
1 Reducing Stigma toward the Mentally Ill: The Impact of Exposure versus Information Stephanie...
21
1 Reducing Stigma toward the Mentally Ill: The Impact of Exposure versus Information Stephanie Turner Hanover College
-
date post
21-Dec-2015 -
Category
Documents
-
view
215 -
download
0
Transcript of 1 Reducing Stigma toward the Mentally Ill: The Impact of Exposure versus Information Stephanie...

1
Reducing Stigma toward the Mentally Ill:
The Impact of Exposure versus Information
Stephanie Turner
Hanover College

2
Stigma
Goffman (1963) defines stigma as an attribute of an individual that “makes him different from others…and of a less desirable kind-in the extreme, a person who is quite thoroughly bad, or dangerous, or weak”.

3
Definitions
Stigma: more specific, negative form of attitudes; directed toward specific group
Exposure: any association or connection with mentally ill which involves seeing them as full human beings, capable of humor, warmth, intelligence, etc. and deserving of empathy
Empathy: “vicarious emotional experience of others” (Mehrabian, 1972)
4
Tested Interventions to Reduce Stigma
Angermeyer (1996) and Dietrich (2006) discuss how close contact with the mentally ill impacts and shapes attitudes
Addison and Thorpe (2004)
Found that factual knowledge alone did not positively alter attitudes
Used Community Attitudes Toward the Mentally Ill Scale (CAMI)

5
Pre- / Post-Intervention Design
Demographics 2 surveys pre-intervention
Empathy scale, CAMI
Participant sees one of two videos Information: “Professional Lecture” Exposure: “Robert Documentary”
Post-intervention surveys Empathy scale, CAMI

6
Hypotheses
Hypothesis 1: Participants in the Exposure Condition (“Robert Documentary”) will show a decrease in stigmatizing attitudes compared to participants in the Information Condition (“Professional Lecture”).
Hypothesis 2: Participants in the Exposure Condition will show an increase in empathy as compared to the participants in the Information Condition.

7
Participants
Students (N = 25)n = 22 female; n = 3 male
Wide range of previous experience with mental illness, including acquaintance, friend, family member, and self
Majority (76%) reported some previous experience or contact with mentally ill persons

8
Materials: CAMI
Community Attitudes Toward the Mentally Ill (CAMI) (Taylor & Dear, 1981)
Four dimensions of attitudes: 5 point Likert Scale Benevolence
“We need to adopt a far more tolerant attitude toward the mentally ill in our society”
Authoritarianism “The best way to handle the mentally ill is to keep them
behind locked doors” Social Restrictiveness
“The mentally ill should not be given any responsibility” Community Mental Health Ideology
“The best therapy for many mental patients is to be a part of a normal community”

9
Materials: Revised Empathy Scale
Based on the Emotional Empathetic Tendency Scale (EET) (Mehrabian, 1971)
Specified empathy toward mentally ill people
16 items total
5 point Likert Scale
8 concepts- 2 question each

10
Empathy Scale Sample Questions
Concept: Sympathy for the mentally ill
Negative: “People make too much of the feelings and sensitivity of the mentally ill.”
Positive: “The mentally ill deserve our sympathy.”

11
Materials: Professional Lecture
Video created for this study
Licensed Clinical Psychologist and director of a college counseling center
Discusses three mental disorders: Schizophrenia, Bipolar disorder, and Schizoaffective disorder
Formal lecture style, no empathic or humanizing information present

12
Materials: Robert Documentary
Imagining Robert: My Brother, Madness, and Survival (Hott, 2004)
Film by two brothers Robert, who has suffered with mental illness Jay, primary caretaker over the last 38 years Shows how family copes with mental illness
Realistic, humanizing portrayal of Robert

13
Results: CAMI
Mixed Model ANOVA CAMI- significant interaction (p = 0.005)
Follow up analysis for simple main effects of time also significant (p < 0.05)
Benevolence subscale- significant interaction (p < 0.05) Follow up analysis for simple main effects of
time also significant (p < 0.05)
Other subscales showed no significant differences

14
Pre-/Post- CAMI Changes
149.8155.3 146.8150.9
020406080
100120140160180200
Robert Lecture
Pre
Post
CAMI Score Significant
interaction(p = 0.005)

15
Pre-/Post- Benevolence Changes
38.8 39.440.3 38.9
0
5
10
15
20
25
30
35
40
45
50
Robert Lecture
Pre
Post
Benevolence Score
Significant interaction(p < 0.05)

16
Discussion of CAMI
Hypothesis 1 confirmed: Participants showed more benevolent, and thus less stigmatizing attitudes after Exposure intervention
CAMI and Benevolence differences might be even greater with a neutral or more stigmatizing sample.

17
Results: Empathy Scale
Reliability was achieved: Empathy Scale revised to specify the Mentally Ill was found to be reliable (α = 0.71)
Hypothesis 2 not supported: No significant main effects or interaction found
18
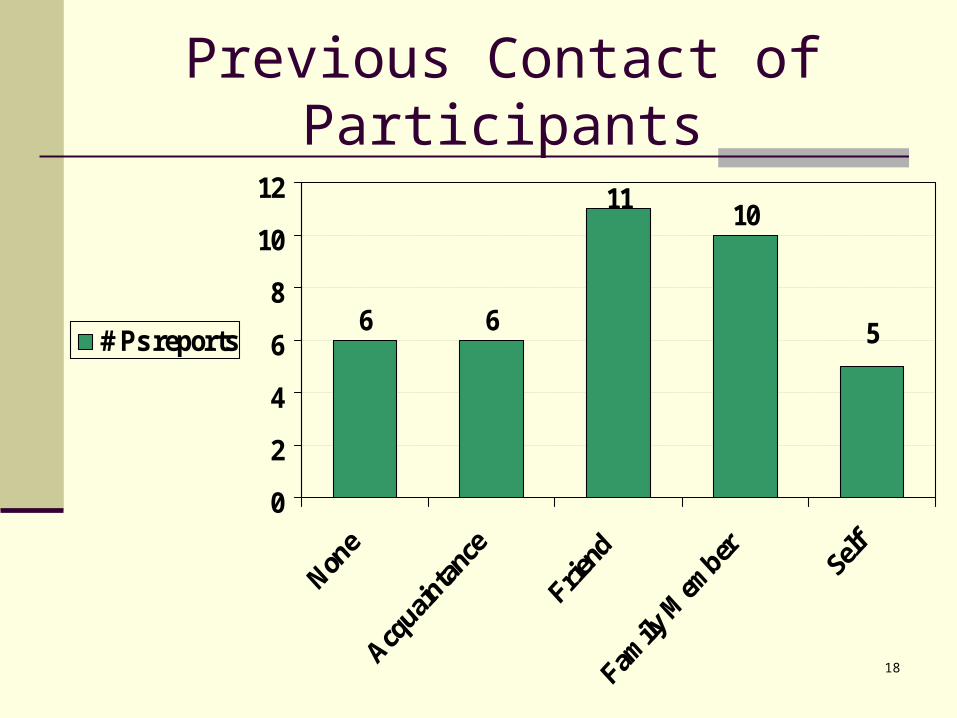
Previous Contact of Participants
6 6
1011
5
0
2
4
6
8
10
12
# Ps reports

19
Empathy Discussion
Participants displayed high levels of empathy pre-intervention. Mean: 61.4 Range: 49-70
High empathy levels may have restricted the amount of change that could be evoked by intervention.

20
Target sample low in empathy and high in stigmatizing attitudes toward mentally ill
Further research is needed to Test intervention with more participants Explore the role benevolence plays in
reducing stigmatizing attitudes and how it is related to empathy
Implications and Future Research

21
Pre-/Post- Empathy Changes
61.4 60.4
0
10
20
30
40
50
60
70
80
Empathy Scale
PrePost
No significant Interactionp = 0.737
Empathy Score
















![Theory of Planned Behavior, Self‑Stigma, and Perceived ...file.qums.ac.ir/repository/sdh/Theory of Planned...self-stigma (also known as internalized stigma).[5,6] Self-stigma was](https://static.fdocuments.in/doc/165x107/5f59324ffcada40fd01f4b2a/theory-of-planned-behavior-selfastigma-and-perceived-filequmsacirrepositorysdhtheory.jpg)
