading plot reveals metabolites responsible fordifferentiating the control group and HF group. The upper section of the loadings plot represents metabolites increased in the control group, whereas the low section representsmetabolites increased in the HF group. The goodness of fit and predictability for the models was evaluated by values of R2 of 0.78 and Q2 of 0.39.
Fig 3. Heat-map of 24 urinary metabolites showing metabolic difference between HF patient and control groups. Metabolite concentrations were measured by targeted profilingthrough the use of Chenomx NMR Suite 5.1 (Chenomx Inc. Edmonton, Canada) and concentrations were determined using the 600-MHz library from Chenomx NMR Suite, whichcompares the integral of a known reference signal (DSS-d6) with signals derived from a library of compounds containing chemical shifts and peak multiplicities.
296 S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299

297S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299
indicating different metabolic patterns between the control and HFpatients group. The metabolite concentrations of 1-methylnicotina-mide (MNM amide), 2-hydroxyisobutyrate, 2-oxoglutarate, adenine,cis-aconitate, citrate, glutamine, histidine, phenylalanine, and pyru-vate were relatively lower in the HF patients group compared tothe control group, whereas concentrations of acetate, acetoacetate,acetone, betain, cytosine, dimethylamine, glutarate, hippurate,methylmalonate, and PAG were relatively higher in the HF patientsgroup. The metabolites responsible for the observed differencesbetween the two groups are summarized in Table 2, along withthe relative concentrations of metabolites in the groups.
Quantification of metabolites in control and HF patients
To further analyze the metabolic changes, we performed thecomparison of the urinary metabolites normalized by creatinine usingStudent's t-test between the control and HF patient groups. The resultsshowed that urinary metabolite levels of acetate (pb0.05), acetone(pb0.01), cytosine (pb0.01), methylmalonate (pb0.001), and PAG(pb0.01) were significantly higher in the HF patients compared to thecontrol group, whereas levels of 1-MNM amide (pb0.01) weresignificantly lower in the HF patients (Fig. 4). Subsequent analysiswith urine from additional subjects (29 healthy controls and 27 HFpatients) showed that HF patients had higher urinary levels of acetate(pb0.05), acetone (pb0.01), cytosine (pb0.005), methylmalonate(pb0.001), and PAG (pb0.01) and lower urinary levels of 1-MNM
Table 21H chemical shift assignment of metabolites observed in urine from control and HFpatient groups and their relative concentrations.
Fold change in patientwith heart failure
Metabolite Chemical shift (δ) Q2=0.39
R2=0.78
1-Methylnicotinamide 9.27(s), 8.96(d), 8.88(d),8.18(m), 4.47(s)
0.47
2-Hydroxyisobutyrate 1.35(s) 0.862-Oxoglutarate 2.98(t), 2.43(t) 0.834-Hydroxyphenylacetate 7.15(d), 6.85(d),
3.44(s)1.68
Acetate 1.91(s) 1.45Acetoacetate 3.44(s), 2.28(s) 1.41Acetone 2.22(s) 1.57Adenine 8.20(s), 8.18(s) 0.76Betaine 3.89(s), 3.26(s) 1.74Citrate 2.67(d), 2.52(d) 0.65Cytosine 7.49(d), 5.97(d), 2.64Dimethylamine 2.71(s) 1.26Glutamine 2.46(m), 2.41(m), 2.13(m) 0.83Glutarate 2.17(t), 1.78(m) 1.23Hippurate 7.82(d), 7.62(t),
7.54(t), 3.96(d)1.42
Histidine 7.90(s), 7.10(s), 3.98(m),3.25(m), 3.14(m)
0.69
Methylguanidine 2.82(s) 1.73Methylmalonate 3.16(m), 1.24(d) 1.46Phenylacetylglycine 7.41(t), 7.35(t),
3.74(d), 3.66(s)1.57
Phenylalanine 7.41(t), 7.34(m),3.99(m),3.27(m), 3.11(m)
0.88
Pyruvate 2.36(s) 0.90Succinate 2.39(s) 0.95Taurine 3.42(t), 3.26(t) 1.30Trimethylamine N-oxide 3.26(s) 1.10Tyramine 7.19(d), 6.88(d),
3.23(t), 2.91(t)1.34
cis-Aconitate 5.70(d), 3.11(s) 0.90
Letters in parentheses indicate the peak multiplicities: s, singlet; d, doublet; t, triplet;m, multiplet.
amide (pb0.005) compared to the healthy controls (see SupplementaryTables 1–2).
Discussion
In the present study, we explored metabolite profiling discrimi-nation by examining the urine samples of HF patients and age- andgender-matched healthy controls. Using a comprehensive NMRscreening process, we identified alterations of metabolites in path-ways such as the tricarboxylic acid (TCA) cycle, fatty acid metabolism,methylamalnote and nucleotide metabolism.
Energy metabolism in HF
The metabolite profiles of the HF patients were characterized byincreased urinary excretion of acetone, acetoacetate, and acetate, anddecreased urinary excretion of TCA cycle intermediates such as citrate,succinate, 2-oxo-glutarate, and cis-aconitate. It has been recognizedthat the failing heart is characterized by alterations in myocardialenergy metabolism, including mitochondrial dysfunction and areduction in the fatty acid (FA) oxidation rate, which is partiallycompensated by an increase in glucose utilization [16]. The rate ofmetabolism along these different pathways is determined by variousenzymes and substrate–product relationships including pyruvatedehydrogenase (PDH) and palmitoyltransferase-1 (CPT-1) [16,17].Alternatively, it has been postulated that a reduction in the expressionof genes involved in fatty acid metabolism may be associated withcardiac hypertrophy and heart failure [16]. Indeed, several mitochon-drial β-oxidative enzymes have reduced activity [18] in heart failure,and are partly responsible for the reduction in fatty acid metabolism.It may be that increases in urinary ketone bodies shown in the presentstudy could possibly be due to alterations in myocardial utilization.
Cardiomyocyte levels of TCA cycle intermediates are regulated toprovide adequate through-put of substrates which were derived fromglycolysis and ß-oxidation of fatty acids [10]. While there is a constantrate of mitochondrial efflux of TCA cycle intermediates as evidencedby cataplerosis in normal cardiomyocytes [19], the TCA cycle inter-mediates in the setting of acute ischemia are preserved to defendATP production [10]. In the present study, the patients were all diag-nosed with ischemia-origin HF; thus, the depressed pattern of urinaryTCA cycle intermediatesmay support the previous notion of ischemia-related TCA cycle impairment and reflect the relative maintenanceof the myocardial TCA cycle. Although an alteration in myocardialsubstrate metabolism in the failing heart has been suggested, themolecular mechanisms and consequences of metabolic alterationsin myocardial substrate utilization are poorly understood and remainto be elucidated.
Methylmalonate metabolism in HF
Methylmalonate (MMA) is the metabolite that is converted to theTCA cycle intermediate succinate with the help of the cofactor vitaminB12. It was previously demonstrated that plasma and urinary con-centrations of MMA and homocysteine will rise in cases of intra-cellular cobalamin deficiency [20], and MMA is now considered abiomarker for vitamin B12 deficiency. In the present study, sig-nificantly higher levels of urinary MMA were observed in the HFpatients compared to the healthy controls, which could possibly leadto reduced levels of urinary succinate as shown in this study. It ispossible that the subjects of this study had potentially deficientvitamin B12 status from either nutritional B vitamin deficiency or bythe depletion of stores required for homocysteine metabolism. Asa result, hyperhomocys teinemia can occur in HF patients, whichwas not experimentally examined in the present study. Given thathyperhomocysteinemia is a predictive risk marker of HF [21] as wellas associated with the severity of HF [22], adequate intake of B

Fig 4.Quantification of identifiedmetabolites in healthy controls (green) and HF (red) patients. Data are given asmeans±SD. Urinary metabolite concentrations were normalized tocreatinine (μM/mM creatinine). *Pb0.05; **Pb0.01; ***Pb0.001.
298 S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299
vitamins needs to be placed as a priority for preventive measure inHF and the pathogenic role of vitamin B12 deficiency in HF needsto be further determined. Moreover, MMA was reported to inhibitsuccinate-supported oxygen consumption by interfering with mito-chondrial succinate uptake [23], therefore it can be speculated thatthe accumulation of MMA would be associated with impaired TCAcycle flux.
With regard to the adequacy of the subjects' vitamin B12 intakes inthis study, the results showed that about 38% of the total subjects hadinferior intakes according to the dietary reference intakes (DRIs);however, their actual daily intakes met the DRIs for Koreans (data notshown). This indicates that the proportion of low intakes wassubstantial, which could lead to potential nutritional complicationsin these HF patients.
Nucleotide metabolism in HF
In the present study, urinary levels of 1-methylnicotinamide weresignificantly lower and urinary levels of cytosine were significantlyhigher in the HF patients compared with healthy controls. N-
methylnicotinamide (NMN amide) is involved in the tryptophan-NAD+pathway, which supplies pyridine nucleotides to the liver[24], and NMN amide has been suggested as a urinary and plasmabiomarker of peroxisome proliferation in rats [25]. The observedpattern for reduced NMN amide may simply reflect niacin defi-ciency in the HF patients. Alternatively, it is also possible that thetryptophan-NAD+pathway was modified in the HF patients, result-ing from the alteration of gene transcription of encoding keyenzymes in the tryptophan-NAD+pathway with relation to PPARs[25,26].
On the other hand, the urinary excretion of modified nucleosidesincluding cytidine, pseudouridine, and methylguanosine is consid-ered to be indicators of RNA degradation and cell turnover [27]. Ithas been reported that elevated urinary levels of modified nucleo-sides were found in patients with leukemia and lymphoma [28], andseveral types of cancer [29–31]. In the present study, urinary levelsof cytosine, a metabolite of cytidine, were significantly higher in theHF patients than in the healthy controls. This is in line with a recentreport demonstrating that serum levels of pseudouridine wereraised in documented HF patients, suggesting that it reflects the

299S.-M. Kang et al. / Clinical Biochemistry 44 (2011) 293–299
remodeling process in the heart itself or increased catabolic activityin the peripheral tissues [32]. Along with the perturbations innucleotide metabolism, increases in PAG were also observed in theHF patients compared to the healthy controls. In addition, levels ofmethylamines such as dimethylamine, TMAO, and tyramine tendedto be increased in the HF patients, possibly indicating infection,disturbances in gut microflora, and drug-induced phospholipids inthese patients [33].
This study has the limitation that it is difficult to draw con-clusions about dynamic processes including flux rates and influencesof drugs. Moreover, it should be acknowledged that urinary metab-olite profiling may not account the changes in myocardial metabo-lites for all. Furthermore, given our relatively small sample size, ourobservation still remains to be verified in larger studies. Furtherstudy is needed to characterize the differential metabolite profilingaccording to the grade of HF with large cohort enough to distinguishmetabolite pattern. Finally, subjects confined only to ischemic HFmay limit the observed results to generalize in HF patients withwhole spectrum of etiologies. However, global measurement ofmetabolite changes using simple urine specimen seems to beuseful tool to detect metabolic perturbations, in addition, the multi-variate statistical approach considers all of the metabolic changessimultaneously.
To conclude, we identified metabolites by comparing stable HFpatients and healthy controls using NMR spectroscopy. The metab-olite profiles of the HF patients exhibited increased urinary levelsof ketone bodies accompanied by reduced levels of TCA cycle inter-mediates, suggesting altered energy metabolism including changesin the TCA cycle and fatty acid metabolism. Furthermore, we observedperturbations in metabolic pathways involved in methylmalonateand nucleotide metabolism. Further studies are needed to investigatewhether or not these metabolic changes are associated with thepotential pathogenesis of HF.
Acknowledgment
This study was supported by a grant of the Korea Healthcaretechnology R&D Project, Ministry for Health & Welfare, Republic ofKorea (A085136).
Appendix A. Supplementary data
Supplementary data to this article can be found online atdoi:10.1016/j.clinbiochem.2010.11.010.
References
[1] Sliwa K, Damasceno A, Mayosi BM. Epidemiology and etiology of cardiomyopathyin Africa. Circulation 2005;112:3577–83.
[2] Anker SD, von Haehling S. Inflammatory mediators in chronic heart failure: anoverview. Heart 2004;90:464–70.
[3] Miyagishima K, Hiramitsu S, Kimura H, Mori K, Ueda T, Kato S, et al. Long termprognosis of chronic heart failure: reduced vs preserved left ventricular ejectionfraction. Circ J 2009;73:92–9.
[4] AsakuraM, KitakazeM. Global gene expression profiling in the failingmyocardium.Circ J 2009;73:1568–76.
[5] Kaddurah-Daouk R, Krishnan KR. Metabolomics: a global biochemical approach tothe study of central nervous system diseases. Neuropsychopharmacology2009;34:173–86.
[6] Salek RM, Maguire ML, Bentley E, et al. A metabolomic comparison of urinarychanges in type 2 diabetes in mouse, rat, and human. Physiol Genomics 2007;29:99–108.
[7] Gao H, Lu Q, Liu X, et al. Application of 1H NMR-based metabonomics in the studyof metabolic profiling of human hepatocellular carcinoma and liver cirrhosis.Cancer Sci 2009;100:782–5.
[8] Tukiainen T, Tynkkynen T, Mäkinen VP, et al. A multi-metabolite analysis of serumby 1H NMR spectroscopy: early systemic signs of Alzheimer's disease. BiochemBiophys Res Commun 2008;375:356–61.
[9] Bogdanov M, Matson WR, Wang L, et al. Metabolomic profiling to develop bloodbiomarkers for Parkinson's disease. Brain 2008;131:389–96.
[10] Sabatine MS, Liu E, Morrow DA, et al. Metabolomic identification of novelbiomarkers of myocardial ischemia. Circulation 2005;112:3868–75.
[11] Lewis GD, Wei R, Liu E, et al. Metabolite profiling of blood from individualsundergoing planned myocardial infarction reveals early markers of myocardialinjury. J Clin Invest 2008;118:3503–12.
[12] Turer AT, Stevens RD, Bain JR, et al. Podgoreanu. Metabolomic profiling revealsdistinct patterns of myocardial substrate use in humans with coronary arterydisease or left ventricular dysfunction during surgical ischemia/reperfusion.Circulation 2009;119:1736–46.
[13] Larsen FH, van den Berg F, Engelsen SB. An exploratory chemometric study of 1HNMR spectra of table wines. J Chemometr 2006;20:198–208.
[14] Hotelling H. The generalization of studient's ratio. Ann Math Stat 1931;2:360–78.
[15] Kind T, Tolstikov V, Fiehn O, Weiss RH. A comprehensive urinary metabolomicapproach for identifying kidney cancer. Anal Biochem 2007;363:185–95.
[16] van Bilsen M, van Nieuwenhoven FA, van der Vusse GJ. Metabolic remodelling ofthe failing heart: beneficial or detrimental? Cardiovasc Res 2009;81:420–8.
[17] Lopaschuk GD, StanleyWA, Lopaschuk CC. Metabolic approach in heart failure: therationale for metabolic interventions. Heart Metab 2005;27:5–10.
[18] Sack MN, Rader TA, Park S, et al. Fatty acid oxidation enzyme gene expression isdownregulated in the failing heart. Circulation 1996;94:2837–42.
[19] Brunengraber H, Roe CR. Anaplerotic molecules: current and future. J InheritMetab Dis 2006;29:327–31.
[20] Lewerin C, Nilsson-Ehle H, Matousek M, et al. Reduction of plasma homocysteineand serum methylmalonate concentrations in apparently healthy elderly subjectsafter treatment with folic acid, vitamin B12 and vitamin B6: a randomised trial.Eur J Clin Nutr 2003;57:1426–36.
[21] Vasan RS, Beiser A, D'Agostino RB, et al. Plasma homocysteine and risk forcongestive heart failure in adults without prior myocardial infarction. JAMA2003;289:1251–7.
[22] Jacques PF, Bostom AG, Wilson PW, et al. Determinants of plasma totalhomocysteine concentration in the Framingham off-spring cohort. Am J ClinNutr 2001;73:613–21.
[23] Mirandola SR, Melo DR, Schuck PF, et al. Methylmalonate inhibits succinate-supported oxygen consumption by interfering with mitochondrial succinateuptake. J Inherit Metab Dis 2008;31:44–54.
[24] Wolf H. The effect of hormones and vitamin B6 on urinary excretion of metabolitesof the kynurenine pathway. Scand J Clin Lab Investig 1974;136:1–186.
[25] Connor SC, Hodson MP, Ringeissen S, et al. Development of a multivariatestatistical model to predict peroxisome proliferation in the rat, based on urinary1H-NMR spectral patterns. Biomarkers 2004;9:364–85.
[26] Ringeissen S, Connor SC, Brown HR, et al. Potential urinary and plasma biomarkersof peroxisome proliferation in the rat: identification of N-methylnicotinamide andN-methyl-4-pyridone-3-carboxamide by 1H nuclear magnetic resonance and highperformance liquid chromatography. Biomarkers 2003;8:240–71.
[27] Seidel A, Brunner S, Seidel P, Fritz GI, Herbarth O. Modified nucleosides: anaccurate tumour marker for clinical diagnosis of cancer, early detection andtherapy control. Br J Cancer 2006;94:1726–33.
[28] Rasmuson T, Björk GR. Urinary excretion of pseudouridine and prognosis ofpatients with malignant lymphoma. Acta Oncol 1995;34:61–7.
[29] McEntire JE, Kuo KC, Smith ME, et al. Classification of lung cancer patients andcontrols by chromatography of modified nucleosides in serum. Cancer Res1989;49:1057–62.
[30] Zheng YF, Kong HW, Xiong JH, et al. Clinical significance and prognostic value ofurinary nucleosides in breast cancer patients. Clin Biochem 2005;38:24–30.
[31] Masuda M, Nishihira T, Itoh K, et al. An immunohistochemical analysis for cancerof the esophagus using monoclonal antibodies specific for modified nucleosides.Cancer 1993;72:3571–8.
[32] Dunn WB, Broadhurst DI, Deepak SM, et al. Serum metabolomics reveals manynovel metabolic markers of heart failure, including pseudouridine and 2-oxogluratate. Metabolomics 2007;3:413–26.
[33] Nicholls AW, Mortishire-Smith RJ, Nicholson JK. NMR spectroscopic-basedmetabonomic studies of urinary metabolite variation in acclimatizing germ-freerats. Chem Res Toxicol 2003;16:1395–404.


















