1 Heart Sounds and Murmurs J.B. Handler, M.D. Physician Assistant Program University of New England.
Upload
melina-charlesCategory
view
216download
2
1
Thyroid DiseaseThyroid Disease
J.B. Handler, M.D.J.B. Handler, M.D.
Physician Assistant ProgramPhysician Assistant Program
University of New EnglandUniversity of New England

2
AbbreviationsAbbreviations
TSH- Thyroid stimulating TSH- Thyroid stimulating hormonehormone
TBG- thyroid binding globulinTBG- thyroid binding globulin TBPA- thyroid binding pre-TBPA- thyroid binding pre-
albuminalbumin IT- iodothyroxineIT- iodothyroxine Tg- thyroglobulinTg- thyroglobulin TPO- thyroperoxidaseTPO- thyroperoxidase TSI- thyroid stimulating TSI- thyroid stimulating
immunoglobulinimmunoglobulin
PTU- propylthiouracilPTU- propylthiouracil FNA- fine needle aspirateFNA- fine needle aspirate Ca- cancerCa- cancer RAI- radioactive iodineRAI- radioactive iodine D/C- discontinueD/C- discontinue CHD- coronary heart diseaseCHD- coronary heart disease HF- heart failureHF- heart failure ST- sinus tachycardiaST- sinus tachycardia

3
Thyroid PhysiologyThyroid Physiology
Hypothalamic-Pituitary-Thyroid axisHypothalamic-Pituitary-Thyroid axis TSH- turns thyroid on and off- binds to TSH- turns thyroid on and off- binds to
receptors of follicular cells.receptors of follicular cells. Iodine essential for manufacture of thyroid Iodine essential for manufacture of thyroid
hormones- need 0.2 mg daily dietary intake, hormones- need 0.2 mg daily dietary intake, 60 ug into thyroid.60 ug into thyroid.
Iodine deficiency – significant source of Iodine deficiency – significant source of hypothyroidism world wide; rare in U.S.A hypothyroidism world wide; rare in U.S.A because of iodized salt.because of iodized salt.

4
Thyroid Hormone SynthesisThyroid Hormone Synthesis
Iodine trapping followed by thyroid Iodine trapping followed by thyroid peridoxidase linking of I to tyrosine.peridoxidase linking of I to tyrosine.
MIT+DIT+TG = TMIT+DIT+TG = T33- Triiodothyronine - Triiodothyronine
DIT+DIT+TG = TDIT+DIT+TG = T4 4 -- ThyroxineThyroxine
– Thyroid makes Thyroid makes 15x more T15x more T44 than T than T33
MIT- monoiodotyrosineDIT- diiodotyrosine

5
Thyroid Hormone SynthesisThyroid Hormone Synthesis
TT44 99.98% protein bound, .025% free 99.98% protein bound, .025% free TT33 99.7% protein bound, 0.3% free (3-4x more 99.7% protein bound, 0.3% free (3-4x more
biologically active than Tbiologically active than T44))– Only free hormone (TOnly free hormone (T44 or T or T33) enters cells and ) enters cells and
exhibits biologic activity.exhibits biologic activity. TT44 conversion to conversion to TT33 in periphery (liver, brain, in periphery (liver, brain,
heart) by deiodinase enzymes after release from heart) by deiodinase enzymes after release from gland. Clinical application: see Rx of gland. Clinical application: see Rx of hyperthyroidism.hyperthyroidism.– Conversion represents 80-90% of circulating TConversion represents 80-90% of circulating T33

6
Thyroid Hormone TransportThyroid Hormone Transport
Thyroxine Binding Globulin (TBG) made Thyroxine Binding Globulin (TBG) made in liver binds 80% thyroid hormone; in liver binds 80% thyroid hormone; remainder bound to TBPA and albumin.remainder bound to TBPA and albumin.
Alterations of TBG will lead to changes in Alterations of TBG will lead to changes in total Ttotal T44 and T and T33 in in absence of clinical absence of clinical diseasedisease. Example: TBG levels increased . Example: TBG levels increased with estrogen (pregnancy, OCP)- total Twith estrogen (pregnancy, OCP)- total T44 will be elevated but will be elevated but free Tfree T44 and TSH and TSH will will be normal. (see below).be normal. (see below).

7
Thyroid Hormone ActionsThyroid Hormone Actions
Bind to nuclear receptors in most tissues, Bind to nuclear receptors in most tissues, especially brain, heart, kidneys, muscle, especially brain, heart, kidneys, muscle, pituitary and liver.pituitary and liver.
Crucial role in cell differentiation during Crucial role in cell differentiation during development- cell growth, maturation, and development- cell growth, maturation, and gene expression. If absent at birthgene expression. If absent at birthsevere severe mental retardationmental retardation “cretinism”; TSH “cretinism”; TSH screening in all newborns in USA.screening in all newborns in USA.

8
Thyroid Hormone ActionsThyroid Hormone Actions
Help maintain Help maintain thermogenic and metabolic thermogenic and metabolic homeostasis in the adulthomeostasis in the adult. Essential for normal . Essential for normal metabolism, protein synthesis and metabolism, protein synthesis and organ organ functionfunction..
The most common disorders of the thyroid gland The most common disorders of the thyroid gland are the result of are the result of autoimmune processesautoimmune processes that that either cause glandular destruction and either cause glandular destruction and underproduction of thyroid hormone or stimulate underproduction of thyroid hormone or stimulate overproduction of thyroid hormone.overproduction of thyroid hormone.

9
History and PhysicalHistory and Physical
HistoryHistory: Wt. changes, energy level, heat/cold : Wt. changes, energy level, heat/cold intolerance, skin/hair changes, fluid retention, intolerance, skin/hair changes, fluid retention, mood changes (anxiety, depression), visual mood changes (anxiety, depression), visual disturbance, diarrhea/constipation, neck swelling, disturbance, diarrhea/constipation, neck swelling, palpitations, SOB, and more (see below).palpitations, SOB, and more (see below).
PEPE: VS, weight, scalp, hair, eyes, neck, skin, : VS, weight, scalp, hair, eyes, neck, skin, heart, abdomen, extremities, neuro/reflexes.heart, abdomen, extremities, neuro/reflexes.– Detailed Detailed thyroid examthyroid exam: size, tenderness, enlargement, : size, tenderness, enlargement,
texture, nodularity, firmness, bruits.texture, nodularity, firmness, bruits.

GoiterGoiter
Google.images.com

11
Evaluation of Thyroid FunctionEvaluation of Thyroid Function
Numerous tests available; interpretation can Numerous tests available; interpretation can be confusing.be confusing.
Thyroid Stimulating Hormone (TSH)Thyroid Stimulating Hormone (TSH) and and free Tfree T44 are the most informative tests of are the most informative tests of thyroid function and have replaced the need thyroid function and have replaced the need in most situations to order additional in most situations to order additional testing.testing.
TT33 levels (total or free) may be useful in levels (total or free) may be useful in special circumstances (below). special circumstances (below).

12
Thyroid Stimulating HormoneThyroid Stimulating Hormone
Secretion controlled via negative feedback from Secretion controlled via negative feedback from thyroid hormones.thyroid hormones.
Extremely sensitive indicator of thyroid Extremely sensitive indicator of thyroid function.function.
Normal range: 0.27-4.2mU/LNormal range: 0.27-4.2mU/L (varies by lab) (varies by lab)– 95% of euthythyroid patients have TSH < 2.5mU/L 95% of euthythyroid patients have TSH < 2.5mU/L
(goal Rx in pts with hypothyroidism)(goal Rx in pts with hypothyroidism)
– Asymptomatic patients with TSH levels 3-6 mU/L Asymptomatic patients with TSH levels 3-6 mU/L should be followed for development of hypothyroidism.should be followed for development of hypothyroidism.

13
Thyroid Stimulating HormoneThyroid Stimulating Hormone
Decreased in primary hyperthyroidism Decreased in primary hyperthyroidism (Graves, toxic nodular goiter, etc.).(Graves, toxic nodular goiter, etc.).
Increased in primary hypothyroidism.Increased in primary hypothyroidism. New generation assays are sensitive New generation assays are sensitive
to .01mU.to .01mU. With rare exceptions, normal TSH With rare exceptions, normal TSH
excludes hypo/hyperthyroidism.excludes hypo/hyperthyroidism.

14
TSH and ScreeningTSH and Screening
Part of prenatal, mood disorder, atrial Part of prenatal, mood disorder, atrial fibrillation, wt change, dementia/delerium fibrillation, wt change, dementia/delerium and certain dyslipidemia work-ups.and certain dyslipidemia work-ups.
Almost always abnormal with Almost always abnormal with hypo/hyperthyroid states hypo/hyperthyroid states
Neonatal screeningNeonatal screening InexpensiveInexpensive Highly sensitive/specific marker of primary Highly sensitive/specific marker of primary
thyroid disease.thyroid disease.

15
Free TFree T44
Occasionally needed to confirm presence of Occasionally needed to confirm presence of hypo/hyperthyroidism.hypo/hyperthyroidism.
Direct measure of unbound TDirect measure of unbound T44 Useful in Useful in management of thyrotoxicosismanagement of thyrotoxicosis (severity (severity
and response to Rx).and response to Rx). Goal is FTGoal is FT44 in the normal range. in the normal range. May be normal in patients with TMay be normal in patients with T33 thyrotoxicosis; if thyrotoxicosis; if
TSH low, FTTSH low, FT44 normal and patient clinically normal and patient clinically hyperthyroid – essential to check total or free Thyperthyroid – essential to check total or free T33. .
Normal 9-24 pmol/L or 0.7-2.0 ng/dl (varies with Normal 9-24 pmol/L or 0.7-2.0 ng/dl (varies with method)method)

16
Anti-thyroid AntibodiesAnti-thyroid Antibodies
Autoimmune thyroid disease is common.Autoimmune thyroid disease is common. Antibodies elevated in Antibodies elevated in Hashimoto’s thyroiditisHashimoto’s thyroiditis
(vs TPO and Tg) and (vs TPO and Tg) and Graves diseaseGraves disease (see below) (see below) – the most common thyroid diseases.– the most common thyroid diseases.
TSH-R AB (TSAb) - Thyroid stimulating TSH-R AB (TSAb) - Thyroid stimulating hormone receptor antibodies (IgG) that stimulate hormone receptor antibodies (IgG) that stimulate gland activity. gland activity. – Also referred to as Also referred to as TSI: TSI: Thyroid Stimulating Thyroid Stimulating
Immunoglobulin Immunoglobulin – Elevated in 80% patients with Elevated in 80% patients with Graves diseaseGraves disease..– stimulatestimulate hormone production hormone production

17
Other TestsOther Tests
Total TTotal T4: 4: normal 5-11 ug/dL- screening as adjunct normal 5-11 ug/dL- screening as adjunct to TSH; to TSH; usually not neededusually not needed
Total and free TTotal and free T33: normal total is 95-190 ng/dL: normal total is 95-190 ng/dL RAIRAI131131 uptake/scan: Oral I uptake/scan: Oral I131131 taken up by thyroid; taken up by thyroid;
% uptake indicates activity. Scan provides picture % uptake indicates activity. Scan provides picture of the gland; useful for differentiating types of of the gland; useful for differentiating types of thyrotoxicosis and in f/u of thyroid cancer:thyrotoxicosis and in f/u of thyroid cancer:– Thyrotoxicosis: Diffuse (Grave’s) vs toxic noduleThyrotoxicosis: Diffuse (Grave’s) vs toxic nodule– Follow-up of patients treated for thyroid Follow-up of patients treated for thyroid
cancercancerrecurrent local disease or metastasesrecurrent local disease or metastases

18
Fine Needle AspirationFine Needle Aspiration
Definitive test for evaluating Definitive test for evaluating thyroid thyroid nodulesnodules; more information than scans.; more information than scans.
Essential for diagnosis of thyroid cancerEssential for diagnosis of thyroid cancer

19
Hypothyroidism Hypothyroidism
Autoimmune – Hashimoto’s ThyroiditisAutoimmune – Hashimoto’s Thyroiditis– Idiopathic- absence of anti-thyroid antibodiesIdiopathic- absence of anti-thyroid antibodies
Iatrogenic: post Rx with RAI for Iatrogenic: post Rx with RAI for hyperthyroidismhyperthyroidism
Congenital: 1/4000 newbornsCongenital: 1/4000 newbornsscreeningscreening Drug induced: amiodarone (hypo and Drug induced: amiodarone (hypo and
hyper)hyper) Secondary forms- hypothalamic or pituitary Secondary forms- hypothalamic or pituitary
disease (uncommon)disease (uncommon)

20
Autoimmune HypothyroidismAutoimmune Hypothyroidism
Symptoms may vary from mild to floridSymptoms may vary from mild to florid Goiter often present Goiter often present 4/1000 woman, 1/1000 men (annual incidence)4/1000 woman, 1/1000 men (annual incidence) Lymphocytic infiltration of gland – Lymphocytic infiltration of gland – early phase early phase
may be hyperthyroidism may be hyperthyroidism (release of stored (release of stored hormone)hormone) but end result is hypothyroidism. but end result is hypothyroidism.
TPO TPO and Tg antibodies- often high titers and Tg antibodies- often high titers Insidious onsetInsidious onset Diffusely enlarged, firm, finely nodular thyroid.Diffusely enlarged, firm, finely nodular thyroid.

21
Symptoms (Hypothyroidism)Symptoms (Hypothyroidism)
EarlyEarly Fatigue, LethargyFatigue, Lethargy Weakness, arthralgiasWeakness, arthralgias Cold intoleranceCold intolerance ConstipationConstipation Dry skin, hair lossDry skin, hair loss HeadachesHeadaches MenorrhagiaMenorrhagia
LateLate Slow speechSlow speech Altered mentationAltered mentation Muscle crampsMuscle cramps Hoarse voiceHoarse voice Weight gainWeight gain AmenorrheaAmenorrhea

22
SignsSignsEarlyEarly Thin, brittle nailsThin, brittle nails Thin, dry hairThin, dry hair Delayed DTR Delayed DTR
relaxationrelaxation
LateLate GoiterGoiter Facial/eyelid puffinessFacial/eyelid puffiness AlopeciaAlopecia BradycardiaBradycardia *Edema- non-pitting*Edema- non-pitting Pleural/Pericardial Pleural/Pericardial
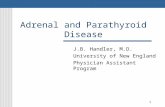
effusionseffusions*Myxedema: abnormal interstitial fluid accumulation *Myxedema: abnormal interstitial fluid accumulation (mucopolysacchrides) in skin giving it a waxy/coarsened (non-(mucopolysacchrides) in skin giving it a waxy/coarsened (non-pitting) appearance; pleural/pericardial effusions in severe cases.pitting) appearance; pleural/pericardial effusions in severe cases.

HypothyroidHypothyroid
Images.google.com

24
LabsLabs
Increased TSHIncreased TSH Decreased FTDecreased FT4 4 (not needed for eval or Rx)(not needed for eval or Rx)
Dyslipidemia – Dyslipidemia – TC & TC & tryglyceridestryglycerides, , HDLHDL
Anti-thyroid antibodiesAnti-thyroid antibodies Anemia, elevated LFT’s, lateAnemia, elevated LFT’s, late

25
ComplicationsComplications
CV – pericardial effusions, CV – pericardial effusions, cardiomyopathy, accelerated CHD, HFcardiomyopathy, accelerated CHD, HF
Encephalopathy- rare, can progress to Encephalopathy- rare, can progress to confusionconfusioncomacoma

26
TreatmentTreatment
Levothyroxine (Synthroid, Levoxyl, others)Levothyroxine (Synthroid, Levoxyl, others) Full replacement dose 1.6 ug/kg/dFull replacement dose 1.6 ug/kg/d Initiate 50-100 ug/day and titrate towards Initiate 50-100 ug/day and titrate towards
full dose full dose over timeover time, following TSH levels. , following TSH levels. Caution: age >60; patients with CHDCaution: age >60; patients with CHDlower lower starting dose, slower titration.starting dose, slower titration.
Check TSH levels every 2-3 mos. until normal Check TSH levels every 2-3 mos. until normal (0.5-2.5 mU/L for most patients)(0.5-2.5 mU/L for most patients)
Goal: clinically euthyroid state: symptoms Goal: clinically euthyroid state: symptoms improve slowly (months or more).improve slowly (months or more).

27
Congenital HypothyroidismCongenital Hypothyroidism
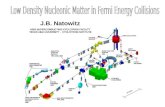
Early detection essential to prevent Early detection essential to prevent cretinismcretinism
Neonatal screening of TSH should Neonatal screening of TSH should eliminate this diseaseeliminate this disease
Replacement therapy 10-15 ug/kg/dReplacement therapy 10-15 ug/kg/d

CretinismCretinism
Google.images.com

29
HyperthyroidismHyperthyroidism
Thyrotoxicosis- clinical syndrome associated with Thyrotoxicosis- clinical syndrome associated with with excessive levels of thyroid hormone.with excessive levels of thyroid hormone.
Graves diseaseGraves disease Toxic/“hot” adenomas/nodule(s) Toxic/“hot” adenomas/nodule(s) Early phase of Hashimoto’s or sub-acute (viral) Early phase of Hashimoto’s or sub-acute (viral)
thyroiditis- self limited; release of stored hormonethyroiditis- self limited; release of stored hormone Factitious- excessive thyroid hormone intake Factitious- excessive thyroid hormone intake TSH secreting adenoma (rare)TSH secreting adenoma (rare) Amiodarone (both hypo and hyperthyroidism) Amiodarone (both hypo and hyperthyroidism)

30
Graves’ DiseaseGraves’ Disease
Most common cause of hyperthyroidismMost common cause of hyperthyroidism Autoimmune- TSH-R Ab (TSAb) - IgG Autoimmune- TSH-R Ab (TSAb) - IgG
antibodies (aka: antibodies (aka: TSITSI) directed to TSH ) directed to TSH receptor: over-activate glandreceptor: over-activate gland hypersecretion, hypertrophy and hypersecretion, hypertrophy and hyperplasia- goiter common. hyperplasia- goiter common.
8x more common in women8x more common in women Onset 20-40 year oldOnset 20-40 year old

31
SymptomsSymptoms
Hyperactivity, irritability, restlessness, anxietyHyperactivity, irritability, restlessness, anxiety Heat IntoleranceHeat Intolerance SweatingSweating PalpitationsPalpitations Fatigue, weakness Fatigue, weakness Increased appetite, weight lossIncreased appetite, weight loss DiarrheaDiarrhea Decreased libido, oligomenorrheaDecreased libido, oligomenorrhea

32
SignsSigns
TachycardiaTachycardia Arrhythmias Arrhythmias (ST, Afib)(ST, Afib)
Fine TremorFine Tremor Goiter/bruitGoiter/bruit Warm, moist skinWarm, moist skin Oily, fine hairOily, fine hair
Proximal muscle Proximal muscle weaknessweakness
OpthalmopathyOpthalmopathy DermopathyDermopathy HyperreflexiaHyperreflexia

Goiter Goiter
Google.images.com

34
Hyperthyroid LabsHyperthyroid Labs
Very low TSHVery low TSH – often <0.1 mU – requires – often <0.1 mU – requires sensitive TSH assay.sensitive TSH assay.
Total and Total and FTFT44 elevated (exception is T3 elevated (exception is T3
thyrotoxicosis- below); need to follow FTthyrotoxicosis- below); need to follow FT44 during during
treatment phase to document euthyroid state; TSH treatment phase to document euthyroid state; TSH may remain suppressed).may remain suppressed).
Do not need TSH-R Ab (TSI) for diagnosisDo not need TSH-R Ab (TSI) for diagnosis TT33 thyrotoxicosis in 2-5% of patients with Graves thyrotoxicosis in 2-5% of patients with Graves
– requires total or free T– requires total or free T33 for diagnosis. for diagnosis.

35
Opthalmopathy/DermopathyOpthalmopathy/Dermopathy
Unique to “Graves” disease; 20-40% of casesUnique to “Graves” disease; 20-40% of cases Proptosis/exophthalmos,“lid-lag”, conjunctival Proptosis/exophthalmos,“lid-lag”, conjunctival
inflammation/edema, corneal dryinginflammation/edema, corneal drying Pathology- lymphocytic infiltration of orbit, Pathology- lymphocytic infiltration of orbit,
muscles, eyelids; may cause diplopia and muscles, eyelids; may cause diplopia and compression of optic nerve.compression of optic nerve.
Skin: Non-inflammatory induration and plaque Skin: Non-inflammatory induration and plaque formation of pre-tibial areas leading to edema, formation of pre-tibial areas leading to edema, thickened skin with “orange skinned” appearance.thickened skin with “orange skinned” appearance.– ““Pre-tibial myxedema”Pre-tibial myxedema”

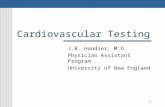
Graves OpthalmopathyGraves Opthalmopathy
Google.images.com
Proptosis/exopthamos
“lid lag”

Graves OpthalmopathyGraves Opthalmopathy
Elsevier Inc.
Severe exopthalmos

Graves DermopathyGraves Dermopathy
Images.google.com
“Pre-tibial myxedema”

39
ComplicationsComplications
Cardiac arrhythmias – ST, new onset Cardiac arrhythmias – ST, new onset atrial atrial fibrillationfibrillation
High-output cardiac failure – toxic, dilated High-output cardiac failure – toxic, dilated cardiomyopathy.cardiomyopathy.
Thyroid storm and crises – extreme Thyroid storm and crises – extreme thyrotoxicosis with delerium, high fever, thyrotoxicosis with delerium, high fever, dehydration and death. dehydration and death. UncommonUncommon with with current approaches to thyrotoxicosis.current approaches to thyrotoxicosis.

40
Treatment of GravesTreatment of Graves
Endocrinology consult essential Endocrinology consult essential if availableif available.. Propranolol – IV/PO will reduce symptoms and Propranolol – IV/PO will reduce symptoms and
stabilize heart. Dose 20-40 mg 4x/d, then stabilize heart. Dose 20-40 mg 4x/d, then conversion to long acting forms.conversion to long acting forms.
Thiourea drugs- Propylthiouricil (PTU) or Thiourea drugs- Propylthiouricil (PTU) or Methimazole- Methimazole- inhibit thyroid peroxidase and inhibit thyroid peroxidase and block organification of iodineblock organification of iodine; ; hormone hormone production. Useful in production. Useful in mild to moderatemild to moderate thyrotoxicosis, presence of small goiter.thyrotoxicosis, presence of small goiter.

41
Thiourea DrugsThiourea Drugs
Agranulocytosis (PTU>Methimazole) can occur- Agranulocytosis (PTU>Methimazole) can occur- essential to essential to follow WBCfollow WBC..
Pruritus (common) and allergic dermatitis occurPruritus (common) and allergic dermatitis occur Methimazole 30- 60 mg/dailyMethimazole 30- 60 mg/daily PTU 75-150 mg q.i.d. – also stops peripheral PTU 75-150 mg q.i.d. – also stops peripheral
conversion of Tconversion of T44TT33
Essential to monitor Essential to monitor FTFT44
Treat for 12-18 monthsTreat for 12-18 months Recurrent thyrotoxicosis in 50% Recurrent thyrotoxicosis in 50% after drug after drug
D/C’dD/C’d

42
Other Meds (Severe Sx - IO) Other Meds (Severe Sx - IO)
Saturated Iodine solution: Block Thyroid release Saturated Iodine solution: Block Thyroid release of hormone- of hormone- severe thyrotoxicosissevere thyrotoxicosis
Iodinated Contrast agents: Used for temporary Iodinated Contrast agents: Used for temporary relief of relief of severe thyrotoxicsevere thyrotoxic symptoms or thyroid symptoms or thyroid storm.storm.– Inhibit peripheral conversion of TInhibit peripheral conversion of T44TT33
– TT33 levels drop by up top 60% within 24 hours. levels drop by up top 60% within 24 hours. Glucocorticoids: Glucocorticoids: severe thyrotoxicosissevere thyrotoxicosis
– Inhibit peripheral conversion of TInhibit peripheral conversion of T44TT33
need for cortisol during thyroid stormneed for cortisol during thyroid storm
IO- interest only

43
Radioactive IodineRadioactive Iodine
Definitive therapyDefinitive therapy: : 131131I used to destroy I used to destroy overactive thyroid tissue.overactive thyroid tissue.
Preferentially concentrated by thyroid Preferentially concentrated by thyroid because of iodine component of because of iodine component of 131131I.I.
No associated risks of radiation. This has No associated risks of radiation. This has become become definitive treatment of choice in definitive treatment of choice in USA.USA.– Must avoid during pregnancy Must avoid during pregnancy

44
Radioactive Iodine (RAI)Radioactive Iodine (RAI)
Essential to follow FTEssential to follow FT44 and clinical status and clinical status
Permanent hypothyroidism often occurs within Permanent hypothyroidism often occurs within one year – thyroid replacement therapy then one year – thyroid replacement therapy then necessary for life.necessary for life.
OphthalmopathyOphthalmopathy may appear or worsen may appear or worsen following treatment, especially in following treatment, especially in smokerssmokers; does ; does not improve with RAI alone. Unclear as to why.not improve with RAI alone. Unclear as to why.– Rx with prednisone post RAI decreases Rx with prednisone post RAI decreases
progression/improves opthalmopathy in up to 2/3progression/improves opthalmopathy in up to 2/3rdrd of of patients.patients.

45
Thyroid SurgeryThyroid Surgery
No longer first line therapyNo longer first line therapy– Treatment of choice for Graves in children or Treatment of choice for Graves in children or
hyperthyroidism during pregnancy when sx hyperthyroidism during pregnancy when sx can’t be controlled with thiourea drugs. can’t be controlled with thiourea drugs.
Indicated in patients with recurrent Graves Indicated in patients with recurrent Graves following failed Rx with following failed Rx with 131131I.I.
Subtotal thyroidectomy performed with Subtotal thyroidectomy performed with preservation of parathyroid glands to preservation of parathyroid glands to prevent hypoparathyroidism.prevent hypoparathyroidism.

46
Graves’ PrognosisGraves’ Prognosis
Recurrences common if only treatment is Recurrences common if only treatment is thioureathiourea, and sometimes occur post , and sometimes occur post 131131I or I or subtotal thyroidectomy.subtotal thyroidectomy.
Cardiac, ocular and psychological Cardiac, ocular and psychological complications may persist following complications may persist following treatment.treatment.
Post treatment hypothyroidism is common Post treatment hypothyroidism is common but easily treated with replacement Rx.but easily treated with replacement Rx.

47
Thyroid NodulesThyroid Nodules
Evaluation essential; may be single or Evaluation essential; may be single or multiplemultiple likely to be found on PE. likely to be found on PE.
When single, usually a benign adenoma or When single, usually a benign adenoma or colloid cyst, but colloid cyst, but cancercancer is a possibility. is a possibility.
Nodules may hypersecrete thyroid hormone Nodules may hypersecrete thyroid hormone leading to thyrotoxicosis “hot nodule”.leading to thyrotoxicosis “hot nodule”.
Fine needle aspirate essentialFine needle aspirate essential to exclude to exclude thyroid cancer.thyroid cancer.

48
Toxic Thyroid NodulesToxic Thyroid Nodules
Present with thyrotoxicosis (no eye/skin Present with thyrotoxicosis (no eye/skin findings).findings).
Nodules may be single (young) or multiple Nodules may be single (young) or multiple (elderly).(elderly).
Treatment of solitary nodule:Treatment of solitary nodule:RAI is preferred over surgery for patients > RAI is preferred over surgery for patients > 40 y/o; surgery or RAI if younger40 y/o; surgery or RAI if younger
Treatment of multinodular goiter- RAITreatment of multinodular goiter- RAI

49
Thyroid CancerThyroid Cancer
30,000 cases/yr/USA; 3x 30,000 cases/yr/USA; 3x incidence in women.incidence in women. Most are well differentiated, slow growing and Most are well differentiated, slow growing and
treatable, often with cure. treatable, often with cure. Do notDo not effect thyroid effect thyroid function.function.
76% are papillary Ca, 16% follicular Ca.76% are papillary Ca, 16% follicular Ca. Risk factor: prior head and neck radiation or Risk factor: prior head and neck radiation or
radiation exposure.radiation exposure. PE: PE: firm, non-tender nodulefirm, non-tender nodule Dx via FNA, ultrasound of neckDx via FNA, ultrasound of neck

50
TreatmentTreatment
Surgery- near total thyroidectomy with Surgery- near total thyroidectomy with preservation of parathyroid gland(s). preservation of parathyroid gland(s).
Post-op suppression therapy with Post-op suppression therapy with levothyroxine to suppress TSH stimulation levothyroxine to suppress TSH stimulation of any remaining thyroid tissue.of any remaining thyroid tissue.
Follow up total body RAI scan to detect any Follow up total body RAI scan to detect any remaining thyroid tissue/metastasis with remaining thyroid tissue/metastasis with further treatment (further treatment (131131I) if indicated.I) if indicated.