
1 MYELOPROLIFERATIVE SYNDROMES & LEUKEMIA Doç. Dr. Işın Doğan Ekici.
71
1 MYELOPROLIFERATIVE SYNDROMES & LEUKEMIA Doç. Dr. Işın Doğan Ekici
-
Upload
ginger-hardy -
Category
Documents
-
view
223 -
download
1
Transcript of 1 MYELOPROLIFERATIVE SYNDROMES & LEUKEMIA Doç. Dr. Işın Doğan Ekici.

1
MYELOPROLIFERATIVE SYNDROMES &LEUKEMIA
Doç. Dr. Işın Doğan Ekici

2
Myeloproliferative syndromesMyeloproliferative syndromes ( (MPSMPS; ; blast crisisblast crisis))
Excess proliferation of marrow cells (myelopoiesis) with dysplasia
Progress to Leukemia Ineffective Myelopoiesis
marrow hyperplasia with pancytopenia.
Primary or Secondary

3
Bone Marrow Cellularity
Normal Hypercellular Hypocellular

4
Primary MPS
Agnogenic myeloid metaplasia
Polycythemia rubra veraChronic myeloid leukemiaEssential hemorrhagic
thrombocythemia Myelofibrosis

5
The following "myeloproliferative diseases" are all "tumors of the multipotent myeloid stem cell", and can transform into one another (usually from a mild one to a bad one): polycythemia rubra vera (PV) essential (hemorrhagic) thrombocythemia
(ET) agnogenic myeloid metaplasia (AMM) idiopathic "aplastic anemia" (AA) chronic myeloid leukemia. (CML)

6
Myeloproliferative syndromesMyeloproliferative syndromes:: PathogenesisPathogenesis

7
AAgnogenicgnogenic (idiopathic) (idiopathic) myeloid myeloid metaplasiametaplasia
• Proliferation of neoplastic stem cells in the – bone marrow (becomes hypercellular) – red pulp of the spleen (enlarges greatly;
splenomegaly).
• the cells that enter the blood are fully functional
• neutrophilia/neutropenia/normal neutrophil counts
• no tendency to over-produce red cells.• Peripheral smear shows a
leukoerythroblastic pattern:– red cells made in the spleen tend to be
teardrop-shaped (poikilocyte), – nucleated red-cell precursors from the spleen.

8
• Bone marrow dense fibrosis (several years) Cytopenia or transformation to acute leukemia.
• Differential diagnosis (if there is an unexplained myelofibrosis without splenomegaly) : – Chronic myeloid leukemia, – Polycythemia vera, – Metastatic carcinoma.

9
Polycythemia rubra vera (PV)Polycythemia rubra vera (PV)
• Syn.:Osler's polycythemia; erythrocytosis.
• An abnormally high hemoglobin.
10
Classification• Relative
polycythemia – Dehydration
• Absolute polycythemia (increased circulating
red cell mass): – Primary
polycythemia• Polycythemia vera
rubra
– Secondary polycythemia• Effective renal arterial
hypoxia – Emphysema – Tetralogy of Fallot – Hemoglobins with too
much oxygen affinity
• Erythropoietin-producing tumors
– Renal cell carcinoma – Hepatocellular carcinoma – Cerebellar
hemangioblastoma (?!)
• Anabolic steroid users • Sleep apnea • After kidney transplant • Altitude

11
• Polycythemia vera is a proliferation of stem cells:– they are very
erythropoietin-sensitive – mostly mature into red
cells– in addition to a high red
cell count, white cells and platelets are likely to be high.
• Older middle-age. • Increased volume of
hyperviscous blood.
On biopsy:• a very hypercellular
marrow, • with all cell
lineages increased. • In the late stages:
– marrow fibrosis – replacement by
blasts– transformation to
acute myelogenous leukemia.

12
Complications:• Congestion (widespread; red
face)
• Venous stasis• Rupture of dilated veins
– hemorrhage
• GI bleedings• Hemorrhagic stroke.

13
MyelofibrosisMyelofibrosis The marrow is replaced by fibrous (scar) tissue. Causes blood formation to take place in sites
other than the bone marrow, such as the liver and spleen, causing enlargement of these organs. Primary
Idiopathic myeloid metaplasia Secondary
Autoimmune SLE Polycytemia vera Carcinoma infiltration Leukemias
Complications: Sever anemia with low platelet & splenomegaly Hepatomegaly & Liver failure Acute myelogenous leukemia.

14
Myelofibrosis
teardrop cells

15

16
(P(Preleukemias ; releukemias ; Carl Sagan's disease)Carl Sagan's disease) Ineffective Myelopoiesis
marrow hyperplasia with pancytopenia.
Excess proliferation with dysplasia. This is a family of disorders in which
there are problems in producing red cells, granulocytes, platelets.
MyeloMyelodysplasticdysplastic syndromes syndromes

17
FAB classificationFAB classification
• 1. Refractory anemia (poor hemoglobinization, too few red cells): (Blasts <1%)
• 2. Refractory anemia with ringed sideroblasts (>15% of nucleated red cells)
• 3. Refractory anemia with excess blasts (5-20% myeloblasts)
• 4. Refractory anemia with excess blasts in transformation (20-30% myeloblasts)
• 5. Chronic myelocytic leukemia.

18
WHO 2008 MDS CLASSIFICATION ● Refractory anemia (RA): <5% blasts, <15% ringed
sideroblasts; variable marrow cellularity, unicytopenia or bicytopenia, unilineage dysplasia >10% in one myeloid lineage● RA with Ringed Sideroblasts (RARS): 15% or more sideroblasts, less than 5% blasts, erythroid dysplasia only● Refractory cytopenia with multilineage dysplasia (RCMD): cytopenia, <5% blasts, dysplasia in >10% of cells in two or more lineages, no Auer rods● RA with Excess Blasts (RAEB): type 1 has 5-9% blasts in blood/marrow, peripheral cytopenia, unilineage or multilineage dysplasia, no Auer rods; type 2 has 10-19% blasts in blood/marrow, unilineage or multilineage dysplasia, Auer rods may be present, peripheral cytopenia ● MDS with isolated 5q- syndrome: anemia, <5% blasts, del(5q), no Auer rods, normal/increased hypolobated megakarycoytes ● MDS, unclassified: cytopenia(s), dysplasia in <10% of cells in one or more myeloid cell lines, accompanied by cytogenetic abnormalities with presumptive evidence of MDS, <5% blasts ● Therapy related MDS

19
20
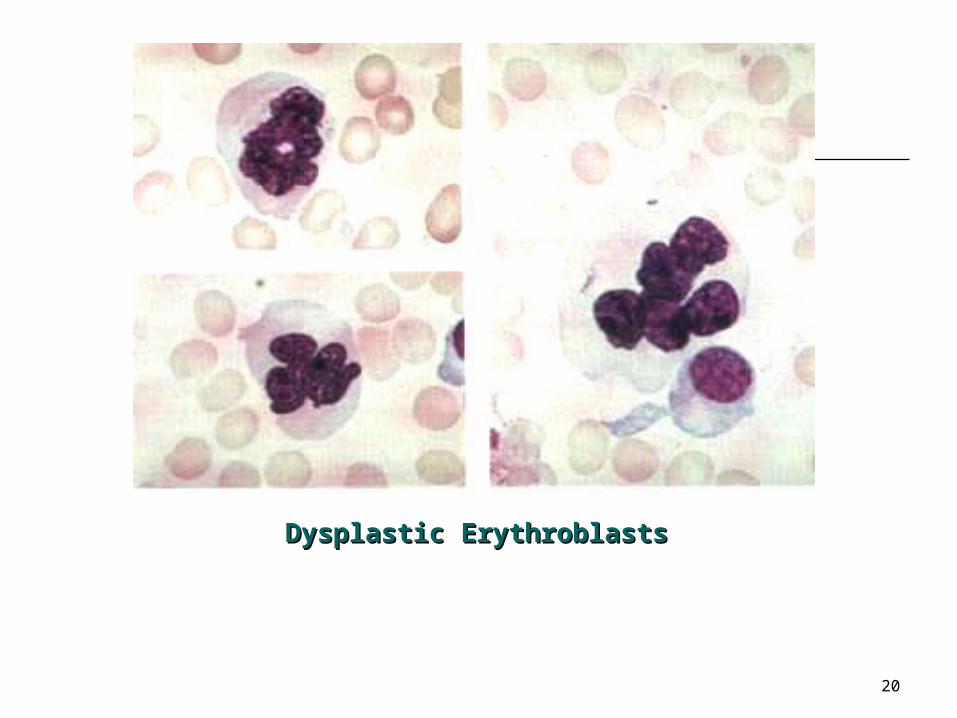
Dysplastic ErythroblastsDysplastic Erythroblasts

21
Clinical findings
• Most patients are older adults,• often asymptomatic (detected on
routine screening) • in the more aggressive forms,
death follows in a few years. • Propensity to transform into acute
myeloid leukemia.

22
LEUKEMIAS
ACUTE & CHRONIC
23
WBC Neoplastic disorders
Leukemias Bone marrow, blood, blast cells Acute/Chronic & Myeloid/Lymphoid AML / ALL & CML / CLL
Lymphomas – Lymph nodes, tumor Hodgkins - Non-Hodgkins. Myeloma
Premalignant conditions: Myeloproliferative syndromes (MPS) Myelodysplastic syndromes (MDS)

24
Introduction:
No Benign Neoplasms – All are considered malignant or premalignant.
Neoplastic Cells flood blood stream – Leukemia.
Commonly arise in marrow (myelo/ly) or Lymph node (lymphoid),
Spread to blood & other RES tissues rarely to other organs
Symptoms are due to deficient normal hemopoiesis. RBC, WBC & Plt.

25
Leukemia - Clinical Features
Anemia (low RBC) Fever - Infections (low WBC) Bleeding tendency (low PLT) Tender bones, lymphadenopathy,
spleenomegaly etc. (Leukemic infiltration)

26
Leukemia Classification
Acute Leukemias: Acute Myeloid Leukemia - AML
AML M0, M1, M2, M3, M4, M5, M6 & M7
Acute Lymphoid Leukemia - ALL ALL - L1, L2 & L3 - maturity
Chronic Leukemias: Chronic Myeloid Leukemia- CML Chronic Lymphoid Leukemia - CLL

27
ACUTE LEUKEMIA
Genetic disorder characterized by uncontrolled clonal proliferation of expansion of hematopoietic cells that do not retain the capacity to differentiate normally to mature cells

28
Triggers of Differentiation Mishap Not really known
Virus Clusters of leukemia
Ionizing radiation Survivors of Hiroshima and Nagasaki
Genetics Higher incidence in siblings and twins of affected
pt Higher incidence in children with fragile
chromosomes and impaired DNA repair mechanisms
Down syndrome, Fanconi syndrome, Bloom Syndrome Ataxia-telangiectasia, congenital
hypogammaglobulinemia
29
ACUTE LEUKEMIASystemic Findings Cytopenias
anemia, neutropenia, thrombocytopenia.
Bone pain expansion of the marrow infiltration of the periosteum.
Involvement of all other organs brain involvement is especially troublesome. T-cell leukemias often produce a mass in the anterior
mediastinum. Death
hemorrhage (cerebral, GI, other), infection (neutropenia, chemotherapy), complications of bone marrow transplantation.
30
ALL-Acute Lymphocytic Leukemia
Common in Children. FAB classification L1, L2 & L3 CD10 + and, Pre B cell type
common. Growth failure, Fever, Anemia
Lymphadenopathy, bleeding. Moderate Hepatosplenomegaly

31
The Cause
Clonal expansion of lymphoid progenitor cells is altered
Progenitor cells get stuck at a particular stage of differentiation and do not progress

32
Acute Lymphocytic Leukemia (ALL)
Acute lymphoid / lymphocytic leukemia “Childhood leukemia", with peak age in
four year old kids. Risk Factors:
Radiation exposure Down's syndrome kids are at 15x the
normal risk, Viruses (as-yet-unidentified) an unusual
response to.
33
Subclassification of Acute lymphoblastic leukemia by blast morphology “FAB classification”
L1 (85%): Cells <= 2x the diameter of a normal lymphocyte; smooth nuclei; common in kids.
L2 (14%): Bigger cells, lots of clefts, often nucleoli; more common in adults.
L3 (1%): Even bigger cells; leukemic form of Burkitt's lymphoma.

34
ALL-L1

35
ALL-L2

36
ALL-L3
37
The immunologic classification: B-cell (80%) leukemia “pre-B” cell leukemia (Burkitt's) T-cell (15%) leukemia

38

39
ALL:Cervical Lymphadenopathy
40
Mediastinal Lymphadenopathy - ALL

41
AML-Acute Myeloid Leukemia
Adults common FAB classification - M0 to M7. Anemia, Fever, Bleeding Hepatosplenomegaly moderate No significant lymphadenopathy
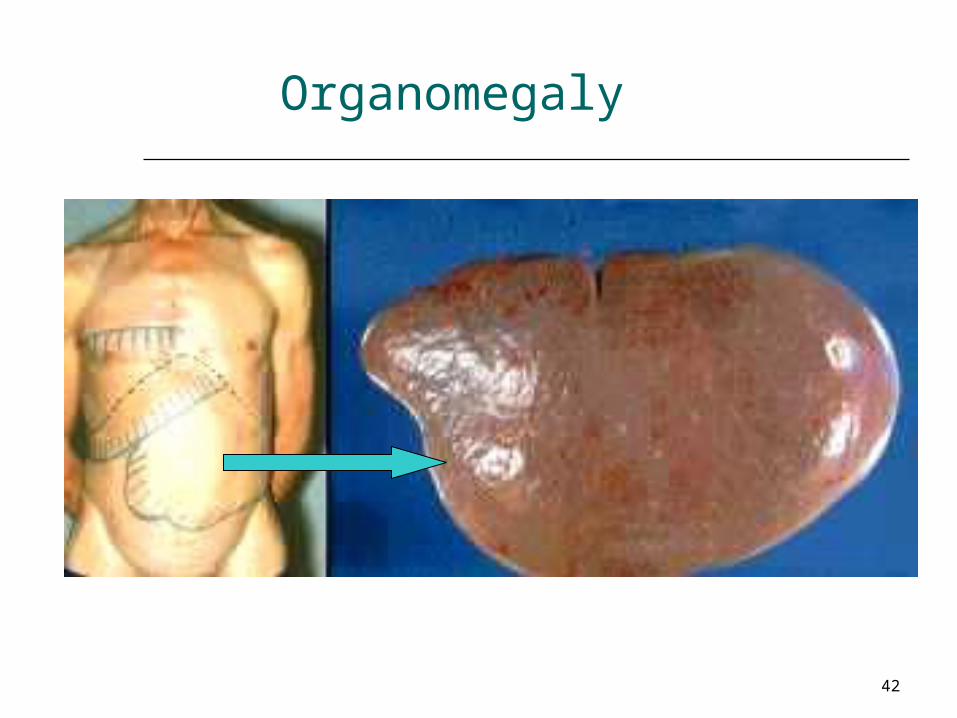
42
Organomegaly

43

44
Platelet Coagulation
Petechiae, Purpura Hematoma, Joint bl.

45
Acute Myeloblastic Leukemia (AML)
“Poorly differentiated granulocytic leukemia", “Acute non-lymphocytic leukemia",
This is the common acute leukemia of adults (seldom over age 40, occasionally children are affected)
Bleeding tendency: DIC Gum bleeding common

46
AML-M5 - Gum Hypertrophy:

47
Risk factors
Down's syndrome
Fragile chromosome syndromes Bloom's ataxia telangiectasia Fanconi's anemia
Benzene exposure Ethylene oxide exposure Radiation exposure
Previous cancer chemotherapy Myelodysplastic syndromes (preleukemia) Any "chronic myeloproliferative syndrome" ("blast crisis")
agnogenic myeloid metaplasia polycythemia vera rubra "essential" hemorrhagic thrombocythemia chronic myelogenous leukemia idiopathic aplastic anemia.

48
The FAB classification of AML
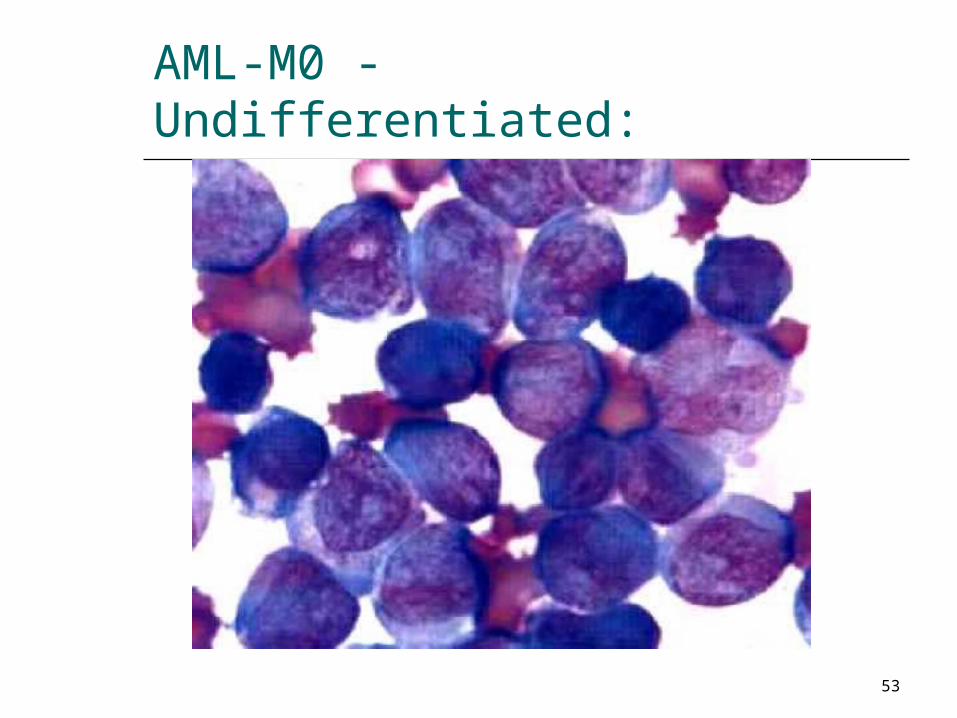
M0: undifferentiated myeloblasts without myeloperoxidase
M1: undifferentiated myeloblasts with myeloperoxidase
M2: some promyelocytic differentiation, maybe a few Auer rods;
M3: very granular promyelocytes, often many Auer rods, DIC (from annexin II on the surfaces which activates plasmin).
M4: myeloid and monocytic differentiation
M5: monocytic differentiation only M6: features of red cell precursors
predominate; "erythroleukemia" M7: platelet markers; acute
marrow fibrosis.

49

50
Promyelocytic M3
Monocytic leukemiaM5

51
M0 - AML No maturation (<3% Peroxidase +) M1 - AML Min.Maturation(>3% Peroxidase +) M2 - AML With full maturation M3 - Acute Promyelocytic leukemia M4 - Acute Myelomonocytic leukemia M5 - Acute Monocytic L (Monocytic, Monoblastic) M6 - Acute Erythroleukemia M7 - Acute Megakaryocytic leukemia.

52
53
AML-M0 - Undifferentiated:

54
AML-M2 - with maturation

55
AML-M3 - Auer Rods

56
AML-M4 - Myelomonocytic

57
AML-M6 : Erythroleukemia

58
AML-M7 : Megakaryocytic
59
Chronic Myeloid Leukemia
Middle age 40-60y Philadelphia chromosome, t(9:22) BCR-
ABL Anemia, Fever & Bleeding Marked leucocytosis – >50,000
(abnormal) Marked splenomegaly, Hepatomegaly
60
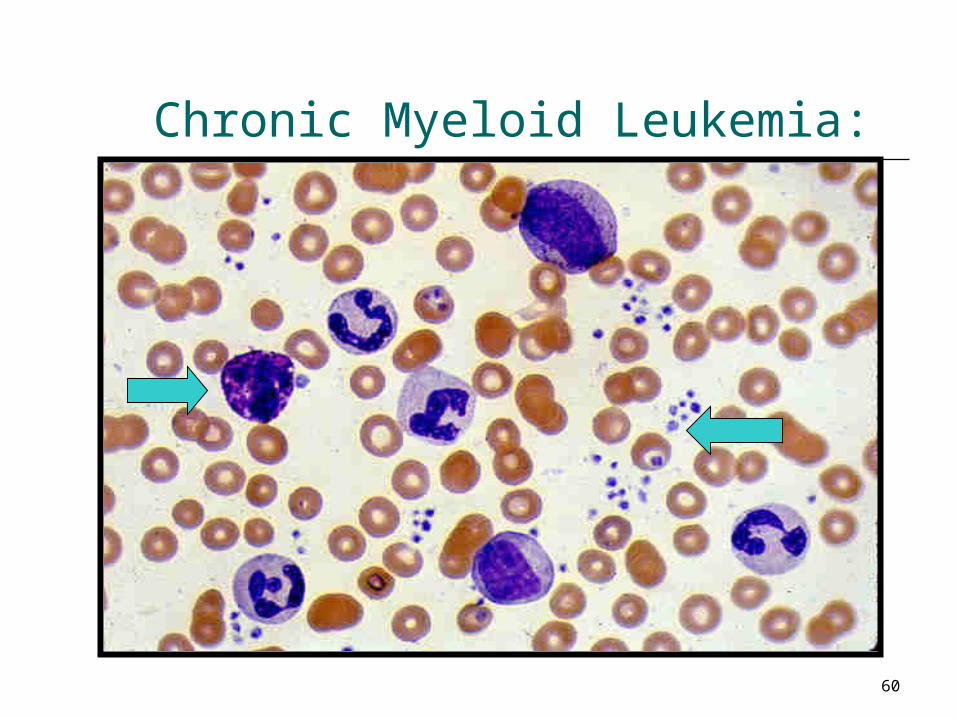
Chronic Myeloid Leukemia:
61
Chronic Myeloid Leukemia (CML)
Syn: Chronic myelogenous leukemia, Well-differentiated granulocytic leukemia
This is cancer of the myeloid stem cells in which there is overgrowth of normally-maturing myeloid cells
Middle age Risk Factors:
radiation exposure to chemicals (notably benzene)
Marked leukocytosis 50,000 (abnormal) high counts of neutrophils and their precursors (and
almost always basophils

62
Marked splenomegaly with little infarcts White cells plugging important small vessels
("leukostatic ischemia" of the brain, etc.) Hyperuricemia (gout, renal impairment) After a few years, in blast crisis, (50%/50%). The following "myeloproliferative diseases" are
all "tumors of the multipotent myeloid stem cell", and can transform into one another (usually from a mild one to a bad one): polycythemia vera rubra essential hemorrhagic thrombocythemia agnogenic myeloid metaplasia idiopathic "aplastic anemia" chronic myelogenous leukemia.

63
64
Chronic Lymphocytic LeukemiaCLL
Elderly age Anemia, fever & bleeding – slow over
years. Lymphocytosis & Lymphadenopathy Spleen, & liver enlargement Common B cell (CD5 +)
65
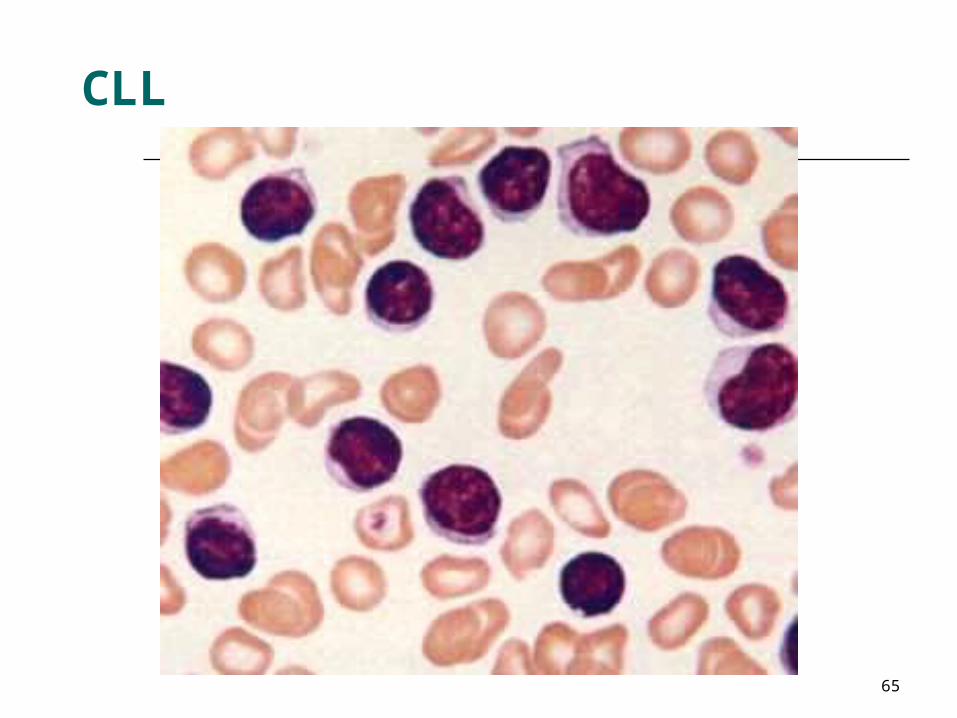
CLL
66
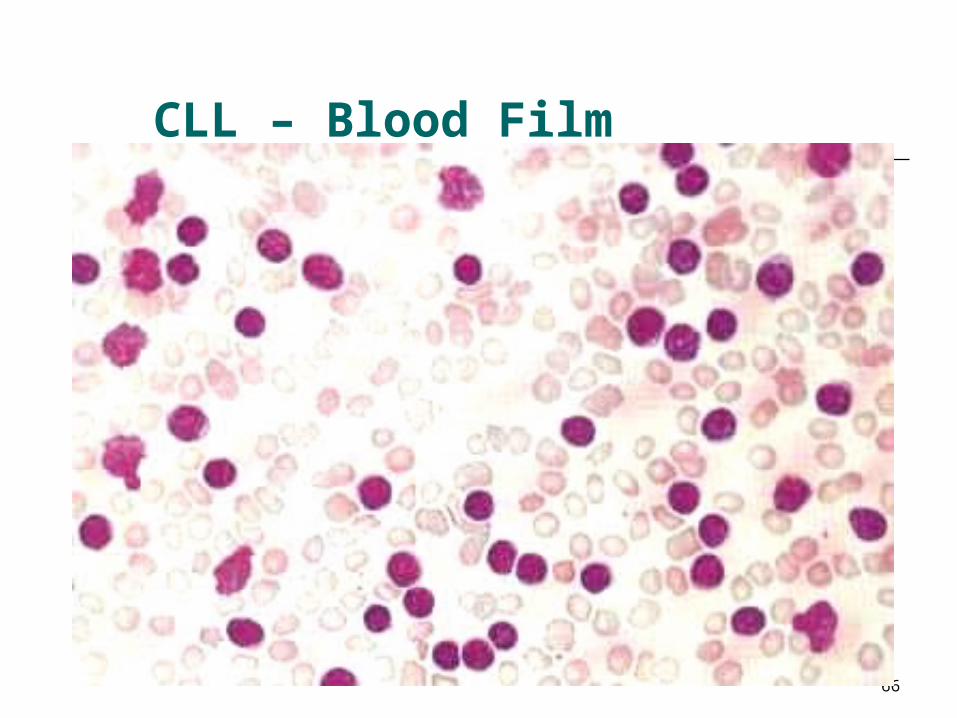
CLL – Blood Film

67
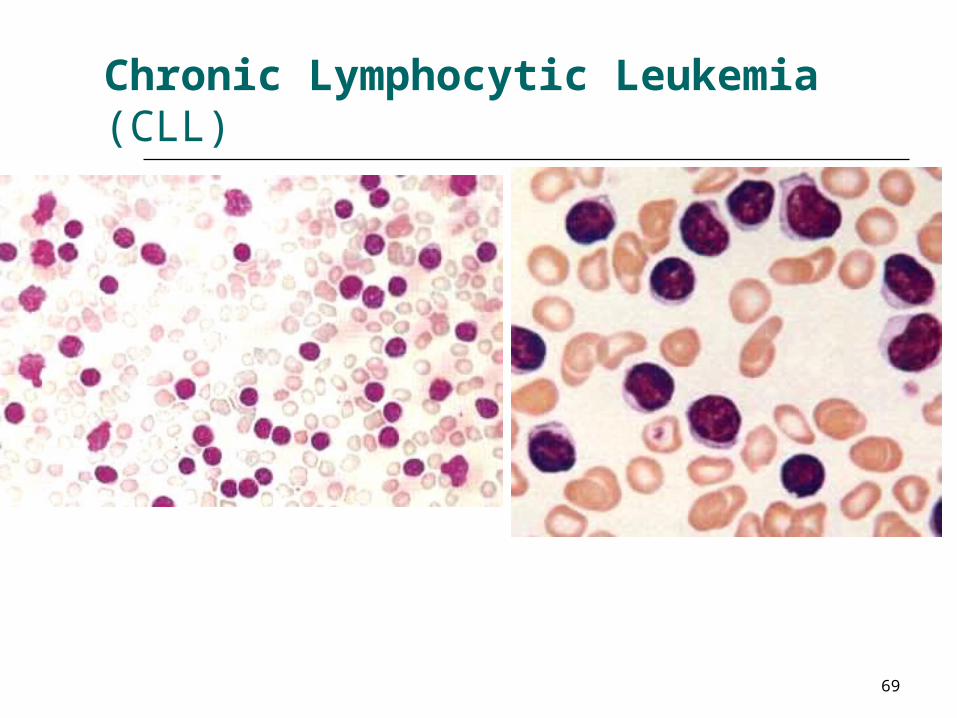
Chronic Lymphocytic Leukemia (CLL)
Well-differentiated lymphocytic leukemia The liquid phase of well-differentiated lymphocytic
lymphoma, A clone of B-cells which multiply slowly and do nothing
useful. The lymphocytes:
do somewhat suppress the heathy plasma cells, the patients have troubles with infections.
Risk factor: ataxia-telangiectasia. Elderly age Anemia, fever & bleeding (slow, over years). Lymphocytosis & Lymphadenopathy Hepatosplenomegaly

68
Paraneoplastic syndromes are more troublesome in this disease than in most other leukemias.
Autoimmune hemolytic anemia (15%) Richter's syndrome: a few percent of
patients develop a diffuse large-cell lymphoma (rapidly-fatal).
Around 1% of CLL terminates as ALL ("blast crisis of CLL").
69
Chronic Lymphocytic Leukemia (CLL)

70
Summary
Leukemias – Starts in marrow spread to blood Anemia, infections & Bleeding Enlargement of Liver, Spleen lymph nodes Acute/Chronic & Myeloid & Lymphoid.

71
THANK YOU!


















