110215_Managing-and-treating-chronic-kidney-disease.pdf

of 4
-
Upload
kelompok14rssa -
Category
Documents
-
view
216 -
download
0
Transcript of 110215_Managing-and-treating-chronic-kidney-disease.pdf
-
8/16/2019 110215_Managing-and-treating-chronic-kidney-disease.pdf
1/4
16 Nursing Times 11.02.15 / Vol 111 No 7 / www.nursingtimes.net
Nursing PracticeReviewRenal
Keywords: Anaemia/Dialysis/eGFR/ Kidney disease/Renal failure
● This article has been double-blindpeer reviewed
Arterio-venous stula: this is formed formost patients requiring haemodialysis C a
t h e r
i n e
H o
l l i c k
Author Belinda Dring is nurse specialist atNottingham University Hospitals Trust; VickiHipkiss is renal nurse specialist at BradfordTeaching Hospitals Foundation Trust.Abstract Dring B, Hipkiss V (2015)Managing and treating chronic kidneydisease. Nursing Times; 111: 7, 16-19.Chronic kidney disease is a long-termcondition that commonly exists with otherconditions such as diabetes, hypertensionand heart failure. The majority of peoplewith CKD are managed in the communityby a GP and community nursing teamrather than a nephrologist. This articleprovides an overview of its stages,management and treatment.
T he 2010 health survey for Englandfound 6% of men and 7% of women had stage 3-5 chronickidney disease. It showed a large
variation by age: fewer than 1% of men and women aged 16–24 years had stage 3-5CKD, compared with 29% of men and 35%of women aged 75 years and over (Rothet al, 2011).
Patients with CKD have irreversiblekidney damage; as kidneys have severalfunctions, this can lead to multiple healthproblems. CKD has several causesincluding hereditary diseases such as poly-cystic kidney disease, structural deformi-ties, infection or long-term conditionssuch as diabetes and hypertension. Patientscan develop complications such as high blood pressure, poor nutritional health,low haemoglobin levels and heart disease.
Late management of people with CKDincreases morbidity, mortality and associ-ated healthcare costs. Early detection andtreatment can improve the outcome (RenalAssociation, 2013a).
5 keypoints
1 Chronic kidney
disease is anirreversible, long-term condition
2 CKD should bemonitored andtreated in the earlystages to optimiseoutcome and slowdeterioration
3 Dialysis andtransplants aretreatments, notcures, and are notsuitable for allpatients
4 Patientsrequire closemanagement ofdiet, uid andmedicines tocompensate forreduced kidneyfunction
5 Specialistguidelines areavailable to helpwith management
Kidney functionThe gut absorbs nutrients from the gastro-intestinal tract into the bloodstream. Waste from metabolism is deposited backin the bloodstream; the blood is ltered bythe kidneys and what is not required by the body (toxins and water), is ltered out inthe form of urine to be excreted.
If the kidneys are not working properly,toxins and water are retained in the body. When kidney function deteriorates, toxinlevels and water retention both increase,causing CKD symptoms (Box 1). Toxins and water retention can rise to dangerous levelsand, if not adequately treated, lead to death.
The most practical way of assessing thelevel of kidney function is to calculate theglomerular ltration rate. GFR is a meas-urement of how much waste uid the kid-neys lter from the blood per minute(mL/min); in normal kidney function, thisshould be >90mL/min. As it is difcult tomeasure the GFR directly, an estimatedGFR (eGFR) is calculated using a formulausing creatinine levels and taking intoaccount age, gender and ethnic group.
Classifying CKDIdentifying the CKD stage helps with careplanning. The National Institute forHealth and Care Excellence (2014) recom-mends classifying CKD using the albumin/creatinine ratio (ACR), which measures theamount of albumin in urine and takes intoaccount the level of creatinine in the blood.
EGFR and ACR are important becausethe lower the eGFR or the higher the ACR,the more likely are complications of CKD.These complications require monitoringand intervention depending on the CKDstage. NICE (2014) and the National KidneyFoundation (2002) have developed charts
In this article... The classications of chronic kidney disease
Treatment options available for different stages of CKD Complications that can occur as a result of CKD
Chronic kidney disease is irreversible, but management and treatment options areavailable to help patients self-manage the condition and maintain their quality of life
Managing and treatingchronic kidney disease
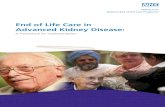
Bag containingdialysis solution
Fromdialysismachine
Vein
Artery
Fistula
Todialysismachine
-
8/16/2019 110215_Managing-and-treating-chronic-kidney-disease.pdf
2/4
www.nursingtimes.net / Vol 111 No 7 / Nursing Times 11.02.14 17
and tools to help with classication and,once the stage has been identied, guidanceon monitoring and intervention (Table 1).
Managing and treating CKDCaring for patients with CKD means man-aging treatments that carry out the kid-ney’s functions. Most patients can be man-aged by their GP but some may needinvestigations to nd the cause of CKD andany reversible factors. The Renal Associa-tion (2013b) provides clear guidelines on when to refer a patient to a nephrologist.
In the early stages of CKD, toxin and water control can be managed by dietaryrestrictions, which should be monitored by a renal dietitian. Depending on CKDseverity, dietary advice may include potas-sium, phosphate, calorie and uid intake.
As too much potassium in the bloodcan cause heart dysfunction, the rst die-tary change is usually to follow a low-potassium diet. This involves limiting theintake of fruit, potatoes, mushrooms andchocolate, as well as learning to cook cer-tain foods differently; for example, boiling vegetables before adding them to recipes.
Special diets should be provided by pro-fessionals to ensure patients are properlyassessed and that the education and man-agement provided is appropriate to them.
A low-protein diet should not be offeredas this can lead to malnourishment if sus-tained over a long period. Renal teams mustmonitor and manage kidney function toensure symptoms are kept to a minimum;once they are unmanageable using dietand medicines, renal replacement therapyof the patient’s choice should be started.
When patients have later-stage CKD(stages 4 and 5), they must be given robustinformation on treatment options. Thesecomprise dialysis, transplantation andconservative management. Not everyoption will be appropriate for every patient;suitability will be determined by thepatient’s physical and mental condition.
DialysisPatients at stage 5 CKD or those who havean eGFR below 10 are offered dialysis.There are two types of dialysis: peritonealdialysis; and haemodialysis.
Peritoneal dialysisThis uses the peritoneal membrane, whichlines the abdomen. A dialysis catheter isinserted into the membrane and a specialdialysis uid drained through the catheterinto the peritoneum. Toxins, waste prod-ucts and excess uid are pulled from themembrane’s blood supply into the uid byosmosis and diffusion (Fig 1). The uid
must be changed regularly; the frequencydepends on the type of PD carried out.
Continuous ambulatory peritoneal dial- ysis requires the patient to drain the uidout and replace it with more uid (do anexchange), which takes around 30 minutes,four times a day (roughly every six hours).The uid is drained into the peritoneumand left there for four to eight hours. Thepatient can carry out everyday activities,such as working and sleeping, during thistime but it may not suit some occupations.This form of dialysis gives patients control
of their treatment. The volume of uidinserted into the abdomen can lead to her-nias and infection (peritonitis) which, ifspotted quickly, can be treated effectively.
Automated PD requires the patient to be connected to a dialysis machine. Smallamounts of uid are put in and removedfrom the peritoneum as the patient sleepsso exchanges are not required during theday. This appeals to people who want tocontrol their treatment but have commit-ments that mean they cannot carry outfour exchanges a day.
Haemodialysis This type of dialysis removes toxins and waste products using a haemodialysismachine. The machine creates a continualcycle of blood being taken from thepatient, cleaned using an articial kidney(lter), then returned to the patient. It canalso remove excess uid. Most patientsattend a dialysis unit three times a weekand have a four-hour dialysis session; asmaller proportion dialyse more fre-quently and/or at home.
Access is needed to the blood supplyand, for most patients, this is by an arterio- venous stula. This is formed by joining
Most people do not have CKD symptomsuntil the later stages. These include:● Fatigue, lack of energy● Poor appetite● Nausea, vomiting, taste changes● Need to pass urine more often,especially at night● Swollen feet and/or ankles● Shortness of breath● Dry, itchy skin● Difficulty concentrating
BOX 1. CKD SYMPTOMS
TABLE 1. CHRONIC KIDNEY DISEASE CLASSIFICATION
GFR categories (mL/min/1.73m2),description and range
ACR categories (mg/mmol), descriptionand range
I n cr
e a s i n
g r i s k
30Severelyincreased
A1 A2 A3
≥ 90Normal and high
G1 No CKD in theabsence ofmarkers ofkidney damage
60-89Mild reduction related tonormal range for a youngadult
G2
45-59Mild–moderate reduction
G3a 1
30-44Moderate–severereduction
G3b
15-29Severe reduction
G4
-
8/16/2019 110215_Managing-and-treating-chronic-kidney-disease.pdf
3/4
18 Nursing Times 11.02.14 / Vol 111 No 7 / www.nursingtimes.net
an artery to a vein in the arm, whichrequires a small operation. The blood inthe artery goes directly into the vein
causing the vein to enlarge, therebymaking venous access easier. Fistula nee-dles can then be inserted into the stula atthe start of each dialysis session.
A smaller proportion of patients dialyseusing a:» Graft – this is similar to a stula but an
articial tube is used to connect theartery and vein;
» Permcath – a exible plastic catheterinserted into the internal jugular veinand tunnelled over the chest wall.
Transplantation
Kidney transplantation is not appropriatefor all patients who progress to stage 5,especially those with comorbidities.Patients can receive a transplant through:» Cadaver donation – from someone who
has died;» Living donation – from a living person
the patient knows (family/friend), ananonymous donor (altruistic), or aspart of a chain in which the relativedonates to another kidney patient andthe original patient receives a kidneyfrom the family of the other kidneypatient (paired exchange).
The type of transplant offered depends onthe transplant unit the patient attends,personal circumstances, organ availabilityand preferences.
Conservative managementSome patients, especially if they are veryold, very frail or have other medical prob-lems, may nd dialysis too much of a burden. In these cases, medications can betaken to control symptoms. These medica-tions do not replace dialysis or transplanta-tion and discussing end-of-life care is partof management. These patients are usuallymanaged in the community by a commu-nity team and/or a specialist renal nurse.
Anaemia in CKDAnaemia is a common complication of CKDand has many causes, the most common of which is reduced erythropoietin produc-tion. Erythropoietin, a hormone producedmainly by the kidneys, controls the produc-tion of red blood cells in the bone marrow.Reduced kidney function leads to less cir-culating erythropoietin so fewer red bloodcells are produced; this leads to anaemia.
Another factor contributing to renalanaemia is iron deciency. This can be:» Functional – iron stores exist but are
not available for the body to use;» Absolute – iron stores are so low the
bone marrow does not have enough tosupport red blood cell manufacture.Anaemia in CKD can occur as early as at
stage 3. In general, the lower the level ofkidney function, the greater the severity ofthe anaemia. There are many guidelines tohelp practitioners treat renal anaemia,including NICE’s (2011) guidance. Thisadvises that anaemia be considered, inves-tigated and managed in people with CKD if:» Haemoglobin levels fall to 11g/dL or
less (or 10.5g/dL or less if under two years old);
» They develop symptoms attributable toanaemia (such as tiredness, shortnessof breath, lethargy and palpitations).Measuring the eGFR is an important
part of investigations – if it is >60mL/min,anaemia is unlikely to be due to CKD andother causes should be investigated.
TreatmentThe rst-line treatment of anaemia in CKDis correction of any iron deciency. Ironsupplements can be administered:» Orally – sometimes tried in patients not
receiving dialysis, but treatment may beineffective or cause side-effects includingnausea, constipation, diarrhoea andgastrointestinal discomfort;
» Intramuscularly – rarely used in CKD asit often requires painful injections;
» Intravenously – commonly used,especially in patients receiving dialysis,and can be administered as a bolusinjection, an infusion or directly intothe lines of a haemodialysis machine.Blood transfusions are avoided because
of potential complications and as alterna-tive therapies are available. This is espe-cially the case for potential transplantrecipients as blood transfusion canincrease the percentage of cytotoxic anti- bodies, which can cause rejection of adonor organ. This makes it difcult to nda cross-match negative donor and maymean a longer wait for a transplant.
Erythropoiesis stimulating agent (ESA)– a genetically engineered copy of erythro-poietin – should be considered if the
patient remains anaemic once the irondeciency has been corrected. Oncepatients start treatment for anaemia, it isusually indenite (unless they receive akidney transplant), so frequent moni-toring of haemoglobin and iron levels arerequired. It can be harmful to correctanaemia to a normal range when patientsare treated with ESA because of anincreased risk of stroke, hypertension and vascular access (stula) thrombosis; NICE(2011) recommends treating to keep thehaemoglobin at 100-120g/L.
Blood pressureControlling blood pressure can slow theprogression of CKD in some people. Unfor-tunately, hypertension is a complication ofCKD so its management can become dif-cult. Recommendations suggest people with CKD should aim to keep their systolic blood pressure
-
8/16/2019 110215_Managing-and-treating-chronic-kidney-disease.pdf
4/4
www.nursingtimes.net / Vol 111 No 7 / Nursing Times 11.02.14 19
blood rise. This leads to lower levels of cal-cium in the blood and higher PTH levels,and the loss of calcium from the bones.
Healthy kidneys convert vitamin D intoan active form called calcitriol. This helpsthe body absorb dietary calcium and phos-phorus into the blood and bones. Calcitrioland PTH work together to keep calcium balance normal and bones healthy. Askidney function decreases, less vitamin Dis converted to calcitriol and less calciumis absorbed; as a result, PTH levelsincrease, removing calcium from the bones. The combination of decreased cal-cium absorption from food and PTHdrawing calcium from the bones makesthe bones weak and brittle.
Another complication of CKD-MBD is vascular or soft tissue calcication. Thereason for this is not completely under-stood, but is thought to be due to high cal-cium and phosphate levels in the blood.Calcium is deposited outside the skeleton,in tissues such as the blood vessels, lungs,kidneys, heart and gastric mucosa. Thiscan cause problems with tissue or bloodsupply function, including tissue necrosis.
The underlying principle of treatmentfor CKD-MBD is to keep the levels of cal-cium and phosphate in the blood as close tonormal as possible to prevent the parathy-roid glands from becoming overactive. Thisis achieved through diet and medication.
DietReducing dietary intake of phosphate isone of the most important steps in pre- venting bone disease. A dietitian canadvise on foods that contain high levels ofphosphate, such as milk, cheese and nuts, which should be avoided.
MedicationIf diet alone is not enough to keep phos-phate levels normal, a phosphate bindercan be prescribed. This is taken withmeals; it binds with phosphate and passesthrough the gut, preventing absorption.
Various forms of vitamin D can be pre-scribed. These increase calcium absorp-tion from the diet and suppress the para-thyroid gland. Calcimimetic drugs “trick”the body into thinking calcium levels areraised, which causes PTH levels to decreaseand calcium levels to fall to normal.
Regulation of acid-base balanceAcids are produced primarily from themetabolism of ingested protein. To main-tain acid-base balance, acid productionmust balance with neutralisation orexcretion. The lungs and kidneys controlthis balance.
The lungs eliminate carbon dioxide.This is mildly acidic so exhaling decreasesthe blood’s acidity. The kidneys maintain
the body’s pH balance by excreting eitherhydrogen ions (acid) or bicarbonate ions(alkaline) from body uids. If the bicarbo-nate concentration is greater than normal,the kidneys excrete more bicarbonate ionsand the urine will become more alkaline. Ifthe hydrogen ion concentration is greaterthan normal, the kidneys will excrete morehydrogen ions and urine becomes moreacidic (White, 2005). Control is also main-tained by the kidneys reabsorbing bicarbo-nate, which can act as a buffer to take upthe excess hydrogen ions.
In CKD, acidosis is often seen when theGFR decreases to