1. INTRODUCTION 2. DEVELOPMENT OF THE PANCREAS
18
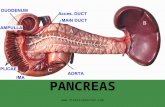
1. INTRODUCTION 2. DEVELOPMENT OF THE PANCREAS 3. DEVELOPMENT OF CELL-BASED THERAPIES FOR DIABETES 4. FETAL TISSUE AS SOURCE FOR ISLET CELLS 5. ADULT TISSUE AS SOURCE FOR ISLET CELLS 6. EMBRYONIC STEM CELLS 7. FUTURE DIRECTIONS
-
Upload
lysandra-jarvis -
Category
Documents
-
view
20 -
download
3
description
1. INTRODUCTION 2. DEVELOPMENT OF THE PANCREAS 3. DEVELOPMENT OF CELL-BASED THERAPIES FOR DIABETES 4. FETAL TISSUE AS SOURCE FOR ISLET CELLS 5. ADULT TISSUE AS SOURCE FOR ISLET CELLS 6. EMBRYONIC STEM CELLS 7. FUTURE DIRECTIONS. INTRODUCTION. Diabetes Mellitus. - PowerPoint PPT Presentation
Transcript of 1. INTRODUCTION 2. DEVELOPMENT OF THE PANCREAS

1. INTRODUCTION2. DEVELOPMENT OF THE PANCREAS3. DEVELOPMENT OF CELL-BASED THERAPIES FOR DIABETES4. FETAL TISSUE AS SOURCE FOR ISLET CELLS5. ADULT TISSUE AS SOURCE FOR ISLET CELLS6. EMBRYONIC STEM CELLS7. FUTURE DIRECTIONS

Diabetes Mellitus
Type 1 DM( beta cell destruction) - Immune-mediated - Idiopathic
Type 2 DM( insulin resistance and/or deficiency)
INTRODUCTION
- Control of blood glucose and Symptoms - Prevention of chronic complications
- Diet - Exercise - Pharmacotherapy
- Oral agent - Insulin
Problem; chronic complications
Current Treatment of Diabetes

Complications of DM
Heart disease; x2-4 higherStroke; x4 higherHigh blood pressure ; 73% of hypertensive ptBlindness; leading cause of new cases Kidney disease; leading cause of end-stage renal disease, 44% of new casesNervous system disease; About 60 percent to 70 percent of people with diabetes Amputations; More than 60 percent of nontraumatic lower-limb amputations Dental disease; one-third of people with diabetes Complications of pregnancyOther complications

0%
20%
40%
60%
0 3 6 9 12 15
% o
f pa
tient
s w
ith a
n ev
ent
Years from randomisation
Intensive (2729)
Conventional (1138)
Risk reduction 12%(95% CI: 1% to 21%)
p=0.029
UKPDSAny Diabetes Related Endpoint (cumulative )
UK Prospective Diabetes Study
- multi-centre- randomized controlled trial: of different therapies of Type 2 diabetes
UKPDS : need for a long-term study
complications of Type 2 diabetes developover decades
Protocol written 1976Recruitment 1977-1991End of study Sept. 1997
Clinical Centres 23Type 2 diabetic patients 5102Person years follow-up 53,000

Any Diabetes Related EndpointFirst occurrence of any one of: 1401 of 3867 patients (36%)
- diabetes related death - non fatal myocardial infarction, heart failure or angina - non fatal stroke - amputation - renal failure - retinal photocoagulation or vitreous haemorrhage - cataract extraction or blind in one eye
The Effect of Intensive Treatment of Diabetes on the Development and Progression of
Long-Term Complications in Insulin-Dependent Diabetes Mellitus
The Diabetes Control and Complications Trial Research Group
Cumulative Incidence of Urinary AlbuminExcretion 300 mg per 24 Hours (Dashed Line) and 40 mg per 24 Hours (Solid Line) in Patients with IDDM Receiving Intensive or Conventional Therapy
329:977-986 (1993)

New Treatment of Diabetes
- Transplantation- Whole or segmental pancreas transplantation- Islet transplantation
- Implantable devices Closed loop systems
Bio-responsive membrane Pump, insulin reservoir and glucose sensor- Hybrid artificial pancreas
- Gene Therapy
Islet Cell Transplantation
- Attractive possibility for the treatment of diabetes - Reversibility of late complication - More safer and simpler than pancreas transplantation
- Auto-transplantation: Chronic Pancreatitis, trauma- Allo-transplantation
Type 1 DM with renal problem (Limited indication) Type 2 DM with kidney transplantation.

The Benefits of Islet Transplant
- No need for insulin therapy - Improved glucose control (provided graft function persists)- Elimination of comas, hypoglycemic reactions & metabolic labiality- Normal HbA1C (impossible with intensive insulin therapy)- Prevention/stabilization/reversal of early 2º complications- Better quality of life- Much lower risk than whole (vascularized) pancreas transplant

Total Number of Adult islet allografts 1974-2000: 445
Cumulative 3 year patient and graft survival in C-peptideNegative type-1 Diabetic Recipients: 1990-1997: n=200

Islet Volume 11,547±1,604 EIN/kg
Steroid free Immunosuppression
Silolimus(Rapamune, Wyeth-Ayerst)tacrolimus(Prograf, Fujisawa)Daclizumab(Zenapax, Roche): IL-2R mAb
Blood glucose levels: Before and after islet transplantation

Barriers of Islet TransplantationBarriers of Islet Transplantation
- Immunosuppression- Diabetogenic effects of some immunosuppressants- Immunological rejection- Oncogenic effects of long term use of immunosuppressive treatment
- Shortage of donor pancreas and islets
Insulin secretion cells from other source
- Genetically designed insulin secreting artificial beta-cells :- Tumor or transformed cell lines
:- Proliferating islet cells of human origin :- Fetal pancreatic tissue :- Pancreatic ductal cell ?- Stem cells: adult or embryonic
- Xenotransplantation: Animal tissue

Development Of Cell-based Therapies For Diabetes
- Source for Islet Cells :- Fetal tissue :- Adult tissue :- Embryonic stem cells
Fetal tissue
Diabetes 46(2): 244-248 (1997)
Functional beta-Cell Mass After Transplantation of Human Fetal Pancreatic Cells: Differentiation or Proliferation?Beattie, Gillian M.; Otonkoski, Timo; Lopez, Ana D.; Hayek, Alberto
Comparison of insulin content; fetal islets, freshly isolated islets and ICCs
ß-Cell Differentiation from a Human Pancreatic Cell Line in Vitro and in Vivo
D. Dufayet de la Tour, T. Halvorsen, C. Demeterco, B. Tyrberg, P. Itkin-Ansari, M. Loy, S.-J. Yoo, E. Hao, S. Bossie & F. Levine
Molecular Endocrinology 15 (3): 476-483
- transformed pancreatic ß-cell lines :- expression of dominant oncogenes transcription factor PDX-1
- Major problem :- Balance growth and differentiation
Growth (+) cell: insulin secretion(-) Insulin secretion(+) cell: no proliferation

Adult tissue
- Islet progenitor cells? :- Pancreatic ductal cells
:- CHIBs (cultivated human islet buds) :- Subset of stem-cell like islet progenitor cells
:- Nestin positive cells
CHIBs(Cultivated Human Islet Buds)
Pancreatic ductal cell culture
immunostained for pan-cytokeratin (FITC green); Insulin-positive cells (Texas red)
Cultivated Human Islet Buds(CHIBs)
20 mM glucose
5 mM glucose

Diabetes 2001 50: 521-533
Stem-like Cells Within Islet and Duct
Expression of the neural stem cell–specific markernestin in a distinct cell population within pancreaticislets
Nestin-positive cells are expressed in localized regions of the ducts in the rat pancreas
Secretion of pancreatic endocrine hormones from differentiation human NIP cells

Embryonic stem cells
Mouse ES cellsDiabetes 2000 49:157-162
ES derived insulin secreting cells
Glucose-induced insulinrelease in IB/3x-99 cells
Changes in blood glucose levels after implantation of IB/3x-99 cells

ES cells generate insulin-positive cells that associate with neurons
Double-immunofluorescence staining for insulin/nestin during and at the end of stage 3,and for insulin-[ beta] -III tubulin at the end of stages 4 and 5.Bar,100 µ m
Insulin-producing cells contain different hormone-producing cell types and are organized in three-dimensional clusters with topological organization similar to pancreatic islets

Islet clusters release insulin in response to glucose using normal pancreatic mechanisms

Diabetes 2001 50: 1691-1697
Human ES cells
Differentiation of hES cells in suspension culture
Insulin-expressing cells in EBs
Normal Human pancreas EBs at day 19 after differentiation
Insulin secretion at various glucose concentrations and growth conditions

Pluripotent Stem cells
Inner cell massES
Primordial Gonads EG Teratocarcinoma
EC
Adult
BrainBone marrowMuscleSkinIntestinal Epithelia •In vitro differentiation
•Cell-lineage selection•Maturation
Beta-cell
Cell transplantation
Ductal Cells
Summary









![Human pancreas developmentdev.biologists.org/content/develop/142/18/3126.full.pdf · Human pancreas development ... (dpc)]; this is subtly 1Centre for Endocrinology and Diabetes,](https://static.fdocuments.in/doc/165x107/5b95d55b09d3f2d7438ce05c/human-pancreas-human-pancreas-development-dpc-this-is-subtly-1centre.jpg)