188488994 copd
35
Chronic Obstructive Pulmonary Disease: COPD dr. Tjatur Winarsanto SpPD
Transcript of 188488994 copd
Chronic Obstructive Pulmonary Disease: COPD
dr. Tjatur Winarsanto SpPD
Chronic Obstructive Pulmonary Disease: COPD
Disease of airflow obstruction that is not totally reversibleChronic BronchitisEmphysema

COPD: Etiology
Cigarette smoking #1 Recurrent respiratory infection Alpha 1-antitrypsin deficiency Aging
Def: Chronic Bronchitis Excessive tracheobronchial mucus production
sufficient to cause cough with expectoration for most days of at least 3 months of the year for 2 consecutive years.
Classification:
1. Simple chronic bronchitis
2. Chronic mucopurulent bronchitis
3. Chronic bronchitis with obstruction
4. Chronic bronchitis with obstruction and airway hyperreactivity.
Chronic Bronchitis
Recurrent or chronic productive cough for a minimum of 3 months for 2 consecutive years.
Risk factors Cigarette smoke Air pollution

Chronic Bronchitis Pathophysiology Chronic inflammation Hypertrophy &
hyperplasia of bronchial glands that secrete mucus
Increase number of goblet cells
Cilia are destroyed

Chronic Bronchitis Pathophysiology Narrowing of airway
Starting w/ bronchi smaller airways
airflow resistance work of breathing Hypoventilation & CO2
retention hypoxemia & hypercapnea

Chronic Bronchitis Pathophysiology
Bronchospasm often occurs End result
Hypoxemia Hypercapnea Polycythemia (increase RBCs)
Cyanosis Cor pulmonale (enlargement of right side of heart)
Chronic Bronchitis: Clinical Manifestations In early stages
Clients may not recognize early symptoms Symptoms progress slowly May not be diagnosed until severe episode with a
cold or flu Productive cough
• Especially in the morning• Typically referred to as “cigarette cough”
Bronchospasm Frequent respiratory infections
Chronic Bronchitis: Clinical Manifestations
Advanced stages Dyspnea on exertion Dyspnea at rest Hypoxemia & hypercapnea Polycythemia Cyanosis Bluish-red skin color Pulmonary hypertension Cor pulmonale
Chronic Bronchitis: Diagnostic Tests PFTs
FVC: Forced vital capacity FEV1: Forcible exhale in 1 second FEV1/FVC = <70%
ABGs PaCO2 PaO2
RBC Hct

Emphysema Abnormal distension
of air spaces Actual cause is
unknown
Def: Emphysema Permanent abnormal distention of air spaces distal to
the terminal bronchiole with destruction of alveolar septa (containing alveolar capillaries) and attachments to the bronchial walls.
Classification:
1. Centriacinar ( centrilobular) emphysema
2. Panacinar emphysema
3. Paraseptal emphysema
4. Senile emphysema

Emphysema: Pathophysiology Structural changes
Hyperinflation of alveoli Destruction of alveolar &
alveolar-capillary walls Small airways narrow Lung elasticity decreases

Emphysema: Pathophysiology Mechanisms of
structural change Obstruction of small
bronchioles Proteolytic enzymes destroy
alveolar tissue Elastin & collagen are
destroyed Support structure is destroyed “paper bag” lungs
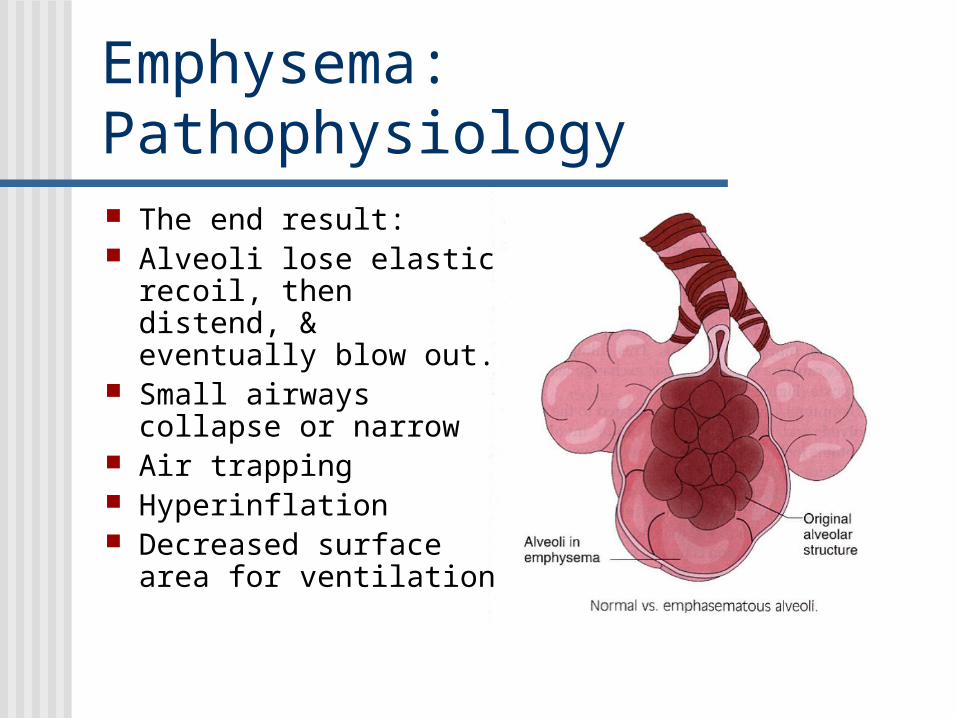
Emphysema: Pathophysiology The end result: Alveoli lose elastic recoil,
then distend, & eventually blow out.
Small airways collapse or narrow
Air trapping Hyperinflation Decreased surface area
for ventilation

Emphysema: Clinical Manifestations Early stages
Dyspnea Non productive cough Diaphragm flattens A-P diameter increases
• “Barrel chest” Hypoxemia may occur
• Increased respiratory rate• Respiratory alkalosis
Prolonged expiratory phase

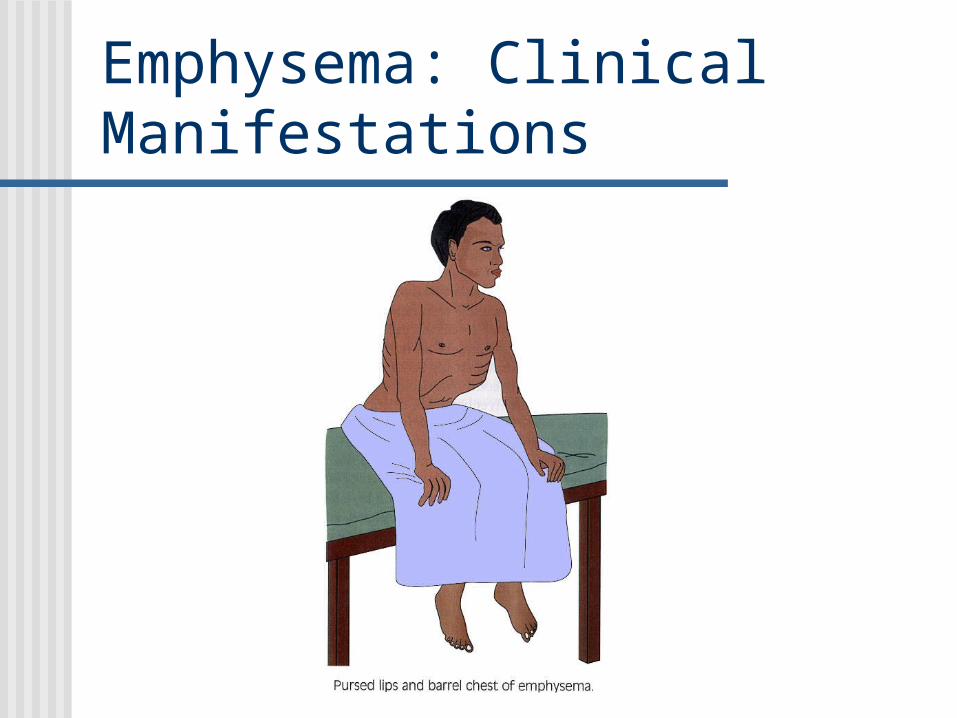
Later stages Hypercapnea Purse-lip breathing Use of accessory muscles to breathe Underweight
• No appetite & increase breathing workload Lung sounds diminished
Emphysema: Clinical Manifestations
Emphysema: Clinical Manifestations

Emphysema: Clinical Manifestations
Pulmonary function residual volume, lung capacity, DECREASED FEV1,
vital capacity maybe normal
Arterial blood gases Normal in moderate disease May develop respiratory alkalosis Later: hypercapnia and respiratory acidosis
Chest x-ray Flattened diaphragm hyperinflation

Assess for COPD:A Common Story Cough
intermittent or daily present throughout day- seldom only nocturnal
Sputum Any pattern of chronic sputum production
Dyspnea Progressive and Persistent "increased effort to breathe" "heaviness" "air hunger" or
"gasping" Worse on exercise Worse during respiratory infections
Exposure to risk factors Tobacco smoke Occupational dusts and chemicals Smoke from home cooking and heating fuels

Assess and Monitor Disease Classification of COPD
Stage 0 At RiskStage I Mild COPDStage II Moderate COPDStage III Severe COPDStage IV Very Severe COPD

Stage 0 At Risk
Normal spirometry +/- Chronic symptoms (cough, sputum,
production)
Stage I Mild COPD
FEV1/FVC <70% FEV1 >80% predicted With or without chronic symptoms (cough,
sputum production)
Stage II Moderate COPD
FEV1/FVC <70% 50% <FEV1 <80% predicted With or without chronic symptoms (cough,
sputum production)

Stage III Severe COPD
FEV1/FVC <70% 30% <FEV1 <50% predicted With or without chronic symptoms (cough,
sputum production)

Stage IV Very Severe COPD
FEV1/FVC <70% FEV1 <30% predicted or FEV1 <50%
predicted plus chronic respiratory failure
Goals of Treatment: Emphysema & Chronic Bronchitis
Improved ventilation Remove secretions Prevent complications Slow progression of signs & symptoms Promote patient comfort and participation
in treatment

Collaborative Care: Emphysema & Chronic Bronchitis
Treat respiratory infection Monitor spirometry and PEFR Nutritional support Fluid intake 3 lit/day O2 as indicated

Collaborative Care: Medications
Anti-inflammatory Corticosteroids
Bronchodilators Beta-adrenergic agonist: Proventil Methylxanthines: Theophylline Anticholinergics: Atrovent
Mucolytics: Expectorants: Antihistamines:
Collaborative Care: Emphysema & Chronic Bronchitis
Client teaching Support to stop smoking Conservation of energy Breathing exercises
• Pursed lip breathing• Diaphragm breathing
Chest physiotherapy• Percussion, vibration• Postural drainage
Self-manage medications• Inhaler & oxygen equipment

Therapy by Stage- Pretty Simple

Bronchodilators Beta2-agonists
Short-acting Fenoterol Salbutamol (albuterol) Terbutaline
Long-acting Formoterol Salmeterol

BronchodilatorsAnticholinergics
Mode of Action Cholinergic tone is only reversible component of COPD Normal airway have small degree of vagal cholinergic
tone
Short-acting Ipratropium bromide Oxitropium bromide
Long-acting Tiotropium

Bronchodilators- Combos and Methylxanthines
Combination beta2-agonists plus anticholinergic in one inhaler Fenoterol/Ipratropium Salbutamol/Ipratropium
Methylxanthines Aminophylline (slow release preparations) Theophylline (slow release preparations) RARELY OF SIGNIFICNAT BENEFIT LEVEL 8-12 mcg/ml