1247-1442-1-PB
6
UTMJ • Volume 87, Number 3, May 2010 155 Introduction G lioblastoma multiforme (GBM) is the most common and aggressive adult brain malignancy, with an annual inci- dence of 3 cases per 100,000 people in the United States. 1 Current treatments for GBM, including surgery, radio- therapy, and chemotherapy, are considered palliative 2 and the median survival time of one year has remained the same for the last 30 years. 1 GBM tumours are composed of heterogeneous mixtures of poorly differentiated astrocytes and are identified by distinct morphological features, including pseudopalisades (dense arrays of tumour cells around necrotic areas) and exten- sive neovascularity. 3 The “cell of origin” for GBM remains elusive, although the traditional theory posits that, like many other can- cers, GBM arises from clonal expansion of a mature cell that has undergone malignant transformation. 4,5 As the postnatal brain was believed to be quiescent, the oncogenic target was thought to be an astrocyte that de-differentiated to gain proliferative func- tion. 5,6 However, recent studies have suggested that a stem cell or progenitor population, rather than a differentiated astrocyte, may be the cell of origin. 5,7,8 Tumour initiating, stem-like cells have already been isolated in a number of malignancies, which has lead to the cancer stem cell (CSC) theory (Figure 1). 2,4,6,9-17 With the recent discovery of stem cells in the human brain, it has been proposed that neural stem cells (NSCs) may act as a depot of tissue-specific stem cells in the brain that are transformed into CSCs. 2,6,8-13,18,19 The aim of this paper is to critically evaluate the evidence for the NSC→CSC transformation hypothesis for GBM. Figure 1. The cancer stem cell (CSC) model. The traditional model (left) assumes that a cancer “cell of origin” underwent malignant transformation and expansion to generate clones with equal abilities of dividing and form- ing new tumours. In this model, subpopulations enriched for tumour-initiat- ing activit y cannot be consist ently isola ted. According to the cancer stem cell hypothesis (right), most cells in a tumour have limited proliferative potential. Only a small percentage of isolatable tumour cells, with stem- cell properties of self renewal and multipotency , “seed” the tumour . Adapted from: Dirks PB. Cancer: stem cells and brain tumours. Nature 2006;444:687-688, with permission. Neural Stem Cells (NSCs) NSCs are a small percentage (>0.1) of adult brain cells that are highly undifferentiated and have the ability to generate all neural cell types (Figure 2A). 6,8,20 In the adult brain, NSCs exist in vascular niches within the dentate gyrus of the hippocampus, sub-ventricular zone (SVZ) of the forebrain’s lateral ventricles, and olfactory bulb. 6,8,20 NSCs are characterized by their ability to maintain their numbers in the brain at a steady level throughout life. 6,8,20 This self-renewal ability can be shown in vitro . In serum- free culture systems supplemented with epidermal growth factor (EGF) and basic fibroblast growth factor (bFGF), most differen- tiating/differentiated neural cells rapidly die. On the other hand, NSCs proliferate to form floating aggregates or “neurospheres” (Figure 2, inset) that can be dissociated and re-plated to Review Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells? Samira B. Jeimy, PhD (1T2), Faculty of Medicine, University of Toronto Abstract Glioblastoma, the most common and aggressive adult brain malignancy, is characterized by the presence of morphologically diverse neural cell types that differ in their ability to form and maintain tumours. The marked resistance of this cancer to conventional treat- ments has sparked attempts to identify therapeutically targetable cellular populations. Defined pools of tumour-initiating cells have already been identified in other malignancies, e.g., leukemia. Like normal stem cells, these “cancer stem cells” (CSCs) have extensive self renewal capacity and multipotency; however, the origin of the CSC remains elusive. Recently, a small percentage of quiescent, undifferentiated, multipotent cells, termed neural stem cells (NSCs), were found in the hippocampus, sub‐ ventricular zone (SVZ), and olfactory bulb of the adult human brain. Since their discovery, it has been hypothesized that NSCs may act as a depot of tissue‐specific stem cells in the brain that may be transformed into CSCs. The purpose of this article is to critically review the literature that demon- strates that oncogenic mutations in NSCs allow these cells to become CSCs in glioblastomas. Insights into the mechanism of CSC formation in the brain may allow for the optimization of current therapeutic approaches as pathways in NSC→CSC formation will provide opportunities to specifically target this notori- ously treatment ‐resistant malignancy .
-
Upload
diana-munoz -
Category
Documents
-
view
213 -
download
0
Transcript of 1247-1442-1-PB

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 1/6

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 2/6
UTMJ • Volume 87, Number 3, May 2010156
generate secondary spheres.20-22 The presence of NSCs in theneurospheres is confirmed by their simultaneous expression of neural (Figure 2, B and C) and stem-cell specific markers by immunohistochemistry.20-22 The multipotency of NSCs can alsobe tested in culture; when plated on adhesive substrates without
the mitogens EGF and bFGF, NSCs differentiate into neurons,astrocytes and oligodendrocytes.2,20-22
Figure 2. Neural stem cells (NSC) and their characterization in culture
systems. NSCs undergo highly regulated, self-renewing divisions to
regenerate themselves (Panel A). They are multipotent and generate line-
age-committed progenitor cells that can then differentiate into the three
main neural cell types: neurons, astrocytes and oligodendrocytes. NSCs
derived from healthy adult brains can be grown in culture to give rise to
floating aggregates or neurospheres (inset). NSCs in the spheres can bedouble immunolabeled with antibodies against astrocyte markers (glial fib-
rillary acidic protein (GFAP), blue, Panel B) and neuronal markers (b-III
tubulin, green, Panel C). Adapted from: Singh SK, Clarke ID, Hide T, Dirks
PB. Cancer stem cells in nervous system tumors. Oncogene 2004;23:7267-
727; and Ignatova TN, Kukekov VG, Laywell ED et al. Human cortical glial
tumors contain neural stem-like cells expressing astroglial and neuronal
markers in vitro. Glia 2002;39:193-206, with permission.
Stem-like Cells can be Isolated from GBM Tumours
To give credibility to the NSC→CSC theory, it was important to show that GBM tumour specimens contained populations
with stem-cell like properties. To this end, several groups showedthat a small fraction of cells from dissociated GBM tumourscould proliferate in suspension as neurospheres that were mor-
phologically indistinguishable from normal NSC derived neu-rospheres.22-28 These cell aggregates could be dissociated repeat-edly at the level of a single cell to give rise to new neurospheres(subspheres),22,23,25-28 establishing their self-renewal ability.Unlike normal NSCs, tumour-derived cells were alive longer,23
with enhanced abilities to give rise to new subspheres.25 Further, when differentiated cells were switched to proliferating condi-tions, only GBM derived cells gave rise to new neurospheres,demonstrating their efficiency in maintaining the CSC pool.25
Immunohistochemistry was used to compare molecular markersexpressed by clonal neurospheres grown under proliferation anddifferentiation conditions. Undifferentiated tumour derived
neurospheres could be stained for the NSC markers Nestin andMusashi-2 (Figure 3, A and B).14,22-28 Salmaggi et al. used ELISAs toshow that GBM neurospheres secreted vascular endothelial growthfactor (VEGF),28 which is implicated in endothelial cell migrationand may be important for tumour angiogenesis.2,29 Like NSCs,
clonally derived GBM cells underwent differentiation on mitogenremoval.22-28 The majority of clones from each tumour gave rise tocells resembling both neurons (expressing b-III-tubulin) and glia(expressing glial fibrillary acidic protein, or GFAP) (Figure 3C).22-
28 The NSC, neural, and astrocytic markers could also be seen inthe original tumour tissue (Figure 3, D and E).22-28 Interestingly,only tumour derived cells gave rise to neurospheres with abnor-mal, dual phenotype cells expressing b-III-tubulin and GFAP(Figure 3C).22-25 The percentage of differentiated cell types gener-ated varied considerably from one tumour to another,15,23 whichmay be related to the heterogeneity of GBM tumours seen in vivo .
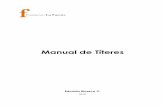
Figure 3. Cultured tumour-derived neurospheres are multipotent, andretain immuno-histochemical properties of original tumour samples.Adapted from: Hemmati HD, Nakano I, Lazareff JA et al. Cancerous stemcells can arise from pediatric brain tumors. PNAS 2003;100:15178-15183,
with permission.
Review
Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells?
A B
CTumour Derived Neurospheres:
Undifferentiated neurospheres from a representative tumour could be
immunostained for expression of the NSC markers Nestin (green, Panel A)
and Musashi (green, Panel B). Under differentiating culture conditions
(Panel C), neural and glial cells could be detected in the neurospheres, by
staining with anti b-III tubulin (Tuj1, red) and anti-GFAP (green) antibodies.
Some cells (indicated by arrows) simultaneously expressed both neural
and glial markers.
Original Tumours:
Paraffin-embedded sections of original tumours could also be labelled with
antibodies to Nestin (green, panel D), Tuj1 (red, Panel E) and GFAP (green,
Panel E). Counterstaining for nuclei with DAPI (blue, Panels B, D, and E) is
indicated.
Semi-quantitative RT-PCR was used to analyze expression of stem cell
markers in a representative tumour and tumour derived neurospheres
(NS). Like control (normal brain) tissue, GBM tumours expressed the stem
cell marker CD133. However, tumour NS over expressed genes involved in
NSC proliferation, i.e. BMI-1 and SOX2 (-, no/minor signal; +, weak signal;
++, moderate signal; +++, strong signal).
A B C
D E C

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 3/6
Figure 4. Tumour forming ability of intracranially injected neurosphere
and non-neurosphere forming cells. Adapted from: Yuan X, Curtin J,
Xiong Y et al. Isolation of cancer stem cells from adult glioblastoma mul-
tiforme. Oncogene 2004;23:9392-9400, with permission.
CD133+ CSCs May Comprise the Tumour-Initiating Cells
As the above assays represent retrospective analyses of CSCphenotype and function, a few groups also prospectively isolatedCSCs to confirm their presence in tumour specimens.
Dissociated brain tumour cells were fractionated into CD133+and CD133- populations by fluorescence activated cell sorting(FACS); in culture, only the CD133+ cells proliferated togenerate self-renewing neurospheres that, when differentiated,recapitulated the phenotype of the parental tumour.27,30-32
CD133, a cell surface protein that was originally described as ahaematopoietic stem cell marker,9,14,17 may also be useful to iden-tify brain CSCs, as these studies have shown. The numbers of CD133+ cells derived from different brain cancer samplesshowed correlation with the aggressiveness of the originaltumour.17,31,32 For example, neurospheres derived from low-grade gliomas contained ≤5% CD133+ cells, whereas up to 30%of the cells in GBM derived spheres expressed the marker.32
When affinity purified with an antibody against CD133, as few as
100 CD133+ cells from the tumour neurospheres initiatedserially transplantable tumours in NOD/SCID mice (Figure 5A),
whereas up to 100,000 injected CD133- cells failed to inducetumour formation.30-32 Further, transplantations of constant amounts of tumour cells with increasing percentages of CD133+cells increased the growth and vascularization of resultant tumours (Figure 5B).31
UTMJ • Volume 87, Number 3, May 2010 157
GBM Neurosphere Derived Cells Aberrantly Express
NSC-specific Genes
RT-PCR based genetic profiling studies showed that GBMtumour specimens had normal expression of the stem cellmarker CD133 , but overexpressed genes required for NSC pro-
liferation, including SOX2 (Figure 3F).16,25,26 Interestingly, someCD133 expression was detected in undifferentiated tumour-derived, but not control neurospheres. This suggests that theculture conditions may have selected for and allowed expansionof stem-like cells in the tumour samples. Tumour-derivedneurospheres also overexpressed the NSC genes BMI-1 and SOX2 .Overexpression of BMI-1 was previously shown to modulate theSonic Hedgehog growth signalling pathway, by transcriptionalrepression of the tumour suppressors INK4A and ARF.2,6,14
Accordingly, deletions of the INK4A and ARF loci induced GBMin the NSC containing regions of murine brains.8 The functionof the transcription factor SOX2 is not clear, although it isbelieved to be crucial to NSC maintenance, based on impairedneurogenesis and neurological defects in SOX2 knockout mice.6
The molecular signatures of undifferentiated GBM-derived cellsmirrored those of the parental tumours (Figure 3F), and wereunique from patient to patient,26 which suggests that geneexpression profiles specific to a given tumour could help developindividualized therapies for GBM patients.
GBM Neurosphere Derived Cells Can Initiate Tumours
in Immunocompromised Mice
To validate the hypothesis that CSCs were indeed isolatedfrom the GBM specimens, several groups demonstrated that these cells had tumourigenic potential. Neurospheres derivedfrom pediatric GBM tumours were shown to be able to engraft,migrate, proliferate, and differentiate in neonatal rat brains.11
This finding was expanded in non-obese, diabetic, severe com-bined immunodeficient (NOD/SCID) mice; transplanted GBM
neurospheres reproducibly gave rise to heterogeneous, GBM-like tumours,25,26,28 whereas normal human NSCs,28 commercial-ly available GBM cell lines,26 and non-neurosphere formingcells25 did not (Figure 4, A-I). The success of engraftment wasgreater when neurosphere-derived cells were injected ortho-topically (as opposed to subcutaneously),26 which emphasizesthe importance of the right microenvironment to support tumour growth. Two groups also demonstrated the tumouri-genic potential of the GBM-neuropsheres in serial transplanta-tion assays.25,26 Cells isolated from tumours in primary recipients
were re-cultured to give rise to new neurospheres that retainedmultipotentiality, could be identified by human specificmarkers, and resembled their parental line in gene expressionprofile.25,26 When transplanted into secondary recipients, these
cells could recapitulate tumour formation.25,26
Review
Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells?
Cells isolated from GBM neurospheres were able to form GBM-like tumours
(Panels A, B), but non-sphere forming cells did not (H&E stained in Panel C),
even when implanted at 50-fold excess of the GBM sphere cells.
Tumours developed in the mice brains could be stained by human-
specific antibodies against NSC markers Nestin (green, Panels D and E),
and CD133 (red, Panel G). Panel I is a merged version of Panels G and H.
Counterstaining for nuclei with DAPI (blue, Panels F, H) is also indicated.
A B C
D E F
G H I

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 4/6
UTMJ • Volume 87, Number 3, May 2010158
Review
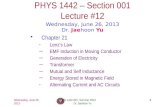
Figure 5. GBM derived CD133+ cells form tumours on intracranial trans-
plantation into NOD/SCID mice. Adapted from: Bao S, Wu Q, McLendon
RE et al. Glioma stem cells promote radioresistance by preferential acti-
vation of the DNA damage response. Nature 2006;444:756-760; and
Singh SK, Hawkins C, Clarke ID et al. Identification of human brain tumour-
initiating cells. Nature 2004;432:396-401, with permission.
CD133+ CSCs May Comprise the Treatment Resistant
Cell Population
It is tempting to propose that acquired mutations in any tumour cell that confer treatment resistance may lead to selectiveclonal expansion of that cell. However, the alternate hypothesisthat CD133+ CSCs may comprise the tumour-initiating, treatment-resistant subpopulation of cells in GBM has been supported by recent studies. Liu et al. exposed CD133+ and CD133- CSCs (FACSsorted from GBM cultures) to conventional chemotherapeuticagents, i.e., temozolomide, and showed that cell proliferation of the CD133+ cells was less sensitive to the drugs.27 The CD133+pool also overexpressed stem cell genes known to enhance drug-
resistance, i.e., the multi-drug resistance (MDR) gene BCRP-1,DNA-mismatch repair genes including MGMT, and apoptosis-inhibiting genes including BCL-2.27 These findings were corrobo-rated by FACS analyses showing significantly higher expression of MDR proteins by GBM tumour neurosphere cells compared tothose derived from control NSC neurospheres.28
The importance of characterizing the CD133+ CSC to developGBM treatment strategies was highlighted by a study that identified surface receptors for bone morphogenic proteins(BMPs), soluble factors that induce NSC→astrocyte differentia-tion, on CD133+ human GBM cells.33 In culture, the addition of exogenous BMP reduced the proliferation of GBM-derived
CD133+ cells, and led to reduced tumour size/malignancy whentreated cells were grafted into immunodeficient mice.33 In thisstudy, the small size of the secondary tumours precluded isola-tion of enough CD133+ cells for further characterization or seri-al transplantation studies.33 Nonetheless, the data implied that
GBM tumours contain hierarchically organized, stem-cell-basedpopulations.
The mechanism of radiation resistance of the CD133+ cells was recently evaluated by Bao et al., who isolated tumour cellsfrom human GBM specimens and murine xenograft tumours.31
On exposure to high dose radiation ex vivo , the percentage of CD133+ in cultured neurospheres increased. When serially transplanted, the irradiated CD133+ cells yielded more aggres-sive tumours.31 CD133+ cells from original and transplantedtumours showed enhanced activation of checkpoint proteins inresponse to radiation-induced DNA damage, repaired theirdamaged DNA damage more efficiently than CD133- cells, andshowed resistance to apoptosis.31 Further, their radiationresistance could be pharmacologically inhibited by blocking the
checkpoint kinases Chk1 and Chk2.
31
These studies may haveidentified potentially targetable vulnerabilities in CSCs. Forfuture studies, it should be interesting to evaluate whether thesupportive stroma of NSC niches contributes to the radiationresistance of CD133+ CSCs.
NSCs as Candidates for Oncogenic Mutations in GBM
Indirect evidence implicating NSCs, even before their disco- very, as the cells of origin in GBM came from animal studies where the exposure to oncogenic viruses or administration of carcinogens resulted in greater numbers of tumour formation inthe SVZ2,8,14 – a NSC niche. Further indirect support is providedby the long lifespan and self-renewal abilities of NSCs,6,8,20 whichincrease the possibility for these cells to acquire mutations.
Although astrocyte and oligodendrocyte generations have simi-
larly long lifespans, they are also quiescent in vivo ,20 makingthem unlikely targets for transforming mutations. Genetic pro-filing studies have shown that oncogenic mutations in GBM aremost frequent in genes that encode regulatory proteins involvedin growth factor signaling cascades (i.e., Sonic Hedgehog path-
way) or cell cycle control (i.e., Chk1 and Chk2) known to mod-ulate NSC proliferation.2,6,16,25,26 Further support for NSCs asGBM cells of origin was seen in a transgenic mouse model,
where genes encoding activated forms of Ras and Akt were trans-ferred to astrocytes and neural progenitors in a tissue-specificmanner.34 The combination of Ras and Akt induced GBM only after transducing neural progenitor cells, but not astrocytes.34
Although the disruption of regulatory mechanisms may indeed be involved NSC→CSC pathway, these correlational
findings may merely represent mechanistic similarities betweenNSC and CSC renewal. Several murine studies also suggest that,given the right combination of genetic aberrations that interrupt critical signalling pathways, mature neural cells can also causeGBM. Bachoo et al. retrovirally transfected a constitutively activeform of epidermal growth factor (EGF) receptor in either NSCsor astrocytes from Ink4a/Arf-/- mice.4,8,35 Both the mutated NSCsand astrocytes were capable of inducing high-grade gliomas
when they were transplanted in the brains of NOD/SCID mice.35
In another study, a human astrocyte cell line was retrovirally transfected with human telomerase reverse transcriptase, humanpapillomavirus 16 E6/E7 (to inactivate tumour suppressors
Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells?
Patient Xenograft
M A P 2
G F A P
M I B - 1
N e s t i n
H & E
Panel A: CD133+ cells
from a GBM patient
transplanted in a NOD/SCID
recipient resembled the
original patient tumour.
H&E stained sections of thexenograft showed
histological features of GBM.
Immunohistochemically,
both the xenograft and the
patient’s original tumour
showed expression of
Nestin, had high proliferative
indices (MIB-1/Ki67
staining), and expression of
both astrocytic (GFAP) and
neuronal (MAP2) markers.
Panel B: CD133+ expressing
cells from a human GBM
specimen were sorted by
FACS and mixed withCD133- cells in different
ratios, for injection into
mouse brains (100,000 total
cells per mouse). Gross
morphology of mouse
brains bearing
secondary tumours showed
correlation between the
percentage of CD133+ cells
injected, with tumour size
and vascularity.
A
B

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 5/6
UTMJ • Volume 87, Number 3, May 2010 159
p53 and Rb), and activated Ras/Akt.36 When intracranially trans-planted into immuno-compromised rats, the transformed astro-cytes were able to initiate GBM-like tumours.36
Study Limitations
A number of studies have shown that a stem-cell like popula-tion can be isolated from GBM tumour specimens, and that these cells can initiate GBM when transplanted into immuno-compromised mice. However, a number of questions still needto be addressed. It is unclear whether the tumour heterogeneity in GBM is caused by differentiation of CSCs or merely repre-sents the unstable gene expression pattern inherent in cancercells.12 This complexity is compounded by the fact that,although most studies showed cancer-initiation by CSC enrichedcell populations, CD133+ CSCs were not purified to homogene-ity from GBM samples, based partially on the lack of availablemarkers to identify these cells.27,30-32 Additionally, these cells havenot been shown to be conclusively of neural origin,27,30-32 likewise
with the relative lack of characterization of the newly identified
NSCs.It is difficult to accept findings from studies based largely oncell culture systems as a layer of cells in a culture dish is vastly dif-ferent than the dynamic environment of the human brain andmay lack key players involved in disease pathogenesis in vivo .The current studies extensively used neurosphere cultures toassess CSC presence in GBM tumour samples. Cell proliferationin this system is dependent on their responsiveness to EGF andbFGF,37 which may not represent the niche where GBM tumoursare growing in the brain. Depending on plating density, neu-rosphere formation was previously shown to result from sponta-neous cell aggregation of mature cells.37 The multipotency of neurosphere-forming cells was assessed by immunohistochemi-cal staining, without functionally confirming the identity of thedifferentiated cells.37 The formation of self-renewing neu-
rospheres that differentiated into multiple cell types thus repre-sent supportive, but not conclusive data on CSC isolation fromGBM tumours.
The use of immuno-compromised or transgenic mice tomodel human GBM adds some difficulty to data interpretation.This is due, firstly, to the well known differences between miceand humans, allowing limited extrapolation between species.Secondly, the tumourigenic potential of CSCs was shown by xenotransplantation in mice lacking an immune system, whosebrain microenvironments may differ significantly from thosesupporting CSC generation or tumour growth in healthy sub-
jects. Lastly, in studies that generated transgenic mice, often-times multiple proteins were mutated to manifest the full spec-trum of clinical abnormalities. It is currently unclear how close-
ly these genetic backgrounds resemble those actually found inhuman GBM.5 The use of non-human primates or other largeanimals for future studies may be helpful for characterizing theinvolvement of CSCs in GBM.
There is some evidence to suggest that NSCs may comprisethe CSC population in GBM, although conflicting data showedthat differentiated cells can also give rise to cancer, given theright combination of mutations.4,8,35,37 These findings suggest that, during tumour progression, CSCs could spontaneously arise at any time from a cell acquiring de-differentiating muta-tions. Further questions regarding NSCs as the CSC source inGBM are raised by the possibility that CSCs from other tissues
can migrate to and initiate cancer in the brain.38 For example,adult haematopoietic stem cells injected into the brain wereshown to home towards distant brain tumour sites,4,20 throughinteractions between CXCR4 on their surface and thechemokine SDF-1 (stromal cell derived factor 1).20 Interestingly,
circulating hematopoietic stem cells have been shown to fuse with various target cells, including cardiac myocytes and oligo-dendrocytes, producing hybrid cells with abnormal gene expres-sion patterns.4 In GBM, fusion between migratory hematopoiet-ic cells with normal neural cells could endow resultant hybrids
with CSC properties,4 including enhanced proliferation, infiltra-tion, and radiation/chemotherapy resistance.
Conclusion
A CSC population appears to play an important role in seed-ing and maintaining tumours in GBM. This was shown by theirprospective isolation from tumour specimens, demonstration of their self-renewing and multipotent properties, and recapitula-tion of heterogeneous tumours when CSCs were serially trans-
planted into NOD/SCID mice. The theory that GBM tumoursdepend on a small population of CSCs for their long-termgrowth and propagation provides an explanation for why con-
ventional therapies fail. Retrospective characterization of CSCsidentifed possible mechanisms for their treatment resistance,and identified potentially targetable genetic abnormalities inthese cells. However, given the available data, it is not clear
whether CSCs arise from NSCs, or mature neural cells that de-differentiated to unmask latent stem cell properties.
Alternatively, a migratory stem cell from another organ may act as or fuse with a normal brain cell to become a CSC. For clinicaltranslation, further characterization of CSCs is needed to iden-tify ways in which they differ from normal stem cells. Insight intothe molecular characteristics of CSCs, including the identifica-tion of cell-specific markers, analysis of their gene expression
profile, identification of the signalling pathways and microenvi-ronment required to support their growth and maintenance,could potentially result in effective drugs for this currently incur-able malignancy.
References1. Legler JM, Ries LA, Smith MA et al. Cancer surveillance series: brain and other cen-
tral nervous system cancers: recent trends in incidence and mortality. J Natl CancerInst. 1999;91:1382-1390.
2. Vescovi AL, Galli R, Reynolds BA. Brain tumour stem cells. Nat Rev Cancer.2006;6:425-436.
3. Rees JH, Smirniotopoulos JG, Jones RV, Wong K. Glioblastoma multiforme: radio-logic-pathologic correlation. Radiographics. 1996;16:1413-1438.
4. Bjerkvig R, Tysnes BB, Aboody KS, Najbauer J, Terzis AJ. Opinion: the origin of thecancer stem cell: current controversies and new insights. Nat Rev Cancer.2005;5:899-904.
5. Merlo A. Genes and pathways driving glioblastomas in humans and murine diseasemodels. Neurosurg Rev. 2003;26:145-158.
6. Nicolis SK. Cancer stem cells and "stemness" genes in neuro-oncology. NeurobiolDis. 2007;25:217-229.
7. Bansal K, Liang ML, Rutka JT. Molecular biology of human gliomas. TechnolCancer Res Treat. 2006;5:185-194.
8. Sanai N, varez-Buylla A, Berger MS. Neural stem cells and the origin of gliomas. NEngl J Med. 2005;353:811-822.
9. Wang JC, Dick JE. Cancer stem cells: lessons from leukemia. Trends Cell Biol.2005;15:494-501.
10. Kondo T. Brain cancer stem-like cells. Eur J Cancer. 2006;42:1237-1242.11. Dirks PB. Cancer: stem cells and brain tumours. Nature. 2006;444:687-688.12. Fomchenko EI, Holland EC. Stem cells and brain cancer. Exp Cell Res.
2005;306:323-329.13. Galderisi U, Cipollaro M, Giordano A. Stem cells and brain cancer. Cell Death
Differ. 2006;13:5-11.14. Pilkington GJ. Cancer stem cells in the mammalian central nervous system. Cell
Prolif. 2005;38:423-433.
Review
Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells?

8/8/2019 1247-1442-1-PB
http://slidepdf.com/reader/full/1247-1442-1-pb 6/6
UTMJ • Volume 87, Number 3, May 2010160
Review
15. Nakano I, Kornblum HI. Brain tumor stem cells. Pediatr Res. 2006;59:54R-58R.16. Soltysova A, Altanerova V, Altaner C. Cancer stem cells. Neoplasma. 2005;52:435-
440.17. Singh S, Dirks PB. Brain tumor stem cells: identification and concepts. Neurosurg
Clin N Am. 2007;18:31-8, viii.18. Dirks PB. Brain tumor stem cells. Biol Blood Marrow Transplant. 2005;11:12-13.19. Singh SK, Clarke ID, Hide T, Dirks PB. Cancer stem cells in nervous system tumors.
Oncogene. 2004;23:7267-7273.20. Ming GL, Song H. Adult neurogenesis in the mammalian central nervous system.
Ann Rev Neurosci. 2005;28:223-250.21. Taupin P. Neural progenitor and stem cells in the adult central nervous system. Ann
Acad Med Singapore. 2006;35:814-820.22. Ignatova TN, Kukekov VG, Laywell ED et al. Human cortical glial tumors contain
neural stem-like cells expressing astroglial and neuronal markers in vitro. Glia.2002;39:193-206.
23. Hemmati HD, Nakano I, Lazareff JA et al. Cancerous stem cells can arise from pedi-atric brain tumors. Proc Natl Acad Sci USA. 2003;100:15178-15183.
24. Steindler DA. Redefining cellular phenotypy based on embryonic, adult, and can-cer stem cell biology. Brain Pathol. 2006;16:169-180.
25. Yuan X, Curtin J, Xiong Y et al. Isolation of cancer stem cells from adult glioblas-toma multiforme. Oncogene. 2004;23:9392-9400.
26. Galli R, Binda E, Orfanelli U et al. Isolation and characterization of tumorigenic,stem-like neural precursors from human glioblastoma. Cancer Res. 2004;64:7011-7021.
27. Liu G, Yuan X, Zeng Z et al. Analysis of gene expression and chemoresistance of CD133+ cancer stem cells in glioblastoma. Mol Cancer. 2006;5:67.
28. Salmaggi A, Boiardi A, Gelati M et al. Glioblastoma-derived tumorospheres identify a population of tumor stem-like cells with angiogenic potential and enhanced mul-tidrug resistance phenotype. Glia. 2006;54:850-860.
29. Visted T, Enger PO, Lund-Johansen M, Bjerkvig R. Mechanisms of tumor cell inva-sion and angiogenesis in the central nervous system. Front Biosci. 2003;8:e289-e304.
30. Uchida N, Buck DW, He D et al. Direct isolation of human central nervous systemstem cells. Proc Natl Acad Sci USA. 2000;97:14720-14725.
31. Bao S, Wu Q, McLendon RE et al. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature. 2006;444:756-760.
32. Singh SK, Hawkins C, Clarke ID et al. Identification of human brain tumour initi-ating cells. Nature. 2004;432:396-401.
33. Piccirillo SG, Reynolds BA, Zanetti N et al. Bone morphogenetic proteins inhibit thetumorigenic potential of human brain tumour-initiating cells. Nature. 2006;444:761-765.
34. Holland EC, Celestino J, Dai C et al. Combined activation of Ras and Akt in neuralprogenitors induces glioblastoma formation in mice. Nat Genet. 2000;25:55-57.
35. Bachoo RM, Maher EA, Ligon KL et al. Epidermal growth factor receptor andInk4a/Arf: convergent mechanisms governing terminal differentiation and trans-formation along the neural stem cell to astrocyte axis. Cancer Cell. 2002;1:269-277.
36. Sonoda Y, Ozawa T, Hirose Y et al. Formation of intracranial tumors by genetically modified human astrocytes defines four pathways critical in the development of human anaplastic astrocytoma. Cancer Res. 2001;61:4956-4960.
37. Fan X, Salford LG, Widegren B. Glioma stem cells: Evidence and limitation. SeminCancer Biol. 2006.
38. Houghton J, Stoicov C, Nomura S et al. Gastric cancer originating from bone mar-row-derived cells. Science. 2004;306:1568-1571.
Does Glioblastoma arise from Oncogenic Transformation of Neural Stem Cells into Cancer Stem Cells?