1 Texas and National Health Reform: Overview and Update Webinar You must dial in to hear the audio...
35
1 Texas and National Health Reform: Overview and Update Webinar You must dial in to hear the audio for this presentation! Phone number: 1.866.740.1260 Access code: 3200112
-
Upload
nathan-richard -
Category
Documents
-
view
214 -
download
1
Transcript of 1 Texas and National Health Reform: Overview and Update Webinar You must dial in to hear the audio...

1
Texas and National Health Reform: Overview and Update Webinar
You must dial in to hear the audio for this presentation!
Phone number: 1.866.740.1260 Access code: 3200112

2
Texas and National Health Reform: Overview and Update Webinar
October 6, 2009
Eva DeLuna Castro, Senior Fiscal Analyst, [email protected] Kymberlie Quong Charles, TVHR Coordinator, [email protected]
Anne Dunkelberg, Associate Director, [email protected] Stacey Pogue, Senior Policy Analyst, [email protected]
Center for Public Policy PrioritiesPhone (512) 320-0222 (X102) – www.cppp.org
www.texasvoiceforhealthreform.org

3
Texas Voice for Health
Reform Principles1. Affordable access to good health care must be available for all Americans.
It should:• Be affordable for people at all income levels • Remain available and affordable when family and economic circumstances change• Establish both a responsibility for the public to contribute and an assurance of cost
containment for individuals and families• Eliminate health costs as the #1 cause of bankruptcy in America.
2. A decent standard of comprehensive care must be established. It should:• Keep people healthy and treat them when they’re ill• Cover the whole person• Not be lost or reduced based on pre-existing conditions or pregnancy
• These first 2 steps will not happen by accident: Americans must choose to do this and demand it.
3. To be effective, sustainable, equitable, and balanced with our other important priorities as a nation, national health reform should also address safe and high quality care; costs and cost-effectiveness of health care; consumer choice; and eliminating non-financial barriers to care
• Just working on Step 3 will not make Steps 1 or 2 happen.

4
Texas: the Most to Gain
• In 2008, Texas remained the state with the highest uninsured rate in the nation (24.1%) with an uninsured population that now tops 6 million people.
• With so many Texans lacking health security, Texas has more to gain than other states from national health reform legislation, which the Congressional Budget Office projects will cover 94 percent of Americans under age 65.

5
Texas Worst Among the States
Texas: 24.1%
Massachusetts: 4.1%
U.S. average: 15.1%
All Ages, 2008

6
Almost All Congressional Districts Worse than U.S. Average
% Uninsured (All Ages) by U.S. Congressional District, 2008
U.S. average: 15.1% — Texas average: 24.1%
Inset: Dallas/ Fort Worth
Inset: Houston Area
District 3
District 26
2432
7
District 16
2815
27
2520

7
For Children, All Districts are Worse than U.S.
% Under 18 Uninsured by U.S.
Congressional District, 2008
U.S. average: 9.9% — Texas average: 17.8%
Inset: Dallas/ Fort Worth
Inset: Houston AreaDistrict 16
28
15
27
2520
District 3
32
11

8
0
5
10
15
Under 19 19 to 64 65 and over
Millions of Texans
Job-based coverage Medicaid Medicare Uninsured
Working-Age Texans Are Most Likely to be Uninsured
19% uninsured
3% uninsured
32% uninsured
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

9
57.4 56.253 53 54 53.1 52.2
50.4 49.5
64.2 63.2 61.9 61 60.5 60.2 59.7 59.3 58.5
30
45
60
75
2000 2001 2002 2003 2004 2005 2006 2007 2008
% of Residents With Job-Based Insurance
Employer-Sponsored Coverage Declining in Texas and Nationwide, Even Before Recession
U.S. Average
Texas
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

10
Only the Highest-Income Families Have Better-Than-U.S.-Average Chance of Being Insured
Texas average: 25.1%
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html
12%
29%
35%
42%
Below poverty 100 to 200% ofpoverty
200 to 300% ofpoverty
Above 300% ofpoverty
11%
16%
24%
34% 36%
Below $25,000 $25,000 to $49,999 $50,000 to $74,999 $75,000 to $99,999 $100,000 and over

11
12%
30%
37%
22%
15%
White Black Hispanic Asian All Other
Uninsured Problem Especially Bad for Young Adults, Hispanics
Texas average: 25%
19%
46%
36%
23%
3%
Under 19 19 to 24 25 to 44 45 to 64 65+
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

12
U.S.-born citizen
68%
Naturalized U.S. Citizen
6%
Not a U.S. Citizen
26%
Uninsured by Citizenship Status, 2007-08 Average
Most Uninsured Texans are U.S. Citizens
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

13
Over 400%8%
300 to 400% of poverty
8%
200 to 300% of poverty
20%
100-200% of poverty
33%
Below 100% of poverty
31%
Uninsured Texas Children (0-18) in
2007-08, By Family Income
Source: March 2008 and 2009 CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html
Total Uninsured Children: 1.418
million

14
IT'S NOT CROWDOUT!!Since 2003, Texas Kids in Moderate to High Income
Families Saw the Biggest Increases in Number of Uninsured
4.3%
-5.0%
29.5%
16.4%
Below 100% 100% to below 200% 200% to below 300% 300% and above
Source: 3-year average data (2002-2004 vs. 2006-2008) for children ages 0-18, Current Population Survey, U.S. Census Bureau
Number of Uninsured Kids betw een 100-
200% poverty declined
Wor
seB
ette
r

15
• Three bills drafted: Senate Finance; Senate HELP; House “Tri-Committee” (E&C, W&M, Ed & Labor)
– Senate Finance: Most influential, least adequate in affordability– HELP: Most adequate affordability, Kennedy Bill
• HELP-Finance merger process will begin as soon as Finance votes. • Senate Leadership hopes to merge quickly and hold floor vote after Columbus Day.
They still hope to move a package under “regular order,” rather than through the reconciliation process.
– House: 3 committees’ amendments must be merged before a full House vote can happen. • Leaders pare back the bill’s $1.2 B price tag while trying to preserve key provisions-- e.g.
the subsidy structure. • Leaders still hope to bring the bill to the House floor in mid-October.
• House-Senate compromise process starts as soon as Chambers vote their bills.
• If successful, bill could be voted on and signed in November, December.
• If no deal reached, large portions of (but not all of) reform can/will be passed through “Budget Reconciliation,” but this is less than ideal, both politically and from policy standpoint.
– Budget Reconciliation only requires 51 Senate votes, but limits what you can do.
Health Reform Process

16
• Key elements of all 5 bills:– Builds on current system: If you like what you have now, you can keep it.
– Medicaid expansion (e.g., cover all up to 133% of poverty (FPL): $14,404 for one; $29,327 for 4).
– Reform Private Health Insurance: standardize benefits, limits on price variation, no denial of coverage, no excluding pre-existing conditions, no annual or lifetime maximums. Changes focused on individual and small employer coverage.
– Create health insurance exchanges where participating private options can be compared and purchased (like Amazon or Travelocity for insurance).
• Will there be a Public or Non-profit plan option?
• Exchange is just a framework: depends on subsidies, market reforms, standardized benefits, individual mandate, and inclusion of most sellers to be effective
– Premium assistance up to 300% or 400% of FPL? ($66,150 to $88,200 for family of 4)
• What is maximum % of family income you must spend before getting help?
– Out-of-pocket caps, too, to ensure real affordability/end (reduce?) medical bankruptcy
• Needed at EVERY income level, including folks ABOVE the premium subsidy level.
– Individual mandate to have coverage: but only if affordable coverage exists!
– Requirements for employers to contribute, with exemptions for smallest employers;
• Problematic SF “free rider” idea requires firms to pay for only employees who get premium assistance; opposed by advocates for low-income Americans because creates disincentive to hire low-income and single-parent workers.
Health Reform Basics

17
• Will premiums and out-of-pocket be affordable for ALL?
– low-and moderate income families need both adequate help with premiums, and caps on out-of-pocket spending.
– Middle-income and up need affordable, predictable premiums and out-of-pocket caps.
• Small Business: encouraging employer responsibility without excessive new costs.
• Children: Maintain comprehensive coverage and out-of-pocket protections in the transition to reform?
• Public plan is not more important than affordable access for all. Public plan is one tool to reduce overall coverage costs. But Germany, the Netherlands and Switzerland all have universal, secure coverage with no public option.
Policy: Some Top Health Reform
Concerns

18
Affordability is Key to Successful Reform
• Special considerations:– Low- and moderate-income populations– People with high medical costs– Small employers
• Components of affordability:– Premiums (including rate variation, e.g. age rating)– Out-of-pocket medical costs – Covered benefits– Employer contribution– Exceptions (individual mandate and exchange access with ESI)
• If reform requires people to buy coverage, coverage must be affordable at all income levels. If affordability provisions are not done well:– People may be required to buy coverage they can’t afford or pay
penalties, leaving them unable to pay for other necessities; or– Bills will have to exempt more people from the coverage requirement,
further reducing universal coverage.

19
Senate Finance Bill is Less Affordable for Low-Income Individuals
% FPL $ amount (family of
three)
Premium $ (% of income)
Maximum Out-of-Pocket Costs (% of income)
Premium $ (% of income)
Maximum Out-of-Pocket Costs (%
of income)133% $24,352 $0 (Medicaid) n/a (Medicaid) $901 (3.7%) $3,867 (16%)150% $27,465 $275 (1%) $2,320 (8%) $1,236 (4.5%) $3,867 (14%)200% $36,620 $1,208 (3.3%) $2,320 (6%) $2,563 (7.0%) $5,800 (16%)250% $45,775 $2,563 (5.6%) $5,800 (13%) $4,349 (9.5%) $5,800 (13%)300% $54,930 $4,339 (7.9%) $5,800 (11%) $6,592 (12.0%) $7,733 (14%)350% $64,085 $6,537 (10.2%) $11,600 (18%) $7,690 (12.0%) $7,733 (12%)400% $73,240 $9,155 (12.5%) $11,600 (16%) $8,789 (12.0%) $7,733 (11%)
% FPL$ amount (family of
three)
Premium $ (% of income)
Maximum Out-of-Pocket Costs (% of income)
Premium $ (% of income)
Maximum Out-of-Pocket Costs (%
of income)133% $24,352 $365 (1.5%) $900 (4%) $365 (1.5%) $900 (4%)150% $27,465 $824 (3%) $1,450 (5%) $824 (3%) $1,450 (5%)200% $36,620 $1,831 (5%) $4,400 (12%) $,2014 (5.5%) $4,400 (12%)250% $45,775 $3,204 (7%) $7,450 (16%) $3,662 (8%) $7,450 (16%)300% $54,930 $4,944 (9%) $8,520 (16%) $5,493 (10%) $8,520 (16%)350% $64,085 $6,409 (10%) $8,520 (16%) $7,049 (11%) $8,520 (16%)400% $73,240 $8,056 (11%) $10,000 (14%) $8,789 (12%) $10,000 (14%)
Income Senate Heath, Education, Labor, and Pensions
Senate Finance(Chairman’s mark revised 9/22)
Income House Education and Labor and Ways and Means
Committees
House Energy and Commerce Committee
A family just over 150% FPL would pay much higher premiums and
OOP costs under the SFC bill than
the other versions.
For the most part, bills do not protect against being underinsured (health coverage that does not adequately protect against high medical expenses). The Commonwealth Fund standard includes out-of-pocket medical expenses exceeding 5% of income for families under 200% FPL and 10% for others.

20
Reform Help Targeted at Small Employers
• All bills protect small employers from new, high costs for coverage by excluding them from employer coverage mandates
– House bill: exempts employers with annual payrolls less that $500,000 (82% of Texas businesses)
– Senate HELP: exempts employers with 25 or fewer workers (67% of Texas businesses)– Senate Finance: exempts employers with 50 or fewer workers (72% of Texas businesses)
• Generous tax credits will help small employers offer coverage– House bill: fewer than 25 employees & average annual wages under $40K. Credit up to 50%
of the premium cost.– Senate HELP: fewer than 50 employees & average annual wages under $50K. Credit up to
$2,000 per employee– Senate Finance: fewer than 25 employees & average annual wages under $40K. Credit up
50% of the employers contribution.
• Penalties for mid-size and large employers who do not offer coverage vary, but are less than the costs of coverage.
– For example, under the House Energy and Commerce Committee bill, a business with 30 full-time employees and a payroll of $750,000 could either provide health insurance at a cost of around $108,000 a year (to cover 75 percent of the premium for employee-only coverage) or pay an assessment of $60,000 (8 percent of payroll). Under the Senate HELP bill, that same business would face a penalty of just $3,750, but would also qualify for tax credits if it provides coverage.
• Standards for mid-size and large employer contributions toward coverage (60-72.5% of premiums) will help ensure affordability for employees.

21
Reform will Reduce Rate Variation for Small Employers
Average Annual Per-Worker Premium
MAXIMUM Annual Per-Worker Premium
$3,851 $22,413
Average and Maximum Rates Being Paid by Texas Small Employers(2006 market average for businesses with 2-50 employees)
• Small employer premiums in Texas today can vary by a factor of 26:1 – greater variation than most states.
• Rating factors used today that will be prohibited by reform: health status; gender; industry type; number of employees.
• In the exchange, rates will vary only by geography (reflects regional differences in medical costs) and age (also tobacco use in SFC bill).
• Senate Finance allows 4:1 variation for age; Senate HELP and House have a much better 2:1 limit.
House Tri-Comm Senate HELP Senate Finance
annual premium (% of income at 401% FPL for individual)
annual premium (% of income at 401% FPL for individual)
annual premium (% of income at 401% FPL for individual)
24 $2,730 (6.3%) $3,042 (7%) $2,153 (5%)64 $5,460 (12.6%) $6,084 (14%) $8,614 (19.8%)
Age
22
Health Care: Family Budget Wild CardUnlike food, shelter, transportation, and education, the cost of needed
health care varies wildly across otherwise similarly situated families
• A family with serious chronic condition, illness or injury may need hundreds of thousands of dollars in care in a year, while one with routine needs may need only thousands for basic preventive and primary care.
Current public programs:
• cover too few adults,
• end coverage abruptly at arbitrary income points (“cliffs”), creating disincentives for increased earnings
• Often present major barriers to enrollment by eligible persons
In Private marketplace:
• No system TODAY to ensure that all can purchase coverage at or near the average cost; thus average costs are meaningless - can even be misleading
• No system TODAY to fully address (in a progressive manner) the mismatch between AVERAGE costs of family coverage ($13,000-$14,000 a year) and median family incomes: e.g., ~$47,000 overall, $64,000 family of 4

23
Health Reform and Family Self-Sufficiency:Bootstraps Out of Poverty
Social Security, Medicare, SSI, and Medicaid coverage of long-term care (70% of U.S. nursing home residents) have made it possible for the generations since their creation to develop assets for home ownership, higher education, and general economic advancement.
Without these programs, income and assets would have been devoted to the care of parents.
A progressively financed system of affordable comprehensive care for every income level will have a similar effect on enabling many more families in poverty to reach and hold middle-class income and assets.
Also: Child well-being is directly improved when parents have access to physical and behavioral health care they need.

24
• Every Texan will have new health security. You cannot lose, be denied, or priced out of coverage no matter your age, health status, or employment status.
• Annual caps on out-of-pocket costs and no annual/lifetime benefit limits mean critical financial protection at all income levels that does not exist today.
• About 4.5 million Texans would gain coverage
– About 1 million uninsured Texan adults would get Medicaid—up to 133% FPL
– About 2.3 million uninsured Texans would get premium assistance--above Medicaid and below 400% of poverty ($88,200 for family of 4)
• Small businesses and individuals can pay what large businesses do for health insurance. Under Texas law today, small employers pay an average high premium of $22,000 a year for a single worker.
• Depending on wages they pay, businesses with fewer than 25 employees (67% of Texas businesses) can get tax credits to cover up to ½ the cost of coverage.
Benefits of Health Reform

25
• Medicaid expansion—up to 133% FPL.
– CPPP conservatively estimates Medicaid expansion (1 million adults at current costs) will add $3.9 billion a year in new federal dollars to the Texas economy ($3.5 billion if 90% federal share); with a multiplier effect of $10 to $13 billion a year, and
– Could convert Texas from being a “donor state” that sends more to DC in taxes than we get back by covering low-income adults in Medicaid.
– What share will Texas have to pay for required Medicaid expansions & increased Medicaid provider payment rates?
• 100% federally funded in House proposal; E&C amends to 90% from year 3 onward
• Senate Finance uses a more complicated formula with a similar effect (i.e., ~ <10% state share)
• 10% state share would mean $391 million state cost to pull down $3.5 billion federal funds, a one-year net gain of $3.1 billion to the state economy.
• Premium subsidies—up to 400% FPL
– even more funding will flow to Texas from premium assistance to low-to-moderate income families (Estimates likely available once House and Senate settle on bills).
• Goal is to make the final bill 100% paid for (combo of cuts/savings and new revenues); if “pay-fors” are cut, expect to see loss of affordability and/or health benefits!
Cost of Health Reform

26
Recent Quotes by Sen. Cornyn
On Sept.22nd, Senator Cornyn cited preliminary estimates of the impact of the Senate Finance health reform bill, produced by the Texas Health & Human Services Commission (HHSC).
• The Senator stated that Texas Medicaid program costs would increase by “$20.4 billion over
10 years” and said that 2.5 million more Texans would end up “on a government plan.”
• HHSC’s model is generally reasonable, though:– Some questionable key assumptions do result in dramatically higher numbers. – The way their numbers were quoted inflates the costs and disregards the benefits.
Big Picture:
• Gain in federal funding is 6 times more than cost to the state: Net increase in federal funding of $124 billion compared to state investment of $20.4 billion.
Numbers are Still In Flux:• Range of estimates between CBO, Senate Finance, National Governors Association, and
Texas HHSC suggests that we need to look more deeply into all the projections, and not rely too heavily on these preliminary efforts.
– SF predicts an increase in state-dollar layout from 2010 to 2019 (different period from HHSC’s model) of $2.9 billion, or a 2.8% increase above the baseline without reform.
– CBO projects total net increase in Medicaid and CHIP 2010-2019 of 11 million nationwide;
– HHSC’s projected net increase of 1.7 million Medicaid, plus 768,000 in CHIP would mean Texans would make up an unlikely 23% of CBO’s assumed total national enrollment growth in Medicaid and CHIP (Texans just 13% of nation’s uninsured)

27
More on HHSC’s Preliminary Estimate
Texas HHSC’s numbers are significantly higher than CBO, SF because:
• Texas HHSC assumes very high percentage of eligible Texans (94%, vs. current 78%) will enroll in Medicaid, and
• Texas HHSC projects costs for 10 years (instead of the 7 used by CBO); – thus producing a bigger number primarily due to inflation and population growth. – This means the numbers cannot be compared to any of the CBO, SF, or NGA official
estimates, which are based on 2010-2019. • Even at the $20.4 billion figure, the cost of reform would be 8% higher than the cost of
the status quo, to cover 2.5 million more Texans (in a program that covers 2.9 million Texans today).
• Our state must pay more to catch up to what other states are already doing, because we have been stingy historically, not because reform is too costly.
• Of the $20.4 billion HHSC estimates, about $8.4 billion is due to Medicaid and CHIP expansion (less than a 4% increase over current Medicaid trend).
• The remainder is due to:
– removing red-tape barriers and bureaucratic failures that keep eligible children out of Medicaid today; plus
– $6 billion if the state takes over paying its share of bonus (DSH) hospital payments that currently are borne by local hospital districts. These are Texas legislative choices.
• Reference to 2.5 million uninsured Texans being added to “government” health care includes some 768,000 kids who would be covered with private insurance through their parents and the health insurance exchange, but protected by a CHIP “wrap-around.”

28
• Having 5 different bills has made educating folks tough
• Supporters of Health Reform must be heard loudly in D.C.
– Texans should not “sit out” health reform
– Don’t let health care vested interests and far right be the only voices!
– Tell Congress what matters to YOU
• Those who believe real reform is needed should tell our elected officials and communicate that strong support FIRST, before your special issues or concerns.
• POSTIVE MESSAGES MUST BE REPEATED OFTEN (not just corrections to lies)
Consumer Voices Are Needed in Health
Reform!
29
Get Involved with Texas Voice for Health Reform
•Join our email list for the latest updates on national health reform
•Follow us on Facebook and Twitter
•Visit www.texasvoiceforhealthreform.org for Fact Sheets, MythBusters, News and More
•Get your organization involved in organizing for health reform by joining the TVHR Partner’s Network (email [email protected] to join)
•Communicate with your elected representatives using the tools in our online Citizen Advocacy Center: calls, letters Congress and newspapers, op-eds needed!
•Educate your community, congregation, friends and family using Texas Voice for Health Reform Resources
•Contribute to our Story Bank project
www.texasvoiceforhealthreform.org

30
Use of This Presentation
The Center for Public Policy Priorities encourages you to reproduce and distribute these slides, which were developed for use in making public presentations.
If you reproduce these slides, please give appropriate credit to CPPP.
The data presented here may become outdated.
For the most recent information or to sign up for our free E-Mail Updates, visit www.cppp.org.
© CPPP
Center for Public Policy Priorities900 Lydia StreetAustin, TX 78702
P 512/320-0222 F 512/320-0227

31
Additional Materials

32
Senate Finance Senate H.E.L.P. House 3-Committee
Medicaid to 133% FPL. Medicaid to 150% FPL Medicaid to 133% FPL
Reform Small Group 1-50; allows 4:1 for age; total premium range of 7.5:1.
Reform All Coverage (except large self-insured); Max range 2:1 for age.
Reform ALL private insurance: Max range 2:1 for age.
Health Insurance Exchange:•State-based•Nonprofit coop instead of public option
Health “Gateways”: • state-based• Public Option
Health Insurance Exchange:•national•Public Option
Individual Mandate: exempt if lowest premium >8% of income; income <100% FPL; other “hardship.” Penalty = $1,500/family at 100-300% FPL; and $1,900/family > 300% FPL
No penalty under <150% FPL; penalty = 50% of price of least expensive qualifying plan for others; IRS collects.
Penalty of 2% tax on income, not to exceed average cost of a basic health plan; hardship exemptions.
Premium Help: to 400% FPL, cap at 12% of income
Out-of-Pocket limit: $5,800 individual; $11,600 for a family
Premiums: to 400% FPL, cap at 12.5% of income
OOP limit: X% family income (not set yet)
Premiums: to 400% FPL, cap at 10% of income
OOP limit: $5,000 individual; $10,000 for a family
Employer Responsibility: pay fine only for workers getting premium help in exchange (exempt under 50 workers)
Cover, or pay $750/yr per worker (exempt under 25 workers)
Cover, or pay 8% of payroll. (Some small firms exempt, and some tax credits for small businesses)
* As of 10/5/09
33
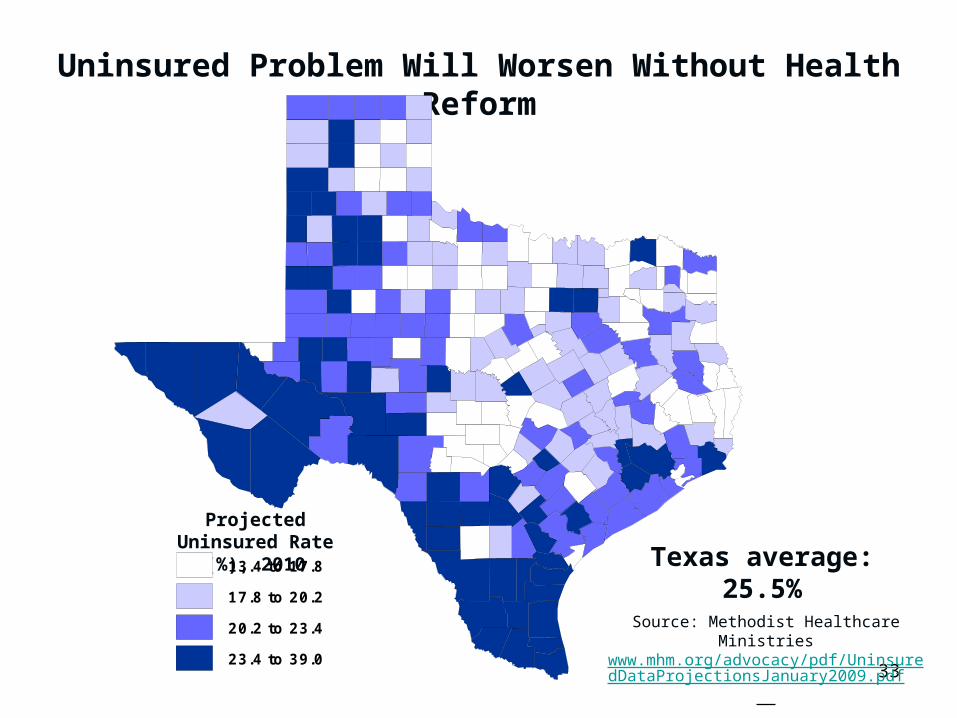
Uninsured Problem Will Worsen Without Health Reform
Projected Uninsured Rate (%), 2010
Source: Methodist Healthcare Ministrieswww.mhm.org/advocacy/pdf/UninsuredDataProjectionsJanuary2009.pdf
13.4 to 17.8
17.8 to 20.2
20.2 to 23.4
23.4 to 39.0
Texas average: 25.5%

34
Employed65%
Unemployed7%
Not in Labor Force28%
Uninsured by Labor Force Status, 2007-08 Average
2 Out of 3 Uninsured Working-Age Texans Have a Job
Source: CPS Annual Social & Econ. Supplementwww.census.gov/hhes/www/hlthins/hlthins.html

35
Medicare • NO CUTS to Medicare benefits • Changes to slow the growth rate of Medicare costs (shores up Medicare’s finances) • Ends subsidies to private health insurance companies that cost 14% more than regular
Medicare • HOUSE Phases out Part D “donut hole.” • No rationing in Medicare based on age, life-expectancy, disability, etc.
End-of-Life-Care Planning (living wills, advance directives)• NO provisions to encourage euthanasia• Will let doctors get reimbursed (for first time) for discussing end-of-life planning with patients• Planning is completely voluntary• Planning cannot presume the withdrawal of treatment of encourage hastening of death• These provisions may end up removed from reform because of the disinformation campaign
Undocumented Immigrants • Health reform does not include undocumented immigrants• Just like today, they are explicitly excluded from Medicaid or CHIP• They are explicitly excluded from premium subsidies
Reform Basics: Truth vs. Big Fat Lies





![CUBE Media Proxy - Cisco · media-recording proxy [dial-peer-tag1 dial-peer-tag2 dial-peer-tag3 dial-peer-tag4 dial-peer-tag5] Example: Step4 Note Youcanspecifymaximumoffivedial-peertags.](https://static.fdocuments.in/doc/165x107/600896c15662324ac908e474/cube-media-proxy-cisco-media-recording-proxy-dial-peer-tag1-dial-peer-tag2-dial-peer-tag3.jpg)