144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999

of 14
-
Upload
humayoun-zia -
Category
Documents
-
view
220 -
download
0
Transcript of 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
1/14
Psychological Medicine, 1999, 29, 199212. Printed in the United Kingdom# 1999 Cambridge University Press
Psychometric properties of the Liebowitz Social
Anxiety Scale"
R. G. HEIMBERG,# K. J. HORN ER, H. R. JUS TE R, S. A. SA FR EN, E. J. BRO WN,F. R. SCHNEIE R M. R. LIE BOW ITZ
From the Department of Psychology, Temple University, Philadelphia and Western Psychiatric Institute andClinic of the University of Pittsburgh School of Medicine, Pittsburgh, PA: University of Albany, StateUniversity of New York and New York State Psychiatric Institute and Columbia University College of
Physicians and Surgeons, New York, NY: and Massachusetts General Hospital\Harvard Medical School,Boston, MA, USA
ABSTRACT
Background. The present study provides data on the reliability, validity and treatment sensitivity ofthe Liebowitz Social Anxiety Scale (LSAS), one of the most commonly used clinician-administered
scales for the assessment of social phobia.Method. Three hundred and eighty-two patients from several studies of the treatment of socialphobia were evaluated. An independent assessor administered the LSAS to each patient prior to theinitiation of treatment. Patients also completed other measures of social anxiety and avoidance,although the specific measures varied across samples.
Results. The LSAS and its subscales were normally distributed and demonstrated excellent internalconsistency. The convergent validity of the LSAS was demonstrated via significant correlations withother commonly-used measures of social anxiety and avoidance. These correlations also tended tobe larger than correlations with measures of depression, especially after treatment. However, thepattern of correlations of LSAS subscales with one another and with the other measures suggest thatthe fear subscales and the avoidance subscales may not be sufficiently distinct in clinical samples.The LSAS was also demonstrated to be sensitive to the effects of pharmacological treatments ofsocial phobia over time and in comparison to double-blind pill placebo.
Conclusion. The LSAS appears to be a reliable, valid and treatment sensitive measure of socialphobia. Further study of the LSAS, both in samples with severe social phobia and in communitysamples, is needed.
INTRODUCTION
Social phobia received little research attentionand was not officially classified as a psychiatricdisorder until the publication of the DSM-III(American Psychiatric Association, 1980). How-ever, recent years have witnessed a significantincrease in clinical research, and since that time,there have been substantial contributions to thediagnosis, assessment and treatment of social
" Some parts of this paper were presented at the annual meeting ofthe Anxiety Disorders Association of America, Pittsburgh, PA, inMarch 1996.
# Address for correspondence: Dr Richard G. Heimberg, De-partment of Psychology, Temple University, Weiss Hall, 1701 N.13th Street, Philadelphia, PA 19122-6085, USA.
phobia (Liebowitz et al. 1985; Heckelman &Schneier, 1995; Heimberg & Juster, 1995;Heimberg et al. 1995; Herbert, 1995; Potts &Davidson, 1995; Stein, 1995).
Social phobia is defined by a persistent fear ofembarrassment or negative evaluation whileengaged in social interaction or public per-formance. Activities such as meetings or inter-actions with strangers, attending social gather-ings, formal presentations and those requiring
assertive behaviour are commonly feared byindividuals with social phobia (Rapee, 1995).The recent National Comorbidity Survey (Kess-ler et al. 1994) reported a lifetime prevalenceof 13n3% for social phobia as defined in
199
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
2/14
200 R. G. Heimberg and others
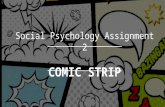
F. 1. TheLiebowitz SocialAnxiety Scale.(FromM. R. Liebowitz (1987). Socialphobia. Modern Problems in Pharmacopsychiatry22, 141173. Published by S. Karger AG: Basel, Switzerland and reproduced here with the permission of the publishers.)
DSM-III-R (APA, 1987), and its prevalenceappears to be increasing (Magee et al. 1996).Social phobia is highly co-morbid with otheranxiety disorders, depression and substance
abuse, and it significantly increases the risk forthese disorders (Schneier et al. 1992). It runs achronic course and is associated with significantimpairments in functioning and overall quality
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
3/14
Liebowitz Social Anxiety Scale 201
of life, as well as an increased risk of suicidalideation and attempts (Leibowitz et al. 1985;Cox et al. 1994; Schneier et al. 1994; Safren etal. 1997). As research in this area continues togain momentum, it is imperative that psycho-
metrically sound assessments of social phobiabe developed and utilized (Cox & Swinson,1995; Greist et al. 1995).
Assessments of social phobia have mostcommonly been conducted in self-report orclinician-administered format. To date, the self-report measures have received more extensiveexamination, and several are considered to bepsychometrically sound (see reviews by Cox &Swinson, 1995; McNeil et al . 1995). Twoclinician-administered scales have been com-monly used in studies of the pharmacotherapyof social phobia, but relatively little informationhas yet been published regarding their psycho-
metric characteristics. These are the LiebowitzSocial Anxiety Scale (LSAS) (Liebowitz, 1987)and the Brief Social Phobia Scale (Davidson etal. 1991, 1997). The purpose of the present studyis to examine the reliability, validity and treat-ment sensitivity of the LSAS.
The LSAS, the first clinician-rating scaledeveloped for the assessment of social phobia(Greist et al. 1995), was designed to assess therange of social interaction and performancesituations that individuals with social phobiamay fear and\or avoid (Liebowitz, 1987). Its 24items are divided into two subscales that addresssocial interactional (11 items) and performance
(13 items) situations. The clinician asks thepatient to rate fear and avoidance during thepast week on 03 Likert-type scales; however,the clinician is given latitude to question thepatients responses and adjust the ratings ac-cordingly. Thus, the LSAS provides six subscalescores: total fear, fear of social interaction, fearof performance, total avoidance, avoidance ofsocial interaction and avoidance of performance.An overall total score is often calculated bysumming the total fear and total avoidancescores, and this index is the one most commonlyemployed in studies of the pharmacotherapy ofsocial phobia. The LSAS is shown in Fig. 1.
The LSAS has been widely used in studies ofpharmacological treatment of social phobia(Reich & Yates, 1988; Munjack et al. 1991;Liebowitz et al. 1992; Versiani et al. 1992;Davidson et al. 1993; Lott et al. 1997; Noyes et
al. 1997) and has also been used in studies ofcognitive behavioural group treatment for socialphobia (Brown et al. 1995; Heimberg et al.1998), but there has been little formal evaluationof its psychometric properties. In the studies of
pharmacological treatments, the LSAS has beenresponsive to change both within treatments andin comparisons between active treatment andplacebo. However, demonstration of change ortreatment-placebo differences does not assurethat an assessment device provides validmeasurement unless we also know that it isreliable and relates to criterion measures (i.e.external indicators) in a predictable manner.
Other studies have reported data directlyrelevant to the psychometric properties of theLSAS. Heimberg et al. (1992) reported thatscores on LSAS subscales were significantlycorrelated with scores on the Social Interaction
Anxiety Scale and the Social Phobia Scale(Mattick & Clarke, 1998), two self-reportmeasures of social phobia with demonstratedreliability and validity. It is of interest that thefear of social interaction subscale of the LSASwas more strongly related to the Social In-teraction Anxiety Scale, which measures anxietyin interactions in dyads or groups, while the fearof performance subscale of the LSAS was morestrongly related to the Social Phobia Scale, ameasure of the fear of being observed orscrutinized by others. Holt et al. (1992) reportedthat LSAS total fear scores discriminated be-tween three groups of participants with social
phobia: those with non-generalized social pho-bia, those with generalized social phobia, andthose with both generalized social phobia andavoidant personality disorder (for informationon subtypes of social phobia, see Heimberg et al.1993; Schneier et al. 1996). Brown et al. (1995)reported that both the total fear and totalavoidance scores of the LSAS discriminatedamong these three groups. In contrast, Herbertet al. (1991) reported in their psychometric studyof the Social Phobia and Anxiety Inventory(Turner et al. 1989) that all measures except theLSAS correlated significantly with this self-report scale. These studies provide data relevant
to the psychometric properties of the LSAS, butno studies to date have specifically focused onevaluating its psychometric adequacy.
The LSASs central position in social phobiaresearch requires that its psychometric properties
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
4/14
202 R. G. Heimberg and others
be formally evaluated. The present study pro-vides data on the distribution characteristics,reliability, validity and treatment sensitivity ofthe LSAS in a large sample of patients withsocial phobia. Patients were pooled from several
treatment studies conducted by the authors toprovide a large enough sample for effectivepsychometric analysis. We addressed the fol-lowing questions: (1) What is the nature of thedistribution of scores on the LSAS and itsvarious subscales? ; (2) What is the internalconsistency of the LSAS and its subscales? (3)Do the fear and avoidance subscales of theLSAS provide distinct information?; (4) Doesthe LSAS correlate with other measures of fearand avoidance in social interaction and per-formance situations?; (5) Does the LSAS cor-relate more strongly with other measures ofsocial anxiety and social phobia than it does
with measures of a different disorder (depres-sion)? ; and (6) Does the LSAS demonstratesensitivity to the effects of treatment comparableto that of other measures of social phobia?
METHOD
Subjects
Three hundred and eighty-two subjects wereadministered the LSAS by an independentassessor prior to the initiation of treatment forsocial phobia. Patients were pooled from severalstudies of social phobia treatment: (1) a studycomparing phenelzine, atenolol and pill placebo(Nl 91) (Liebowitz et al. 1992); (2) the Albany,
New York, site of a collaborative study com-paring cognitivebehavioural group therapy,education supportive group therapy, phenelzineand pill placebo (Nl57) (Heimberg et al. 1998)and other studies of the efficacy of cogni-tivebehavioural group treatment conducted inAlbany (Nl 86) (Brown et al. 1995; Juster et al.1995; Leung & Heimberg, 1996) (total Nl143); (3) the New York site of the collaborativestudy described above (Nl73); and (4) a studycomparing moclobemide and pill placebo (Nl75) (Schneier et al. 1998). Pre-treatment datawere included for all samples as were post-treatment data from the collaborative study.
All subjects met criteria for a DSM-III-R orDSM-IV (APA, 1994) diagnosis of social phobiaas determined by either the Schedule forAffective Disorders and Schizophrenia, Lifetimeversion (modified for the study of anxiety
disorders) (SADS-LA; Mannuzza et al. 1986),the Structured Clinical Interview for DSM-III-R(SCID) (Spitzer et al. 1992), the Anxiety Dis-orders Interview Schedule-Revised (ADIS-R;DiNardo & Barlow, 1988), or the Anxiety
Disorders Interview Schedule for DSM-IV;Lifetime Version (ADIS-IV-L; DiNardo et al.1994). Specific inclusion and exclusion criteriadiffered from sample to sample. Demographicdata for each sample are presented in Table 1.
Assessment of social phobia
Assessor-administered measures
In addition to the LSAS, the independentassessor also completed the Clinicians SeverityRating, a 08 Likert-type rating included in theADIS-R or ADIS-IV-L interview. This ratingindexes distress and impairment experienced bythe patient as a result of his\her social phobia
and is widely used in studies of cognitivebehavioural treatment of social phobia (e.g.Heimberg et al. 1990). Scores on the assessor-administered Hamilton Anxiety Scale (HAMA;Hamilton, 1959) (pre-treatment only) and theHamilton Rating Scale for Depression (HRSD;Hamilton, 1960) were also available for col-laborative study patients.
Self-report questionnaires
Several commonly-used self-report measures ofsocial anxiety and avoidance were also adminis-tered, and these data were used to evaluate thevalidity and treatment sensitivity of the LSAS.
These include the Social Interaction AnxietyScale (SIAS), which measures the anxiety ex-perienced in social interactional situations(Heimberg et al . 1992; Brown et al . 1997;Mattick & Clarke, 1998); the Social PhobiaScale (SPS), which measures the levels of anxietywhen people are scrutinized by others (Heimberget al. 1992; Brown et al. 1997; Mattick &Clarke, 1998); the Social Avoidance and DistressScale (SADS), which measures the level ofanxiety and distress people feel when in socialsituations and their desire to avoid thesesituations (Watson & Friend, 1969) ; the Fear ofNegative Evaluation Scale (FNE), which
measures the concerns people have about thedisapproval of others (Watson & Friend, 1969);and the social phobia subscale of the FearQuestionnaire (FQ-So), which, despite its name,is a measure of the extent of avoidance of feared
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
5/14
Liebowitz Social Anxiety Scale 203
Table 1. Demographic characteristics of patients with social phobia
Total sample(Nl382)
Sample 1(Nl91)
Sample 2(Nl143)
Sample 3(Nl73)
Sample 4(Nl75)
Age (yr)Mean 35n1 34n7 36n3 33n7 34n7.. 9n4 9n0 9n7 10n0 8n5Range 1861 1954 1861 1961 19n59
N % N % N % N % N %
GenderWomen 165 43n4 29 32n6 68 47n6 38 52n1 30 40n0Men 215 56n6 60 67n4 75 52n4 35 47n9 45 60n0
Marital statusSingle 115 54n8 71 49n7 44 65n7 Married 71 33n8 54 37n8 17 25n4 Divorced 23 11n0 17 11n9 6 9n0 Widowed 1 0n5 1 0 n7 0 0
EmploymentFull-time 129 59n7 87 60n8 42 57n5 Part-time 27 12n5 21 14n7 6 8n2 Homemaker 4 1n9 3 2 n1 1 1n4 Student 32 14n8 20 14n0 12 16n4 Retired 2 0n9 2 1 n4 0 0
Unemployed 22 10n2 10 7n0 12 16n4 Education
Some high school 5 2n4 2 1 n4 3 4n3 High school graduate 21 9n9 14 9n8 7 10n1 Some college 46 21n7 25 17n5 21 30n4 College graduate 74 34n9 57 39n9 17 24n6 Graduate work 66 31n1 45 31n5 21 30n4
Ns vary because of missing data. These data were not available for specific samples.
social situations (Marks & Mathews, 1979). TheBeck Depression Inventory (BDI ; Beck et al.1961) was also administered to patients in thecollaborative study and is used here to examinethe discriminant validity of the LSAS.
Data analyses
Psychometric analysis is essentially a statisticalundertaking, and a range of statistical techniqueswere employed. Preliminary analyses involvedthe examination of the demographic charac-teristics of the study sample and of differencesamong the various subsamples. Subsampledifferences in response to the LSAS were alsoevaluated. Chi-square tests were employed forcategorical variables and analyses of variance(ANOVAs) for continuous variables. SignificantF tests were followed with Duncans MultipleRange Tests to examine differences between
pairs of means with alpha levels controlled(P0n05).
Primary analyses addressed the characteristicsof the LSAS in the full sample (Nl382) (allanalyses were also conducted separately for each
subsample; results are available from RichardHeimberg). Skewness (the accumulation of casesin a tail of the distribution) and kurtosis (thetendency for cases to accumulate in the centre ofthe distribution) were examined. These indices
describe deviations from the normal distri-bution. Non-significant skewness and kurtosisindices (1n0) suggest that the distribution isnormal and that parametric statistics may beproperly applied to the data. Internal consistency(the reliability of a test based on the correlationsamong all items) of the LSAS was evaluatedwith Cronbachs (1951) alpha coefficient. Alphacoefficients of approximately 0n800n85 or highermay be considered sufficiently reliable for use inclinical settings (Rosenthal & Rosnow, 1991).However, alpha increases as a function of scalelength (Cronbach, 1970), and direct comparisonsof alpha coefficients for LSAS subscales of
differing length should not be undertaken.Person productmoment correlations were
calculated among the LSAS subscales, betweenLSAS subscales and other measures of socialanxiety and avoidance and between LSAS
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
6/14
204 R. G. Heimberg and others
subscales and the measures of general anxietyand depression. Differences in the magnitude ofspecific pairs of correlations were evaluated withHotellings t test (Rosenthal & Rosnow, 1991).
We examined treatment sensitivity, the ability
of a measure to detect the effects of anintervention, in two different ways. First, weexamined whether the LSAS was sensitive tochange over time (uncontrolled within-treatmentcomparisons). Effect sizes were calculated foreach of the LSAS subscales. Effect sizes werealso calculated for the other measures of socialanxiety to provide a context within which theeffect sizes for the LSAS could be evaluated.This analysis was conducted on pre-treatmentand post-treatment data for patients treatedwith phenelzine in the collaborative study. Thewithin-treatment effect size (d) was calculatedfrom means (M) and standard deviations (..)
using the following formula (Cohen, 1988):
dl(M
Pre-treatmentkM
Post-treatment)
N(..#Pre-treatment
j..#Post-treatment
)\2.
A within-treatment effect size is analogous tothe change demonstrated by a patient in an opentrial. A d ofj1n0 represents improvement equalto 1n0 standard deviation unit from pre-treat-ment to post-treatment. A 95% confidenceinterval (CI) was also calculated for the effectsize associated with each measure. The degree ofchange on any measure is significantly different(P0n05) from zero if the CI for that measuredoes not include zero (Alliger, 1995).
The second analysis of treatment sensitivityexamined the ability of the LSAS to detect theeffect of active treatment over and above theeffects of a control condition. For this purpose,we derived effect sizes for phenelzine in com-parison to pill placebo after 12 weeks oftreatment. Between-treatment effect sizes andCIs were calculated to the following formula(Hedges & Olkin, 1985):
Effect sizel(M
ControlkM
Treatment)
..Pooled
,
where
..Pooledl ((NTreatmentk1) (..Treatment)#j(NControlk1) (..Control)#)(N
TreatmentjN
Controlk2)
.
A between-group effect size indexes theamount of change by which a treatment sur-passes the effects of placebo. Therefore, it isinherently more conservative that the within-treatment effect size. A between-treatment effect
size ofj1n0 represents that the score of thephenelzine group is 1n0 standard deviation unitbetter than that of the placebo group at post-test.
CIs were calculated according to the formulaoffered by Alliger (1995) which corrects forextreme conservatism in the use of CIs in thecomparison of between-condition effect sizeestimators. The difference between the effectsizes for any two measures is significant (P0n05) if the CIs for the measures do not overlap,and the difference between treatments on anymeasure is significant if the CI for that measuredoes not include zero (Alliger, 1995).
RESULTS
Demographic characteristics
Demographic data are presented in Table 1 forthe total sample and each subsample. Data onage and gender were collected for all subsamples.No differences in age were detected (F(3,375)l1n35, NS). The overall sample mean was 35n1years (..l 9n4). Neither were there significantdifferences in the gender composition of thesubsamples (# (3, Nl380)l7n82, NS). Over-all, 56n6 % of patients were male. Remaining
demographic data were reported only for Albanypatients (sample 2) and patients from the NewYork site of the collaborative study (sample 3).These subsamples did not differ in education (#(2, Nl212)l0n47, NS) or in the percentage ofpatients employed on a full-time basis (# (1, Nl216)l0n10, NS). However, a somewhatlarger percentage of Albany patients (37n8 %)than New York patients (25n4 %) were married(# (2, Nl210)l4n74, P0n10).
Subsamples differences in LSAS scores
One-way ANOVAs were conducted on each ofthe pre-treatment LSAS scores of the four
subsamples (see Table 2). All analyses revealedsignificant differences. Duncan Multiple RangeTests (P0n05) demonstrated that patients fromthe moclobemide study (sample 4) achieved thehighest scores in every analysis.
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
7/14
Liebowitz Social Anxiety Scale 205
Table 2. Means (M), standard deviations (S.D.), and analyses of variance for the Liebowitz SocialAnxiety Scale (LSAS) and subscales
Total sample(Nl382)
Sample 1(Nl91)
Sample 2(Nl143)
Sample 3(Nl73)
Sample 4(Nl75) Analyses of
variance
LSAS subscale M (
.
.) M (
.
.) M (
.
.) M (
.
.) M (
.
.) F P
LSAS total score 67n2 (27n5) 65n0 a (27n9) 63n0 a (23n5) 66n5 a (28n0) 78n4 b (30n7) 5n7 0n001Total fear 35n5 (13n6) 34n2 a (14n2) 34n0 a (11n6) 35n3 a (13n7) 40n1 b (15n2) 3n8 0n05Fear of social interaction 16n9 (7n7) 15n7 a (7n6) 16n4 a (6n9) 17n0 ab (8n1) 19n0 b (8n7) 2n9 0n05Fear of performance 18n6 (6n8) 18n5 a (7n6) 17n5 a (5n6) 18n3 a (6n5) 21n0 b (7n5) 4n6 0n05Total avoidance 31n6 (14n5) 30n8 a (14n2) 28n9 a (12n7) 31n1 a (14n7) 38n3 b (16n2) 7n4 0n001Avoidance of social interaction 15n7 (8n2) 15n1 a (8n2) 14n6 a (7n3) 15n6 a (8n5) 18n5 b (9n0) 4n0 0n05Av oi da nc e of pe rfor man ce 16n0 (7n3) 15n6 a (6n9) 14n4 a (6n5) 15n6 a (7n2) 19n7 b (8n2) 9n8 0n001
Means followed by different letters are significantly different ( P0n05) according to Duncans Multiple Range Test.
LSAS distribution characteristics
LSAS total scores were normally distributed(skewnessl 0n17; kurtosislk0n26), as were
total fear (skewnessl0n10; kurtosislk0n22)and total avoidance scores (skewnessl 0n23 ;kurtosislk0n38). Fear and avoidance scoresfor both social interaction and performancewere similarly distributed, with minor positiveskew and minor negative kurtosis.
Table 3. Cronbachs alpha coefficients for theLiebowitz Social Anxiety Scale (LSAS) and
subscales
LSAS subscales
Totalsample
(Nl382)
LSAS total score 0n96Total fear 0n92Fear of social interaction 0n89Fear of performance 0n81Total avoidance 0n92Avoidance of social interaction 0n89Avoidance of performance 0n83
Table 4. Correlations among the Liebowitz Social Anxiety Scale subscales (Nl382)
LSAS subscalesTotalfear
Fear of socialinteraction
Fear ofperformance
Totalavoidance
Avoidance ofsocial
interactionAvoidance ofperformance
LSAS total score 0n98 0n92 0n90 0n98 0n93 0n90Total fear 0n94 0n92 0n91 0n87 0n83Fear of social interaction 0n73 0n86 0n92 0n68Fear of performance 0n83 0n68 0n88Total avoidance 0n94 0n92Avoidance of social interaction 0n74
Internal consistency
Alpha coefficients for all LSAS scores wereuniformly high. Alphas for performance scores
were somewhat lower than alphas for socialinteraction scores, but all were in the excellentrange (see Table 3).
Correlations among LSAS subscale scores
Table 4 presents the correlations among theLSAS scales and subscales for the full sample.Correlations were uniformly high, ranging from0n68 to 0n98. The LSAS total score was so highlycorrelated with total fear and total avoidancethat these indices may be considered inter-changeable (both rsl0n98). The total score wasalso highly correlated with all other subscales (rsl0n9 0 t o 0n93). Fear and avoidance ratings were
also highly correlated, whether they were ex-amined at the level of totals (rl0n91), withinperformance situations (rl0n88), or withinsocial interaction situations (rl0n92). Fearratings in social interaction v. performancesituations were also highly correlated (rl0n73),as were avoidance ratings in social interactions
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
8/14
206 R. G. Heimberg and others
v. performance situations (rl0n74). However,the correlations between fear subscales in socialinteraction v. performance situations and be-tween avoidance subscales in social interactionsv. performance situations were of significantly
lesser magnitude than the correlations betweenfear and avoidance subscales (all Ps0n00001).Correlations among the LSAS subscales after 12weeks of treatment in the collaborative studyrevealed a similar pattern (available fromRichard Heimberg).
Convergent validity
Convergent validity of the LSAS was assessedvia correlations with other self-report andclinician-rated measures of social anxiety andavoidance (see Table 5). These analyses wereconducted on the subgroup of patients whocompleted the entire assessment battery (Nl
178) in order to facilitate the testing of thesignificance of differences between correlations.All correlations between LSAS scores and themeasures of social anxiety and avoidance werehighly significant (P0n001).
The relationships between the LSAS subscalesand the SIAS and SPS were specifically examinedas these correlations have been the focus ofprevious research. The fear of social interactionsubscale of the LSAS correlated 0n76 with theSIAS, a measure of anxiety in social interaction,but only 0n50 with the SPS, a measure of anxietywhile being observed (t(175)l5n81, P0n000001). The avoidance of social interaction
subscale of the LSAS correlated 0n77 with theSIAS, but only 0n47 with the SPS (t(175)l6n79,P0n000001). For the performance subscales,this pattern was reversed. The fear of per-formance subscale correlated 0n52 with the SIASbut 0n65 with the SPS (t(175)l2n54, P0n012).The avoidance of performance subscales corre-lations with the SIAS (rl 0n55) and the SPS (rl0n60) were not significantly different. Whenexamined from another perspective, both per-formance subscales were more highly correlatedwith the SPS than the corresponding socialinteraction subscale, and both social interactionsubscales were more highly correlated with the
SIAS than the corresponding performance sub-scale (all ts2n66, 175 df, all Ps 0n009).
The relative strength of the relationship of theLSAS subscales to the other measures of socialanxiety and avoidance was also examined with a
series of significance tests. Because of the largenumber of these tests, Pwas setat 0n003 (0n05\15tests of differences for each LSAS subscalel0n003. Details of these tests can be obtained fromRichard Heimberg). The LSAS total score was
more strongly correlated with the SIAS thanwith the ADIS Clinicians Severity Rating or theFNE. Total fear was more strongly correlatedwith the SIAS than with the ADIS CliniciansSeverity Rating, the SADS, or the FNE. Thefear of social interaction subscale was morestrongly related to the SIAS than to any othermeasure. The fear of performance subscale wasmore strongly related to the SPS than the ADISClinicians Severity Rating, the SADS, or theFNE. Results were similar for the avoidancesubscales. However, there were generally fewersignificant findings for avoidance than fearsubscales. There were no differences in the
magnitude of correlations between the LSASfear and avoidance subscales and the FQ-So, theonly measure of avoidance included in ourbattery.
Correlations of the LSAS subscales with theother measures of social anxiety and avoidancewere also calculated for the sample of patientswho completed 12 weeks of treatment in thecollaborative study (available from RichardHeimberg). We wished to examine the possibilitythat the correlations reported in Table 5 mighthave been suppressed because of range restric-tion (all patients in treatment-seeking samplesmay receive high scores, artificially restricting
sample variance; improvement as a function oftreatment by some patients may increase samplevariance, allowing stronger relationships to berecognized). In fact, post-treatment correlationswere substantially higher between the ADISClinician Severity Rating and the LSAS sub-scales (rs ranged from 0n74 to 0n81 at post-testcompared to 0n400n52 for the full sample beforetreatment). Smaller increases in magnitude werealso noted for correlations between the LSASscales and the SADS and FQ-So.
Discriminant validity
Discriminant validity of the LSAS was examined
by its correlations with the HAMA, a measureof general anxiety, and the BDI and HRSD,measures of depression. The discriminant val-idity of the LSAS is supported to the extent thatits correlations with other measures of social
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
9/14
Liebowitz Social Anxiety Scale 207
Table 5. Correlations between Liebowitz Social Anxiety Scale (LSAS) and subscales andmeasures of social anxiety and avoidance (Nl178)
LSAS subscales ADIS CSR SADS SIAS SPS FNE FQ-So
LSAS total score 0n52 0n63 0n73 0n61 0n49 0n63
Total fear 0n50 0
n59 0
n70 0
n62 0
n51 0
n61Fear of social interaction 0n50 0n62 0n76 0n50 0n50 0n55
Fear of performance 0n40 0n45 0n52 0n65 0n43 0n59Total avoidance 0n51 0n64 0n72 0n58 0n45 0n61Avoidance of social interaction 0n50 0n67 0n77 0n47 0n46 0n52Avoidance of performance 0n42 0n49 0n55 0n60 0n35 0n60
ADIS CSR, Independent assessor rating of overall distress and interference from the Anxiety Disorders Interview Schedule; SADS, SocialAvoidance and Distress Scale; SIAS, Social Interaction Anxiety Scale; SPS, Social Phobia Scale; FNE, Fear of Negative Evaluation Scale;FQ-So, social phobia subscale of the Fear Questionnaire. All correlations significant at P0n001.
Table 6. Within-treatment effect sizes for theLiebowitz Social Anxiety Scale (LSAS) andother measures of social anxiety for social phobicpatients treated with phenelzine
MeasureEffect
size95%
CI
LSASTotal score 1n34 1n001n67Total fear 1n38 0n991n72Fear of social interaction 1n18 0n781n57Fear of performance 1n40 1n051n75Total avoidance 1n26 0n951n57Avoidance of social interaction 1n15 0n821n48Avoidance of performance 1n24 0n921n56
ADIS CSR 1n72 1n312n13Social Interaction Anxiety Scale 1n35 0n831n88Social Phobia Scale 0n92 0n431n41Fear of Negative Evaluation Scale 1n11 0n551n67Fear Questionnaire Social Phobia Subscale 1n18 0n681n68Soc ia l A voi da nc e a nd Di stres s Sc ale 1n76 1n292n24
ADIS CSR, independent assessor rating of overall distress andinterference from the Anxiety Disorders Interview Schedule.
anxiety and avoidance are higher than itscorrelations with the HAMA, HRSD and BDI.Tests for differences between correlations wereconducted in a subset of patients from thecollaborative study who completed the requisitemeasures at pre-treatment (Nl94) and after 12weeks (Nl83). Because of the large number ofthese tests, P was set at 0n0083 (0n05\6 tests ofdifferences for each LSAS subscale for each ofthe discriminant measuresl0n0083).
At pre-treatment, the correlations of the LSAS
total score with the HAMA, HRSD and BDIwere 0n48, 0n39 and 0n52, respectively. Thesecorrelations may be contrasted with the corre-lations of the LSAS total score with the othermeasures of social anxiety and avoidance in this
sample of 94 patients, which ranged from 0n46 to0n68, with a median of 0n57. However, in onlyone of 18 tests was the LSASs correlation withthe social anxiety measure significantly greaterthan the correlation with the discriminant
measure. After 12 weeks of treatment, the LSAS,the BDI and HRSD, and the other measures ofsocial anxiety and avoidance were readminis-tered, and the pattern was more clear-cut. Thecorrelation of the LSAS total score with theHRSD was 0n52 and its correlation with the BDIwas 0n56. These correlations contrast with thecorrelations of the LSAS total score with theother measures of social anxiety and avoidance,which ranged from 0n45 to 0n82 in this sample,with a median of 0n76. Statistical tests revealedthat the correlation with the social anxietymeasure was significantly greater than thecorrelation with the discriminant measure in 8 of
12 instances, clearly supporting the discriminantvalidity of the LSAS total score. The HAMAwas not administered at post-test.
Results for the remaining LSAS subscaleswere generally similar to those for the LSAStotal score, although somewhat weaker for theavoidance subscales than for the fear subscales.These data are available from Richard Heim-berg.
Treatment sensitivity
Within-treatment (uncontrolled) effect sizes
As seen in Table 6, patients treated withphenelzine demonstrated significant within-con-
dition effect sizes for all measures. Effect sizesfor the LSAS scales ranged from 1n151n40.These effect sizes were within the range of effectsizes for the other measures (0n921n76) and notsignificantly different from any.
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
10/14
208 R. G. Heimberg and others
Table 7. Between-treatment effect sizes for the Liebowitz Social Anxiety Scale (LSAS) subscalesand other measures of social anxiety: phenelzine versus pill placebo
Measure Effect size 95 % CI
N(Phenelzine\
placebo)
LSASTotal score 0n67 0n560n78 26\27Total fear 0n65 0n540n76 26\27Fear of social interaction 0n58 0n470n69 26\27Fear of performance 0n69 0n580n80 26\27Total avoidance 0n67 0n560n78 26\27Avoidance of social interaction 0n65 0n540n76 26\27Avoidance of performance 0n61 0n500n72 26\27
ADIS-R CSR 0n71 0n600n82 25\26Social Interaction Anxiety Scale 0n55 0n430n67 22\25Social Phobia Scale 0n50 0n390n61 24\25Fear of Negative Evaluation Scale 0n39 0n280n50 24\26Fear Questionnaire Social Phobia Subscale 0n61 0n500n72 23\24Social Avoidance and Distress Scale 0n80 0n680n92 24\26
ADIS CSR, independent assessor rating of overall distress and interference from the Anxiety Disorders Interview Schedule.
Between treatment (controlled) effect sizes
In Table 7, the effect sizes and confidenceintervals for these comparisons are listed. Theeffect sizes for the LSAS subscales ranged from0n5 8 t o 0n67, indicating that phenelzine wasassociated with LSAS scores at post-treatmentthat surpassed those of placebo patients by one-half a standard deviation or more. The othersocial anxiety measures had a wider range ofeffect sizes, from 0n39 to 0n80. The FNE was themeasure least sensitive to phenelzine-placebodifferences, but there were few other differences.
DISCUSSION
In this paper, we have presented the results ofseveral analyses of the psychometric charac-teristics of the LSAS. Data from nearly 400patients with social phobia were utilized toexamine the distribution characteristics, internalconsistency, convergent validity, discriminantvalidity and treatment sensitivity of the LSASsubscales. The majority of our findings providestrong support for the continued use of theLSAS and provide a degree of confidence in thevalidity of previous studies that have employedthis measure of fear and avoidance associated
with social phobia.Fear and avoidance as measured by the LSAS
scales and subscales were normally distributedin this sample. Neither skewness (lack of sym-metry of the distribution) nor kurtosis (the
degree to which scores cluster in the centre of thedistribution) were problematical, suggesting thatparametric statistics may be safely applied toLSAS scores. More importantly, the shape ofthe distribution suggests that, even within apatient population, fear and avoidance arecontinuous variables that may differ from patientto patient with social phobia.
The LSAS demonstrated excellent internalconsistency for the total score as well as thespecific subscale scores (total fear, fear ofperformance, fear of social interaction, totalavoidance, avoidance of performance,avoidanceof social interaction). Higher alphas coefficients
for the total score, total fear, and total avoidanceare a probable artefact of greater scale length.Avoidance subscales demonstrated somewhatlower alphas than the fear subscales, but all wereclearly in the acceptable range.
Evidence for the convergent validity of theLSAS was derived from its significant andsometimes substantial correlations with othercommonly used self-report and clinician-ratedmeasures of social anxiety and avoidance.Interestingly, the LSAS was more highly corre-lated with several of the self-report measuresthan it was with the Clinicians Severity Ratingfrom the Anxiety Disorders Interview Schedule,
suggesting that method variance was not a largecontributor to the magnitude of these corre-lations. The relatively modest correlations be-tween the LSAS and the ADIS rating may arisefrom at least two sources. First, the LSAS
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
11/14
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
12/14
210 R. G. Heimberg and others
social anxiety\avoidance, general anxiety, ordepression. The lack of separation of fear andavoidance may or may not reflect the true stateof nature. Since avoidance behaviour is thetheoretical consequent of fear, the two constructs
may actually be highly correlated. However, onoccasion in clinical practice, we see social phobiapatients whose levels of avoidance do not matchtheir levels of fear (e.g. the highly anxious singlemother who endures the anxiety of a stressful
job to make certain that her children are fed). Itmay be that the format of the rating of eitherfear or avoidance or the collection of avoidanceratings after fear ratings have been obtainedmay spuriously increase the correlations betweenthese sets of ratings. Alternatively, fear andavoidance may be more strongly related amongclinical subjects than among persons whosesocial fears are not associated with extreme
impairment. Study of the responses of normal ornormally anxious individuals to the LSAS andof alternative rating formats may shed light onthe relationship between fear and avoidance.
The current lack of discriminability betweenLSAS fear and avoidance raises the question ofthe utility of the calculation of overall totalscores (i.e. adding fear and avoidance scorestogether). In fact, it appears that there was littleto gain in our sample since the correlation of thetotal score with either fear or avoidance totalswas 0n98. Clearly, the LSAS total score per-formed well in this study. However, since theavoidance scale mimicked the fear scale in most
of its relationships with other measures, butseemed to do so a bit less strongly, the additionof avoidance items to fear items added littleclarity. However, it remains possible that newertreatments for social phobia may have differen-tial effects on fear and avoidance and futurestudies should evaluate this prospect.
The data presented here provide support forthe use of the LSAS. However, they do notimply that the current subscale structure of theLSAS is the most valid or the most useful. Sincethe items on the LSAS and the social interactionversus performance subscales were rationallyrather than empirically generated, it is possible
that some items classified as social interactionalmay actually fit better with the items on theperformance scale or vice versa, or that somesituations have aspects of both interactional andperformance demands, or that the social inter-
actional versus performance distinction is notthe most efficient construct on which to baseseparate subscales. In fact, in a recent study ofthe SIAS and SPS (Safren et al . 1998), aconfirmatory factor analysis failed to uphold the
social interaction versus performance distinctionand exploratory factor analyses revealed thatthe SPS (mostly having to do with performing infront of or being observed by others) containedseparate factors foranxiety about being observedby others and for fear that others will noticeones anxiety symptoms. A similar analysis ofthe LSAS will be reported in a separate paper.
While this study was conducted with a largesample of patients and its results are highlysupportive of the reliability and validity of theLSAS, it is important to note some limitations.First, we conducted a series of analyses todetermine whether the various subsamples in-
volved in the study were equivalent. While thiswas the case for many measures, there weresome differences. Moclobemide study (sample 4)patients scored higher on the LSAS than all ofthe other subsamples. The reasons for thisoutcome are unclear. Secondly, the total samplewas a relatively well functioning one. Approxi-mately one-half the sample was married; two-thirds had graduated from college, and a similarnumber were employed on a full-time basis.Although preliminary analyses in our datasetsuggest that greater impairment is associatedwith higher LSAS scores," the reliability, val-idity, the utility of the LSAS with more severely
impaired samples is a topic for future research.Other topics for future studies of the LSASinclude the development of a briefer form of themeasure, the relative utility of the LSAS as aclinician-administered measure versus a self-report questionnaire, and the performance ofthe LSAS in other cultures.
In conclusion, the LSAS was found to be areliable and valid measure of social phobia in alarge out-patient sample. Our findings supportits past and continued use in the assessment of
" To examine this issue in a preliminary way in our own sample,
we conducted tests of the relationship of education (high school orless v. college v. post-graduate education), employment (unemployedv. employed on a full-time basis), marital status (single v. married),andliving situation(living alone or with parents v. living with spouse,significant others, peers, or children). Poorer functioning in each ofthese areas was related to higher scores on LSAS subscales. Fulldetails are available from Richard Heimberg.
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
13/14
Liebowitz Social Anxiety Scale 211
social phobia. Further development of the LSASis an important agenda for future research.
This study was supported by grants from the NationalInstitute of Mental Health to Dr R. G. Heimberg
(MH44119), Dr M. R. Liebowitz (MH40121) and DrF. R. Schneier (MH47831) and to the New YorkState Psychiatric Institute MHCRC (PO5 MH30906).
REFERENCES
Alliger, G. M. (1995). The small sample performance of four tests ofthe difference between pairs of meta-analytically derived effectsizes. Journal of Management 21, 789799.
American Psychiatric Association (1980). Diagnostic and StatisticalManual of Mental Disorders, 3rd edn. APA: Washington, DC.
American Psychiatric Association (1987). Diagnostic and StatisticalManual of Mental Disorders, 3rd edn. revised. APA : Washington,DC.
American Psychiatric Association (1994). Diagnostic and StatisticalManual of Mental Disorders, 4th edn. APA: Washington, DC.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. E. & Erbaugh,
J. K. (1961). An inventory for measuring depression. Archives ofGeneral Psychiatry 4, 561571.
Brown, E. J., Heimberg, R. G. & Juster, H. R. (1995). Social phobiasubtype and avoidant personality disorder: Effect on severity ofsocial phobia, impairment, and outcome of cognitivebehavioraltreatment. Behavior Therapy 26, 457486.
Brown, E. J., Turovsky, J., Heimberg, R. G., Juster, H. R., Brown,T. A. & Barlow, D. H. (1997). Validation of the Social InteractionAnxiety Scale and the Social Phobia Scale across the anxietydisorders. Psychological Assessment 9, 2127.
Cohen, J. (1988). Statistical Power Analysis for the BehavioralSciences, 2nd edn. Lawrence Erlbaum Associates: Hillsdale, NJ.
Cox, B. J., Direnfeld, D. M., Swinson, R. P. & Norton, G. R. (1994).Suicidal ideation and suicide attempts in panic disorder and socialphobia. American Journal of Psychiatry 151, 882887.
Cox, B. J. & Swinson, R. P. (1995). Assessment and measurement. InSocial Phobia: Clinical and Research Perspectives (ed. M. B. Stein),pp. 261291. American Psychiatric Press: Washington, DC.
Cronbach, L. J. (1951). Coefficient alpha and the internal consistency
of tests. Psychometrica 16, 297334.Cronbach, L. J. (1970). Essentials of Psychological Testing, 3rd edn.
Macmillan: New York.Davidson, J. R. T., Potts, N. L. S., Richichi, E. A., Ford, S. M.,
Krishnan, K. R. R., Smith, R. D. & Wilson, W. H. (1991). TheBrief Social Phobia Scale. Journal of Clinical Psychiatry 52,(supplement), 4851.
Davidson, J. R. T., Potts, N. L. S., Richichi, E. A., Krishnan,K. R. R., Ford, S. M., Smith, R. D. & Wilson, W. H. (1993).Treatment of social phobia with clonazepam and placebo. Journalof Clinical Psychopharmacology 13, 423428.
Davidson, J. R. T., Miner, C. M., DeVeaughGeiss, J., Tupler, L. A.,Colket, J. T. & Potts, N. L. S. (1997). The Brief Social PhobiaScale: a psychometric evaluation. Psychological Medicine 27,161166.
DiNardo, P. A. & Barlow, D. H. (1988). The Anxiety DisordersInterview Schedule, Revised (ADIS-R), Graywind Publications:Albany, NY.
DiNardo, P. A., Brown, T. A. & Barlow, D. H. (1994). Anxiety
DisordersInterviewSchedule for DSM-IV: LifetimeVersion (ADIS-IV-L). Graywind Publications: Albany, NY.
Greist, J. H., Kobak, K. A., Jefferson, J. W., Katzelnick, D. J. &Chene, R. L. (1995). The clinical interview. In Social Phobia:Diagnosis Assessment and Treatment (ed. R. Heimberg, M. Liebo-witz, D. Hope and F. Schneier), pp. 185201. Guilford Press: NewYork.
Hamilton, M. (1959). The assessment of anxiety states by rating.British Journal of Medical Psychology 32, 5055.
Hamilton, M. (1960). A rating scale for depression. Journal ofNeurology, Neurosurgery, and Psychiatry 23, 5662.
Heckelman, L. R. & Schneier, F. R. (1995). Diagnostic issues. InSocial Phobia: Diagnosis Assessment, and Treatment (ed.R. G. Heimberg, M. R. Liebowitz, D. A. Hope and F. R.
Schneier), pp. 320. Guilford Press: New York.Hedges, L. V. & Olkin, I. (1985). Statistical Methods for Meta-analysis. Academic Press: Orlando.
Heimberg, R. G. (1994). Cognitive assessment strategies and themeasurement of outcomeof treatment for social phobia. BehaviourResearch and Therapy 32, 269280.
Heimberg, R. G. & Juster, H. R. (1995). Cognitivebehavioraltreatment: literature review. In Social Phobia: Diagnosis, As-sessment and Treatment (ed. R. Heimberg, M. Liebowitz, D. Hopeand F. Schneier, pp. 261309. Guilford Press: New York.
Heimberg, R. G., Dodge, C. S., Hope, D. A., Kennedy, C. R. Zollo,L. & Becker, R. E. (1990). Cognitive behavioral group treatmentof social phobia: comparison to a credible placebo control.Cognitive Therapy and Research 14, 123.
Heimberg, R. G., Mueller, G. P., Holt, C. S., Hope, D. A. &Liebowitz,M. R.(1992). Assessmentof anxiety in social interactionand being observed by others: the Social Interaction Anxiety Scaleand the Social Phobia Scale. Behavior Therapy 23, 5773.
Heimberg, R. G., Holt, C. S., Schneier, F. R., Spitzer, R. L. &
Liebowitz, M. R. (1993). The issue of subtypes in the diagnosis ofsocial phobia. Journal of Anxiety Disorders 7, 249269.
Heimberg, R. G., Liebowitz, M. R., Hope, D. A. & Schneier, F. R.(eds.) (1995). Social Phobia: Diagnosis, Assessment and Treatment.Guilford Press: New York.
Heimberg, R. G., Liebowitz, M. R., Hope, D. A., Schneier, F. R.,Holt, C. S., Welkowitz, L., Juster, H. R., Campeas, R., Bruch,M. A., Cloitre, M., Fallon, B. & Klein, D. F. (1998). Cognitivebehavioral group therapy versus phenelzine in social phobia: 12-week outcome. Archives of General Psychiatry (in the press).
Herbert, J. D. (1995). An overview of the current status of socialphobia. Applied and Preventive Psychology 4, 3951.
Herbert, J. D., Bellack, A. S. & Hope, D. A. (1991). Concurrentvalidity of the Social Phobia and Anxiety Inventory. Journal ofPsychopathology and Behavioral Assessment 13, 357368.
Holt, C. S., Heimberg, R. G. & Hope, D. A. (1992). Avoidantpersonality disorder and the generalized subtype in social phobia.Journal of Abnormal Psychology 101, 318325.
Kessler, R. C., McGonagle, K. A., Zhao, S., Nelson, C. B., Hughes,
M., Eshleman, S., Wittchen, H. U. & Kendler, K. S. (1994).Lifetime and 12-month prevalence of DSM-III-R psychiatricdisorders in the United States: results from the NationalComorbidity Survey. Archives of General Psychiatry 51, 819.
Juster, H. R., Heimberg, R. G. & Engelberg, B. (1995). Self selectionand sample selection in a treatment study of social phobia.Behaviour Research and Therapy 33, 321324.
Leung, A. W. & Heimberg, R. G. (1996). Homework compliance,perceptions of control, and outcome of cognitivebehavioraltreatment of social phobia. Behaviour Research and Therapy 34,423432.
Liebowitz, M. R. (1987). Social phobia. Modern Problems inPharmacopsychiatry 22, 141173.
Liebowitz, M. R., Gorman, J. M., Fryer, A. J. & Klein, D. F. (1985).Social phobia: review of a neglected anxiety disorder. Archives ofGeneral Psychiatry 42, 72936.
Liebowitz, M. R., Schneier, F. R., Campeas, R., Hollander, E.,Hatterer, J., Fyer, A., Gorman, J., Papp, L., Davies, S., Gully, R.& Klein, D. F. (1992). Phenelzine vs atenolol in social phobia: a
placebo-controlled comparison. Archives of General Psychiatry 49,290300.
Lott, M., Greist, J. H., Jefferson, J. W., Kobak, K. A., Katzelnick,D. J., Katz, R. J. & Schaettle, S. C. (1997). Brofaromine for socialphobia: a multicenter, placebo-controlled, double-blind study.Journal of Clinical Psychopharmacology 17, 255260.
McNeil, D. W., Ries, B. J. & Turk, C. L. (1995). Behavioral
-
7/31/2019 144- Heimberg Et Al Psychological Medicine LSAS Psycho Metrics 1999
14/14
212 R. G. Heimberg and others
assessment: self-report, physiology and overt behavior. In SocialPhobia: Diagnosis, Assessmentand Treatment (ed.R. G. Heimberg,M. R. Liebowitz, D. A. Hope and F. R. Schneier), pp. 202231.Guilford Press: New York.
Magee, W. J., Eaton, W. W., Wittchen, H.-U., McGonagle, K. A. &Kessler, R. C. (1996). Agoraphobia, simple phobia, and socialphobia in the National Comorbidity Survey. Archives of General
Psychiatry 53, 159168.Mannuzza, S., Fyer, A. J., Klein, D. F. & Endicott, J. (1986).Schedule for Affective Disorders and Schitzophrenia-LifetimeVersion modified for the study of anxiety disorders (SADS-LA):rationale and conceptual development. Journal of PsychiatricResearch 20, 217325.
Marks, I. M. & Mathews, A. M. (1979). Briefstandard self-rating forphobic participants. Behaviour Research and Therapy 17, 263267.
Mattick, R. P. & Clarke, J. C. (1998). Development and validationofmeasures of social phobia scrutiny fear and social interactionanxiety. Behaviour Research and Therapy 36, 455470.
Munjack, D. J., Burns, J., Baltazar, P. L., Brown, R., Leonard, M.,Nagy, R.,Koek, R.,Crocker,B. & Schafer, S. (1991). A pilot studyof buspirone in the treatment of social phobia. Journal of AnxietyDisorders 5, 8798.
Noyes, R., Moroz, G., Davidson, J. R. T., Liebowitz, M. R.,Davidson, A., Siegel, J., Bell, J., Cain, J. W., Curlik, S. M., Kent,T. A., Lydiard, B., Mallinger, A. G., Pollack, M. H., Rapaport,M., Rasmussen, S. A., Hedges, D., Schweizer, E. & Uhlenhuth,
E. H. (1997). Moclobemide in social phobia: a controlled dose-response trial. Journal of Clinical Psychopharmacology 17, 247254.Potts, N. L. S. & Davidson, J. R. T. (1995). Pharmacological
treatments: literature review. In Social Phobia: Diagnosis As-sessment and Treatment (ed. R. Heimberg, M. Liebowitz, D. Hopeand F. Schneier), pp. 334365. Guilford Press: New York.
Rapee, R. M. (1995). Descriptive psychopathology of social phobia.In Social Phobia: Diagnosis, Assessment and Treatment (ed.R. Heimberg, M. Liebowitz, D. Hope and F. Schneier), pp. 4166.Guilford Press: New York.
Reich, J. R. & Yates, W. (1988). A pilot study of treatment of socialphobia with alprazolam. American Journal of Psychiatry 145,590594.
Rosenthal, R. & Rosnow, R. L. (1991). Essentials of BehavioralResearch: Methods and Data Analysis. McGraw-Hill: New York.
Safren, S. A., Heimberg, R. G., Brown, E. J. & Holle, C. (1997).Quality of life in social phobia. Depression and Anxiety 4, 126133.
Safren, S. A.,Turk, C. L. & Heimberg,R. G. (1998). Factorstructureof the Social Interaction Anxiety Scale and the Social PhobiaScale. Behaviour Research and Therapy 36, 443453.
Schneier, F. R., Johnson, J., Hornig, C. D., Liebowitz, M. R. &Weissman, M. M. (1992). Social phobia: comorbidity and mor-
bidity in an epidemiologic samples. Archives of General Psychiatry49, 282288.
Schneier, F. R., Heckelman, L. R., Garfinkel, R., Campeas, R.,Fallon, B. A., Gitow, A., Street, L., Del Bene, D. & Liebowitz,M. R. (1994). Functional impairment in social phobia. Journal ofClinical Psychiatry 55, 322331.
Schneier, F. R., Liebowitz, M. R., Beidel, D. C., Fyer, A. J., George,M. S., Heimberg, R. G., Holt, C. S., Klein, A. P., Lydiard, R. B.,Mannuzza,S., Martin, L. Y., Nardi, E. G., Roscow, D. B., Spitzer,R. L., Turner, S. M., Uhde, T. W., Vasconcelos, I. L. & Versiani,M. (1996). Social phobia. In DSM-IV Source Book, Vol. 2 (ed.T. A. Widiger, A. H. Frances, H. A. Pincus, M. J. First, R. RossandW. Davis), pp.507548.AmericanPsychiatric Press: Washing-ton, DC.
Schneier, F. R., Goetz, D., Campeas, R., Marshall, R., Fallon, B. &Liebowitz, M. R. (1998). Placebo-controlled trial of moclobemidein social phobia. British Journal of Psychiatry, 172, 7077.
Spitzer, R. L., Williams, J. B. W., Gibbon, M. & First, M. B. (1992).The Structured Clinical Interview for DSM-III-R (SCID). I.
History, rationale, and description. Archives of General Psychiatry49, 624629.
Stein, M. B. (ed.) (1995). Social Phobia: Clinical and ResearchPerspectives. American Psychiatric Press: Washington, DC.
Turner, S. M., Beidel, D. C., Dancu, C. V. & Stanley, M. A. (1989).An empirically derived inventory to measure social fears andanxiety: the Social Phobia and Anxiety Inventory. PsychologicalAssessment 1, 3540.
Versiani, M., Nardi, A. E., Mundim, F. D., Alves, A. B., Liebowitz,M. R. & Amrein, R. (1992). Pharmacotherapy of social phobia: acontrolled study with moclobemide and phenelzine. British Journalof Psychiatry 161, 353360.
Watson, D. & Friend, R. (1969). Measurement of social evaluativeanxiety. Journal of Consulting and Clinical Psychology 33, 448457.