16. Mechanical Ventilation
76
Best Practices Clinical Guidelines for Mechanical Ventilation in Neonates Mammady Al maghayreh Date: October 17-19, 2011 Venue: Pr. Rahma Hospital/Auditourium
-
Upload
mohdmaghyreh -
Category
Documents
-
view
27 -
download
0
description
free
Transcript of 16. Mechanical Ventilation

Best Practices Clinical Guidelines for Mechanical Ventilation in Neonates
Mammady Al maghayrehDate: October 17-19, 2011
Venue: Pr. Rahma Hospital/Auditourium

Introduction It is an invasive life-support procedure with many
effects on the cardiopulmonary system The goal is to optimize both gas exchange and clinical
status at minimum FiO2 and ventilator pressure. The ventilator strategy employed to accomplish this goal depends in part on the infant disease process.
Conventional positive pressure ventilation remains the mainstay of assisted ventilation in neonates despite the development of new ventilatory techniques.
2

Physiologic functions of the lung
VentilationThe movement of air between the atmosphere and the
respiratory portion of the lungs
PerfusionThe flow of blood through the lungs
DiffusionThe transfer of gases between the air-filled spaces in the
lungs and the blood.




Ventilation
Depends on the conducting airways:
Nasopharynx and oropharynxLarynxTracheobronchial tree
Open AlveoliFunction:
Moves air in and out of the lung, warms and humidifes. Airways do not participate in gas exchange.

Lung ComplianceThe ease with which lungs can be expandedSpecifically, the measure of the change in lung
volume that occurs with a given change in transpulmonary pressure
Determined by two main factors Distensibility of the lung tissue and
surrounding thoracic cage Surface tension of the alveoli

Pulmonary Mechanics during Assisted Ventilation
Compliance (ml/cmH2O) =Distensible nature of lungs and chest wall. = Change in volume (ml) X change in
pressure (cmH2O)Neonates have greater chest wall
CompliancePremature infants with RDS have stiffer lungs
(poorly compliant lungs).
Neonatal lung Normal 0.003-0.006 L/cm H2Owith RDS 0.0005-0.001 L/cm H2O

Resistance
10
Resistance (cmH2O/L/sec)= Property of airways and lungs to resist gas. = Change in pressure (cmH2O) X Change in flow
(L/sec) Time constant of the respiratory system = Resistance x
Compliance
Resistance in infants with normal lungs ranges from 25 to 50 cm H2O/L/sec.It is increased in intubated babies and ranges from 50 to 100 cm H2O/L/sec.

Pulmonary mechanics
Time constant The time taken for the airway pressure (and
volume) changes to equilibrate throughout the lung is proportional to the compliance and resistance of the respiratory system
Time constant = Compliance x Resistance

12

Pulmonary mechanics
Almost full equilibration: 3-5 time constants
100
80
60
40
20
01 2 3 4 5 Time constants
Cha
nge
in p
ress
ure
)%(
6386
95 98 99

14
Time ConstantInspiratory time must be 3-5 X time constant1(„ One time conststant = time for alveoli to discharge 63% of its volume through the airway.2(„Two time constant = 84% of the volume leaves3(„ Three time constant = 95% of volume leaves.

Lung Mechanics Differ in Different Disease States
DiseaseCompliance
ml/cm H2O
Resistance
(cm/H2O/ml/s)
Time
Constant(s)
FRC
(ml/kg)
V/Q
Matching
Work
Normal
Term4-620-400.2530------
RDSDecreasedDecreasedDecreasedDecreasedDecreasedIncreased
Meconium
AspirationDecreasedIncreasedIncreasedIncreasedDecreasedIncreased
BPDIncreased/
DecreasedIncreasedIncreasedIncreasedDecreasedIncreased
Air leakDecreasedIncreasedIncreasedIncreasedDecreasedIncreased
VLBW apnea
DecreasedDecreasedDecreasedDecreasedDecreasedIncreased
15

Basic Ventilator Parameters
FiO2
Fractional concentration of inspired oxygen delivered expressed as a % (21-100)
Breath Rate (f)The number of times over a
one minute period inspiration is initiated (bpm)
Tidal volume (VT)
The amount of gas that is delivered during inspiration expressed in mls or Liters. Inspired or exhaled.
FlowThe velocity of gas flow or
volume of gas per minute

Phase Variables
Trigger (start)- begins inspiratory flowCycling (end)- ends inspiratory flowLimiting (continue)- places a maximum value on a
“control variable”pressurevolumeflow
time

Breath Type… Only Two (for now)!
MandatoryVentilator does the workVentilator controls start and stop
SpontaneousPatient takes on workPatient controls start and stop

Trigger Variable- Start of a Breath
Time - control ventilationPressure - patient assistedFlow - patient assistedVolume - patient assistedManual - operator control

The Control Variable-Inspiratory Breath Delivery
Flow (volume) controlledpressure may vary
Pressure controlledflow and volume may vary
Time controlled (HFOV)pressure, flow, volume may vary

Inspiratory - delivery limits
Maximum value that can be reached but will not end the breath-VolumeFlowPressure

Expiratory - baseline
Positive End Expiratory PressureExpiratory RetardNegative End Expiratory PressureExpiratory HoldTime Limited Exhalation

PEEP
DefinitionPositive end expiratory pressureApplication of a constant, positive pressure such that at end
exhalation, airway pressure does not return to a 0 baseline
Used with other mechanical ventilation modes such as A/C, SIMV, or PCV
Referred to as CPAP when applied to spontaneous breaths

PEEP
Increases functional residual capacity (FRC) and improves oxygenationRecruits collapsed alveoliSplints and distends patent alveoliRedistributes lung fluid from alveoli to perivascular
space
55 cm cm HH22OO
PEEPPEEP

Gas Exchange during Assisted Ventilation
Carbon Dioxide (CO2)
Diffuses rapidly from the blood into the alveoli. Its elimination depends largely on alveolar
ventilation.Minute alveolar ventilation= (Tidal volume –
Dead space) x Frequency.Tidal volume is determined by the pressure
gradient between inspiration and expiration.
25
CPAP
DefinitionContinuous positive airway pressureApplication of constant positive pressure throughout the
spontaneous ventilatory cycle
No mechanical inspiratory assistance is provided Requires active spontaneous respiratory drive
Same physiologic effects as PEEP

Gas Exchange during Assisted Ventilation (cont.)
Carbon Dioxide (CO2) - (cont.)
Inspiratory duration may partially determine the tidal volume
Tidal volume can be decreased by shortening the inspiratory time.
Changes in ventilator frequency have a strong effect on CO2 elimination
27

OxygenOxygen exchange depends on matching perfusion
with ventilation. Oxygenation is determined by the mean airway
pressure applied. Paw = (PIP –PEEP) [Ti/ (Ti +Te)] + PEEP
28
Gas Exchange during Assisted Ventilation (cont.)

Mean airway pressure will be augmented by increasing any of the following: Inspiratory flowPIP I:E ratioPEEPFrequency (or rate) by shortening Te
29
Gas Exchange during Assisted Ventilation (cont.)

The effect of mean airway pressure on oxygenation is related to:Optimizing the lung volumePreventing atelectasis and consequently
improving ventilation perfusion relationships.
30
Gas Exchange during Assisted Ventilation (cont.)
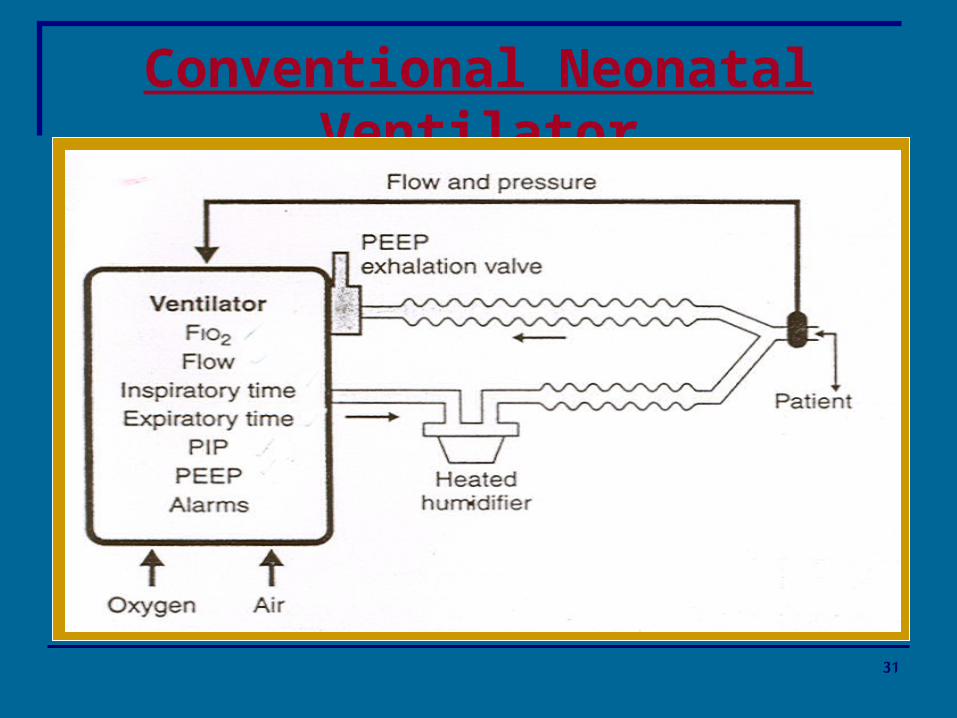
Conventional Neonatal Ventilator
31

Volume-Cycled Ventilators
Less used to ventilate neonates Deliver a fixed volume irrespective of pressure Flow and I:E ratio determine the tidal volume Does not work well for RDS patient
32

Pressure-Limited, Time-Cycled
Peak inspiratory pressure, and inspiratory timing are selected
Continuous flow of fresh heated humidified gas It allows the infant to make spontaneous
respiratory efforts Fighting neonates may face air leak syndrome
33

Patient Triggered Ventilation
Neonate is able to initiate ventilatory breath by:1) „ Abdominal motion2) „ Chest wall impedance3) „ Airway flow4) „ Great degree of synchronacy between patient and
ventilator
34

Patient–Triggered Ventilators (PTV)
The patient is able to initiate ventilator breaths by1) Abdominal motion2) „ Chest wall impedance3) „ Airway flow4) „ Great degree of synchronacy between patient and ventilator
Triggering the ventilator setting detector The system support the patient if it didn't breath improved tidal volume and blood gases It can be Synchronized (SIMV) or Assisted/ control (A/C) modes Weaning is by reducing the PIP Cerebral blood flow is controlled Reduce the duration of ventilation and ease weaning
35

Troubleshooting Changes in Tidal Volume during Pressure Ventilation of the Neonate
Tidal Volume Change
Possible CuesSolutions
Increase Increased compliance, decreased resistance, decreased PEEP, increased inspiratory time, decreased leak.
Reduce peak inspiratory pressure.
Decrease Decreased compliance, increased resistance, decreased peak inspiratory pressure, increased PEEP, decreased inspiratory time, increased leak.
Suction airway
Administer surfactant.
Increase inspiratory pressure, performing a transillumination to check for pneumothorax, obtaining chest radiography, and check tube positioning.
36

Indications for Mechanical Ventilation
Absolute indicationsSevere hypoxemia with a PaO2 less than 50mm
Hg despite FiO2 of 0.8Respiratory acidosis with pH of less than 7.20 to
7:25 or PaCO2 above 60mm Hg.Severe prolonged apnea
37

USAID-Funded Health Systems Strengthening II Project 38

Relative indicationsFrequent intermittent apnea unresponsive to
drug therapyEarly treatment when use of mechanical
ventilation is anticipated because of deteriorating gas exchange
Relieving work of breathing in an infant with signs of respiratory difficulty
Initiation of exogenous surfactant therapy in infants with RDS
39
Indications for Mechanical Ventilation (cont.)

Volume vs… Pressure Control Ventilation
Volume Ventilation
Volume delivery constant Inspiratory pressure
varies Inspiratory flow constant Inspiratory time
determined by set flow and VT
Pressure Ventilation
Volume delivery varies Inspiratory pressure
constant Inspiratory flow varies Inspiratory time set by
clinician

The Effects of Ventilator Setting Changes on Blood Gases
Effects on Blood Gas Tensions
Ventilator setting changesPaCO2PaO2
Increase PIPDecreaseIncrease
Increase PEEPIncreaseIncrease
Increase FrequencyDecreaseIncrease
Increase I:E Ratio------Increase
Increase FiO2------Increase
Increase FlowDecreaseIncrease
41

Starting Ventilator Settings
Guidelines for Endotracheal Tube Size
Infant Weight (gm)Endotracheal Tube Internal Diameter
< 1,0002.5mm
1,000-2,0003.0mm
2,000-3,0003.5mm
> 3,0003.5 - 4.00mm
42

Initial Settings for mechanical ventilationSettingInstructions for Use
Peak inspiratory pressure (PIP)As needed to provide tidal volume of 5-7ml/kg.
Positive end-expiratory pressure (PEEP)
3-5cm H2O
Rate40- 60/minute.
Inspiratory time0.3- 0.4 seconds
Fractional inspired oxygen concentration (FiO2)
maintain SpO (88-93%)
Flow8-12L/minute.
43
Starting Ventilator Settings (cont.)

The subsequent settings for mechanical ventilation
Subsequent SettingsPEEPPIP
Low PaO2, low PaCO2Increase
Low PaO2, high PaCO2Increase
High PaO2, high PaCO2Decrease
High PaO2, low PaCO2Decrease
44
Starting Ventilator Settings (cont.)

Monitoring the infant during mechanical ventilation First blood gas after 15-30 mins Blood gas after 15-30 mins of every change Regularly blood gas every 6 hrs Continuous vital sings monitoring
45
Starting Ventilator Settings (cont.)

Deterioration during Mechanical Ventilation
Sudden clinical deterioration Mechanical or electrical ventilator failure Disconnected tube or leaking connection Endotracheal tube displacement or blockage Pneumothorax
46

Deterioration during Mechanical Ventilation (cont.)
Gradual deterioration Inappropriate ventilator setting Intraventricular hemorrhage Baby fighting against the ventilator PDA Anemia Infection
47

Paralysis and Sedation
The use of neuromuscular blockade is not routinely indicated
Sedation is restricted to cases when agitation interferes with ventilatory support and when infants fight the ventilator.
It is necessary to increase ventilator pressure after initiation of neuromuscular blockade.
48

Weaning
When the patient is stable, FiO2 and PIP are weaned first.
Decrease PIP as tolerated and as chest rise diminishes.
When PIP is around 20, attention is directed to FiO2 and then to the respiratory rate alternating with each other
As frequency is decreased, Te should be prolonged For larger infants, endotracheal CPAP when PIP 15-
18 cm H2O and FiO2 40%
49

Weaning (cont.)
The infant can be weaned to oxygen hood when PEEP is 4cm H2O
For less than 1.750gm, when PIP is less than 15cm and FiO2 30% decrease respiratory rate to 15-20/ min then to nasal CPAP
In most infants, when ventilator frequency of approximately 15 breaths per minute is tolerated, endotracheal CPAP may be tried for a short period of time before extubation.
50

Weaning (cont.)
Atelectasis after extubation is common in preterm infants recovering from RDS.
Use of nasal CPAP may prevent atelectasis. Steroids are not routine before extubation, but if
there was prolonged intubation or previous failed attempts of extubation, a short course of steroids may facilitate extubation.
If strider developed epinephrine aerosols and steroids may be helpful
51

Complications of Mechanical Ventilation
Endotracheal tube complications and tracheal lesions
Airway injury Air leak Chronic lung disease/Oxygen toxicity Intraventricular hemorrhage Decreased cardiac output Feeding intolerance
52

Pulmonary Hygiene
Chest physiotherapy
Suction
53

Goals of Pulmonary Hygiene
Maintain a patent airway by clearing secretions Promote optimal pulmonary oxygenation and
ventilation Prevent pulmonary infection from accumulated
secretions Facilitate removal of pulmonary debris
54

Chest Physiotherapy Indication
Intubated neonates: Chest physiotherapy should only be applied if it is
clearly indicated. No CPT after surfactant administration CPT in early RDS increases incidence of
intraventricular hemorrhage Post-extubation Chronic lung disease of prematurity
55

Physiotherapy and surgeryAfter abdominal or cardiac surgery Postoperative physiotherapy should never be
“routine” but should be used judiciously.
56
Chest Physiotherapy Indication (cont.)

Chest Physiotherapy Technique
Positioning
Vibration
57

When It Is Indicated
During intubation and ventilation Post ex-tubation Premature with chronic lung disease After abdominal and chest surgery
58

Suction
Methods of suctioning: Open Closed
Catheter suction ca be: Deep Shallow
Suctioning should be performed under strict sterile preparation
59

Suction Procedure
Shallow suction is recommended to prevent trauma Deep suction may cause apnea and vagal
stimulation Duration of suction should be 15 seconds
60

Follow-up Care
Hyper-oxygenation for at least 1 min especially for hypoxemic infants
Hyperventilation should not be routinely used. The patient should be monitored for adverse
reactions
61

Indications
Secretions in peripheral airways should not be directly removed by endotracheal suctioning
Suctioning should be performed only when clinically indicated
To remove accumulated pulmonary secretions To maintain the patency and integrity of the
artificial airway
62

Signs of Increased Pulmonary Secretions
Increased peak inspiratory pressure during volume-controlled mechanical ventilation
Decreased tidal volume during pressure-controlled ventilation
Deterioration of oxygen saturation and/or arterial blood gas values
Visible secretions in the airway Acute respiratory distress Suspected aspiration of gastric or upper-airway
secretions The need to obtain a sputum specimen
63

Complications Decrease in dynamic lung compliance and functional
residual capacity Atelectasis Hypoxia/hypoxemia Tissue trauma Bronchoconstriction/bronchospasm Increased microbial colonization Changes in cerebral blood flow and increased
intracranial pressure Hypertension or hypotension Cardiac dysrhythmias
64
Assessment of Outcome
Improvement in appearance of ventilator graphics and breath sounds
Decreased need for ventilation support Improvement in arterial blood gas values or
saturation Removal of pulmonary secretions
65

The following should be monitored prior to, during, and after the procedure:Breath soundsOxygen saturationPulse rateSkin colorRespiratory rate and patternSputum characteristics: color, volume,
consistency, and odorVentilator
66
Monitoring during suction (cont.)

Recommendations
Endotracheal suctioning should be performed only when secretions are present and not routinely. (1C)
Pre-oxygenation should be considered if the patient has a clinically important reduction in oxygen saturation with suctioning. (2B)
Performing suctioning without disconnecting the patient from the ventilator (2B)
Use of shallow suction (2B)
67

Routine use of normal saline instillation prior to endotracheal suction should not be performed. (2C)
A suction catheter is used that occludes less than 70% of the lumen of the ETT in infants. (2C)
The duration of the suctioning event be limited to less than 15 seconds. (2C)
68
Recommendations (cont.)

High Frequency Ventilation(HFV)
Rescue following failure of conventional ventilation (PPHN, Meconium).2,3
Air leak syndromes (pneumothorax, pulmonary interstitial emphysema) 4
To reduce barotrauma when conventional ventilator settings are high

Frequency
•High frequency ventilation rate (Hz, cycles per second)
MAP
•Mean airway pressure (cmH2O) Amplitude
•delta P or power is the variation around the MAP
Oxygenation is dependent on MAP and FiO
2
•MAP provides a constant distending pressure equivalent to CPAP. •This inflates the lung to a constant and optimal lung volume maximising the area for gas exchange and preventing alveolar collapse in the expiratory phase. •Ventilation is dependent on amplitude and to lesser degree frequency. •Thus when using HFV CO2 elimination and oxygenation are independent

The clinician sets
The amplitude . Frequency of the pressure wave generated by the
ventilator piston or diaphragm Mean airway pressure (MAP) Inspiratory time. Fractional inspired concentration (FiO2)
USAID-Funded Health Systems Strengthening II Project 71

Optimal lung volume strategy(aim to maximise recruitment of alveoli).
Set MAP 2-3 cmH2O above the MAP on conventional ventilation
MAP in 1-2 cmH2O steps until oxygenation improves
Set frequency to 10 Hz

73

HFV
Low volume strategy(aim to minimise lung trauma)
Set MAP equal to the MAP on conventional ventilation
Set frequency to 10 Hz Adjust amplitude to get an adequate chest
wall vibration.

Making adjustments once established on HFVMaking adjustments once established on HFV
Poor Oxygenatio
n
Over Oxygenatio
n
Under Ventilation
Over Ventilation
Increase FiO2
Decrease FiO2
Increase Amplitude
Decrease Amplitude
Increase MAP
(1-2cmH2O)
Decrease MAP
(1-2cmH2O)
Decrease Frequency (1-2Hz)
if Amplitude Maximal
Increase Frequency (1-2Hz)
if Amplitude Minimal