1445 Simon Board Simulation in Nephrology and Hypertension

of 51
-
Upload
nizar-shorman -
Category
Documents
-
view
222 -
download
0
Transcript of 1445 Simon Board Simulation in Nephrology and Hypertension
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
1/51
Nephrology Board Simulation
James F. Simon, MDNephrology Fellowship Program Director
Department of Nephrology and HypertensionCleveland Clinic
Objectives
The practice taking the Internal Medicine Board
exam using board-related Nephrology questions
To review key educational points in determining
the correct responses to board-relatedNephrology questions
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
2/51
Case 1
A 26-year old male presents with leg edema forone week
He has been using ibuprofen 800 mg 3x/day for
one month for a shoulder injury
Exam is significant for a blood pressure of 130/90
and 3+ lower extremity edema
Urinalysis: 4+ protein, no blood
24-hour urine protein: 10.8 grams, no hematuria
Serum creatinine: 0.9 mg/dL (eGFR >60cc/min)
Question 1: The most likely disordercausing this clinical picture is:
A. Human Immunodeficiency Virus (HIV)
nephropathy
B. Focal segmental glomerulosclerosis
C. Acute tubular necrosis
D. Minimal change disease
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
3/51
Answer 1. D
Minimal Change Disease Nephrotic syndrome without hematuria
Preserved renal function most commonly
15% of adults may present with ATN due to volume
depletion
Steroids first-line therapy
Answer 1. D (Minimal Change Disease)
5 ways glomerular disease can present:
1. Asymptomatic hematuria
2. Acute nephritis
3. Rapidly progressive glomerulonephritis4. Chronic nephritis
5. Nephrotic syndrome:>3gm proteinuria,
edema, low albumin, hyperlipidemia
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
4/51
Answer 1. D (Minimal Change Disease)
Secondary causes of minimal change
disease
**NSAIDs Other medications include Gold, Lithium
Blood tumors:Hodgkins, leukemias
Insect bites, other antigenic stimuli
Treat underlying illness or remove offendingagents
Answer 1. D (Minimal Change Disease)
Treatment of Primary Minimal Change
1. High dose steroids8-12 weeks
2. Oral cyclophosphamide
3. Oral cyclosporine
Responses to Treatment
1. Steroid responsive
2. Steroid dependent
3. Steroid resistant
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
5/51
Answer 1. Other Options
A. HIV Associated Nephropathy (HIVAN)
Nephrotic syndrome with decreased kidney
function
Collapsing FSGS is the classic lesion
Echogenic kidneys on US
HAART mainstay of therapy Predisposition to African Americans with a
mutation in the APOL-1 genes
Answer 1. Other Options
B. Focal Segmental Glomerulosclerosis
(FSGS)
Nephrotic syndrome, bland urinary sediment,
decreased kidney function
Most common cause of nephrotic syndrome in
adults, especially African Americans
Secondary disease
Common end-point of glomerular injury
Hyper-filtration of remnant glomeruli
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
6/51
Answer 1. Other Options
C. Acute Tubular Necrosis
Acute kidney injury manifested by
decreased kidney function
Minimal proteinuria
Ischemic, toxic most common causes
Does not present with nephrotic syndrome
Case 2
A 19 year-old male presents with tea-colored
urine, arthralgias, and a heart murmur
He lives in a dorm room at college
He had an upper respiratory infection and sore
throat 10 days agoExam reveals
Swollen and tender right wrist and left elbow
Prominent cervical/submandibular nodes
2/6 systolic ejection murmur
2+ edema
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
7/51
Case 2 (cont.)
Labs Urinalysis:
SG 1.013
No glucose
pH 6.0
3+ protein
Large blood
Microscopy: 20 RBC/HPF
3 to 5 RBC casts
Blood work:
Creatinine 2.2 mg/dL
Low C3; nml C4
Glucose 51 mg/dL
Elevated rheumatoid
factor
FeNa 3.2%
Question 2: The most likely causefor this clinical scenario is:
A. Membranous glomerulonephritis
B. Wegener's granulomatosis
C. Poststreptococcal glomerulonephritisD. Acute tubular necrosis
E. Fanconi's syndrome
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
8/51
Answer 2: C (Post-Streptococcal
Glomerulonephritis)5 ways glomerular disease can present:
1. Asymptomatic hematuria
2. Acute nephritis
3. Rapidly progressive glomerulonephritis
4. Chronic nephritis
5. Nephrotic syndrome: >3gm proteinuria,
edema, low albumin, hyperlipidemia
Answer 2: C (Post-Streptococcal
Glomerulonephritis)
Nephritic syndrome
Glomerular hematuria, tea-colored urine
Hypertension
Renal failure, often oliguric Proteinuria usually mild
Mild edema
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
9/51
Answer 2: C (Post-Streptococcal
Glomerulonephritis)
Post-Pharyngitic Nephritis
Acute nephritis 10-14 days after a strep infection
Differentiation from IgA Nephropathy
Pharyngitis or skin infections (impetigo)
May require transient dialysis
Self-limited course, may result in permanentkidney dysfunction
If strep has been cleared, supportive treatment
Culture if active infection (and treat)
Serologies: ASO and DNAse both (or streptozyme panel)
Low C3 level during the first week
Elevated rheumatoid factor and circulating cryoglobulins
Renal failure and hematuria resolve first
Proteinuria can persist for months
Answer 2: C (Post-Streptococcal
Glomerulonephritis)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
10/51
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
11/51
Answer 2: Other Options
B. Wegeners Granulomatosis (GPA) Pulmonary-renal syndrome
ANCA-associated vasculitis
Systemic vasculitis symptoms common
Rapidly progressive crescentic GN
Life-threatening illness requiring prompt
diagnosis and treatment Steroids, cyclophosphamide or rituximab,
+/- plasmapheresis
Answer 2: Other Options
E. Fanconi Syndrome
Not associated with renal dysfunction
Proximal renal tubular acidosis (RTA)
Hyperchloremic metabolic acidosis
Glycosuria, phosphaturia, amino acidouria
Mild proteinuria
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
12/51
Case 3
A 36 year old female with recurrent kidneystones presents for further evaluation
First kidney stone approximately 15 years ago
Has passed approximately 50 stones since
Strong family history of kidney stones in her
father and brother, but no kidney failure
Type of stone is unknown She was told to restrict her calcium intake for
the past few years
Question 3: Which of the following, ifdeficient in the urine, promotes calcium
stone formation?
A. Oxalate
B. Citrate
C.Sodium
D.Proteins/amino acids
E. Uric acid
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
13/51
Answer 3: B. Low Urinary Citrate
Promotes Kidney Stone Formation Urinary citrate binds urinary calcium
Non-dissociable but soluble complex
Prevents calcium from binding to oxalate or phosphate
Examples of diagnoses associated with low urinary
citrate
RTA (distal)
Medullary sponge kidney
Polycystic kidney disease
Metabolic acidosis: malabsorption, ureteral diversion
Answer 3: Other Options
Low urine volume
Hypercalciuria
-Idiopathic
-High sodium intake
-Loop diuretics
-Hyperparathyroidism
-RTA
Hypocitraturia
-RTA
Hyperoxaluria
- Diet
- Calcium restriction
- Malabsorption
Hyperuricosuria
Urine pH
- Stone dependent
Protein loading
Risk Factors for Calcium Nephrolithiasis:
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
14/51
Answer 3: Other Options
Common management of all kidney stones
to decrease recurrence:
Increasing urine volume to over 2 L per day
2000mg daily sodium restriction
DO NOT restrict calcium intake
Limit high animal fat diets
Question 4: Renal manifestations of HIV
infection include which of the following?
A. Hyponatremia
B. Tubuloreticular inclusions
C. Focal segmental glomerular sclerosis
D. Acute tubular necrosis
E. All the above
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
15/51
Answer 4: E (all the above)
A. Hyponatremia
Seen in 60% of HIV patients during their
disease
Volume depletion with up-regulation of AVP
SIADH with pulmonary and intracranial disease
Toxoplasmosis
Tuberculosis Pneumocystis
Answer 4: E (all the above)
B. Tubuloreticular Inclusions
Associated with IFN up-regulation
Can also be seen in lupus nephritis and after
treatment of HCV with IFN
Seen on biopsy
C. Focal Segmental Glomerulosclerosis
Previously discussed
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
16/51
Answer 4: E (all the above)
D. Acute Tubular Necrosis
Acute renal failure in HIV:
ATN: medications, hypovolemia, shock
AIN: medications, infection
HUS/TTP
Crystal-induced:
acyclovir, indinavir,sulfa drugs
Indinavir Crystals
Case 5
A 65 year-old male with BPH presents for follow-up 5
days into treatment of a urinary tract infection with
trimethoprim-sulfamethoxazole. His symptoms have
resolved. Temperature 37.5 C; the remainder of the
physical exam is normal. Lab work obtained shows:
2 weeks prior Current
BUN 12 mg/dl 12 mg/dl
Creatinine 1.4 mg/dl 2.0 mg/dl
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
17/51
Urinalysis:
S.G. 1.010
Heme: neg.
Protein: neg.
Leukocyte esterase: negative
No casts or cells
Case 5 (Contd)
Question 5: In the above patient, themost likely reason for the creatinine
increase to 2.0 mg/dL is:
A. Acute interstitial nephritis
B. Acute pyelonephritis
C. Obstructive uropathyD. Reduced creatinine excretion
E. Acute tubular necrosis
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
18/51
Answer 5: D: Reduced Creatinine
Excretion
Properties of serum creatinine excretion
Filtered by the glomerulus
Excreted by the proximal tubule
Slightly over-estimates true GFR
Certain organic cations (e.g. trimethoprim,
cimetidine) competitively inhibit creatininesecretion
Solute Clearance
Serum Concentration
Endogenous
Production
Exogenous
Addition
Glomerular
Filtration
Tubular
concentration
Urinary
excretion
Tubular
Reabsorption
Tubular
Secretion
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
19/51
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
20/51
Answer 5: Other Options
A. Acute Interstitial Nephritis Associated with sulfa use
Sterile pyuria, WBC casts on urine
Can be associated with fever or rash
B. Acute pyelonephritis
Infection has cleared without clinicalpyelonephritis
Not typically associated with AKI
Answer 5: Other options
C. Obstructive Uropathy
Sulfa crystals can lead to tubular obstruction,
hematuria, but not overt obstruction
Early obstruction may appear like pre-renal
azotemia, and have a low FeNa Stable BUN suggests against true AKI
E. Acute Tubular Necrosis
Stable BUN, no urinary evidence of ATN
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
21/51
A 54yo Caucasian male comes to see you in
clinic
PMH:
Diabetes Mellitus Type 2Hb A1C 8.5
HypertensionHome BPs 140s/90s
HyperlipidemiaLDL 125
Stage 4 CKDeGFR 28cc/min/1.73m2
He takes aspirin 81mg daily with his other
medications
Case 6
Case 6
As part of your discussion of CKD and the risk of
progressing to ESRD, you discuss the elevated
cardiovascular risk associated with CKD
Which of the following changes has been shownto decrease cardiovascular risk in this patient?
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
22/51
(A) Lowering the glycated hemoglobin level to lessthan 6%, compared with 77.9%
(B) Controlling the systolic blood pressure to less
than 120 mmHg, compared with less than 140
mmHg
(C) Administering aspirin 325 mg daily, compared
with 81 mg daily(D) Administering simvastatin plus ezetimibe,
compared with placebo
Question 6
First prospective trial to demonstrate CV
risk reduction with lipid lowering agents in
patients with CKD 4
9270 patients, >40 years old with SCr
>1.7mg/dL in men, >1.5mg/dL in women Mean eGFR 26.6cc/min
Dialysis and non-dialysis dependent CKD
Ezetimide/simvasatin vs. placebo
Primary prevention
SHARP Trial
Baigent, Lancet, 377, 2011
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
23/51
Primary outcome: atherosclerotic events
Nonfatal MI, coronary death, non-hemorrhagic stroke,
arterial revascularization
Median follow-up 4.9 years
Outcomes favored treatment arm
11.3% vs. 13.4% (RR 0.83, 95% CI 0.74-0.94)
Subgroup analysis: (not power for subgroups) No benefit in ESRD: RR 0.9 (0.75-1.08)
Benefit in non-dialysis CKD: RR 0.78 (0.67-0.91)
SHARP Trial
Baigent, Lancet, 377, 2011
(Allpost-hoc)
Primary Prevention:
CARDS: atorvastatin, DM and CKD
MEGA: pravastatin, Japanese
JUPITER: rosuvastatin, high CRP
AFCAPS: lovastatin
Secondary Prevention:
ALLIANCE: atorvastatin
4S: simvastatin
Trials Showing Benefit of
Statins in CKD 3
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
24/51
AURORA: rosuvastatin
3.8-year follow-up
4D: atorvastatin
4-year follow-up
SHARP
Despite significant LDL reduction
Statins of No Benefit in ESRD
Statin therapy demonstrated benefits:
Primary prevention in CKD 3
Secondary prevention in CKD 3
No proven benefit (yet) in CKD 4 Combination simvastatin/ezetimide
Primary prevention in CKD 4
No benefits in ESRD
Summary of Lipid Therapy in CKD
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
25/51
Other Options ACCORD Trial
CV risk reduction in diabetes mellitus
No benefit of intensive BP control
SBP
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
26/51
Medications: clonidine 0.1mg bid, atenolol 50mgdaily, HCTZ 25mg daily, lisinopril 20mg daily (new 1
year ago)
Labs:
Plasma renin activity 6 mg/L/hr; Aldosterone 10 ng/dL
Na+ 136; K+ 3.3; CO2 27; BUN 45; Creatinine 1.6Urinary protein:creatinine ratio 0.6gm/gm
Renal artery duplex: 60-99% bilateral RAS
Case 7 (Contd)
Question 7: If renal artery stenosis is found onangiography, which indication for angioplasty
and stenting does this patient have?
A. Resistant hypertension
B. Preservation of renal function
C. Worsening renal function on an ACE
inhibitor
D. Hypokalemia
E. Congestive heart failure
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
27/51
Answer 7:
E. Congestive Heart FailureUnderstanding the ACC/AHA guidelines for
revascularization of renal artery stenosis
Accelerated, resistant or malignant
hypertension
Progressive renal dysfunction in the setting of
bilateral RAS or RAS to a solitary functioningkidney
Congestive heart failure or unstable angina
Answer 7:E. Congestive Heart Failure
Retrospective studies consistently support the
link between CHF and RAS
Flash pulmonary edema or recurrent CHF
exacerbations with RAS occur in bilateral RAS or
RAS to solitary functioning kidney
Intervention can improve symptoms, BP control and
kidney function
Prospective studies suggest improvement in
chronic CHF with bilateral RAS
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
28/51
Often present with acute pulmonary edema and
hypertension
Catecholamine-driven process that cycles
BP may spike and drop multiple times during an
admission
Pulmonary edema will trend with BP spikes
Answer 7:E. Congestive Heart Failure
Answer 7: Other Answers
A. Resistant Hypertension
Refractory to 3 maximally dosed anti-hypertensive
medications, including a diuretic
Make sure of three things:
The drugs are maximally dosed (amlodipine 2.5mg/day) The dosing intervals are appropriate (clonidine bid or
atenolol daily)
The drugs are the most efficacious in their class (atenolol,
+/- HCTZ)
Does not meet definition of resistant HTN
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
29/51
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
30/51
Answer 7: Other Answers
D. Hypokalemia
While hypokalemia might suggest an up-regulated
renin/angiotensin/aldosterone system, it certainly is
not an indication alone
Thiazide therapy can explain this
Safian, NEJM 344(6):431, 2001
Presentations of RAS
HTN
Renal Failure
Both
Neither
CHF
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
31/51
Renovascular Hypertension
Onset in women 55 years old (AS)
Newly worsening hypertension
Resistanthypertension
Abdominal bruitsnon-specific in elderly
patients
Secondary Hypertension:
Obstructive sleep apnea
Hyper/Hypo-Thyroidism
Contraceptives, Coarcation of aorta, Cushings
Renal artery stenosis, Renal diseaseAldosteronism (primary and other)
Pheochromocytoma
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
32/51
Case 8:
A 55-year-old male with a history of smallcell lung cancer is admitted to the hospital
with weakness and confusion for the past 48
hours. He became minimally arousable this
morning
BP 126/70, weight 65kg
He is arousable, not orientedOral mucosa are moist
Lungs are clear, no edema
Case 8, contd:
Serum
Sodium 118 mmol/L
Potassium 4.0 mmol/L
Cl 84 mmol/L
CO2 22 mmol/LBUN 9 mg/L
Creatinine 0.9 mg/dL
Glucose 90 mg/dL
Uric acid 2.5 mg/dL
Urine
Osmolality 450 mOsm/L
Sodium 50 mmol/L
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
33/51
Question 8: Which of the following
treatments will NOT lead to a rise in
serum sodium in this patient?
A. Effective treatment of the malignancy if
available
B. Free water restriction
C. Vasopressin antagonists
D. Isotonic saline
E. Furosemide
Answer 8: D. Isotonic saline
Syndrome of Inappropriate ADH Secretion
(SIADH)
Known small cell lung cancer
Hyponatremia
High urinary sodium and osmolality Low serum uric acid level
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
34/51
Urine Parameters and
Hyponatremia
Intravascular
Vol. Depletion SIADH Polydipsia
UNa
UOsm
Renal Handling of Water
Osmolality
1200
Osmolality
50
Na
K
2Cl
AQ2
H2O
Osmolar
load
Water load
Urine
Osmolality
AVP
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
35/51
Renal Handling of a Water Load
Assume 600mOsmo dietary intake
Minimal urinary osmolality of 50 mOsm/L
Maximum urinary osmolality of 1200 mOsm/L
What is the minimum and maximum amount of
water you can drink in a day and still handle the
water load solely through urination?
0.5L12L
Renal Handling of a Water Load
Assume 200mOsmo dietary intake
Minimal urinary osmolality of 100 mOsmo/L
Maximum urinary osmolality of 800 mOsmo/L
(elderly female tea and toaster)
What is the minimum and maximum amount of
water you can drink in a day and still handle the
water load solely through urination?
0.25L2L (8 cups of tea per day)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
36/51
Renal Handling of a Water Load
Any water intake beyond the maximum amount
for a given minimum urinary osmolality must be
retained as free water
Leads directly to hyponatremia
Renal Handling of a Water Load:SIADH
Assume 600mOsmo dietary intake
Urinary osmolality fixed at 450mOsmo/L
What is the maximum amount of water you candrink in a day and not retain free water leading
to hyponatremia?
1.3L (600/450)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
37/51
Renal Handling of a Water Load
SIADH Assume 600mOsmo dietary intake
Urinary osmolality fixed at 450mOsmo/L
What is the impact of infusing 1L normal saline
(osmolality = 308 mOsmo/L)?
0.67L urinated at 450mOsmo/L
0.33L retained free water
Sodium goes down!
Treatments for SIADH
Osmolality
1200
Osmolality
50
Na
K
2Cl
AQ2
H2O
Osmolar
load
Water load
Urine
Osmolality
AVP
Demeclocycline
Vaptans
(caution)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
38/51
Case 9
A 65yo AAM presents to your office to establish
care. He has chronic kidney disease, diabetes
mellitus, hypertension and hyperlipidemia.
H/O coronary artery disease s/p stenting to LAD
and RCA lesions 2 years ago.
Medications
Losartan 50mg twice daily -HCTZ 25mg once daily Amlodipine 5mg once daily -Pravachol 20mg at night
ASA 325mg once daily -Metformin 500mg twice daily
Glipizide 10mg daily
Case 9
BP 138/82, HR 87, BMI 32
On exam:
Lungs are clear to auscultation
Heart is regular rhythm, S4 present, 1/6 systolic
crescendo murmur at left upper sternal border
No carotid bruits
JVP 6cm
Abd: without bruits, abnormal pulsation
Extremities: diminished distal pulses, 2+ bilateral
ankle edema (which he blames on amlodipine)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
39/51
Case 9
Labs
Creatinine 2.0mg/dL, eGFR 41cc/min/1.73m2
Na 138, K 5.0, Bicarb 23, glucose 156
A1C 8.5, LDL 67, Hb 11.0
Home blood pressure readings run 130-140/75-
85
Blood sugars run 150-200 when checked in themornings
Question 9: What is the next besttherapeutic change to make?
A. Increase metformin to 1000mg twice daily
B. Add lisinopril 10mg once daily
C. Increase amlodipine to 10mg once daily
D. Add metoprolol 25mg twice daily
E. Increase pravachol to 40mg at night
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
40/51
Answer 9:
D: Add metoprolol 25mg bid
Target BPs for hypertension treatment (JNC 7):
General population:
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
41/51
Question 9: Other Answers
A. Increase metformin to 1000mg twice daily
Given his CKD, strong consideration should be given
to switching to another agent rather than increasing it
B. Add lisinopril 10mg once daily
ON-TARGET suggested that dual ACEi and ARB
therapy increases risk for hyperK and cardiac events
Practice not abandoned, but should be approached with
caution
High-normal K would make adding ACEi hazardous
Lancet. 2008; 372:547553
Question 9: Other Answers
C. Increase amlodipine to 10mg once daily
Patient already complains of edema on 5mg dose,
likely to be exacerbated by increase dose
Further rise in heart rate also an unwanted
consequence
E. Increase pravachol to 40mg at night
LDL goal
For CKD without CAD:
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
42/51
Question 10
A 36 yo female nurse presents for furtherevaluation of fatigue and muscle cramping.
Blood pressure is normal
Examination is unremarkable
Plasma 24-hour Urine
Na+ 140 mEq/L Na+ 80 mEq/d
K+ 2.5 mEq/L K+ 170 mEq/d
Cl- 86 mEq/L Cl- 40 mEq/dCO2 28 mEq/L Ca+2 76 mg/d
Mag 1.5 mEq/L Mg+2 7 mg/d
Question 10Continued
After replenishment of her hypokalemia and
hypomagnesemia with IV solutions, her symptoms
resolve
Her only medical problem is GERD for which she
has been taking omeprazole for the past 8 months
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
43/51
Question 10: Which of the following
would be the best next move?
A. Start amiloride
B. Stop the omeprazole
C. Check a diuretic screen
D. Discuss your concerns about surreptitious
vomiting
E. Start spironolactone
Hypokalemia
Etiology
1. Lack of intake
2. Cellular shifts
3. Renal wasting
Often associated with metabolic alkalosis
Hypokalemia can drive and maintain an alkalosis
24-hour urine potassium
Renal vs. non-renal
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
44/51
Renal K wasting
Normo-hypotensive:
Diuretics
Diuretic mimickers
LoopBartters
ThiazideGitelmans
Hypomagnesemia
Emesis
Hypertensive:
Hyperaldosterone statesprimary / secondary
Hypomagnesemia
Etiology
Decreased intake/malabsorption
Renal wasting (cause of or association with low K)
24-hour urine magnesium vs. FeMag
GI wasting:
Short gut syndrome/malabsorption
PPIs
H+important for absorption of metals from gut
Upregulates TRPM6/7 (magnesium channels)
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
45/51
Answer 10: Incorrect Options
A.Amiloride for Gitelmans syndrome Low/normal BP, low urine Ca+2, high urine Cl-,
high urine mag+2
C. Diuretic abuse Low/normal BP, high urine Cl-, high urine mag+2
D. Surreptitious vomiting
Low/normal BP, low urinary Cl-
E. Spironolactone for hyperaldostone state High BP, hypomag less not seen
Differentiating Diuretic Abuse fromBartters/Gitelmans
Both have:
High urine chloride
Upregulated renin and aldosterone
Renal wasting of K/Mag and metabolic alkalosis
History Recurring issueespecially if since childhood, think
genetic
Medical field, weight loss or other medical field
diuretic abuse
Diuretic screen will answer the question
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
46/51
Differentiating Bartters from
Gitelmans Bartters:
Mimics loop diuretics
Acts at NKC2 triporter in thick ascending limb
Causes increased calcium excretion in the urine
Gitelmans:
Mimics thiazide diuretics
Acts at NaCl transporter in distal convoluted tubule Causes calcium reabsorption and low urine calcium
24 hour urine calcium collection differentiates
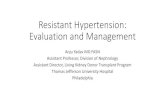
Hypomagnesemia-InducedRenal K+Wasting
Magnesium increases inward movement of
potassium movement through ROMK in the
collecting duct
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
47/51
U
R
I
N
E
3Na+
2K+
K+
Aldo
CORTICAL COLLECTING DUCT
PRINCIPLE CELL
ENaC
BL
O
O
D
Mag+2
U
R
I
N
E
3Na+
2K+
K+
Aldo
CORTICAL COLLECTING DUCT
PRINCIPLE CELL
ENaC
B
L
O
O
D
Mag+2
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
48/51
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
49/51
Case 11
A 28 yr-old female with 18-yr history of diabetes
mellitus is seen at 12 weeks gestation of her first
pregnancy
Enalapril 5 mg/day for HTN and diabetic nephropathy
BP 160/100. The remainder exam is normal.
Laboratory studies reveal: Hgb A1C 10%Cr 0.8 mg/dl
24 hr protein excretion 1.2 gm
Question 11: Which of the followingwould you advise?
A. Increase enalapril to 10 mg per day
B. Replace enalapril with hydrochlorothiazide 12.5mg
per day
C. Continue enalapril and add alpha-methyldopa 250mg twice a day
D. Replace enalapril with alpha-methyldopa 250 mg
twice a day
E. Continue enalapril and add amlodipine 5 mg per day
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
50/51
Answer 11:
D. Replace enalapril with methyldopa Issue: Hypertension in pregnancy
(BP>140/90) Common Internal Medicine issue
Identify medications safe for use during pregnancy or
when attempting to become pregnant
Hypertension in Pregnancy
Angiotensin converting enzyme inhibitors Cross the placenta
Angiotensin II important in the regulation of placental
blood flow and normal fetal growthAssociated with fetal developmental abnormalities in
all trimesters
CV and CNS in first trimester
Renal, limb and others later
-
8/10/2019 1445 Simon Board Simulation in Nephrology and Hypertension
51/51
Answer 11: Hypertension in
Pregnancy
Methyldopa
Labetolol
Long acting CCBs
nifedipine best studied
Hydralazine Thiazides considered safe if
already taking
Safe Meds
Answer 11: Hypertension in
Pregnancy
Classifications of Hypertension in Pregnancy
1. Pre-existing hypertension
Before 20 weeks gestation or lasting 12 weeks
post-partum2. Pre-eclampsia
HTN after 20 weeks, edema, proteinuria
3. Gestation hypertension