
11 acquired heart disease i
60
ACQUIRED HEART DISEASE I: THE CHEST RADIOGRAPH CARDIOVASCULAR SYSTEM DAVID SUTTON 11
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
9 -
download
0
Transcript of 11 acquired heart disease i

ACQUIRED HEART DISEASE I: THECHEST RADIOGRAPH
CARDIOVASCULAR SYSTEMDAVID SUTTON
11

DAVID SUTTON PICTURES
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

Fig. 11.1 The assessment of cardiac enlargement. The cardiac diameter should be the maximum cardiac diameter (r + I). The transverse thoracic diameter is measured in various ways; here it is measured as the maximum internal diameter of the thorax.
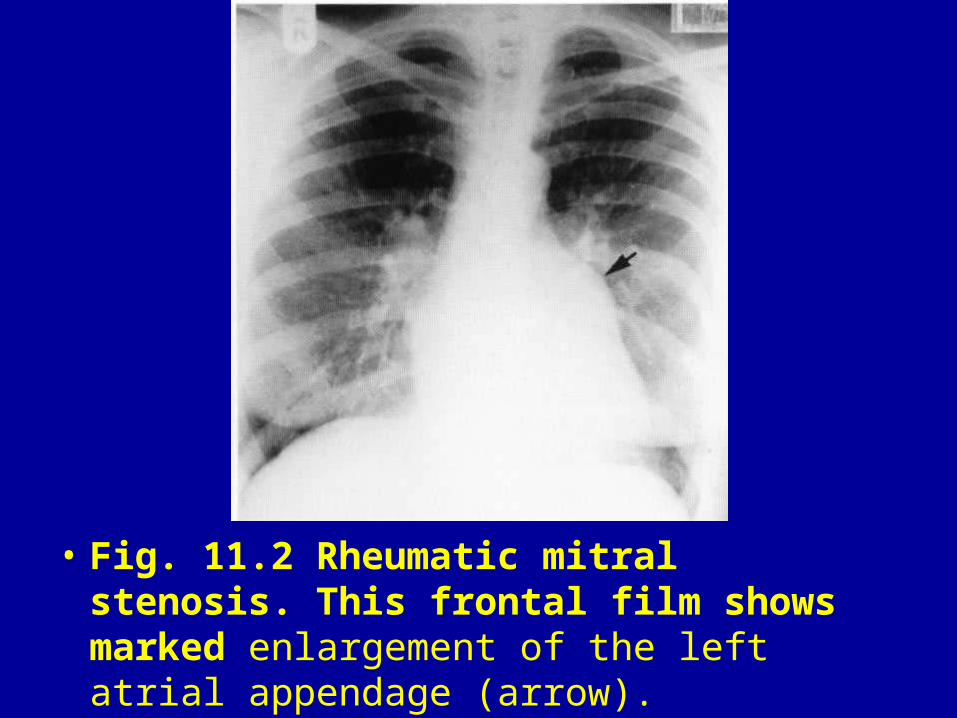
• Fig. 11.2 Rheumatic mitral stenosis. This frontal film shows marked enlargement of the left atrial appendage (arrow).

• Fig. 11.3 Left atrial enlargement. A PA (A) and penetrated chest film (B) in the same patient. The double right heart border and splaying of the carina, due to enlargement of this posterior chamber, is easily visualised on the penetrated film.

• Fig. 11.4 Right atrial enlargement. Right atrial enlargement is often difficult to detect with only subtle enlargement of the right heart border present on the PA view.

• Fig. 11.5 Selective left ventricular enlargement in aortic incompetence. (A) Frontal view shows that the left ventricle has enlarged along its long axis, taking the apex of the heart to the left and downward (white arrow). (B) Lateral view shows the left ventricle extending behind the line of the barium-filled oesophagus (arrow).

• Fig. 11.6 Gross right ventricular enlargement due to isolated right ventricular cardiomyopathy. The right ventricular enlargement occurs on the left heart border between the left ventricular contour and the pulmonary outflow tract (A) and is well seen on the lateral film (B).

• Fig. 11.7 Normal chest radiograph. In the normal subject there is a marked difference between the size of the upper and lower zone vasculature, the lower zone vessels being much more prominent.

• Fig. 11.8 Pulmonary arterial hypertension. The heart has a large triangular shape with large main and central pulmonary arteries. There is complete infilling of the pulmonary artery/ventricular concavity on the left heart border. The pulmonary arteries within the lungs are enlarged but there is rapid tapering of the vessels as they run towards the periphery.

• Fig. 11.9 Pulmonary arterial hypertension. If the pulmonary artery hyper-tension is severe and chronic, the pulmonary arteries may become very large and calcified (arrows).

• Fig. 11.10; Pulmonary venous hypertension. There is a mild haziness in the lower zones with attenuation of the lower zone vessels and prominence of the upper zone vessels. There is loss of definition of the heart and mediastinal contours. This is most notable when viewing the branches of the right pulmonary artery. The difference in density at the lung bases is due to a right mastectomy.

• Fig. 11.11 Kerley B lines are caused by interstitial fluid and are defined as subpleural perpendicular lines 1-3 cm in length (A). These lines often resolve following treatment (B).

• Fig. 11.12 Pulmonary plethora due to high-output cardiac failure. This PA chest radiograph demonstrates pulmonary plethora (A). The pulmonary vessels are considerably enlarged and also more tortuous than usual. The central pulmonary arteries are also large. This patient had a large femoral arteriovenous fistula (arrow) due to venous surgery 20 years previously. The calcified fistula is evident on a plain film (B).

• Fig. 11.13 Depressed sternum. (A) Frontal view. The heart is displaced to the left. Its left border is straight and there is a prominence in the position of the main pulmonary artery. There is an ill-defined shadow to the right of the vertebral column. The clue to those appearances is given by the visualisation of the intervertebral discs at the level of the lower thoracic spine where normally they would disappear. (B) Lateral view. This demonstrates the enormous sternal depression. This patient was thought to have a normal heart.

• Fig. 11.14 Pre- and post-mitral valve replacement. The preoperative film shows mild cardiac enlargement and pulmonary venous hypertension with good aeration of both lungs (A). On the mobile AP film (B) on the second postoperative day there is poor air entry to the chest leading to basal atelectasis. Small bilateral pleural effusions are also present and the mitral prosthesis can be identified.

• Fig. 11.15 Post cardiac surgery. The midline sternotomy sutures are difficult to visualise on the PA film. There are surgical clips in the anterior mediastinum which have been used to occlude small side branches of the left internal mammary artery (arrow), which has being used as a graft.

• Fig. 11.16 Cardiac surgery complication. On the PA chest radiograph (A) the right heart border has an unusual configuration and on closer inspection a metallic strip can be visualised (arrows). This soft-tissue opacity is anterior to the heart and clearly visualised (arrows) on the lateral film (B). This was a retained swab.

• Fig. 11.17 Coronary artery stent. This patient presented with a cough. On the PA chest radiograph (A), a 3-cm soft-tissue mass is present due to an adenocarcinoma of the left bronchus. A stent is seen in the left anterior descending coronary artery (arrow). The detailed configuration of the stents clearly seen (arrow) on the magnified view (B).

• Fig. 11.18 Prosthetic mitral and aortic valves with biventricular pacemaker insertion. This treatment for heart failure allows synchronous contraction of both ventricles. There is one lead with its tip in the coronary sinus (black arrow) to pace the left ventricle (A). This position is best visualised on the lateral view (B). The other lead has its tip in the apex of the right ventricle (white arrow).

• Fig. 11.19 Automatic implantable defibrillator. The electrode is heavier than a normal pacing electrode with additional discharge electrodes in the SVC and the right ventricle. The generator is larger than the current generation pacemaker generators.

• Fig. 11.20 Pneumothorax post pacemaker placement. A single-chamber pacemaker has been inserted. The tip is in a good position on both the PA film (A) and lateral film (B) in the apex of the right ventricle. The lateral film taken within 24 hours of pacemaker insertion is obtained using a non-standard method with the arms by the side. There is a large left pneumothorax.
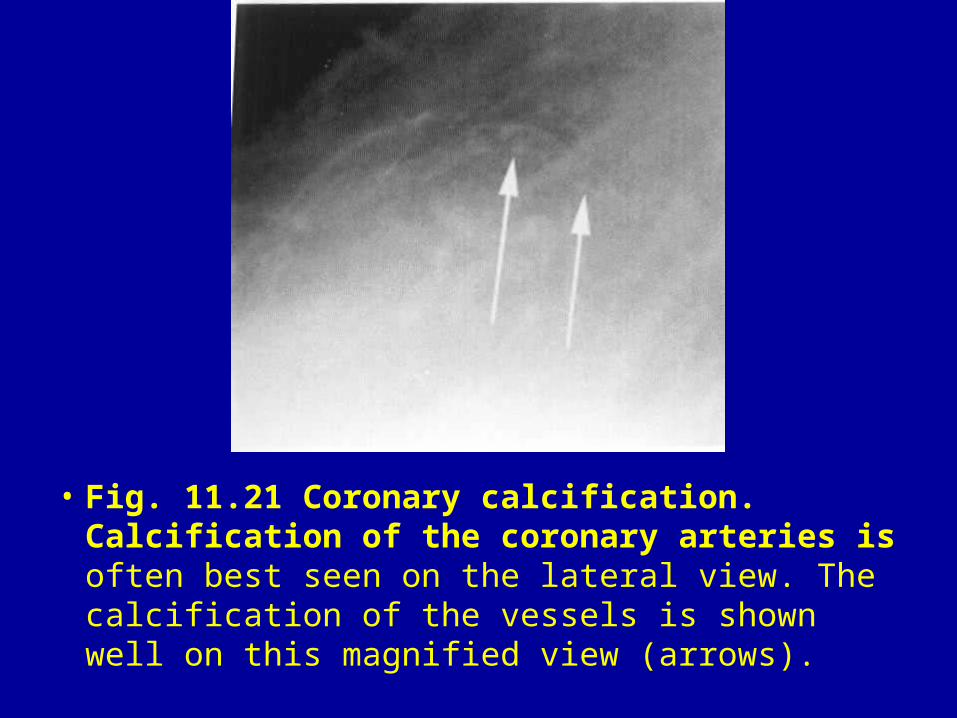
• Fig. 11.21 Coronary calcification. Calcification of the coronary arteries is often best seen on the lateral view. The calcification of the vessels is shown well on this magnified view (arrows).

• Fig. 11.22 Cardiac failure post myocardial infarction. A previous PA film obtained before the infarction is normal. Marked cardiomegaly is seen 2 weeks after a large anterior myocardial infarction, indicating left ventricular damage. Pulmonary venous hypertension has also developed.

• Fig. 11.23 Post myocardial infarction ventricular septal defect. This patient developed breathlessness on day 4 after an acute myocardial infarction. The interventricular septum has ruptured producing left to right shunting and heart failure. There is engorgement of the pulmonary vasculature (pulmonary plethora).

• Fig. 11.24 Anterior left ventricular aneurysm. There is a bulge of the anterior border of the left ventricle shown on both the PA (A) and lateral (B) films (arrows). This patient suffered a large infarct and has developed an anterior aneurysm of the left ventricle.

• Fig. 11.25 Posterior left ventricular aneurysm. The PA chest radiograph shows a sharply defined and rounded left heart border due to the profiling of the margin of the aneurysm (A). The bulge of the posterior border of the left ventricle due to the aneurysm is clearly seen on the lateral film (B) (arrows).

• Fig. 11.26 Calcification of a left ventricular aneurysm. In a small number of cases a fine line of calcification within the aneurysm can be identified (arrows).

• Fig. 11.27 Postmyocardial infarction (Dressler's) syndrome. Small effusions are seen in both costophrenic angles, together with ill-defined basal shadows resembling pulmonary infarcts.

• Fig. 11.28 Ischaemic cardiomyopathy. There is biventricular dilatation of the ventricles producing a globular large heart in this patient with ischaemic cardiac failure.

• Fig. 11.29 Calcified aortic stenosis. The heart has a slightly prominent left ventricular contour on the PA chest radiograph and there is dilatation of the ascending aortic arch (arrow) caused by the poststenotic dilatation (A). Calcification of the aortic valve (arrow) is more apparent on the lateral film (B).
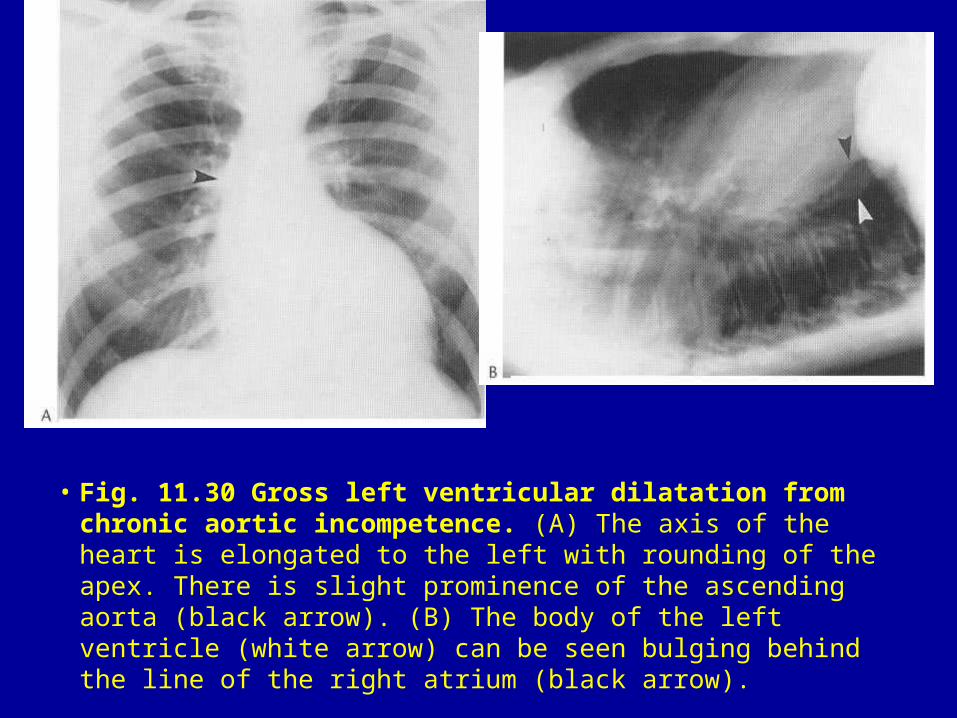
• Fig. 11.30 Gross left ventricular dilatation from chronic aortic incompetence. (A) The axis of the heart is elongated to the left with rounding of the apex. There is slight prominence of the ascending aorta (black arrow). (B) The body of the left ventricle (white arrow) can be seen bulging behind the line of the right atrium (black arrow).

• Fig. 11.31 Left atrial dilatation in mitral stenosis. The grossly enlarged left atrium (arrows) extends beyond the right heart border. Note that the border of the right atrium can be identified where it is joined by the IVC coming up through the diaphragm.

• Fig. 11.32 Mitral stenosis with a normal size heart. In the early years of this chronic disease there is often a normal heart size with only subtle signs of left atrial enlargement being evident. The left atrial appendage is prominent and there is pulmonary venous hypertension.
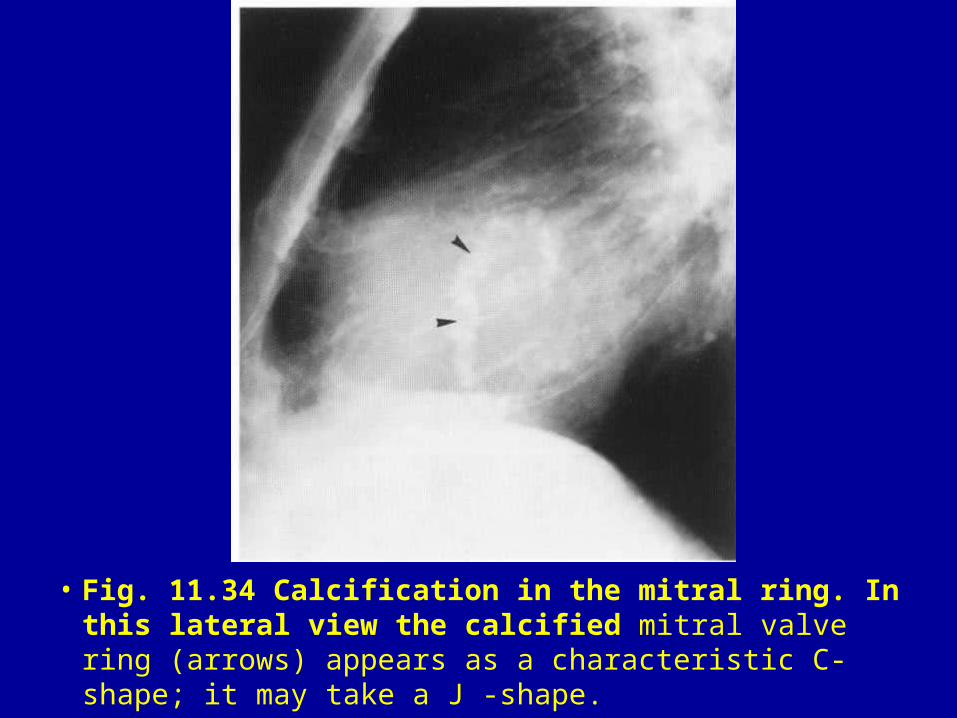
• Fig. 11.34 Calcification in the mitral ring. In this lateral view the calcified mitral valve ring (arrows) appears as a characteristic C-shape; it may take a J -shape.

• Fig. 11.33 (A, B) Calcified mitral valve in rheumatic mitral stenosis. The calcification is best seen in the lateral view (arrow).

• Fig. 11.35 Pulmonary haemosiderosis secondary to longstanding mitral valve disease. The fine granular background pattern to the lung is typical of haemosiderosis. In addition, note changes suggestive of mitral valve disease: straightening of the left heart border and some upper-lobe blood diversion.
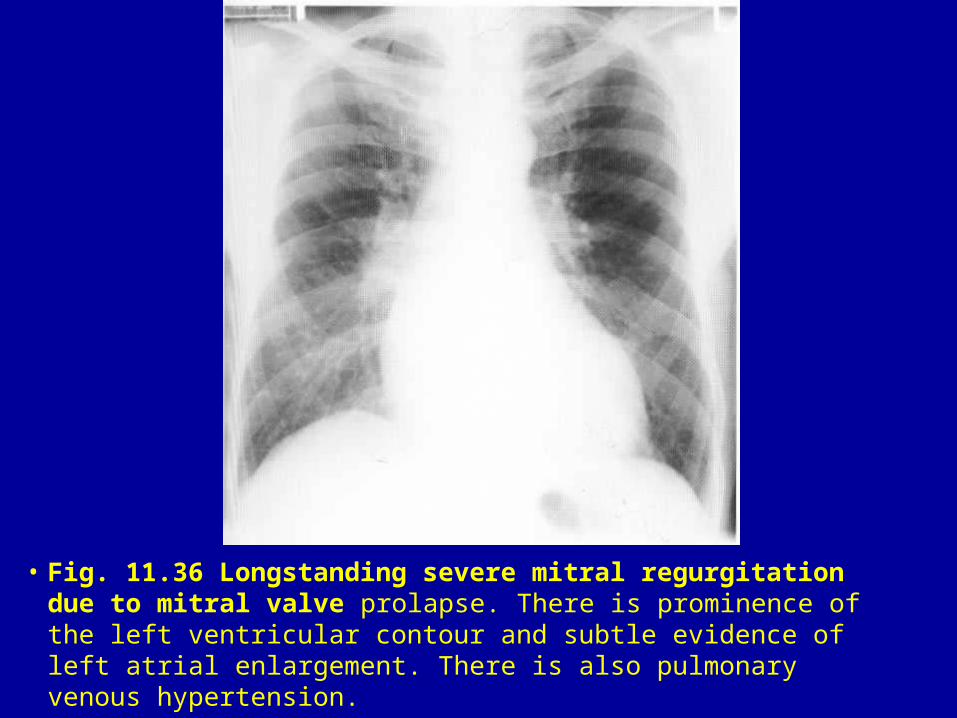
• Fig. 11.36 Longstanding severe mitral regurgitation due to mitral valve prolapse. There is prominence of the left ventricular contour and subtle evidence of left atrial enlargement. There is also pulmonary venous hypertension.

• Fig. 11.37 Acute non-rheumatic mitral regurgitation. (A) Frontal view in the acute phase. The heart size is virtually normal, even in the presence of high left atrial pressure as evidenced by the preferential dilatation of the upper-lobe vessels and interstitial oedema. (B) Frontal film 2 weeks later. This shows clearing of the oedema though upper-lobe blood diversion can still be seen.

• Fig. 11.38 Tricuspid stenosis. (A) The right heart border has bulged to the right and its radius of curvature has increased. (B) In the lateral view, the gap between the front of the heart and the sternum is filled in.

• Fig. 11.39 Pericardial effusion. A chest film taken 6 months previously was normal. (A) Frontal chest film. The heart silhouette has dramatically increased in size. There is an ill-defined bulge (arrow) above the cardiac apex. The lungs show no features of cardiac failure, which might be expected if this were a dilated heart. (B) Lateral chest film. Epicardial fat is clearly identified (arrows), displaced away from the edge of the cardiac silhouette and indicating the presence of a pericardial effusion.

• Fig. 11.40 Pericardial effusion. The first film in a patient who has had a left mastectomy for a carcinoma of the breast demonstrates a normal heart (A). However, during the course of treatment the patient became breathless and a follow-up film (B) shows marked enlargement of the cardiac silhouette as a result of a malignant pericardial effusion. A right-sided pleural effusion has also developed.

• Fig. 11.41 Constrictive pericarditis with calcification of the pericardium. Often with constrictive pericarditis there is straightening of the right heart border and roughening of the cardiac outline as a result of pleuropericardial thickening. Calcification often has a characteristic distribution involving the anterior and lateral aspects of the heart as shown on the PA (A) and lateral films (B) (arrows).

• Fig. 11.42 Cardiac fat pad. There is a low-density soft-tissue opacity adjacent to the right heart border (arrow). The triangular nature of the lesion with the characteristic position suggests the diagnosis of a pericardial fat pad.

• Fig. 11.43 Pericardial cyst. (A) Frontal chest radiograph, there is a sharply defined abnormal shadow in the right pericardiophrenic angle. (B) Lateral view. This is seen to lie anteriorly, and is one of the characteristic sites for a pericardial cyst.

• Fig. 11.44 A congenital pericardial defect. An isolated pericardial defect is usually left sided (arrows) and can allow prolapse of the left atrium beyond the normal left heart contour.

• Fig. 11.45 Pericardial cysts. The outline of the left ventricle has an undulating appearance (arrows); this was due to the presence of multiple pericardial cysts, which were tuberculous in origin.

• Fig. 11.46 Hydatid pericardial disease. Multiple large cysts (arrows) distort the cardiac outline.

• Fig. 11.47 Left atrial myxoma. The chest X-ray shows selective enlargement of the left atrium; the left atrial appendage is also enlarged.

• Fig. 11.48 Aortic dissection. There is unfolding of the aorta on this PA film in a patient who presented with severe back pain. There is a double density within the aortic arch that is unusual but suggests the possibility of a false lumen. A type A dissection was diagnosed on CT (black/white arrows).

• Fig. 11.49 Traumatic aortic rupture. This patient was involved in a high speed road traffic accident. The film demonstrates several important features of a transected aorta. There is a widened mediastinum. This is nonspecific finding, but a mediastinal width of greater than 8 cm or a mediastinum to chest ratio of greater than 0.25 are highly suggestive of a large mediastinal haematoma associated with this diagnosis. There is a left pleural effusion producing hazy opacification in this supine patient. There is also poor definition of the lateral border of the descending aorta.

• Fig. 11.50 Calcified saccular aneurysm of the aortic arch. Both the PA (A) and lateral films (B) demonstrate the large saccular aneurysm of the aortic arch (arrow). The aneurysm has calcified.

• Fig. 11.51 Aortic stab wound. The supine view shows marked widening of the mediastinum indicating haemorrhage. There is also an increase in density in the left hemithorax, due to the presence of a left-sided pleural effusion.

• Fig. 11.52 Aneurysm of the ascending and descending aorta. This PA film demonstrates marked dilatation of the ascending aorta consistent with a large aneurysm, in a patient with atheromatous disease.

• Fig. 11.53 Aneurysm of the descending aorta. The descending aorta has become dilated and tortuous with a marked increase in size (arrows). These changes are often well visualised on both PA (A) and lateral (B) films.

• Fig. 11.54 Expanding aortic aneurysm. These serial PA films of a patient with Marfan's disease demonstrate expansion of the ascending aorta as an aneurysm develops. The initial film shows mild prominence of the ascending aorta, unusual in a young adult male (A). The second film taken 2 years later shows obvious increase in prominence of the ascending aorta (arrow) as the aortic root has expanded (B).

• Fig. 11.55 Aortic incompetence due to syphilitic aortic root aneurysm. (A) Frontal view, showing left ventricular dilatation extending to the left and only a slight prominence in the position of the ascending aorta, with a barely visible rim of calcium. (B) Lateral view, showing a large saccular aortic root aneurysm clearly outlined by calcification.

• Fig. 11.56 Acute massive pulmonary embolism. (A) Frontal chest film (portable). The right lung and the left upper zone are hypertransradiant due to oligaemia, and there is overperfusion of the left mid and lower zones. (B) Pulmonary arteriogram, same patient. The leading edge of an embolus is seen impacted in the right pulmonary artery, producing virtually complete obstruction. Another embolus is seen in the supply to the left upper lobe which is also impaired. Only the left lower lobe fills adequately with contrast medium.

• Fig. 11.57 Pulmonary arteriovenous malformations. (A) Frontal chest film. Abnormal pulmonary shadows, typically elongated, can be identified in the right mid zone. (B) Pulmonary arteriogram. The pulmonary arteriovenous malformations in the right mid zone, associated with premature venous filling, can be identified. Additional abnormal pulmonary vessels are clearly visible in the right upper zone and throughout the left lung.



















