17 TECHNIQUE TO MAKE - Aligarh Muslim University TO MAKE.pdfcobalt chromium metal.(fig:4)The denture...
7
ABSTRACT:The fracture of acrylic resin denture is an unresolved problem in removable prosthodontics despite numerous attempts to determine causes. Midline fracture was the most common problem of these 71% midline fracture seen in maxillary denture and in mandibular denture its 29%. Fractures in Reinforcement has been attempted through the incorporation of solid metal forms and various types of fibers in fracture-prone areas. Metals can be added in the form of wire, plates, nets or fillers. The present case series deal with oral rehabilitation of maxillary and mandibular arch by incorporating various reinforcement material in denture base to combat the masticatory forces and improve the longevity of the prosthetic replacement at the same time prevent resorption of the underlying residual ridge. 1 2 3 Abbad Nikhil, Srivastava Rajeev, Choukse Vivek Modern Dental College And Research Centre INTRODUCTION: Patients who has become entirely edentulous in one jaw and retaining either or all or some of natural teeth in the others with several difficulties in providing successful single complete denture is common1. Fracture of an acrylic resin denture base can be a problem in prosthodontics1,2,3. The material most commonly used for the fabrication of dentures is the acrylic resin, poly methyl methacrylate4,5. This material is not ideal in every respect and it is the combination of properties rather than one single desirable property that accounts for its popularity and usage5,6. Causes of fractures include occlusal disharmony, flexure and fatigue of the denture base as a result of alveolar resorption and impact as a result of dropping the denture5,6,7. Midline fracture was the most common type of fracture during the period of study 195(61%)8.The midline fracture in a denture is often a result of flexural fatigue 2,6. There are many different approaches to solve the problems of repeated denture fracture2,9,10,11. Through this case series denture reinforced with metal, Denture reinforced with metal mesh have been discuss although there are three routes which improve the impact properties of PMMA alternative material to PMMA; the chemical modification of PMMA such as by the addition of a rubber graft copolymer; and the reinforcement of PMMA with other materials such as carbon fibers, glass fibers and ultra-high modulus polyethylene4,10. Advantages of metal denture base: (1) They have excellent strength to volume ratios and may be cast in thin sheets maintaining rigidity and fracture resistance4.(2) Thinner metallic denture base decrease interference with phonation12.(3) They display desirable dimensional characteristics and may be cast accurately4,9.(4) More retentive12.(5) Deform less during lateral mandibular function.(6) High thermal significant conductors12,13. Disadvantages of metal denture base: (1) There is increased cost, difficulty in fabrication, difficult to rebase4. (2) They may be indicated when polymer-based systems fail to provide acceptable physical properties.(3) Time consuming and added steps needed.(4) Encroachment of interocclusal space.(5) Weight of the denture may be inconvenient initially4,12. Indications of metal denture base: (1) Patients with atrophied ridges.(2) Patient with compromised neuromuscular coordination, who may drop their dentures.(3) Patients with increased rate of residual ridge resorption. a. Like postmenopausal women b. Diabetic patients.(4) Patients with flabby tissues which may require soft liner.(5) Patients who TECHNIQUE TO MAKE SINGLE COMPLETE DENTURES ROBUST: CASE SERIES Journal of Dental Sciences University University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 78 University J Dent Scie 2017; No. 3, Vol. 2 Case Report Keywords- Residual ridge resorption, metal denture base, single complete denture, metal reinforced denture, metal mesh. Source of support : Nil Conflict of interest: None
Transcript of 17 TECHNIQUE TO MAKE - Aligarh Muslim University TO MAKE.pdfcobalt chromium metal.(fig:4)The denture...

ABSTRACT:The fracture of acrylic resin denture is an unresolved problem in removable
prosthodontics despite numerous attempts to determine causes. Midline fracture was the most
common problem of these 71% midline fracture seen in maxillary denture and in mandibular
denture its 29%. Fractures in Reinforcement has been attempted through the incorporation of
solid metal forms and various types of fibers in fracture-prone areas. Metals can be added in the
form of wire, plates, nets or fillers. The present case series deal with oral rehabilitation of
maxillary and mandibular arch by incorporating various reinforcement material in denture base
to combat the masticatory forces and improve the longevity of the prosthetic replacement at the
same time prevent resorption of the underlying residual ridge.
1 2 3Abbad Nikhil, Srivastava Rajeev, Choukse Vivek
Modern Dental College And Research Centre
INTRODUCTION: Patients who has become entirely
edentulous in one jaw and retaining either or all or some of
natural teeth in the others with several difficulties in
providing successful single complete denture is common1.
Fracture of an acrylic resin denture base can be a problem in
prosthodontics1,2,3. The material most commonly used for
the fabrication of dentures is the acrylic resin, poly methyl
methacrylate4,5. This material is not ideal in every respect
and it is the combination of properties rather than one single
desirable property that accounts for its popularity and
usage5,6. Causes of fractures include occlusal disharmony,
flexure and fatigue of the denture base as a result of alveolar
resorption and impact as a result of dropping the denture5,6,7.
Midline fracture was the most common type of fracture
during the period of study 195(61%)8.The midline fracture in
a denture is often a result of flexural fatigue 2,6. There are
many different approaches to solve the problems of repeated
denture fracture2,9,10,11. Through this case series denture
reinforced with metal, Denture reinforced with metal mesh
have been discuss although there are three routes which
improve the impact properties of PMMA alternative material
to PMMA; the chemical modification of PMMA such as by
the addition of a rubber graft copolymer; and the
reinforcement of PMMA with other materials such as carbon
fibers, glass fibers and ultra-high modulus polyethylene4,10.
Advantages of metal denture base: (1) They have excellent
strength to volume ratios and may be cast in thin sheets
maintaining rigidity and fracture resistance4.(2) Thinner
metallic denture base decrease interference with
phonation12.(3) They display desirable dimensional
characteristics and may be cast accurately4,9.(4) More
retentive12.(5) Deform less during lateral mandibular
function.(6) High thermal significant conductors12,13.
Disadvantages of metal denture base: (1) There is increased
cost, difficulty in fabrication, difficult to rebase4. (2) They
may be indicated when polymer-based systems fail to provide
acceptable physical properties.(3) Time consuming and
added steps needed.(4) Encroachment of interocclusal
space.(5) Weight of the denture may be inconvenient
initially4,12.
Indications of metal denture base: (1) Patients with atrophied
ridges.(2) Patient with compromised neuromuscular
coordination, who may drop their dentures.(3) Patients with
increased rate of residual ridge resorption. a. Like
postmenopausal women b. Diabetic patients.(4) Patients with
flabby tissues which may require soft liner.(5) Patients who
TECHNIQUE TO MAKE SINGLE COMPLETE DENTURES ROBUST: CASE SERIES
Journal of Dental Sciences
University
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 78
University J Dent Scie 2017; No. 3, Vol. 2
Case Report
Keywords-
Residual ridge
resorption, metal denture
base, single complete
denture, metal reinforced
denture, metal mesh.
Source of support : Nil
Conflict of interest: None

are allergic to metal, with a history of denture
fractures4,12,13,14,15.
Materials used for metal denture base: Cr-Co – most retentive,
Ni – Cr, Titanium etc4,10,12,13,14,15..
Case report 1: (Metal denture)
A 70-year-old male patient, reported to the Department of
Prosthodontics (Institute of dental sciences) with a chief
complaint of recurrent fracture of maxillary single complete
denture.
Intraoral examination revealed shallow palatal vault, high
frenal attachment on buccal side bilaterally and opposing
mandibular natural dentition with few edentulous area.
Missing 31,32,35,36,41,42,44,46.(Fig:1). Mucosa was
normal and opposing dentition required minor alterations.
Saliva was of medium consistency and patient was
cooperative and philosophical according to House
classification. His primary concern for the new denture was a
denture with increased strength. Appropriate treatment plan
was formulated taking into consideration. Considering all the
factors and history of denture fractures, metal denture base
was planned for the patient12,13,14,15.
Impression of the lower natural teeth was made with an
irreversible hydrocolloid material and the dental stone
diagnostic cast was poured. Preliminary impression of the
edentulous maxilla was made with impression compound and
plaster cast was poured for the fabrication of a customtray.
The peripheral tracing procedures were completed tray with
green stick impression compound and the secondary
impression was made with zinc oxide eugenol impression
material.(fig:2) Master cast was made with dental stone type
IIIand the mold of the same was made with reversible
hydrocolloid (agar) and a refractory cast was poured with
phosphate bonded investment material. On the refractory cast
the denture base pattern wax was adapted and sprues were
attached and invested. The denture base was casted with
cobalt chromium metal.(fig:4)The denture base covered the
palate and residual ridges and the posterior palatal seal area
for mechanical retention of acrylic resin and teeth to the
metal12,13,14,15.
The vertical dimension of occlusion was established and
occlusion rim on the maxillary denture base was constructed
and contoured for adequate lip support in the anterior region
to simulate the vertical and horizontal overlap of the anterior
teeth. The anterior region of the occlusal rim had the same
thickness as the incisal edges of the anterior teeth to allow for
this vertical overlap. After this with the face bow orientation
jaw relation recorded and transferred on the Hanau wide
articulator.(fig: 5). After this with the help of functional chew
in method the centric is recorded. Cast partial was planned for
lower arch after alginate impression mouth preparation was
done and putty light body final impression was made. The
final cast was duplicated in agar and refractory cast was
poured (fig:6)
Arrangement of the artificial teeth was carried out to revel the
necessary changes to be made on the lower teeth. Adjustment
in the artificial teeth were incorporated in the preference to
making changes to the natural teeth.(fig:7) A trial of waxed up
maxillary complete denture was made followed by
acrylization of complete denture with heat polymerized
acrylic resin.(fig:8) The interference in denture were
eliminated and denture given to the patient.(fig:9) Post
insertion instruction were given to the patient regarding its
maintenance and hygiene12,13,14,15.
Fig. 1 a)
b)
c)
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 79
University J Dent Scie 2017; No. 3, Vol. 2

Fig. 2 a) b)
Fig.3 c) d)
Fig. 4 a b) c)
d) e)
Fig. 5 a)
Fig. 6 a) b)
c) d)
Fig. 7 a)
b)
Fig. 8 a)
b)
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 80
University J Dent Scie 2017; No. 3, Vol. 2

Fig. 9 a) b)
Case report 2: (Metal mesh denture)
A completely edentulous 59 year old male good general
health, reported to the Department of Prosthodontics, Crown
and Bridge (Institute of dental sciences) with a history of
repeated fracture of Mandibular Denture. History revealed
that he was completely edentulous for last 7 years and was
wearing the present dentures for last 6 years. Since last 1 year
the lower denture had been repaired thrice with routine
Laboratory procedures. His primary concern for fabrication
of new dentures was dentures with increased strength. History
taking revealed a personality of philosophic type intraoral
examination revealed that ridge form of mandibular arch was
Class 3 -thin inverted 'V'(Fig:10). Appropriate treatment plan
was formulated taking into consideration, the repeated
episodes of fracture. Our objective was to enhance the
fracture resistance of the denture. Considering the availability
of the resources and keeping in mind the patient's concern
about the cost and function it was decided to fabricate a metal
mesh reinforced denture4,5. The step involved are primary
impression followed by final impression of lower arch by
light body (fig:12). Wax rim were made face bow was
recorded transfer to Hanau articulator. Arrangement of the
artificial teeth was carried out to revel the necessary changes
to be made on the upper teeth. Adjustment in the artificial
teeth were incorporated in the preference to making changes
to the natural teeth. Processing of denture include additional
step is incorporation of metal mesh during packing
stage.(fig:13,14).The interference in denture were eliminated
and denture given to the patient.(fig:15,16) Post insertion
instruction were given to the patient regarding its
maintenance and hygiene
Fig. 10 a) b)
Fig. 11 a) b)
Fig. 12 a) b)
Fig. 13 a) b)
Fig. 14 a) b)
Fig. 15 a) b)
Fig. 16 a) b)
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 81
University J Dent Scie 2017; No. 3, Vol. 2

Case report 3: (Metal mesh)
A 55 years old male, partially edentulous with good general
health, reported to the Department of Prosthodontics,Crown
and Bridge (Institute of dental science) with a history of
repeated fracture of Mandibular Denture. Intraoral
examination revealed highly resorbed mandibular ridgeand
opposing full complement of natural dentition. Mucosa was
normal and the opposing teeth required minor alterations.
Saliva was of medium consistency and patient was co-
operative and philosophical according to House
classification. Procedure for case 3 is same as in case 2
procedure4,5from (fig: 12,13,14)
Fig. 17 a) b)
c)
Fig. 18 a) b)
Fig. 19 a) b)
Fig. 20 a) b)
Fig. 21 a) b) c)
Fig. 22 a) b)
Fig. 23 a) b)
Case report 4:(Metal mesh)
A 45-year-old male reported to the Department of
Prosthodontics Crown and Bridge, (Institute of dental
science) with a chief complaint of inability to chew food due
to missing teeth in the maxillary and mandibular arches
(Figure.1). Detailed case history was recorded and no
significant medical concerns were observed. Similar
treatment plan as case 2and 3 were planned4,5 from (fig:
12,13,14)
Fig. 24 a) b)
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 82
University J Dent Scie 2017; No. 3, Vol. 2
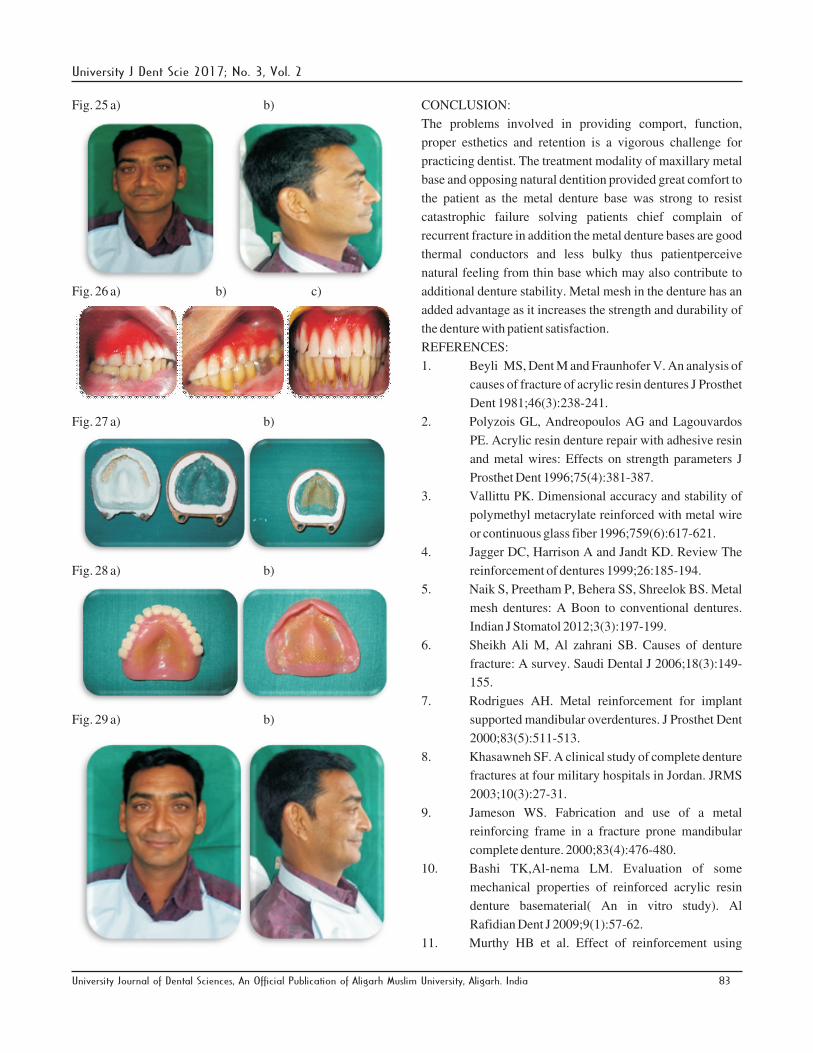
Fig. 25 a) b)
Fig. 26 a) b) c)
Fig. 27 a) b)
Fig. 28 a) b)
Fig. 29 a) b)
CONCLUSION:
The problems involved in providing comport, function,
proper esthetics and retention is a vigorous challenge for
practicing dentist. The treatment modality of maxillary metal
base and opposing natural dentition provided great comfort to
the patient as the metal denture base was strong to resist
catastrophic failure solving patients chief complain of
recurrent fracture in addition the metal denture bases are good
thermal conductors and less bulky thus patientperceive
natural feeling from thin base which may also contribute to
additional denture stability. Metal mesh in the denture has an
added advantage as it increases the strength and durability of
the denture with patient satisfaction.
REFERENCES:
1. Beyli MS, Dent M and Fraunhofer V. An analysis of
causes of fracture of acrylic resin dentures J Prosthet
Dent 1981;46(3):238-241.
2. Polyzois GL, Andreopoulos AG and Lagouvardos
PE. Acrylic resin denture repair with adhesive resin
and metal wires: Effects on strength parameters J
Prosthet Dent 1996;75(4):381-387.
3. Vallittu PK. Dimensional accuracy and stability of
polymethyl metacrylate reinforced with metal wire
or continuous glass fiber 1996;759(6):617-621.
4. Jagger DC, Harrison A and Jandt KD. Review The
reinforcement of dentures 1999;26:185-194.
5. Naik S, Preetham P, Behera SS, Shreelok BS. Metal
mesh dentures: A Boon to conventional dentures.
Indian J Stomatol 2012;3(3):197-199.
6. Sheikh Ali M, Al zahrani SB. Causes of denture
fracture: A survey. Saudi Dental J 2006;18(3):149-
155.
7. Rodrigues AH. Metal reinforcement for implant
supported mandibular overdentures. J Prosthet Dent
2000;83(5):511-513.
8. Khasawneh SF. A clinical study of complete denture
fractures at four military hospitals in Jordan. JRMS
2003;10(3):27-31.
9. Jameson WS. Fabrication and use of a metal
reinforcing frame in a fracture prone mandibular
complete denture. 2000;83(4):476-480.
10. Bashi TK,Al-nema LM. Evaluation of some
mechanical properties of reinforced acrylic resin
denture basematerial( An in vitro study). Al
Rafidian Dent J 2009;9(1):57-62.
11. Murthy HB et al. Effect of reinforcement using
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 83
University J Dent Scie 2017; No. 3, Vol. 2

stainless steel mesh, glass fibers and polyethylene
on the impact strength of heat cure denture base
resin-An in vitro study. J Inter Oral Health
2015;7(6):71-79.
12. Rathod N, Pawar S,Naitam D and Pasam N. Metal
denture base an approach to overcome the failure of
acrylic denture bases . IJRID 2015;5(2):69-72.
13. Prasad A, Prasad K and Hegde C. Management of
completely edentulous maxillary arch opposing
natural dentition- A case report. NUJHS
2012;2(3):39-42.
14. Memon S, Patel JR, Sethuraman R and Patel RS.
Management of single mandibular complete denture
with custom metal mesh- A case report .EJDTR
2013;2;137-139.
15. Kaira LS,Singh R. Single complete denture in
mandibular arch opposing natural dentition – A case
report. NUJHS 2013;3(1):72-75.
Figures Legends:
Figure 1: (a) maxillary edentulous arch (b) mandibular
edentulous arch (c) inter arch
Figure 2: (a) pre-operative frontal view (b) lateral view
Figure 3: (a) alginate lower impression (b) upper final
impression with zinc oxide eugenol
Figure 4: (a) wax spacer adapted on refractory maxillary cast
(b) sprue attached to the cast (c) obtained metal framework (d)
adapted metal mesh on the cast (e) occlusal wax rim on cast
Figure 5: (a) facebow record on the patient (b) facebow
transfer on Hanau articulator
Figure 6: (a) block out mandibular cast (b) duplication of cast
(c) duplication by agar (d) Refractory mandibular cast
Figure 7: (a) right side occlusion (b) left side occlusion
Figure 8: (a) maxillary flasking (b) mandibular flasking
Figure 9: (a) post-operative frontal view (b) smile at rest
position
Figure 10: (a) maxillary arch (b) mandibular arch
Figure 11: (a) pre-operative frontal view (b) lateral view
Figure 12: (a) alginate maxillary impression (b) elastomeric
mandibular final impression
Figure 13: (a) flasking of mandibular denture (b) metal mesh
for mandibular
Figure 14: (a) metal mesh adapted on mandibular cast
(b)intaglio surface of denture
Figure 15: (a) right side occlusion (b) left side occlusion
Figure 16: (a) post-operative (b) smile at rest position
Figure 17: (a) maxillary arch (b) mandibular arch (c) interarch
Figure 18: (a) pre-operative frontal view (b) lateral view
Figure 19: diagnostic cast
Figure 20: facebow record
Figure 21: (a) frontal view of occlusion (b) right side
occlusion (c) left side occlusion
Figure 22: flasking of mandibular denture
Figure 23: (a) post-operative view (b) smile at rest position
Figure 24: (a) maxillary arch (b) mandibular arch
Figure 25: (a) pre-operative frontal view (b) lateral view
Figure 26: (a) right side occlusion (b) left side occlusion (c)
frontal view occlusion
Figure 27: (a) flasking of maxillary denture (b) metal mesh
adapted on cast
Figure 28: (a) maxillary denture (b)intaglio surface
Figure 29: (a) post-operative frontal view (b) lateral view
CORRESPONDING AUTHOR:
Dr. Abbad Nikhil Bharat
Modern Dental College And Research Centre
Email address: [email protected]
Mobile No.: 9713435111
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 84
University J Dent Scie 2017; No. 3, Vol. 2