1774.full.pdf
7
Risk Factors for Metabolic Syndrome Independently Predict Arterial Stiffness and Endothelial Dysfunction in Patients With Chronic Kidney Disease and Minimal Comorbidity PAJAREE LILITKARNTAKUL, MD 1 NEERAJ DHAUN, MBCHB, PHD 1,2 VANESSA MELVILLE, BSC 1 DEBBIE KERR, BSC 1 DAVID J. WEBB, MD, FRCP 1 JANE GODDARD, MBCHB, PHD 2 OBJECTIVEdMetabolic syndrome (MS) is common in patients with chronic kidney disease (CKD), but its contribution to arterial stiffness and endothelial dysfunction in CKD is not well defined. We hypothesized that risk factors for MS would independently predict arterial stiffness and endothelial dysfunction in CKD patients. RESEARCH DESIGN AND METHODSdRisk factors for MS, carotid-femoral pulse wave velocity (CF-PWV) and flow-mediated dilation (FMD) as measures of arterial stiffness and endothelial dysfunction, respectively, were assessed in 113 minimally comorbid CKD patients and in 23 matched control subjects. RESULTSdCF-PWV correlated with systolic blood pressure (SBP), waist circumference, and plasma glucose (r 2 = 0.25, 0.09, and 0.09; P , 0.01 for all). FMD correlated with SBP (r 2 = 0.09; P , 0.01) and waist circumference (r 2 = 0.03; P , 0.05). CF-PWV increased progressively (r 2 = 0.07; P , 0.01) with increasing number of risk factors for MS. In multiple linear regression, SBP and waist circumference were independent determinants of CF-PWV, whereas only SBP pre- dicted FMD. CONCLUSIONSdThe number of MS risk factors is an important determinant of arterial stiffness in CKD patients irrespective of the degree of renal impairment. Although BP remains the major determinant of arterial stiffness and endothelial dysfunction, waist circumference inde- pendently predicts arterial stiffness. MS risk factors, particularly abdominal girth, are potential targets for future interventional studies in patients with CKD. Diabetes Care 35:1774–1780, 2012 C hronic kidney disease (CKD) is common and associated with an in- creased risk of cardiovascular disease (CVD) (1). Conventional (Framingham) CVD risk factors, including high blood pressure (BP), hypercholesterolemia, and diabetes, all of which are common in CKD patients, only partly explain the high cardiovascular risk (2). CKD is now regarded as an independent risk factor for CVD (1,3), and we have recently shown that renal dysfunction also contributes to arterial stiffness and endothelial dysfunc- tion in a group of minimally comorbid CKD patients (4). Increased arterial stiffness, as mea- sured by pulse wave velocity (PWV), is a commonly recognized feature of CKD (4), a marker of cardiovascular risk (5,6), and an independent predictor of mortality and survival in dialysis patients (6). The vascu- lar endothelium is an important regulator of arterial stiffness (7), and endothelial dys- function is also a common feature of CKD (8) and a predictor of CVD (9). Metabolic syndrome (MS) is a clus- tering of metabolic abnormalities and risk factors for CVD and includes abdominal obesity, hyperglycemia, hypertension, hypertriglyceridemia, and reduced HDL cholesterol (10). As MS is associated with increased risks of diabetes and CVD (11,12), its treatment and prevention have become one of the major public health challenges worldwide. The risk factors for MS, either together or individ- ually, are also associated with arterial stiff- ness and endothelial dysfunction both in health (13,14) and disease (15,16). MS is widely prevalent in CKD (17) and is itself a risk factor for CKD (18). Although a recent study has suggested that MS and its risk factors contribute to arterial stiffness and endothelial dysfunc- tion in dialysis patients (19), there are no data relating to predialysis CKD. This is clearly important because targeting MS risk factors in early CKD may retard CKD progression, delaying the onset of dialysis and its associated morbidity, as well as reducing the overall risk of CVD. In this current study, we investigated the relationships of MS and its individual components to arterial stiffness and endo- thelial dysfunction in CKD patients across a wide range of renal function from early CKD to predialysis. Importantly, we planned to recruit patients without diabetes or car- diovascular comorbidity. We hypothesized that the presence of MS, or its components, would be associated with increased arterial stiffness and endothelial dys- function and that these relationships would be independent of renal function and other well-established risk factors for CVD. RESEARCH DESIGN AND METHODSdThe rationale and study design have been reported in detail else- where (4). In brief, subjects were recruited ccccccccccccccccccccccccccccccccccccccccccccccccc From the 1 Clinical Pharmacology Unit, Queen’s Medical Research Institute, University of Edinburgh, Edinburgh, U.K.; and the 2 Department of Renal Medicine, Royal Infirmary of Edinburgh, Edinburgh, U.K. Corresponding author: Jane Goddard, [email protected]. Received 2 December 2011 and accepted 14 March 2012. DOI: 10.2337/dc11-2345 This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10 .2337/dc11-2345/-/DC1. © 2012 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.org/ licenses/by-nc-nd/3.0/ for details. 1774 DIABETES CARE, VOLUME 35, AUGUST 2012 care.diabetesjournals.org Cardiovascular and Metabolic Risk O R I G I N A L A R T I C L E
-
Upload
hfathiardi -
Category
Documents
-
view
216 -
download
0
Transcript of 1774.full.pdf

Risk Factors for Metabolic SyndromeIndependently Predict Arterial Stiffnessand Endothelial Dysfunction in PatientsWith Chronic Kidney Disease andMinimal ComorbidityPAJAREE LILITKARNTAKUL, MD
1
NEERAJ DHAUN, MBCHB, PHD1,2
VANESSA MELVILLE, BSC1
DEBBIE KERR, BSC1
DAVID J. WEBB, MD, FRCP1
JANE GODDARD, MBCHB, PHD2
OBJECTIVEdMetabolic syndrome (MS) is common in patients with chronic kidney disease(CKD), but its contribution to arterial stiffness and endothelial dysfunction in CKD is not welldefined. We hypothesized that risk factors for MS would independently predict arterial stiffnessand endothelial dysfunction in CKD patients.
RESEARCH DESIGN AND METHODSdRisk factors for MS, carotid-femoral pulsewave velocity (CF-PWV) and flow-mediated dilation (FMD) as measures of arterial stiffnessand endothelial dysfunction, respectively, were assessed in 113 minimally comorbid CKDpatients and in 23 matched control subjects.
RESULTSdCF-PWV correlated with systolic blood pressure (SBP), waist circumference, andplasma glucose (r2 = 0.25, 0.09, and 0.09; P, 0.01 for all). FMD correlated with SBP (r2 = 0.09;P, 0.01) and waist circumference (r2 = 0.03; P, 0.05). CF-PWV increased progressively (r2 =0.07; P, 0.01) with increasing number of risk factors for MS. In multiple linear regression, SBPand waist circumference were independent determinants of CF-PWV, whereas only SBP pre-dicted FMD.
CONCLUSIONSdThe number of MS risk factors is an important determinant of arterialstiffness in CKD patients irrespective of the degree of renal impairment. Although BP remains themajor determinant of arterial stiffness and endothelial dysfunction, waist circumference inde-pendently predicts arterial stiffness. MS risk factors, particularly abdominal girth, are potentialtargets for future interventional studies in patients with CKD.
Diabetes Care 35:1774–1780, 2012
Chronic kidney disease (CKD) iscommon and associated with an in-creased risk of cardiovascular disease
(CVD) (1). Conventional (Framingham)CVD risk factors, including high bloodpressure (BP), hypercholesterolemia, anddiabetes, all of which are common inCKD patients, only partly explain thehigh cardiovascular risk (2). CKD is nowregarded as an independent risk factor forCVD (1,3), and we have recently shown
that renal dysfunction also contributes toarterial stiffness and endothelial dysfunc-tion in a group of minimally comorbidCKD patients (4).
Increased arterial stiffness, as mea-sured by pulse wave velocity (PWV), is acommonly recognized feature ofCKD (4), amarker of cardiovascular risk (5,6), and anindependent predictor of mortality andsurvival in dialysis patients (6). The vascu-lar endothelium is an important regulator
of arterial stiffness (7), and endothelial dys-function is also a common feature of CKD(8) and a predictor of CVD (9).
Metabolic syndrome (MS) is a clus-tering of metabolic abnormalities and riskfactors for CVD and includes abdominalobesity, hyperglycemia, hypertension,hypertriglyceridemia, and reduced HDLcholesterol (10). As MS is associated withincreased risks of diabetes and CVD(11,12), its treatment and preventionhave become one of the major publichealth challenges worldwide. The riskfactors for MS, either together or individ-ually, are also associated with arterial stiff-ness and endothelial dysfunction both inhealth (13,14) and disease (15,16).
MS is widely prevalent in CKD (17)and is itself a risk factor for CKD (18).Although a recent study has suggestedthat MS and its risk factors contribute toarterial stiffness and endothelial dysfunc-tion in dialysis patients (19), there are nodata relating to predialysis CKD. This isclearly important because targeting MSrisk factors in early CKD may retardCKD progression, delaying the onset ofdialysis and its associated morbidity, aswell as reducing the overall risk of CVD.
In this current study, we investigatedthe relationships of MS and its individualcomponents to arterial stiffness and endo-thelial dysfunction inCKDpatients across awide range of renal function from earlyCKD topredialysis. Importantly,weplannedto recruit patients without diabetes or car-diovascular comorbidity.We hypothesizedthat the presence ofMS, or its components,would be associated with increasedarterial stiffness and endothelial dys-function and that these relationshipswould be independent of renal functionand other well-established risk factors forCVD.
RESEARCH DESIGN ANDMETHODSdThe rationale and studydesign have been reported in detail else-where (4). In brief, subjects were recruited
c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c c
From the 1Clinical PharmacologyUnit, Queen’sMedical Research Institute, University of Edinburgh, Edinburgh,U.K.; and the 2Department of Renal Medicine, Royal Infirmary of Edinburgh, Edinburgh, U.K.
Corresponding author: Jane Goddard, [email protected] 2 December 2011 and accepted 14 March 2012.DOI: 10.2337/dc11-2345This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10
.2337/dc11-2345/-/DC1.© 2012 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and thework is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
1774 DIABETES CARE, VOLUME 35, AUGUST 2012 care.diabetesjournals.org
C a r d i o v a s c u l a r a n d M e t a b o l i c R i s kO R I G I N A L A R T I C L E

from the renal outpatient clinic at the RoyalInfirmary of Edinburgh. They were catego-rized into the five stages of CKD on thebasis of the Kidney Disease OutcomeQual-ity Initiative (K/DOQI) classification (20).Age-matched healthy volunteers were re-cruited from the community as a controlgroup.
The inclusion criteria were as follows:male or female CKD patients, 18–65 yearsold, and clinic BP #160/100 mmHg,whether or not on antihypertensive med-ication.We excluded patients with a renaltransplant or on dialysis, systemic vascu-litis or connective tissue disease, a historyof established CVD, peripheral vasculardisease, diabetes, respiratory or neuro-logic disease, and current alcohol abuseor pregnancy and those treated with anorganic nitrate or b-agonist. Patients con-tinued their usual medications until thestudy morning. Smokers and hypercho-lesterolemic patients were not excluded,but the latter had to be established on statinmedication, with good cholesterol control,for at least 3 months before taking part inthe study.
Diagnosis of MSMS was diagnosed according to the crite-ria from the third report of the NationalCholesterol Education Program (NCEP)expert panel on detection, evaluation, andtreatment of high blood cholesterol inadults (Adult Treatment Panel [ATP] III)(10,21). The diagnosis of MS was madewhen subjects had three or more risk fac-tors for MS. Subjects with zero to one andtwo risk factors for MS were classified asno MS and risk for developing MS, re-spectively (Supplementary Table 1).
MeasurementsBrachial systolic and diastolic BP (SBP andDBP) were recorded in duplicate, with anappropriately sized cuff, using a validatedoscillometric sphygmomanometer (OmronHEM-705CP) (22), and values were pre-sented as an average of two recordings.BMI was calculated as weight (kg)/(height[m])2. Waist and hip circumferences (cm)were measured on a subject in a standingposition with feet 15 cm apart. Waist cir-cumference was measured at themidpointbetween the iliac crest and lowest rib. Hipcircumference was measured at the mid-point between the waist and groin. Duringthe measurement, the tape measure wasparallel to the ground.
Arterial stiffness was assessed by mea-suring carotid-femoral PWV (CF-PWV),as previously described (23), using the
SphygmoCor apparatus (SphygmoCorBPAS-1; AtCor Medical, Sydney, Australia).Central augmentation index (cAIx) was esti-mated using the same system (23). Brachialartery flow-mediated dilation (FMD) wasused to assess endothelium-dependent vaso-motor function as described elsewhere (24).FMD was quantified as a percentage changefrom baseline in brachial artery diameter after5 min of forearm ischemia. Endothelium-independent vasomotor function was as-sessed using 25 mg nitroglycerine (NTG)by sublingual administration (25).
Renal function assessmentCreatinine clearance, as an estimate ofglomerular filtration rate (eGFR), wascalculated according to the Cockcroft andGault (C&G) equation (26): (140 2 age[years] 3 weight [kg] 3 1.23 for maleor 1.05 for female)/serum creatinine(mmol/L). The C&G equation was se-lected to assess renal function in thisstudy because it is more accurate thanthe Modification of Diet in Renal Disease(MDRD) equation when used to assessmild renal insufficiency (27). It was fur-ther corrected by body surface area.
Statistical analysesData were statistically analyzed usingSPSS program for Windows (SPSS 15.0;SPSS Inc., Chicago, IL). Descriptive dataare given as mean 6 SD unless otherwisestated. Means of the categorical data (sub-jects without MS, subjects with risk of
developing MS, and subjects with MS)were compared by one-way ANOVA.Continuous data (risk factors for MS aszero to five risk factors) were analyzedby correlation coefficients calculated us-ing the Pearson method. Stepwise linearregression was used for multivariateanalysis. A significant level was taken asP value ,0.05.
RESULTSdCKD patients (n = 113) andage-matched non-CKD control subjects(n = 23) were enrolled into the study. Base-line characteristics of the studied subjectsare given in Supplementary Table 2.Causes of CKD and medication used bythe patients are described in Supplemen-tary Table 3.
Subjects were classified into threecategories according to the number of riskfactors for MS (see RESEARCH DESIGN AND
METHODS). Twenty-six subjects (19%) hadMS and 27 (20%) were defined as at riskfor developing MS. All three categorieswere comparable in respect to age andeGFR. As expected, subjects with MShad a higher BMI, waist circumference,SBP, DBP, plasma glucose, and triglycer-ides and lower HDL cholesterol comparedwith those without MS or those at risk fordeveloping it (Table 1). With regard to therelationship of the risk factors for MS torenal function, only SBP increased as eGFRdeclined (r2 =0.11;P,0.01);waist circum-ference, DBP, plasma glucose, triglycerides,and HDL cholesterol showed no
Table 1dRisk factors for MS, arterial stiffness, and endothelial function
No MS Risk for MS MS
N 83 27 26Male/female (n) 50/33 18/9 20/6Smoker/nonsmoker (n) 14/69 2/25 9/17Age (years) 46 6 10 49 6 11 50 6 8eGFR (mL/min/1.73 m2) 73 6 34 65 6 33 59 6 36BMI (kg/m2)* 26 6 4 28 6 5 33 6 4Risk factors for MSWaist circumference (cm)* 90 6 11 96 6 13 111 6 12SBP (mmHg)* 113 6 13 124 6 15 124 6 13DBP (mmHg)* 72 6 10 76 6 8 76 6 8Glucose (mmol/L)* 4.8 6 0.5 5.1 6 0.5 5.4 6 0.6Triglycerides (mmol/L)* 1.1 6 0.4 1.4 6 0.8 2.4 6 1.2HDL cholesterol (mmol/L)* 1.4 6 0.3 1.2 6 0.3 0.9 6 0.2
Arterial stiffness and endothelialdysfunction
CF-PWV (m/s)* 6.4 6 1.0 7.0 6 1.4 7.5 6 1.7cAIx (%) 22 6 13 22 6 13 25 6 11FMD (%) 4.8 6 2.9 3.4 6 2.8 3.5 6 2.8NTG (%) 12.4 6 5.2 10.6 6 4.1 10.2 6 4.6
No MS, subjects with zero to one risk factor for MS; risk for MS, subjects with two risk factors for MS; MS,subjects with three or more risk factors for MS. *P , 0.05 for one-way ANOVA by MS groups.
care.diabetesjournals.org DIABETES CARE, VOLUME 35, AUGUST 2012 1775
Lilitkarntakul and Associates

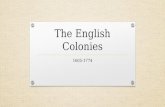
relationship to renal function. CF-PWVwas higher in the MS group (Table 1 andFig. 1A and C) whereas cAIx showed norelationship to MS (Table 1). FMD waslower in the MS group and subjects atrisk for MS compared with those withoutMS (Table 1 and Fig. 1B and D) but thisdid not reach statistical significance. Theendothelium-independent response toNTG had no relationship to MS (Table 1).
Relationships and predictors ofarterial stiffnessUnivariate analysis to assess the relation-ship of CF-PWV to individual MS risk
factors, the number of MS risk factors,and related parameters that are not in-cluded in the National Cholesterol Edu-cation Program (NCEP) ATP III criteria(eGFR, age, BMI, and waist-to-hip ratio)was performed. CF-PWV only correlatedwith eGFR when all subjects were con-sidered together (r2 = 0.07; P, 0.01) butnot when split into the three groups ac-cording to the presence, risk, or absenceof MS (Fig. 1A). However, PWV in subjectswith MS was significantly higher than insubjects without MS (Fig. 1A and C).With regard to the individual risk factorsfor MS, CF-PWV increased with waist
circumference, waist-to-hip ratio, SBP,and plasma glucose (Fig. 2A–D). Addition-ally, CF-PWV correlated with age (r2 =0.25; P , 0.01), BMI (r2 = 0.06; P ,0.01), DBP (r2 = 0.07; P , 0.01), andplasma triglycerides (r2 = 0.05; P , 0.05)but not sex, smoking status, or HDLcholesterol.
In multivariate analysis, when renalfunction and conventional risk factorswere entered into the model, age and sexwere independent predictors of arterialstiffness (Table 2, model 1). When eitherthe presence of MS or the number of riskfactors for MS that a subject had were
Figure 1dScatter and box plots showing associations between the number of the MS risk factors and CF-PWV (A and C) and FMD (B and D). NoMS (○, solid fitted line), subjects without MS (zero to one risk factor); risk for MS (-, long-dashed fitted line), subjects at risk for developing MS(two risk factors); MS (4, short-dashed fitted line), subjects with MS (three or more risk factors). P values are for one-way ANOVA (C and D).
1776 DIABETES CARE, VOLUME 35, AUGUST 2012 care.diabetesjournals.org
Metabolic syndrome and vascular dysfunction in CKD

considered, both of them, together with ageand sex, independently predicted CF-PWV(Table 2, models 2 and 3). When the indi-vidual risk factors for MS were considered,sex was replaced by waist circumference,SBP, and DBP as independent predictorsof CF-PWV (Table 2, model 4).
Relationship and predictors ofendothelial dysfunctionIn univariate analysis, FMD correlatedwith eGFR when all subjects were con-sidered together (r2 = 0.04; P , 0.05)but not when subjects were divided intothe three MS groups. FMD did not changeaccording to the presence, risk, or absenceofMS (Fig. 1B andD). FMD correlatedwithwaist circumference, waist-to-hip ratio, andSBP but not plasma glucose (Fig. 2E–H).Additionally FMD did not correlate withage, BMI, DBP, plasma triglycerides, HDLcholesterol, or smoking status.
In multivariate analysis assessing re-nal function and conventional risk fac-tors, eGFR was an independent predictorof FMD (Table 2, model 1). Although thepresence or absence of MS did not predictendothelial dysfunction, the number ofMS risk factors did (Table 2, models 2and 3). When the risk factors for MS wereconsidered individually in the model, SBPand DBP alone were independent predic-tors of FMD (Table 2, model 4).
CONCLUSIONSdIn a cohort of sub-jects withminimal comorbidity and an eGFRranging from 8 to 154 mL/min/1.73 m2,wehavepreviously shown that renal functionis related to an increase in arterial stiffnessand endothelial dysfunction, as measuredby CF-PWV and FMD, respectively (4). Wenow show that subjects in this cohort withMS have increased arterial stiffness com-pared with those without MS. Importantly,this is independent of the level of renal func-tion (eGFR). Both the presence of MS andthe number of MS risk factors are indepen-dent predictors of arterial stiffness in this co-hort. Furthermore, when risk factors for MSwere considered individually, waist circum-ference and blood pressure were determi-nants of arterial stiffness, independent ofrenal function, age, sex, and smoking status.
Our study cohort was carefully se-lected to have low comorbidity. Thus, theprevalence of MS in this CKD populationis lower than previously reported in di-alysis (19,28), hypertensive (15), and di-abetic patients (16) but is comparable tohealthy subjects (18 vs. 10–19%) (14).Interestingly, despite this selection biasagainst MS and its risk factors, we have
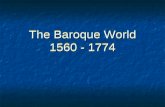
Figure 2dScatter plots showing correlations between CF-PWV and waist circumference (A),waist-to-hip ratio (B), SBP (C), and plasma glucose (D). Scatter plots showing correlationsbetween FMD and waist circumference (E), waist-to-hip ratio (F), SBP (G), and plasma glucose(H). Male:-, dashed line; female: ○, solid line.
care.diabetesjournals.org DIABETES CARE, VOLUME 35, AUGUST 2012 1777
Lilitkarntakul and Associates

shown that, irrespective of renal function,there is an increase in arterial stiffness inour subjects with MS or risk factors forMS, and that these independently predictarterial stiffness when considered along-side conventional risk factors. This find-ing is in keeping with previous data fromhealthy subjects (13,14,29,30), hyperten-sive patients (15), and patients with dia-betes (16).
Our data also show that waist circum-ference is a predictor of arterial stiffness inthis population and this is independentof renal function, age, BP, and sex. Ouranalysis considered the whole cohort of113 CKD patients and 23 age-matched,non-CKD control subjects, but waist cir-cumference remains an independent pre-dictor of arterial stiffness when the CKDpatients are considered alone. This haspreviously only been shown in hyperten-sive patients (15). Obesity is associatedboth with increased arterial stiffness (31)
and an increased risk of CVD (32). Ourdata suggest that, in patients with CKD,waist circumference, a marker of centralobesity, may be a better surrogate for arte-rial stiffness than BMI or cholesterol sub-types such as HDL cholesterol andtriglycerides.
In the current study, subjects withMSdid not have significantly impaired endo-thelial function compared with thosewithout MS, regardless of renal function.This is similar to data from studies inhealthy subjects (33,34), those at risk fordeveloping diabetes (35,36), and thosewith peripheral vascular disease (37).However, in a study of ;1,000 elderlysubjects, including those with CVD anddiabetes, where endothelial function wasassessed using both an invasive forearmtechnique and FMD (38), the formershowed significantly impaired endothe-lial function in the MS group. The inva-sive forearm technique is considered to
assess vascular function of the resistance ar-teries, whereas FMD is a measure of conduitartery function. Thus, it is possible that MSis associated with a predominant dysfunc-tion of the resistance vessels and, hence, byusing FMD, we did not detect significantendothelial dysfunction in our study cohort.We also observed no association betweenthe number of risk factors for MS andFMD. This is in contrast to a previous studyin subjects at risk for developing diabetes(36), but this may in part be explained bygenetic influences in diabetes (and insulinresistance states) not currently consideredto be of importance in the majority ofCKD patients.
Of all the risk factors studied here,conventional and MS related, only BP isan independent predictor of endothelialdysfunction (Table 2, model 4). This re-sult both confirms and contradicts thoseof previous studies. Similar to our find-ings, Scuteri et al. (35) found BP (bothSBP and DBP) to be an independent pre-dictor of endothelial dysfunction in nor-moglycemic first-degree relatives ofpatients with diabetes. However, Kovaiteet al. (29) found this not to be the casewhen studying 186 “asymptomatic sub-jects without overt cardiovascular disease.”Notably, one-third of subjects studied ful-filled criteria for MS. A study in CKD hasshown that, similar to the current data, re-nal function is a predictor of endothelialdysfunction (39). However, this studywas performed in CKD patients with dia-betes and this may act as a significant con-founder. Furthermore, in that study, aninvasive forearm technique measured en-dothelial function in a different vascularbed compared with the technique of FMDused in the current study.
Interestingly, we found an inverseassociation between DBP and CF-PWV(Table 2) and a positive association be-tween DBP and FMD (Table 2). However,these may be explained by an effect ofpulse pressure, which is positively associ-ated with CF-PWV and inversely relatedto FMD, since both SBP and DBP wereentered into the analysis.
We recognize some limitations to thecurrent study. There are several criteriafor the diagnosis of MS (14). As our pa-tients were not diabetic, we cannot use thecriteria proposed by the World HealthOrganization and, therefore, the evaluationof an effect of insulin resistance to arterialstiffness and endothelial dysfunction is lim-ited and does not allow data comparisonwith other studies using World Health Or-ganization criteria. Also, an increased girth
Table 2dMultivariate analysis of renal function, conventional cardiovascular risk factors,and risk factors for MS, as independent predictors for CF-PWV and FMD
CF-PWV
Predictors Model 1 Model 2 Model 3 Model 4
eGFR 20.11 20.11 20.12 20.11Age 0.52* 0.49* 0.47* 0.39*Sex (male/female) 0.18† 0.15† 0.16† 0.01Smoking status (yes/no) 20.09 20.14 20.10 20.03Presence of MS (yes/no) d 0.20* d dNumber of MS risk factors (0–5) d d 0.23* dWaist circumference d d d 0.24*SBP d d d 0.53*DBP d d d 20.27*Plasma glucose d d d 0.03Triglycerides d d d 0.06HDL cholesterol d d d 20.09r2 0.28* 0.31* 0.32* 0.48*
FMD
Predictors Model 1 Model 2 Model 3 Model 4
eGFR 0.02† 0.02† 0.18† 0.10Age 20.10 20.10 20.07 20.05Sex (male/female) 20.11 20.11 20.11 20.06Smoking status (yes/no) 20.02 20.02 20.01 20.02Presence of MS (yes/no) d 20.10 d dNumber of MS risk factors (0–5) d d 20.18† dWaist circumference d d d 20.14SBP d d d 20.50*DBP d d d 0.28†Plasma glucose d d d 20.02Triglycerides d d d 20.05HDL cholesterol d d d 0.08r2 0.04† 0.04† 0.07† 0.12*
The table gives standard regression coefficients (b values). *P , 0.01. †P , 0.05.
1778 DIABETES CARE, VOLUME 35, AUGUST 2012 care.diabetesjournals.org
Metabolic syndrome and vascular dysfunction in CKD

has the potential to artifactually increasethe measurement entered for the distancetraveled by the pulse wave (compared withthe actual distance) in calculating PWV.Thus, the reported PWV will be higherthan the “true” value. It is possible that thisis responsible, in part, for the higher PWV inthe MS group in this study. However, oursubjects were chosen because of low comor-bidity and are not typical of “general” CKDpatients (including patients with diabetes)particularly in their body habitus. MedianBMI was 26.9 kg/m2, and the patient withthe highest BMI did not have MS by ATP IIIcriteria. Additionally, the 54 patients whosewaist measurement was above the defininglevel for a risk factor for MS were spreadthroughout the three groups: 16 patientswere in the “no MS” group, 17 in the “riskof MS” group, and 21 in the “MS” group.Some of the medications taken by our pa-tients, such as angiotensin-convertingenzyme inhibitors, angiotensin receptorblockers, b-blockers, and statins, may havehad effects on both CF-PWV and FMD.However, all patients were stabilized ontheir therapies and did not receive theirmedications on the study day until aftermeasurements weremade. The low numberof smokers in this study may be responsiblefor the lack of expected relationships be-tween smoking status and both arterialstiffness and endothelial dysfunction; al-though when only the CKD patients areconsidered in the multivariate analysis,smoking is an independent predictor ofPWV in models 2 and 3. Finally, as thiswas a cross-sectional study, we cannot fullydefine the causal relationships behind theassociations described, though they dohave a sound mechanistic basis.
In summary, the current study showsthat, in the absence of CVD and diabetesand irrespective of renal function, age,smoking status, and sex, CKD patientswith MS have increased arterial stiffnesscompared with those without MS but nodifference in endothelial function. AlthoughBP remains the strongest determinant ofboth arterial stiffness and endothelial dys-function, the presence of MS or its riskfactors is also an important determinant ofarterial stiffness in this CKD cohort. Impor-tantly, waist circumference is an indepen-dent predictor of arterial stiffness in thiscohort; hence, educationon lifestyle changesand weight management interventionsoffer a different therapeutic perspective,complementary to drug management oftraditional cardiovascular risk factors, suchas hypertension and hypercholesterolemia,that should not be overlooked in patient
care. Given these currently noncomorbidpatients in this cohort only had modestincreases in BMI, the early and aggressivecontrol of weight should be a focus forintervention. As this is not related torenal function, it provides an additionaltarget for therapies aimed at improvingcardiovascular outcomes at all stages ofCKD.
AcknowledgmentsdThis study was fundedby a British Heart Foundation project grant(PG/05/91). P.L. was supported by the RoyalThai Government for her PhD training. Thiswork was undertaken within Edinburgh’sBritish Heart Foundation Centre of ResearchExcellence.No potential conflicts of interest relevant to
this article were reported.P.L. designed and performed the study and
prepared the manuscript. N.D. designed thestudy and revised and edited the manuscript.V.M. and D.K. performed the study. D.J.W.and J.G. designed and supervised the studyand revised and edited the manuscript. J.G. isthe guarantor of this work and, as such, hadfull access to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.This study was presented in poster form at
the 10th International Conference on Endo-thelin, Bergamo, Italy, 16–19 September 2007,and the American Society of Nephrology An-nual Meeting, San Francisco, California, 31October–5 November 2007.
References1. Sarnak MJ, Levey AS, Schoolwerth AC,
et al.; American Heart Association Coun-cils on Kidney in Cardiovascular Disease,High Blood Pressure Research, ClinicalCardiology, and Epidemiology and Pre-vention. Kidney disease as a risk factor fordevelopment of cardiovascular disease:a statement from the American Heart As-sociation Councils on Kidney in Cardio-vascular Disease, High Blood PressureResearch, Clinical Cardiology, and Epi-demiology and Prevention. Circulation2003;108:2154–2169
2. Zoccali C. Traditional and emerging car-diovascular and renal risk factors: an epi-demiologic perspective. Kidney Int 2006;70:26–33
3. Schiffrin EL, Lipman ML, Mann JF. Chronickidney disease: effects on the cardiovascularsystem. Circulation 2007;116:85–97
4. Lilitkarntakul P, Dhaun N, Melville V, et al.Blood pressure and not uraemia is the majordeterminant of arterial stiffness and endo-thelial dysfunction in patients with chronickidney disease and minimal co-morbidity.Atherosclerosis 2011;216:217–225
5. Guérin AP, Pannier B, Métivier F, MarchaisSJ, London GM. Assessment and signifi-cance of arterial stiffness in patients withchronic kidney disease. Curr OpinNephrolHypertens 2008;17:635–641
6. Blacher J, Guerin AP, Pannier B, MarchaisSJ, SafarME, LondonGM. Impact of aorticstiffness on survival in end-stage renaldisease. Circulation 1999;99:2434–2439
7. Wilkinson IB, Franklin SS, Cockcroft JR.Nitric oxide and the regulation of large arterystiffness: from physiology to pharmacology.Hypertension 2004;44:112–116
8. van Guldener C, Lambert J, Janssen MJ,Donker AJ, Stehouwer CD. Endothelium-dependent vasodilatation and distensibilityof large arteries in chronic haemodialysispatients. Nephrol Dial Transplant 1997;12(Suppl 2):14–18
9. Perticone F, Ceravolo R, Pujia A, et al.Prognostic significance of endothelial dys-function in hypertensive patients. Circula-tion 2001;104:191–196
10. Grundy SM, Brewer HB Jr, Cleeman JI,Smith SC Jr, Lenfant C; American HeartAssociation; National Heart, Lung, andBlood Institute. Definition of metabolicsyndrome: report of the National Heart,Lung, and Blood Institute/American HeartAssociation conference on scientific issuesrelated to definition. Circulation 2004;109:433–438
11. Ahluwalia N, Drouet L, Ruidavets JB, et al.Metabolic syndrome is associated withmarkers of subclinical atherosclerosis in aFrench population-based sample. Ath-erosclerosis 2006;186:345–353
12. Sattar N, Gaw A, Scherbakova O, et al.Metabolic syndrome with and withoutC-reactive protein as a predictor of coronaryheart disease and diabetes in the West ofScotland Coronary Prevention Study. Cir-culation 2003;108:414–419
13. van Popele NM,Westendorp IC, Bots ML,et al. Variables of the insulin resistancesyndrome are associated with reduced ar-terial distensibility in healthy non-diabeticmiddle-aged women. Diabetologia 2000;43:665–672
14. Ferreira I, Boreham CA, Twisk JW, et al.Clustering of metabolic syndrome riskfactors and arterial stiffness in youngadults: the Northern Ireland YoungHeartsProject. J Hypertens 2007;25:1009–1020
15. Schillaci G, Pirro M, Vaudo G, et al. Met-abolic syndrome is associated with aorticstiffness in untreated essential hyperten-sion. Hypertension 2005;45:1078–1082
16. Martens FM, van der Graaf Y, Dijk JM,Olijhoek JK, Visseren FL. Carotid arterialstiffness is marginally higher in the meta-bolic syndrome and markedly higher intype 2 diabetes mellitus in patients withmanifestations of arterial disease. Athero-sclerosis 2008;197:646–653
17. Johnson DW, Armstrong K, Campbell SB,et al. Metabolic syndrome in severe chronickidney disease: prevalence, predictors,
care.diabetesjournals.org DIABETES CARE, VOLUME 35, AUGUST 2012 1779
Lilitkarntakul and Associates

prognostic significance and effects of riskfactor modification. Nephrology (Carlton)2007;12:391–398
18. Chen J, Muntner P, Hamm LL, et al. Themetabolic syndrome and chronic kidneydisease inU.S. adults. Ann InternMed 2004;140:167–174
19. Zhe XW, Zeng J, Tian XK, et al. Pulse wavevelocity is associated with metabolic syn-drome components in CAPD patients. AmJ Nephrol 2008;28:641–646
20. Anonymous; National Kidney Founda-tion. K/DOQI clinical practice guidelinesfor chronic kidney disease: evaluation, clas-sification, and stratification. Am JKidneyDis2002;39(Suppl. 1):S1–S266
21. Anonymous; National Cholesterol Edu-cation Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment ofHigh Blood Cholesterol in Adults (AdultTreatment Panel III). Third Report of theNational Cholesterol Education Program(NCEP) Expert Panel on Detection, Eval-uation, and Treatment of High BloodCholesterol in Adults (Adult TreatmentPanel III) final report. Circulation 2002;106:3143–3421
22. O’Brien E, Mee F, Atkins N, Thomas M.Evaluation of three devices for self-measurement of blood pressure accordingto the revised British Hypertension SocietyProtocol: the Omron HEM-705CP, PhilipsHP5332, and Nissei DS-175. Blood PressMonit 1996;1:55–61
23. Wilkinson IB, Fuchs SA, Jansen IM, et al.Reproducibility of pulse wave velocity andaugmentation index measured by pulsewave analysis. J Hypertens 1998;16:2079–2084
24. Corretti MC, Anderson TJ, Benjamin EJ,et al.; International Brachial Artery ReactivityTask Force. Guidelines for the ultrasound
assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery:a report of the International Brachial ArteryReactivity Task Force. J Am Coll Cardiol2002;39:257–265
25. Oliver JJ, Bowler A, Beudeker Q, Cate T,Webb DJ. Dose-response relationship ofsublingual nitroglycerin with brachial ar-tery dilatation and change in central andperipheral augmentation index. Clin Phar-macol Ther 2005;77:337–338
26. Cockcroft DW, Gault MH. Prediction ofcreatinine clearance from serum creati-nine. Nephron 1976;16:31–41
27. Mafham MM, Niculescu-Duvaz I, Barron J,et al. A practical method of measuring glo-merular filtration rate by iohexol clearanceusing dried capillary blood spots. NephronClin Pract 2007;106:c104–c112
28. Young DO, Lund RJ, Haynatzki G, DunlayRW. Prevalence of the metabolic syn-drome in an incident dialysis population.Hemodial Int 2007;11:86–95
29. Kovaite M, Petrulioniene Z, Ryliskyte L,et al. Systemic assessment of arterial wallstructure and function in metabolic syn-drome. Proc West Pharmacol Soc 2007;50:123–130
30. Czernichow S, Bertrais S, Blacher J, et al.;SU.VI.MAX. Vascular Study. Metabolicsyndrome in relation to structure andfunction of large arteries: a predominanteffect of blood pressure. A report from theSU.VI.MAX. Vascular Study. Am J Hy-pertens 2005;18:1154–1160
31. Orr JS, Gentile CL, Davy BM, Davy KP.Large artery stiffening with weight gain inhumans: role of visceral fat accumulation.Hypertension 2008;51:1519–1524
32. Elsayed EF, SarnakMJ, Tighiouart H, et al.Waist-to-hip ratio, body mass index, and
subsequent kidney disease and death. AmJ Kidney Dis 2008;52:29–38
33. Wendelhag I, Fagerberg B, Hulthe J,Bokemark L, Wikstrand J. Endothelium-dependent flow-mediated vasodilatation,insulin resistance and the metabolic syn-drome in 60-year-old men. J Intern Med2002;252:305–313
34. Mattsson N, Rönnemaa T, Juonala M,et al. Arterial structure and function inyoung adults with the metabolic syn-drome: the Cardiovascular Risk in YoungFinns study. Eur Heart J 2008;29:784–791
35. Scuteri A, Tesauro M, Rizza S, et al. En-dothelial function and arterial stiffness innormotensive normoglycemic first-degreerelatives of diabetic patients are inde-pendent of the metabolic syndrome. NutrMetab Cardiovasc Dis 2008;18:349–356
36. Ghiadoni L, Penno G, Giannarelli C, et al.Metabolic syndrome and vascular alter-ations in normotensive subjects at risk ofdiabetes mellitus. Hypertension 2008;51:440–445
37. Golledge J, Leicht AS, Crowther RG, et al.Determinants of endothelial function in acohort of patients with peripheral arterydisease. Cardiology 2008;111:51–56
38. Lind L. Endothelium-dependent vaso-dilation, insulin resistance and the me-tabolic syndrome in an elderly cohort:the Prospective Investigation of theVasculature in Uppsala Seniors (PIVUS)study. Atherosclerosis 2008;196:795–802
39. Annuk M, Lind L, Linde T, Fellström B.Impaired endothelium-dependent vaso-dilatation in renal failure in humans.Nephrol Dial Transplant 2001;16:302–306
1780 DIABETES CARE, VOLUME 35, AUGUST 2012 care.diabetesjournals.org
Metabolic syndrome and vascular dysfunction in CKD