13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf

of 22
-
Upload
timothy-blankenship -
Category
Documents
-
view
217 -
download
0
Transcript of 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
1/22
Accid. And. & Pw. Vol. 21. No. 6. pp. 553-574, 1989 caol-4575/89 s3.00+ .ooPrinted in Great Britain. 0 1989 Pergamon Press pk
BIOMECHANICS OF THE HUMAN CHEST,ABDOMEN, AND PELVIS IN LATERAL IMPACTDAVID C. VIANO, IAN V. LAU, and CORBIN ASBURYBiomedical Science Department, General Motors Research Laboratories,Warren, MI 480909055, U.S.A.
andALBERT I. KING and PAUL BEGEMANBioengineering Center, Department of Mechanical Engineering, Wayne State University,Detroit, MI 48202, U.S. A.
(Receiv ed 22 December 1988)Abstract-Fourteen unembalmed cadavers were subjected to 44 blunt lateral impacts at velocitiesof approximately 4.5,6.7, or 9.4 m/s with a 15 cm flat circular interface on a 23.4 kg pendulumaccelerated to impact speed by a pneumatic impactor. Chest and abdominal injuries consistedprimarily of rib fractures, with a few cases of lung or liver laceration in the highest severityimpacts. There were two cases of pubic ramus fracture in the pelvic impacts. Logist analysis ofthe biomechanical responses and injury indicated that the maximum Viscous response had aslightly better correlation with injury than maximum compression for chest and abdominal im-pacts. A tolerance level of VC = 1.47 m/s for the chest and VC = 1.98 m/s for the abdomenwere determined for a 25% probability of critical injury. Maximum compression was similarlyset at C = 38% for the chest and at C = 44% for the abdomen. The experiments indicate thatchest and abdominal injury may occur by a viscous mechanism during the rapid phase of bodycompression, and that the Viscous and compression responses are effective, complementarymeasures of injury risk in side impact. Although serious pelvic injury was infrequent, lateralpublic ramus fracture correlated with compression of the pelvis, not impact force or pelvicacceleration. Pelvic tolerance was set at 27% compression.
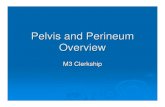
INTRODUCTIONOne of the next frontiers in automotive safety is to improve occupant protection in sideimpact crashes. The basis for product improvements is an understanding of crash typesand interior contacts that result in serious and fatal injury when the vehicle is struck onthe side. It is also important to understand the underlying mechanism of injury andhuman response to lateral impact forces since these are the bases to develop applicableinjury criteria and set human tolerance levels. This information is also pivotal to thedevelopment of anthropomorphic test devices or surrogates that have human-like re-sponses to force and can be used in crash or impact tests to evaluate potential counter-measures. The foundation for this study is injury biomechanics [National Research Coun-cil (NRC) 1985; Viano et al. 1989a; Viano 19881.An evaluation of side impact crash injuries from the 1986 Fatal Accident ReportingSystem (FARS) [National Highway Traffic Safety Administration (NHTSA) 19881 in-dicates that 31.8% of passenger car fatalities occur in crashes with the principal directionof force lateral on the vehicle (Fig. 1). Two thirds of the fatalities are in multivehicleaccidents where the car is struck by a passenger car, truck, or other vehicle, while theother third involve single vehicle accidents into primarily fixed objects. Approximatelyan equal number of fatalities occur in driver side and passenger side lateral impactcrashes, and the toll in human life is about 8,000 victims annually.A recent study of individual multivehicle side impact crashes was conducted byViano et al. (forthcoming) using selected cases from National Accident Sampling System(NASS) and National Crash Severity Study (NCSS). It indicates that a majority of thefatal crashes occur at an intersection and that the victim is primarily an older occupant.An evaluation of national statistics from NASS indicates that when side and frontalimpact crashes are compared side impacts represent about 47% of the crashes involvingserious to fatal passenger car injury. When crashes are separated into multivehicle (car-
553
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
2/22
554 D. C. VIANO et al.SINGLE VEHICLE ACCIDENTS MULTI-VEHICLE ACCIDENTS
(31.1% SIDE) (66.9% SIDE)
1.146 6.9n10.1%14.6xI(_11,322 TOTAL2,465 SIDE 11
13,600 TOTAL5,450 SIDE m
Fig. 1. Distribution of impacts by principle direction of force in single-vehicle and multivehicle fatalcrashes (1986 FARS). Side impacts are 31.8% of the fatalities.
car) or fixed object impacts, the age of the occupant emerges as an important factor inside impact crashes. In particular, multivehicle side impact crashes are a major fraction(40%-54%) of the cause of injuries to occupants over the age of 40, whereas occupantsof this age range are infrequently involved in side impact crashes into fixed objects.
Additional studies of individual fatal multivehicle side impact crashes in NASS andNCSS indicates that a majority (52%) of fatal injury involves the chest and abdomenwith impact on the side interior a principal factor. This level of involvement is similarto that observed in other epidemiologic studies (Malliaris et al. 1982; Foret-Bruno et al.1983; Partyka and Rezabek 1983; Mills and Hobbs 1984; Otte et al. 1984; Danner et al.1985; Rouhana and Foster 1985; Thomas et al. 1987). However, hip fractures are animportant complicating injury in older patients (Kelsey et al 1978, Holbrook et al 1984)and should be considered in side impact testing. Based on this information, the currentstudy addresses the biomechanics of chest, abdominal, and pelvic impact in simulatedmultivehicle crashes where serious injury may occur from side interior contact. Theresearch focuses on an investigation of the mechanisms of injury and tolerance to bluntlateral impact of unembalmed cadavers.The current study simulates the forces of contact on the chest, abdomen, and pelvisin a side impact crash. A pendulum impact mass is used to load the body over a rangeof impact speeds and follows a protocol that has been used previously to study frontalimpact responses (Kroell 1976; Kroell et al. 1981, 1986; Hess et al. 1982; NHTSA 1986;Viano 1978). This allows direct comparison of the lateral impact responses to the currentunderstanding from frontal tests, and takes advantage of a proven methodology forresearch on impact biomechanics.
The study also addresses a range of candidate mechanical responses for injuryassessment. These include the Viscous (Viano and Lau 1983,1988; Lau and Viano 1986,Rouhana et al. 1984) and compression (Nahum et al. 1970; Kroell et al. 1971; Neathery1974; Sacrests et al. 1982) responses for the chest and abdomen since they are an effectivemeasure of injury risk by impact and crushing mechanisms, respectively. Based on Cesariet al. (1980) and Cesari and Ramet (1982), hip acceleration is investigated for pelvicfracture.The Viscous response is evaluated since it is an underlying mechanism of soft tissuetrauma to internal organs and vessels in frontal impact. It also helps pinpoint the timeof greatest injury risk in an impact. This has focused efforts on vehicle design changesto improve product safety (Lau et al. 1987). The Viscous response measures the risk ofserious and life-threatening trauma in cadaver and animal studies. In addition, there areLogist risk functions currently available to assess severe injury risk as part of routinecrash and impact testing with the Hybrid III dummy (Horsch, et al. 1985; Lau et al.1987).
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
3/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact 555Although response and injury will be compared with peak acceleration measure-
ments, acceleration is an unsatisfactory correlate and not a causal factor in soft tissuehuman chest and abdomin~ injury (Kroell et al. 1974; Cesari et al. 1981; Brun-Cassanet al. 1987). Even so, accelerations have been included in this study to further evaluatethe sufficiency of this approach for safety assessment. Although acceleration criteriahave a rich history in product safety testing, our current understandings of human injuryindicate that body deformations are the causal factor of soft tissue chest and abdominalinjury and such deformation is not adequately assessed by acceleration measures (Viano1987a; Lau and Viano 1988; Tarriere et al. 1988). Because of the high compliance ofthe hip to lateral forces, pelvic acceleration may be a measure of skeletal injury risk,but we will also evaluate deformation of the pelvis as a potential injury criterion.
A scientific understanding of frontal impact injury biomechanics has been developedby using the pendulum impact methods of this study. This approach has successfully ledto the development of human-like body deformation characteristics that include theforce-deflection or compliance behavior of the chest and abdomen under impact loading.The data has enabled the development of improved anthropomorphic test devices (ATD)that realistically simulate the human response in frontal impact (Foster et al. 1977; Horschand Viano 1984) and better assess product safety improvements (Melvin et al. 1985;Mertz 1985). There has also been an advance in our understanding of the mechanismsof injury and tolerance criteria of the human body to impact force. Much of this hasbeen based on human cadaver tests, which help define body compliance and assess injuryseverity based on skeletal trauma. Comparable research (Viano et al. 1989c; Kroell etal. 1986) has been conducted for frontal and lateral impacts with a physiological modelto study life-threatening trauma by laceration or rupture of internal organs and vesselsor by interruption of normal cardiac or respiratory function. In frontal and lateral impact,the Viscous response has been shown to be the principal mechanical cause of soft tissueinjury and this study aimed to assess its comparable tolerance level and risk function inlateral impacts of human cadavers while furthering our understanding of lateral impactbiomechanics .
MATERIALS AND METHODSUnembahned cadavers were provided through the Department of Anatomy at Wayne
State University Medical School as part of a willed-body program. * They had an averageage of 53.8 it 13.9 years and body mass of 67.2 * 16.2 kg (Table 1). Anthropometricdata were compiled for each specimen prior to testing and followed recommended prac-tices of the National Highway Traffic Safety Administration, Department of Transpor-tation.Specimen selecti on and handl i ngThe specimens were selected on an age, condition, and cause of death criteria, whichlimited age to approximately 65 years unless the specimen was of good skeletal condition,to specimen not having a long period of bed rest or debilitating disease prior to death,and to specimen without infectious disease. Each specimen was examined radiologicallyto assure against preexisting fractures or anomalies that would influence experimentalresponses. All cadavers were tested after rigormortis had passed. In some of the spec-imens, the average time lapsed between expiration and actual testing was one to twoweeks. In other specimens, the time lapse was greater between the expiration and testing,so the specimen was frozen (4F) for a period of time. Prior to testing, the specimenswere stored in a refrigerator unit at 35F. No attempt was made to bring internal body
*The rationale and experimental protocol for use of human cadaver research subjects in this programhave been reviewed by the Research Laboratories Human Research Committee. The research complies withthe provisions of the Uniform Anatomical Gift Act, follows guidelines established by the U.S. Departmentof Trans~rtation, National Highway Traffic Safety Administration and commendations of the NationalResearch Council of the National Academy of Sciences, and adheres to the provisions of The Declaration ofHelsinki.
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
4/22
556 D. C. VIANOet al.Table 1. WSU lateral impact cadaver information
Chant Waist HipRuns Cadaver SSX 44 Weight Height Breadth Breadth Breadth# # be=.) w (-1 (=I (-1 (cm): 863RNfl4 935x 8479:10 954lNY211-13 95614-16 99317-22 98623-28 047
4976633866:492962
107.00 176.044.00 153.669.85 174.056.25 166.556.26 159.061.69 171.076.20 175.070.76 173.070.30 173.083.91 176.5
37.5 37.026.8 28.5Z:oO 25.67.0 28.01.527.0 as.5 29.028.0 33.0 35.029.5 33.5 39.531.5 31.6 32.530.0 28.0 33.532.5 34.5 37.029-33 008 Female 52 53.07 157.0 28.5 29.5 33.034,35 063 YSlS 64 46.54 173.0 32.0 34.0 32.036-39 UOMI Yale 37 67.59 186.5 30.5 30.5 32.540-4s uoM2 Yale 64 75.76 178.6 33.5 34.5 39.5
temperature up to physiologic levels at the time of testing. However, the specimens wereexposed to room temperature for several hours during instrumentation and preparation.
Znstrumentut ion and preparati on. The cadaver was instrumented with an array ofaccelerometers attached to the spine and pelvis. A triaxial accelerometer package wasattached to the first, eighth, and twelfth thoracic vertebrae and a similar triaxial accel-erometer package attached to the pelvic region at the third sacral vertebra. Targets wereattached to the triaxial clusters for photographic coverage and film analysis.The arterial system of the cadaver was pressurized by normal saline infused througha Foley catheter inserted with its end in the aorta above the diaphragm. A vent tubewas inserted in the brachial artery. Prior to an experiment, the catheter balloon waspressurized to block the flow below it and saline was pumped into the body until itflowed out of the vent tube. The vent was then clamped, thus ensuring that the systemabove the blockage included the chest and upper abdominal organs. The lung wascarefully drained of fluid and aerated repeatedly with room air prior to testing. The lungwas pressurized.
Necropsy. After testing, x-rays were taken, instrumentation was removed from thespecimen, and the cadaver was returned to cold storage. Autopsy was performed by aboard certified pathologist, and special attention was paid to injury of the chest, ab-domen, and pelvis. At the completion of the necropsy, the specimen was returned tothe Department of Anatomy for appropriate disposition.Data analysis. High-speed movies of the impact were taken at 2,000 frames persecond from the frontal and 500 frames per second from the posterior and overheadviews. Frame-by-frame analysis of the impact formed the basis for the instantaneousdeflection data of the torso and hip. Deflection data were processed using an establishedalgorithm by Viano and Lau (1988) and Lau and Viano (1986) to derive the compressionand Viscous responses. Contact was indicated by a flash on a movie frame and a si-multaneous tick mark on an electronic data channel, generated by the same contactswitch closure. This defined time zero. In the film analysis, interpolation was madebetween adjacent frames to establish time zero where necessary. The acceleration chan-nels were processed according to a digital Society of Automotive Engineers (1987)channel class or a finite impulse response filter. A summary follows of the injury criteriaand injury functions that were examined for their discriminating ability in linking me-chanical inputs with injury outcomes and defining tolerance levels for critical injury.Inj ury funct i onsViscous Response [VC(t)]-A time function produced by multiplying the instan-teous velocity of deformation and compression responses (units in m/s, derived fromfilm data).Compression Response [ C(t)]-The instantaneous deformation divided by the initialtorso thickness along the axis of the impact (dimensionless, derived from film data).
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
5/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact 557Spinal Acceleration Response [ Gsp(t)]-Instantaneous lateral acceleration of the
spine measured by an accelerometer on Tl, T8, T12, or pelvis at S3 (units in g derivedfrom electronic data).
Force [F(t)]-Impact force resulting from pendulum contact (units in kN, derivedfrom acceleration of the pendulum from electronic data multiplied by the pendulummass).Injury cr i ter ia
Viscous Criterion [VC]max-The peak Viscous response.Compression Criterion [ C]max-The peak compression response.Spinal Acceleration Criterion [Gsplmax-The peak lateral or resultant spinal ac-celeration response.
Force Criterion [F]mar-The peak force acting on the body.Stat isti cal methods. Injury risk functions were computed using the logist function in
the Statistical Analysis Package (SAS). This function relates the probability of injuryoccurrence P(X) to the magnitude of a response parameter x based on a statistical fit toa sigmoidal function P(X) = [l + exp(cw - Qx)]-. The goodness-of-fit of the statisticis quantified by the chi-squared x2, p-value (p), and correlation coefficient (R).
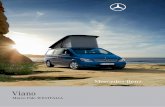
The impact. While the initial tests were conducted with the WSU translationalimpactor, subsequent experiments were conducted with a power-assisted pendulum (Fig.2). The 23.4 kg pendulum was freely suspended by guide wires and accelerated to impactspeeds of approximately 4.5,6.7, or 9.4 m/s in 5 cm by a pneumatically charged cylinderwith thrust piston. The impactor operates on the following principle. The thrust pistonis attached to a disc that slides tightly in the charge cylinder and is set against an orificeplate by a holding pressure. A small diameter O-ring seals the set chamber from theopening to the charge cylinder. Because of the area difference, a much larger pressurecan be put into the charge cylinder with equilibrium being maintained (a higher forceon the disc from the set chamber). The level of charge pressure determines the thrustvelocity.
Impact is initiated by injecting a triggering pressure between the sliding disc and
ATIC IMPACTOR
ACCELERATIO
Fig. 2.MP21:6-D
Experimental set-up with a pneumatic power-assisted pendulum and upright supported specimen.
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
6/22
558 D. C. VIANO et al.orifice plate and venting the set chamber. This allows the greater charge pressure to acton the entire diameter of the disc and rapidly accelerates the piston and power pendulumto impact speed. After 10 cm of travel, the disc and piston are decelerated by an internalpad allowing the pendulum to continue in free flight. Impact speed was confirmed by alight-beam trap and time-interval counter. The forward motion of the pendulum wasabruptly stopped after 20 cm of contact by a force-limiting cable tether. The cadaverwas suspended upright with hands and arms overhead. The specimen was rotated 30so the point of pendulum contact was lateral on the thorax or abdomen. This protocolwas used to assure that full lateral thoracic and abdominal impact occurred with the axisof force through the center of gravity of the torso. It resulted in controlled compressionof the torso without coincident rotation of the body about the spine axis. The center ofpendulum impact on the thorax was aligned with the xiphoid process (7.5 cm belowmidsternum). Abdominal impact was aligned 7.5 cm below the xiphoid (1.5 cm belowmidsternum). Pelvic impacts were conducted at 90 lateral with the impactor centeredon the greater trochanter.
The pendulum interface was a smooth, flat, 15 cm diameter circular disc with theedges rounded. The axis of impact force was aligned through the center of gravity ofthe torso for chest and abdomen tests (approximately 2 cm anterior of the intrathoracicsurface of the vertebrae). A uniaxial accelerometer was attached to the pendulum andits response was multiplied by the pendulum mass to give the force of impact. A sus-pension system released the arms at impact and approximated a free torso response toimpact. The off-side of impact was padded to gradually support the free body response.Multiple tests were conducted on a specimen to increase biomechanical response data.This could include a low-severity left abdominal impact, an injurious high-severity tho-racic test, and a lateral pelvic impact. Injuries were assigned to the appropriate impactcondition.
RESULTSPeak biomechanical responses and resulting injuries are summarized in Tables 2-4
for the three severities of impact on the chest, abdomen, and pelvis. Data on individualimpacts is published separately in a companion paper (Viano 1989). Three of six testsin the high-velocity chest impact series resulted in lacerative injury of the lung, liver,diaphragm, kidney, or spleen. These injuries were associated with flail chest of thethoracic rib cage, which was defined as two fractures on four consecutive ribs or morethan eight rib fractures in the thorax. In the high-velocity chest impact series, five of sixspecimens had flail chest with an average of 14 rib fractures. There were only two casesof severe upper abdominal injury in the high-severity impacts and they consisted oflaceration of the liver and diaphragm. In these impacts, only one of four specimenexperienced more than eight rib fractures. There were six high-velocity lateral impactsof the hip and, in spite of the high severity of loading, there were only two incidents ofskeletal injury. The fractures involved the pubic ramus in both cases. In terms of overallinjury severity, each exposure was summarized by the number of rib fractures or skeletal
Table 2. Summary biomechanics and injury for lateral thoracic impactTest Speed (q's)4.42 * 0.86 6.52 f 0.32 9.33 * 0.71
Force (kN)Defl ecti on (cmCompression X)VC (0)GT1-y9T8-yGT12-y!&ERib Fractures #)
2.67 * 0.99 3.10 f 0.48 6.30 * 0.908.40 t 1.30 1x. 20 f 1.35 14. 18 * 1.7926. 1 * 4.1 34. 9 f 4.5 43. 2 f 3.9
0.82 t 0.23 1.10 t 0.18 2.06 i 0.4114.0 * 6.0 40.1 t a.316.5 * 6.5 33.8 f 8.1 62.6 t 20.412.6 f 3.5 26.4 i 5.1 54.6 t 25.30.4 f 0.9 2.8 * 0.5 4.0 * 0.60.4 f: .9 2.8 t 0.6 3.8 f 0.40.4 * 0.9 5.2 f 1.5 12.7 A 4.5
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
7/22
B~omechani~ of the human chest, abdomen, and pe.lvis in lateral impactTable 3. Summary biome~hani~ and injury for 1ateraI abdominal impact
559
4.79 f 0.77 T-i $y $d$ 9.40 f 0.87Force (kh')Deflection cm)Compression 1x)vc (m/s)GT1-7QT8-7'112-y!E:Rib Fractures (#)
2.41 * 0.49 3.71 f 0.48 6.60 f 1.1010.83 * 2.30 11.43 t 0.76 14.80 t 2.3832.0 f 6.6 36.2 f 1.a 46.8 f 3.10.77 f 0.23 1.26 t 0.12 2.22 * 0.416.9 i 2.0 17.6 t 1.9 37.5 t 11.010.8 f 4.4 26.9 f 7.1 29.1 t 6.911.6 t 6.2 29.8 f 12.4 44.3 f 9.00.7 t 1.2 2.0 t 1.4 2.0 t 2.30.7 * 1.2 2.0 f 1.4 1.8 f 2.10.8 f 1.6 3.3 t 3.0 3.8 t 4.6
injury, the maximum severity of skeletal trauma (SAIS), and the maximum overallseverity of injury (MAIS). In all chest and abdominal impacts the responses increasedas the severity of impact speed increased. The experimental protocol maximized theopportunity to define a correlation between injury and the measured response parametersbut also set up the possibility that unrelated or weakly related parameters would alsocorrelate with injury. While this maximized the possibility of defining relationships, itminimized the chance of pinpointing underlying causal biomechanics.
A comparison of the chest and abdominal impacts indicates a similar level of peakforce, deflection, and compression for each level of impact severity. The Viscous re-sponse was higher in the abdominal impacts probably because of less skeletal structureresisting the low-deflection response. A lack of vitality in the upper abdominal organsmay have led to a lower average severity of abdominal injury than occurred in chestimpacts of comparable impact severity. Internal chest injury was frequently associatedwith multiple rib fractures indicative of flail chest from the lateral impact. For the pelvicimpacts, the force increased with the increasing severity of impact speed. In contrast,the average deflection went down between the higher severity impacts, although therewas an increase in variability in the responses. This, in part, may be due to higherdeflections with pubic ramus fracture and lower levels without. For pelvic impacts, thehigher forces and accelerations in the highest severity impacts imply more whole-bodyacceleration with lower average levels of pelvic compression. The blunt lateral pelvicimpacts generally resulted in no injury with these test conditions.
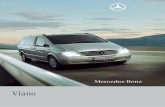
Figures 3-5 summarize key biomechanical responses obtained for the experimentsat the low-, middle-, and high-severity impact of the chest, abdomen, and pelvis. Theforce-deflection responses define the compliance of the torso or pelvis under lateralimpact and the area under each curve represents the amount of energy absorbed bybody deformation. The force-time, deflection-time, and Viscous-time responses furtherdefine impact biomechanics of the human. Figure 6 is an example of the dynamic re-sponses of other measurements made during the experiment. Impact usually involves ahigh, short-duration acceleration of the nearside structures causing a rapid velocity changeas the tissues and loaded structure are quickly brought to a common velocity with the
Table 4. Summary biomechanics and injury for iateral petvic impact
Force (LN) 5.45 .t 1.66 6.81. 1.60 11.20 t 1.48Deflection cm) 4.80 f 1.60 9.88 t 1.34 7.83-i 2.27Compression a) 13.6 f 4.0 26.0 f 0.3 22.9 f 6.0QT8-y 7.7 f 3.1'T12-7 15.0 f 12.6 18.6 f 3.9 31.6 f 8.6QL3-, 34.4 * 15.0 23.6 f 3.6 39.9 i 26.8MAIS 0 0 0.7 r 1.0SAIS 0Pelvic Fracture 0 : 0.7 * 1.00.3 * 0.6
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
8/22
4.42 m/s
0E
D. C. VIANO et al."1
/.. .I ..!
e-..;, e....II..
I! . .I..0.1
D
-0.aFJJ*-_? * \\. * --_).. *-.. ._.......,,.. J.._. -e&m S.33 m/sFig. 3. Grouped dynamic responses for lateral thoracic impacts.
impactor. Loads are transferred through skeletal structures which have compliance andmay delay the peak responses at sites distant from the point of loading. Internal tissuesand organs respond to the rate and amount of body deformation.Logist analysis was applied to the biomechanical responses to identify risk functionsfor four or more rib fractures (MAIS 3 +) or critical injury (MAIS 4+ or 9+ ribfractures). The Viscous response had a strong correlation with serious to critical injuryfor chest and abdominal impact (Tables 5 and 6). Maximum chest compression was alsoa good correlate with serious injury, whereas none of the responses correlated with therisk of moderate skeletal injury in the lateral abdominal impacts. Pelvic compressionemerged as the only correlate with pubic ramus fracture (Table 7). Although based ononly two cases of injury, there is a strong correlation in contrast to acceleration responses.
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
9/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact 561
4.70 mls 6.03 ml5 9.40 mlaFig. 4. Grouped dynamic responses for lateral abdominal impacts.
The Viscous response emerged as an effective measure of injury risk. The Logistinjury probability functions are plotted in Fig. 7 for the probability of critical injurybased on the Viscous and compression response of the chest and abdomen, and compres-sion for lateral pelvic impact. A 95% confidence interval is also given. The functionsare sigmoidal, indicating three distinct regions. For low values of the response, there isa region of very low risk of injury. Similarly, for the very high values of the response,there is a flat high-risk of critical injury. In between is a region where injury risk isproportional to the associated response. The sigmoidal function is typical of a riskdistribution with a biomechanical response. In addition to the underlying relationshipbetween the biomechanical response and injury, it represents the distribution in toleranceof a population with weaker and stronger subjects.
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
10/22
562 D. C. VIANO et al.
1 r--\I
iG/---~-.%.__..-! i--_-_-J
ii l!IE\..., . ._. 2/1 . .-..-.... lz_...,(.... . ._......_..__ 1)1_!;. I.?? . .I%__.0 0 90 10 10 .o 50 (0TIME(ms)4.03 mls 6.77 ml-a 9.65 m/s
Fig. 5. Grouped dynamic responses for lateral pelvic impacts.
Based on Logist analysis, it was possible to determine tolerance levels of the mea-sured responses. A risk level of 25% probability of critical injury was used to establishtolerance levels for the chest and abdomen (Table 8). This probability level is consistentwith previous studies of injury risk from human cadaver and animal impacts (Lau andViano 1986, 1988; Lau et al. 1987; Viano and Lau 1988). This level of injury risk issimilar to that found in current crash protection standards. For pelvic impact, the tol-erance is set for 25% probability of pubic ramus fracture.
DISCUSSIONThis study has shown that the Viscous response is an effective biomechanical pa-
rameter to assess injury risks in lateral impact of the chest and abdomen. The findingis consistent with previous research (Viano and Lau 1983, 1988; Lau and Viano 1986)on impact injury in frontal loading of the chest and similar research on the abdomen(Lau et al. 1987; Horsch et al. 1985). In those studies the Viscous response was found
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
11/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact 563Table 5. Logist analysis of lateral thoracic impact injuries
Logist StatisticsCritsria/Ssvarity@D50 a P X2 P E4+ Rib Fxs (MA18 +)_
vc = 1.0 m/ac = 33.9%
CT8- J = 28.5 gQT12_y = 20.4 gF =3.f%kN
%+ Bib Fxs (IUIS +),vc = 1.55 m/sc = 39.5%
GT8- y = 49.5 gCTlZ-7= 45.2 gF = 5.4% kfi
58.03 87.96 21.2 O.CW109.53 3.23 21.2 O.#C3.62 0.123 7.2 0.0074.15 0.204 10.2 0.0013.62 1.10 5.2 0.009
10.02 5.08 13.7 O.CCC31.22 0.785 13.5 O.COO12.95 0.252 10.2 O.ooO3.66 0.031 7.8 0.002515.92 112.25 19.9 O.CCC
0.950.960.520.520.48
0.770.750.76O.&p0.95
to be the causal mechanism and strongest correlate with injury. Recent experiments byLau and Viano (1988) have shown that serious injury to soft tissues and organs occurat the time of peak Viscous response, well before maximum deflection. We expect thatserious abdominal and thoracic injury from high-speed lateral impact may be similarlyassociated with the rapid phase of compression.
Recent experiments by Viano et al. (1989~) with anesthetized swine show that lateralimpact injury is associated with a Viscous mechanism. Serious internal thoracic andabdominal injury occurred with minimal skeletal damage, a finding that is consistentwith tests on small animal models (Jonsson et al. 1979; Rouhana et al. 1984). The recentresearch with swine confirms that in a physiologic model with organ sizes and weightssimilar to that of man the Viscous response is an effective measure of injury risk inlateral impact. The finding is also supported by Cooper and Maynard (1986)) who founda relationship between lung injury and the Viscous response when anesthetized swineare struck in the side with a high-velocity, light-weight rubber disk.
Table 6. Logist analysis of lateral abdominal impact injuries
0 P4+ Rib Fxs (MAIS +]
vc = 2.01 O/8c = 51.211
'TS- J = 28.2 gc+l2_7 30.1 gF = 5.10 kN
Critical njury (MAIS +lVC = 2.25 m/sc = 45.8%
QTS- y = 35.0 g'TlZ-y= 46.5 gF = 5.87 kN
1.83 0.913 1.1 0.295 (NS) 0.002.19 0.043 0.3 0.687 (NS) 0.003.04 0.108 3.1 0.078 (HS) 0.252.08 0.059 2.5 0.114 (NS) 0.181.75 0.288 0.9 0.348 (NS) 0.00
8.54 3.81 5.1 0.013 0.5015.29 0.348 4.6 0.032 0.487.39 0.206 3.6 0.051 (Ns) 0.367.73 0.159 4.9 0.027 0.5363.37 7.70 8.6 0.004 0.75
Logist StatisticsX2
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
12/22
D. C. VIANO et al.
60
70-60-50-
g 40- 9Sg 30- ;_5 9e, 20- ij:: lo-
o--10--20 -f
7060
1
-20
lmpoct Fore*6- ACCEL - 18-A-
- I0 ;0 :0 TOTime (ms)
10
i
ABDOMEN - 6.738
bnpoel Fore*ACCEL. - TOem-
-2- 60Time (ms)
10
1PfxViS - 8.70
Lumbar Ace.---
-2- 60Time (ms)
601
RUNP - T 12
RUNIJ-TlRUN 8 - 112---
4Q- RUN 45 - T 8RUN rS - 1 12---
60-j
( (0 20 40 60Time (ms)
Fig. 6a. Examples of impact force and spinai acceleration for lateral thoracic, abdominal, and pelvicimpacts at 6.7 m/s.
The correlation of maximum deflection or compression with injury is consistent withrelationships found in previous studies on the frontal impact of human cadavers (Kroell1976; Viano 1978; Tarriere et al. 1988) and anesthetized swine (Viano and Warner 1976;Viano et al. 1977; Kroell et al. 1981, 1986). However, a relationship was not foundbetween compression and injury in recent lateral chest impacts of anesthetized swine(Viano et al. 1989c). In those tests, a relationship existed between low- and middle-severity impacts but was not found between the middle- and high-severity tests. Spinalacceleration was higher between the middle- and high-severity tests as well as impact
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
13/22
60 e
6
Gomechanics of the human chest, abdomen, and pelvis in lateral impactCHEST - O-TO m/o a0
lmpoct Form 1565
RUN 16 - f 1
7060so
i a
e
0 I a-10-20 1 -2
i 1 -40 -4 1 7, 20 40 60 0 20 40 60
70
6050
Time (ms)ABDOMEN - 9.80 mla 60
hPOSl Fore *ACCEL T e- - -
1 -20 t I 120 40 60 20 40 60lime (ms) Tme (ms)
PELVIS - 9.50 ml8e-
6-Impact Fort*Lumbar Act.
-2-0 20 40 60Time (ms)
Time (ms)
RUNJ4-11
60
1
-*O; 60lime (ms)
Fig. 6b. Examples of impact force and spinal acceleration for lateral thoracic, abdominal, and pelvicimpacts at 9.5-9.8 m/s.
force, resulting in more whole-body displacement of the animal. The failure of maximumcompression to correlate with an increased severity of injury is further evidence thatsoft tissue trauma may not be related in all cases to rib fractures and the peak value ofbody defo~ation. However, in some circumstan~s injury may occur by a crushing loadon the body, in which maximum compression would be an important factor.Although acceleration correlates with some injury in this study, it has been shownin other research to be unrelated when a range of test-types are merged. In two studiesby Lau and Viano (1986, 1988), pendulum and sled tests data independently correlated
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
14/22
566 D. C. VIANOet al.Table 7. Logist analysis of lateral pelvic impact injuries
Criteria/SeverityPubic Rams Fracture
c = 27.4 %d = 10.3 cm
CTS- y = 46.1 g%2-y
1,I;;
:%y *F = 17.3 kN
Logist Statisticsa P x2 P rl
84.02 3.07 11.411 0.001 0.90816.91 1.84 3.64 0.010 (NS) 0.6356.80 0.120 1.87 0.172 (NS) 0.03.65 0.047 0.78 0.378 (NS) 0.03.16 0.022 0.34 0.661 (NS) 0.03.71 0.218 0.70 0.402 (NS) 0.6
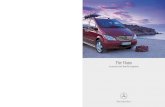
body acceleration and injury, but, when the data were merged no relationship existedbetween peak accelerations and injury. This situation has been shown for frontal impactand is a result of acceleration being the sum of two independent components: oneassociated with deflection of the body and the other with whole-body displacement. Ourstudies have shown that body deformation is the key factor in impact injury and thatwhole-body acceleration primarily brings the body to a common velocity with the im-pactor or sled. When a test series tightly controls the relative contribution of eachcomponent, correlation may be found between acceleration and injury. However, withtests that vary the relative contribution of each component to the overall response,correlation is generally lost. We did not attempt to measure near-side rib accelerationin these tests as the transducer could be the cause of rib fracture as found in earlierresearch. Thus, it was not possible to assess acceleration functions, such as TTI (Eppingeret al. 1984; Morgan et al. 1986).We reanalyzed data from the frontal impact cadaver tests by Kroell et al. (1974)and Kroell (1976) according to an identical protocol to that used in this study. High-speed photographs of body deformation from the frontal impact tests were reanalyzedto determine external deflection. The Viscous response was computed from the deflectionfollowing our routine procedure (Lau and Viano 1986; Viano and Lau 1988). The rean-alyzed data are shown in the bottom portion of Fig. 8 for direct comparison to the resultsof the current study. The force-deflection behavior of the human chest in lateral impactis similar to that of the chest in blunt frontal loading of equivalent severity. However,the individual and boundary responses for force-deflection show that the force plateauand initial stiffness are lower in lateral impact of the chest. This is consistent with therib cage geometry since the ribs are flatter and less supported for a lateral loadingdirection.This work is part of an effort to define the global biomechanics of the human chestand abdomen. It is possible to characterize the force-deflection response by an initialstiffness, and average plateau force in the mid-deflection region. This was done for thefrontal and lateral chest impacts and is plotted in Fig. 9 for an orientation from frontal(O), through 60 lateral, to 120 lateral. Solid lines connect regions where test data areavailable and dotted lines represent an estimate of what the full global biomechanicalresponse may be when a complete set of responses is collected for the 6.7 m/s bluntimpact condition. The orientation of impact is also shown using a skeleton to aid in theinterpretation of test conditions.The force-deflection characteristics of the human chest are an important responsefor the development of anthropometric test devices that simulate the human responseto impact and assess injury risks. Figure 10 summarizes the peak force and deflectionresponses from lateral impacts of human cadavers at three test speeds, as well as infor-mation from recent tests with the DOTSID and EUROSID at similar speeds (note thatdeflection is an internal measurement made in the dummy). Current side impact dummiesdevelop significantly higher plateau forces and lower deflections even assuming 25 mmadditional skin compression of the human cadaver and anesthetized swine. This lack of
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
15/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact
Fig. 7. Probability of AIS 4 I- injury as a function of the maximum Viscous and compression (deflection)response from Logist analysis of thoracic, abdominal, and pelvic impact data (the broken lines are a95% confidence interval).
bio~delity in force-dejection response of the current side impact ATDs is a signi~~antdeficiency in their ability to simulate the human response and injury in side impact testsand assess energy management concepts.Biofidelity is important because the design of side interior padding to optimizeresponse in the dummies will result in much stiffer materials to be compatible with thehigh-force levels developed by the dummies. Stiff materials may essentially eliminatethe safety potential for real occupants who develop much lower forces and thus needsofter materials (Rouhana et al. 1986; Viano 1987a, 1987b, 1987~). The difference incompliance between current test dummies and the human will also result in significantdifferences in occupant kinematics during a side impact. In particular, the greater de-flection experienced by the human chest and abdomen will allow the head to move more
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
16/22
568 D. C. VIANO t al.Table 8. Tolerance levels for lateral impact
Chest AIS 4+1vc = 1.47 a/s0 = 38.4%
%-y = 46.2 gc l2_y = 31.6 gF = 5.48 kN
Abdolnen AIS '1VC = 1.98 m/sc = 43.7x
GT8-y = 30.7 S (119)GT12-y= 39.0 gF = 6.73 kN
Pelvis (Pubic ams Fracturesc = 27%D = 9.6 cm (NS)
%3-y = 93.1 g (NS)F = 12.0 kN (NS)
Based on 25% Probability njury
laterally with respect to the vehicles side interior and will result in a signi~cantly differenttrajectory of the head. In addition, the shoulder may be an important load path for sideimpact protection as side interior loading on the shoulder may reduce forces on the chestand abdomen and may limit lateral displacement of the head. Therefore, proper torsoand shoulder biofidelity in a side impact dummy should be assured. Recent evaluationof normal driving (Viano et al. 1989b) indicates that a majority of drivers have their lefthand on the steering wheel while passing through an intersection and fewer than 10%have their arm at their side. This indicates that direct loading on the side of the chestand abdomen should most frequently occur in multivehicle side impact crashes. Theseaspects are important to a systems engineering approach to improving side impactprotection.Direct loading of the chest and abdomen is an important cause of injury to near-side occupants in multivehicle side impact crashes. Injuries can occur during the rapidcompression phase of loading since the occupant experiences hid-velocity impact bythe side interior in a severe crash. Since the population at risk in side impact crashes issignficantly older than that in frontal impacts (Viano et al 1989), the understanding ofinjury mechanisms and tolerances from this study should have direct application to thedevelopment of improved side interiors. In addition, the selection of appropriate sideinterior pads requires the use of a test device with human-like force-deflection charac-teristics and proper injury response measurements. This needs to be the first step in aneffort to match side interior padding with human tolerances, thus improving side impactcrash protection. Previous and current research on human cadavers shows that theViscous response is the best correlate of soft tissue, internal organ, and skeletal injuryrisk in the chest and abdomen of elderly specimen. Use of VC offers the possibility ofmaking realistic improvements in side impact safety. We should also underscore the pointthat improper use of an acceleration-based criteria may reduce or eliminate the ultimate
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
17/22
Biomechanics of the human chest. abdomen, and pelvis n iateral impact 569
0: 10 2 * 6 a 10DEFLECTION (cm)
8i
DZOf u- -* gem-__ .O m4- .n1ml. . - - . . . . . .XECL-_0 12fF
x 14FF___
0 zoFM__. 19FMI *_0 18FM
TIME (ms)
P\ . 22FM.19FM-._,016FM- .dl SfM.Xl 4ff- - _ _VlZFf
1 -0.3 !0 110 20 Tk4Ff;mS) A0 50 SO 0 10 20 TIM:~ms) 40 50 60Fig. 8. Corridors for the force-deflection response of human cadavers impacted frontally at midsternumon the thorax [from a reanalysis of data previously published by Kroell (1976)] and for the lateralthoracic impacts of the study. Response data for the frontal thoracic impacts are shown in the lowerportion of the figure.
benefits of padding in side impact crashes, and may pa~icularly place the elderly at riskof injury, when the use of proper injury criteria may lead to realistic improvements insafety (Viano 1987a, 1987b, 1987~).In terms of side impact loading of the pelvis, our experiment complements theresearch work conducted in Europe as part of the EUROSID development (Cesari etal. 1980; Cesari and Ramet 1982; TN0 1987). Figure 11 summarizes the data from ourstudy and that of previous experiments using a 17.3 kg impactor with a spherical contactsurface. The slightly higher force levels from our study are consistent with the flatpendulum face used in our experiments. Our trend of increasing peak force with higher
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
18/22
D. C. VIANO et al.
1.ABDOMEN
icI
,c
1-
,
CHEST
120 90 60 30 00 30 60 90 1200
:INITIAL STIFFNESS (kN/cn;)
,I I I I I I I I I120 90 60 30 00 30 60 90 1204
Fig. 9. The global impact response of the chest and abdomen is represented by the plateau force andinitial stiffness of the average (and + 1 standard deviation) human response. Solid lines connect knowndata and broken lines represent estimates of the human responses. The photos at the bottom of thecurve define the location and orientation of impact on a human skeleton.
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
19/22
Biomechanics of the human chest, abdomen, and peivis in lateral impact 571
0 001Sl00 EUROSIO
a.... 0 CAOAVCR
ICHESTI
-.....By-b.2m/s-.*...... I....;. .C..
6.7 m/t0.. x.
I., -..h y. . + ,
t 0PA& Oaflection (G)
u
o..... 0 oolslo6.2 m/s 0 EURO!30..*%.-....+ 0 CAOAVfRi. 5...., .I_
0.. -...0 . ~~77~,,. +_9 +..Y.., ... .
.,m/r ,&,$I+0
0 OOTSlO0 NROSIOl ADAVER
lo 20 SOTIma (ms)
10 20 JOTine (ms)
Fig. 10. Plot of the peak force and deflection from blunt lateral impact of the human cadaver andcurrent side impact test dummies at three levels of impact severity.
impact speed is similar to the trend of the European study (TN0 1987). As seen in theirwork, the EUROSID dummy develops higher forces than the human cadaver response,particularly at the higher impact speeds. Our study does permit some observations onappropriate injury criteria to assess hip injuries in side impacts. The average fractureforce for the pubic ramus was 9.78 + 0.52 kN . This value is higher than the averagefracture force for pubic ramus injury from ten experiments conducted in Europe. Intheir study, the average fracture force was 7.15 + 2.08 kN . Those injuries occurred witha lighter impact mass at an average impact velocity of 9.98 + 1.64 m/s, which is similarto the speed of our injury experiments. A spherical impact interface may cause lowerforces for similar deflections of the hip. Logist analysis of our data indicated a strongcorrelation of injury with compression of the pelvis. In contrast, no correlation was foundwith pelvic acceleration or impact force (Table 7).On the basis of this study and our previous research, we believe that the maximumViscous response should be limited to protect against critical injury during the rapidphase of body deformation of the chest and abdomen during a side impact. As shownin previous work by Lau and Viano (1988), serious internal injury can occur without asignificant number of rib fractures or rib cage injury at all. This evidence supports thepotential for the early occurrence of soft tissue injury at about the time of maximumViscous response and where deflection or compression of the body has reached onlyabout half of its rn~irn~n value. We also believe in the need to limit max~um compres-sion during crash testing to protect against crushing injuries that may occur by largedeformations of the chest and abdomen, This is clearly a different mechanism of injurythan the Viscous mechanism. Limiting the Viscous and compression response is a com-
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
20/22
572 D. C. VIANO et al.SIDE IMPACT OF THE HIP
GM ELjROSlD/
/ INRETS/ SURoSD
25
20
2s, 158
9+j 10c?
5
0 +0
GM ostrFlat lmpoctor0 Avrra o Roaponrr0 Pubic P(amus Fracture
Sphrrlcol lmpoctorl ubic RamurFracturr
I 1 I I 13Impa6ct Velocity &-I/S)
12 15
Fig. 11. Peak force as a function of impact velocity for blunt lateral impact of the pelvis. Data areshown for cadaver impacts with a spherical impact interface conducted by INRETS (TN0 1987) withaverage values for the fracture level of the pubic ramus and similar data from the current experimentswith a blunt impact interface. Also shown are similar tests conducted on the EUROSID andDOTSID dummies.plementary approach to assessing safety systems (Lau and Viano 1986; Viano and Lau1988). Our data also indicate that compression of the pelvis may be a better predictorof hip fracture than pelvic acceleration or force.
REFERENCESBrun-Cassan, F.; Pincemaille, Y.; Mack, P.; Tarriere, C. Contribution to the evaluation of the criteria proposedfor thorax-abdomen orotection in lateral impact. In Proceedings of the 11th International ESV Conference,1987:280-301; Washington, DC.Cesari, D.; Ramet, M. Pelvic tolerance and protection criteria in side impact. In Proceedings of the 26thStapp Car Crash Conference. SAE 821159. Warrendale, PA: Society of Automotive Engineers; 1982:145-154.Cesari, D.; Ramet, M.; Bloch, J. Influence of arm position on thoracic injuries in side impact. In Proceedingsof the 25th Stapp Car Crash Conference. SAE 811007. Warrendale, PA: Society of Automotive Engineers;
1981:271-297.Cesari, D.; Ramet, M.; Clair, P. Y. Evaluation of pelvic fracture tolerance in side impact. In Proceedings ofthe 24th Staoo Car Crash Conference. SAE 801306. Warrendale, PA: Society of Automotive Engineers;1980:229-254:Cooper, G. J.; Maynard, R. L. An experimental investigation of the biokinetic principles governing non-penetrating impact to the chest and the influence of the rate of body deformation. In Proceedings of the1986 International Research Council on the Biokinetics of Impact Conference, 1986:331-342; Zurich,Switzerland.Danner, M.; Langwieder, K.; Schmelzing, W. Aspects in optimizing car structures and passenger protectionby a comprehensive analysis of car-to-car and car-to-object collisions. SAE 850514. Detroit, MI: Societyof Automotive Engineers; 1985.Eppinger, R. H.; Marcus, J. H.; Morgan, R. M. Development of dummy and injury index for NHTSAsthoracic side impact protection research program. SAE 840885. SAE Government/Industry Meeting andExposition, May 21-24, Washington, DC. Warrendale, PA: Society of Automotive Engineers; 1984.Foret-Bruno, J. Y.; Hartemann, F.; Tarriere, C.; Got, C.; Pate& A. Conditions required to avoid being killedin cars in side impact. SAE 830461. Warrendale, PA: Society of Automotive Engineers; 1983.Foster, J. K.; Kortge, J. 0.; Wolanin, M. J. Hybrid III-a biomechanically based crash test dummy. InProceedings of the 21st Stapp Car Crash Conference. SAE 770938. Warrendale, PA: Society of AutomotiveEngineers; 1977:973-1014.Hess, R.; Weber, K.; Melvin, J. Review of research on thoracic impact tolerance and injury criteria relatedto occupant protection. In: Viano, D. C., editor. Occupant Crash Interaction with the Steering Systems.SP-507. SAE 820480. SAE International Congress and Exposition, February, Detroit, MI. Warrendale,PA: Society of Automotive Engineers; 1982:93-119.Holbrook, T. L.; Graxier, K.; Kelsey, J. L.; Stauffer, R. N. The frequency of occurrence, impact and costof selected musculoskeletal conditions in the United States. Chicago, IL: American Academy of Ortho-paedic Surgeons; 1984.Horsch, J. D.; Lau, I. V.; Viano, D. C.; Andrzejak, D. V. Mechanism of abdominal injury by steering wheel
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
21/22
Biomechanics of the human chest, abdomen, and pelvis in lateral impact 573loading, In Proceedings of the 29th Stapp Car Crash Conference. SAE 851724. Warrendale, PA: Societyof Automotive Engineers; 1985:69-78.Horsch, J. D.; Viano, D. C. Influence of the surrogate in laboratory evaluation of energy-absorbing steeringsystem. In Proceedings of the 28th Stapp Car Crash Conference. SAE 841660. Warrendale, PA: Societyof Automotive Engineers; 1984:261-274.Jonsson, A.; Clemedson, C. J.; Sundquist, A. B.; Arvebo, E. Dynamic factors influencing the production oflung injury in rabbits subjected to blunt chest wall impact. J. Avia. Space Environ. Med. 50:325-337;1979.Kelsey, J. L.; Pastides, H.; Bisbee, G. E., Jr. Muscuioskeletal disorders: Their frequency of occurrence andtheir impact on the population of the United States. New York: Prodist; 1978.Kroell, C. K. Thoracic response to blunt frontal loading. In The human thorax anatomy, injury and biome-chanics. SAE Publication P-67. Warrendale, PA: Society of Automotive Engineers; 1976:49-78.Kroell, C. K.; Alien, S. D.; Warner, C. Y.; Perl, T. R. Interrelationship of velocity and chest compressionin blunt thoracic impact to swine II. In Proceedings of the 30th Stapp Car Crash Conference. SAE 861881.Warrendale, PA: Societv of Automotive Engineers; 1986:99-121.Kroell, C. K.; Pope, M. E.;Viano, D. C. Interrelationship of velocity and chest compression in blunt thoracicimoact. In Proceedines of the 25th Staoo Car Crash Conference. SAE 811016. Warrendale. PA: Societyof Automotive Enginiers; 19813549-582:Kroell, C. K.; Schneider, D. C.; Nahum, A. M. Impact tolerance and response of the human thorax. InProceedings of the 15th Stapp Car Crash Conference. SAE 710851. Warrendale, PA: Society of AutomotiveEngineers; 1971:84-134.Kroell, C. K.; Schneider, D. C.; Nahum, A. M. Impact tolerance and response of the human thorax II. InProceedings of the 18th Stapp Car Crash Conference. SAE 741187. Warrendale, PA: Society of AutomotiveEngineers; 1974:383-458.Lau, I. V.; Horsch, J. D.; Viano, D. C.; Andrzejak, D. V. Biomechanics of liver injury by steering wheelloading. J. Trauma. 27(3):225-235; 1987.Lau, I. V.; Viano, D. C. The viscous criterion: Bases and applications of an injury severity index for softtissues. In Proceedings of the 30th Stapp Car Crash Conference. SAE 861882. Warrendale, PA: Societyof Automotive Engineers; 1986:123-142.Lau, I. V.; Viano, D. C. How and when blunt injury occurs: Implications to frontal and side impact protection.In Proceedings of the 32nd Stapp Car Crash Conference. SAE 881714. Warrendale, PA: Society of Au-tomotive Engineers; 1988:81-100.Malliaris, A. C.; Hitchcock, R.; Hedlund, J. A search for priorities in crash protection. In Crash protection.SP-513. SAE 820242. SAE International Congress and Exposition. Warrendale, PA: Society of AutomotiveEngineers; 1982: -34.Melvin, J. W.; King, A. I.; Alem, N. M. AATD system technical characteristics, design concepts, and traumaassessment criteria. Contract No. DTNH22-83X07005, Task E-F, Final Report. Ann Arbor, MI: TheUniversity of Michigan, Department of Mechanical Engineering and Applied Mechanics; September 1985.Mertz. H. J. Anthrooomorohic models. In: Nahum. A. M.: Melvin. J. W.. editors. The biomechanics oftrauma. Norwalk,CT: Appleton-Century-Crofts; 1985:31-61.Mills, P. J.; Hobbs, C. A. The probability ofinjury to car occupants in frontal and side impacts. In Proceedingsof the 28th Stapp Car Crash Conference. SAE 841652. Warrendale, PA: Society of Automotive Engineers;1984:223-236.Morgan, R. M.; Marcus, J. H.; Eppinger, R. H. Side impact-the biofidelity of NHTSAs proposed ATDand efficacv of TTI. In Proceedines of the 30th Stanp Car Crash Conference, SAE 861877. Warrendale,PA: Society of Automotive Engineers; 1986:27-40. - -Nahum, A. M.; Gadd, C. W.; Schneider, D. C.; Kroeil, C. K. Deflection of the human thorax under sternalimpact. In Proceedings of the SAE International Automobile Safety Conference. SAE 700400. Warrendale,PA: Society of Automotive Engineers; 1970:797-807.National Highway Traffic Safety Administration, U.S. Department of Transportation. Melvin, J. W.; Weber,K., editors. In: Review of biomechanical impact response and injury in the automotive environment. DOTHS 807-042. Washington, DC; 1986.National Highway Traffic Safety Administration, U.S. Department of Transportation. Fatal Accident Re-porting System 1986. DOT HS-807-245. Washington, DC; March, 1988.National Research Council. Injury in America: A continuing public health problem. Washington, DC: Com-mittee on Trauma Research, Commission on Life Sciences, National Academy Press; 1985.Neathery, R. F. Analysis of chest impact response data and scaled performance recommendations. In Pro-ceedings of the 18th Stapp Car Crash Conference. SAE 741188. Warrendale, PA: Society of AutomotiveEngineers: 1974:459-494.Otte, D.; Suren, E. G.; Appel, H.; Nehmzow, J. Vehicle parts causing injuries to front-seat car passengersin lateral impacts. In Proceedings of the 28th Stapp Car Crash Conference. SAE 841651. Warrendale, PA:Societv of Automotive Engineers; 1984:13-24.
Partyka, S. C.; Rezabek, S. ETOccupant injury patterns in side impacts-a coordinated industry/governmentaccident data analysis. SAE 830459. SAE International Congress and Exposition, February 28-March 4,Detroit, MI. Warrendale, PA: Society of Automotive Engineers; 1983.Rouhana, S. W.; Foster, M. E. Lateral impact-an analysis of the statistics in the NCSS. In Proceedings ofthe 29th Stapp Car Crash Conference P-167. SAE 851727. Warrendale, PA: Society of Automotive En-gineers; 1985:79-78.Rouhana, S. W.; Lau, I. V.; Ridelia, S. A. Influence of velocity and forced compression on the severity ofabdominal injury in blunt, nonpenetrating lateral impact. J. Trauma. 25:490-500; 1984.Rouhana, S. W.; Ridella, S. A.; Viano, D. C. The effects of limiting impact force on abdominal injury: Apreliminary study. In Proceedings of the 30th Stapp Car Crash Conference. SAE 861879. Warrendale, PA:Society of Automotive Engineers; 1986:65-80.Sacreste, J.; Brun-Cassan, F.; Fayon, A.; Tarrier, C.; Got, C.; Patel, A. Proposal for a thorax tolerance levelin side impact based on 62 tests performed with cadavers having known bone condition. In ProceedingsLAP 21:6-E
-
7/28/2019 13-Viano D. C. 1989-Biomechanics of the human chest, abdomen, and pelvis in lat.pdf
22/22
574 D. C. VIANO t al.of the 26th Stapp Car Crash Conference. SAE 821157. Warrendale, PA: Society of Automotive Engineers;1982:155-172.Society of Automotive Engineers, SAE handbook on-highway vehicles and off-highway machinery. Instru-mentation for impact tests-SAE 5211, Jun80. Warrendale, PA: Society of Automotive Engineers; 34:156-158; 1987.Tarriere, C.; Brun-Cassan, F.; Thomas, C. Specific highlights relative to injury parameters in side impactsincludine unanimo~ oninions of IS0 SC12 Workine Grouns 5 and C. ISOITC22iSC121GTG. No. 256.Internat~onaI Standards Organization, Geneva; 1988: Thomas, C.; Henry, C.; Hartemann, F.; Patel, A.; Got, C. Injury pattern and parameters to assess severityfor occupants involved in car-to-car lateral impacts. In Proceedings of the 11th International TechnicalConference on Experimental Safety Vehicles, 1987:49-61; Washington, DC.TN0 Road-Vehicle Research Institute. EUROSID Information Bulletin 2 Reference Number 87.LP 1049/TS/EVB. Renort Number 7005640-02-B; Delft. Holland: March 1987.Viano, D. C. Thbracic iniury potential. In Proceedings of the 1978 International Meeting on the Simulationand Reconstruction ofmpacts n Collisions, 1978:142-156; IRCOBI Secretariat, Lyon, France.Viano. D. C. Evaluation of the SID dummv and IT1 iniurv criterion for side imnact test&r. In Proceedingsof the 31st Stapp Car Crash ConferenceSAE 872208: Warrendale, PA: Socieiy of Automotive Engineers;1987a: 143-160.Viano, D. C. Evaluation of the benefit of energy-absorbing material for side impact protection: Part I. InProceedings of the 31st Stapp Car Crash Conference. SAE 872212. Warrendale, PA: Society of AutomotiveEngineers; 1987b:185-204.Viano, D. C. Evaluation of the benefit of energy-absorbing material for side impact protection: Part II. InProceedings of the 31st Stapp Car Crash Conference. SAE 872213. Warrendale, PA: Society of AutomotiveEngineers; 1987c:205-224.Viano, D. C. Cause and control of automotive t.auma. Bull. N.Y. Acad. Med., Second Series. 64(5):376-421; 1988.Viano, D. C. Biomechanical response and injuries in blurt lateral impact. In Proceedings of the 33rd StappCar Crash Conference. SAE 89. Warrendale, PA: Society of Automotive Engineers; 1989.Viano, D. C.; Culver, C. C.; Evans, L.; Frick, M.; Scott, R. Involvement of older drivers in multive~cleside impact crashes. To be presented at the 33rd Annual Meeting of the Association for the Advancementof Automotive Medicine, &ober 1989; forthcoming.Viano, D. C.; King, A. I.; Melvin, J. W.; Weber, K. Injury biomechanics research: An essential element inthe prevention of trauma. J. Biomech. 22(5):403-417; 1989a.Viano, D. C.; Kroell, C. K.; Warner, C. Y. Comparative thoracic impact responses of living and sacrificedoorcine siblinas. In Proceedines of the 21st Staoo Car Crash Conference. SAE 770930. Warrendale. PA:Society of Au;omotive Engine