19 Anterior Pituitary-4pp (2)
8
Anterior Pituitary Outline • Regulation of hormone secretion: Feedback inhibition • Properties of hypothalamic releasing hormones • Anterior pituitary hormones: – Growth Hormone – Prolactin – ACTH Anterior pituitary Posterior pituitary There are several types of cells in the anterior pituitary. Each of them secretes a different hormone and affects a different tissue.
-
Upload
lelouchdamien -
Category
Documents
-
view
240 -
download
0
description
pharm ant pit
Transcript of 19 Anterior Pituitary-4pp (2)
Anterior Pituitary
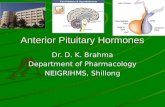
Outline
• Regulation of hormone secretion: Feedback inhibition
• Properties of hypothalamic releasing hormones
• Anterior pituitary hormones:
– Growth Hormone
– Prolactin
– ACTH
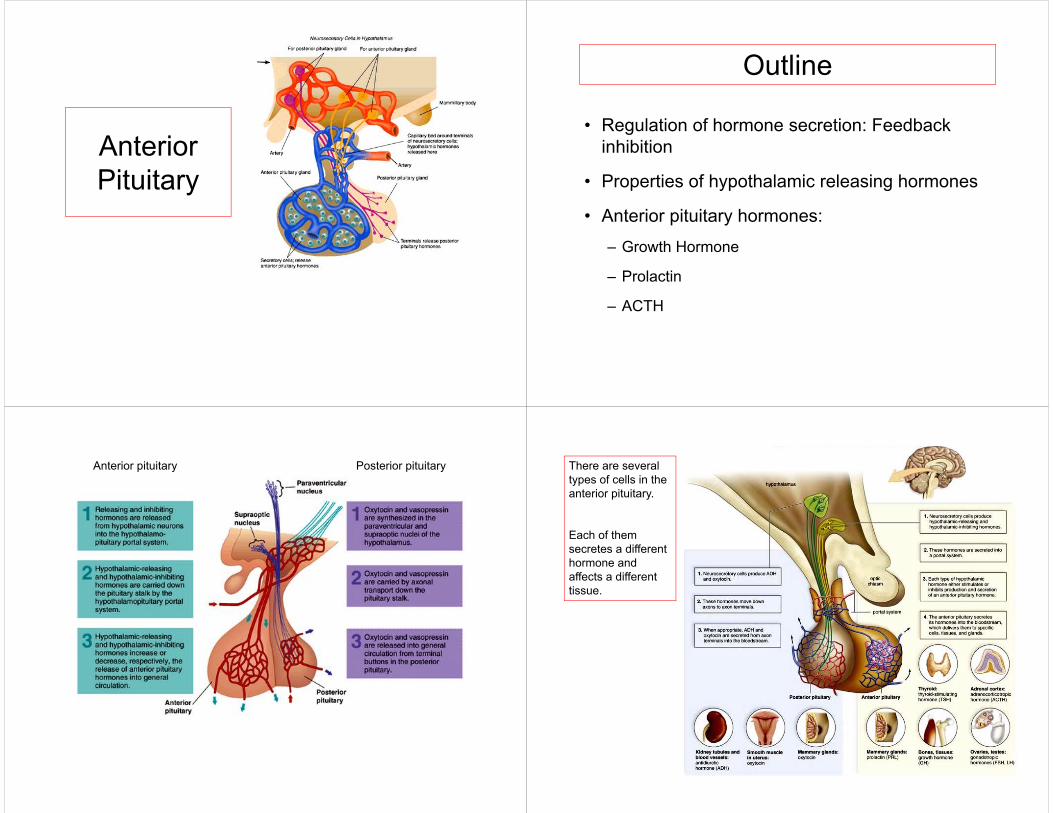
Anterior pituitary Posterior pituitary There are several types of cells in the anterior pituitary.
Each of them secretes a different hormone and affects a different tissue.
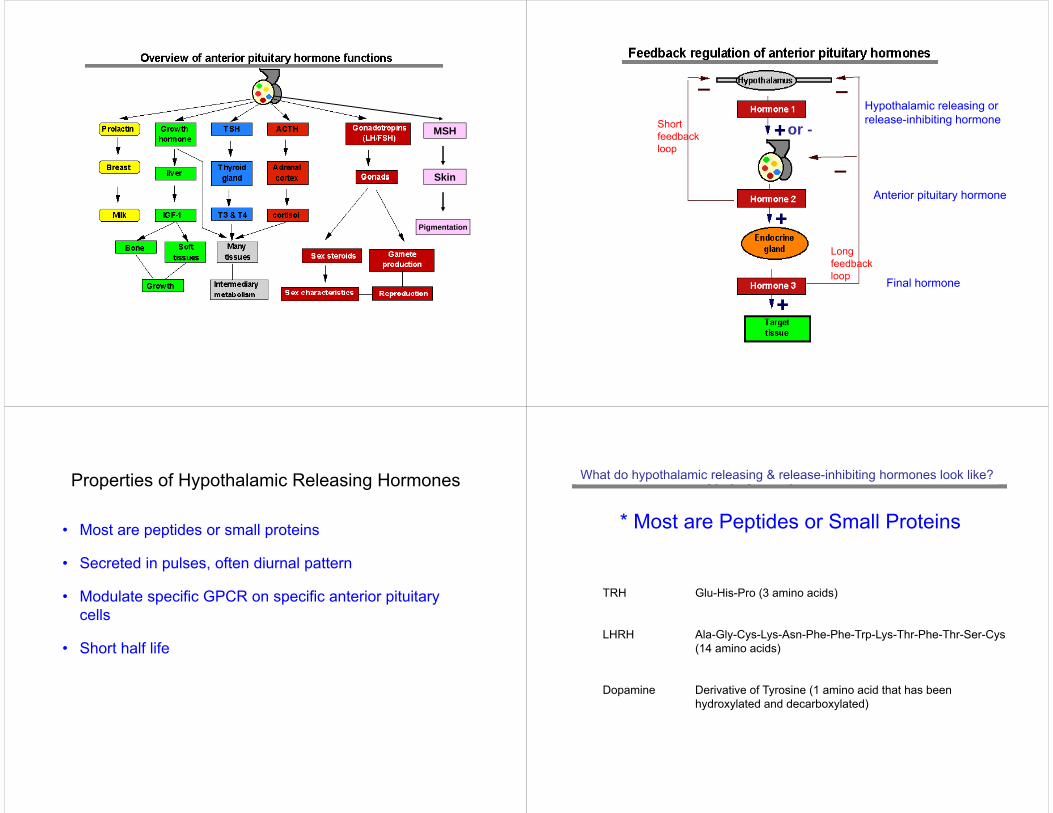
MSH
Skin
Pigmentation
or -Hypothalamic releasing or release-inhibiting hormone
Anterior pituitary hormone
Final hormone
Short feedback loop
Long feedback loop
Properties of Hypothalamic Releasing Hormones
• Most are peptides or small proteins
• Secreted in pulses, often diurnal pattern
• Modulate specific GPCR on specific anterior pituitary cells
• Short half life
What do hypothalamic releasing & release-inhibiting hormones look like?
* Most are Peptides or Small Proteins
TRH Glu-His-Pro (3 amino acids)
LHRH Ala-Gly-Cys-Lys-Asn-Phe-Phe-Trp-Lys-Thr-Phe-Thr-Ser-Cys(14 amino acids)
Dopamine Derivative of Tyrosine (1 amino acid that has been hydroxylated and decarboxylated)
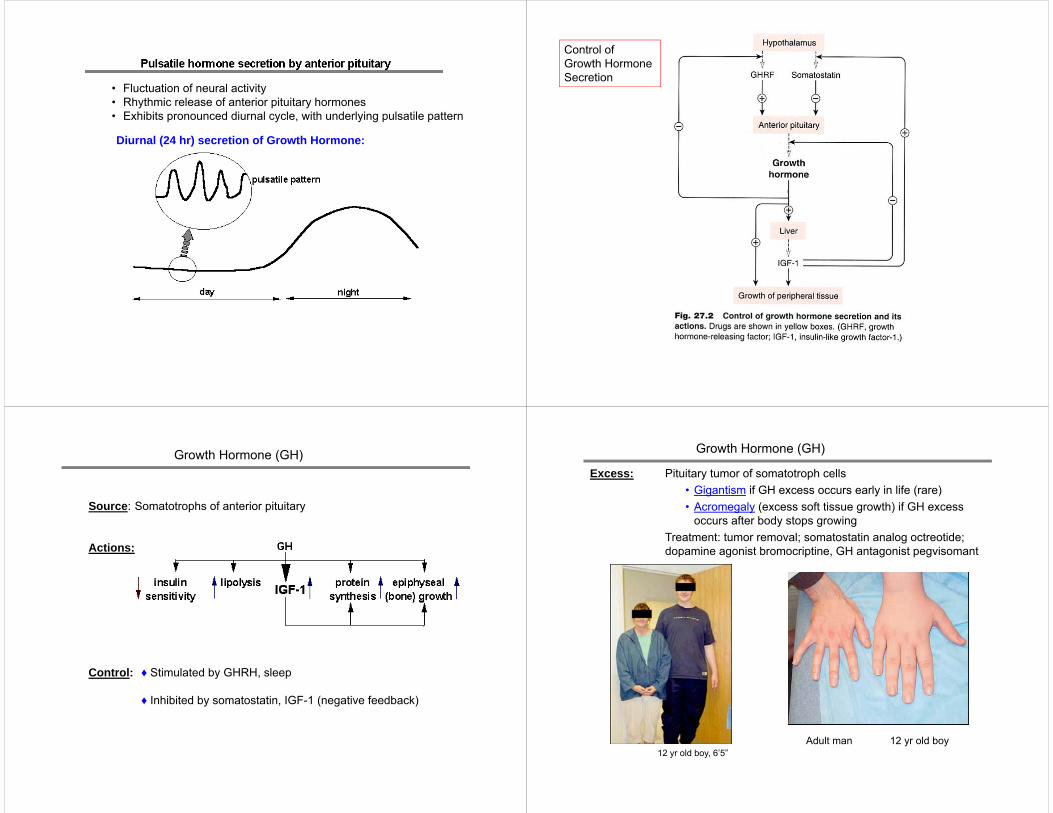
• Fluctuation of neural activity• Rhythmic release of anterior pituitary hormones• Exhibits pronounced diurnal cycle, with underlying pulsatile pattern
Diurnal (24 hr) secretion of Growth Hormone:
Control of Growth Hormone Secretion
Source: Somatotrophs of anterior pituitary
Actions:
Control: ♦ Stimulated by GHRH, sleep
♦ Inhibited by somatostatin, IGF-1 (negative feedback)
Growth Hormone (GH) Growth Hormone (GH)
12 yr old boy, 6’5”Adult man 12 yr old boy
Excess: Pituitary tumor of somatotroph cells• Gigantism if GH excess occurs early in life (rare)• Acromegaly (excess soft tissue growth) if GH excess
occurs after body stops growingTreatment: tumor removal; somatostatin analog octreotide; dopamine agonist bromocriptine, GH antagonist pegvisomant
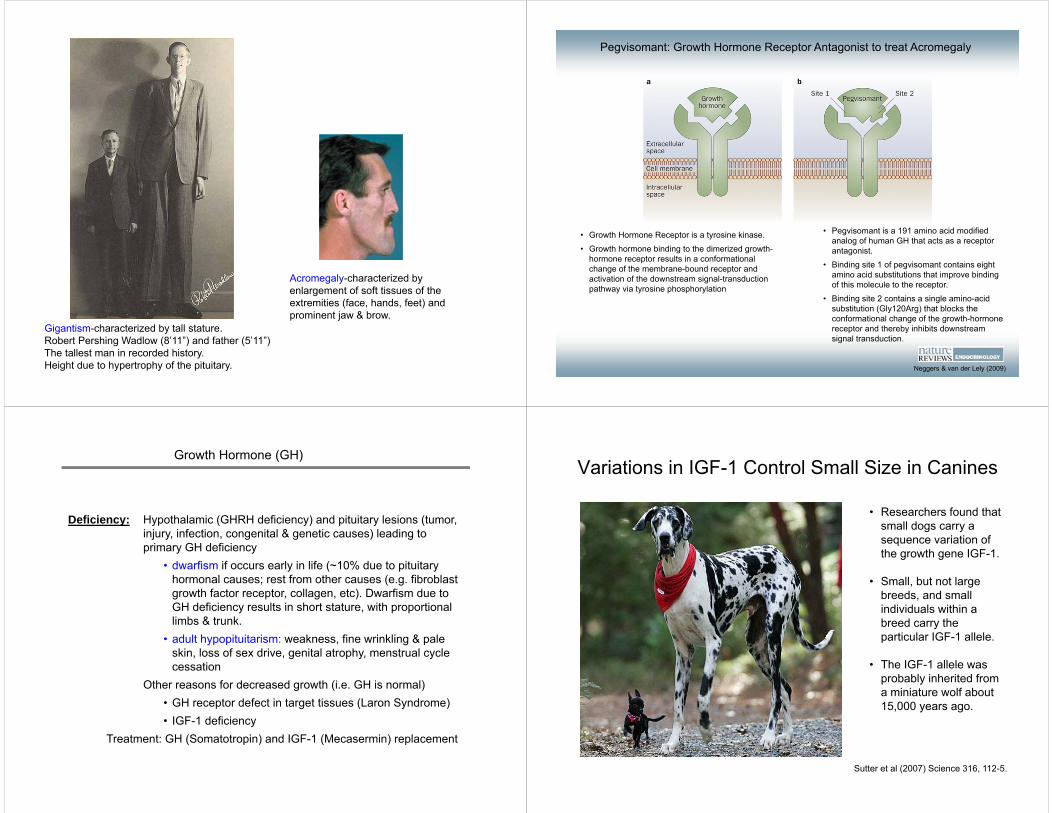
Gigantism-characterized by tall stature.Robert Pershing Wadlow (8’11”) and father (5’11”)The tallest man in recorded history.Height due to hypertrophy of the pituitary.
Acromegaly-characterized by enlargement of soft tissues of the extremities (face, hands, feet) and prominent jaw & brow.
Pegvisomant: Growth Hormone Receptor Antagonist to treat Acromegaly
• Growth Hormone Receptor is a tyrosine kinase. • Growth hormone binding to the dimerized growth-
hormone receptor results in a conformational change of the membrane-bound receptor and activation of the downstream signal-transduction pathway via tyrosine phosphorylation
• Pegvisomant is a 191 amino acid modified analog of human GH that acts as a receptor antagonist.
• Binding site 1 of pegvisomant contains eight amino acid substitutions that improve binding of this molecule to the receptor.
• Binding site 2 contains a single amino-acid substitution (Gly120Arg) that blocks the conformational change of the growth-hormone receptor and thereby inhibits downstream signal transduction.
Neggers & van der Lely (2009)
Growth Hormone (GH)
Deficiency: Hypothalamic (GHRH deficiency) and pituitary lesions (tumor, injury, infection, congenital & genetic causes) leading to primary GH deficiency
• dwarfism if occurs early in life (~10% due to pituitary hormonal causes; rest from other causes (e.g. fibroblast growth factor receptor, collagen, etc). Dwarfism due to GH deficiency results in short stature, with proportional limbs & trunk.
• adult hypopituitarism: weakness, fine wrinkling & pale skin, loss of sex drive, genital atrophy, menstrual cycle cessation
Other reasons for decreased growth (i.e. GH is normal)• GH receptor defect in target tissues (Laron Syndrome)• IGF-1 deficiency
Treatment: GH (Somatotropin) and IGF-1 (Mecasermin) replacement
Variations in IGF-1 Control Small Size in Canines
• Researchers found that small dogs carry a sequence variation of the growth gene IGF-1.
• Small, but not large breeds, and small individuals within a breed carry the particular IGF-1 allele.
• The IGF-1 allele was probably inherited from a miniature wolf about 15,000 years ago.
Sutter et al (2007) Science 316, 112-5.
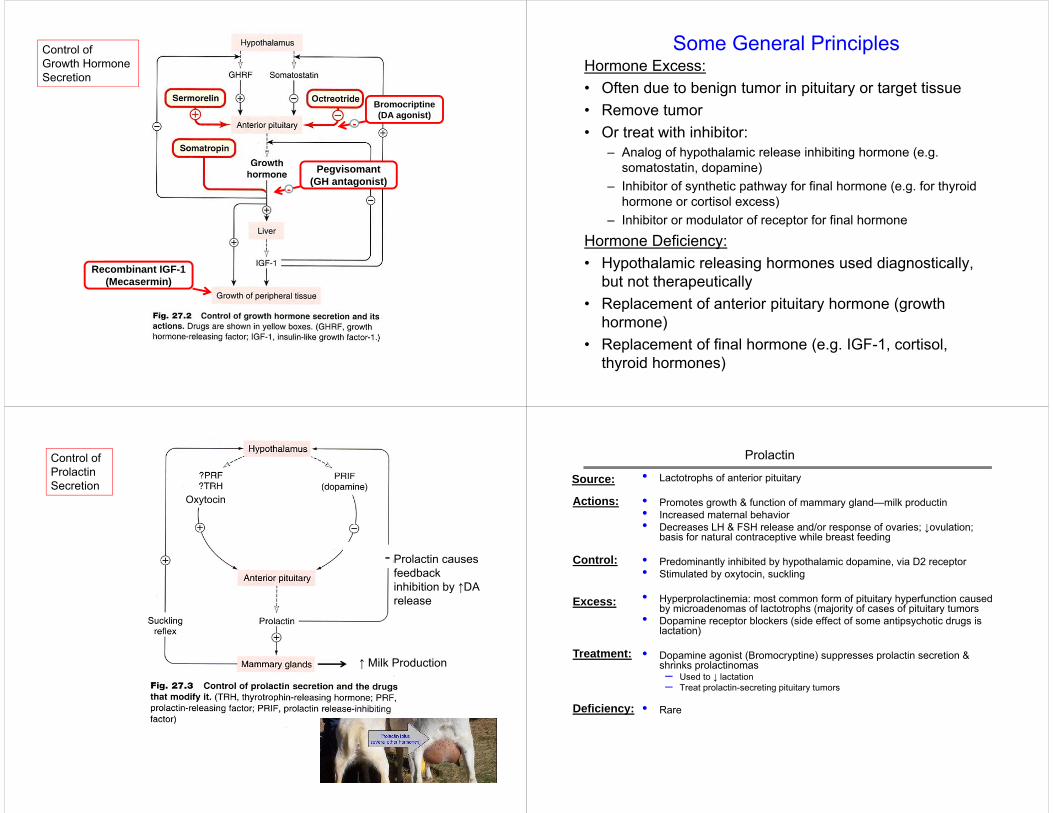
Control of Growth Hormone Secretion
Recombinant IGF-1(Mecasermin)
Pegvisomant(GH antagonist)
-
Bromocriptine(DA agonist)
-
Hormone Excess:• Often due to benign tumor in pituitary or target tissue• Remove tumor• Or treat with inhibitor:
– Analog of hypothalamic release inhibiting hormone (e.g. somatostatin, dopamine)
– Inhibitor of synthetic pathway for final hormone (e.g. for thyroid hormone or cortisol excess)
– Inhibitor or modulator of receptor for final hormone
Hormone Deficiency:• Hypothalamic releasing hormones used diagnostically,
but not therapeutically• Replacement of anterior pituitary hormone (growth
hormone)• Replacement of final hormone (e.g. IGF-1, cortisol,
thyroid hormones)
Some General Principles
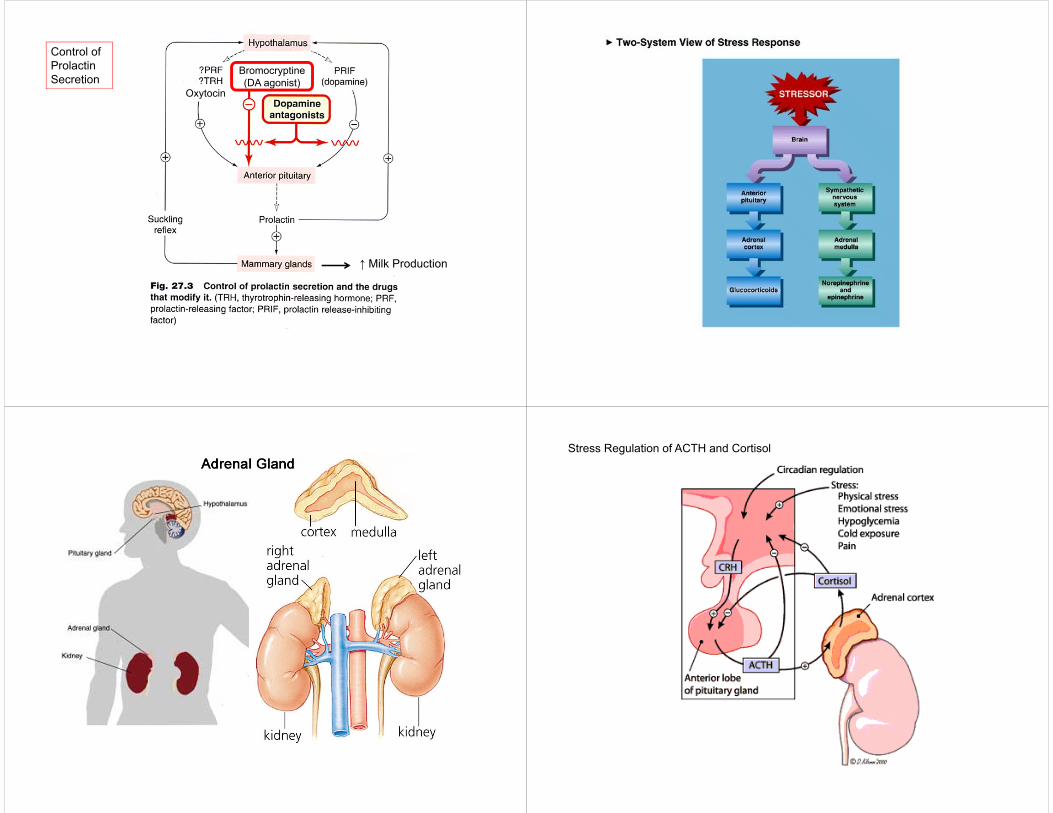
Control of Prolactin Secretion
Oxytocin
↑ Milk Production
Prolactin causes feedback inhibition by ↑DA release
-
• Lactotrophs of anterior pituitary
• Promotes growth & function of mammary gland—milk productin• Increased maternal behavior• Decreases LH & FSH release and/or response of ovaries; ↓ovulation;
basis for natural contraceptive while breast feeding
• Predominantly inhibited by hypothalamic dopamine, via D2 receptor• Stimulated by oxytocin, suckling
• Hyperprolactinemia: most common form of pituitary hyperfunction caused by microadenomas of lactotrophs (majority of cases of pituitary tumors
• Dopamine receptor blockers (side effect of some antipsychotic drugs is lactation)
• Dopamine agonist (Bromocryptine) suppresses prolactin secretion & shrinks prolactinomas– Used to ↓ lactation– Treat prolactin-secreting pituitary tumors
• Rare
Source:
Actions:
Control:
Excess:
Deficiency:
Treatment:
Prolactin
Control of Prolactin Secretion
Oxytocin
↑ Milk Production
Bromocryptine(DA agonist)
Stress Regulation of ACTH and Cortisol
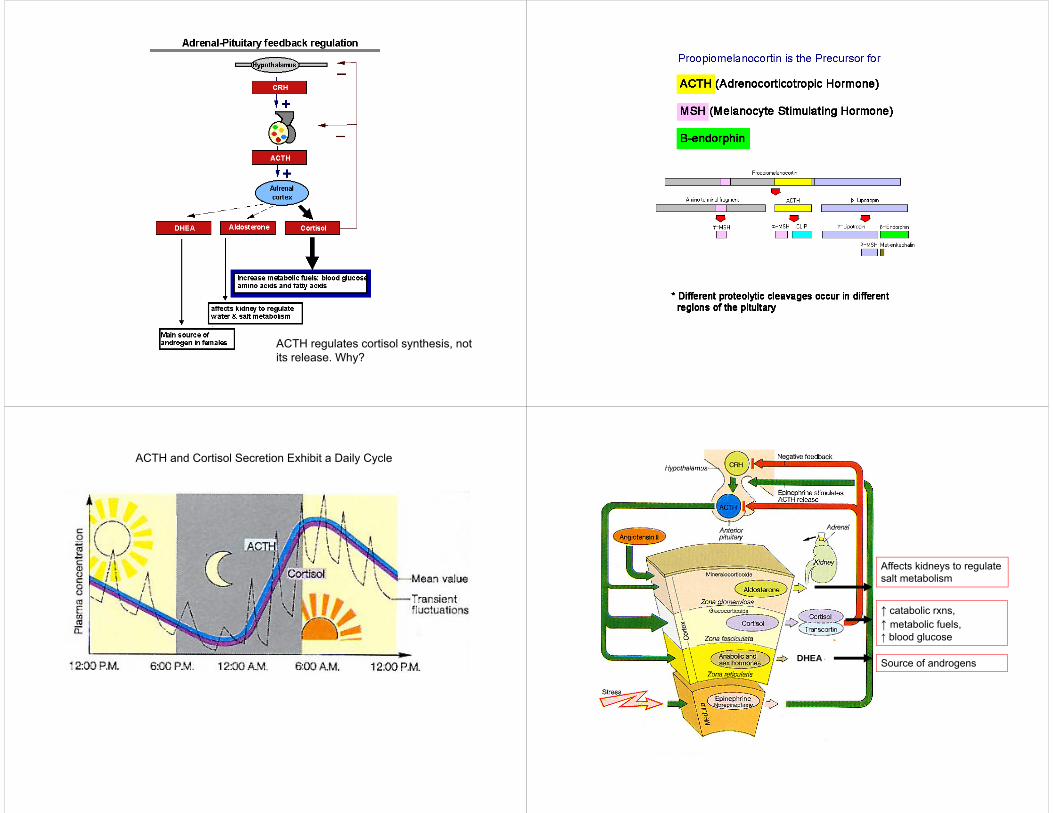
ACTH regulates cortisol synthesis, not its release. Why?
ACTH and Cortisol Secretion Exhibit a Daily Cycle
DHEA
Affects kidneys to regulate salt metabolism
↑ catabolic rxns, ↑ metabolic fuels,↑ blood glucose
Source of androgens
Summary
• Hypothalamic releasing hormones are small peptides that are secreted in a diurnal pulsatile rhythm
• Tight control of [hormones] by feedback inhibition
• Growth hormone released in response to GHRH (inhibited by somatostatin); causes release of IGF-1 from liver to stimulate bone & tissue growth
• Prolactin released in response to oxytocin, suckling (inhibited by dopamine); causes milk production
• ACTH released in response to CRH (stimulated by stress); causes cortisol synthesis; increases glucose, metabolic fuels