10 Ferrara Ring for ectasia after refractive surgery
5
Click here to load reader
-
Upload
ferrara-ophthalmics -
Category
Health & Medicine
-
view
49 -
download
0
Transcript of 10 Ferrara Ring for ectasia after refractive surgery

ARTICLE
Intrastromal corneal rin
g segment implantationfor ectasia after refractive surgeryLeonardo Torquetti, MD, PhD, Paulo Ferrara, MD, PhD
SubmittFinal revAccepte
From a
Additionthe Ferr
CorrespClinic, CBelo Hocom.br.
Q
P
986
ed: Octision sd: Dece
private
al finanara intr
ondingontornrizonte
2010 A
ublished
PURPOSE: To evaluate the clinical outcomes of implantation of Ferrara intrastromal corneal ringsegments (ICRS) in patients with corneal ectasia after refractive surgery.
SETTING: Private clinic, Belo Horizonte, Brazil.
METHODS: Charts of patients with corneal ectasia after refractive surgery were retrospectivelyreviewed. The following parameters were studied: uncorrected distance visual acuity (UDVA),corrected distance visual acuity (CDVA), keratometry, corneal asphericity, and pachymetry. Allpatients were evaluated by Scheimpflug scanning-slit tomography (Pentacam).
RESULTS: Charts of 25 eyes (20 patients) with corneal ectasia (20 after laser in situ keratomileusis,4 after radial keratotomy, 1 after photorefractive keratectomy) were reviewed. Postoperatively, themean UDVA increased from 20/185 to 20/66 (P Z .005) and the mean CDVA, from 20/125 to 20/40(P Z .008). The mean asphericity decreased from �0.95 preoperatively to �0.23 postoperatively(P Z .006). The mean pachymetry at the apex of the cornea increased from 457.7 mm G 48.7 (SD)preoperatively to 466.2 G 49.8 mm postoperatively (P Z .025) and the mean pachymetry at thethinnest point, from 436.3 G 46.2 mm to 453.9 G 49.3 mm (P Z .000). The mean keratometrydecreased from 45.41 G 5.63 diopters (D) to 42.88 G 4.44 D, respectively; the decrease wasstatistically significant (P Z .000).
CONCLUSION: Intrastromal corneal ring segment implantation significantly improved UDVA andCDVA in patients with corneal ectasia.
Financial Disclosure: Dr. Torquetti has no financial or proprietary interest in any material or methodmentioned. Additional disclosures are found in the footnotes.
J Cataract Refract Surg 2010; 36:986–990 Q 2010 ASCRS and ESCRS
Corneal ectasia is an infrequent but potentially seriouscomplication of refractive surgery and occurs morecommonly after laser in situ keratomileusis(LASIK).1–3 After LASIK, the cornea is structurallyweakened, not only by the laser central stromal abla-tion but also by the creation of the flap. The cornea
ober 16, 2009.ubmitted: December 10, 2009.mber 10, 2009.
clinic, Belo Horizonte, Brazil.
cial disclosuce: Dr. Ferrara has a financial interest inastromal cornea ring.
author: Paulo Ferrara, MD, PhD, Paulo Ferrara Eyeo Avenida 4747, Suite 615, Lifecenter, Funcionarios,MG 30110-031, Brazil. E-mail: pferrara@ferrararing.
SCRS and ESCRS
by Elsevier Inc.
may assume an irregular conical shape, and this leadsto a decrease in visual acuity secondary to high irreg-ular astigmatism, as occurs in primary ectatic cornealdisorders such as keratoconus.4,5
Even though corneal ectasia is relatively rare afterLASIK, it can have a profoundly negative effect onthe refractive properties of the cornea. The cause andthe biomechanical changes that induce keratectasiaafter refractive surgery are unknown. The cause ofcorneal ectasia has not been clearly established, al-though collagen abnormalities, as seen in keratoconus,have been reported. The disease usually evolves withprogressive deterioration in uncorrected distancevisual acuity (UDVA) and corrected distance visualacuity (CDVA) caused by the irregular astigmatisminduced by the corneal ectasia.6
Several possible alternatives to manage post-LASIKcorneal ectasia have been reported, including sclera-fitted gas-permeable contact lenses,3,7 collagen
0886-3350/$dsee front matter
doi:10.1016/j.jcrs.2009.12.034
leonardotorquetti
Riscado
leonardotorquetti
Texto de substituição
Twenty-five eyes
leonardotorquetti
Riscado
leonardotorquetti
Texto de substituição
evaluated

987INTRASTROMAL CORNEAL RING SEGMENTS IN CORNEAL ECTASIA
crosslinking,8 deep lamellar keratoplasty,9 and intra-stromal corneal ring segment (ICRS) implantation.10–13 Intrastromal corneal ring segments were designedto achieve a refractive adjustment by flattening thecentral corneal curvature while maintaining clarity inthe central optical zone; theywere first used in patientswith low myopia. Because ICRS are removable andsave tissue, the technique’s application was expandedto eyes with corneal thinning disorders in which re-fractive surgery is not suitable.
Implantation of ICRS has been used largely for treat-ment of primary and secondary ectatic corneal disor-ders. Several studies show the efficacy of ICRS intreating many corneal conditions, such as keratoco-nus,14–15 post-radial keratotomy ectasia,16 astigma-tism,17 and myopia.18
The purpose of this study was to evaluate the visualand keratometric outcomes of ICRS implantation tocorrect ectasia, stabilize ectasia, or both after refractivesurgery.
PATIENTS AND METHODS
In this study, charts of patients who had Ferrara ICRS (Fer-rara Ophthalmics) implantation were reviewed. All patientscompleted at least 6 months of follow-up and had clear cen-tral corneas and contact lens intolerance.
Patients were excluded after the preoperative examinationif they had a history of herpes, keratitis, corneal dystrophy,diagnosed autoimmune disease, systemic connective tissuedisease, and acute or grade IV keratoconus.
Surgical Technique
Table 1. Preoperative patient characteristics.
Parameter Value
The same surgeon (P.F.) performed all ICRS implantationprocedures using topical anesthesia, the manual technique,and the Ferrara ring nomogram.14 With the patient lookingat a red light attached to the turned-off surgical microscope,a reference point was marked in the center of the cornea. Theincision was made at the steepest meridian of the anteriorcornea surface with a calibrated diamond knife set atapproximately 80% of the corneal thickness, was determinedby Scheimpflug scanning-slit tomography (Pentacam, Ocu-lus, Inc.). Corneal pockets were then created with a spreaderhook. One semicircular dissector was placed sequentially inthe lamellar pocket and steadily advanced by rotationalmovement (counterclockwise and clockwise dissectors). Af-ter creation of the tunnels, the ICRS was inserted in thetunnels.
After surgery, moxifloxacin 0.5% and dexamethasone0.1% eyedrops were used 4 times daily for 2 weeks. The pa-tients were instructed to avoid rubbing the eye and to usepreservative-free artificial tears (polyethylene glycol 4000.4%) frequently.
Eyes 25Patients 20
Patient AssessmentSex (M/F) 13/7Age (y)Mean G SD 38.7 G 9.2Range 28–57
A complete ophthalmologic examination was performedbefore and after surgery and includedUDVA, CDVA, biomi-croscopy, corneal topography, pachymetry, and measure-ment of corneal asphericity using the Scheimpflugscanning-slit tomography system.
J CATARACT REFRACT SURG
On the first postoperative day, a slitlamp biomicroscopicexamination was performed. Wound healing and segmentmigration were evaluated. At the last follow-up examina-tion, manifest refraction, UDVA and CDVA, slitlamp, andtopographic examinations were performed.
Statistical Analysis
Statistical analysis was performed using Minitab software(version 2007, Minitab, Inc.). The Student t test for paireddata was used to compare preoperative and postoperativedata.
RESULTS
Twenty-five eyes of 20 patients with corneal ectasia af-ter refractive surgery were evaluated. The refractivesurgery was LASIK in 20 eyes, radial keratotomy in4 eyes, and photorefractive keratectomy in 1 eye.Table 1 shows the characteristics of the patients. Themean follow-up was 39.8 months G 21.1 (SD). All pa-tients had implantation of a single segment. The arcring was 160 degrees in 18 eyes and 210 degrees in 7eyes. The ICRS segment was implanted uneventfullyin all cases.
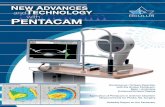
Table 2 shows the postoperative results. The in-crease in mean UDVA andmean CDVA from preoper-atively to postoperatively was statistically significant(P Z .005 and P Z .008, respectively) (Figure 1). Thedecrease in mean corneal asphericity was also statisti-cally significant (P Z .006).
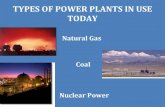
The increase in the mean pachymetry at the apex ofthe cornea and at the thinnest point of the cornea wasstatistically significant (P Z .025 and P Z .000, respec-tively). There was a statistically significant reductionin keratometric values from preoperative to the lastfollow-up examination (P Z .000) (Figure 2).
One patient required additional surgery to reposi-tion the ring. There were no other complications.
DISCUSSION
Thewidespread use of LASIK has not resulted in nota-bly serious complications. Despite the number of stud-ies that support the efficacy of LASIK,19 concern aboutthe occurrence of postoperative keratectasia is grow-ing. The tissue ablation and lamellar cut in LASIK
- VOL 36, JUNE 2010
leonardotorquetti
Texto digitado
which
leonardotorquetti
Riscado
leonardotorquetti
Texto de substituição

Table 2. Preoperative versus postoperative results.
Parameter Preoperative Postoperative P Value
Mean UDVA 20/185 20/66 .005Mean CDVA 20/125 20/40 .008Pachymetry (mm) .025
At apexMean G SD 457.7 G 48.7 466.2 G 49.8 .000Range 361–542 381–559
At thinnest pointMean G SD 436.3 G 46.2 453.9 G 49.3 .000Range 348 to 533 370 to 548
Mean asphericity �0.95 �0.23 .006Keratometry (D) .000
Mean G SD 45.41 G 5.63 42.88 G 4.44Range 37.3–55.5 31.2–54.1
CDVAZ corrected distance visual acuity; UDVA Z uncorrected distancevisual acuity
print&web4C=FPO
988 INTRASTROMAL CORNEAL RING SEGMENTS IN CORNEAL ECTASIA
substantially weaken the mechanical strength and ef-fective thickness of the cornea. There is concern thatat some point, the tensile strength of the cornea maybe reduced to a level that predisposes to postoperativeectasia.20
In our study of ICRS segment implantation forcorneal ectasia after refractive surgery, there was a sig-nificant improvement in UDVA and CDVA postoper-atively. Moreover, there was significant increase incorneal thickness. This can be explained theoreticallyby the cornea collagen remodeling induced by ICRSimplantation.21
We also found a significant decrease in corneal as-phericity after ICRS implantation. The mean postoper-ative asphericity value was�0.23, which is considerednormal in the general population.22 This means thatthe normal physiologic asphericity of the cornea variessignificantly among individuals, ranging from mild
Figure 1. Mean preoperative and postoperative UDVA and CDVACDVS Z corrected distance visual acuity; UDVA Z uncorrecteddistance visual acuity).
J CATARACT REFRACT SURG
oblate to moderate prolate.23,24 In an unpublishedstudy, we evaluated corneal asphericity changes in-duced by ICRS implantation in eyes with keratoconus.We found that ICRS implantation significantly re-duced the mean corneal asphericity, from �0.85 to�0.32. It is well known that after ablation laser proce-dures, most corneas tend to become oblate and whenectasia develops, the corneas usually become prolate.However, the excess prolateness usually found in ker-atoconus (primary) is much greater than that occur-ring in ectasia after refractive surgery. That is theprobable reason the asphericity value after ICRS be-comes closer to normal than when the ICRS is usedfor keratoconus. Asphericity is one marker of visualquality; a normal asphericity value after treatmentcan be a predictor of improvement of quality of vision.
In our study, all eyes had significantly lower kera-tometry values after ICRS implantation. The meanpreoperative values in such cases are usually lowerthan in keratoconus (primary). This can be partially ex-plained by the corneal flattening induced by the refrac-tive procedure, usually in an optic zone of greaterextent than the location of the ectasia.
Most ICRS implanted in our study were conven-tional models, having an arc ring of 160 degrees. TheICRS in the other eyes had an arc ring of 210 degrees.The latter is usually reserved for central cones of thenipple type. Some ectasias assume the same topo-graphic pattern of nipple cones, in which we usuallyuse a 210-degrees arc ring with excellent results.15
This ring is reserved for cases with low astigmatismin which we want to flatten the cornea with minimalinduction of astigmatism.
There are several potential advantages of ICRS im-plantation over keratoplasty in eyes with post-LASIKectasia. First, ICRS implantation avoids further lasertreatment, eliminating central corneal wound healing.
print&web4C=FPO
Figure 2. Scattergram of the mean preoperative and postoperativekeratometry.
- VOL 36, JUNE 2010

989INTRASTROMAL CORNEAL RING SEGMENTS IN CORNEAL ECTASIA
This leaves the optical center of the cornea untouched,enhancing refractive outcomes. Second, the techniqueis reversible in cases of an unsatisfactory refractive orclinical outcomes. Third, adjustment can be performedusing thinner or thicker rings. In cases of unexpectedcorneal shape changes, 1 segment can be removed orexchanged. Fourth, it avoids the complications ofintraocular surgery.
Alio et al.11 found significant improvement in visualacuity after ICRS implantation in eyes with ectasia. In2 eyes, the UDVA was 20/40 postoperatively. In thethird eye, there was a residual refractive error; theUDVA was 20/50 and the CDVA, 20/40.
In a post-LASIK ectasia study, Kymionis et al.8 im-planted ICRS in eyes with a mean preoperativeUDVA of 20/100. At the last follow-up examination,6 (75%) of 8 eyes had a UDVA 20/40 or better. Atthe end of the first postoperative year, UDVA,CDVA, and topography were stable and remained soduring the follow-up period.
In a recent studyof ICRS implantation in corneaswithpellucid marginal degeneration by Pinero et al.,25
UDVA did not improve after surgery (P Z .17). TheCDVA increased significantly at 6 months (P Z .02).Approximately 39% of the eyes gained 2 or more linesof CDVA at 6 months; this percentage increased to60% at 24 months. The cornea was, on average, flatterat 6 months (P!.01), with nonsignificant posterior re-gression of the achieved flattening (P Z .73). In ourstudy, the mean UDVA increased from 20/185 to 20/66(P Z .005) and the mean CDVA, from 20/125 to 20/40(P Z .008).
This study has potential limitations, such as thesmall sample of treated eyes and the lack of a compar-ative group. However, the results were similar to thosein post-LASIK studies in which ICRS were used fortreatment.
In conclusion, ICRS implantation in eyes with cor-neal ectasia after refractive surgery provided satisfac-tory visual outcomes. Larger comparative studies areneeded to confirm the results in our study.
REFERENCES1. Seiler T, Koufala K, Richter G. Iatrogenic keratectasia after
laser in situ keratomileusis. J Refract Surg 1998; 14:
312–317
2. McLeod SD, Kisla T, Caro NC, McMahon TT. Iatrogenic kerato-
conus: corneal ectasia following laser in situ keratomileusis for
myopia. Arch Ophthalmol 2000; 118:282–284
3. Amoils SP, Deist MB, Gous P, Amoils PM. Iatrogenic keratec-
tasia after laser in situ keratomileusis for less than �4.0
to �7.0 diopters of myopia. J Cataract Refract Surg 2000;
26:967–977
4. Kerautret J, Colin J, Touboul D, Roberts C. Biomechanical char-
acteristics of the ectatic cornea. J Cataract Refract Surg 2008;
34:510–513
J CATARACT REFRACT SURG
5. Binder PS. Analysis of ectasia after laser in situ keratomi-
leusis: risk factors. J Cataract Refract Surg 2007; 33:
1530–1538
6. Pallikaris IG, Kymionis GD, Astyrakakis NI. Corneal ectasia in-
duced by laser in situ keratomileusis. J Cataract Refract Surg
2001; 27:1796–1802
7. Tan BU, Purcell TL, Torres LF, Schanzlin DJ. New surgical ap-
proaches to the management of keratoconus and post-LASIK
ectasia. Trans Am Ophthalmol Soc 2006; 104:212–218. discus-
sion, 219–220. Available at: http://www.pubmedcentral.nih.gov/
picrender.fcgi?artidZ1809910&blobtypeZpdf. Accessed Feb-
ruary 21, 2010
8. Kymionis GD, Diakonis VF, Kalyvianaki M, Portaliou D,
Siganos C, Kozobolis VP, Pallikaris AI. One-year follow-up of
corneal confocal microscopy after corneal cross-linking in
patients with post laser in situ keratomileusis ectasia and kerato-
conus. Am J Ophthalmol 2009; 147:774–778
9. McAllum PJ, Segev F, Herzig S, Rootman DS. Deep anterior
lamellar keratoplasty for post-LASIK ectasia. Cornea 2007;
26:507–511
10. Lovisolo CF, Fleming JF. Intracorneal ring segments for iat-
rogenic keratectasia after laser in situ keratomileusis or
photorefractive keratectomy. J Refract Surg 2002; 18:
535–541
11. Alio JL, Salem TF, Artola A, Osman AA. Intracorneal rings to
correct corneal ectasia after laser in situ keratomileusis. J Cata-
ract Refract Surg 2002; 28:1568–1574
12. Pokroy R, Levinger S, Hirsh A. Single INTACS segment for post-
laser in situ keratomileusis keratectasia. J Cataract Refract Surg
2004; 30:1685–1695
13. Kymionis GD, Siganos CS, Kounis G, Astyrakakis N,
Kalyvianaki MI, Pallikaris IG. Management of post-LASIK cor-
neal ectasia with Intacs inserts; one-year results. Arch Ophthal-
mol 2003; 12:322–326. Available at: http://archopht.ama-assn.
org/cgi/reprint/121/3/322. Accessed February 21, 2010
14. Torquetti L, Berbel RF, Ferrara P. Long-term follow-up of intra-
stromal corneal ring segments in keratoconus. J Cataract
Refract Surg 2009; 35:1768–1773
15. Ferrara P, Torquetti L. Clinical outcomes after implantation of
a new intrastromal corneal ring with a 210-degree arc length.
J Cataract Refract Surg 2009; 35:1604–1608
16. Dias de Silva FB, Franca Alves EA, Ferrara de Almeida
Cunha P. Utilizacao do Anel de Ferrara na estabilizacao e corre-
cao da ectasia corneana pos PRK. (Use of Ferrara’s ring in the
stabilization and correction of corneal ectasia after PRK). Arq
Bras Oftalmol 2000; 63:215–218. Available at: http://www.scie-
lo.br/pdf/%0D/abo/v63n3/13587.pdf. Accessed February 21,
2010
17. Ruckhofer J, Stoiber J, Twa MD, Grabner G. Correction of
astigmatism with short arc-length intrastromal corneal ring
segments; preliminary results. Ophthalmology 2003; 110:
516–524
18. Nose W, Neves RA, Burris TE, Schanzlin DJ, Belfort R Jr. Intra-
stromal corneal ring: 12-month sighted myopic eyes. J Refract
Surg 1996; 12:20–28
19. Bailey MD, Zadnik K. Outcomes of LASIK for myopia with FDA-
approved lasers. Cornea 2007; 26:246–254
20. Randleman JB. Post-laser in-situ keratomileusis ectasia: current
understanding and future directions. Curr Opin Ophthalmol
2006; 17:406–412
21. Maguen E, Rabinowitz YS, Regev L, Saghizadeh M, Sasaki T,
Ljubimov AV. Alterations of extracellular matrix components
and proteinases in human corneal buttons with INTACS for
post-laser in situ keratomileusis keratectasia and keratoconus.
Cornea 2008; 27:565–573
- VOL 36, JUNE 2010

print&web4C=FPO
990 INTRASTROMAL CORNEAL RING SEGMENTS IN CORNEAL ECTASIA
22. Yebra-Pimentel E, Gonzalez-Meijome JM, Cervino A, Giraldez MJ,
Gonzalez-Perez J, Parafita MA. Asfericidad corneal en una pobla-
cion de adultos jovenes. Implicaciones clınicas. [Corneal aspheric-
ity in a young adult population. Clinical implications]. Arch Soc Esp
Oftalmol 2004; 79:385–392. Available at: http://scielo.isciii.es/scie-
lo.php?pidZS0365-66912004000800006&scriptZsci_arttext.
Accessed February 21, 2010
23. Kiely PM, Smith G, Carney LG. The mean shape of the human
cornea. Optica Acta 1982; 29:1027–1040
24. Calossi A. The Optical Quality of the Cornea. Canelli, Italy, Fabiano
Editore, 2002. Available at: http://www.mendeley.com/download/
public/35931/118865215/8268674c23188424a5075d2d9c0cf031
e2b488d3. Accessed February 21, 2010.
25. Pinero DP, Alio JL, Morbelli H, Uceda-Montanes A, El Kady B,
Coskunseven E, Pascual I. Refractive and corneal aberrometric
J CATARACT REFRACT SURG
changes after intracorneal ring implantation in corneas with
pellucid marginal degeneration. Ophthalmology 2009;
116:1665–1674
- VO
L 36, JUNE 2010First author:Leonardo Torquetti, MD, PhD,
Private clinic, Belo Horizonte, Brazil.