1045 Patient Radiation Exposure During ERCP Can Be Successfully Reduced by Education of...
2
patients with successful vs. failed (recurrent bleeding during hospitalization) gastric variceal obturation following injection of OCA were analyzed using non- parametric statistical techniques. Results: Out of a total of 89 patients (58 men; mean age 58 13 years) who underwent OCA injection for GV, eleven were excluded since they were treated electively as outpatients. The remaining 78 patients, hospitalized for acute GVH, were analyzed. Causes of GV included alcoholic cirrhosis (37%), NASH (19%), hepatitis B/C (15%) and splenic vein thrombosis (29%). GV were categorized as GOV-1 (4%), GOV-2 (64%) and IGV-1 (32%) per Sarin classification. Initial control of bleeding was achieved in 78 (100%) patients following OCA therapy, and long-term hemostasis was sustained in 71 (91%) patients. Seven (9%) patients had recurrent GVH during their hospital stay; 4 had early (48 hrs) and 3 had late (48 hrs) rebleeding. Glue- related pulmonary embolism (PE) occurred in two patients, which was fatal in one. All-cause, in-hospital mortality was 15% due to recurrent GVH (n3), acute renal failure (n6), advanced cancer (n1), hemorrhagic stroke (n1) and glue- related PE (n1). The all-cause mortality rate was 49% at a median follow-up of 47 weeks. Comparison of clinical and endoscopic variables in patients with successful (n71) versus failed (n7) glue injection therapy did not show any significant difference except for MELD score (Table 1). On univariate logistic regression analysis, high MELD score was associated with an increased risk of rebleeding after OCA injection [OR 1.22 (95% CI 1.11-1.42)]. Conclusions: Endoscopic injection of OCA achieves long-term hemostasis in 90% of patients with acute GVH, with a 2.5% risk of embolic complications. A high MELD score was associated with an increased risk of rebleeding following OCA therapy. Table 1. Comparison of Variables in Patients with Successful vs. Failed Gastric Variceal Obturation (GVO) with 2-Octyl Cyanoacrylate Variables Successful GVO (n71) Failed GVO (n7) p-value Age (median, yrs) 59 57 0.87 Male, n (%) 47 (66) 4 (57) 0.69 Fundal varices (GOV2/IGV1), n (%) 68 (96) 7 (100) 0.57 Large varices 10 mm, n (%) 23 (32) 3 (43) 0.10 High risk stigmata, n (%) 15 (21) 4 (57) 0.08 Ascites, n (%) 34 (48) 5 (71) 0.43 Encephalopathy, n (%) 17 (24) 2 (29) 0.89 MELD score (median) 12 28 0.0003 1044 Over the Scope Clip for Therapy of Dieulafoy Lesions-a Case Series Kondal R. Kyanam Kabir Baig* 1 , Timothy a. Woodward 1 , Thomas Kratt 2 1 Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, FL; 2 University Department of General, Visceral and Transplant Surgery, University of Tuebingen, Tuebingen, Germany Background: Dieulafoy lesions are abnormally large, tortuous, submucosal arterioles in the stomach wall that can erode and bleed. These are rare causes of upper gastrointestinal bleeding (UGIB) but can cause hemodynamically significant and massive bleeding due to the nature of the vessel and are difficult to diagnose or treat especially in the absence of active bleeding. Various endoscopic therapeutic modalities have been described for the treatment of Dieulafoy lesions but the superiority of any one modality has not been demonstrated. The Over-The-Scope Clip (OTSC) is a novel endoscopic device that has recently been described in literature for the treatment of refractory UGIB due to large visible vessels within ulcers. In theory, the size of the clip and its large compressive force provide an advantage in the treatment of large vascular lesions. This concept has been borne out in animal models of active arterial bleeding. This is the first international, two center, case series of successful OTSC therapy of Dieulafoy lesions. Objective: To evaluate the utility of the OTSC for treatment of Dieulafoy lesions. Methods: Retrospective case series of six patients who had UGIB due to Dieulafoy lesions in the stomach successfully treated with OTSC. Hemostasis at endoscopy after OTSC use was the main outcome measure. Lack of bleeding at four weeks of follow-up was a secondary measure. Results: The success rate in our case series was 100%. All cases of Dieulafoy lesions treated with OTSC met the criteria for the immediate outcome of successful hemostsasis by the end of the procedure. There was one complication during endoscopy directly related to OTSC use. A superficial mucosal tear of the esophagus occurred during passage of the OTSC through the esophagus. The tear was successfully closed using through the scope (TTS) clips and the patient had an uneventful recovery. There were no other immediate or delayed complications. All patients remained without any further bleeding after follow-up for at least 4 weeks. Four of six patients had subsequent upper endoscopy which showed a scar in one and OTSC in situ in three patients. Neither passage of the clip nor its persistence in the stomach caused any symptoms or complications. Conclusion: OTSC is an important and useful tool that can be used in the treatment of Dieulafoy lesions with a high success rate as demonstrated in this case series. Patient charecteristics Age/Sex Location in stomach Forrest Classification Prior Therapy Primary outcome met (Yes/No) Complications 1 70/M Proximal body IIa None Yes None 2 F/72 Distal body IIb Clips and glue injection Yes None 3 73/M Body IIa None Yes None 4 73/M Cardia Ia None Yes None 5 82/M Cardia IIa Clips and coagulation Yes Superficial Esophageal tear 6 74/M Body Ia None Yes None 1045 Patient Radiation Exposure During ERCP Can Be Successfully Reduced by Education of Endoscopists: Prospective Evaluation of the Impact of an Educational Program. Rajan Kochar* 1 , Shivangi Kothari 1 , Shai Friedland 1 , Ann M. Chen 1 , Charles Liao 2 , Subhas Banerjee 1 1 Division of Gastroenterology and Hepatology, Stanford University, Stanford, CA; 2 Department of Internal Medicine, Stanford University, Stanford, CA Background: Patients exposure to radiation during ERCP may increase their lifetime risk of developing cancer. Endoscopists increasingly perform their own fluoroscopy at ERCP and consequently control fluoroscopy unit settings and patient radiation exposure. In a recent study we demonstrated that low volume endoscopists (LVE) exposed patients to significantly higher amounts of radiation during ERCP compared to high volume endoscopists (HVE). Aim: To prospectively evaluate the impact of a brief educational program for endoscopists, on minimizing radiation exposure to patients during ERCP. Methods: All endoscopists performing ERCP at a tertiary care center received education on fluoroscopy best practices to minimize patient radiation exposure, including minimizing fluoroscopy time, image collimation, use of lower magnification images, reducing frame rates and spot films. A fluoroscopy ‘Time Out’ was performed before each ERCP to ensure these measures were incorporated. Fluoroscopy data on all the above parameters was then prospectively collected over 4 months for 2 HVE and 7 LVE (endoscopists performing 200 ERCPs a year). The radiation dose was recorded using a dose area product (DAP) meter mounted under the X-ray collimator. Fluoroscopy data was then compared with data on patients who underwent ERCP by the same endoscopists over a 6-month period prior to the educational program. Endoscopists completed a questionnaire to assess if following fluoroscopy best practices compromised their ability to interpret and perform ERCP. Results: Data on 331 patients undergoing ERCP prior to the educational program was compared with that of 251 patients undergoing ERCP following education (Table 1). For LVE, education resulted in significant decreases in mean DAP and mean Effective Radiation Dose. Significant increases were noted in the use of collimation and in the proportion of lower magnification images. A trend towards lower fluoroscopy time and lower number of images was seen, but did Successful deployment of OTSC. Abstracts www.giejournal.org Volume 77, No. 5S : 2013 GASTROINTESTINAL ENDOSCOPY AB182
Transcript of 1045 Patient Radiation Exposure During ERCP Can Be Successfully Reduced by Education of...

patients with successful vs. failed (recurrent bleeding during hospitalization)gastric variceal obturation following injection of OCA were analyzed using non-parametric statistical techniques. Results: Out of a total of 89 patients (58 men;mean age 58 � 13 years) who underwent OCA injection for GV, eleven wereexcluded since they were treated electively as outpatients. The remaining 78patients, hospitalized for acute GVH, were analyzed. Causes of GV includedalcoholic cirrhosis (37%), NASH (19%), hepatitis B/C (15%) and splenic veinthrombosis (29%). GV were categorized as GOV-1 (4%), GOV-2 (64%) and IGV-1(32%) per Sarin classification. Initial control of bleeding was achieved in 78(100%) patients following OCA therapy, and long-term hemostasis was sustainedin 71 (91%) patients. Seven (9%) patients had recurrent GVH during theirhospital stay; 4 had early (�48 hrs) and 3 had late (�48 hrs) rebleeding. Glue-related pulmonary embolism (PE) occurred in two patients, which was fatal inone. All-cause, in-hospital mortality was 15% due to recurrent GVH (n�3), acuterenal failure (n�6), advanced cancer (n�1), hemorrhagic stroke (n�1) and glue-related PE (n�1). The all-cause mortality rate was 49% at a median follow-up of47 weeks. Comparison of clinical and endoscopic variables in patients withsuccessful (n�71) versus failed (n�7) glue injection therapy did not show anysignificant difference except for MELD score (Table 1). On univariate logisticregression analysis, high MELD score was associated with an increased risk ofrebleeding after OCA injection [OR 1.22 (95% CI 1.11-1.42)]. Conclusions:Endoscopic injection of OCA achieves long-term hemostasis in �90% of patientswith acute GVH, with a 2.5% risk of embolic complications. A high MELD scorewas associated with an increased risk of rebleeding following OCA therapy.
Table 1. Comparison of Variables in Patients with Successful vs. Failed GastricVariceal Obturation (GVO) with 2-Octyl Cyanoacrylate
VariablesSuccessful GVO
(n�71)Failed GVO
(n�7) p-value
Age (median, yrs) 59 57 0.87Male, n (%) 47 (66) 4 (57) 0.69Fundal varices (GOV2/IGV1), n (%) 68 (96) 7 (100) 0.57Large varices � 10 mm, n (%) 23 (32) 3 (43) 0.10High risk stigmata, n (%) 15 (21) 4 (57) 0.08Ascites, n (%) 34 (48) 5 (71) 0.43Encephalopathy, n (%) 17 (24) 2 (29) 0.89MELD score (median) 12 28 � 0.0003
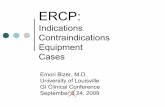
1044Over the Scope Clip for Therapy of Dieulafoy Lesions-a CaseSeriesKondal R. Kyanam Kabir Baig*1, Timothy a. Woodward1, Thomas Kratt21Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, FL;2University Department of General, Visceral and Transplant Surgery,University of Tuebingen, Tuebingen, GermanyBackground: Dieulafoy lesions are abnormally large, tortuous, submucosalarterioles in the stomach wall that can erode and bleed. These are rare causes ofupper gastrointestinal bleeding (UGIB) but can cause hemodynamicallysignificant and massive bleeding due to the nature of the vessel and are difficultto diagnose or treat especially in the absence of active bleeding. Variousendoscopic therapeutic modalities have been described for the treatment ofDieulafoy lesions but the superiority of any one modality has not beendemonstrated. The Over-The-Scope Clip (OTSC) is a novel endoscopic devicethat has recently been described in literature for the treatment of refractory UGIBdue to large visible vessels within ulcers. In theory, the size of the clip and itslarge compressive force provide an advantage in the treatment of large vascularlesions. This concept has been borne out in animal models of active arterialbleeding. This is the first international, two center, case series of successful OTSCtherapy of Dieulafoy lesions. Objective: To evaluate the utility of the OTSC fortreatment of Dieulafoy lesions. Methods: Retrospective case series of six patientswho had UGIB due to Dieulafoy lesions in the stomach successfully treated withOTSC. Hemostasis at endoscopy after OTSC use was the main outcome measure.Lack of bleeding at four weeks of follow-up was a secondary measure. Results:The success rate in our case series was 100%. All cases of Dieulafoy lesionstreated with OTSC met the criteria for the immediate outcome of successfulhemostsasis by the end of the procedure. There was one complication duringendoscopy directly related to OTSC use. A superficial mucosal tear of theesophagus occurred during passage of the OTSC through the esophagus. Thetear was successfully closed using through the scope (TTS) clips and the patienthad an uneventful recovery. There were no other immediate or delayedcomplications. All patients remained without any further bleeding after follow-upfor at least 4 weeks. Four of six patients had subsequent upper endoscopywhich showed a scar in one and OTSC in situ in three patients. Neither passageof the clip nor its persistence in the stomach caused any symptoms orcomplications. Conclusion: OTSC is an important and useful tool that can beused in the treatment of Dieulafoy lesions with a high success rate asdemonstrated in this case series.
Patient charecteristics
Age/SexLocation in
stomachForrest
ClassificationPrior
Therapy
Primaryoutcome
met(Yes/No) Complications
1 70/M Proximal body IIa None Yes None2 F/72 Distal body IIb Clips and glue
injectionYes None
3 73/M Body IIa None Yes None4 73/M Cardia Ia None Yes None5 82/M Cardia IIa Clips and
coagulationYes Superficial Esophageal
tear6 74/M Body Ia None Yes None
1045Patient Radiation Exposure During ERCP Can Be SuccessfullyReduced by Education of Endoscopists: Prospective Evaluationof the Impact of an Educational Program.Rajan Kochar*1, Shivangi Kothari1, Shai Friedland1, Ann M. Chen1,Charles Liao2, Subhas Banerjee1
1Division of Gastroenterology and Hepatology, Stanford University,Stanford, CA; 2Department of Internal Medicine, Stanford University,Stanford, CABackground: Patients exposure to radiation during ERCP may increase theirlifetime risk of developing cancer. Endoscopists increasingly perform their ownfluoroscopy at ERCP and consequently control fluoroscopy unit settings andpatient radiation exposure. In a recent study we demonstrated that low volumeendoscopists (LVE) exposed patients to significantly higher amounts of radiationduring ERCP compared to high volume endoscopists (HVE). Aim: Toprospectively evaluate the impact of a brief educational program forendoscopists, on minimizing radiation exposure to patients during ERCP.Methods: All endoscopists performing ERCP at a tertiary care center receivededucation on fluoroscopy best practices to minimize patient radiation exposure,including minimizing fluoroscopy time, image collimation, use of lowermagnification images, reducing frame rates and spot films. A fluoroscopy ‘TimeOut’ was performed before each ERCP to ensure these measures wereincorporated. Fluoroscopy data on all the above parameters was thenprospectively collected over 4 months for 2 HVE and 7 LVE (endoscopistsperforming �200 ERCPs a year). The radiation dose was recorded using a dosearea product (DAP) meter mounted under the X-ray collimator. Fluoroscopy datawas then compared with data on patients who underwent ERCP by the sameendoscopists over a 6-month period prior to the educational program.Endoscopists completed a questionnaire to assess if following fluoroscopy bestpractices compromised their ability to interpret and perform ERCP. Results: Dataon 331 patients undergoing ERCP prior to the educational program wascompared with that of 251 patients undergoing ERCP following education (Table1). For LVE, education resulted in significant decreases in mean DAP and meanEffective Radiation Dose. Significant increases were noted in the use ofcollimation and in the proportion of lower magnification images. A trendtowards lower fluoroscopy time and lower number of images was seen, but did
Successful deployment of OTSC.
Abstracts
www.giejournal.org Volume 77, No. 5S : 2013 GASTROINTESTINAL ENDOSCOPY AB182

not reach significance. For HVE, education resulted in smaller, but significantdecreases in mean DAP and mean Effective Radiation Dose. A significantdecrease was also noted in the number of images. Prior to education, LVE hadsignificantly a higher mean DAP and mean Effective Radiation Dose compared toHVE. Following education, no significant differences were seen between the twogroups. None of the endoscopists reported any compromise in their ability tointerpret and perform ERCP despite incorporating fluoroscopy best practices.Conclusion: Educating endoscopists in fluoroscopy best practices significantlyreduces patient radiation exposure during ERCP. This benefit is morepronounced in LVE. All endoscopists (HVE and LVE) benefited from fluoroscopyeducation, allowing reduction in patient radiation exposure, withoutcompromising their ability to interpret and perform ERCP.
Table 1. Impact of education of LVE on patient radiation exposure during ERCP
Parameter Pre-Education Post-Education P value
Mean Dose Area Product(DAP) (Gycm^2)
21.3 8.3 0.002
Mean Total Effective Dose(mSv)
5.5 2.15 0.002
Mean Fluoroscopy time (min) 5.6 4.3 0.2Mean No. of images/
procedure6.51 5.22 0.1
Collimation of any image (%) 22 54 0.01Collimation of >50% images
(%)12 51 0.001
% of images that are lowmagnification (%)
47 67 0.001
Table 2. Impact of education of HVE on patient radiation exposure during ERCP
Parameter Pre-Education Post-Education P value
Mean Dose Area Product(DAP) (Gycm^2)
11.3 8.5 0.001
Mean Total Effective Dose(mSv)
2.9 2.2 0.001
Mean Fluoroscopy time (min) 4.3 4.1 0.6Mean No. of Images/
procedure6.45 5.23 0.0001
1046Can Early Double Guidewire Technique Facilitate Common BileDuct Cannulation and Reduce Post ERCP Pancreatitis? -Resultsof a Multicenter Prospective Randomized Controlled Trial:EDUCATION Trial-Naoki Sasahira*1,2, Hiroyuki Isayama1,3, Hiroshi Kawakami1,4,Yukiko Ito1,5, Saburo Matsubara1,6, Hirotoshi Ishiwatari1,7,Minoru Uebayashi1,8, Rie Uchino1,9, Hiroshi Yagioka1,10,Osamu Togawa1,11, Nobuo Toda1,12, Naoya Sakamoto1,4, Junji Kato1,7,Kazuhiko Koike1,3
1Japan EDUCATION study group, Tokyo, Saitama, and Hokkaido,Japan; 2Department of Gastroenterology, Sempo Tokyo TakanawaHospital, Tokyo, Japan; 3Department of Gastroenterology, TheUniversity of Tokyo, Tokyo, Japan; 4Department of Gastroenterology,Hokkaido University, Hokkaido, Japan; 5Department ofGastroenterology, Japan Red Cross Medical Center, Tokyo, Japan;6Department of Gastroenterology, Tokyo Metropolitan Police Hospital,Tokyo, Japan; 7Department of Gastroenterology, Sapporo MedicalUniversity, Hokkaido, Japan; 8Department of Gastroenterology,Japanese Red Cross Kitami Hospital, Hokkaido, Japan; 9Department ofGastroenterology, Kanto Central Hospital, Tokyo, Japan; 10Departmentof Gastroenterology, JR Tokyo General Hospital, Tokyo, Japan;11Department of Gastroenterology, International Medical Center,Saitama Medical University, Saitama, Japan; 12Department ofGastroenterology, Mitsui Memorial Hospital, Tokyo, JapanBackground: Double guidewire cannulation method (DGW) is one of the rescuetechniques for wire-guided cannulation (WGC) during endoscopic retrogradecholangiography (ERC). It is usually applied after several times of unintentionalinsertion of a guidewire (GW) into the main pancreatic duct (MPD). Wehypothesized that early DGW at the first unexpected insertion of GW into MPDmight facilitate common bile duct (CBD) cannulation and reduce post ERCPpancreatitis (PEP). Therefore, we conducted this multicenter randomizedcontrolled trial of early DGW vs. repeated WGC. Patients and Methods: Allpatients with naïve papilla who was to undergo therapeutic ERC were enrolled
and primarily registered before ERC. ERC was performed using WGC and afterthe first unintentional insertion of GW into MPD, patients were randomized intoearly DGW vs. repeated WGC. Initial standard WGC or subsequent randomizedmethod was limited in 10 attempts and 10 minutes, and any rescue techniquescould be applied after these limits. Primary endpoint was a success rate of biliarycannulation within 10 attempts or 10 minutes from the randomization. Secondaryendpoints were final cannulation rate and PEP rate in the randomized group aswell as in all primarily registered participants. Sample size of 280 patients forrandomization was calculated, based on an assumption of success rate of biliarycannulation of 84% in early DGW and 70% in repeated WGC. Results: A total of715 participants were primarily enrolled to complete the final randomization of280 patients and 707 of them were included in final analyses. The successfulcannulation into CBD on the first attempt was achieved in 334 patients (47.2%)with a PEP rate of 3.9%. After unintentional insertion of GW into MPD, 274patients were randomized (137 patients in each group). Patient characteristicsand the subsequent interventional procedures were not different between twogroups. The success rate of CBD cannulation within 10 minutes or 10 attemptswas 75.2% and 70.1% in early DGW and repeated WGC (p � 0.42). The finalcannulation rate was 97.8% and 97.1% (p � 0.70). PEP rate was 19.7% and 16.8%in early DGW and repeated WGC (p � 0.64). Among 98 patients with failedcannulation into both CBD and MPD within the first 10 attempts or 10 minutes,79 patients finally completed the planned therapeutic procedure with otherrescue techniques with PEP rate of 15.3%. Overall final cannulation rate and PEPrate in total study population of 707 patients were 96.3% and 11.0%, respectively.Conclusion: In therapeutic ERC using WGC, early DGW neither facilitated CBDcannulation nor reduced PEP compared to repeated WGC. Of all 707 patientsenrolled in this study, only patients with successful CBD cannulation withoutunintentional GW insertion into MPD achieved a low rate of PEP (clinical trialregistration number: UMIN000005437).
Abstracts
AB183 GASTROINTESTINAL ENDOSCOPY Volume 77, No. 5S : 2013 www.giejournal.org