
SPINAL CORD ANATOMY & PHYSIOLOGY HONORS ANATOMY & PHYSIOLOGY.

1. Review unique anatomy and physiology of obese pediatric patients that are important in the acute care setting
2. Describe risks associated with pediatric obesity in the acute care setting
3. Describe nursing interventions that increase the safety of obese pediatric patients in the acute care setting
Seventeen percent of children in the US are considered obese.
*Obesity is defined as a BMI of greater than 95th percentile


• WA State 12% according to WA Dept of Health

• Hypercholesterolemia/dyslipidemia • Hypertension • Obstructive Sleep Apnea • Mental health issues • Orthopedic issues • Skin breakdown/infection • Gallbladder disease • Type 2 diabetes • Pancreatitis • Venous thrombosis


• Bones are more prone to fractures
• Skin is at risk for breakdown
• High risk for poor skin healing
• Circulating blood volume and increased cardiac workload = intolerant of fluid boluses

• Fat deposits around neck narrow airway and increase the collapsibility
• Fat deposits around the trunk decrease lung compliance and increase oxygen demand
• Changes can cause obstructive sleep apnea


Sleep Apnea Hypoxemia Hypercapnia triggers the sympathetic nervous system to “startle” or take a deep breath.
Chronic hypoventilation decreased oxygen reserve

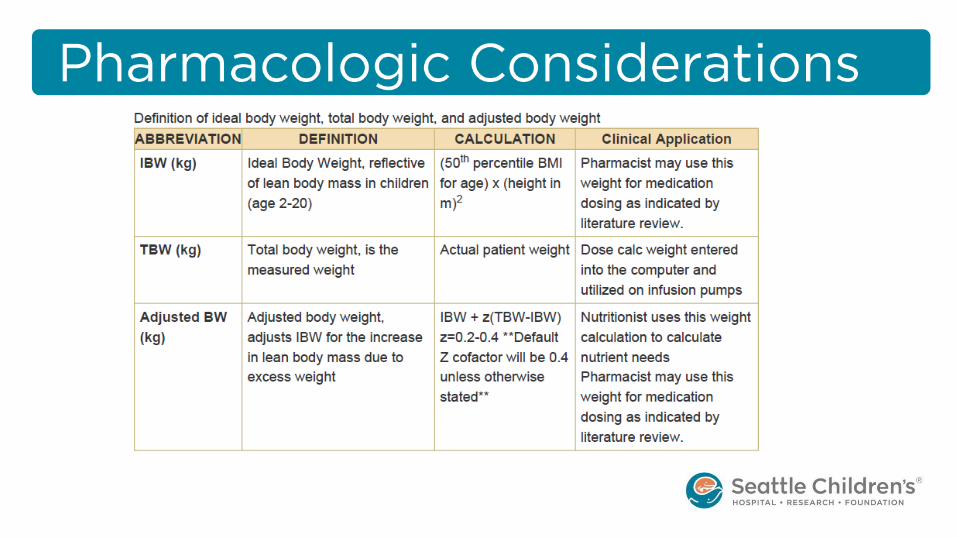
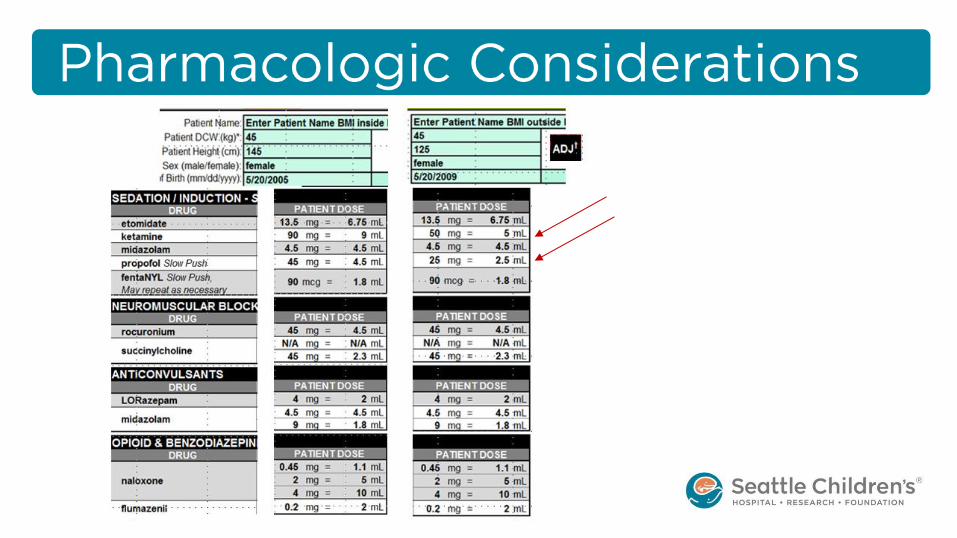
• Dosing by weight, except if it exceeds adult dosing
• Dosing by total body weight vs. ideal body weight
– Often depends if medication is lipophilic or hydrophilic
• Chronic hypoxemia and diminished response to CO2 + pain meds dosed by TBW =


• Equipment is ill-fitting
– Insufficient monitoring
– Falls risks
– Pressure sores
• Resuscitation can be more difficult

• Resuscitation Difficulties
– Difficult to seal
– Increased airway and chest wall resistance
– Reduced pulmonary compliance
– Difficult airway to intubate
– Increased force for chest compressions


• Identify obese patients and flag them as at risk
• Follow Guidelines of Care for Obese Patients

• System to calculate BMI and flag patients at risk.

• SCH Obese Care Clinical Standard Work Pathway6 – guidance for providers and nurses
– Recommends providers use Pediatric Obesity orderset
• Guideline of care for nurses


• ASA and sedation safety information
• Cues about resuscitation needs
• Comment on special equipment in bed request

The ASA score is a subjective assessment of a patient’s overall health that is based on five classes (I to V)4. I Patient is a completely healthy fit patient. II Patient has mild systemic disease. III Patient has severe systemic disease that is not incapacitating. IV Patient has incapacitating disease that is a constant threat to life. V A moribund patient who is not expected to live 24 hour with or without surgery.

Modified Mallampati Scoring:[3] •Class I: Soft palate, uvula, fauces, pillars visible. •Class II: Soft palate, uvula, fauces visible. •Class III: Soft palate, base of uvula visible. •Class IV: Only hard palate visible.


• Nursing Guideline of Care
– System review of risk factors
– Medication safety
– Equipment needs
– Mobility safety
• Admission checklist





Photo may be switched out for any in the from your own files, or it may be
deleted altogether. Written by Tessa Strickland and Kate DePalma Illustrated by David Dean

1. Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions Between Obesity and Obstructive Sleep Apnea: Implications for Treatment. Chest. 2010;137(3):711-719. doi:10.1378/chest.09-0360.
2. Institute of Medicine (US) Committee on Sleep Medicine and Research; Colten HR, Altevogt BM, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington (DC): National Academies Press (US); 2006. 3, Extent and Health Consequences of Chronic Sleep Loss and Sleep Disorders. Available from: https://www.ncbi.nlm.nih.gov/books/NBK19961/
3. Matson KL, Horton ER, Capino AC, on behalf of the Advocacy Committee for the Pediatric Pharmacy Advocacy Group. Medication Dosage in Overweight and Obese Children. The Journal of Pediatric Pharmacology and Therapeutics : JPPT. 2017;22(1):81-83. doi:10.5863/1551-6776-22.1.81.
4. Daabiss M. American Society of Anaesthesiologists physical status classification. Indian Journal of Anaesthesia. 2011;55(2):111-115. doi:10.4103/0019-5049.79879.
5. Porter RM, Thrasher J, Krebs NF. Implementing a pediatric obesity care guideline in a freestanding children's hospital to improve child safety and hospital preparedness. J Pediatr Nurs [CSWPO]. 2012;27(6):707-714. Accessed 20121029; 12/9/2016 1:09:43 PM. http://dx.doi.org/10.1016/j.pedn.2011.11.005.
6. Seattle Children’s Hospital, Kim, G; Johnson, J; Lorenzo, K; O’Hare, P; Popalisky, J; Reichert, E; Villavicencio, C; 2017 June. Obese Care Pathway. Available from: http:// www.seattlechildrens.org/pdf/Obese-Care-pathway.pdf


















