1210 DIASTOLIC Hypertension[2]
![download 1210 DIASTOLIC Hypertension[2]](https://fdocuments.in/public/t1/desktop/images/details/download-thumbnail.png)
of 44
-
Upload
boysz-thebest -
Category
Documents
-
view
218 -
download
0
Transcript of 1210 DIASTOLIC Hypertension[2]
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
1/44
Hypertension
Dr Moynul Haque
GPST3
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
2/44
Overview
Background
NICE Guideline
AKT Question
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
3/44
Epidemiology 15-20% of the adult population (>half of those older than 60) are
hypertensive
Risk associated with increasing blood pressure is continuous
-with each 2 mmHg rise in systolic blood pressureassociated with a 7% increased risk of mortality from IHD and a10% from strokeDiastolic pressure is more commonly elevated in people youngerthan 50
With ageing, systolic hypertension becomes a more significantproblem, as a result of progressive stiffening and loss of
compliance of larger arteries
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
4/44
Aetiology
Essential / Primary 95%
Secondary (only 5%)
Renal 80%-GLomerulonephritis
-Pyelonephritis
-Adult PCKD-Renal artery stenosis
Endocrine causes 15%-Cushing's syndrome
-Conn's syndrome
-Liddle's syndrome
-Congenital adrenal hyperplasia
-Phaeochromocytoma
- Acromegaly
Others 5%-Pregnancy
-Coarctation of Aorta
-Steroid use
-COC pill
-MAOI
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
5/44
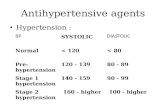
Definition of Hypertension
Stage 1: Clinic BP 140/90 or higher andABPM daytime / HBPM 135/85 or higher
Stage 2: Clinic BP 160/100 or higher andAMBP daytime / HBPM 150/95
Severe : Clinic SBP 180 or higher or Clinic DBP 110 or higher
Accelerated: Clinic BP 180/110 or higherwith Sign of papilloedema or Retinal haemorrhage
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
6/44
Clinic BP recording
Measure BP in both arms If difference >20 repeat the
measurements
If remains >20 on 2nd time
Measure BP again in the arm
with the higher reading
If clinic BP140/90
Take a second measurement If 2nd measure is different from
1st , take 3rd
Record the lower of the last 2
measurements as the clinic BP
http://eachthingonline.com/wp-content/uploads/2011/04/high-blood-pressure-remedy.jpg -
7/30/2019 1210 DIASTOLIC Hypertension[2]
7/44
Key points
If clinic BP 140/90 (180/110)ABPM/HBPM
If ABPM-At least 2 measurement / hour during waking
hours (eg 08:00 & 22:00)-Use avg value (at least 14 measurement)
If HBPM-2 consecutive BP taken at least 1 min apart & with
the person seated-Ideally twice daily , am & pm-Recording for 7 days ( at least 4 days)-Discard the measurement taken on the 1st day and
use the avg value of all remaining measurements
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
8/44
Management
Lifestyle interventions
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
9/44
20112011
1997
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
10/44
Lifestyle interventions
Diet
Exercise
Cut down of Alcohol consumption
Stop Smoking Low salt intake
Discourage excessive consumption of coffee & other
caffeine-rich products
Relaxation therapy can be advised ( PCT will not provideroutinely)
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
11/44
Initiating medication
If Stage 1(Clinic BP140/90 + ABPM135/85) +one of the following
-Target organ damage eg, LVH,
-Established CVD disease-Renal disease eg,albuminuria/proteinuria,haematuria
-Diabetes
-A 10 yrs CV risk equivalent to 20%If Stage 2 ( Clinic BP160/100 + ABPM150/95)
Severe hypertension (Clinic SBP180 or DBP110) Start antihypertensive medication immediately
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
12/44
Investigation
Urine dips for haematuria
Urine for ACR (Albumin: creatinine ratio)
-if DM ACR>2.5 in men and >3.5 in womenIf non-DM ACR> 30 significant proteinuria
Blood for U&Es, glucose, total cholesterol
and HDL cholesterol
Fundoscopy for hypertensive retinopathy
12 lead ECG
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
13/44
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
14/44
Drugs treatments
Key points
Offer drugs taken only once a day Do not combine ACE inhibitor with ARB If > 55yrs or Afro-Caribbean offer CCB If diuretics considered offer a thiazide-like
diuretics eg, Indapamide (1.5 mg MR od or 2.5 mgod) or Chlortalidone ( 12.5- 25.0 mg od) inpreference to conventional thiazide eg,Bendroflumathiazide or hrdrochlorthiazide ( if
already taken & well controlled then continue tx) In step 4 treatment Consider further diuretics with low dose of Spironolactone 25mg od if
K level 4.5
Consider further diuretic high dose of Thiazide like diuretics if K level4.5
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
15/44
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
16/44
Drug of choice
HTN + DM ACE/ARB
HTN + IHD B blocker
HTN + HF ACE/ARB HTN + CKD ACE/ARB
HTN + Pregnancy Methyledopa/ B blocker
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
17/44
MONITORING
When using further diuretics (eg, Spironolactone orhigher dose of Thiazide-like diuretics)
Monitor blood Na, K and U&Es within 1 month and repeat as required
If ACE inhibitor or ARB
Monitor U&Es before and after initiation and also afterincreasing the dose.
Rise in Creatinine up to 30% from base line
Reduce eGFR up to 20% from base line
Increase K level up to 5.5
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
18/44
Specialty referrals
If stage1 hypertension and 20) +
symptoms persist eg, fall, postural dizzy
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
19/44
Target BP
Under 80yrs Clinic BP140/90
Daytime avg ABPM/ HBPM 135/85
Over 80yrs-Clinic BP 150/90
-Daytime avg ABPM/ HBPM 145/85
Hypertension with diabetes Clinic BP 140/80
If target organ damage 130/80
9/6/11
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
20/44
MCQ
AKT
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
21/44
You review a 67-year-old woman who has a history of
chronic obstructive pulmonary disease and hypertension.
She has develop cor pulmonale and her current
medications include frusemide 80 mg bd, amlodipine 10mg
od and atenolol 50 mg od. You want to initiate an ACEinhibitor. What is the most appropriate action?
A. Stop frusemide for 2 days + start ramipril 1.25 mg od + checkU&Es in 2 weeks
B. Start ramipril 1.25 mg od + check U&Es in 2 weeks
C. Refer to secondary care
D. Reduce frusemide to 80mg od + start ramipril 1.25mg od + check U&Es in 2 weeks
E. Start ramipril 1.25 mg od + check U&Es in 5 days
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
22/44
C
Both the BNF and Clinical Knowledge
Summaries recommend referring people on
larger doses of diuretics to specialists for
initiation of ACE inhibitors.
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
23/44
You review an 81-year-old man with regards to his
hypertensive therapy. He is currently taking a
combination of losartan and amlodipine which is
failing to keep his blood pressure withing target.
What is the most appropriate next step assuming
he has no relevant contraindications?
A. Add indapamide MR 1.5mg odB. Add atenolol 50mg od
C. Add ramipril 1.25mg od
D. Add doxazosin 1mg od
E. Add bendroflumethiazide 2.5mg od
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
24/44
NICE now advise using alternatives to
bendroflumethiazide. Patients already taking
bendroflumethiazide should however not be
switched over to alternative thiazide-typediuretics.
A
This patient is taking an angiotensin 2
receptor blocker (losartan), possibly due to
having problems with ACE inhibitor therapy
previously, for example a dry cough. Patients
should not normally take an ACE inhibitor and
A2RB at the same time.
A 65 ld f l ith k hi t f h t
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
25/44
A 65 year old female with a known history of heart
failure presents to her GP for an annual check-up.
She is found to have a blood pressure of 170/100
mmHg. Her current medications are furosemide and
aspirin. What is the most appropriate medication toadd?
A. Bendroflumethiazid
B. SpironolactonC. Bisoprolol
D. Verapamil
E. Enalapril
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
26/44
E
Both enalapril and spironolactone have been
shown to improve prognosis in patients with
heart failure.
NICE guidelines recommend the introductionof an ACE inhibitor prior to a beta-blocker in
patients with chronic heart failure
A 71-year-old woman is reviewed in her local GP surgery She has
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
27/44
A 71-year-old woman is reviewed in her local GP surgery. She has
recently changed practices and is having a routine new patient
medical. Her blood pressure is 146/ 94 mmHg. This is confirmed on a
second reading. In line with recent NICE guidance, what is the most
appropriate management?
A. Ask her to come back in 6 months for a blood pressurecheck
B. Arrange 3 blood pressure checks with the practicenurse over the next 2 weeks with medical review following
C. Arrange ambulatory blood pressure monitoring
D. Reassure her this is acceptable for her age
E. Start treatment with a calcium channel blocker
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
28/44
C
Hypertension - NICE now recommend
ambulatory blood pressure monitoring toaid diagnosis
The 2011 NICE guidelines recognise that
in the past there was overtreatment of
'white coat' hypertension. The use of
ambulatory blood pressure monitoring
(ABPM) aims to reduce this.
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
29/44
A 52-year-old man is seen in the hypertension clinic. He was
diagnosed around three months ago and started on ramipril. This
has been titrated up to 10mg od but his blood pressure remains
around 156/92 mmHg. What is the most appopriate next step in
management?
A. Add bendroflumethiazide
B. Add bisoprolol
C. Switch ramipril to perindopril
D. Add amlodipine
E. Add losartan
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
30/44
D
Calcium channel blockers are nowpreferred to thiazides in the treatment of
hypertension
The 2011 NICE guidelines reflected the
changing evidence base supporting theuse of calcium channel blockers in
preference to thiazide-type diuretics in
the management of hypertension.
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
31/44
You review a 60-year-old man in the hypertension clinic. His past
medical history includes depression and peripheral arterial disease. He
is currently prescribed aspirin, simvastatin, citalopram and co-codamol
8/500. Two weeks ago he was started on ramipril 1.25 mg od. His bloodpressure has decreased from 160/100 mmHg to 114/ 72 mmHg and the
creatinine has increased from 102 mol/l to 230 mol/l. Which one of
the following is most likely to explain the rise in creatinine?
A.Medication-induced urinary retention with
secondary obstructive nephropathyB. Concurrent paracetamol overdose
C. ACE-related nephropathy
D. Normal, acceptable rise in creatinine forpatients taking an ACE inhibitor
E. Underlying renovascular disease
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
32/44
You admit a woman who is 34 weeks pregnant to the obstetric ward.
She has been monitored for the past few weeks due to pregnancy-
induced hypertension but has now developed proteinuria. Her blood
pressure is 162/94 mmHg. Which one of the following
antihypertensives is she most likely to be commenced on?
A. Moxonidine
B. Atenolol
C. Methyldopa
D. Losartan
E. Verapamil
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
33/44
C
Consensus guidelines recommend treating bloodpressure > 160/110 mmHg although many clinicians have
a lower threshold
Oral methyldopa is often used first-line with oral labetalol,
nifedipine and hydralazine also being used
For severe hypertension IV labetalol and IV hydralazine
are used
Addition to the above
Delivery of the baby is the most important and definitive
management step. The timing depends on the individual
clinical scenario.
A 74 year old man presents to his GP for a medication
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
34/44
A 74-year-old man presents to his GP for a medication
review. Blood pressure is recorded as 184/72. This is
confirmed on two further occasions. What is the most
appropriate first line therapy?
A. Ramipril
B. Losartan
C. BendroflumethiazideD. Amlodipine
E. Atenolol
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
35/44
DThe 2011 NICE guidelines
recommended treating isolated
systolic hypertension the same wayas standard hypertension. In this age
group calcium channel blockers
would be first-line.
The use of beta-blockers in treating hypertension has
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
36/44
The use of beta-blockers in treating hypertension has
declined sharply in the past five years. Which one of the
following best describes the reasons why this has
occurred?
A. Less likely to prevent stroke + potential impairment ofglucose tolerance
B. Less likely to prevent myocardial infarctions + potentialimpairment of glucose tolerance
C. High rate of interactions with other commonlyprescribed medications (e.g. Calcium channel blockers)
D. Increased incidence of reported adverse effects
E. Increased incidence of chronic obstructive pulmonarydisease
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
37/44
AThis was demonstrated in the
Anglo-Scandinavian Cardiac
Outcomes Trial-BloodPressure Lowering Arm
(ASCOT-BPLA).
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
38/44
You review an 82-year-old woman in clinic. Last month she had
a one-off blood pressure reading of 150/92 mmHg and was
offered ambulatory blood pressure monitoring. This shows an
average reading of 146/94 mmHg. She has no significant pastmedical history of note other than hypothyroidism. What is the
most appropriate management?
A. Arrange further ambulatory blood pressure monitoring
B. Start a thiazide-type diureticC. Give lifestyle advice and repeat blood pressure in 6
months
D. Start an ACE inhibitor
E. Start a calcium channel blocker
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
39/44
C
NICE now only recommend
diagnosing people over the age of
80 years as hypertensive if they
have stage 2 hypertension (ABPM
daytime average or HBPM average
BP >= 150/95 mmHg).
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
40/44
Your next appointment is with a 47-year-old woman. She has come
for the results of her ambulatory blood pressure monitoring
(ABPM). This was arranged as a clinic reading one month ago was
noted to be 146/92 mmHg. The results of the ABPM show an
average reading of 126/78 mmHg. What is the most appropriatecourse of action?
A. Make the final decision based on a clinic blood pressurereading today
B. Offer repeat ABPM in 6 months time
C. Offer repeat ABPM in 12 months timeD. Reassure her that she does not need another blood pressure
check for 10 years
E. Offer to measure the patient's blood pressure at least every 5years
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
41/44
EIn this situation where the ABPM has
shown a sub-threshold average blood
pressure
NICE recommend offering to measure
the patient's blood pressure at least
every 5 years.
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
42/44
An 83-year-old woman is reviewed in the
hypertension clinic. What should her target blood
pressure be once on treatment?
A. 140/80 mmHg
B. 140/90 mmHg
C. 130/80 mmHgD. 140/85 mmHg
E. 150/90 mmHg
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
43/44
E
Blood pressure target (based
on clinic readings) forpatients > 80 years - 150/90
mmHg
-
7/30/2019 1210 DIASTOLIC Hypertension[2]
44/44
Many Thanks
?