10 Molecular Regulation of...
6
124 10 Molecular Regulation of Cardiogenesis VISHAL NIGAM AND DEEPAK SRIVASTAVA C ongenital heart malformations, the most common of all human birth defects, occur in almost 1% of the population worldwide, regardless of race (Hoffman and Kaplan, 2002). An additional 1%–2% of the population harbor more subtle cardiac developmental anomalies that only become apparent as age-dependent phenomena reveal the underlying pathology. With more than 1 million survivors of congenital heart disease (CHD) in the United States, it is becoming apparent that genetic disruptions which predispose to developmental defects can have ongoing consequences in the maintenance of specic cell types and cellular processes over decades (Srivastava, 2004). A more precise understanding of the causes of CHD is imperative for the recognition and potential intervention of progressive degenerative conditions among the survivors of CHD. Although genetic approaches have been important in understand- ing human CHD, detailed molecular analysis of cardiac development in humans has been difcult. The recognition that genetic pathways which dictate cardiac development are highly conserved across vastly diverse species ranging from ies to man has resulted in a rapid expansion of information from the studies in more tractable biologi- cal models (Srivastava and Olson, 2000; Chien and Olson, 2002). Despite the diversity of body plans adopted by different species, there seems to exist a common genetic program for the early formation of a circulatory system. Cardiovascular systems seem to have developed increasing complexity to adapt to specic environments. In a simpli- ed view, it appears that higher organisms have retained the morpho- logic steps used by lower organisms and have built complexity into the heart as needed. In particular, the specication of chamber structures and the advent of a parallel circulation through chamber duplication and outow tract division by neural crest derivatives have facilitated the development of larger, air-breathing organisms using complex cir- culatory systems. In such a scheme, defects in particular regions of the heart may arise from specic genetic and environmental effects dur- ing discrete developmental windows of time. To simplify the complex events of cardiogenesis and CHD, different regions of the developing heart will be considered individually in the context described earlier, weaving knowledge from model systems and human genetics when available. ORIGIN OF CARDIOMYOCYTE PRECURSORS Despite decades of cell lineage tracings and descriptive embryology of the heart’s origins, a more complete and accurate picture of cardio- genesis emerged only recently (reviewed in Buckingham et al., 2005; Srivastava, 2006). Two distinct mesodermal heart elds that share a common origin appear to contribute cells to the developing heart in a temporally and spatially specic manner. The well-studied “rst heart eld” (FHF) is derived from cells in the anterior lateral plate meso- derm, which align in a crescent shape at approximately embryonic day 7.5 (E7.5) in the mouse embryo, roughly corresponding to week 2 of human gestation (Fig. 10–1). By mouse E8.0, or 3 weeks in humans, these cells coalesce along the ventral midline to form a primitive heart tube that consists of an interior layer of endocardial cells and an exte- rior layer of myocardial cells, separated by the extracellular matrix necessary for reciprocal signaling between the two layers. The tubular heart initiates rhythmic contractions at about day 23 in humans. Previous lineage tracings using dye-labeling techniques suggested that cells along the anterior–posterior (AP) axis of the heart tube were destined to contribute to specic chambers of the future heart (reviewed in Srivastava and Olson, 2000). However, such studies could not determine the clonal contributions of individual cells (Meilhac et al., 2004). More recent studies using Cre-lox technologies to mark progenitor cells and all their descendents indicate—in stark contrast to previous models—that the heart tube derived from the FHF may predominantly provide a scaffold which enables a second population of cells to migrate and expand into cardiac chambers (Buckingham et al., 2005). These additional cells arise from an area often referred to as the “second heart eld (SHF)” or “anterior heart eld” based on its location anterior and medial to the crescent-shaped primary heart eld (Kelly et al., 2001; Mjaatvedt et al., 2001; Waldo et al., 2001; Fig. 10–1). Both heart elds appear to be regulated by complex posi- tive and negative signaling networks involving members of the bone morphogenetic protein (Bmp), sonic hedgehog (Shh), broblast growth factor (Fgf), Wnt and Notch proteins. Such signals often arise from the adjacent endoderm, although the precise nature and role of these sig- nals remain unknown (reviewed in Schultheiss et al., 1997; Marvin et al., 2001; Schneider and Mercola, 2001; Zaffran and Frasch, 2002). SHF cells remain in an undifferentiated progenitor state until incorporation into the heart, and this may in part be due to the closer proximity to inhibitory Wnt signals emanating from the midline. Recent work has raised the possibility that the Tbx18 may be required for the formation of a venous pole, which contributes portions of the atria and venous structures ( Christoffels et al., 2006). As the heart tube forms, the SHF cells migrate into the midline and position themselves dorsal to the heart tube in the pharyngeal meso- derm. Upon rightward looping of the heart tube, SHF cells cross the pharyngeal mesoderm into the anterior and posterior portions, popu- lating a large portion of the outow tract, future right ventricle and atria ( Cai et al., 2003; Fig. 10–1). Precursors of the left ventricle are sparsely populated by the SHF and appear to be largely derived from the FHF. In contrast to the FHF, SHF cells do not differentiate into cardiac cells until they are positioned within the heart. Once within the heart, FHF and SHF cells appear to proliferate in response to endocar- dial-derived signals such as neuregulin and epicardial signals depen- dent on retinoic acid, although the mechanisms through which these noncell autonomous events occur remain poorly understood ( Garratt et al., 2003; Stuckmann et al., 2003). CARDIOMYOCYTE AND HEART TUBE FORMATION Fruities have a primitive heart-like structure known as the dorsal ves- sel that is analogous to the straight heart tube of the vertebrate embryo. It contracts rhythmically and pumps hemolymph through an open circulatory system. Formation of the dorsal vessel in ies is depen- dent on a protein, tinman, whose name is based on the Wizard of Oz character that lacks a heart (Bodmer, 1993). Tinman belongs to the homeodomain family of proteins, and was initially described to play a role in establishing the regional identity of cells and organs during embryogenesis. In contrast to the requirement of tinman for heart formation in ies, its mammalian ortholog, Nkx2.5, is not essential for specication of the cardiac lineage in mice, suggesting either that other genes may share functions with Nkx2.5 or that cardiogenesis in ies and vertebrates dif- fers with respect to its dependence on this family of homeobox genes (Lyons et al., 1995; Tanaka et al., 1999). The possibility of functional 10-Epstein-Chap10.indd 124 10-Epstein-Chap10.indd 124 8/21/2007 8:35:16 PM 8/21/2007 8:35:16 PM
Transcript of 10 Molecular Regulation of...

124
10 Molecular Regulation of Cardiogenesis
VISHAL NIGAM AND DEEPAK SRIVASTAVA
Congenital heart malformations, the most common of all human birth defects, occur in almost 1% of the population worldwide,
regardless of race (Hoffman and Kaplan, 2002). An additional 1%–2% of the population harbor more subtle cardiac developmental anomalies that only become apparent as age-dependent phenomena reveal the underlying pathology. With more than 1 million survivors of congenital heart disease (CHD) in the United States, it is becoming apparent that genetic disruptions which predispose to developmental defects can have ongoing consequences in the maintenance of speci( c cell types and cellular processes over decades (Srivastava, 2004). A more precise understanding of the causes of CHD is imperative for the recognition and potential intervention of progressive degenerative conditions among the survivors of CHD.
Although genetic approaches have been important in understand-ing human CHD, detailed molecular analysis of cardiac development in humans has been dif( cult. The recognition that genetic pathways which dictate cardiac development are highly conserved across vastly diverse species ranging from * ies to man has resulted in a rapid expansion of information from the studies in more tractable biologi-cal models (Srivastava and Olson, 2000; Chien and Olson, 2002). Despite the diversity of body plans adopted by different species, there seems to exist a common genetic program for the early formation of a circulatory system. Cardiovascular systems seem to have developed increasing complexity to adapt to speci( c environments. In a simpli-( ed view, it appears that higher organisms have retained the morpho-logic steps used by lower organisms and have built complexity into the heart as needed. In particular, the speci( cation of chamber structures and the advent of a parallel circulation through chamber duplication and out* ow tract division by neural crest derivatives have facilitated the development of larger, air-breathing organisms using complex cir-culatory systems. In such a scheme, defects in particular regions of the heart may arise from speci( c genetic and environmental effects dur-ing discrete developmental windows of time. To simplify the complex events of cardiogenesis and CHD, different regions of the developing heart will be considered individually in the context described earlier, weaving knowledge from model systems and human genetics when available.
ORIGIN OF CARDIOMYOCYTE PRECURSORS
Despite decades of cell lineage tracings and descriptive embryology of the heart’s origins, a more complete and accurate picture of cardio-genesis emerged only recently (reviewed in Buckingham et al., 2005; Srivastava, 2006). Two distinct mesodermal heart ( elds that share a common origin appear to contribute cells to the developing heart in a temporally and spatially speci( c manner. The well-studied “( rst heart ( eld” (FHF) is derived from cells in the anterior lateral plate meso-derm, which align in a crescent shape at approximately embryonic day 7.5 (E7.5) in the mouse embryo, roughly corresponding to week 2 of human gestation (Fig. 10–1). By mouse E8.0, or 3 weeks in humans, these cells coalesce along the ventral midline to form a primitive heart tube that consists of an interior layer of endocardial cells and an exte-rior layer of myocardial cells, separated by the extracellular matrix necessary for reciprocal signaling between the two layers. The tubular heart initiates rhythmic contractions at about day 23 in humans.
Previous lineage tracings using dye-labeling techniques suggested that cells along the anterior–posterior (AP) axis of the heart tube were
destined to contribute to speci( c chambers of the future heart (reviewed in Srivastava and Olson, 2000). However, such studies could not determine the clonal contributions of individual cells (Meilhac et al., 2004). More recent studies using Cre-lox technologies to mark progenitor cells and all their descendents indicate—in stark contrast to previous models—that the heart tube derived from the FHF may predominantly provide a scaffold which enables a second population of cells to migrate and expand into cardiac chambers (Buckingham et al., 2005). These additional cells arise from an area often referred to as the “second heart ( eld (SHF)” or “anterior heart ( eld” based on its location anterior and medial to the crescent-shaped primary heart ( eld (Kelly et al., 2001; Mjaatvedt et al., 2001; Waldo et al., 2001; Fig. 10–1). Both heart ( elds appear to be regulated by complex posi-tive and negative signaling networks involving members of the bone morphogenetic protein (Bmp), sonic hedgehog (Shh), ( broblast growth factor (Fgf), Wnt and Notch proteins. Such signals often arise from the adjacent endoderm, although the precise nature and role of these sig-nals remain unknown (reviewed in Schultheiss et al., 1997; Marvin et al., 2001; Schneider and Mercola, 2001; Zaffran and Frasch, 2002). SHF cells remain in an undifferentiated progenitor state until incorporation into the heart, and this may in part be due to the closer proximity to inhibitory Wnt signals emanating from the midline. Recent work has raised the possibility that the Tbx18 may be required for the formation of a venous pole, which contributes portions of the atria and venous structures (Christoffels et al., 2006).
As the heart tube forms, the SHF cells migrate into the midline and position themselves dorsal to the heart tube in the pharyngeal meso-derm. Upon rightward looping of the heart tube, SHF cells cross the pharyngeal mesoderm into the anterior and posterior portions, popu-lating a large portion of the out* ow tract, future right ventricle and atria (Cai et al., 2003; Fig. 10–1). Precursors of the left ventricle are sparsely populated by the SHF and appear to be largely derived from the FHF. In contrast to the FHF, SHF cells do not differentiate into cardiac cells until they are positioned within the heart. Once within the heart, FHF and SHF cells appear to proliferate in response to endocar-dial-derived signals such as neuregulin and epicardial signals depen-dent on retinoic acid, although the mechanisms through which these noncell autonomous events occur remain poorly understood (Garratt et al., 2003; Stuckmann et al., 2003).
CARDIOMYOCYTE AND HEART TUBE FORMATION
Fruit* ies have a primitive heart-like structure known as the dorsal ves-sel that is analogous to the straight heart tube of the vertebrate embryo. It contracts rhythmically and pumps hemolymph through an open circulatory system. Formation of the dorsal vessel in * ies is depen-dent on a protein, tinman, whose name is based on the Wizard of Oz character that lacks a heart (Bodmer, 1993). Tinman belongs to the homeodomain family of proteins, and was initially described to play a role in establishing the regional identity of cells and organs during embryogenesis.
In contrast to the requirement of tinman for heart formation in * ies, its mammalian ortholog, Nkx2.5, is not essential for speci( cation of the cardiac lineage in mice, suggesting either that other genes may share functions with Nkx2.5 or that cardiogenesis in * ies and vertebrates dif-fers with respect to its dependence on this family of homeobox genes (Lyons et al., 1995; Tanaka et al., 1999). The possibility of functional
10-Epstein-Chap10.indd 12410-Epstein-Chap10.indd 124 8/21/2007 8:35:16 PM8/21/2007 8:35:16 PM

Molecular Regulation of Cardiogenesis 125
outer curvature of the heart (Biben and Harvey, 1997; Thomas et al., 1998). Remodeling of the inner curvature occurs, allowing migration of the in* ow tract to the right and out* ow tract to the left, facilitating proper alignment and separation of right- and left-sided circulations. Defects of inner curvature remodeling may underlie a host of human congenital heart malformations that involve improper alignment of the atria, ventricles and out* ow tract, and are often observed in the setting of abnormalities of left–right (LR) asymmetry. Other cardiac defects are a result of genetic defects that cause disruption of discrete devel-opmental events, making it useful to consider the molecular processes governing central morphogenetic aspects of cardiogenesis.
COMPLEX REGULATION OF CARDIAC MORPHOGENESIS
While the pathways regulating individual cell lineages contributing to the heart are deeply understood, the subsequent complex events involved in integrating multiple cell types, formation of chambers and patterning of the distinct regions of the heart are also being elucidated now. Some aspects of these morphogenetic events are described below, while others have been reviewed in depth elsewhere (Olson, 2004; Parmacek and Epstein, 2005; Srivastava, 2006). Notably, develop-ment of the cardiac electrical conduction system, derived in part from specialized cardiac muscle cells that respond to secreted signals from the vascular endothelium and endocardium (Gourdie et al., 1998; Rentschler et al., 2003), is an area not discussed here but which is essential to normal cardiac function (reviewed in Mikawa et al., 2003). The recent ( nding that Irx5-mediated regulation of key ion channels in the myocardium patterns the propagation wave of electrical activity highlights the importance of integration between specialized conduc-tion cells and the myocardium (Costantini et al., 2005).
DV PolarityConsistent with the “balloon” model of chamber formation described earlier, numerous genes, including the transcription factor Hand1 and the sarcomeric protein Serca2, are expressed speci( cally on the outer
redundancy between Nkx2.5 and other cardiac-expressed homeobox genes in vertebrates is supported by the ability of dominant-negative versions of Nkx2.5 to block cardiogenesis in frog and zebra( sh embryos (Fu et al., 1998; Grow and Krieg, 1998). Similarly, the transcriptional co-activator, myocardin, is necessary and suf( cient in frogs for cardiac gene expression, likely through the activation of serum response fac-tor (SRF)-dependent genes (Wang et al., 2001; Small et al., 2005). Combinations of these transcription factors along with Mef2, Gata, Hand, and Tbx family members appear to form core regulatory circuits that control early events during cardiogenesis (reviewed in Srivastava et al., 2006).
The cardiac out* ow tract (conotruncus) and parts of the right ven-tricle are the last segments to form and are derived from SHF cells as described earlier. The transcription factor, Tbx1, which appears to be a cause of cardiac and craniofacial disorders in humans (Lindsay et al., 1999; Jerome and Papaioannou, 2001; Lindsay et al., 2001; Merscher et al., 2001), is a major transcriptional regulator of the SHF and is necessary for proper development of conotruncal myocardium and Fgf secretion (Yamagishi et al., 2003; Hu et al., 2004; Xu et al., 2004). Islet1 (Isl1), a transcription factor involved in pancreatic devel-opment, also marks this population and is necessary for its develop-ment (Cai et al., 2003). Interestingly, Isl1-positive cells mark niches of cardiac progenitor cells in the postnatal heart (Laugwitz et al., 2005), suggesting that understanding the regulation of SHF-derived progeni-tor pools may be useful in developing approaches for cardiac repair.
In addition to the AP segmentation, a discrete dorsal–ventral (DV) polarity is present in the primitive heart tube. As the heart tube loops to the right, the ventral surface of the tube rotates, becoming the outer curvature of the looped heart with the dorsal surface forming the inner curvature. The outer curvature becomes the site of active growth, while remodeling of the inner curvature is essential for ulti-mate alignment of the in* ow and out* ow tracts of the heart. A model in which individual chambers “balloon” from the outer curvature in a segmental fashion has been proposed (Moorman and Christoffels, 2003). Consistent with this model, numerous genes, including the tran-scription factor Hand1, are expressed speci( cally on the ventral and
miR1-2miR1-1
BA
ht
h
av
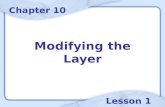
Figure 10–1. Illustration of cardiac development. Illustrations depict cardiac development, with morphologically related regions color-coded, seen from a ventral view. (A) Two distinct cardiogenic precursor ( elds form a crescent that is speci( ed to form speci( c regions of the heart tube (A, artery; V, ven-tricle), which is patterned to form the various regions and chambers of the looped and mature heart. (B) The secondary heart ( eld (SHF) contributes to much of the right ventricle and out* ow tract as the heart loops. (C) Each cardiac chamber balloons from the outer curvature of the looped heart tube in a segmental fashion. Neural crest cells populate the bilaterally symmetric
aortic arch arteries (III, IV, and VI) and aortic sac, which together contrib-ute to speci( c segments of the mature aortic arch, also color-coded. (C, D) Mesenchymal cells form the cardiac valves from the conotruncal (CT) and atrioventricular valve (AVV) segments, which divide into separate left- and right-sided valves. Corresponding days of human embryonic development are indicated. Ao, aorta; DA, ductus arteriosus; LA, left atrium; LCC, left common carotid; LSCA, left subclavian artery; LV, left ventricle; PA, pul-monary artery; RA, right atrium; RCC, right common carotid; RSCA, right subclavian artery; RV, right ventricle.
10-Epstein-Chap10.indd 12510-Epstein-Chap10.indd 125 8/21/2007 8:35:16 PM8/21/2007 8:35:16 PM

PATTERNS OF DEVELOPMENT126
and cause out* ow tract defects similar to those observed in humans (Hutson and Kirby, 2003). Embryos de( cient in cardiac neural crest cell migration or differentiation display a variety of cardiac out* ow tract and aortic arch defects resembling those in humans. These include tetralogy of Fallot, persistent truncus arteriosus, double-outlet right ventricle, ventricular septal defects and defects of aortic arch pat-terning. Thus, abnormalities in neural crest migration or differentia-tion likely underlie many of the conotruncal and aortic arch defects seen in humans. Indeed, human mutations of the neural crest–enriched transcription factor, TFAP2β result in persistent patency of the ductus arteriosus, a specialized aortic arch vessel essential for fetal cardiac physiology (Satoda et al., 2000; Fig. 10–1). It is likely that other genetic mutations affect speci( c regions of the aortic arch.
Disruption of SHF development by mutation of genes such as Tbx1, Fgf8, and Isl1 results in the defects similar to those observed with neural crest disruption, including persistent truncus arteriosus (failure of out* ow septation), malalignment of the out* ow tract of the heart with the ventricular chambers and ventricular septal defects (Jerome and Papaioannou, 2001; Abu-Issa et al., 2002; Frank et al., 2002; Cai et al., 2003). Since SHF-derived myocardial cells neighbor neural crest–derived cells and secrete growth factors such as Fgf8 in a Tbx1-dependent manner that in* uence neural crest cells (Hu et al., 2004), reciprocal interactions between the SHF- and neural crest–derived cells in the out* ow tract are likely essential for normal development. Consistent with this, humans with deletion or mutation of Tbx1 (Yagi et al., 2003), expressed in the SHF, appear to have cell-autonomous defects of SHF development and noncell-autonomous anomalies of neural crest–derived tissues. It will be interesting to determine if a large number of human cardiac out* ow tract defects is a direct result of SHF migration, differentiation or proliferation.
Cardiac Valve FormationAppropriate placement and function of cardiac valves is essential for chamber septation and for unidirectional * ow of blood through the heart. A molecular network involving Bmp2 and Tbx2 de( nes the position of the valves relative to the chambers (Harrelson et al., 2004; Beis et al., 2005; Ma et al., 2005). During early heart tube formation, “cushions” of extracellular matrix between the endocardium and myocardium presage valve formation at each end of the heart tube. Reciprocal signaling, mediated in part by transforming growth factor-βTGF-β family members, between the myocardium and endocardium in the cushion region induces a transformation of endocardial cells into mesenchymal cells that migrate into the extracellular matrix cushion (Brown et al., 1999; Kim et al., 2001; Gaussin et al., 2002). These mes-enchymal cells differentiate into the ( brous tissue of the valves and are involved in septation of the common atrioventricular canal into right- and left-sided ori( ces.
The Smad proteins are intracellular transcriptional mediators of sig-naling initiated by TGF-β ligands. Smad6 is speci( cally expressed in the atrioventricular cushions and out* ow tract during cardiogenesis, and is a negative regulator of TGF-β signaling. Targeted disruption of Smad6 in mice results in thickened and gelatinous atrioventricular and semilunar valves, comparable to those observed in human aortic and pulmonary valve disease (Galvin et al., 2000). Similarly, the absence of PTPN11, which encodes the protein tyrosine phosphatase Shp-2, results in dysplastic out* ow valves through its involvement in a signaling path-way mediated by epidermal growth factor receptor (Chen et al., 2000). The importance of PTPN11 in CHD was shown by the presence of point mutations in PTPN11 in patients with Noonan’s syndrome, who com-monly have pulmonic valve stenosis (Tartaglia et al., 2001). Finally, mice lacking Ephrin B2 also have thickened valves and, although the mechanism for this remains unclear, it will be interesting to determine how these signaling pathways intersect (Cowan et al., 2004).
In contrast to the thickened lea* ets described earlier, disruption of signaling pathways converging on the transcription factor Nfatc revealed a requirement of this calcium-activated regulator. Nfatc is expressed speci( cally in the forming embryonic valves, and targeted deletion of Nfatc in mice results in the absence of cardiac valve forma-tion (de la Pompa et al., 1998; Ranger et al., 1998). Signaling via the phosphatase, calcineurin results in nuclear translocation of Nfatc and
curvature of the heart (Biben and Harvey, 1997; Thomas et al., 1998). Also, through a complex transcriptional network, the unique identity of inner curvature cells is determined by Tbx2-mediated repression of genes typically found on the outer curvature (Harrelson et al., 2004). Another Tbox transcription factor, Tbx20, serves to repress Tbx2 activ-ity in the outer curvature as it expands into the cardiac chambers, thereby establishing the regional patterning of expanding or remodeling myo-cardium (Singh et al., 2005; Stennard et al., 2005; Takeuchi et al., 2005). Remodeling of the inner curvature allows migration of the in* ow tract to the right and the out* ow tract to the left, facilitating proper align-ment and separation of right- and left-sided circulations. In addition to its role in repressing Tbx2, Tbx20 affects expansion of both the FHF- and the SHF-derived cells and is necessary for out* ow tract development, possibly via regulation of Nkx2.5 and Mef2c (Takeuchi et al., 2005). Expansion of the ventricular chambers and the regulation of number of myocytes may also be regulated by the homeodomain-only protein, Hop, a downstream target of Nkx2.5 (Chen et al., 2002; Shin et al., 2002).
LR AsymmetryDefects of inner curvature remodeling may underlie a host of human congenital heart malformations that involve improper alignment of the atria, ventricles and out* ow tract. These include situations where both atrioventricular valves empty into the left ventricle (double-inlet left ventricle), or when the aorta and pulmonary artery both exit from the right ventricle (double-outlet right ventricle), similar to those observed in many mutant mouse models (reviewed in Kathiriya and Srivastava, 2000; Franco and Campione, 2003). Such defects are often observed in the setting of abnormalities of LR asymmetry determination. Thus, LR decisions may affect not only the direction of cardiac looping but also the proper alignment of chambers, likely through the regulation of gene expression along the inner versus outer curvature and ventral versus dorsal surface of the developing heart.
The elegant molecular network regulating LR asymmetry of the body plan has been reviewed (Palmer, 2004) and will not be summarized here. However, it is worth highlighting several clues about the rela-tionship between LR asymmetry and proper alignment of the cardiac chambers. The cascade of LR signals, including Shh and Nodal, con-verge on the transcription factor Pitx2 (Piedra et al., 1998). Pitx2 is initially LR asymmetric in the linear heart tube, but this asymmetry is translated into a DV polarity in the looped heart tube. Because Pitx2 regulates cell proliferation via cyclin D2 and also controls cell migra-tion events (Kioussi et al., 2002), it is a potential link between the signals regulating the direction and process of cardiac looping. Within certain subdomains, regulation of Pitx2 by Tbx1 integrates the tran-scriptional pathways controlling morphogenesis and LR asymmetry (Nowotchin et al., 2006).
Cardiac Outfl ow Tract RegulationCongenital cardiac defects involving the cardiac out* ow tract, aortic arch, ductus arteriosus and proximal pulmonary arteries account for 20%–30% of all CHD. This region of the heart undergoes extensive and rather complex morphogenetic changes with contributions from neural crest cells and the SHF, as discussed earlier. Mesenchymal cells originating from the crest of the neural folds are essential for proper septation and remodeling of the out* ow tract and aortic arch (reviewed in Hutson and Kirby, 2003). Such neural crest–derived cells migrate away from the neural folds and retain the ability to differentiate into multiple cell types. The migratory path and ultimate fate of these cells depends on their relative position of origin along the AP axis and are partly regulated by the Hox code (LeDourin et al., 2004). Neural crest cells differentiate and contribute to diverse embryonic structures, including the cranial ganglia, peripheral nervous system, adrenal glands and melanocytes. Neural crest cells that arise from the otic pla-code to the third somite migrate through the developing pharyngeal arches and populate the mesenchyme of each of the aortic arch arter-ies and the mesenchyme necessary to septate the out* ow tract septum (Fig. 10–1). Because of their migratory path and role, this segment of the neural crest is often referred to as the cardiac neural crest.
Mutations in many signaling cascades affect neural crest migration or development, including the endothelin and semaphorin pathways,
10-Epstein-Chap10.indd 12610-Epstein-Chap10.indd 126 8/21/2007 8:35:19 PM8/21/2007 8:35:19 PM

Molecular Regulation of Cardiogenesis 127
structural motifs in the protein. One potential cofactor is NKX2-5, as the two physically interact and cooperate to activate common target genes (Hiroi et al., 2001).
Like the NKX2.5 and TBX5 mutations, mutations in the zinc- ( nger-containing protein GATA4 cause similar atrial and ventricular septal defects in autosomal dominant nonsyndromic human pedi-grees (Garg et al., 2003). GATA4 or related proteins are essential for cardiogenesis in * ies, ( sh, and mice (Kuo et al., 1997; Molkentin et al., 1997; Gajewski et al., 2001; Reiter et al., 2001). Like NKX2.5, GATA4 and TBX5 also form a complex to regulate downstream genes, such as myosin heavy chain (MHC). Consistent with an important role for such combinatorial interactions, a familial GATA4 point mutation disrupts GATA4’s ability to interact with TBX5 (Garg et al., 2005). Conversely, several human TBX5 mutations disrupt TBX5 interaction with GATA4, suggesting that the two cooperate in cardiac septation events (Garg et al., 2003). Con( rming a genetic interaction between the two proteins, mice heterozygous for Gata4 and Tbx5 are embryonic lethal from a myocardial defect and severe hypoplasia of the endocar-dial cushion tissue necessary for valvuloseptal development (V. Garg and D. Srivastava, unpublished observations). GATA4, TBX5, and NKX2-5 may form a common complex that is necessary for proper cardiac septation. Disruption of any one of the three proteins or their interactions can result in atrial or ventricular septal defects. Although the compendium of septal genes regulated by these transcription fac-tors is unknown, it is intriguing that mutations in human MHC, a direct target of GATA4, TBX5, and NKX2-5, also cause atrial septal defects (Ching et al., 2005). This observation suggests a possible mechanism by which these genes cause septation defects.
microRNA REGULATION OF CARDIOMYOCYTE DIFFERENTIATION
While transcriptional and epigenetic events regulate many critical cardiac genes, translational control by small noncoding RNAs, such as microRNAs (miRNAs), has recently emerged as another mechanism to “( ne-tune” dosages of key proteins during cardiogenesis (Kwon et al., 2005; Zhao et al., 2005). miRNAs are genomically encoded 20–22 nucleotide RNAs that target messenger RNAs (mRNAs) for translational inhibition or degradation by many of the same pathways as small interfer-ing RNA (siRNA) (Ambros, 2004; He and Hannon, 2004). More than 400 human miRNAs have been identi( ed (Cummins et al., 2006), but in only a few cases are the biological function and mRNA targets known.
The miRNA-1 family (miR-1-1 and miR-1-2) is highly conserved from worms to humans and is speci( cally expressed in the develop-ing cardiac and skeletal muscle progenitor cells as they differentiate
is similarly involved in cardiac valve formation, in part through the regulation of vascular endothelial growth factor (Vegf) expression in the endocardium (Chang et al., 2004).
The Notch signaling pathway is required for cell fate and differ-entiation decisions throughout the embryo (Artavanis-Tsakonas et al., 1999), but only recently have Notch proteins been implicated in vertebrate cardiac development. In ( sh and frogs, Notch appears to be involved in the development of endocardial cushions that contribute to valve tissue (Timmerman et al., 2004). In humans, heterozygous NOTCH1 mutations disrupt normal development of the aortic valve and, occasionally, the mitral valve (Garg et al., 2005). The severity of valve disease associated with NOTCH1 mutations in humans varies widely from the mild disease in which the aortic valve has two, rather than three, lea* ets (bicuspid aortic valve) to the severe defects in valve patency in utero, resulting in left ventricular growth failure. Consistent with this genetic ( nding, 15% of “normal” relatives of children with hypoplastic left heart syndrome (HLHS) have subclinical bicuspid aortic valves (Cripe et al., 2004; Loffredo et al., 2004), suggesting that disruption of the NOTCH signaling cascade may underlie a spec-trum of aortic valve disease. While not speci( cally affecting valves, human mutations in JAGGED1, a NOTCH ligand, also cause out* ow tract defects associated with the autosomal dominant disease, Alagille syndrome (Li et al., 1997; Oda et al., 1997; Krantz et al., 1999). The hairy-related family of transcriptional repressors (Hrt1, Hrt2, and Hrt3) may mediate the Notch signal during valve and myocardial development; however, their targets for repression remain unknown (Nakagawa et al., 1999; reviewed in Kokubo et al., 2005).
MOLECULAR REGULATION OF SEPTAL FORMATION
Recent ( ndings with the cardiac transcription factors NKX2.5, TBX5, and GATA4 exemplify the synergy between human genetics and stud-ies of model organisms for understanding the etiology of human CHD. Numerous point mutations have been identi( ed in Nkx2.5 in families with atrial septal defects and progressive cardiac conduction abnormal-ities (Schott et al., 1998). Retrospective analysis of mice heterozygous for Nkx2.5 disruption revealed a similar phenotype and progressive apoptotic loss of conduction cells, suggesting a likely mechanism for the human phenotype (Biben et al., 2000; Jay et al., 2004).
Humans with Holt–Oram syndrome caused by mutations in Tbx5 have cardiac anomalies, similar to those with Nkx2.5 mutations (atrial and ventricular septal defects), as well as limb abnormalities (Basson et al., 1997; Mori and Bruneau, 2004). Intriguingly, muta-tions responsible for defects in the heart and limbs are clustered in dif-ferent regions of the protein, suggesting that TBX5 engages different downstream genes or cofactors in these tissues that depend on unique
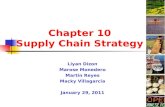
Figure 10–2. miR-1-1 and miR-1-2 enhancer-driven lacZ expression. The expression patterns of miR-1-1 (A) and miR-1-2 (B) are demonstrated by the β-gal (blue) staining in embryonic day 11.5 mouse embryos. h, head; ht, heart; arrowhead indicates somites.
10-Epstein-Chap10.indd 12710-Epstein-Chap10.indd 127 8/21/2007 8:35:20 PM8/21/2007 8:35:20 PM

PATTERNS OF DEVELOPMENT128
well-understood organs in biology. This knowledge is now being used to discover the underlying genetics of CHD and the basis for many adult-onset diseases that have their origin in the mutations of developmental genes. What remains lacking is a coherent picture of the hierarchical pathways that govern most developmental processes and the mechanisms through which such pathways regulate the cell biology of morphogenesis. Such knowledge will require a better understanding of the target genes of critical transcriptional and signaling pathways that control cardiogenesis. This will be an essential step as the targets will be the most amenable sites of intervention, both in a therapeutic sense and for prevention. For exam-ple, the identi( cation of dietary substances, such as the folic acid used to prevent neural tube defects, that modulate key developmental pathways will be necessary for preventive efforts. In addition, genetic identi( cation of those at risk for adult-onset disease, which has its origin in a cardiac developmental defect such as the age-related calci( cation that occurs in bicuspid aortic valve, will provide ample time for intervention to slow the progression of disease. The convergence of addition developmental knowledge and improved genetic tools should make this vision a reality in the coming years.
ACKNOWLEDGMENTSThe authors thank B. Taylor for editorial assistance. V.N. is supported by an NIH T32 grant; D.S. is supported by grants from NHLBI/NIH, March of Dimes Birth Defects Foundation, and is an Established Investigator of the American Heart Association.
ReferencesAbu-Issa R, Smyth G, Smoak I, Yamamura K, Meyers EN (2002). Fgf8 is required for pharyn-geal arch and cardiovascular development in the mouse. Development 129: 4613–4625.
Artavanis-Tsakonas S, Rand MD, Lake RJ (1999). Notch signaling: cell fate control and signal integration in development. Science 284: 770–776.
Basson CT, Bachinsky DR, Lin RC, Levi T, Elkins JA, Soults J, Grayzel D, Kroumpouzou E, Traill TA, Leblanc-Straceski J, et al. (1997). Mutations in human TBX5 cause limb and cardiac malformation in Holt-Oram syndrome. Nat Genet 15: 30–35.
Biben C, Harvey RP (1997). Homeodomain factor Nkx2-5 controls left/right asymmet-ric expression of bHLH gene eHand during murine heart development. Genes Dev 11: 1357–1369.
Bodmer R (1993). The gene tinman is required for speci( cation of the heart and visceral muscles in Drosophila. Development 118: 719–729.
Buckingham M, Meilhac S, Zaffran S (2005). Building the mammalian heart from two sources of myocardial cells. Nat Rev Genet 6: 826–835.
Cai CL, Liang X, Shi Y, Chu PH, Pfaff SL, Chen J, Evans S (2003). Isl1 identi( es a cardiac progenitor population that proliferates prior to differentiation and contributes a majority of cells to the heart. Dev Cell 5: 877–889.
Chen B, Bronson RT, Klaman LD, Hampton TG, Wang JF, Green PJ, Magnuson T, Douglas PS, Morgan JP, Neel BG (2000). Mice mutant for Egfr and Shp2 have defective cardiac semilunar valvulogenesis. Nat Genet 24: 296–299.
Chien KR, Olson EN (2002). Converging pathways and principles in heart development and disease: CV@CSH. Cell 110: 153–162.
Christoffels VM, Mommersteeg MT, Trowe MO, Prall OW, de Gier-de Vries C, Soufan AT, Bussen M, Schuster-Gossler K, Harvey RP, Moorman AF, et al. (2006). Formation of the venous pole of the heart from an Nkx2-5-negative precursor population requires Tbx18. Circ Res 98: 1555–1563.
Cohen LS, Friedman JM, Jefferson JW, Johnson EM, Weiner ML (1994). A reevaluation of risk of in utero exposure to lithium. JAMA 271: 146–150.
Costantini DL, Arruda EP, Agarwal P, Kim K-H, Zhu Y, Lebel M, Cheng CW, Park CY, Pierce S, Guerchicoff A, et al. (2005). The homeodomain transcription factor Irx5 estab-lishes the mouse cardiac ventricular repolarization gradient. Cell 123: 347–358.
Cowan CA, Yokoyama N, Saxena A, Chumley MJ, Silvany RE, Baker LA, Srivastava D, Henkemeyer M (2004). Ephrin-B2 reverse signaling is required for axon path( nding and cardiac valve formation but not early vascular development. Dev Biol 271: 263–271.
Cripe L, Andel( nger G, Martin LJ, Shooner K, Benson DW (2004). Bicuspid aortic valve is heritable. J Am Coll Cardiol 44: 138–143.
de la Pompa JL, Timmerman LA, Takimoto H, Yoshida H, Elia AJ, Samper E, Potter J, Wakeham A, Marengere L, Langille BL, et al. (1998). Role of the NF-ATc transcription factor in morphogenesis of cardiac valves and septum. Nature 392: 182–186.
Franco D, Campione M (2003). The role of Pitx2 during cardiac development. Linking left-right signaling and congenital heart diseases. Trends Cardiovasc Med 13: 157–163.
Frank DU, Fotheringham LK, Brewer JA, Muglia LJ, Tristani-Firouzi M, Capecchi MR, Moon AM (2002). An Fgf8 mouse mutant phenocopies human 22q11 deletion syndrome. Development 129: 4591–4603.
Fu Y, Yan W, Mohun TJ, Evans SM (1998). Vertebrate tinman homologues XNkx2-3 and XNkx2-5 are required for heart formation in a functionally redundant manner. Development 125: 4439–4449.
Gajewski K, Zhang Q, Choi CY, Fossett N, Dang A, Kim YH, Kim Y, Schulz RA (2001). Pannier is a transcriptional target and partner of Tinman during Drosophila cardiogen-esis. Dev Biol 233: 425–436.
Galvin KM, Donovan MJ, Lynch CA, Meyer RI, Paul RJ, Lorenz JN, Fairchild-Huntress V, Dixon KL, Dunmore JH, Gimbrone MA Jr, et al. (2000). A role for smad6 in develop-ment and homeostasis of the cardiovascular system. Nat Genet 24: 171–174.
AQ1
(Zhao et al., 2005). Enrichment of miR-1-1 is initially observed in the atrial precursors before becoming ubiquitous in the heart, while miR-1-2 is speci( c for the ventricle throughout development, sug-gesting that the two may have chamber-speci( c effects in vivo. Both are highly expressed in the SHF-derived cells of the cardiac out* ow tract (Fig. 10–2). Interestingly, expression of these miRNAs is directly controlled by well-studied transcriptional regulatory networks that promote muscle differentiation. Cardiac expression is dependent on SRF, and skeletal muscle expression requires the myogenic transcrip-tion factors, MyoD and Mef2. SRF recruits the potent co-activator, myocardin, to cardiac and smooth muscle–speci( c genes that control differentiation (Wang et al., 2001). Consistent with a role in differen-tiation, overexpression of miR-1 in the developing mouse heart results in a decrease in ventricular myocyte expansion, with fewer proliferat-ing cardiomyocytes remaining in the cell cycle. In vivo validation of Hand2, a transcription factor that regulates ventricular expansion, as a miR-1 target suggests that tight regulation of Hand2 protein levels may be involved in controlling the balance between cardiomyocyte proliferation and differentiation. Disruption of the single * y ortholog of miR-1 had catastrophic consequences resulting in uniform lethality at embryonic or larval stages with a frequent defect in maintaining cardiac gene expression (Kwon et al., 2005). In a subset of * ies lacking miR-1, a severe defect of cardiac progenitor cell differentiation pro-vided loss-of-function evidence that miR-1 was involved in muscle dif-ferentiation events, similar to the gain-of-function ( ndings in mice.
ENVIRONMENTAL FACTORS ASSOCIATED WITH CHD
A number of maternal conditions and/or exposures have been associ-ated with congenital cardiac defects. We will brie* y highlight a few examples of maternal in* uences below.
Both maternal systemic lupus erythematosus and diabetes mellitus have well-established linkages to congenital heart defects. Maternal systemic lupus is a cause of congenital heart block. The proposed pathophysiology is that maternal anti-Ro or anti-La antibodies cross the placenta and damage the fetal cardiac conduction system, espe-cially the atrioventricular node. On the other hand, the mechanism by which maternal diabetes mellitus causes congenital heart defects is not clear. In a review of the Baltimore–Washington Infant Study, a large population-based study of CHD, maternal diabetes was associated with increased incidence of congenital heart defects, including ventricular septal defects, out* ow tract abnormalities, and cardiac hypertrophy (Loffredo et al., 2001). One hypothesized mechanism for the struc-tural defects is that hyperglycemia represses VEGF expression, thereby disrupting proper formation of the endocardial cushions (reviewed in Pinter et al., 2001; Enciso et al., 2003; Armstrong and Bischoff, 2004). The cardiac hypertrophy may involve excess glycogen deposition; how-ever, a recent study reported increased expression of genes associated with cardiac hypertrophy, including cardiac actin and myosin, in the offspring of hyperglycemic rats (Gopinath et al., 2005).
Exposure to an extensive list of medications and illicit drugs, espe-cially during the ( rst trimester, has also been linked to cardiac defects. Based upon a retrospective study, in utero lithium exposure was linked to increased incidence of Ebstein’s anomaly, a malformation of the tri-cuspid valve. However, several prospective studies have raised questions about the degree of risk posed by lithium exposure (Zalzstein et al., 1990; Jacobson et al., 1992; Cohen et al., 1994). Experiments in chick embryos suggest that lithium may cause defects by inappropriate activa-tion of the Wnt signaling pathway (Klein and Melton, 1996; Manisastry et al., 2006). In addition, ethanol exposure during critical periods of car-diogenesis may also contribute, as children with fetal alcohol syndrome often have ventricular septal defects. While it is dif( cult to assign the risk to environmental agents because only those genetically at risk are likely to be affected, the teratogenic effects of medications and drugs are prob-ably greatest during the ( rst trimester when organogenesis is occurring.
SUMMARY
Over the last decade, we have seen remarkable advances in our under-standing of cardiogenesis, and the heart has become one of the most
10-Epstein-Chap10.indd 12810-Epstein-Chap10.indd 128 8/21/2007 8:35:23 PM8/21/2007 8:35:23 PM

Molecular Regulation of Cardiogenesis 129
Oda T, Elkahloun AG, Pike BL, Okajima K, Krantz ID, Genin A, Piccoli DA, Meltzer PS, Spinner NB, Collins FS, et al. (1997). Mutations in the human Jagged1 gene are respon-sible for Alagille syndrome. Nat Genet 16: 235–242.
Palmer AR (2004). Symmetry breaking and the evolution of development. Science 306: 828–833.
Piedra ME, Icardo JM, Albajar M, Rodriguez-Rey JC, Ros MA (1998). Pitx2 participates in the late phase of the pathway controlling left-right asymmetry. Cell 94: 319–324.
Ranger AM, Grusby MJ, Hodge MR, Gravallese EM, de la Brousse FC, Hoey T, Mickanin C, Baldwin HS, Glimcher LH (1998). The transcription factor NF-ATc is essential for cardiac valve formation. Nature 392: 186–190.
Reiter JF, Kikuchi Y, Stainier DY (2001). Multiple roles for Gata5 in zebra( sh endoderm formation. Development 128: 125–135.
Rentschler S, Morley GE, Fishman GI (2003). Patterning of the mouse conduction system. Novartis Found Symp 250: 194–205; discussion 205–209, 276–279.
Satoda M, Zhao F, Diaz GA, Burn J, Goodship J, Davidson HR, Pierpont ME, Gelb BD (2000). Mutations in TFAP2B cause Char syndrome, a familial form of patent ductus arteriosus. Nat Genet 25: 42–46.
Schneider VA, Mercola M (2001). Wnt antagonism initiates cardiogenesis in Xenopus lae-vis. Genes Dev 15: 304–315.
Schott JJ, Benson DW, Basson CT, Pease W, Silberbach GM, Moak JP, Maron BJ, Seidman CE, Seidman JG (1998). Congenital heart disease caused by mutations in the transcrip-tion factor NKX2-5. Science 281: 108–111.
Schultheiss TM, Burch JB, Lassar AB (1997). A role for bone morphogenetic proteins in the induction of cardiac myogenesis. Genes Dev 11: 451–462.
Singh MK, Petry M, Haenig B, Lescher B, Leitges M, Kispert A (2005). The T-box tran-scription factor Tbx15 is required for skeletal development. Mech Dev 122: 131–144.
Small EM, Warkman AS, Wang DZ, Sutherland LB, Olson EN, Krieg PA (2005). Myocardin is suf( cient and necessary for cardiac gene expression in Xenopus. Development 132: 987–997.
Srivastava D (2004). Heart disease: an ongoing genetic battle? Nature 429: 819–822.Srivastava D (2006). Making or breaking the heart: from lineage determination to mor-phogenesis. Cell 126: 1037–1048.
Srivastava D, Olson EN (2000). A genetic blueprint for cardiac development. Nature 407: 221–226.
Stennard FA, Costa MW, Lai D, Biben C, Furtado MB, Solloway MJ, McCulley DJ, Leimena C, Preis JI, Dunwoodie SL, et al. (2005). Murine T-box transcription factor Tbx20 acts as a repressor during heart development, and is essential for adult heart integ-rity, function and adaptation. Development 132: 2451–2462.
Stuckmann I, Evans S, Lassar AB (2003). Erythropoietin and retinoic acid, secreted from the epicardium, are required for cardiac myocyte proliferation. Dev Biol 255: 334–349.
Takeuchi JK, Mileikovskaia M, Koshiba-Takeuchi K, Heidt AB, Mori AD, Arruda EP, Gertsenstein M, Georges R, Davidson L, Mo R, et al. (2005). Tbx20 dose-dependently regulates transcription factor networks required for mouse heart and motoneuron devel-opment. Development 132: 2463–2474.
Tanaka M, Wechsler SB, Lee IW, Yamasaki N, Lawitts JA, Izumo S (1999). Complex modular cis-acting elements regulate expression of the cardiac specifying homeobox gene Csx/Nkx2.5. Development 126: 1439–1450.
Tartaglia M, Mehler EL, Goldberg R, Zampino G, Brunner HG, Kremer H, van der Burgt I, Crosby AH, Ion A, Jeffery S, et al. (2001). Mutations in PTPN11, encoding the protein tyrosine phosphatase SHP-2, cause Noonan syndrome. Nat Genet 29: 465–468.
Thomas T, Kurihara H, Yamagishi H, Kurihara Y, Yazaki Y, Olson EN, Srivastava D (1998). A signaling cascade involving endothelin-1, dHAND and msx1 regulates development of neural-crest-derived branchial arch mesenchyme. Development 125: 3005–3014.
Timmerman LA, Grego-Bessa J, Raya A, Bertran E, Perez-Pomares JM, Diez J, Aranda S, Palomo S, McCormick F, Izpisua-Belmonte JC, et al. (2004). Notch promotes epithe-lial-mesenchymal transition during cardiac development and oncogenic transformation. Genes Dev 18: 99–115.
Waldo KL, Kumiski DH, Wallis KT, Stadt HA, Hutson MR, Platt DH, Kirby ML (2001). Conotruncal myocardium arises from a secondary heart ( eld. Development 128: 3179–3188.
Wang D, Chang PS, Wang Z, Sutherland L, Richardson JA, Small E, Krieg PA, Olson EN (2001). Activation of cardiac gene expression by myocardin, a transcriptional cofactor for serum response factor. Cell 105: 851–862.
Xu H, Morishima M, Wylie JN, Schwartz RJ, Bruneau BG, Lindsay EA, Baldini A (2004). Tbx1 has a dual role in the morphogenesis of the cardiac out* ow tract. Development 131: 3217–3227.
Yagi H, Furutani Y, Hamada H, Sasaki T, Asakawa S, Minoshima S, Ichida F, Joo K, Kimura M, Imamura S, et al. (2003). Role of TBX1 in human del22q11.2 syndrome. Lancet 362: 1366–1373.
Yamagishi H, Maeda J, Hu T, McAnally J, Conway SJ, Kume T, Meyers EN, Yamagishi C, Srivastava D (2003). Tbx1 is regulated by tissue-speci( c forkhead proteins through a common Sonic hedgehog-responsive enhancer. Genes Dev 17: 269–281.
Zaffran S, Frasch M (2002). Early signals in cardiac development. Circ Res 91: 457–469.Zalzstein E, Koren G, Einarson T, Freedom RM (1990). A case-control study on the asso-ciation between ( rst trimester exposure to lithium and Ebstein’s anomaly. Am J Cardiol 65: 817–818.
Zhao Y, Samal E, Srivastava D (2005). Serum response factor regulates a muscle-speci( c mircroRNA that targets Hand2 during cardiogenesis. Nature 436: 214–220.
Garg V, Kathiriya IS, Barnes R, Schluterman MK, King IN, Butler CA, Rothrock CR, Eapen RS, Hirayama-Yamada K, Joo K, et al. (2003). GATA4 mutations cause human congenital heart defects and reveal an interaction with TBX5. Nature 424: 443–447.
Garg V, Muth AN, Ransom JF, Schluterman MK, Barnes R, King IN, Grossfeld PD, Srivastava D (2005). Mutations in NOTCH1 cause aortic valve disease. Nature 437: 270–274.
Garratt AN, Ozcelik C, Birchmeier C (2003). ErbB2 pathways in heart and neural dis-eases. Trends Cardiovasc Med 13: 80–86.
Gourdie RG, Wei Y, Kim D, Klatt SC, Mikawa T (1998). Endothelin-induced conversion of embryonic heart muscle cells into impulse-conducting Purkinje ( bers. Proc Natl Acad Sci USA 95: 6815–6818.
Grow MW, Krieg PA (1998). Tinman function is essential for vertebrate heart develop-ment: elimination of cardiac differentiation by dominant inhibitory mutants of the tin-man-related genes, XNkx2-3 and XNkx2-5. Dev Biol 204: 187–196.
Hoffman JI, Kaplan S (2002). The incidence of congenital heart disease. J Am Coll Cardiol 39: 1890–1900.
Hu T, Yamagishi H, Maeda J, McAnally J, Yamagishi C, Srivastava D (2004). Tbx1 regu-lates ( broblast growth factors in the anterior heart ( eld through a reinforcing autoregula-tory loop involving forkhead transcription factors. Development 131: 5491–5502.
Hutson MR, Kirby ML (2003). Neural crest and cardiovascular development: a 20-year perspective. Birth Defects Res C Embryo Today 69: 2–13.
Jacobson SJ, Jones K, Johnson K, Ceolin L, Kaur P, Sahn D, Donnenfeld AE, Rieder M, Santelli R, Smythe J, et al. (1992). Prospective multicentre study of pregnancy outcome after lithium exposure during ( rst trimester. Lancet 339: 530–533.
Jerome LA, Papaioannou VE (2001). DiGeorge syndrome phenotype in mice mutant for the T-box gene, Tbx1. Nat Genet 27: 286–291.
Kathiriya IS, Srivastava D (2000). Left-right asymmetry and cardiac looping: implications for cardiac development and congenital heart disease. Am J Med Genet 97: 271–279.
Kelly RG, Brown NA, Buckingham ME (2001). The arterial pole of the mouse heart forms from Fgf10-expressing cells in pharyngeal mesoderm. Dev Cell 1: 435–440.
Kioussi C, Briata P, Baek SH, Rose DW, Hamblet NS, Herman T, Ohgi KA, Lin C, Gleiberman A, Wang J, et al. (2002). Identi( cation of a Wnt/Dvl/beta-Catenin --> Pitx2 pathway mediating cell-type-speci( c proliferation during development. Cell 111: 673–685.
Krantz ID, Smith R, Colliton RP, Tinkel H, Zackai EH, Piccoli DA, Goldmuntz E, Spinner NB (1999). Jagged1 mutations in patients ascertained with isolated congenital heart defects. Am J Med Genet 84: 56–60.
Kuo CT, Morrisey EE, Anandappa R, Sigrist K, Lu MM, Parmacek MS, Soudais C, Leiden JM (1997). GATA4 transcription factor is required for ventral morphogenesis and heart tube formation. Genes Dev 11: 1048–1060.
Kwon C, Han Z, Olson EN, Srivastava D (2005). MicroRNA1 in* uences cardiac differ-entiation in Drosophila and regulates Notch signaling. Proc Natl Acad Sci USA 102: 18986–18991.
Laugwitz KL, Moretti A, Lam J, Gruber P, Chen Y, Woodard S, Lin LZ, Cai CL, Lu MM, Reth M, et al. (2005). Postnatal isl1+ cardioblasts enter fully differentiated cardiomyo-cyte lineages. Nature 433: 647–653.
Li L, Krantz ID, Deng Y, Genin A, Banta AB, Collins CC, Qi M, Trask BJ, Kuo WL, Cochran J, et al. (1997). Alagille syndrome is caused by mutations in human Jagged1, which encodes a ligand for Notch1. Nat Genet 16: 243–251.
Lindsay EA, Botta A, Jurecic V, Carattini-Rivera S, Cheah YC, Rosenblatt HM, Bradley A, Baldini A (1999). Congenital heart disease in mice de( cient for the DiGeorge syn-drome region. Nature 401: 379–383.
Lindsay EA, Vitelli F, Su H, Morishima M, Huynh T, Pramparo T, Jurecic V, Ogunrinu G, Sutherland HF, Scambler PJ, et al. (2001). Tbx1 haploinsuf( ciency in the DiGeorge syndrome region causes aortic arch defects in mice. Nature 410: 97–101.
Loffredo CA, Chokkalingam A, Sill AM, Boughman JA, Clark EB, Scheel J, Brenner JI (2004). Prevalence of congenital cardiovascular malformations among relatives of infants with hypoplastic left heart, coarctation of the aorta, and d-transposition of the great arteries. Am J Med Genet A 124: 225–230.
Lyons I, Parsons LM, Hartley L, Li R, Andrews JE, Robb L, Harvey RP (1995). Myogenic and morphogenetic defects in the heart tubes of murine embryos lacking the homeo box gene Nkx2-5. Genes Dev 9: 1654–1666.
Marvin MJ, Di Rocco G, Gardiner A, Bush SM, Lassar AB (2001). Inhibition of Wnt activ-ity induces heart formation from posterior mesoderm. Genes Dev 15: 316–327.
Meilhac SM, Esner M, Kelly RG, Nicolas JF, Buckingham ME (2004). The clonal ori-gin of myocardial cells in different regions of the embryonic mouse heart. Dev Cell 6: 685–698.
Merscher S, Funke B, Epstein JA, Heyer J, Puech A, Lu MM, Xavier RJ, Demay MB, Russell RG, Factor S, et al. (2001). TBX1 is responsible for cardiovascular defects in velo-cardio-facial/DiGeorge syndrome. Cell 104: 619–629.
Mjaatvedt CH, Nakaoka T, Moreno-Rodriguez R, Norris RA, Kern MJ, Eisenberg CA, Turner D, Markwald RR (2001). The out* ow tract of the heart is recruited from a novel heart-forming ( eld. Dev Biol 238: 97–109.
Molkentin JD, Lin Q, Duncan SA, Olson EN (1997). Requirement of the transcription factor GATA4 for heart tube formation and ventral morphogenesis. Genes Dev 11: 1061–1072.
Moorman AF, Christoffels VM (2003). Cardiac chamber formation: development, genes, and evolution. Physiol Rev 83: 1223–1267.
Mori AD, Bruneau BG (2004). TBX5 mutations and congenital heart disease: Holt-Oram syndrome revealed. Curr Opin Cardiol 19: 211–215.
AQ1: Did you mean “additional”?
10-Epstein-Chap10.indd 12910-Epstein-Chap10.indd 129 8/21/2007 8:35:23 PM8/21/2007 8:35:23 PM