1- Recent brain haemorrhage › sites › patomorfologia.wum.edu.… · (Haemorrhagia cerebri...
3
1 Hemodynamic disorders 1 - Recent brain haemorrhage 2 - Inveterated brain haemorrhage 3 - Chronic passive liver congestion 4 - Pulmonary brown induration 5 - Pulmonary oedema 1- Recent brain haemorrhage (Focus haemorrhagicus cerebri recens) Haemorrhage generally indicates extravasation of blood due to vessels rupture Cerebral haemorrhages range from small perivascular extravasations to massive haemorrhages causing stroke. The latter conditions most commonly result from arterial hypertension The vessels most commonly ruptured are arteriae lenticulostriatae – small branches of middle cerebral artery (therefore internal capsule and adjacent basal ganglia are most frequent site of cerebral haemorrhage. Clinical significance of cerebral haemorrhage depends upon its size and localization 1- Recent brain haemorrhage MACROSCOPICALLY cerebral hemisphere affected with massive haemorrhage is swollen, showing flattening of gyri. On cut surface one can see a blood clot lacerating brain substance, surrounded by compressed oedematous, soft white matter, often with multiple small extravasations Fig. Fatal intracerebral bleed. Fig. Massive hemorrhage rupturing into a lateral ventricle. 1 - Recent brain haemorrhage HISTOLOGICAL EXAMINATION reveals irregular mass of compactly arranged extravasated erythrocytes with trapped remnants of nervous cells. This mass has ill- definedborders and is surrounded by changed brain substance. The latter exhibits patchy necrosis with loss of numerous neurones and glial cells, as well as oedema and vacuolization. 2- Inveterated (old) brain haemorrhage (Haemorrhagia cerebri inveterata) In cases of the survival of patient the blood mixed with necrotic brain mass is removed by macrophages. These cells phagocytize: -The red cells; their heme is transformed into brown hemosiderin, and -Cerebral lipids; the macrophages accumulate them in the cytoplasm which becomes foamy. The removal of the destroyed masses results in formation of postapopletic cavern (lacuna postapopletica) – fluid-filled pseudocyst (pathologic cavity without epithelial lining) lined with astroglial cells with scattered haemosiderin-laden macrophages MI: the slide reveals the margin of haemorrhagic pseudocyst with haemosiderin-loaded macrophages and free haemosiderin granules derived from ingested erythrocytes 3- Chronic passive liver congestion („nutmeg liver”) The term „congestion” designates increase in blood volume in dilated vessels. Passive (venous) congestion results from the impairment of blood outflow from affected area. Passive congestion of the liver is most commonly subsequent to the right-sided heart failure, but in some cases to compression or obstruction of inferior vena cava as well as hepatic veins. As passive congestion prolongs, congested liver develops morphological changes. They mostly arise from hypoxia of hepatocytes which is caused by decreased oxygen content of blood and reduction of hepatic blood flow.
Transcript of 1- Recent brain haemorrhage › sites › patomorfologia.wum.edu.… · (Haemorrhagia cerebri...

1
Hemodynamic disorders
1 - Recent brain haemorrhage
2 - Inveterated brain haemorrhage
3 - Chronic passive liver congestion
4 - Pulmonary brown induration
5 - Pulmonary oedema
1 - Recent brain haemorrhage(Focus haemorrhagicus cerebri recens)
Haemorrhage generally indicates extravasation of blood due to vesselsrupture
Cerebral haemorrhages range from small perivascular extravasations to
massive haemorrhages causing stroke. The latter conditions most
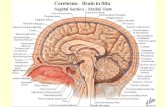
commonly result from arterial hypertensionThe vessels most commonly ruptured are arteriae lenticulostriatae – smallbranches of middle cerebral artery (therefore internal capsule and adjacentbasal ganglia are most frequent site of cerebral haemorrhage.
Clinical significance of cerebral haemorrhage depends upon its size andlocalization
1 - Recent brain haemorrhage
MACROSCOPICALLY cerebral hemisphere affected with massivehaemorrhage is swollen, showing flattening of gyri. On cut surface one can see a blood clot lacerating brain substance, surrounded by compressed oedematous, soft white matter, often withmultiple small extravasations
Fig. Fatal intracerebral bleed.
Fig. Massive hemorrhage rupturing into a lateral ventricle.
1 - Recent brain haemorrhage
HISTOLOGICAL EXAMINATION reveals irregularmass of compactly arranged extravasated erythrocyteswith trapped remnants of nervous cells. This mass hasill- defined borders and is surrounded by changed brainsubstance. The latter exhibits patchy necrosis with lossof numerous neurones and glial cells, as well as oedema and vacuolization.
2 - Inveterated (old) brain haemorrhage(Haemorrhagia cerebri inveterata)
In cases of the survival of patient the blood mixed with necrotic brainmass is removed by macrophages. These cells phagocytize:-The red cells; their heme is transformed into brown hemosiderin, and-Cerebral lipids; the macrophages accumulate them in the cytoplasmwhich becomes foamy.
The removal of the destroyed masses results in formation ofpostapopletic cavern (lacuna postapopletica) – fluid-filled pseudocyst(pathologic cavity without epithelial lining) lined with astroglial cells withscattered haemosiderin-laden macrophages
MI: the slide reveals the margin of haemorrhagic pseudocyst withhaemosiderin-loaded macrophages and free haemosiderin granulesderived from ingested erythrocytes
3 - Chronic passive liver congestion („nutmeg liver”)
The term „congestion” designates increase in blood volume in dilatedvessels. Passive (venous) congestion results from the impairment ofblood outflow from affected area.
Passive congestion of the liver is most commonly subsequent to theright-sided heart failure, but in some cases to compression orobstruction of inferior vena cava as well as hepatic veins.
As passive congestion prolongs, congested liver develops morphologicalchanges. They mostly arise from hypoxia of hepatocytes which is causedby decreased oxygen content of blood and reduction of hepatic bloodflow.

2
3 - Chronic passive liver congestion („nutmeg liver”)
MACROSCOPICALLY, liver is often diminished with characteristic two-colored, mottled cut surface resembling a cut nutmeg (nutmeg liver).Lobular pattern is accentuated: there are dark-red centrilobular areascontrasting with pale, yellowish peripheral zones of lobules
Central areas are red and slightly depressed compared with the surrounding tan viable parenchyma, forming the so-called "nutmeg liver" pattern.
3 - Chronic passive liver congestion („nutmeg liver”)
MI: centrilobular congestion- the center of all hepatic lobules is highlyengorged by blood; centrilobular hepatocytes may become atrophic oreven necrotic due to severe hypoxia of this region; lobular peripheryshows either normal parenchyma or its fatty degeneration- hepatocytesfilled with fat are round-shaped and appear empty, since lipids aredissolved during routine preparation of the specimen
4 - Pulmonary brown induration(Induratio fusca pulmonum)
Chronic passive congestion (ch.p.c) of lungs is most commonly seen in caseof long-standing, gradually developing left-sided heart failure or mitralstenosis. Of unclear reasons ch.p.c. leads to fibrosis which is due to thestimulated formation of collagen in the stoma of involved organs. The latterbecome firmer
MACROSCOPICALLY, lungs are brown and firm. This appearance explainsorigin of designation „brown induration”
4 - Pulmonary brown induration(Induratio fusca pulmonum)
MICROSCOPICALLY , there is considerable thickeningof interalveolar septa, resulting from: distension of capillaries, which arepacked with erythrocytes, from edema and fibrosis. Numerous erythrocytescan be seen in alveolar spaces because of extravasations from congestedcapillarie and venules. There are also intra-alveolar macrophagescontaining brown hemosiderin granules („ heart failure cells” ). Hemosiderin originates from breakdown of haemoglobin derived fromingested red blood cells. Deposition of hemosiderin appears also inintestitial pulmonary tissue.
5 - Pulmonary oedema (edema)Pulmonary oedema is a common clinical and morphological conditioncharacterized by excessive accumulation of fluid within lungs.The condition results from:- hemodynamic disturbances – hemodynamic edema
1. increased hydrostatic pressure (pulmonary venous pressure)- common▪ acute left ventricular failure (left-sided heart failure)▪ mitral stenosis, - pulmonary vein obstruction, - overhydration2. decreased oncotic pressure▪ hypoalbuminemia, - liver and renal disease,
- direct increases in capillary permeability - edema due to microvascular injury (alveolar injury)▪ infections: pneumonia▪ inhaled gases: oxygen, smoke▪ liquid aspiration: gastric contents▪ drugs and chemicals, e.g. bleomycin, heroin
- Edema of undetermined origine.g. neurogenic (central nervous system trauma)
5 - Pulmonary oedema
Macroscopically, lungs are enlarged, heavy and pit on pressure. Frothy, blood-tinged, watery fluid can be squeezed from the cutsurface

3
5 - Pulmonary oedema
Microscopically, alveolar septa show congested capillarie whereasalveolar spaces are filled with eosin staining material (transudatecontaining protein, precipituated during fixation). Some scattered red blood cells, hemosiderin- laden macrophages can be seen in alveolarlumina. Occasionaly, empty round spaces are present within intra-alveolar fluid. They represent air bubbles which reflect frothing of edemafluid which is evident grossly.