10 Chest Trauma

of 59
-
Upload
rulisakarozi -
Category
Documents
-
view
230 -
download
0
Transcript of 10 Chest Trauma
-
8/9/2019 10 Chest Trauma
1/59
CHEST TRAUMA CHEST TRAUMA
HOWARD FRIEDLAND DO FACOEPHOWARD FRIEDLAND DO FACOEP
NICOLE MAGUIRE DONICOLE MAGUIRE DO
-
8/9/2019 10 Chest Trauma
2/59
OBJECTIVESOBJECTIVES
Anatomical Review of Chest Anatomical Review of Chest Approach to Chest Trauma Approach to Chest Trauma
Identifying and Treating Immediately LifeIdentifying and Treating Immediately Life
Threatening Conditions.Threatening Conditions.
Identifying and Treating Potentially LifeIdentifying and Treating Potentially Life
Threatening Conditions.Threatening Conditions. Diagnostic Studies and Chest TraumaDiagnostic Studies and Chest Trauma
-
8/9/2019 10 Chest Trauma
3/59
INCIDENCE OF CHEST TRAUMA INCIDENCE OF CHEST TRAUMA
Trauma is the # 1 cause of death in ages 1Trauma is the # 1 cause of death in ages 1--55.55.
Chest trauma causes 1 in 4 deaths inChest trauma causes 1 in 4 deaths in
America. America.
Less than 10% of Blunt Chest TraumaLess than 10% of Blunt Chest Trauma
requires surgery, where as 15requires surgery, where as 15--30% of30% ofPenetrating Chest Trauma requires anPenetrating Chest Trauma requires anopen thoracotomy.open thoracotomy.
-
8/9/2019 10 Chest Trauma
4/59
CAUSES OFCAUSES OF
BLUNT TRAUMA VS CHEST TRAUMA BLUNT TRAUMA VS CHEST TRAUMA
Low VelocityLow Velocity --impalements, knifeimpalements, knife wound. wound.
Medium VelocityMedium Velocity --bullets from mostbullets from mosthand guns and airhand guns and air
powered pellet guns.powered pellet guns. High VelocityHigh Velocity -- riflesrifles
and military weapons.
MVA = 70MVA = 70--80%80%
FALLSFALLS
Act of violence Act of violence -- IE.IE.
•• bat to chest etc.bat to chest etc.
Blast Injuries
and military weapons.Blast Injuries
-
8/9/2019 10 Chest Trauma
5/59
THORACIC CAVITY THORACIC CAVITY
Superior Border of ThoraxSuperior Border of Thorax -- Thoracic Inlet whichThoracic Inlet whichholds the major blood supply to and venousholds the major blood supply to and venousdrainage from the neck.drainage from the neck.
SuperiorSuperior--lateral Border of Thoraxlateral Border of Thorax -- ThoracicThoracicOutlet, Brachial Plexus, Axillary Vein, BrachialOutlet, Brachial Plexus, Axillary Vein, Brachial Artery. Artery.
Inferior BorderInferior Border -- hemidiaphragmhemidiaphragm -- holds theholds thediaphragmatic hiatus = Aorta, Esophagus, Vagaldiaphragmatic hiatus = Aorta, Esophagus, VagalNerve, Thoracic Duct and Vena Cava.Nerve, Thoracic Duct and Vena Cava.
-
8/9/2019 10 Chest Trauma
6/59
ANATOMY REVIEW CONTINUED ANATOMY REVIEW CONTINUED
Within Chest WallWithin Chest Wall -- Muscles, Ribs,Muscles, Ribs,Sternum,Clavicle, Scapulae.Sternum,Clavicle, Scapulae.
Parietal PleuraParietal Pleura
--
inner lining of chest wall.inner lining of chest wall.
Visceral Pleura Visceral Pleura -- invests major organs.invests major organs.
Pleura SpacePleura Space -- potential space between thepotential space between the
two with a small amount of fluid in it.two with a small amount of fluid in it.
-
8/9/2019 10 Chest Trauma
7/59
RESPIRATORY SYSEMRESPIRATORY SYSEM
IN 2 LINES OR LESSIN 2 LINES OR LESS
LungsLungs -- Right has 3 lobes, Left has 2 lobes.Right has 3 lobes, Left has 2 lobes.
Trachea splits into R and L mainstemTrachea splits into R and L mainstembronchi then divides into lobar bronchi.bronchi then divides into lobar bronchi.
-
8/9/2019 10 Chest Trauma
8/59
Incase you forgot about the heartIncase you forgot about the heart
Heart is contained within pericardium.Heart is contained within pericardium.
Blood flow:Blood flow:blood is received from the superior andblood is received from the superior and
inferior vena cava ~RA~RV via tricuspidinferior vena cava ~RA~RV via tricuspid
valve ~ lungs via pulmonic valve ~ LA ~ LV valve ~ lungs via pulmonic valve ~ LA ~ LV
via mitral valve ~ thoracic aorta via aortic via mitral valve ~ thoracic aorta via aortic
valve. valve.
-
8/9/2019 10 Chest Trauma
9/59
Miscellaneous OrgansMiscellaneous Organs
Esophagus lies posterior to the trachea.Esophagus lies posterior to the trachea. To the right of it is the Aortic Arch.To the right of it is the Aortic Arch.
To the left of it is the Descending Aorta.To the left of it is the Descending Aorta.
Thoracic Duct runs posterior and isThoracic Duct runs posterior and isproximal to the spinal column, it enters theproximal to the spinal column, it enters the
Left Subclavian Vein in the neck.Left Subclavian Vein in the neck.
-
8/9/2019 10 Chest Trauma
10/59
Primary Survey (ATLS)Primary Survey (ATLS)
Physician must begin withPhysician must begin with ABC’s Trauma ABC’s Trauma for anyfor anychest trauma patient:chest trauma patient:
A A -- airwayairway
BB -- breathingbreathing
C circulationC circulation
TT -- thoracotomythoracotomy DD -- disabilitydisability -- neuro checkneuro check
EE -- exposureexposure -- remove clothing, roll person.remove clothing, roll person.
-
8/9/2019 10 Chest Trauma
11/59
AIRWAY AIRWAY
Listen for airway movement at patient’sListen for airway movement at patient’snose and mouth.nose and mouth.
Access intercostal and supraclavicular Access intercostal and supraclavicular
muscle retractions.muscle retractions.
Assess oropharynx for foreign body Assess oropharynx for foreign body
obstruction, especially in an unconsciousobstruction, especially in an unconsciouspatient.patient.
-
8/9/2019 10 Chest Trauma
12/59
BREATHINGBREATHING
Expose patient’s chest.Expose patient’s chest. Observe, palpate and listen for respiratoryObserve, palpate and listen for respiratory
movement.movement.
Rate of breathing.Rate of breathing.
Breathing patternBreathing pattern -- shallow breaths areshallow breaths are
ominous.ominous.
CyanosisCyanosis -- late sign of hypoxia.late sign of hypoxia.
-
8/9/2019 10 Chest Trauma
13/59
CirculationCirculation
Check pulse for quality, rate and regularity.Check pulse for quality, rate and regularity. Blood PressureBlood Pressure
Asses and palpate skin for color and Asses and palpate skin for color andtemperature.temperature.
Check neck veins for distentionCheck neck veins for distention -- indicationindication
of cardiac tamponade that may be absent ifof cardiac tamponade that may be absent if
patient is hypovolemic.patient is hypovolemic.
Cardiac MonitorCardiac Monitor -- dysrythmia, PVC, PEA dysrythmia, PVC, PEA
-
8/9/2019 10 Chest Trauma
14/59
Pulseless Electrical ActivityPulseless Electrical Activity
HypovolemiaHypovolemia
HypoxiaHypoxia
HH++ -- Acidosis Acidosis
Hemothorax Hemothorax
HypothermiaHypothermia
Hyperkalemia
Tension Pneumothorax Tension Pneumothorax
TamponadeTamponade
ToxinsToxins
Beta BlockersBeta Blockers
DigitalisDigitalis
TCA TCA
CaCa++++ Channel BlockersChannel Blockers
ThrombusThrombus
Pulmonary EmbolusPulmonary Embolus
Myocardial Infarction
Hyperkalemia
Myocardial Infarction
-
8/9/2019 10 Chest Trauma
15/59
-
8/9/2019 10 Chest Trauma
16/59
OPEN THORACOTOMY OPEN THORACOTOMY
-
8/9/2019 10 Chest Trauma
17/59
THORACOTOMY THORACOTOMY
Use of emergent resuscitative thoracotomyUse of emergent resuscitative thoracotomyhas been reported to result in survival ashas been reported to result in survival asfollows:follows:
99--57% patients with penetrating57% patients with penetratingcardiac injury.cardiac injury.
00--66% patients with non66% patients with non--cardiaccardiacthoracic injury.thoracic injury.
8% overall survival rate.8% overall survival rate.
-
8/9/2019 10 Chest Trauma
18/59
SECONDARY SURVEY SECONDARY SURVEY
Head to foot exam, remember the back.Head to foot exam, remember the back. If the patient is unstable a brief history isIf the patient is unstable a brief history is
applicable at this time =applicable at this time =
A A -- allergiesallergies
MM -- medicationsmedications
PP – – past medical historypast medical history
LL – – last meal eatenlast meal eaten
EE -- events of traumaevents of trauma
-
8/9/2019 10 Chest Trauma
19/59
SECONDARY SURVEY (con’t)SECONDARY SURVEY (con’t)
If the patient is stabilized obtain a more in depthIf the patient is stabilized obtain a more in depth
history including:history including:
Time of injury.Time of injury.
Mechanism of InjuryMechanism of Injury -- velocity and deceleration velocity and decelerationfor MVA.for MVA.
Complete Physical ExamComplete Physical Exam -- including evidence ofincluding evidence of
injuries to other systems.injuries to other systems. Preliminary testsPreliminary tests -- CXR, EKG, ABG.CXR, EKG, ABG.
IMMEDIATELY LIFE THREATENINGIMMEDIATELY LIFE THREATENING
-
8/9/2019 10 Chest Trauma
20/59
IMMEDIATELY LIFE THREATENINGIMMEDIATELY LIFE THREATENING
CHEST INJURIESCHEST INJURIES
These conditions are evidenced in the primaryThese conditions are evidenced in the primarysurveysurvey::
Airway Obstruction and Traumatic Asphyxia Airway Obstruction and Traumatic Asphyxia
Tension Pneumothorax Tension Pneumothorax
Open Pneumothorax Open Pneumothorax
Massive Hemothorax Massive Hemothorax Flail ChestFlail Chest
Cardiac TamponadeCardiac Tamponade
POTENITALLY LIFE THREATENINGPOTENITALLY LIFE THREATENING
-
8/9/2019 10 Chest Trauma
21/59
POTENITALLY LIFE THREATENINGPOTENITALLY LIFE THREATENING
CHEST INJURIESCHEST INJURIES
These conditions are evidenced inThese conditions are evidenced insecondary surveysecondary survey::
Pulmonary ContusionPulmonary Contusion
Myocardial ContusionMyocardial Contusion
Aortic Disruption Aortic Disruption
Traumatic Diaphragmatic RuptureTraumatic Diaphragmatic Rupture
Esophageal RuptureEsophageal Rupture
Blunt injuries to SVC and other major veins.Blunt injuries to SVC and other major veins.
OTHER INJURIES EVIDENCED INOTHER INJURIES EVIDENCED IN
-
8/9/2019 10 Chest Trauma
22/59
OTHER INJURIES EVIDENCED INOTHER INJURIES EVIDENCED IN
CHEST TRAUMA CHEST TRAUMA
Rib FracturesRib Fractures
Clavicular FracturesClavicular Fractures
Scapular FracturesScapular Fractures
Blunt injuries to Thoracic Duct.Blunt injuries to Thoracic Duct.
-
8/9/2019 10 Chest Trauma
23/59
AIRWAY OBSTRUCTION AIRWAY OBSTRUCTION
Evidenced in blunt trauma, especially MVAEvidenced in blunt trauma, especially MVAand blast injuries.and blast injuries.
Will be seen in primary survey duringWill be seen in primary survey during
airway step.airway step. Readjust head to sniffing position.Readjust head to sniffing position.
•• If CIf C--spine has been cleared.spine has been cleared. Attempt direct visualization and removal. Attempt direct visualization and removal.
May need fiberoptics for visualization.May need fiberoptics for visualization.
-
8/9/2019 10 Chest Trauma
24/59
Traumatic AsphyxiaTraumatic Asphyxia
Result of thoracic injury due to strongResult of thoracic injury due to strongcrushing injury.crushing injury.
Signs and Symptoms:Signs and Symptoms:cyanosis of head and neck, subconjuctivalcyanosis of head and neck, subconjuctival
hemorrhage, periorbital ecchymosis,hemorrhage, periorbital ecchymosis,petechiae, edematous moonpetechiae, edematous moon--like face,like face,epistaxis, hemotypmany, LOC, seizure.epistaxis, hemotypmany, LOC, seizure.
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
25/59
TREATMENT OFTREATMENT OF
TRAUMATIC ASHPYXIA TRAUMATIC ASHPYXIA
Maintain adequate airway.Maintain adequate airway. Elevate head of bed to 30 degrees toElevate head of bed to 30 degrees to
decrease pressure to the head.decrease pressure to the head.
ICU admission with serial neuro checks.ICU admission with serial neuro checks.
Associated injuries of head and torso seen Associated injuries of head and torso seen
with this type of injury often need surgery. with this type of injury often need surgery.
No specific surgery for this condition.No specific surgery for this condition.
-
8/9/2019 10 Chest Trauma
26/59
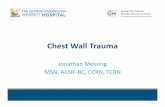
TENSION PNEUMOTHORAX TENSION PNEUMOTHORAX
A one war air leak that collapses the A one war air leak that collapses theaffected lung with mediastinal andaffected lung with mediastinal and
tracheal shift to the opposite side.tracheal shift to the opposite side.
Signs and Symptoms:Signs and Symptoms:
respiratory distress, tachycardia,respiratory distress, tachycardia,hypotension, tracheal deviation, unilateralhypotension, tracheal deviation, unilateral
absent breath sounds, neck veinabsent breath sounds, neck veindistension, cyanosis.distension, cyanosis.
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
27/59
TREATMENT OFTREATMENT OF
TENSION PNEUMOTHORAX TENSION PNEUMOTHORAX
Immediate Decompression with a 14”Immediate Decompression with a 14”gauge needle into the second intercostalgauge needle into the second intercostalspace at midclavicular line of affectedspace at midclavicular line of affected
side.side.
Definitive treatmentDefinitive treatment
--
insertion of a chestinsertion of a chest
tube into the fifth intercostal spacetube into the fifth intercostal spaceanterior to midanterior to mid--axillary line.axillary line.
-
8/9/2019 10 Chest Trauma
28/59
Pneumothorax Pneumothorax
-
8/9/2019 10 Chest Trauma
29/59
S/P CHEST TUBE INSERTIONS/P CHEST TUBE INSERTION
OPEN PNUEMOTHORAXOPEN PNUEMOTHORAX
-
8/9/2019 10 Chest Trauma
30/59
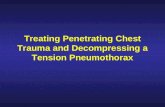
OPEN PNUEMOTHORAX OPEN PNUEMOTHORAX
“SUCKING CHEST WOUND”“SUCKING CHEST WOUND”
A large defect of the chest wall causing A large defect of the chest wall causingequilibration between the interthoracicequilibration between the interthoracic
and atmospheric pressure.and atmospheric pressure.
If the opening is 2/3 or more in diameter ofIf the opening is 2/3 or more in diameter of
the trachea, air will prefer to pass throughthe trachea, air will prefer to pass through
the open chest wound.the open chest wound. Signs and Symptoms:Signs and Symptoms:
a large open wound of the chest,a large open wound of the chest,respiratory distress.respiratory distress.
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
31/59
TREATMENT OFTREATMENT OF
OPEN PNEUMOTHORAX OPEN PNEUMOTHORAX
Promptly close the defect with a sterilePromptly close the defect with a steriledressing taped on 3 sides creating adressing taped on 3 sides creating a
flutterflutter--type valve.type valve.
Closure of all 4 sides of the dressing couldClosure of all 4 sides of the dressing could
cause a tension pneumothorax if chestcause a tension pneumothorax if chest
tube is not in place.tube is not in place. Definitive surgical closure of the defect isDefinitive surgical closure of the defect is
required.required.
-
8/9/2019 10 Chest Trauma
32/59
Massive Hemothorax Massive Hemothorax
Accumulation of more than 1500ml of Accumulation of more than 1500ml ofblood.blood.
Usually secondary to penetrating wound.Usually secondary to penetrating wound.
Signs and Symptoms:Signs and Symptoms:
shock, absent breath sounds, dullness toshock, absent breath sounds, dullness to
percussion on one side of the chest.percussion on one side of the chest.
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
33/59
TREATMENT OFTREATMENT OF
MASSIVE HEMOTHORAX MASSIVE HEMOTHORAX
Manage with simultaneous restoration ofManage with simultaneous restoration ofblood volume and decompression of chestblood volume and decompression of chest
cavity.cavity.
CHEST TUBECHEST TUBE -- 38 french or larger38 french or larger
Prepare for autoPrepare for auto--transfusion with massivetransfusion with massive
blood loss.blood loss.
Thoracotomy.Thoracotomy.
THORACOTOMY ANDTHORACOTOMY AND
-
8/9/2019 10 Chest Trauma
34/59
THORACOTOMY ANDTHORACOTOMY AND
MASSIVE HEMOTHORAX MASSIVE HEMOTHORAX
Thoracotomy is indicated if there isThoracotomy is indicated if there is>1500ml blood loss or 1500ml blood loss or 200ml/hr.continuous loss > 200ml/hr.
Penetrating anterior wound medial toPenetrating anterior wound medial to
nipple line or posterior wound medial tonipple line or posterior wound medial to
scapula may need thoracotomy due toscapula may need thoracotomy due todamage to great vessels, hilar structuresdamage to great vessels, hilar structures
or heart.or heart.
Surgeon must be present!Surgeon must be present!
-
8/9/2019 10 Chest Trauma
35/59
FLAIL CHESTFLAIL CHEST
Secondary to multiple rib fractures.Secondary to multiple rib fractures. A segment of the chest wall does not have A segment of the chest wall does not have
bony continuity with the rest of the thoracicbony continuity with the rest of the thoracic
cage.cage.
Major problem is from the injury to theMajor problem is from the injury to the
underlying lung.underlying lung.
Paradoxical motion alone does not causeParadoxical motion alone does not cause
hypoxia, it is the pain with restricted chesthypoxia, it is the pain with restricted chest wall movement and lung injury . wall movement and lung injury .
SIGNS AND SYMPTOMS OFSIGNS AND SYMPTOMS OF
-
8/9/2019 10 Chest Trauma
36/59
SIGNS AND SYMPTOMS OFSIGNS AND SYMPTOMS OF
FLAIL CHESTFLAIL CHEST
Poor inspiratory effort.Poor inspiratory effort.
Asymmetrical movement of thorax. Asymmetrical movement of thorax.
Crepitus of rib or cartilage fractures.Crepitus of rib or cartilage fractures.
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
37/59
TREATMENT OFTREATMENT OF
FLAIL CHESTFLAIL CHEST
FluidsFluids -- be careful not to overload patient.be careful not to overload patient. Adequate ventilation Adequate ventilation -- some patients maysome patients may
require intubation.require intubation.
Humidified oxygen.Humidified oxygen.
Analgesics. Analgesics.
ReRe--expansion of lung via CT if necessary forexpansion of lung via CT if necessary for
pneumothorax.pneumothorax.
-
8/9/2019 10 Chest Trauma
38/59
CARDIAC TAMPONADECARDIAC TAMPONADE
Usually a result of penetrating injuries.Usually a result of penetrating injuries.
Only a small amount of blood in theOnly a small amount of blood in the
pericardial sac is needed to restrictpericardial sac is needed to restrict
cardiac activity.cardiac activity.
SIGNS AND SYMPTOMS OFSIGNS AND SYMPTOMS OF
-
8/9/2019 10 Chest Trauma
39/59
SIGNS AND SYMPTOMS OFSIGNS AND SYMPTOMS OF
CARDIAC TAMPONADECARDIAC TAMPONADE
Becks Triad:Becks Triad:
Muffled Heart TonesMuffled Heart Tones
Increased Venous PressureIncreased Venous Pressure – – distendeddistended
neck veins (absent with hypovolemia).neck veins (absent with hypovolemia).Decreased Arterial PressureDecreased Arterial Pressure – – HypotensionHypotension
Pulsus ParadoxusPulsus Paradoxus – – decreased pressure duringdecreased pressure during
inspiration in excess of 10mmHg.inspiration in excess of 10mmHg. Kussmaul’s SignKussmaul’s Sign – – rise in venous pressure withrise in venous pressure with
inspiration while breathing normal.inspiration while breathing normal.
CARDIAC TAMPONADECARDIAC TAMPONADE
-
8/9/2019 10 Chest Trauma
40/59
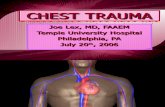
CARDIAC TAMPONADECARDIAC TAMPONADE
SECONDARY TO HEMOPERICARDIUMSECONDARY TO HEMOPERICARDIUM
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
41/59
TREATMENT OFTREATMENT OF
CARDIAC TAMPONADECARDIAC TAMPONADE
PericardiocentesisPericardiocentesis – – use a plasticuse a plasticsheathed needle if available and enter viasheathed needle if available and enter viasubxyphoid route.subxyphoid route.
All patients with a positive All patients with a positivepericardiocentesis secondary to traumapericardiocentesis secondary to trauma will require an open thoracotomy. will require an open thoracotomy.
Open pericardiotomy may be required ifOpen pericardiotomy may be required ifblood in pericardial sac is clotted.blood in pericardial sac is clotted.
-
8/9/2019 10 Chest Trauma
42/59
POTENTIALLY LETHAL CHEST INJURIESPOTENTIALLY LETHAL CHEST INJURIES
These injuries are not obvious on initialThese injuries are not obvious on initialexam and require a high index of suspicionexam and require a high index of suspicion
to diagnose them.to diagnose them.
They are evaluated through the secondaryThey are evaluated through the secondary
survey and are lethal if not detected andsurvey and are lethal if not detected andtreated promptly.treated promptly.
-
8/9/2019 10 Chest Trauma
43/59
-
8/9/2019 10 Chest Trauma
44/59
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
45/59
TREATMENT OFTREATMENT OF
MYOCARDIAL CONTUSIONMYOCARDIAL CONTUSION
Patient is at high risk for suddenPatient is at high risk for sudden
dysrythmias.dysrythmias.
ICU admission with cardiac monitor andICU admission with cardiac monitor and
close observation.close observation.
Treat dysrythmias as per ACLS protocols.Treat dysrythmias as per ACLS protocols.
-
8/9/2019 10 Chest Trauma
46/59
TRAUMATIC AORTIC RUPTURETRAUMATIC AORTIC RUPTURE
Common cause of death after MVA or fallCommon cause of death after MVA or fallfrom a great height.from a great height.
Usually fatal at scene.Usually fatal at scene.
Viable patient’s usually have a tear near Viable patient’s usually have a tear nearthe ligamentum arteriosum and continuitythe ligamentum arteriosum and continuityof the adventitia layer prevents immediateof the adventitia layer prevents immediatedeath.death.
Considered a contained hematoma.Considered a contained hematoma.
SIGNS, SYMPTOMS, AND DIAGNOSTICSIGNS, SYMPTOMS, AND DIAGNOSTIC
-
8/9/2019 10 Chest Trauma
47/59
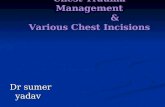
SIGNS, SYMPTOMS, AND DIAGNOSTICSIGNS, SYMPTOMS, AND DIAGNOSTIC
FINDINGS OF AORTIC RUPTUREFINDINGS OF AORTIC RUPTURE
Signs and Symptoms are usually absent.Signs and Symptoms are usually absent.
Pressure usually drops but responds to fluidPressure usually drops but responds to fluidresuscitation.resuscitation.
Radiology SignsRadiology Signs – – widened mediastinum (most widened mediastinum (mostsignificant finding), fracture of first and secondsignificant finding), fracture of first and secondribs, obliteration of the aortic knob, deviation ofribs, obliteration of the aortic knob, deviation ofthe trachea to the right, presence of pleural cap,the trachea to the right, presence of pleural cap,elevation and R shift of R mainstem bronchus,elevation and R shift of R mainstem bronchus,depression of the L mainstem bronchus, deviationdepression of the L mainstem bronchus, deviationof the esophagus (seen via NGT placement).of the esophagus (seen via NGT placement).
TREATMENT OFTREATMENT OF
-
8/9/2019 10 Chest Trauma
48/59
TREATMENT OFO
TRAUMATIC AORTIC RUPTURETRAUMATIC AORTIC RUPTURE
Angiography should be performed liberally Angiography should be performed liberally
if high index of suspicion of injury.if high index of suspicion of injury.
Direct repair of the aorta or resection of theDirect repair of the aorta or resection of the
injured area and grafting.injured area and grafting.
TRAUMATIC DIAPHRAGMATICTRAUMATIC DIAPHRAGMATIC
-
8/9/2019 10 Chest Trauma
49/59
U C G C
RUPTURERUPTURE
More commonly dx on L secondary to liverMore commonly dx on L secondary to liver
obliterating defect on R.obliterating defect on R.
Blunt TraumaBlunt Trauma – – large radial tears that lead tolarge radial tears that lead toherniation.herniation.
Penetrating TraumaPenetrating Trauma – – small perforations that takesmall perforations that take
time even years to develop into hernias.time even years to develop into hernias.
TRAUMATIC DIAPHRAGMATICTRAUMATIC DIAPHRAGMATIC
-
8/9/2019 10 Chest Trauma
50/59
RUPTURERUPTURE
If a laceration of the Left diaphragm isIf a laceration of the Left diaphragm issuspected, place a NGT. If this appears insuspected, place a NGT. If this appears inthe thoracic cavity on CXR need for contrastthe thoracic cavity on CXR need for contrast
study is eliminated.study is eliminated. Right diaphragmatic rupture is rarelyRight diaphragmatic rupture is rarely
diagnosed earlydiagnosed early – – suspect if there is ansuspect if there is an
elevated R. diaphragm on CXR.elevated R. diaphragm on CXR. TreatmentTreatment – – Direct Repair.Direct Repair.
-
8/9/2019 10 Chest Trauma
51/59
ESOPHAGEAL TRAUMA ESOPHAGEAL TRAUMA
Usually due to penetrating trauma.Usually due to penetrating trauma.
Blunt injury causes a forceful expulsion ofBlunt injury causes a forceful expulsion of
gastric contents into mediastinumgastric contents into mediastinum – –
mediastinitis and may be lethal if notmediastinitis and may be lethal if not
recognized.recognized.
Delayed rupture into pleural space mayDelayed rupture into pleural space maycause an empyema.cause an empyema.
SIGNS AND SYMPTOMS OFSIGNS AND SYMPTOMS OF
-
8/9/2019 10 Chest Trauma
52/59
ESOPHAGEAL TRAUMA ESOPHAGEAL TRAUMA
L. pneumothorax or hemothorax without ribL. pneumothorax or hemothorax without ribfracture.fracture.
Severe blow to the sternum or epigastrumSevere blow to the sternum or epigastrum
with pain or shock out of proportion to with pain or shock out of proportion toinjury.injury.
Particulate matter in the chest tube afterParticulate matter in the chest tube afterblood clears.blood clears.
Presence of mediastinal air on CXRPresence of mediastinal air on CXR
-
8/9/2019 10 Chest Trauma
53/59
TREATMENT OF ESOPHAGEAL TRAUMA TREATMENT OF ESOPHAGEAL TRAUMA
Confirm with contrast study orConfirm with contrast study or
esophagoscopy.esophagoscopy.
Wide drainage of the mediastinum andWide drainage of the mediastinum and
pleural space.pleural space.
Direct Repair of injury.Direct Repair of injury.
DIAGNOSTIC STUDIES AND TRAUMA:DIAGNOSTIC STUDIES AND TRAUMA:
-
8/9/2019 10 Chest Trauma
54/59
LABSLABS
To aid in confirmation of diagnosis andTo aid in confirmation of diagnosis andmonitor patient.monitor patient.
CBCCBC – – helps gauge blood loss.helps gauge blood loss.
BMPBMP – – patient’s requiring massive fluidpatient’s requiring massive fluidresuscitation should have electrolytesresuscitation should have electrolytesmonitored. Aids with acidmonitored. Aids with acid--base disorders.base disorders.
Coagulation ProfileCoagulation Profile – – for patient’s receivingfor patient’s receivingmassive transfusions (look for DIC).massive transfusions (look for DIC).
-
8/9/2019 10 Chest Trauma
55/59
LABSLABS Type and CrossType and Cross
ABG ABG – – allows you to evaluate ventilation,allows you to evaluate ventilation,
oxygenation and acidoxygenation and acid--base status.base status.
Cardiac EnzymesCardiac Enzymes – – correlate with patient’s EKG,correlate with patient’s EKG,abnormalities in patients with blunt cardiacabnormalities in patients with blunt cardiac
injury (Myocardial contusion).injury (Myocardial contusion).
Lactate LevelLactate Level – – measure of tissue perfusion.measure of tissue perfusion.
Levels that clear quickly = better outcomes.Levels that clear quickly = better outcomes.
DIAGNOSTIC STUDIES AND TRAUMA:DIAGNOSTIC STUDIES AND TRAUMA:
-
8/9/2019 10 Chest Trauma
56/59
IMAGING STUDIESIMAGING STUDIES
CXRCXR – – aids in confirmation ofaids in confirmation of
pneumothorax, hemothorax, cardiac andpneumothorax, hemothorax, cardiac and
great vessel injuries. (Should not wait forgreat vessel injuries. (Should not wait for
one to confirm clinical suspicion of tensionone to confirm clinical suspicion of tensionpneumothorax).pneumothorax).
CT ScanCT Scan – – useful in more occult oruseful in more occult orundetected injury. CT patient’s withundetected injury. CT patient’s with
possible aortic injuriespossible aortic injuries
-
8/9/2019 10 Chest Trauma
57/59
IMAGING STUDIESIMAGING STUDIES Aortogram Aortogram – – gold standard in diagnosis of aorticgold standard in diagnosis of aortic
and great vessel injury. If CT is positive for aorticand great vessel injury. If CT is positive for aortic
injury, do aortogram to see exact location andinjury, do aortogram to see exact location and
extent of injury.extent of injury.
Thoracic USThoracic US – – usually done in ED duringusually done in ED during
secondary survey. May visualize pericardium,secondary survey. May visualize pericardium,
heart, thoracic cavity. Pericardial effusions,heart, thoracic cavity. Pericardial effusions,tamponade, and hemothoraces are recognizedtamponade, and hemothoraces are recognized
with sensitivity and specificity of 90%. with sensitivity and specificity of 90%.
DIAGNOSTIC STUDIES AND TRAUMA:DIAGNOSTIC STUDIES AND TRAUMA:
-
8/9/2019 10 Chest Trauma
58/59
EKGEKG
Aids in identification of new cardiac Aids in identification of new cardiacabnormalities and underlying cardiacabnormalities and underlying cardiacproblems.problems.
Important in patients with clinicallyImportant in patients with clinicallysignificant blunt cardiac injury.significant blunt cardiac injury.
Most common EKG finding in patients withMost common EKG finding in patients with
myocardial contusionmyocardial contusion – – tachyarrhythmia,tachyarrhythmia,first degree blocks, bundle branch blocks.first degree blocks, bundle branch blocks.
-
8/9/2019 10 Chest Trauma
59/59
SUMMARY SUMMARY Chest Trauma is common in multiple injuredChest Trauma is common in multiple injured
patients and is often associated with lifepatients and is often associated with lifethreatening problems.threatening problems.
Remember Primary SurveyRemember Primary Survey – – ABCT(rauma) ABCT(rauma)
Always treat first step of ABC’s before proceeding Always treat first step of ABC’s before proceedingto the next, a change in vitals start fromto the next, a change in vitals start frombeginning.beginning.
Have high suspicion for potentially lifeHave high suspicion for potentially lifethreatening condition in secondary survey.threatening condition in secondary survey.