
1 s2.0-s0099239908009382-main
4
Defects in Nickel-Titanium Instruments after Clinical Use. Part 2: Fractographic Analysis of Fractured Surface in a Cohort Study Ya Shen, DDS, PhD,* Gary Shun-pan Cheung, BDS, MDS, MSc, PhD, † Bin Peng, DDS, PhD, ‡ and Markus Haapasalo, DDS, PhD* Abstract The purpose of this study was to investigate the mode of failure of three brands of nickel-titanium (NiTi) instruments (ProTaper [Dentsply Maillefer, Bal- laigues, Switzerland], ProTaper for Hand Use [Dentsply Maillefer], and K3 [SybronEndo, Orange, CA]) that sep- arated during clinical use. A total of 79 fractured in- struments were collected from three endodontic clinics over 16 months. The fracture surface of each fragment was examined by scanning electron microscope. Most of the rotary instruments (78% of K3 and 66% of ProTaper) failed because of fatigue fracture, whereas 91% of NiTi hand instruments failed as a result of shear (p 0.01). The fracture mode of shaping files in rotary ProTaper was different between two different clinics (p 0.05). All surfaces with fatigue fracture (n 47) revealed the presence of either one or two crack ori- gins. The vast majority (86%) of K3 fatigue failure had two crack origins that could be found not only at the cutting edge but also at various places along the flute compared with only 28% of ProTaper showing multiple crack origins (p 0.01). The latter showed one crack origin in 81% of the fatigued shaping files but only 37% for finishing files (p 0.01). The results of this study indicated that the failure mode of NiTi instruments is related to preparation technique. (J Endod 2009;35: 133–136) Key Words Clinical, failure, fatigue, nickel-titanium, rotary instru- ment, shear N onsurgical root canal treatment has benefited from the introduction of nickel- titanium (NiTi) rotary instruments (1). However, there is an increasing concern about instrument fracture, as evidenced by the amount of reports on this problem (2–9). A recent survey of endodontic specialists and general dental practitioners in the United Kingdom has indicated that the great majority (92.6%) of endodontists used NiTi rotary systems. The majority of users (93.6% of endodontists and 79.5% of general practitioners) had experienced instrument fracture (10). Increasing numbers of NiTi rotary instruments of various designs are now marketed; new instruments and materials seem to appear faster than clinicians could learn about the preceding versions. This has created an educational challenge for practitioners, universities, and manufacturers, requiring a greater degree of cooperation among these groups than ever before. Clini- cians should use only those instruments and materials shown to be safe and effective in independent studies. Although a number of studies have attempted to examine the reasons for fracture of NiTi rotary instruments after clinical or simulated use (2, 6, 11, 12), very few have performed a systematic examination of the fracture surface to identify the mode or mechanism of fracture. A large-scale clinical study can provide detailed and reliable information about the mechanism of fracture on different NiTi instruments and con- tribute to better understanding of how and why the fracture occurs. Such knowledge is important for the prevention of instrument fracture. Therefore, the aim of this study was to investigate the mode of fracture in NiTi instruments discarded from different clinics to identify the fracture mechanism. Materials and Methods Three NiTi rotary systems: ProTaper rotary (PT) (Dentsply Maillefer, Ballaigues, Switzerland), ProTaper for Hand Use (PHU) (Dentsply Maillefer), and K3 (SybronEndo, Orange, CA) have been adopted at three endodontic clinics, each in a stomatologic school in China (Beijing, Guangdong and Wuhan). Two clinics (A and B, identity not revealed) used only the PT instruments, and the other (clinic C) used both PHU and K3 instruments (by different endodontists who consistently used only one of the three brands). There was a guiding principle in each clinic for their use. Each instrument was a limited to maximum number of uses according to the tooth being treated: 30 root canals in clinic A (PT); 16 canals (for molars) to 30 canals (other teeth) in clinic B (PT), 16 canals (for molars) to 25 canals (other teeth) in clinic C either by PTU or K3. Instruments would also be discarded after a single use in very complex, severely curved, or calcified canals. The collection of clinically used NiTi instruments has been described earlier (13). In short, a total of 79 fractured instru- ments were collected from these three clinics over a 16-month period from January 2006 to April 2007. The fractured instruments were ultrasonically cleaned and auto- claved. The length of the fractured segment was examined under a stereomicroscope (Microdissection; Zeiss, Bernried, Germany) at 30 magnification with a precision of 0.1 mm. The separated fragment was then mounted so that its long axis was normal to the microscope stage for fractographic examination under scanning electron micro- scope (SEM) (Stereoscan 260, Cambridge Instruments, Cambridge, UK). The mode of fracture was classified as “fatigue” or “shear” according to Cheung et al. (14). From the *Division of Endodontics, Department of Oral Biological & Medical Sciences, Faculty of Dentistry, University of British Columbia, Vancouver, Canada; † Area of Endodontics, Faculty of Dentistry, The University of Hong Kong, Hong Kong SAR, China; and ‡ Key Laboratory of Oral Biomedical Engineer- ing of Ministry of Education, School and Hospital of Stoma- tology, Wuhan University, Wuhan, China. Supported in part by Post-Doctoral Fellowship Awards, Faculty of Dentistry, University of British Columbia, Canada. Address requests to reprints to Dr Markus Haapasalo, Division of Endodontics, Oral Biological and Medical Sciences, UBC Faculty of Dentistry, 2199 Wesbrook Mall, Vancouver, BC, Canada V6T 1Z3. E-mail address: markush@interchange. ubc.ca. 0099-2399/$0 - see front matter Copyright © 2008 American Association of Endodontists. doi:10.1016/j.joen.2008.10.013 Basic Research—Technology JOE — Volume 35, Number 1, January 2009 Defects in N.T. Instruments after Clinical Use. Part 2 133
-
Upload
cabinet-lupu -
Category
Education
-
view
7 -
download
0
Transcript of 1 s2.0-s0099239908009382-main

DPCYa
ATm(lMasowoP9(P(rgtcccofir1
KCm
BoFSit
F
DUBu0
d
Basic Research—Technology
J
efects in Nickel-Titanium Instruments after Clinical Use.art 2: Fractographic Analysis of Fractured Surface in aohort Study
a Shen, DDS, PhD,* Gary Shun-pan Cheung, BDS, MDS, MSc, PhD,† Bin Peng, DDS, PhD,‡nd Markus Haapasalo, DDS, PhD*
Na(Urprscrci
opmititt
S(siPtittecim2c(0ts
bstracthe purpose of this study was to investigate theode of failure of three brands of nickel-titanium
NiTi) instruments (ProTaper [Dentsply Maillefer, Bal-aigues, Switzerland], ProTaper for Hand Use [Dentsply
aillefer], and K3 [SybronEndo, Orange, CA]) that sep-rated during clinical use. A total of 79 fractured in-truments were collected from three endodontic clinicsver 16 months. The fracture surface of each fragmentas examined by scanning electron microscope. Mostf the rotary instruments (78% of K3 and 66% ofroTaper) failed because of fatigue fracture, whereas1% of NiTi hand instruments failed as a result of shearp � 0.01). The fracture mode of shaping files in rotaryroTaper was different between two different clinicsp � 0.05). All surfaces with fatigue fracture (n � 47)evealed the presence of either one or two crack ori-ins. The vast majority (86%) of K3 fatigue failure hadwo crack origins that could be found not only at theutting edge but also at various places along the fluteompared with only 28% of ProTaper showing multiplerack origins (p � 0.01). The latter showed one crackrigin in 81% of the fatigued shaping files but only 37%or finishing files (p � 0.01). The results of this studyndicated that the failure mode of NiTi instruments iselated to preparation technique. (J Endod 2009;35:33–136)
ey Wordslinical, failure, fatigue, nickel-titanium, rotary instru-ent, shear
From the *Division of Endodontics, Department of Oraliological & Medical Sciences, Faculty of Dentistry, Universityf British Columbia, Vancouver, Canada; †Area of Endodontics,aculty of Dentistry, The University of Hong Kong, Hong KongAR, China; and ‡Key Laboratory of Oral Biomedical Engineer-ng of Ministry of Education, School and Hospital of Stoma-ology, Wuhan University, Wuhan, China.
Supported in part by Post-Doctoral Fellowship Awards,aculty of Dentistry, University of British Columbia, Canada.
Address requests to reprints to Dr Markus Haapasalo,ivision of Endodontics, Oral Biological and Medical Sciences,BC Faculty of Dentistry, 2199 Wesbrook Mall, Vancouver,C, Canada V6T 1Z3. E-mail address: [email protected]/$0 - see front matter
Copyright © 2008 American Association of Endodontists.
foi:10.1016/j.joen.2008.10.013
OE — Volume 35, Number 1, January 2009
onsurgical root canal treatment has benefited from the introduction of nickel-titanium (NiTi) rotary instruments (1). However, there is an increasing concern
bout instrument fracture, as evidenced by the amount of reports on this problem2–9). A recent survey of endodontic specialists and general dental practitioners in thenited Kingdom has indicated that the great majority (92.6%) of endodontists used NiTiotary systems. The majority of users (93.6% of endodontists and 79.5% of generalractitioners) had experienced instrument fracture (10). Increasing numbers of NiTiotary instruments of various designs are now marketed; new instruments and materialseem to appear faster than clinicians could learn about the preceding versions. This hasreated an educational challenge for practitioners, universities, and manufacturers,equiring a greater degree of cooperation among these groups than ever before. Clini-ians should use only those instruments and materials shown to be safe and effective inndependent studies.
Although a number of studies have attempted to examine the reasons for fracturef NiTi rotary instruments after clinical or simulated use (2, 6, 11, 12), very few haveerformed a systematic examination of the fracture surface to identify the mode orechanism of fracture. A large-scale clinical study can provide detailed and reliable
nformation about the mechanism of fracture on different NiTi instruments and con-ribute to better understanding of how and why the fracture occurs. Such knowledge ismportant for the prevention of instrument fracture. Therefore, the aim of this study waso investigate the mode of fracture in NiTi instruments discarded from different clinicso identify the fracture mechanism.
Materials and MethodsThree NiTi rotary systems: ProTaper rotary (PT) (Dentsply Maillefer, Ballaigues,
witzerland), ProTaper for Hand Use (PHU) (Dentsply Maillefer), and K3SybronEndo, Orange, CA) have been adopted at three endodontic clinics, each in atomatologic school in China (Beijing, Guangdong and Wuhan). Two clinics (A and B,dentity not revealed) used only the PT instruments, and the other (clinic C) used bothHU and K3 instruments (by different endodontists who consistently used only one of
he three brands). There was a guiding principle in each clinic for their use. Eachnstrument was a limited to maximum number of uses according to the tooth beingreated: 30 root canals in clinic A (PT); 16 canals (for molars) to 30 canals (othereeth) in clinic B (PT), 16 canals (for molars) to 25 canals (other teeth) in clinic Cither by PTU or K3. Instruments would also be discarded after a single use in veryomplex, severely curved, or calcified canals. The collection of clinically used NiTinstruments has been described earlier (13). In short, a total of 79 fractured instru-
ents were collected from these three clinics over a 16-month period from January006 to April 2007. The fractured instruments were ultrasonically cleaned and auto-laved. The length of the fractured segment was examined under a stereomicroscopeMicrodissection; Zeiss, Bernried, Germany) at 30� magnification with a precision of.1 mm. The separated fragment was then mounted so that its long axis was normal to
he microscope stage for fractographic examination under scanning electron micro-cope (SEM) (Stereoscan 260, Cambridge Instruments, Cambridge, UK). The mode of
racture was classified as “fatigue” or “shear” according to Cheung et al. (14).Defects in N.T. Instruments after Clinical Use. Part 2 133

imwmsccu(
eoicso0
7Pwr(da(o(ff
abcccas
Fomoa
Basic Research—Technology
1
As for fatigue failure specimens, the crack initiation site(s) wasdentified by noting the chevron pattern, also called “herringbone
arks,” on the fracture surface and by referring to the high-power viewshen necessary. The fractographic appearance of a fatigued metallicaterial always progresses from the crack origin to a zone of fatigue
triations (ie, microscopic, incremental marks left by a growing fatiguerack) and, finally, a region of dimple rupture (15). The number ofrack origin(s) for each specimen was recorded. Data were analyzed bysing a Fisher exact or Student t test, where appropriate, in softwareSPSS for Windows 11.0; SPSS, Chicago, IL).
ResultsOf the 1,682 NiTi instruments collected, 79 (5%) were fractured,
ither because of fatigue (n � 47; 59%) or shear failure (n � 28; 35%)f the material. Fractographically, almost all of the fractured PHU
nstruments (10/11; 91%) had concentric abrasion marks encir-ling a central region with microscopical dimples, indicative ofhear fracture of the material (Fig. 1A); a less amount (31%, n � 18 outf 59) of the PT engine files showed these marks (Fisher exact test, p �.01) (Table 1). Microscopic fatigue striations were found in some
igure 1. (A) Fracture surface of a separated PHU finishing F1 file showing shearf fatigue striations. (B) Fracture surface of a separated PT F1 file showingagnification view of B showing clusters of fatigue striations (arrows). (D) Frac
rigins (arrows): (E) one at the cutting edge and (F) the other at the flute. A hig
rrow) and at the flute (F, arrow), respectively.34 Shen et al.
8% (7 out of 9) of K3 instrument, whereas only 9% of hand-operatedHU instruments showed such sign of material fatigue; the differenceas statistically significant (Fisher exact test, p � 0.01). Most of the
otary instruments (PT and K3) failed because of fatigue fractureFisher exact test, p � 0.05). For PT instruments, there was significantifference in fracture mode on shaping files between two clinics, And B; there were more fatigue failure for clinic B than for clinic AFisher exact test, p � 0.05); however, no significant difference wasbserved in the fracture mode of finishing files between clinic A and BFisher exact test, p � 0.05). The broken fragment caused by shearailure (3.0 � 1.1 mm) was significantly shorter than that for fatigueailure (3.6 � 1.2 mm) collectively (t test, p � 0.05).
For every instrument with fatigue failure, the crack origins andreas showing microscopic fatigue striations and dimple rupture coulde identified on all fracture surfaces. Almost all PT instruments showedrack initiation at the cutting edge (Fig. 1B). For the K3 instruments,rack initiation appeared somewhat erratic; origins of fatigue crackingould be found not only at the cutting edge but also at various placeslong the flute (Fig. 1D–F). The number of crack initiation sites wasignificantly different between PT and K3 (Fisher exact test, p � 0.01);
e of the material; note the presence of circular abrasion marks and the absencee failure with two crack origins at the cutting edge (arrows). (C) A higherrface of a separated K3 size 30 .06 taper showing fatigue failure with two crackagnification view of D showing the crack origin situated at the cutting edge (E,
failurfatiguture suher m
JOE — Volume 35, Number 1, January 2009
8(i(
toubpvmibw(rtpaaiiefro
ccictimebmsfPmdg
w3(gm(hb
mfioTctisbsKmacaNioc(b
s
T
S
*
†
‡
§
�¶
# .05).
TB
*
f
†
Basic Research—Technology
J
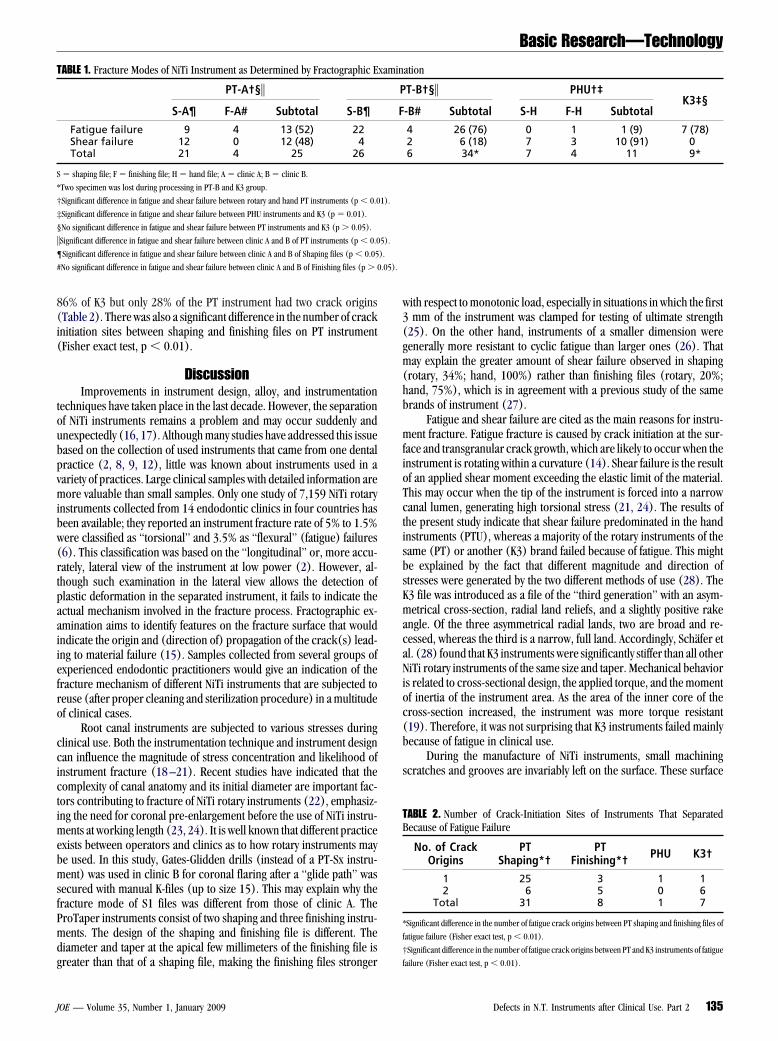
6% of K3 but only 28% of the PT instrument had two crack originsTable 2). There was also a significant difference in the number of cracknitiation sites between shaping and finishing files on PT instrumentFisher exact test, p � 0.01).
DiscussionImprovements in instrument design, alloy, and instrumentation
echniques have taken place in the last decade. However, the separationf NiTi instruments remains a problem and may occur suddenly andnexpectedly (16, 17). Although many studies have addressed this issueased on the collection of used instruments that came from one dentalractice (2, 8, 9, 12), little was known about instruments used in aariety of practices. Large clinical samples with detailed information areore valuable than small samples. Only one study of 7,159 NiTi rotary
nstruments collected from 14 endodontic clinics in four countries haseen available; they reported an instrument fracture rate of 5% to 1.5%ere classified as “torsional” and 3.5% as “flexural” (fatigue) failures6). This classification was based on the “longitudinal” or, more accu-ately, lateral view of the instrument at low power (2). However, al-hough such examination in the lateral view allows the detection oflastic deformation in the separated instrument, it fails to indicate thectual mechanism involved in the fracture process. Fractographic ex-mination aims to identify features on the fracture surface that wouldndicate the origin and (direction of) propagation of the crack(s) lead-ng to material failure (15). Samples collected from several groups ofxperienced endodontic practitioners would give an indication of theracture mechanism of different NiTi instruments that are subjected toeuse (after proper cleaning and sterilization procedure) in a multitudef clinical cases.
Root canal instruments are subjected to various stresses duringlinical use. Both the instrumentation technique and instrument designan influence the magnitude of stress concentration and likelihood ofnstrument fracture (18 –21). Recent studies have indicated that theomplexity of canal anatomy and its initial diameter are important fac-ors contributing to fracture of NiTi rotary instruments (22), emphasiz-ng the need for coronal pre-enlargement before the use of NiTi instru-
ents at working length (23, 24). It is well known that different practicexists between operators and clinics as to how rotary instruments maye used. In this study, Gates-Glidden drills (instead of a PT-Sx instru-ent) was used in clinic B for coronal flaring after a “glide path” was
ecured with manual K-files (up to size 15). This may explain why theracture mode of S1 files was different from those of clinic A. TheroTaper instruments consist of two shaping and three finishing instru-ents. The design of the shaping and finishing file is different. The
iameter and taper at the apical few millimeters of the finishing file is
ABLE 1. Fracture Modes of NiTi Instrument as Determined by Fractographic E
PT-A†§�
S-A¶ F-A# Subtotal S-B¶
Fatigue failure 9 4 13 (52) 22Shear failure 12 0 12 (48) 4Total 21 4 25 26
� shaping file; F � finishing file; H � hand file; A � clinic A; B � clinic B.
Two specimen was lost during processing in PT-B and K3 group.
Significant difference in fatigue and shear failure between rotary and hand PT instruments (p � 0.0
Significant difference in fatigue and shear failure between PHU instruments and K3 (p � 0.01).
No significant difference in fatigue and shear failure between PT instruments and K3 (p � 0.05).
Significant difference in fatigue and shear failure between clinic A and B of PT instruments (p � 0.0
Significant difference in fatigue and shear failure between clinic A and B of Shaping files (p � 0.05
No significant difference in fatigue and shear failure between clinic A and B of Finishing files (p � 0
reater than that of a shaping file, making the finishing files stronger f
OE — Volume 35, Number 1, January 2009
ith respect to monotonic load, especially in situations in which the firstmm of the instrument was clamped for testing of ultimate strength
25). On the other hand, instruments of a smaller dimension wereenerally more resistant to cyclic fatigue than larger ones (26). Thatay explain the greater amount of shear failure observed in shaping
rotary, 34%; hand, 100%) rather than finishing files (rotary, 20%;and, 75%), which is in agreement with a previous study of the samerands of instrument (27).
Fatigue and shear failure are cited as the main reasons for instru-ent fracture. Fatigue fracture is caused by crack initiation at the sur-
ace and transgranular crack growth, which are likely to occur when thenstrument is rotating within a curvature (14). Shear failure is the resultf an applied shear moment exceeding the elastic limit of the material.his may occur when the tip of the instrument is forced into a narrowanal lumen, generating high torsional stress (21, 24). The results ofhe present study indicate that shear failure predominated in the handnstruments (PTU), whereas a majority of the rotary instruments of theame (PT) or another (K3) brand failed because of fatigue. This mighte explained by the fact that different magnitude and direction oftresses were generated by the two different methods of use (28). The3 file was introduced as a file of the “third generation” with an asym-etrical cross-section, radial land reliefs, and a slightly positive rake
ngle. Of the three asymmetrical radial lands, two are broad and re-essed, whereas the third is a narrow, full land. Accordingly, Schäfer etl. (28) found that K3 instruments were significantly stiffer than all otheriTi rotary instruments of the same size and taper. Mechanical behavior
s related to cross-sectional design, the applied torque, and the momentf inertia of the instrument area. As the area of the inner core of theross-section increased, the instrument was more torque resistant19). Therefore, it was not surprising that K3 instruments failed mainlyecause of fatigue in clinical use.
During the manufacture of NiTi instruments, small machiningcratches and grooves are invariably left on the surface. These surface
ation
T-B†§� PHU†‡K3‡§
-B# Subtotal S-H F-H Subtotal
4 26 (76) 0 1 1 (9) 7 (78)2 6 (18) 7 3 10 (91) 06 34* 7 4 11 9*
ABLE 2. Number of Crack-Initiation Sites of Instruments That Separatedecause of Fatigue Failure
No. of CrackOrigins
PTShaping*†
PTFinishing*† PHU K3†
1 25 3 1 12 6 5 0 6
Total 31 8 1 7
Significant difference in the number of fatigue crack origins between PT shaping and finishing files of
atigue failure (Fisher exact test, p � 0.01).
Significant difference in the number of fatigue crack origins between PT and K3 instruments of fatigue
xamin
P
F
1).
5).
).
ailure (Fisher exact test, p � 0.01).
Defects in N.T. Instruments after Clinical Use. Part 2 135

s1ubacfbdbi1a
qoohm(imTciweats
hfmon
w
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
Basic Research—Technology
1
cratches can serve as notches that would concentrate the stress (4, 9,7, 27, 29), limiting the instrument’s fatigue life. The crack origins weresually found at the cutting edge region in most instruments. This is toe expected because when a circular beam is bent, its outermost fibersre subjected to the greatest stress and strain. Indeed, the first fatiguerack often is initiated at the surface (when there is no major internallaw or stress-concentration feature elsewhere) (15). There seemed toe some effect of the cross-sectional shape on crack initiation with someifference between brands in the number of crack origins. For the onerand of instrument (K3) with an irregular cross-sectional shape, cracknitiation occurred at a corner along the flute in some specimens (Fig.D). Similar patterns of cracking have also been reported by Cheungnd Darvell in a laboratory fatigue study (30).
The number of crack origin has never previously been examineduantitatively on discarded NiTi instruments after clinical use. A singlerigin usually indicates a failure with low stress, whereas the presencef multiple origins may be the result of high stress concentrations. Theighly concentrated stresses at the cutting edge of ProTaper instrumentight cause the machining defects to “open” and become microcracks
31), especially more two crack origins instruments occurred on fin-shing files. The potential shortcomings of the original ProTaper instru-
ent in the “Finisher” series were high bending moment and stiffness.he ProTaper Universal file with a reduced bending moment and in-reased flexibility was launched recently as an improvement to the orig-nal design. A mathematical simulation found that stress concentrationas situated at the trailing edge adjacent to rather than at the cuttingdge on the ProTaper Universal file (20). In theory, this could help tolleviate the combined effect of having both the greatest stress concen-ration and the site of rubbing contact with the root canal wall at theame location.
Under the conditions of this study, the fracture mode of rotary andand-operated NiTi instruments appeared to be different, with shearailure being more prevalent in the latter. The K3 instruments failed
ainly because of fatigue fracture, most of which showed the presencef more than one crack origin. The preparation technique has a sig-ificant influence on the fracture behavior of ProTaper instruments.
AcknowledgmentsThe authors thank Mr Andre Wong for the technical assistance
ith the SEM.
References1. Peters OA, Barbakow F, Peters CI. An analysis of endodontic treatment with three
nickel-titanium rotary root canal preparation techniques. Int Endod J2004;37:849 –59.
2. Sattapan B, Nervo GJ, Palamara JE, Messer HH. Defects in rotary nickel-titanium filesafter clinical use. J Endod 2000;26:161–5.
3. Yared GM, Bou Dagher FE, Machtou P. Influence of rotational speed, torque andoperator’s proficiency on ProFile failures. Int Endod J 2001;34:47–53.
4. Alapati SB, Brantley WA, Svec TA, Powers JM, Mitchell JC. Scanning electron micro-scope observations of new and used nickel-titanium rotary files. J Endod2003;29:667–9.
5. Martín B, Zelada G, Varela P, et al. Factors influencing the fracture of nickel-titaniumrotary instruments. Int Endod J 2003;36:262– 6.
6. Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-
titanium endodontic instruments after clinical use. J Endod 2004;30:722–5.36 Shen et al.
7. Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome ofendodontic treatment. J Endod 2005;31:845–50.
8. Shen Y, Cheung GS, Bian Z, Peng B. Comparison of defects in ProFile and ProTapersystems after clinical use. J Endod 2006;32:61–5.
9. Shen Y, Bian Z, Cheung GS, Peng B. Analysis of defects in ProTaper hand-operatedinstruments after clinical use. J Endod 2007;33:287–90.
0. Madarati AA, Watts DC, Qualtrough AJ. Opinions and attitudes of endodontists andgeneral dental practitioners in the UK towards the intracanal fracture of endodonticinstruments: part 1. Int Endod J 2008;41:693–701.
1. Spanaki-Voreadi AP, Kerezoudis NP, Zinelis S. Failure mechanism of ProTaper nick-el–titanium rotary instruments during clinical use: fractographic analysis. Int EndodJ 2006; 39:171– 8.
2. Wei X, Ling J, Jiang J, Huang X, Liu L. Modes of failure of ProTaper nickel-titaniumrotary instruments after clinical use. J Endod 2007;33:276 –9.
3. Shen Y, Haapasalo M, Cheung GS, Peng B. Defects in NiTi instruments after clinicaluse. Part 1: Relationship between defects and factors in a cohort study. J Endod (inpress).
4. Cheung GS, Peng B, Bian Z, Shen Y, Darvell BW. Defects in ProTaper S1 instrumentsafter clinical use: fractographic examination. Int Endod J 2005;38:802–9.
5. Hull D. Fractography: observing, measuring and interpreting fracture surface topog-raphy. Cambridge, UK: Cambridge University Press; 1999.
6. Hülsmann M, Schinkel I. Influence of several factors on the success or failure ofremoval of fractured instruments from the root canal. Endod Dental Traumatol1999;15:252– 8.
7. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. JEndod 2006;32:1031– 43.
8. Berutti E, Chiandussi G, Gaviglio I, Ibba A. Comparative analysis of torsional andbending stresses in two mathematical models of nickel-titanium rotary instruments:ProTaper versus ProFile. J Endod 2003;29:15–9.
9. Xu X, Zheng Y. Comparative study of torsional and bending properties for six modelsof nickel-titanium root canal instruments with different cross-sections. J Endod2006;32:372–5.
0. Kim HC, Cheung GS, Lee CJ, Kim BM, Park JK, Kang SI. Comparison of forces gener-ated during root canal shaping and residual stresses of three nickel–titanium rotaryfiles by using a three-dimensional finite-element analysis. J Endod 2008;34:743–7.
1. Blum JY, Cohen A, Machtou P, Micallef JP. Analysis of forces developed duringmechanical preparation of extracted teeth using ProFile NiTi rotary instruments. IntEndod J 1999;32:24 –31.
2. Peters OA, Peters CI, Schon̈enberger K, Barbakow F. ProTaper rotary root canalpreparation: assessment of torque and force in relation to canal anatomy. Int EndodJ 2003;36:93–9.
3. Roland DD, Andelin WE, Browning DF, Hsu GH, Torabinejad M. The effect of pre-flaring on the rates of separation for 0.04 taper nickel titanium rotary instruments. JEndod 2002;28:543–5.
4. Peters OA, Peters CI, Schönenberger K, Barbakow F. ProTaper rotary root canalpreparation: effects of canal anatomy on final shape analysed by micro CT. Int EndodJ 2003;36:86 –92.
5. Ullmann CJ, Peters OA. Effect of cyclic fatigue on static fracture loads in ProTapernickel-titanium rotary instruments. J Endod 2005;31:183– 6.
6. Fife D, Gambarini G, Britto LL. Cyclic fatigue testing of ProTaper NiTi rotary instru-ments after clinical use. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:251– 6.
7. Cheung GS, Bian Z, Shen Y, Peng B, Darvell BW. Comparison of defects in ProTaperhand-operated and engine-driven instruments after clinical use. Int Endod J2007;40:169 –78.
8. Schäfer E, Dzepina A, Danesh G. Bending properties of rotary nickel-titanium instru-ments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003:96,757– 63.
9. Cheung GS, Shen Y, Darvell BW. Does electropolishing improve the low-cycle fatiguebehavior of a nickel-titanium rotary instrument in hypochlorite? J Endod2007;33:1217–21.
0. Cheung GS, Darvell BW. Low-cycle fatigue of NiTi rotary instruments of variouscross-sectional shapes. Int Endod J 2007;40:626 –32.
1. Peng B, Shen Y, Cheung GS, Xia TJ. Defects in ProTaper S1 instruments after clinical
use: longitudinal examination. Int Endod J 2005;38:550 –7.JOE — Volume 35, Number 1, January 2009


















