11. Bethesda System II
36
CYT 2113 Cytology I Lesson 11 The Bethesda System II
-
Upload
carinajonglee -
Category
Documents
-
view
13 -
download
1
description
Notes
Transcript of 11. Bethesda System II
-
CYT 2113 Cytology I
Lesson 11
The Bethesda System II
-
Automated review
If the case is examined by an automated
device, indicate whether the scanning was
successful, the device and the manufacturers
name
-
Computer Assisted Interpretation
of Cervical Cytology
The type of instrumentation used should be
provided in the report
Data generated from screening devices that
are not intended for patient care, but may be are not intended for patient care, but may be
used for internal laboratory quality assurance,
should not be included in the report
Whether or not the specimen was successfully
processed by the device, regardless of the
result, should be reported
-
If the automated screening provides an
interpretation of the specimen that replaces
manual screening/review, then the result and
any adequacy data derived from the computer
assessment should be stated in the report assessment should be stated in the report
If there is no manual screening, i.e. automated
primary screening only, then, in general, no
name should appear on the report that can be
misconstrued as a person who examined the
slide
-
Results generated by the instrument must be
reviewed and verified by a laboratorian with
appropriate training and authorization
A record of who performed this data
verification should be maintained as an verification should be maintained as an
internal laboratory record
If a specimen is manually screened or
reviewed following automated screening, then
the results of both methods must be
compared and any discrepancy reconciled
-
Ancillary testing
Include the method (name and brief description)
used for reflex human papillomavirus (HPV) test
Results for reflex HPV test can be reported as:
A result only
As a result with a recommendation for clinical As a result with a recommendation for clinical
management
As a result plus the probability of an associated
dysplasia
As a definitive interpretation that reflects both
the cytomorphology and the HPV status
-
Interpretation/Result
Negative for intra-epithelial lesion or
malignancy
When there is no cellular evidence of
neoplasia, state this in the General neoplasia, state this in the General
Categorization previously mentioned and/or in
the Interpretation/Result section of the
report, indicate whether or not there are
organisms or other nonneoplastic findings
-
Organisms
Trichomonas vaginalis
Fungal organisms morphologically consistent
with Candida spp.
Shift in flora suggestive of bacterial vaginosis
Bacterial morphologically consistent with Bacterial morphologically consistent with
Actinomyces spp.
Cellular changes consistent with herpes
simplex virus
-
Individual squamous cells covered by a layer
of bacteria that obscures the cell membrane
(clue cells)
-
NILM: cellular changes consistent with Herpes
simplex virus. Nuclei showing ground-glass
appearance. Multinucleation and dense
eosinophilic intranuclear inclusions surrounded by a
halo are also seen
-
Other non-neoplastic findings
Reactive cellular changes associated with:
Inflammation (includes typical repair)
Radiation
Intrauterine contraceptive deviceIntrauterine contraceptive device
Glandular cells status post-hysterectomy
Atrophy
-
NILM: Reactive cellular changes associated with
radiation
Cells with enlarged nuclei, abundant vacuolated
polychromatic cytoplasm, mild nuclear
hyperchromasia without coarse chromatin,
prominent nucleoli
-
NILM: Atrophy
Parabasal cells with occasional pyknotic
degenerated cells. Globular collections of
basophilic amorphous material (blue blobs) present
-
Other
Endometrial cells after age 40, particlularly
out of phase or after menopause may be
associated with benign endometrium,
humoral alterations and less commonly,
endometrial/uterine abnormalitiesendometrial/uterine abnormalities
Clinical correlation is recommended
-
Endometrial Cells
-
Epithelial cell abnormalities
Squamous cell
Atypical squamous cells of undetermined
significance
Atypical squamous cells cannot exclude high-Atypical squamous cells cannot exclude high-
grade squamous intra-epithelial lesion
Low-grade squamous intra-epithelial lesion,
encompasses HPV/mild dysplasia/cervical
intra-epithelia neoplasia (CIN) 1
-
High-grade squamous intra-epithelia lesion,
encompasses moderate-to-severe dysplasia,
CIN 2, CIN 3/carcinoma in situ
Suspicious for invasive squamous-cell Suspicious for invasive squamous-cell
carcinoma
Squamous-cell carcinoma
-
Glandular cell
Atypical
Glandular cells
Endocervical cellsEndocervical cells
Endometrial cells
Atypical
Endocervical cells, favour neoplastic
Glandular cells, favour neoplastic
-
Endocervical adenocarcinoma in situ
Adenocarcinoma
Endocervical
EndometrialEndometrial
Extrauterine
Other malignant neoplasms
Includes sarcoma, malignant lymphoma and
others
-
Atypical Squamous Cells
-
ASC-H
Metaplastic cells with enlarged nuclei and
nuclear contour irregularities showing
variation in size, shape and ratio of nuclear
to cytoplasmic area
-
Epithelial Abnormalities: Squamous
-
LSIL
HPV nuclear and cytoplasmic changes (binucleation
and koilocytosis) are consistent with LSIL
-
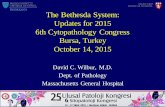
HSIL. Severely dysplastic cells on the left
display a high nuclear to cytoplasmic ratio and
irregular nuclear membranes. Moderately
dysplastic cells on the right have similar nuclei
and more cytoplasm.
-
HSIL.
Isolated abnormal cells with evenly distributed
coarse chromatin, centrally placed enlarged
nuclei, and dense / metaplastic cytoplasm
are consistent with HSIL
-
Epithelial Abnormalities: Glandular
-
Atypical endocervical cells
Sheet of cells with enlarged round or oval
nuclei. Cell borders are well-defined. Mitotic
figures are noted.
-
Other Malignant Neoplasms
Other malignant neoplasms: metastatic gastric
carcinoma
A clean background is a common finding
compatible in metastatic rather than primary
tumours of the cervix
-
Other malignant neoplasms: sarcoma
Single giant cells with malignant nuclear features is
present in a bloody background.
-
Educational Notes and Suggestions
Suggestions are optional
Should be carefully crafted, concise and
consistent with published clinical follow-up
guidelines
Examples where educational notes may be used: Examples where educational notes may be used:
Negative cytology reports to highlight the
limitations of cervical cytology
Alerting clinicians to references containing
consensus guidelines published by different
professional organizations
-
Examples where suggestions may be useful:
On unsatisfactory specimens: to improve the
quality of a repeat specimen
To identify patients with cytologic findings that
may require further triage and management
When morphologic findings are ambigous When morphologic findings are ambigous
In complex cases, if direct contact with provider is
not feasible, general statements such as suggest
follow-up as clinically indicated or further
patient follow-up procedures are suggested as
clinically indicated can be used