1.0 · Web viewFor the latter censuses, that is, 2002 and 2012 censuses, the sex ratio generally...
21
ZIMBABWE ZIMBABWE DEMOGRAPHIC FACT SHEET AUGUST 2015 1 | Page
Transcript of 1.0 · Web viewFor the latter censuses, that is, 2002 and 2012 censuses, the sex ratio generally...

ZIMBABWE DEMOGRAPHIC FACT SHEETSource of data for this Fact Sheet is the 2012 Population Census unless stated otherwise.
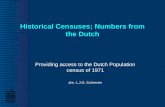
1.0 FERTILITY1.1 Fertility TrendsTotal Fertility Rate (TFR) has generally been declining in Zimbabwe– an implied decline of about 1.8 births during the 30-year inter-census period of 1982-2012. The decline was however halted in 2012 where TFR has slightly increased from 3.6 in 2002 to 3.8 in 2012.
1969 1982 1992 2002 20120
1
2
3
4
5
6
7
86.9
5.6
4.4
3.6 3.8
Year
Tota
l Fer
tility
Rat
e
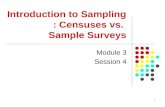
Figure 1 TFRs trend, Zimbabwe from various censuses Figure 2 ASDRs 1992, 2002, 2012
The Age Specific Fertility Rates (ASFRs) have also been declining from 1992. However the 2002 ASFRs are lower than the 2012 rates, which is consistent with a higher TFR in 2012 compared to 2002. Women in the age group 20-39 experienced higher ASFRs in 2012 than their counterparts during 2002.
1.2 Mean Parity Consistent with the decline in fertility is the decline in mean parities
(average number of children ever born to a cohort of women) by age. TFR, which measures current fertility, is consistently lower than the mean parity of women aged 45-49 years, a sign that fertility has been declining over the past three decades. Nevertheless mean parities
2 | P a g e
15-19 20-24 25-29 30-34 35-39 40-44 45-490
0.05
0.1
0.15
0.2
0.25
Observed Age Specific Fertility Rates
1992 2002 2012
Age Group
Age Sp
ecific
Fertilit
y Rate
s

show the same declining trend as fertility and the difference between the two is eroding. Figure 3: Mean Parity, women 45-49 years & TFR
Compared to countries in the SADC region Zimbabwe is ranked in the middle in terms of the level of its Total Fertility Rate. Figure 5 shows that,
generally, countries with higher GDP per capita have lower fertility rates i.e. South Africa, Botswana and Namibia, and those with lower GDP experience higher fertility levels i.e. Zimbabwe, Mozambique and Malawi.
Figure 4. Total Fertility Rates and per Capita GDP by country - Southern AfricaSource: Zimbabwe 2012 Population Census, World Bank (2015)
1.3 Fertility DifferentialsManicaland, Mashonaland Central, Mashonaland East and Mashonaland West provinces had TFRs of at least 4.0. Harare and Bulawayo provinces,
which are predominantly urban had much lower TFR
of 3.1 and 2.7 respectively. Among the rural provinces there is not much variation in TFRs except for the Matabeleland provinces which had much lower TFRs compared to other provinces.
3 | P a g e
South Africa Botswana Lesotho Namibia Swaziland Zimbabwe Mozambique Malawi Zambia Angola0
1000
2000
3000
4000
5000
6000
7000
8000
0
1
2
3
4
5
6
7
2.42.7
3.1 3.13.4
3.8
5.35.5
5.76
TFR GDP Per Capita
Country
Per C
apita
GDP
Tota
l Fer
tilty
Rat
e
Total
Bulawayo
Harare
Matebeleland South
Matebeleland North
Midlands
Masvingo
Mashonaland West
Mashonaland East
Mashonaland Central
Manicaland
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
3.8
2.7
3.1
3.6
3.7
3.8
3.9
4
4.1
4.2
4.2

Figure 5 Total Fertility Rates by Province
1.4 SummaryFertility declined between the 20-year inter-census period from 1992 with the decline of life time fertility accelerating among older women throughout the period while that of younger women declined largely during the 1992-2002 inter census period but receded during the 2002-2012 period. The increase in fertility between 2002 and 2012 most likely occurred after 2008 when the economy dollarized and stabilised. The increase in fertility between 2002 and 2012 can therefore be considered temporary, and will correct itself to levels below the 2002 rates.
Going forward we expect fertility in Zimbabwe to remain high because it still occurs to early and late in the lives of mothers, as shown by the high fertility among adolescent women, and significant fertility beyond age thirty five. In addition fertility remains high despite high educational attainment by Zimbabwean women and relatively high Contraceptive Prevalence rates among Zimbabwean women compared to other countries. Factors that could be propping fertility include parents viewing children as a form of security in old age in the absence of strong social protection systems, therefore the more the better, and children still viewed as economic assets. Meanwhile, it is important to address the increasing adolescent fertility through (i) keeping adolescents in school and colleges, and creating jobs for them (ii) making it easy for adolescents to access family planning information and services and (iii) designing programmes which will encourage contraceptive use intended to delay the first birth within marriage.
2.0 MORTALITY2.1 Mortality in the General PopulationIn Zimbabwe trends and levels of mortality have been influenced by the HIV and AIDS condition. The period 1992 to 2002, when the prevalence of HIV accelerated and when Anti-retroviral therapy (ART) was not widespread, mortality increased among the population. For the intercensus period 2002 to 2012, after widespread adoption of ART, mortality indicators improved significantly. Figures 9 below illustrate the development.
4 | P a g e

Figure 6 Crude Death Rates 1992, 2002 and 2012
The intercensus declining trend is also confirmed by Figure 11 below, which shows that at all ages below 74 years, the ASDRs were lower in 2012 than in 2002.
Figure 7 Age Specific Death Rates 2002 and 2012
2.2 Maternal MortalityMaternal mortality is measured by the Maternal Mortality Ratio, which is the number of maternal deaths per 100,000 live births. The age-pattern of maternal mortality depicts high maternal mortality among teenagers (525 for those aged 15-19 years) and women above 40 years, 1108 among women aged 40-44 years and 2367 among those aged 45-49 years. This
5 | P a g e
1992 2002 20120
2
4
6
8
10
12
14
16
18
20
9.5
17.2
10.2
CDR
- Num
ber o
f dea
ths p
er 1
,000
pop
ulati
on
Under 1
'01 - 04
'05 - 09
'10 - 14
15 - 19
20 - 24
25 - 29
30 - 34
35 - 39
40 - 44
45 - 49
50 - 54
55 - 59
60 - 64
65 - 69
70 - 74
75 - 79
80 - 84
85 - 89
90 - 94
95+0
50
100
150
200
250
2002 Both sexes 2012 Both sexes
Age Group
ASDR
s

shows that it is very risky to give birth at very young ages and at older ages.
Figure 8 Maternal Mortality Ratio by Age Group
The overall MMR
improved by 50% during the inter census period 2002 to 2012. Mashonaland East province registered the most improvement of 60%. Variations by province is also evident with Matabeleland South having the highest MMR of 694 and Harare with the lowest of 379. Just like the general mortality in the population, the decline in maternal mortality is linked
to improvements in the HIV and AIDS condition and possibly to improved access to health services after the economy dollarised. However, the MMR remains high and falls short of the MDG target of 174.Figure 9 Maternal mortality ratios by province, Zimbabwe 2002 and 2012 censuses
2.4 Childhood MortalityThe 2012 Population census shows that from 1997 to 2008 childhood mortality increased albeit within a very narrow range. This trend mimics that of the death rates in the general population as explained by the impact of HIV and AIDS and the harsh economic conditions that prevailed during the latter half of the first decade of the millennium.
6 | P a g e
Bulawayo
Manicaland
Mashonaland Central
Mashonaland East
Mashonaland West
Matabeleland North
Matabeleland South
Midlands
Masvingo
Harare
Total
0 200 400 600 800 1000 1200 1400 1600570
516
627
602
546
591
694
522
579
379
544
1014
1060
1119
1502
1173
1034
1208
1010
1246
649
1069
2002 Census 2012 Census
15 - 19 20 - 24 25 - 29 30 - 34 35 - 39 40 - 44 45 - 49* Zimbabwe0
500
1,000
1,500
2,000
2,500
525401
489601
830
1,108
2,367
544

Figure 10 Childhood Mortality in Zimbabwe
Under 5 mortality rate is generally used as a measure of mortality in childhood because of its
insensitivity to the pattern of mortality. While there is a great deal of disparity in the estimated rates for some overlapping periods in certain cases, there is a fairly good
agreement among the various estimates that under-five mortality has been declining in Zimbabwe during the past three decades. While the declining trend is apparent up to the mid-1990s, it starts to increase thereafter due to the impact of HIV and AIDS on the population and the general deterioration of health services during the hyperinflationary period when the health sector suffered from a lack of resources and a shortage of staff.
7 | P a g e
1997 2000 2003 2005 20080
10
20
30
40
50
60
70
80
Infant Mortal-ity Rate
Child Mortal-ity Rate
Under 5 Mor-tality Rate
19731975
19771979
19811983
19851987
19891991
19931995
19971999
20012003
20052007
2009
92104
75
99 95 9484
9690
101
75 77
91 86 85 84 83
59
77
10290
8170
77
108
58 54
827968
49
63
49
72 74 72 75 80
ZDHS 88 (Dir.) ZDHS 88 (Ind.) ZDHS 94 (Dir.)ZDHS 94 (Ind.) ZDHS 99 (Dir.) ZDHS 99 (Ind.)ZDHS 2005-6 (Dir.) ZDHS 2005-6 (Ind.) 2012 Census (Ind.)
Year
Unde
r 5 M
ortali
ty

Figure 11 Trend in Under 5 Mortality from various sources
2.5 Regional Comparisons of Child mortalityComparing Zimbabwe’s Under 5 mortality rates with regional countries
shows that it is situated
in the middle. However Zimbabwe is way off its MGD target of an Under
5 Mortality of 25.
Figure 12 Under 5 Mortality Rates in Southern Africa Source Zimbabwe Population Census, 2012 and UNICEF (2013)
2.6 Mortality Differentials by Disability StatusUnder 5 mortality of children born to disabled mothers is higher than that of children born to mothers without disability. Policies should therefore be
put in place to improve the survival of children born to this disadvantaged group. The patterns of Under 5 mortality with respect to educational level of mother, marital status and with respect to residence of mother are expected. There is also great variablity of Under 5 mortality among the provinces. Under 5 mortality was lowest
among the Matabeleland and urban provinces. Figure 13 Under 5 Mortality Rates By Disability Status of Mother
8 | P a g e
With disability
Without Disability
Total
0 20 40 60 80 100 120
107
73
74
Under Five Mortality by Disability Status of Mother
Zimbabwe MDG Target
Namibia
South Africa
Botswana
Malawi
Zimbabwe 2008
Swaziland
Zambia
Mozambique
Lesotho
Angola
0 20 40 60 80 100 120 140 160 180
25
39
45
53
71
74
80
89
90
100
164

2.7 Life Expectancy at BirthWhile life expectancy at birth was around 60 years during the first year of independence, it declined to 57 years in 1992 and 43 years in 2002. This trend is explained by the HIV and AIDS trend. After 2002 life expectancy started to gradually increase reaching 60 years in 2012 (57 years for males and 64 years for females). The increase in life expectancy can be attributed to better survival chances of HIV and AIDS victims because of the general availability of ART and the general improvement in the
availability of medicines after dollarisation in 2009. The intercensus period 2002 to 2012 saw life expectancy increasing by 16.5 years i.e. an improvement of 1.65 years per year. We do not believe that this rate of life expectancy improvement is
sustainable into the future, as it is attributed to medical intervention and not substantive changes in the socio-economic conditions of the population.
Figure 14 Zimbabwe Life Expectancy at BirthSource: Zimbabwe Population Census, 2012 and World Bank
A regional comparison of life expectancies shows that Zimbabwe enjoys higher life expectancy than most of the regional countries. Its life expectancy is second to that of Namibia which stands at 63.9 years.
9 | P a g e
19801981
19821983
19841985
19861987
19881989
19901991
19921993
19941995
19961997
19981999
20002001
20022003
20042005
20062007
20082009
20102011
Zimbab
we 2012 Cen
sus
0
10
20
30
40
50
60
70
60.557
42.9
60.7
Year
Life
Expe
ctan
cy
Botswana
Mozambique
Angola
Malawi
South Africa
Zambia
Zimbabwe
Namibia
0 10 20 30 40 50 60 70
47
49
51
54.7
56.1
57
60.7
63.9
Life Expectancy at Birth
Coun
try

Figure 15 Life Expectancy for selected Southern African CountriesSource: Zimbabwe Population Census, 2012 and World Bank
3.0 POPULATION STRUCTURE3.1 Age StructurePopulation pyramids for Zimbabwe for the years 1992, 2002 and 2012 are wider at the base showing that there are more people in the younger age groups than in the older age groups for both sexes. This is explained by the high fertility levels among the population. Figures from the 2012 Population Census show that 41 percent of Zimbabwe’s population is aged
below 15 years. This proportion has changed slightly since 1992. It was the same as in 2002 but lower than the 1992 proportion of 45%. Zimbabwe’s population still remains young with half of it aged below 20 years. Regional comparisons show that South Africa has 30% of its population aged below 15 years and Zambia has 46% (Statistics South Africa, 2015 and Sikanyiti, 2012). The proportion of the population below 15 years to the total population for Zimbabwe and the region is much
higher than that of the UK and the European Union region of 18% and 16% respectively (The UK Office of National Statistics, 2010 and Eurostat, 2015).
Figure 16 Population pyramids, Zimbabwe population 1992, 2002 and 2012
3.2 Sex StructureThe overall sex ratio in 2012 was 92, that is, there were 92 males for every 100 females. Below the age of 15 years, there are almost equal
10 | P a g e

numbers of males and females. This is the case for all the censuses. For the 1982 and 1992 censuses the sex ratio favours females up to age 40 and 50 respectively and males dominate thereafter up to age 69 years. For the latter censuses, that is, 2002 and 2012 censuses, the sex ratio generally favours women throughout all age groups above 14 years. The trend
is that with time women are outliving their male counterparts at every age group.
Figure 17 Age-specific sex ratios, various years
3.3 Population Growth The youthful age structure of Zimbabwe’s population presents a high potential for rapid population growth as well as high dependency burden. Zimbabwe’s population has grown by 74% from 1982 to 2012, registering an average annual growth of 3.1%, 1.1% and 1.2% between 1982 and 1992, 1992 and 2002, and 2002 and 2012, respectively (Zimstat, 2013). At the 2002-2012 annual growth rate of 1.2% the population of Zimbabwe is expected to double in 58 years.
During the first decade of independence the age group 65+ grew fastest. This reflects improvements in life expectancy during this period due to progress made in the health delivery system. The age-pattern of growth
for 1992-2002 is similar to that for the previous decade yet the growth rates are slower. During this period, HIV and AIDS-related deaths had a huge impact on the population. Between 2002 and 2012, the pattern of growth is completely reversed. The age 0-14 grew fastest which could reflect the positive impact on births of the Prevention of Mother-to-Child Transmission (PMTCT) of HIV programme during this period and the fall in HIV prevalence rates. Since the youngest age
group is growing fastest, the population of Zimbabwe may experience rapid growth in future due to population momentum. Figure 18 Zimbabwe population in millions
11 | P a g e
1982 1992 2002 20120
2
4
6
8
10
12
14
7.5
10.411.6
13.1
0
1-4
5-9
10-1
4
15-1
9
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4 75+
50
60
70
80
90
100
110
120
130
1982 Census 1992 Census 2002 Census 2012 Census
Age Group
Sex R
atio

3.4 Dependency RatiosThe child dependency and overall dependency ratios are 70 and 83 per 100 working people, respectively. While in developed countries about two active persons support one dependent person, in Zimbabwe one active
person supports one dependent. The population 65 years and above stands at 4.1% and has slightly increased from 3% in 1982. For developed countries, specifically the EU, this proportion is as high as 18.5% (Eurostat, 2015).
Figure 19 Population age composition comparisonsSource: Zimbabwe 2012 Census and Population Reference Bureau 2012 Population Data Sheet
4.0 POPULATION PROJECTIONSThe 2012 population prjections assumed three scenarios; the high, medium and low scenario. The high scenario assumed a slower decline in fertility, the low scenario – a faster decline in fertility and the medium scenario assumed that fertility will decline at a rate in-between the high
and low scenarios. For all the scenarios life expectancy was assumed to increase to the same levels, the sex ratio was assumed to remain at the 2012 level and international migration was assumed to be zero. Only the low scenario assumed the impact of HIV and AIDS on the population. The population of
12 | P a g e
2012 2022 2017 2027 20320
5
10
15
20
25
13.114.5
1617.2
18.9
13.114.5
16.117.7
19.3
13.114.6
16.2
18
19.9
Low Medium High
Zimbabwe Southern Africa Least Developed Countries
More Developed Countries
4132
41
16
5563
56
68
4 5 316
65+ years 15-64 years <15 years
%

Zimbabwe is projected to grow to between 19 million and 20 million in 2032.
Figure 20 Projected Zimbabwe Population, 2012 to 2032
The development of the age-structure of the population is expected to be more bell-shaped than pyramidal as we go into the future. This in in line with the assumption of declining fertility in the projections and improved
longevity. Figure 21 Population pyramids, 2012 and 2032 Figure 22 Projected Population Composition, 2012 and 2032
As a result, the age composition of of the population is expected to have significantly changed by 2032. The proportion of the young population is expected to decline in 2032 and that of the labour force is expected to rise. The proportion of the elderly will largely remain unchanged. The dependency ratio will decline from 83 per 100 in 2012 to 57 per 100 in 2032. The reduction in the dependency ratio would augur well for economic development as the Government would have a relatively larger labour force to support fewer dependency.
The economically inactive under 15 and over 65 also tend to be bigger recipients of government spending e.g. education, pensions and health care.
13 | P a g e

Figure 23 Population Compositioon
During the projection period the annual average growth rate of the population is expected to be 2.0%, which is higher than the 2002-2012 rate of 1.1%. The rural population is projected to grow at a faster rate than the urban population, that is, 2.2% compared to 2.0%. The age group 0-4 years is projected to grow by 0.3% - this is in line with the assumption of declining fertility. The population of reproductive age is projected to grow by 3.3 percent, from 6.3 million in 2012 to 10.4 million in 2032, implying that the population will continue to grow significantly in spite of
declining fertility due to the phenomenon of population momentum. The projected growth of the working age population at 3.6 percent, which is higher than the growth of the school going age-group, the youth and the elderly creates opportunity for economic growth and
development. This opportunity is created because mortality and fertility are declining and the proportion of the working age population to the total has grown.
Figure 24 Projected annual average population growth rates by age
5. ZIMBABWE’S DEMOGRAPHIC STRUCTURE AND THE SCOPE FOR A DEMOGRAPHIC DIVIDENDDuring a demographic transition, when both mortality and fertility are declining, the population’s age structure also changes. The proportion of children falls while that of older people remains low until the large group
14 | P a g e
Working Age (1
5-64)
Reporductive
Age (15-49)
Young People (15-24)
Older Perso
ns (65+)
School g
oing age (5-24)
Annual Ave
rage Growth Rate
Children (0
-4)01234 3.59 3.27
2.23 2.161.52
2.0
0.39
Projected Population Group
Annu
al A
vera
ge G
row
th R
ates
(%)
<15 years 15-64 years 65+0
10
20
30
40
50
60
70
41.2
54.7
4.1
32.3
63.7
4
2012 2032
Age Group
% C
ompo
sition

of working age people gradually grows older. During this period, there the proportion of people of working age will be increasing while the dependency ratio will be falling, which makes the society more productive because fewer investments are needed to meet the needs of the youngest and oldest age groups, which are largely consumptive. In a country’s demographic development, this window of time between falling birth rates and ageing is referred to as a demographic bonus. If people in the working age group are trained, find employment and have long productive careers before they are dependent themselves, the demographic bonus becomes a demographic dividend. To achieve this there must be deliberate investment in education and the labour market.
The proportion of the population aged 15-64 years to total population has been increasing since 1982. The increasing trend was halted between 2002 and 2012 due to the attrition of the working age population by AIDS deaths. Correspondingly, dependency ratios that had been declining rose
between 2002 and 2012. In comparative terms, it can be said that Zimbabwe has fallen behind in its demographic transition by half a century compared to Eastern Asian countries since the latter had an age structure similar to present day Zimbabwe in 1965. For the three consecutive censuses of 1992, 2002 and 2012 the age pyramid of the population remains bloated in younger ages, showing that the population has remained young with half of it aged below 20 years.
This age structure is not synonymous with a structure conducive for a demographic bonus. Figure 25 Dependency ratios and proportion of population aged 15-64 years
Although Zimbabwe was moving towards a demographic bonus, a prerequisite for a demographic dividend, that trend has been reversed. The situation is exacerbated by the relatively slower growth of the population aged 15-64 years compared to the age group 0-14 years between 2002 and 2012. The age group 15-64 years had grown faster than the 0-14 years between periods 1982-1992 and 1992-2002.
According to the demographic transition theory, mortality decline is antecedent to fertility decline. Fertility still remains high in Zimbabwe, sadly showing signs of an increasing trend between 2002 and 2012, and far much higher than the levels that created a demographic structure amenable to the demographic dividend in Eastern Asia. Unless fertility levels fall, Zimbabwe’s population will remain young, making it difficult to reach for the demographic dividend.
15 | P a g e
1982 1992 2002 201244.0
46.0
48.0
50.0
52.0
54.0
56.0
58.0
0.0
20.0
40.0
60.0
80.0
100.0
120.0
Proportion 15-64 years Dependency ratios
Year
Prop
ortio
n 15-6
4 yea
rs
Depe
nden
cy ra
tios

Population projections based on the 2012 Population Census show that 64 percent of the population of Zimbabwe will be aged 15-64 years in 2032 compared to 55 percent in 2012. The population aged 0-14 years is projected to decline to about 32 percent from the current 41 percent and the population 65 years and above is not expected to change. This is premised on the assumption of a decline in fertility and improved longevity. If this transition takes place, it will be similar to the one that brought about the demographic dividend in Eastern Asia. However such a monumental shift in a country’s demographic structure does not happen spontaneously hence Zimbabwe needs to deliberately adopt policies to achieve it.
Policies to create a demographic bonus and realise the demographic dividendFamily planning programmes need to be scaled up in order to reduce the number of children per woman: The Zimbabwe Demographic and Health Survey 2010-11 shows that 13 percent of currently married women have an unmet need for family planning services. The same survey shows that as the number of children increases, up to 4, contraceptive use also increases. This may indicate the demand for contraception to attain a desired family size. Women’s access to reproductive health should also be improved because it is important for achieving desired family sizes.
There is need to put in place policies that delay the onset of childbearing among girls, as it has been shown that childbearing still occurs too soon in Zimbabwe: This can be achieved through instituting laws against early marriage, as girls who marry early are more likely to have more children than their peers who stay in school and marry later. Early marriage also reduces women’s economic contribution.
Zimbabwe should strive to have the majority of its population attain secondary education: Besides lowering fertility and mortality, higher levels of educational attainment will justify large investments in universities in order to create the human capital necessary for an innovative and productive economy. Emphasis should also be placed on vocational training because it introduces young people to the real working environment. This is important since the realisation of the demographic dividend requires higher levels of productivity to create savings and wealth. Furthermore, education diminishes the economic value of children, as educated parents have more chances of getting a job that provides security in old age. More educated parents have higher aspirations for their children, which increases investment in their health and education, thereby reducing their numbers as a trade off with quality.
Effective medical care should be afforded infants to improve their survival chances and take away the need to have many children as an insurance against child deaths: This is because where demographic transition has taken place, mortality decline preceded fertility decline. This also ensures that investment in education is concentrated in fewer children, even
16 | P a g e

though a huge investment in public health to combat communicable diseases may be required.
The country should create jobs mainly in highly productive sectors with high demand for low skilled workers: However as the level of education increases jobs would need to be created in knowledge intensive sectors that have greater added value. The job market needs to be liberalised and the private sector must also play a part in labour training. There should also be equality of employment opportunity between men and women.
Zimbabwe should further strengthen its social security systems during the demographic transition phase: This is because the demographic bonus will not last forever. As the large population cohorts that created the bonus age into retirement, the following generations are fewer in size, because of declining fertility, so the proportion of the working age population declines whereas the share of the older, economically dependent people increases. Other policies, such as keeping the older generations longer in the labour force, may be an option.
For more information on the results of the 2012 Zimbabwe Population Census Thematic Analysis, please contact:
Zimbabwe National Statistics Agency (Zimstat)Population Census OfficeP.O. Box CY342CausewayHarareTel: 04-793971-2, 04-794756E-mail: [email protected]
United Nations Population Fund (UNFPA)First Floor, Block 7Arundel Office ParkNorfolk RoadMt. Pleasant,P. O. Box 4775HarareTel: +263 4 338836-44, +263 912 572870-73, +263 912 125381 Fax: +263 4 338773E-mail: [email protected]
This fact sheet is based on the results of the 2012 Zimbabwe Population Census Thematic Analysis which was conducted by the Zimbabwe National Statistics Agency (Zimstat) with technical assistance from the United Nations Population Fund (UNFPA). Funding for the analysis was provided by the Government of Zimbabwe through Treasury, Australian Agency for International Development, Royal Danish Embassy, United Kingdom Department for International Development, European Union, 17 | P a g e

Swedish International Development Agency, United Nations Development Programme, United Nations Children’s Fund and the United Nations Population Fund.
18 | P a g e