1 Intervention Delivery Approaches AKA How do we get the interventions delivered? Horizontal vs....
35
1 Intervention Delivery Approaches AKA How do we get the interventions delivered? Horizontal vs. Vertica l Comprehensive Comprehensive vs. Selective Selective Approaches Approaches Facility vs. community based approach Social marketing? Reduced cost? Give away? Disease Eradication/Elimination PHC approach? ntegrated approach? Target universal population? Target the poor?
-
Upload
shon-hampton -
Category
Documents
-
view
218 -
download
0
Transcript of 1 Intervention Delivery Approaches AKA How do we get the interventions delivered? Horizontal vs....

1
Intervention Delivery Approaches AKA How do we get the interventions delivered?
Horizontalvs.
Vertic
al ComprehensiveComprehensive vs. SelectiveSelective Approaches
ApproachesFacility vs. community based approach
Social marketing?
Reduced cost?
Give away?
Disease Eradication/Elimination
PHC approach?Integrated approach?
Target universal population?Target the poor?
Session Learning Objectives
1. Define various strategies for implementing MCH interventions including intersectoral, vertical, comprehensive, primary health care, integrated, social marketing, community-based, facility-based, universal and targeted approaches
2. Describe trends / historical context of various MCH implementation strategies
3. Compare the advantages and disadvantages of the major strategies used in MCH programming
4. Explain the successes and weaknesses of the IMCI strategy as it has been executed
Session Structure
1. Why studies strategies for intervention delivery?
2. Historical basis of strategies
3. Review strategies in the context of VPDs, malaria, injuries
4. IMCI
4
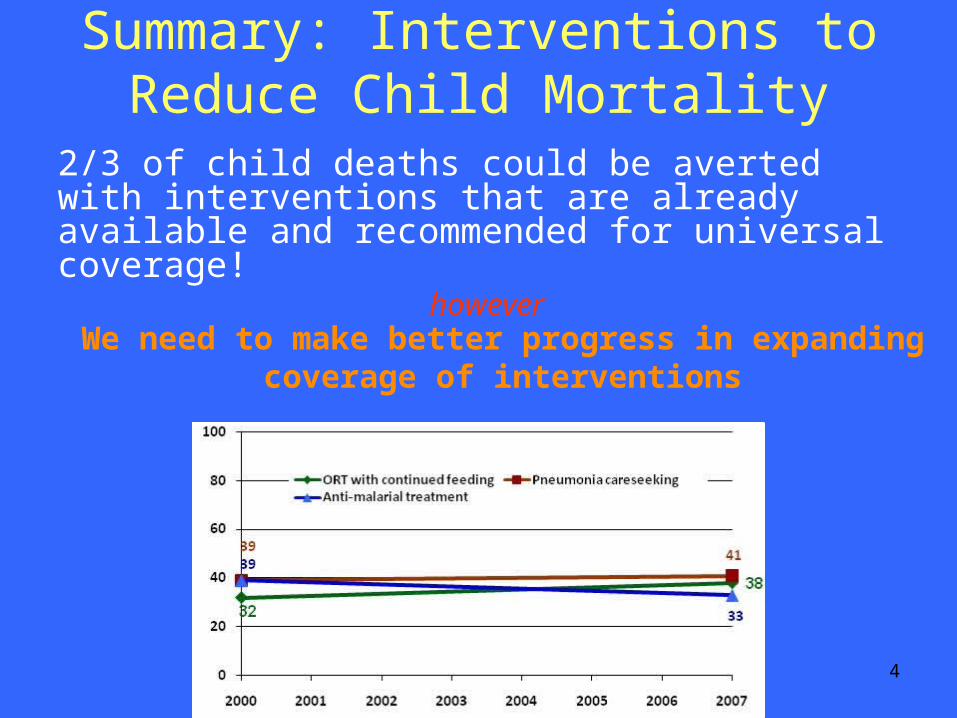
Summary: Interventions to Reduce Child Mortality
2/3 of child deaths could be averted with interventions that are already available and recommended for universal coverage!
however
We need to make better progress in expanding coverage of interventions
Interventions (What)
vs.
Strategy/Approach (How)
6
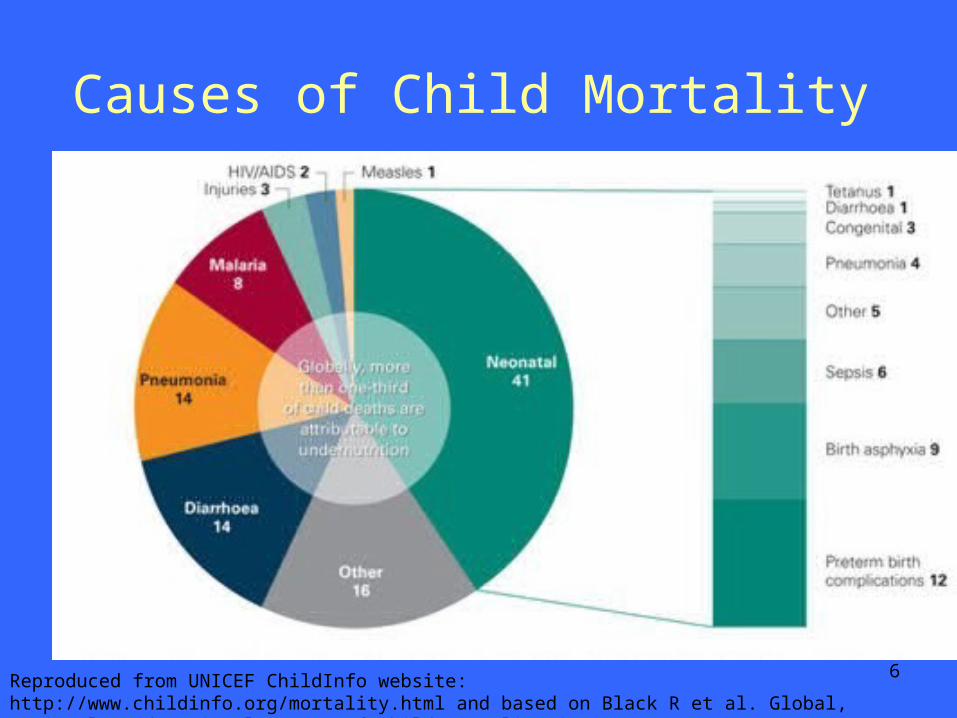
Causes of Child Mortality
Reproduced from UNICEF ChildInfo website: http://www.childinfo.org/mortality.html and based on Black R et al. Global, regional, and national causes of child mortality in 2008. Lancet. 2010;375:1969–1987.
Expanded Program on Immunizations (EPI)
• Established 1974
• Individual countries create and implement their own vaccination program policies
• Universal immunization with standard vaccinations
– Ensure full immunization of children under age one in every district
– Eradicate polio, reduce measles and neonatal tetanus deaths 7
Expanded Program on Immunizations (EPI)
• Expand access to relevant new vaccines
• Expand target groups to older children, adolescents and adults as needed
• Work in synergy with other public health programs
8
9
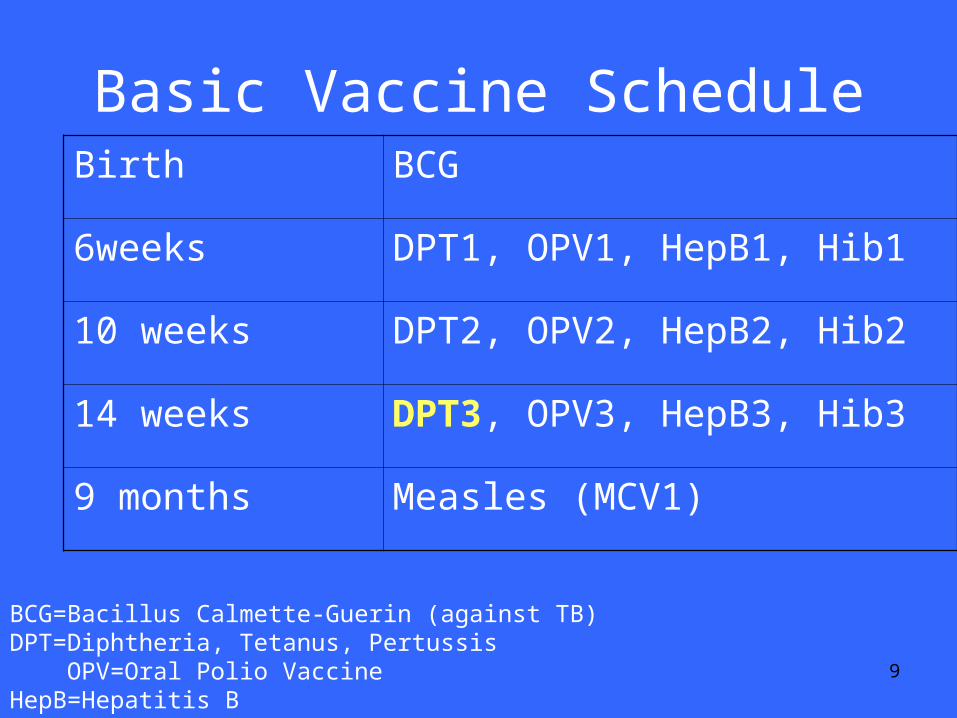
Basic Vaccine ScheduleBirth BCG
6weeks DPT1, OPV1, HepB1, Hib1
10 weeks DPT2, OPV2, HepB2, Hib2
14 weeks DPT3, OPV3, HepB3, Hib3
9 months Measles (MCV1)
BCG=Bacillus Calmette-Guerin (against TB)DPT=Diphtheria, Tetanus, Pertussis OPV=Oral Polio VaccineHepB=Hepatitis B Hib=Hemophilus influenza b
What is the Global Vaccine Coverage Rate?
11
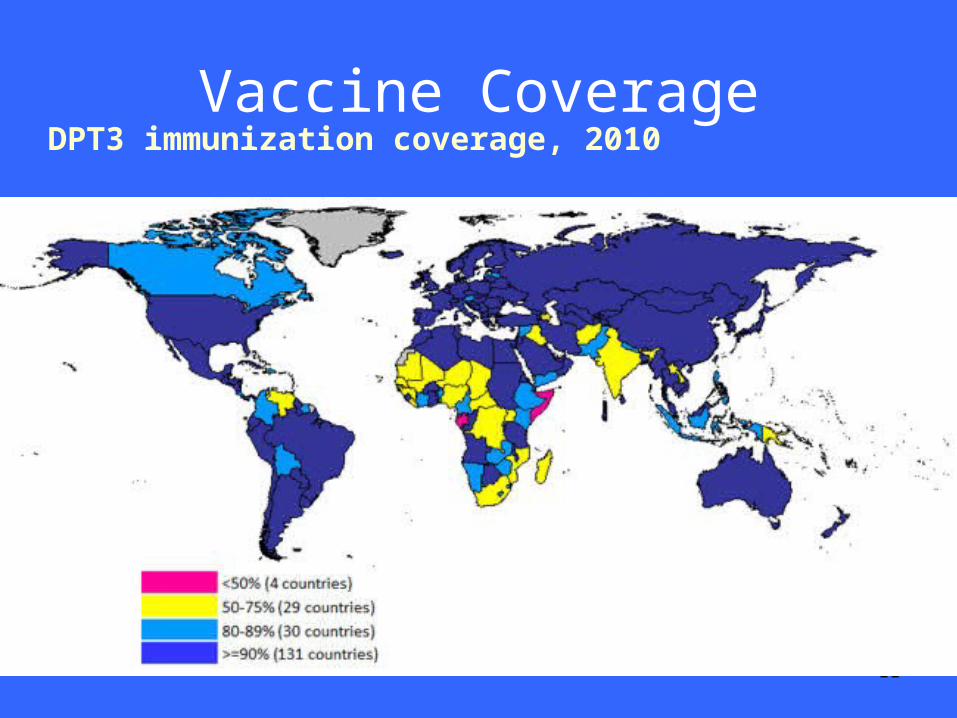
Vaccine Coverage DPT3 immunization coverage, 2010
Immunization Programs:Multifaceted and complex
12
The State of the World’s Vaccines and Immunization. WHO/UNICEF. 2002
Cost profile of immunizations
14
Malaria
• Plasmodium parasites
• Anopheles mosquito--vector – Parasites enter bloodstream via
mosquito saliva– Invade red blood cells (RBCs),
multiply there, lyse RBCs
15
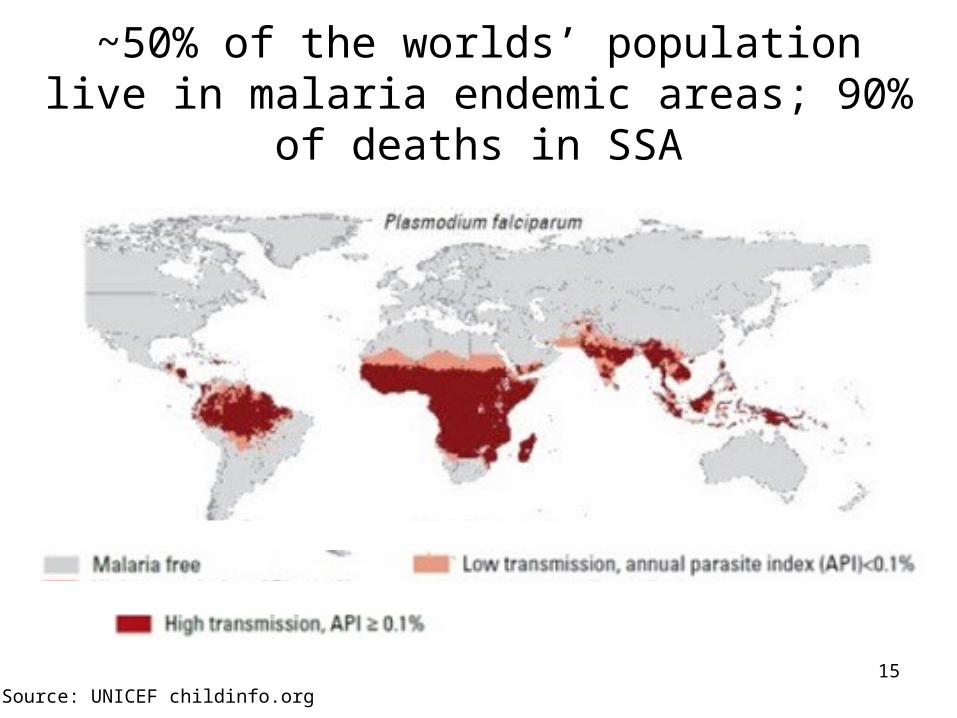
~50% of the worlds’ population live in malaria endemic areas; 90% of deaths in SSA
Source: UNICEF childinfo.org
16
Malaria: Treatment
• Intermittent Preventative Treatment of malaria in pregnancy (IPTp)
• Prompt treatment with appropriate antimalarials
17
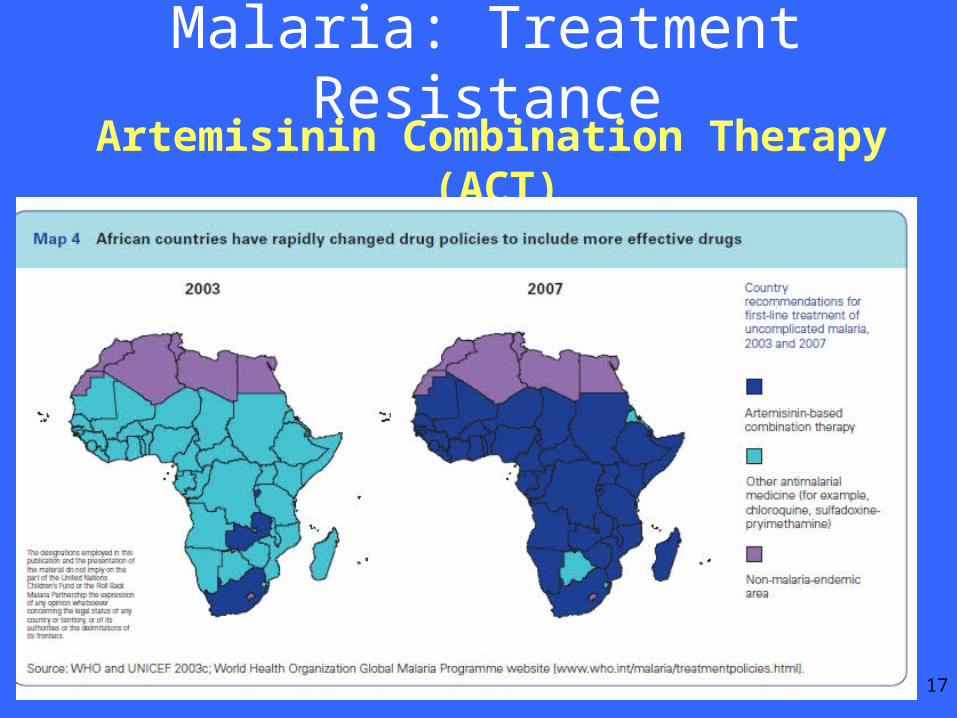
Malaria: Treatment Resistance Artemisinin Combination Therapy (ACT)
18
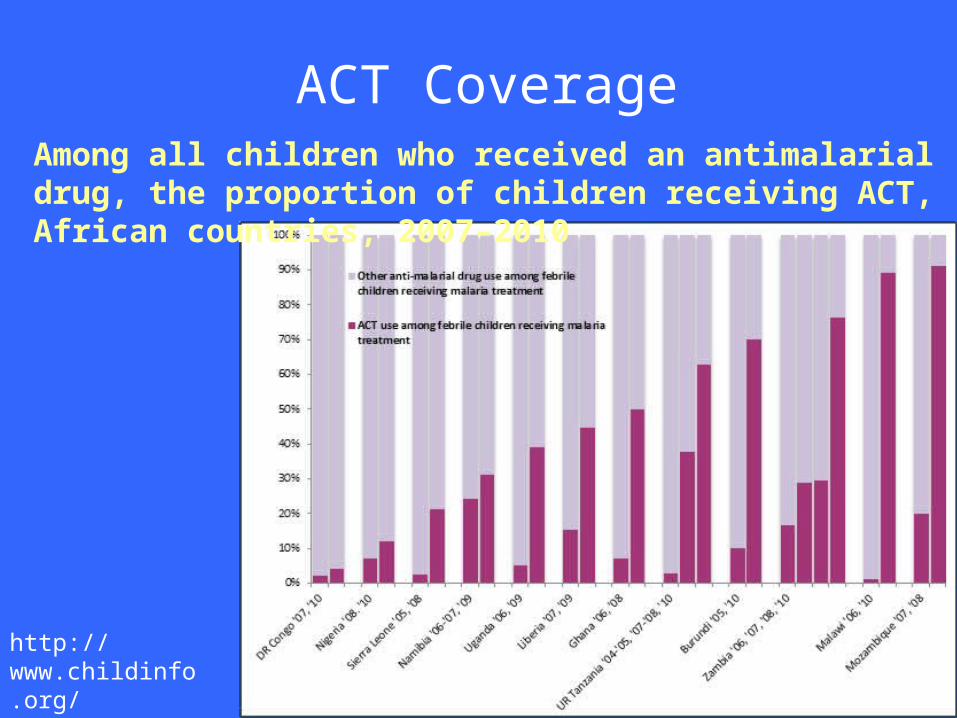
ACT Coverage
http://www.childinfo.org/malaria_progress.html
Among all children who received an antimalarial drug, the proportion of children receiving ACT, African countries, 2007–2010
19
Malaria: Prevention• Vector control
– Indoor Residual Spraying (IRS)– Environmental measures (e.g. reduction of
standing water)
Insecticide Treated Nets (ITNs)• High ITN use 17% reduction in childhood
mortality
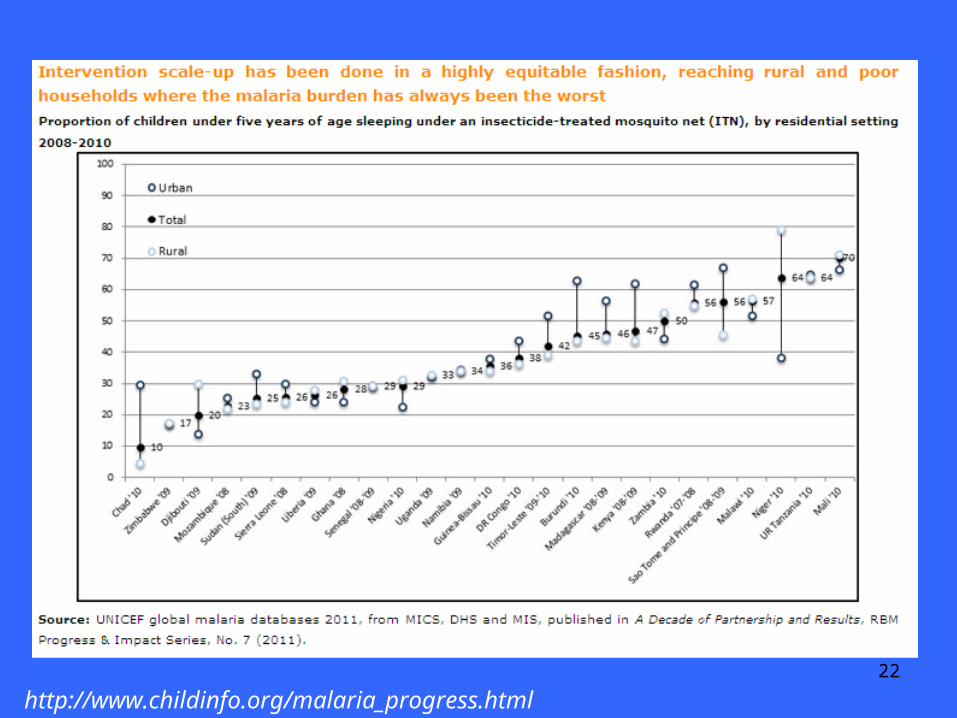
http://www.childinfo.org/malaria_progress.html
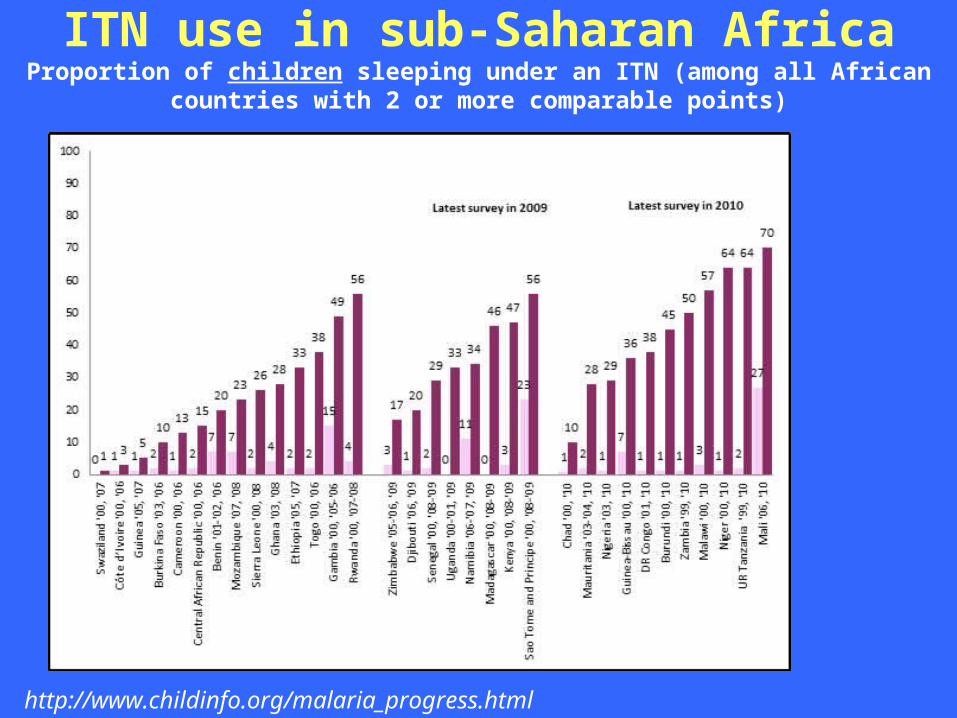
ITN use in sub-Saharan AfricaProportion of children sleeping under an ITN (among all African countries with 2
or more comparable points)
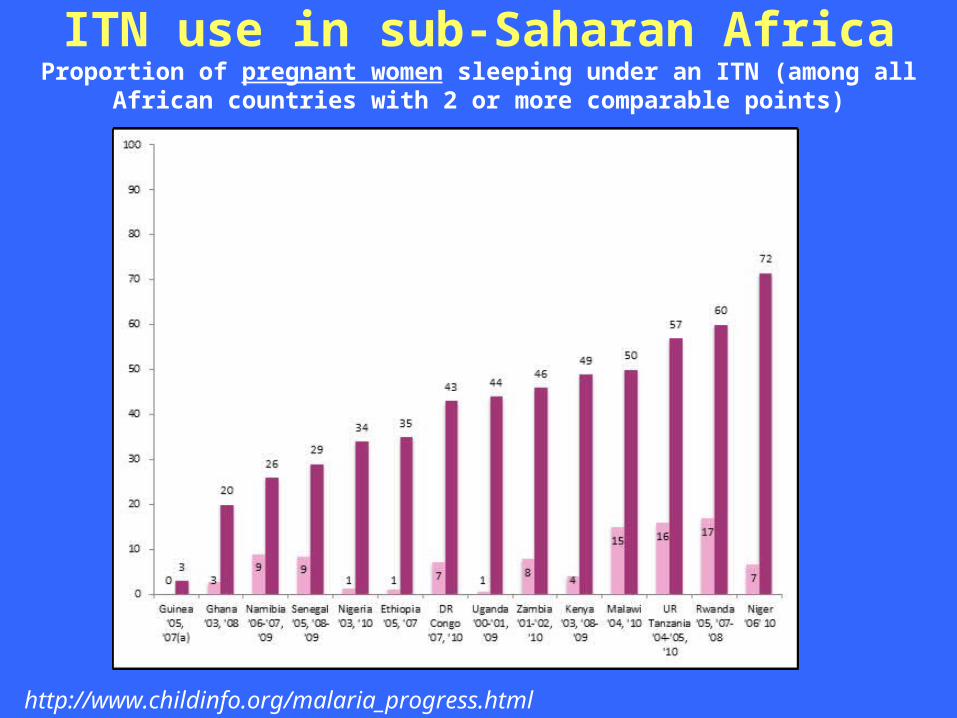
http://www.childinfo.org/malaria_progress.html
ITN use in sub-Saharan AfricaProportion of pregnant women sleeping under an ITN (among all African countries
with 2 or more comparable points)
22
http://www.childinfo.org/malaria_progress.html
23
ITN Distribution in Ghana
Childhood Injuries
• Burns, pedestrian injuries, drowning, falls
• 250,000 deaths of children <5 years
• Most injuries are preventable
• Multi-sector approach to prevent injuries
• Simple protocols can reduce fatality and disability
Session Structure
1. Why studies strategies for intervention delivery?
2. Historical basis of strategies
3. Review strategies in the context of VPDs, malaria, injuries
4. Integrated care / IMCI

Problems with unintegrated care and selective
programming: Example of HIV infected woman
AIDS treatment center of excellenceT&C, ARVs, PMTCT drugs, condoms ANC
FP ClinicBirth controls, condoms
TB clinic
Health post—Malaria, other illness
27
Integrated Management of Childhood Illnesses (IMCI)
• integrated approach
• to reduce death, illness and disability, and to promote growth and development
• preventive and curative elements
• implemented by families, communities and health facilities
28
Three Components of IMCI
• Improves health worker skills
• Improves health systems
• Improves family and community practices
29
IMCI Component 1: Improve Health Worker Skills
• Targets first level health facilities
• Addresses causes of at least 70% of deaths
• Case management guidelines
• Training
• Supervision
• Monitoring
30
IMCI Addresses Most Causes of Death
• Pneumonia• Diarrhea• Measles• Malaria• Malnutrition
• Sepsis• Meningitis• Dehydration• Anemia• Ear infection• HIV/AIDS• Wheezing

31
IMCI Component 2: Improve Family and Community
Practices
• Community participation
• Preventive care– Immunization– Breast-feeding and other nutritional counseling
• Home care of sick children
• Recognition of severe illness
• Care-seeking behavior
32
IMCI Component 3: Improves Health Systems
• Planning and Management
• Availability of drugs and supplies
• Organization of work
• Monitoring and supervision
• Referral pathways and systems
• Health information systems
33
IMCI Multicountry Evaluation• Training health workers improved
performance
• Difficult to maintain & expand existing IMCI sites
• District and national health systems lack sufficient management structure, funding, coordination, supervision, and manpower
• Low utilization rates of health services IMCI cannot impact child mortality
34
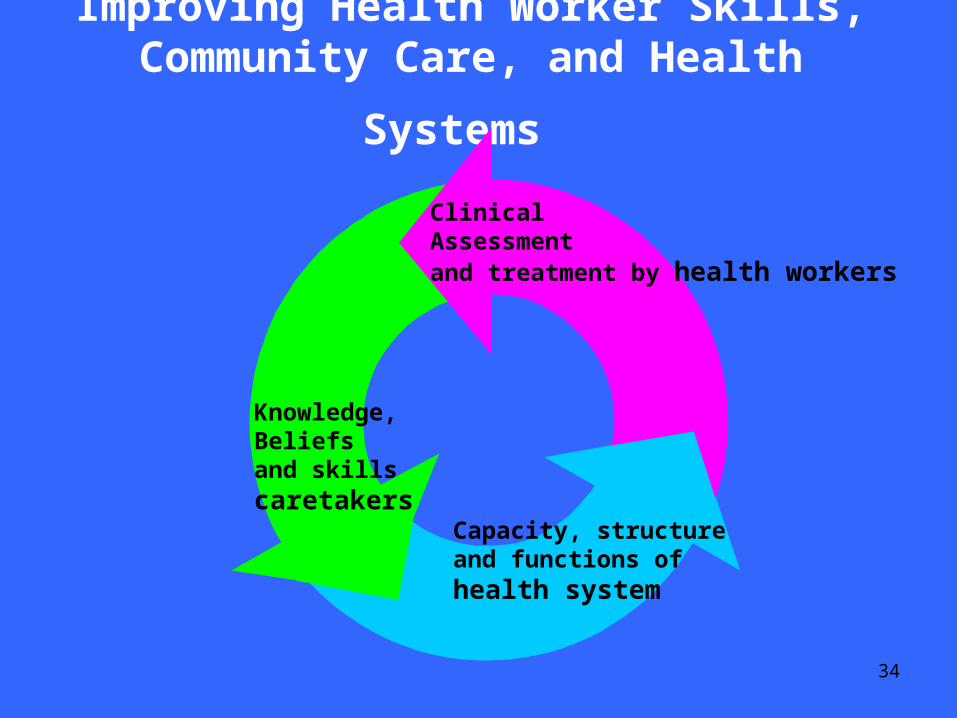
Improving Health Worker Skills,
Community Care, and Health Systems
Capacity, structureand functions ofhealth system
Knowledge,Beliefs and skills caretakers
ClinicalAssessmentand treatment by health workers
35
Conclusion
• Most maternal and child deaths are due to a select number of causes
• Effective interventions exist that are cost effective, feasible and recommended for implementation and can eliminate 2/3 of childhood deaths
• Need effective strategies to deliver interventions, especially to the poorest populations
• Need involved communities and strong health systems